volume 76, number 10 obstetrical and gynecological …
TRANSCRIPT

All authof this CMlationshizations re
Volume 76, Number 10OBSTETRICAL AND GYNECOLOGICAL SURVEYCopyright © 2021 Wolters Kluwer Health,Inc. All rights reserved. CME REVIEWARTICLE 28
CHIEF EDITOR’S NOTE: This article is part of a series of continuing education activities in this Journal through which up to36 AMA PRA Category 1 Credits™ can be earned in 2021. Instructions for how CME credits can be earned appear on the last pageof the Table of Contents.
Gestational Hypertension andPreeclampsia: An Overview of National
and International GuidelinesIoannis Tsakiridis, PhD,* Sonia Giouleka, MSc,† Alexandra Arvanitaki, MSc,‡§
George Giannakoulas, PhD,¶ Georgios Papazisis, PhD,k Apostolos Mamopoulos, PhD,**Apostolos Athanasiadis, PhD,** and Themistoklis Dagklis, PhD††
*Clinical Fellow in Maternal-Fetal Medicine and †Resident, Third Department of Obstetrics and Gynaecology, School ofMedicine, Faculty of Health Sciences, Aristotle University of Thessaloniki, Thessaloniki, Greece; ‡Clinical Fellow in Adult
Congenital Heart Disease, Royal Brompton and Harefield NHS Foundation Trust, London, United Kingdom; §FirstDepartment of Cardiology, School of Medicine, Faculty of Health Sciences, Aristotle University of Thessaloniki, Greece; and¶Associate Professor, First Department of Cardiology, kAssociate Professor, Department of Clinical Pharmacology, and
**Professor and ††Assistant Professor, Third Department of Obstetrics and Gynaecology, School of Medicine, Faculty of HealthSciences, Aristotle University of Thessaloniki, Thessaloniki, Greece
Importance:Gestational hypertension and preeclampsia are leading causes ofmaternal and perinatal morbidity andmortality worldwide. Τhe lack of effective screening and management policies appears to be one of the main reasons.
Objective: The aim of this study was to review and compare recommendations from published guidelines onthese common pregnancy complications.
Evidence Acquisition: A descriptive review of guidelines from the National Institute for Health and Care Excel-lence, the Society of Obstetric Medicine of Australia and New Zealand, the International Society of Hypertension,the International Society for the Study of Hypertension in Pregnancy, the European Society of Cardiology, the In-ternational Federation of Gynecology and Obstetrics, the Society of Obstetricians and Gynaecologists ofCanada, the AmericanCollege of Obstetricians andGynecologists, the International Society of Ultrasound inOb-stetrics and Gynecology, the World Health Organization, and the US Preventive Services Task Force on gesta-tional hypertension and preeclampsia was carried out.
Results: There is an overall agreement that, in case of suspected preeclampsia or new-onset hypertension,blood and urine tests should be carried out, including dipstick test for proteinuria, whereas placental growthfactor–based testing is only recommended by the National Institute for Health and Care Excellence and theEuropean Society of Cardiology. In addition, there is a consensus on the recommendations for the medical treat-ment of severe and nonsevere hypertension, the management of preeclampsia, the appropriate timing of deliv-ery, the optimal method of anesthesia and the mode of delivery, the administration of antenatal corticosteroidsand the use of magnesium sulfate for the treatment of eclamptic seizures, the prevention of eclampsia in casesof severe preeclampsia, and the neuroprotection of preterm neonates. The reviewed guidelines also state that,based on maternal risk factors, pregnant women identified to be at high risk for preeclampsia should receivelow-dose aspirin starting ideally in the first trimester until labor or 36 to 37 weeks of gestation, although the rec-ommended dose varies between 75 and 162 mg/d. Moreover, most guidelines recommend calcium supplemen-tation for the prevention of preeclampsia and discourage the use of other agents. However, controversy exists
ors, faculty, and staff in a position to control the contentE activity have disclosed that they have no financial re-
ps with, or financial interests in, any commercial organi-levant to this educational activity.
I.T. and S.G. share first authorship.Correspondence requests to: Ioannis Tsakiridis, PhD,
Konstantinoupoleos 49, 54642, Thessaloniki, Greece. E-mail:[email protected].
www.obgynsurvey.com | 613
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.

614 Obstetrical and Gynecological Survey
regarding the definition and the optimal screening method for preeclampsia, the need for treating mild hyperten-sion, the blood pressure treatment targets, and the postnatal blood pressure monitoring.
