volumetric and functional assessment of ventricles in
TRANSCRIPT

Circulation Journal Vol.77, January 2013
Circulation JournalOfficial Journal of the Japanese Circulation Societyhttp://www.j-circ.or.jp
emodynamic pressure data are indispensable in the treatment and diagnosis of pulmonary hypertension (PH), but are available only using an invasive tech-
nique. Two-dimensional (D) echocardiography (2DECHO) is a non-invasive diagnostic tool for evaluation of PH patients that provides useful information such as estimated right ven-tricle systolic pressure (RVSP), morphological aspects of the heart, systolic function/wall motion of the ventricles, and tri-cuspid regurgitation (TR) grade. Its usefulness, however, is limited, especially for the quantitative assessment of right ven-tricle (RV) morphology and function.1–3 For instance, RVSP sometimes remains constant or even decreases against an in-
crease in pulmonary vascular resistance (PVR) in cases in which cardiac output (CO) cannot be maintained by failing RV, which is regarded as an afterload mismatch of failing RV. In addition, RVSP may further tend to decrease when the amount of pulmonary flow is reduced as TR increases. Thus, in the presence of advanced RV failure with or without sig-nificant TR, RVSP by itself is no longer reliable to assess PVR or the severity of PH, and may be misleading. Therefore, in-vasive collection of hemodynamic data using a right-sided catheter examination is sometimes needed. Recently, the real-time 3-D echocardiography (3DECHO) technique has been reported to provide reliable volumetric data for the RV as well
H
Received February 14, 2012; revised manuscript received August 3, 2012; accepted September 3, 2012; released online September 28, 2012 Time for primary review: 36 days
Department of Cardiovascular Medicine, Graduate School of Medicine, University of Tokyo, Tokyo (T. Inaba, A.Y., T.N., M.H., H.M., T. Imamura, T. Shiga, T.Y., M.S., K.K., J.S., K.T., Y.H., R.N.), Japan; Cedars-Sinai Medical Center and David Geffen School of Medicine at UCLA, Los Angeles, CA (T. Shiota), USA
Mailing address: Atsushi Yao, MD, PhD, Department of Cardiovascular Medicine, Graduate School of Medicine, University of Tokyo, 7-3-1 Hongo, Bunkyo-ku, Tokyo 113-8655, Japan. E-mail: [email protected]
ISSN-1346-9843 doi: 10.1253/circj.CJ-12-0203All rights are reserved to the Japanese Circulation Society. For permissions, please e-mail: [email protected]
Volumetric and Functional Assessment of Ventricles in Pulmonary Hypertension on 3-Dimensional
EchocardiographyToshiro Inaba, MD; Atsushi Yao, MD, PhD; Tomoko Nakao, MD, PhD; Masaru Hatano, MD;
Hisataka Maki, MD; Teruhiko Imamura, MD; Taro Shiga, MD, PhD; Tadashi Yamazaki, MD, PhD; Makoto Sonoda, MD, PhD; Koichiro Kinugawa, MD, PhD;
Takahiro Shiota, MD, PhD; Junichi Suzuki, MD, PhD; Katsu Takenaka, MD, PhD; Yasunobu Hirata, MD, PhD; Ryozo Nagai, MD, PhD
Background: Non-invasive assessment of volume and function on the right ventricle (RV) for pulmonary hyperten-sion (PH) is limited.
Methods and Results: Patients with PH (n=23) underwent 3-dimensional (D) echocardiography (3DECHO), with cardiac magnetic resonance imaging to confirm its precision, and right heart catheterization. On linear regression analysis the RV end-systolic volume index (ESVI) was positively correlated with pulmonary vascular resistance (PVR) and mean pulmonary arterial pressure (mPAP; R=0.42 and 0.46, P=0.03 and 0.03, respectively). The RV end-diastolic volume index (EDVI) was positively correlated with mPAP (R=0.41, P<0.05). The left ventricular (LV) EDVI was inversely correlated with PVR (R=−0.48, P=0.02). The RV ejection fraction was inversely correlated with PVR and mean right atrial pressure (mRAP; R=−0.57, and −0.45, P=0.004, and 0.03, respectively). RVEDVI/LVEDVI and RVESVI/LVESVI (the diastolic and systolic remodeling indices, respectively) had a significantly positive linear relationship with PVR (R=0.67 and 0.55, P=0.0005 and 0.006, respectively), and the former had a significantly positive linear relationship with mRAP (R=0.42, P<0.05). During the recovery process in 1 specific case, the remod-eling indices maintained a significant linear relationship with the hemodynamic parameters.
Conclusions: Novel indices provided by 3DECHO may be utilized as alternative indicators of hemodynamic changes in PH patients. (Circ J 2013; 77: 198 – 206)
Key Words: 3-D echocardiography; Magnetic resonance imaging; Pulmonary hypertension; Pulmonary vascular resistance; Remodeling index
ORIGINAL ARTICLEPulmonary Circulation

Circulation Journal Vol.77, January 2013
1993DECHO for PH
as the left ventricle (LV).4–10 Using software for volumet-ric analysis (QLAB-3DQadv 7.0, Philips Medical Systems, Andover, MA, USA), we can directly calculate volumes of objects in various shapes on 3DECHO. The aim of the present study was to propose volumetric indices of 3DECHO relevant to the assessment of PH severity.
MethodsSubjectsWe studied 23 consecutive Japanese patients with PH, who were admitted to the University of Tokyo Hospital for diagno-sis or evaluation from January 2007 to September 2010, and who underwent both right-sided catheter examination and 3DECHO. The patient characteristics are listed in Table. This study was performed in full compliance with the most recent amendment of the Declaration of Helsinki and good clinical practice and was approved by the institutional review commit-tee. All subjects gave informed consent.
3DECHOAll patients underwent real-time 3DECHO within 7 days of a right-sided catheter examination. The 3DECHO recording of the LV and RV was performed from the apical window using the Sonos iE33 ultrasound system (Philips Medical Systems, Tokyo, Japan) with an X3-1 matrix array transducer (1.0–3.0 MHz, 2400 elements, Philips Medical Systems) through a full-volume procedure.11 Data acquisition was performed dur-ing breath-holding as triggered by the electrocardiogram (ECG) R-wave of every other heartbeat for a total of 4 heartbeats. All images were stored on a compact disk and transferred for offline analysis using QLAB-3DQadv version 7.0 software (Philips Medical Systems). By placing a total of 5 sample dots (4 in the mitral/tricuspid annulus and 1 in the apex) at the end of the diastolic and systolic frames, a semiautomatic tracing of the endocardial border through the entire cardiac cycle was made, which was followed by manual correction at the ends of the diastolic and systolic frames. Manual correction of the tracing of the endocardial border between the blood pool and myocardium was performed at the ends of the diastolic and systolic frames. After the entire 3-D ventricular cavity was reconstructed at the end of diastole and systole, the end-dia-stolic volume for the LV and RV (LVEDV and RVEDV, re-spectively) and the end-systolic volume for the LV and RV (LVESV and RVESV, respectively) were calculated. The stroke volume for the LV and RV (LVStV and RVStV, respectively) and the ejection fraction for the LV and RV (LVEF and RVEF, respectively) were then calculated. The volume data were di-vided by the body surface area and expressed as an index (denoted as I and added to the end of the name). The echocar-diography recordings and measurements were performed sep-arately and independently by 3 different cardiologists without prior knowledge of the magnetic resonance imaging (MRI) or hemodynamic data.
MRI Volume MeasurementTo confirm the precision of the 3DECHO measurements, MRI measurement was performed independently by another cardi-ologist for 10 of the patients within 7 days of the 3DECHO using the Magnetom Avanto MRI system (Siemens, Erlangen, Germany) with a 1.5-T superconducting magnet as described previously.12,13 Cine loops of LV short-axis images were ob-tained using a steady-state free precession pulse sequence im-aging (true fast imaging with steady precession: FISP). Imag-ing parameters were an echo time of 1.5 ms for FISP, a flip
angle of 30°, a data acquisition matrix of 140×256, and a field of view of 350×350 mm for both sequences. The time delay for the first data acquisition window for the end of diastole was 0 ms after the trigger of the R-wave in the ECG and the window was moved toward the end of the cardiac cycle in increments of 40 ms. The end of systole was defined as the instant when the data set of the smallest areas of the LV blood pool was obtained. The entire LV was encompassed by acquir-ing 10-mm-thick contiguous short-axis cine loops with no interslice gaps. All measurements were collected using stan-dardized MRI display parameters that were calculated with nuclear MRI intensities of the myocardium and the LV blood pool on each MRI image.13,14 The window center was defined as the mean intensity of the myocardium and blood pool, and the window width was calculated by multiplying the intensity difference between the blood pool and LV myocardium by 3. LVEDV, LVESV, RVEDV, and RVESV were calculated by summing the entire area of intraventricular cavity on every short-axis cine MRI image at the end of diastole and systole, respectively. Digital Imaging and Communications in Medi-cine (DICOM) software (DxMM; Medasys, Gif-sur-Yvette, France) was used for volume measurement.