Conclusions: The development and implementation of consistent international protocols will allow cliniciansto adopt effective universal screening, as well as preventive andmanagement strategies with the intention of im-proving maternal and neonatal outcomes.
Target Audience: Obstetricians and gynecologists, family physiciansLearning Objectives: After participating in this activity, the physician should be better able to define gesta-
tional hypertension and preeclampsia; identify the risk factors and explain available screening methods for pre-eclampsia; and describe the recommended antenatal, intrapartum, and postnatal care of womenwith gestationalhypertension or preeclampsia.
Hypertensive disorders in pregnancy (HDPs) repre-sent a group of disorders characterized by elevatedblood pressure (BP) during the antenatal period and in-clude gestational hypertension, chronic (or preexisting)hypertension, preeclampsia, preeclampsia superimposedon chronic hypertension, and eclampsia.1 Despite the ef-forts made in the past few decades by national and inter-national organizations to raise awareness and promoteprenatal care, HDPs complicate approximately 5% to10% of all pregnancies worldwide and are responsiblefor an estimated 10% of maternal deaths every year.2
The vast majority of these deaths occur in low-incomecountries, reflecting the crucial role of robust healthcaresystems, as well as the need for well-designed studies.3–5
Preeclampsia is a multifactorial, inflammatory,pregnancy-specific disease, and its pathogenesis has notbeen elucidated to date, whereas its short- and long-termhealth impacts on both the mother and the fetus imposea significant burden for the society.3 Apart frommortality,gestational hypertension and preeclampsia are associatedwith other severe maternal complications, such as liverand kidney failure, stroke, placental abruption, dissemi-nated intravascular coagulation, diabetes, hypothyroid-ism, impaired cognitive function, deep vein thrombosis,subsequent chronic hypertension, and chronic cardiovas-cular disease.6–9Hypertensive disorders in pregnancy alsoincrease the risk of adverse perinatal outcomes includingfetal growth restriction (FGR), low birth weight, oligo-hydramnios, stillbirth, prematurity, bronchopulmonarydysplasia, and neurodevelopmental deficits.10,11
Thus, there is need for international evidence-basedalgorithms that will allow earlier detection of these condi-tions, better risk stratification and preventive interventions,and improved antenatal and postnatal care in order to re-duce the morbidity and mortality rates. The aim of this de-scriptive review was to summarize and compare the mostrecent recommendations from 11 influential medical socie-ties on gestational hypertension and preeclampsia.
EVIDENCE ACQUISITION
Themost recently published guidelines on gestationalhypertension and preeclampsia were retrieved, and a
Copyright © 2021 Wolters Kluwer
descriptive review was conducted. In particular, 12 guide-lines were identified from the National Institute for HealthandCare Excellence (NICE 2019),12 the Society ofObstet-ric Medicine of Australia and New Zealand (SOMANZ2015),13 the International Society of Hypertension (ISH2020),1 the International Society for the Study of Hy-pertension in Pregnancy (ISSHP 2018),14 the EuropeanSociety of Cardiology (ESC 2018),15 the InternationalFederation of Gynecology and Obstetrics (FIGO 2016 and2019),16,17 the Society of Obstetricians andGynaecologistsof Canada (SOGC 2014),18 the American College ofObstetricians and Gynecologists (ACOG 2020),19 the In-ternational Society of Ultrasound in Obstetrics and Gyne-cology (ISUOG 2018),20 the World Health Organization(WHO 2011),21 and the US Preventive Services TaskForce (USPSTF 2017).22
An overview of the recommendations is presented inTable 1. Of note, the WHO and the USPSTF guidelinesinclude recommendations only for preeclampsia, whereasISUOG refers only to screening for preeclampsia.
DEFINITION AND DIAGNOSIS
There is overall agreement that gestational hyperten-sion is defined as new-onset hypertension arising after20 weeks of gestation, with a systolic BP (SBP) per-sistently equal to or greater than 140 mm Hg and/or adiastolic BP (DBP) equal to or greater than 90mmHg.18
These values should be confirmed by repeated mea-surements: at least 2 measurements within 15 minutesapart (ESC, FIGO, SOGC) or within several hours apart(SOMANZ, ACOG—4 hours), and in case of consis-tently higher BP in 1 arm, this arm should be used forall the following BP measurements (FIGO, SOGC).Of note, gestational hypertension should resolve within6 weeks (ISH, ESC) or 3 months postpartum (SOMANZ).Moreover, according to most guidelines, a BP equal toor greater than 160/110 mm Hg should be classified assevere hypertension, whereas the SOMANZ and ISHguidelines set a threshold of 170 mm Hg for SBP.Blood pressure should be measured by auscultatory
devices (liquid-crystal or aneroid sphygmomanome-ter) using Korotkoff sounds (K1 and K5) or automated
Health, Inc. All rights reserved.