Table. Patient Characteristics
n 23
Age (years) 55.3±17.2 (20–81)
Sex (F/M) 19/4
Etiology
IPAH/HPAH 5
Collagen 13 (SSC 10, SLE 1, MCTD 2)
Congenital 2 (ASD 1, VSD 1)
Portal hypertension 2
CTEPH 1
Hemodynamics
mRAP (mmHg) 4.3±2.5 (1–11)
mPAP (mmHg) 47.0±12.8 (26–73)
CI (L · min–1 · m–2) 2.2±0.6 (1.0–3.8)
PVR (dyne · s–1 · cm–5) 1,122±652 (295–2,942)
3DECHO volume data
LVEDVI (ml/m2) 40.4±18.8
LVESVI (ml/m2) 14.7±9.4 LVStVI (ml/m2) 25.7±10.9
LVEF (%) 0.65±0.11
RVEDVI (ml/m2) 72.5±27.5
RVESVI (ml/m2) 44.7±22.2
RVStVI (ml/m2) 27.8±11.5
RVEF (%) 0.40±0.13
Data given as mean ± SD (range).ASD, atrial septal defect; CI, cardiac index; CTEPH, chronic throm-boembolic pulmonary hypertension; DECHO, dimensional echo-cardiography; HPAH, heritable pulmonary arterial hypertension; IPAH, idiopathic pulmonary arterial hypertension; LVEDVI, left ventricular (LV) end-diastolic volume index; LVEF, LV ejection fraction; LVESVI, LV end-systolic volume index; LVStVI, LV stroke volume index; MCTD, mixed connective tissue disease; mPAP, mean pulmonary arterial pressure; mRAP, mean right atrial pres-sure; PVR, pulmonary vascular resistance; RVEDVI, right ventric-ular (RV) end-diastolic volume index; RVEF, RV ejection fraction; RVESVI, RV end-systolic volume index; RVStVI, RV stroke volume index; SLE, systemic lupus erythematosus; SSC, systemic scle-rosis; VSD, ventricular septal defect.

Circulation Journal Vol.77, January 2013
200 INABA T et al.
Right-Sided Catheter ProcedureAll 23 patients received a right-sided catheter examination in which the hemodynamic data were obtained by cardiologists independently of 3DECHO and MRI in a blind manner as described as follows. A 7-F Swan-Ganz catheter (Nihon
Kohden, Tokyo, Japan) was introduced from the femoral or jugular vein. The hemodynamic parameters were then obtained in the order of mean right atrial, mean pulmonary capillary wedge, and mean pulmonary arterial pressures (mRAP, mPCWP, and mPAP, respectively). Then, blood samples for
Figure 1. Comparison of 3-D echocardiography (3DECHO) and magnetic resonance imaging (MRI) measurements. Linear regres-sion analysis clearly showed that LV end-diastolic volume index (LVEDVI), LV end-systolic volume index (LVESVI), LV stroke volume index (LVStVI), LV ejection fraction (LVEF), RV end-diastolic volume index (RVEDVI), RV end-systolic volume index (RVESVI), RV stroke volume index (RVStVI), and RV ejection fraction (RVEF) measured using 3DECHO were well correlated with and matched those measured on MRI. LV, left ventricular; RV, right ventricular.
Circulation Journal Vol.77, January 2013
2013DECHO for PH
the calculation of Fick CO and cardiac index (CI) were ob-tained from the main pulmonary and femoral arteries. None of the present patients had a left-to-right or right-to-left shunt. Fick CO (L/min) was calculated with the general formula: CO=O2 consumption (ml/min)/arteriovenous oxygen difference (ml/L). The pressure data are expressed as mmHg, and PVR (dyne · s–1 · cm−5) was calculated by the formula: 80 × (mPAP – mPCWP) / CO.
Statistical AnalysisThe data are expressed as mean ± SD. Linear regression analy-sis was performed using Origin version 7.5 software (OriginLab, Northampton, MA, USA). P<0.05 was considered statistically significant.
ResultsComparison of 3DECHO and MRI Volume DataAs shown in Figure 1, the RVEDVI, RVESVI, LVEDVI, and LVESVI raw 3DECHO data were all well-matched with the MRI data. LVStVI, RVStVI, LVEF, and RVEF all showed
significant linear correlations between values obtained on 3DECHO and those on MRI. Because MRI measurement is the gold standard for RV and LV volumetric analysis, these re-sults confirm the reliability of the 3DECHO measurements.
3D Ventricular Volume and Hemodynamics: Patient CharacteristicsAs shown in Table, 3DECHO measurements showed enlarged RVs and small LVs as represented by RVEDVI and LVEDVI, referring to normal values of 3DECHO recently reported in a healthy Japanese population.9 Moreover, RVEF was diminished, while LVEF was maintained at normal levels. An enlarged RV cavity with a decreased RVEF and compressed LV cavity with a preserved LVEF is consistent with the characteristics generally recognized in patients with PH.15 Hemodynamic data have shown moderately increased PVR (mPAP) with mildly decreased CI in these patients.