615Gestational Hypertension and Preeclampsia • CME Review Article
devices that have been validated specifically for use inpregnancy (SOMANZ, ISH, ISSHP, ESC, FIGO, SOGC,and USPSTF). Two parallel studies in 340 pregnantwomen concluded that the auscultatory hybrid sphyg-momanometer is probably more accurate than the auto-mated oscillometric device in pregnancy, especially inhypertensive pregnancies.23 It is important to use aright-sized cuff placed at the patient's bare upper arm;the patient should be in a sitting position, calm, andstill, with the arm resting at the level of the heart andher back supported on the back of the chair.24 The mea-surements should mainly take place at the office/clinic orhospital. The 24-hour ambulatory BPmonitoring (ABPM)is also encouraged by SOMANZ, ESC, ISH, ISSHP,FIGO, and SOGC as it helps diagnose and managethe transient, white-coat, and masked hypertension,but further research is required in order to define its rolein the management of hypertension in pregnancy.25
FIGO points out that ABPMhas not only the advantageof recording the variations of BP levels during daily activ-ities and sleep, but also the disadvantage of limited predic-tive value for adverse outcomes. In particular, evidencefrom a prospective cohort study showed that 24-hourABPMmay distinguish true HDP fromwhite-coat hyper-tension, but it may be associated with increased rates ofcesarean delivery, so it should be used with caution.26
Moreover, based on a study of 276 pregnant women,FIGO defines hypertension in pregnancy using homeor ABPM as SBP ≥135 mm Hg or DBP ≥85 mm Hg.27
These values should then be confirmed by office mea-surements, while all the devices used (either in healthcare facilities or at home) should be regularly checkedand calibrated.It is noteworthy that there is no agreement on the def-
inition of preeclampsia among the studied guidelines.Hence, the WHO's, ISH's, and ESC's older definitionof preeclampsia requires the combination of hyperten-sion with significant proteinuria, that is, >300 mg in a24-hour urine collection or a protein-to-creatinine ratio>30 mg/mmol. On the other hand, 7 guidelines (NICE,SOMANZ, ISSHP, FIGO, SOGC, ACOG, andUSPSTF)have adopted a more recent definition of preeclampsiaas gestational hypertension that is accompanied by 1or more signs of end-organ involvement, that is, renaldysfunction (oliguria, proteinuria, or increased creati-nine levels), liver dysfunction (persistent right upperquadrant or epigastric pain, increased serum levels ofaspartate aminotransferase/alanine aminotransferase/lactatedehydrogenase/bilirubin), hematological complications(platelets [PLTs] <150 � 109/L [NICE, ISSHP, FIGO]or <100 � 109/L [SOMANZ, ACOG], hemolysis, dis-seminated intravascular coagulation), pulmonary edema,neurological signs (convulsions, headaches, hyperreflexia,
Copyright © 2021 Wolters Kluwer
visual disturbances, stroke), or uteroplacental dysfunction(FGR, abnormal umbilical artery [UA]Doppler wave, still-birth, oligohydramnios, placental abruption, nonreassuringfetal heart rate). These medical societies state that pro-teinuria should no longer be an essential parameter forthe diagnosis of preeclampsia, as it is present in only75% of cases.28
SCREENING FOR PREECLAMPSIA
All the reviewed guidelines agree on the need for uni-versal assessment of maternal risk factors for preeclampsia.Most of the guidelines discriminate between high andmoderate risk factors. Commonly accepted high-riskfactors include personal history of hypertensive disor-der in a previous pregnancy, chronic kidney disease,antiphospholipid syndrome, or other autoimmune disease,type 1 or 2 diabetes,8 chronic hypertension,29 and use ofassisted reproduction techniques. Primiparity, advancedmaternal age (≥40 years old), interpregnancy intervalgreater than 10 years, maternal obesity, and family his-tory of preeclampsia are considered moderate risk fac-tors by all guidelines. Multifetal gestation is consideredas a high risk factor by some guidelines (FIGO, ACOG,USPSTF), whereas others (NICE, SOMANZ, ISH, ESC,SOGC, and WHO) classify it as a moderate risk factor.30
Rare risk factors for preeclampsia include fetal hydropsand gestational trophoblastic disease13,31 (Table 2).There is controversy among the guidelines regarding
the optimal screening method for preeclampsia. Thus,FIGO, ISSHP, and ISUOG state that the best way ofidentifying women as high-risk for preeclampsia is theuse of a combined screening test that includes assessmentof maternal risk factors, uterine artery (UtA) Doppler,maternal BP levels, and serum placental growth factorlevels (PlGF). This approach is based on current evidencedemonstrating that this combined screening algorithm caneffectively detect 75% of cases of preterm preeclampsiaand 47% of term preeclampsia, at a false-positive rate of10%.32 In addition, the aforementioned guidelines recom-mend the performance of this test ideally in the first tri-mester, that is, at 11 to 13+0 weeks of gestation, giventhat the administration of low-dose aspirin as a preven-tive strategy is more effective when started at that time,as proven by a large prospective multicenter trial.33
FIGO and ISUOG also state that the mean UtApulsatility index (PI) should be preferred over other ul-trasonographic indices. Moreover, the ESC guidelineacknowledges the usefulness of UtA PI in discriminat-ing women at high risk for preeclampsia. Of note, thepresence of a lateral placenta has been associated witha higher mean UtA PI and in turn a higher risk of pre-eclampsia.34 In addition, FIGO and ISUOG mention
Health, Inc. All rights reserved.

TABLE 1Summary of Recommendations on Diagnosis and Management of Gestational Hypertension and Preeclampsia
Country
NICE SOMANZ ISH ISSHP ESC
United KingdomAustralia andNew Zealand International International European
Issued 2019 2015 2020 2018 2018
Title Hypertension inpregnancy:diagnosis andmanagement
The SOMANZ guidelinesfor the management ofhypertensive disordersof pregnancy 2014
2020 InternationalSociety ofHypertensionglobalhypertensionpracticeguidelines
The hypertensivedisorders ofpregnancy:ISSHPclassification,diagnosis &managementrecommendationsfor internationalpractice
2018 ESC guidelinesfor themanagement ofcardio vasculardiseases duringpregnancy
Pages 55 51 23 20 84References 0 276 142 114 439Definition;
diagnosisof gestationalhypertension
BP ≥140/90 mm Hg;severe if BP ≥160/110 mm Hg
BP ≥140/90 mm Hg after20 wk (confirmed byrepeated readingsover several hours)which returns tonormal within3 mo postpartum;severe if BP ≥170/110 mm Hg
Hypertensionstarting after20 wk and lasting<6 w postpartum;severe if BP ≥170/110 mm Hg
BP ≥140/90 mm Hgstarting after 20 wkwithout proteinuriaor biochemical/hematologicalabnormalities;severe if BP ≥160/110 mm Hg
BP ≥140/90 mm Hgstarting after 20 wkand resolving within42 d postpartum;severe if BP ≥160/110 mm Hg(2 measurements,≥15 min apart)
Definition ofpreeclampsia
Hypertension after20 wk with organinvolvement*
Hypertension after20 wk with organinvolvement*
Hypertension withproteinuria>300 mg/24 h orACR >30 mg/mmol
BP ≥140/90 after20 wk with organinvolvement*
Gestationalhypertension withproteinuria >300mg/24 h or ACR ≥30 mg /mmol
ABPM Not discussed Useful mainly before20 wk gestation
Optimal In order todiagnosewhite-coathypertension
Recommended
Universalscreening forpreeclampsia
Not discussed Not discussed Not discussed Recommended Recommended forproteinuria andmaternal riskfactors
Initialinvestigation inwomen withgestationalhypertension
Blood tests†. Dipstick1–2 times/wk ordaily if admittedto hospital.If ≥1+, use ACRor PCR‡.Fetal US
Physical examination forsigns of preeclampsia,blood tests†,Dipstick 1–2 times/wk(if ≥1+ spot urinePCR ≥30 mg/mmol)US for fetal growth,AF, and UA Doppler
Blood tests†. Dipstickin early pregnancyand in the secondhalf. If >1+, UACR(<30 mg/mmolexcludesproteinuria)
Blood tests†. Dipstick(automated orvisual). If >1+,spot urine PCR‡
Blood tests†. Dipstickin early pregnancyand in the secondhalf. If >1+, UACR(<30 mg/mmolexcludesproteinuria)
24-h urinecollection
Not recommendedas a routine
Not recommended Not discussed Not recommended(only to confirmnephroticsyndrome)
If ACR >30 mg, 24-hurine collection
PlGF-based testingsFlt-1: PlGF)
If suspectedpreeclampsia,between 20and 35 wk
Not recommendedas a routine
Not discussed Not recommendedas a routine
Consider sFlt-1:PlGFratio if suspectedpreeclampsia
616 Obstetrical and Gynecological Survey
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.