3DECHO Ventricular Volume Indices and Hemodynamic ParametersWe examined the correlation of the 3DECHO volume data on
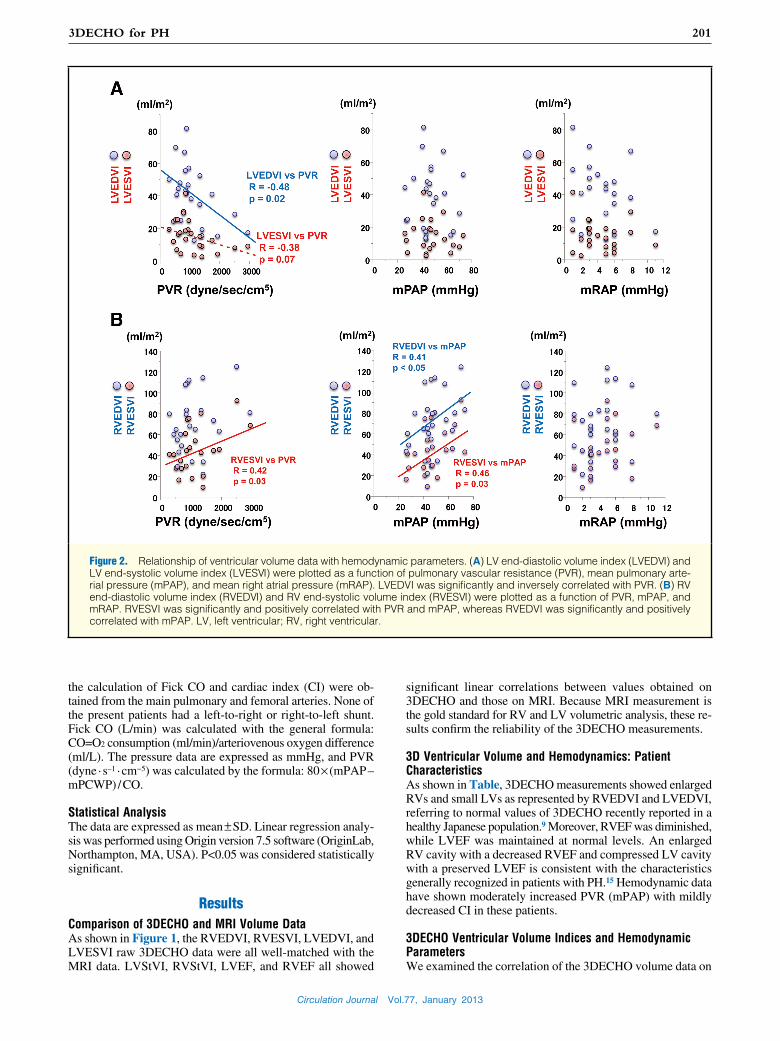
Figure 2. Relationship of ventricular volume data with hemodynamic parameters. (A) LV end-diastolic volume index (LVEDVI) and LV end-systolic volume index (LVESVI) were plotted as a function of pulmonary vascular resistance (PVR), mean pulmonary arte-rial pressure (mPAP), and mean right atrial pressure (mRAP). LVEDVI was significantly and inversely correlated with PVR. (B) RV end-diastolic volume index (RVEDVI) and RV end-systolic volume index (RVESVI) were plotted as a function of PVR, mPAP, and mRAP. RVESVI was significantly and positively correlated with PVR and mPAP, whereas RVEDVI was significantly and positively correlated with mPAP. LV, left ventricular; RV, right ventricular.

Circulation Journal Vol.77, January 2013
202 INABA T et al.
Figure 3. Relationship of right ventricular ejection fraction (RVEF) with hemodynamic parameters. RVEF was significantly and inversely correlated with pulmonary vascular resistance (PVR) and mean right atrial pressure (mRAP), while RVEF and mean pulmonary arterial pressure (mPAP) showed a tendency toward a linear relationship.
Figure 4. Relationship between the remodeling indices and hemodynamic parameters. The diastolic (A) and systolic remodeling indices (B) (right and left ventricular end-diastolic volume index [RVEDVI/LVEDVI] and right and left ventricular end-systolic volume index [RVESVI/LVESVI], respectively) were plotted as a function of pulmonary vascular resistance (PVR), mean pulmonary arte-rial pressure (mPAP), and mean right atrial pressure (mRAP). A strong correlation existed between the remodeling indices and PVR and weak correlation existed and between RVEDVI/LVEDVI and mRAP.

Circulation Journal Vol.77, January 2013
2033DECHO for PH
LV and RV with the mRAP, mPAP, and PVR hemodynamic parameters. Linear regression analysis showed that PVR pos-itively correlated with RVESVI (Figure 2B) and inversely correlated with LVEDVI (Figure 2A). mPAP showed a posi-tive correlation with RVEDVI and RVESVI (Figure 2B), while mRAP did not show any correlation (Figure 2). In con-trast, RVEF was inversely correlated with PVR and mRAP, while the correlation between RVEF and mPAP remained consistent (Figure 3).
Because an enlarged RV accompanied by a compressed LV is characteristic of PH, we proposed 2 indices defined as RVEDVI/LVEDVI and RVESVI/LVESVI, which we named as the diastolic and the systolic remodeling indices, respec-tively. Both indices showed significantly tight and positive linear relationships with PVR, albeit a weak correlation be-tween RVEDVI/LVEDVI and mRAP (Figure 4).