FIGO SOGC ACOG ISUOG WHO USPSTF
International CanadaUnitedStates International International United States
2016/2019 2014 2020 2018 2011 2017
The FIGO Textbookof PregnancyHypertension/The InternationalFederation ofGynecology andObstetrics(FIGO) initiative onpreeclampsia:a pragmatic guidefor first-trimesterscreening and prevention
Diagnosis, evaluation,and managementof the hypertensivedisorders ofpregnancy:executive summary
Gestationalhypertension andpreeclampsia:ACOG practicebulletin, number 222
ISUOG practiceguidelines: roleof ultrasound inscreening forand follow-upof preeclampsia
WHOrecommendationsfor preventionand treatment ofpreeclampsiaand eclampsia
Screening forPreeclampsia.US PreventiveServices TaskForcerecommendationstatement
456/33 23 24 16 48 71428/213 39 175 181 34 32BP ≥140/90 mm Hg starting
after 20 wk (average of 2measurements, ≥15 minapart); severe if BP ≥160/110 mm Hg; resistant if itrequires 3 drugs to becontrolled
BP ≥140/90 mm Hgafter 20 wk; severeif BP ≥160/110 mm Hg(2 measurements,≥15 min apart);resistant if it requires3 drugs to becontrolled
BP ≥140/90 mm Hgafter 20 wk andreturns to normalpostpartum(2 measurements,≥4 h apart); severe ifBP ≥160/110 mm Hg
Not discussed Not discussed Not discussed
BP ≥140/90 after 20 wkwith organ involvement*
Gestationalhypertension withnew onset proteinuriaor ≥1 adversecondition or ≥1 severecomplications
Gestationalhypertension withproteinuria or onesevere feature*
Not discussed New-onsethypertension withproteinuria(>300 mg/24 h)
BP ≥140/90 on 2occasions 4 hapart after 20wkwith proteinuriaor organinvolvement*
Recommended (or homeBP monitoring)Hypertension if BP≥135/85 mm Hg
Recommended (orhome BPmonitoring)
Not discussed Not discussed Not discussed Not discussed
Recommended Recommended forproteinuria andmaternal riskfactors
Not discussed Recommended Not discussed Recommendedfor MAPmeasurementand maternalrisk factors
Blood tests†. Dipstickat each antenatalvisit after 20 wk. If ≥2+or suspicion ofpreeclampsia, PCR or24-h urine collection.Do not repeat if significantproteinuria is confirmed
Blood tests†. Dipstick. If≥1+ or suspicion ofpreeclampsia, PCR or24-h urine collection.Do not repeat ifsignificant proteinuriais confirmed
24-h urine collectionor PCR ≥0.3.Dipstick if the othermethods areunavailable (≥2+)
Not discussed Not discussed Dipstick orACR/PCR
Recommended only forsuspected preeclampsiaor significant proteinuria
Recommended onlyfor suspectedpreeclampsia ordipstick ≥1+
Recommended Not discussed Not discussed Gold standard butnot practical
Not discussed Not discussed Not discussed Not discussed Not discussed Not discussed
(Continued on next page)
617Gestational Hypertension and Preeclampsia • CME Review Article
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.

TABLE 1. (Continued)
Country
NICE SOMANZ ISH ISSHP ESC
United KingdomAustralia andNew Zealand International International European
Issued 2019 2015 2020 2018 2018
Frequency oflaboratorytesting (includingblood tests)
At presentation andthen weekly ingestationalhypertension.Twice a week inpreeclampsia
At presentation and thenweekly. Twice a weekin preeclampsia.Investigation for DICor hemolysis ifthrombocytopenia orfalling Hb. 1–2times/d PLT checkif thrombocytopenia
Not discussed Twice a week inpreeclampsia.