Ventricular Volume and Hemodynamic Parameters in the PH Recovery ProcessWe previously reported a patient with idiopathic pulmonary arterial hypertension (IPAH), who had rapidly progressed to severe PH as represented by low CI (1.0 L · min–1 · m–2) and high PVR (2,942 dyne · s–1 · cm–5) and who dramatically recov-ered to almost normal in 6 months through an aggressive combination therapy with oral drugs.16 In this patient, we per-formed a set of right-sided catheter examinations and 3DECHO before beginning the medication regimen, and at 2, 4, 10, 15, and 27 weeks afterward. We plotted the 3DECHO volume data as a control for each hemodynamic parameter as shown in Figure 5. Significant linear relationships of LVEDVI, LVESVI, RVEDVI, and RVESVI with PVR and mPAP were observed in the PH recovery process, in which the relationship between RVESVI and mPAP was extremely tight (Figures 5A,B). LVESVI showed an inverse correlation with mRAP, while RVEDVI and RVESVI had a positive correlation (Figures 5A,B). RVEF also showed a strong correlation with mPAP, a moder-ate correlation with PVR and an insignificant correlation with mRAP. The systolic and diastolic remodeling indices showed very strong correlations with all the hemodynamic parameters (Figure 5D), which further supported their usefulness as indi-cators for PH severity.
DiscussionIn the present study we have, for the first time, shown a rela-tionship between ventricular volumes and hemodynamic pa-rameters in patients with PH. Consistent with former re-ports,4,6,7 the present 3DECHO volume data are in agreement with the MRI data (Figure 1), confirming the reliability of 3DECHO measurement. Regarding the linear relationship with PVR, LVEDVI, RVESVI, RVEF and the remodeling indices were statistically significant, among which the diastolic remod-eling index (RVEDVI/LVEDVI) had the strongest correlation (Figures 2–4). Regarding the relationship with mPAP, RVESVI, RVEDVI, and the systolic remodeling index (RVESVI/LVESVI) showed a significant relationship, while RVEF and RVEDVI/LVEDVI had only a weak correlation with mRAP (Figures 2–4). Particularly, in the specific patient, the 3DECHO volumetric index maintained a significant linear relationship with the hemodynamic parameters through the recovery process, among which the remodeling indices seemed to most reflect the pa-tient’s hemodynamic status (Figure 5). Although the hemody-namic profile has remained the final determinant for the clini-cal status of patients with PH,17–22 the present data suggest that 3DECHO might be a useful, non-invasive tool, whereas the
novel indices, such as RVEDVI/LVEDVI and RVESVI/LVESVI, can be used as good indicators of PH status.
Ventricular Volumes and Hemodynamic ParametersThe main factor leading to PH is an increase in PVR due to the stenosis and occlusion of the pulmonary vessels. In addition, mRAP and mPAP have reportedly been associated with PH prognosis and severity in several clinical studies.23 In contrast, RVEDVI has been reported to be an independent predictor of hospitalization for right heart failure and mortality in patients with PH.24 Morphologically and generally speaking, PH causes RV hypertrophy and dilatation, finally resulting in RV failure and, concomitantly, a compressed LV. Therefore, we sus-pected that the resultant volume change in LVEDVI, LVESVI, RVEDVI, and RVESVI might be associated with the hemo-dynamic parameters PVR, mPAP, and mRAP. Linear regres-sion analysis showed a significant inverse correlation between LVEDVI and PVR and a significant positive correlation be-tween RVESVI and PVR and between RVEDVI or RVESVI and mPAP (Figure 2). During the recovery process in this specific case, each volume index reverted toward normal val-ues by maintaining a linear relationship with each of the he-modynamic parameters (Figures 5A,B), although the linearity between LVEDVI and mRAP was not statistically significant. There is no clear explanation as to the discrepancy in the linear fitting of the volume indices and hemodynamic parameters between the data from the 23 independent patients and from the 1 specific patient. Given that the linearity and the value of each volume index may differ from patient to patient due to variations in age, sex, body weight and height, etiology of PH, coexisting diseases and so on, the 23 data points from indi-vidual patients contained inevitable data variances to consider-able extents. In contrast, 6 data points were obtained during a relatively short period (approximately 6 months) in the 1 spe-cific patient with IPAH without any concomitant disease.16 In addition, most of the data points were ordered at a proper distance apart (Figure 5), which might increase suitability for statistical analysis itself. Furthermore, we thought that 6 data points from 1 patient seemed to possess fewer confounding factors, thereby diminishing the data variance, which clarified the linear relationship between the volumetric indices of the ventricles and the hemodynamic parameters. Rather than the results from the 23 individual patients, the excellent linear relationships between the volumetric indices and hemody-namic parameters in this specific case might seem to more realistically imply that the ventricular volumes may be af-fected in a linear fashion by PVR, mPAP, and mRAP, al-though we definitely require more individual cases in order to clarify this point. We propose that volumetric analysis should be routinely performed with 3DECHO in patients with PH in order to assimilate the data on the relationship between the volume and hemodynamic parameters, which may offer a solution.
3-D Remodeling Indices for PH EvaluationIn the present study, we proposed the novel indices RVEDVI/LVEDVI and RVESVI/LVESVI (the diastolic and systolic remodeling indices, respectively) to represent the morpho-logical deformities induced by PH (Table). Regarding PVR, the diastolic remodeling index (RVEDVI/LVEDVI) showed the most prominent relationship (Figures 2–4), whereas for mPAP or mRAP, the volumetric data did not indicate such a prominent relationship, although were significant. It is helpful to obtain a linear relationship between the morphological in-dices and hemodynamic parameters in patients with PH. The

Circulation Journal Vol.77, January 2013
204 INABA T et al.
Figure 5. Ventricular volumes change in accordance with hemodynamic parameters in the recovery process of pulmonary hy-pertension (PH). (A) LV end-diastolic volume index (LVEDVI) and LV end-systolic volume index (LVESVI) became larger, inverse-ly and linearly correlating with pulmonary vascular resistance (PVR), mean pulmonary arterial pressure (mPAP), and mean right atrial pressure (mRAP), while the correlation of LVEDVI and mRAP was nearly significant. (B) In contrast, RV end-diastolic volume index (RVEDVI) and RV end-systolic volume index (RVESVI) decreased, and positively and linearly correlated with PVR, mPAP, and mRAP. (C) A significant linear and inverse correlation of RV ejection fraction (RVEF) with PVR and mPAP was also observed, although the correlation of RVEF and mRAP was nearly significant. (D) Both the diastolic and systolic remodeling indices (RVEDVI/LVEDVI and RVESVI/LVESVI, respectively) had an extremely tight linear correlation with PVR, mPAP, and mRAP. LV, left ventricu-lar; RV, right ventricular.

Circulation Journal Vol.77, January 2013
2053DECHO for PH
prominent relationship between the remodeling indices and PVR in these 23 patients suggests the importance of the indi-ces, which was also supported by the result that all hemody-namic parameters showed tremendous linearity with the 2 re-modeling indices during the recovery process in the specific IPAH case (Figure 5D). In addition to the pathophysiological meanings of these indices, the ratio indices may have an ad-vantage in minimizing the influence of individual variance from patient to patient, which may contribute to further im-prove the statistics in comparison with other volumetric indi-ces. We propose to utilize these remodeling indices for assess-ment of PH severity and the therapeutic evaluation of patients with PH.
RVEF and PH SeverityIn contrast to the morphological indices, RVEF is a functional index important for PH patients. RVEF has been reported to be a critical factor for the prognosis of PH patients because fatal events frequently result from RV failure.22,25–27 Accord-ingly, it is necessary to precisely evaluate RV function for PH treatment. It is difficult, however, to evaluate either RVEF or RV function. Using the 3DECHO technique, we can measure RV and LV volumes, the reliability of which has now been confirmed on MRI. A slight underestimation of RV volumes and RVEF on 3DECHO measurement was observed, which was also consistent with the results of a meta-analysis on 3DECHO measurement of RV volumes.28
Interestingly, RVEF was inversely and linearly correlated with PVR and mRAP, while the relationship between RVEF and mPAP was almost statistically significant (Figure 3). In addition, RVEF was recovered to be normal, in maintaining significant linearity with PVR and mPAP and the near-sig-nificant linearity with mRAP in the specific patient with IPAH (Figure 5C). Based on these results, we have, for the first time, shown that RVEF deteriorated along with the impair-ment of the hemodynamic parameters and recovered synergis-tically with improvement of the hemodynamics. These results suggest that RVEF is an indicator for not only RV function, but also for PH severity. Because the number of serial data on the recovery process of PH is limited, further examination is necessary to clarify this point in patients with PH. Nonethe-less, it is very important to report the present data on the rela-tionship between RVEF and hemodynamic parameters. Cur-ing severe PH is very difficult and, such as in the present specific case, it may be necessary to accumulate data on the recovery process from many institutions or even from all over the world.
Study LimitationsIn the present study we have reported data on a linear relation-ship of 3DECHO volumetric indices and hemodynamic pa-rameters. The sample size, however, was not sufficient to omit the possibility of a linear relationship for each combination, which did not pass the threshold of statistical significance. Moreover, it may be important to examine the linear relation-ship of each combination for each cause of PH. Almost all of the combinations had a significant linear relationship when they were examined in 1 specific case (Figure 5), implying that a sufficient sampling size for each etiology might lead to more detailed results. Nonetheless, the present statistically significant results on the linear relationship between 3DECHO volumetric data and hemodynamic parameters (Figure 2) seem to provide novel and useful information for the clinical field. Further examination with a larger amount of data is necessary to confirm these results.