Not discussed
Management(inpatient/outpatient)
Hospital admissionif BP >160/110 mm Hg orconcerns for thewell-being of themother or the fetus
Outpatient managementfor mild cases. Ifsevere and preterm,transfer to a tertiarycenter
Hospital admissionfor severe cases
Hospital assessmentat diagnosis andif BP >160/110 mm Hg.Outpatient if stable.Clinical examinationfor clonus
If BP ≥170/110 mm Hg
Fluid administrationin preeclampsia
80 mL/h unlessother ongoingfluid losses
Extra 250-mL bolus priorto IV hydralazine,regional anesthesia orimmediate delivery;300 mL if oliguria withintravascular volumedeficit
Not discussed Plasma volumeexpansion is notrecommended
Not discussed
Fetal assessment Heart auscultation atevery appointment,US at diagnosisand every 2–4 wk(every 2 wk inpreeclampsia)§,CTG only ifclinically indicated
At each appointment,assessment of fetalwell-being. US atdiagnosis and every3–4 wk (every 2–3 wkin preeclampsia)§;continuous CTG whiletreating severehypertension.CTG twice per week ormore frequently ifclinically indicated inpreeclampsia
Not discussed Monitoring of fetalgrowth especially ifuric acid is elevatedin gestationalhypertension.Assessment of fetalwell-being§ atdiagnosis andevery 2 wk inpreeclampsia.More frequentevaluation ifabnormal UADoppler wave*
Not discussed
Need for medicaltreatment
If BP remains above140/90 mm Hg
If BP ≥160/110 mm Hg. IfBP = 140–160/90–100,optional
If persistent BP >140/90 mm Hg
If persistent BP >140/90 mm Hg in clinicor office (or ≥135/85 mm Hg at home).Stop or reduce ifDBP <80 mm Hg
If persistent BP >140/90 mm Hg
Antihypertensivemedications fornonseverehypertension
Labetalol, nifedipine,methyldopa
Methyldopa, labetalol,oxprenolol (nifedipine,hydralazine, prazosinas second line)
Methyldopa, labetalol,nifedipine
Methyldopa, labetalol,oxprenolol, nifedipine(hydralazine andprazosin assecond line)
Methyldopa, labetalol,nifedipine.Nitroglycerin forpreeclampsia withpulmonary edema
Medicationsrecommendedfor severehypertension
IV or oral labetalol,oral nifedipine orIV hydralazine(+500 mLcrystalloid fluid)
IV labetalol, oral nifedipine,IV hydralazine (+250 mLnormal saline) or IVdiazoxide
IV labetalol, oralmethyldopa ornifedipine, IVhydralazine,nicardipine,esmolol, urapidil
IV or oral labetalol, oralnifedipine or IVhydralazine
IV labetalol, oralnifedipine ormethyldopa(IV hydralazine orurapidil as secondline)
618 Obstetrical and Gynecological Survey
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.

. (Continued)
FIGO SOGC ACOG ISUOG WHO USPSTF
International CanadaUnitedStates International International United States
2016/2019 2014 2020 2018 2011 2017
Not discussed Not discussed Weekly Not discussed Not discussed Not discussed
Outpatient managementfor mild cases. Hospitaladmission if severepreeclampsia and atdiagnosis for fetal andmaternal assessment
Hospital admission ifsevere preeclampsia
Hospital admission ifsevere preeclampsia
Not discussed Not discussed Close fetal andmaternalmonitoring,antihypertensivemedications,magnesiumsulfate
80 mL/h; plasmavolume expansionis notrecommended
Plasma volumeexpansion is notrecommended
With caution Not discussed Not discussed Not discussed
Continuous fetalheart rate monitoringwhile treating severehypertension
Continuous fetalheart ratemonitoring whiletreating severehypertension
US for fetal growthevery 3–4 wk andfor amniotic volumeassessment everyweek
Not discussed Not discussed Recommended
If persistent BP>140/90 mm Hg
Not discussed Recommended foracute-onset severehypertension.Not discussedfor mildhypertension
Not discussed Recommendedfor severehypertension
Not discussed
Methyldopa, labetalol,nifedipine
Methyldopa, labetalolor other β-blockers,nifedipine
Not discussed Not discussed Not discussed Not discussed
IV labetalol, oral nifedipine,IV hydralazine (or orallabetalol, clonidine,captopril postpartum,nitroglycerin infusion)
IV labetalol, oralnifedipine, IVhydralazine (oralmethyldopa, labetalol,clonidine ornitroglycerin infusion)
IV labetalol, oralnifedipine, IVhydralazine
Not discussed Methyldopa,labetalol,nifedipine,hydralazine
Not discussed
(Continued on next page)
619Gestational Hypertension and Preeclampsia • CME Review Article
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.