Technically, the feasibility of 3DECHO measurement is af-fected by 1 particular difficulty. Tamborini et al noted that the major limitation of 3DECHO was the poor detection of the RV anterior wall and the presence of trabeculations, which hampers endocardial tracing.6 We experienced some difficulty in the acquisition of images in other subjects, but in this series of 3DECHO measurements, we fortunately could trace the edge of the RV in all patients. We believe that a success rate of approximately 85% is satisfactory for clinical use, because 3DECHO recording is not a difficult procedure and takes only several minutes in addition to the regular 2DECHO recording. Therefore, 3DECHO recording is worth attempting if the regular 2DECHO recording can visualize the RV edge. Based on our experience, the manual tracing of the RV and LV edges and the calculation of all volumetric indices takes >30 min, which can be done following the clinical work. Therefore, the 3DECHO measurements can be easily and successfully per-formed in most (approximately 85%) of patients with PH.
ConclusionsWe have shown the usefulness of 3DECHO for non-invasive evaluation of patients with PH. The ventricular volume data are very important in that they not only provide morphological information and describe the function of RV and LV, but they also predict the hemodynamic status, which is crucial in PH therapy, especially for therapeutic assessment. We expect that the present 3DECHO indices, especially novel indices, such as the diastolic and the systolic remodeling indices, will help physicians reach correct decisions.
AcknowledgmentsThis paper was presented in part at the 73rd annual scientific meeting of the Japanese Circulation Society (2009) and the 2009 scientific session of the American Heart Association. This research was supported by the Japan Society for the Promotion of Science (JSPS) through its “Funding Program for World-Leading Innovative R&D on Science and Technology (FIRST program)”.
DisclosuresDr Shiota is on the speakers’ bureau of Philips Ultrasound. Funding Sourc-es: None.
References 1. Lai WW, Gauvreau K, Rivera ES, Saleeb S, Powell AJ, Geva T. Ac-
curacy of guideline recommendations for two-dimensional quantifi-cation of the right ventricle by echocardiography. Int J Cardiovasc Imaging 2008; 24: 691 – 698.
2. Danchin N, Cornette A, Henriquez A, Godenir JP, Ethevenot G, Polu JM, et al. Two-dimensional echocardiographic assessment of the right ventricle in patients with chronic obstructive lung disease. Chest 1987; 92: 229 – 233.
3. Prakash R, Matsukubo H. Usefulness of echocardiographic right ven-tricular measurements in estimating right ventricular hypertrophy and right ventricular systolic pressure. Am J Cardiol 1983; 51: 1036 – 1040.
4. Morikawa T, Murata M, Okuda S, Tsuruta H, Iwanaga S, Satoh T, et al. Quantitative analysis of right ventricular function in patients with pulmonary hypertension using three-dimensional echocardiog-raphy and a two-dimensional summation method compared to mag-netic resonance imaging. Am J Cardiol 2011; 107: 484 – 489.
5. Badano LP, Ginghina C, Easaw J, Muraru D, Grillo MT, Lancellotti P, et al. Right ventricle in pulmonary arterial hypertension: Haemo-dynamics, structural changes, imaging, and proposal of a study pro-tocol aimed to assess remodelling and treatment effects. Eur J Echo-cardiogr 2010; 11: 27 – 37.
6. Tamborini G, Brusoni D, Torres Molina JE, Galli CA, Maltagliati A, Muratori M, et al. Feasibility of a new generation three-dimensional echocardiography for right ventricular volumetric and functional mea-surements. Am J Cardiol 2008; 102: 499 – 505.

Circulation Journal Vol.77, January 2013
206 INABA T et al.
7. Nesser HJ, Tkalec W, Patel AR, Masani ND, Niel J, Markt B, et al. Quantitation of right ventricular volumes and ejection fraction by three-dimensional echocardiography in patients: Comparison with magnetic resonance imaging and radionuclide ventriculography. Echocardiography 2006; 23: 666 – 680.
8. Apfel HD, Shen Z, Gopal AS, Vangi V, Solowiejczyk D, Altmann K, et al. Quantitative three dimensional echocardiography in patients with pulmonary hypertension and compressed left ventricles: Com-parison with cross sectional echocardiography and magnetic resonance imaging. Heart 1996; 76: 350 – 354.
9. Fukuda S, Watanabe H, Daimon M, Abe Y, Hirashiki A, Hirata K, et al. Normal values of real-time 3-dimensional echocardiographic parameters in a healthy Japanese population: The JAMP-3D study. Circ J 2012; 76: 1177 – 1181.
10. Cua CL, Feltes TF. Echocardiographic evaluation of the single right ventricle in congenital heart disease: Results of new techniques. Circ J 2012; 76: 22 – 31.
11. Yang HS, Bansal RC, Mookadam F, Khandheria BK, Tajik AJ, Chandrasekaran K. Practical guide for three-dimensional transtho-racic echocardiography using a fully sampled matrix array transducer. J Am Soc Echocardiogr 2008; 21: 979 – 989; quiz 1081 – 1082.
12. Yamazaki T, Suzuki J, Shimamoto R, Tsuji T, Ohmoto-Sekine Y, Ohtomo K, et al. A new therapeutic strategy for hypertrophic nonob-structive cardiomyopathy in humans: A randomized and prospective study with an angiotensin II receptor blocker. Int Heart J 2007; 48: 715 – 724.
13. Suzuki J, Shimamoto R, Nishikawa J, Yamazaki T, Tsuji T, Nakamura F, et al. Morphological onset and early diagnosis in apical hypertro-phic cardiomyopathy: A long term analysis with nuclear magnetic resonance imaging. J Am Coll Cardiol 1999; 33: 146 – 151.
14. Yamazaki T, Suzuki J, Shimamoto R, Tsuji T, Ohmoto Y, Toyo-oka T, et al. Focalized contractile impairment at hypertrophied myocar-dium proven in consideration of wall stress in patients with hyper-trophic cardiomyopathy. Int Heart J 2006; 47: 247 – 258.
15. Jessup M, Sutton MS, Weber KT, Janicki JS. The effect of chronic pulmonary hypertension on left ventricular size, function, and inter-ventricular septal motion. Am Heart J 1987; 113: 1114 – 1122.
16. Maki H, Yao A, Inaba T, Shiga T, Hatano M, Kinugawa K, et al. Ini-tial and programmed combination therapy with oral drugs for severe idiopathic pulmonary arterial hypertension. Int Heart J 2011; 52: 323 – 326.
17. Miura Y, Fukumoto Y, Sugimura K, Oikawa M, Nakano M, Tatebe S,
et al. Identification of new prognostic factors of pulmonary hyperten-sion. Circ J 2010; 74: 1965 – 1971.
18. Sitbon O, Humbert M, Nunes H, Parent F, Garcia G, Herve P, et al. Long-term intravenous epoprostenol infusion in primary pulmonary hypertension: Prognostic factors and survival. J Am Coll Cardiol 2002; 40: 780 – 788.
19. Okada O, Tanabe N, Yasuda J, Yoshida Y, Katoh K, Yamamoto T, et al. Prediction of life expectancy in patients with primary pulmonary hypertension: A retrospective nationwide survey from 1980–1990. Intern Med 1999; 38: 12 – 16.
20. Sandoval J, Bauerle O, Palomar A, Gomez A, Martinez-Guerra ML, Beltran M, et al. Survival in primary pulmonary hypertension: Vali-dation of a prognostic equation. Circulation 1994; 89: 1733 – 1744.
21. Glanville AR, Burke CM, Theodore J, Robin ED. Primary pulmo-nary hypertension: Length of survival in patients referred for heart-lung transplantation. Chest 1987; 91: 675 – 681.
22. D’Alonzo GE, Barst RJ, Ayres SM, Bergofsky EH, Brundage BH, Detre KM, et al. Survival in patients with primary pulmonary hyper-tension: Results from a national prospective registry. Ann Intern Med 1991; 115: 343 – 349.
23. McLaughlin VV, Presberg KW, Doyle RL, Abman SH, McCrory DC, Fortin T, et al. Prognosis of pulmonary arterial hypertension: ACCP evidence-based clinical practice guidelines. Chest 2004; 126: 78S – 92S.
24. Yamada Y, Okuda S, Kataoka M, Tanimoto A, Tamura Y, Abe T, et al. Prognostic value of cardiac magnetic resonance imaging for idio-pathic pulmonary arterial hypertension before initiating intravenous prostacyclin therapy. Circ J 2012; 76: 1737 – 1743.
25. Rosenkranz S. Pulmonary hypertension: Current diagnosis and treat-ment. Clin Res Cardiol 2007; 96: 527 – 541.
26. Eysmann SB, Palevsky HI, Reichek N, Hackney K, Douglas PS. Two-dimensional and doppler-echocardiographic and cardiac catheteriza-tion correlates of survival in primary pulmonary hypertension. Cir-culation 1989; 80: 353 – 360.
27. Fuster V, Steele PM, Edwards WD, Gersh BJ, McGoon MD, Frye RL. Primary pulmonary hypertension: Natural history and the importance of thrombosis. Circulation 1984; 70: 580 – 587.
28. Shimada YJ, Shiota M, Siegel RJ, Shiota T. Accuracy of right ven-tricular volumes and function determined by three-dimensional echo-cardiography in comparison with magnetic resonance imaging: A meta-analysis study. J Am Soc Echocardiogr 2010; 23: 943 – 953.