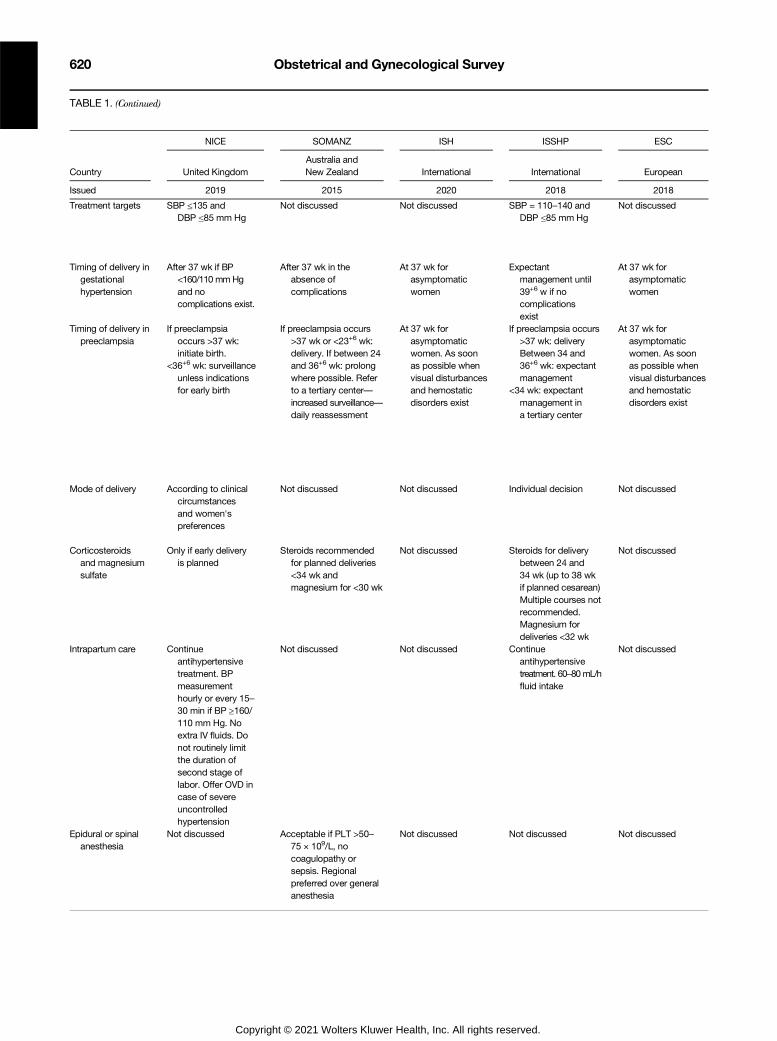
TABLE 1. (Continued)
Country
NICE SOMANZ ISH ISSHP ESC
United KingdomAustralia andNew Zealand International International European
Issued 2019 2015 2020 2018 2018
Treatment targets SBP ≤135 andDBP ≤85 mm Hg
Not discussed Not discussed SBP = 110–140 andDBP ≤85 mm Hg
Not discussed
Timing of delivery ingestationalhypertension
After 37 wk if BP<160/110 mmHgand nocomplications exist.
After 37 wk in theabsence ofcomplications
At 37 wk forasymptomaticwomen
Expectantmanagement until39+6 w if nocomplicationsexist
At 37 wk forasymptomaticwomen
Timing of delivery inpreeclampsia
If preeclampsiaoccurs >37 wk:initiate birth.
<36+6 wk: surveillanceunless indicationsfor early birth
If preeclampsia occurs>37 wk or <23+6 wk:delivery. If between 24and 36+6 wk: prolongwhere possible. Referto a tertiary center—increased surveillance—daily reassessment
At 37 wk forasymptomaticwomen. As soonas possible whenvisual disturbancesand hemostaticdisorders exist
If preeclampsia occurs>37 wk: deliveryBetween 34 and36+6 wk: expectantmanagement
<34 wk: expectantmanagement ina tertiary center
At 37 wk forasymptomaticwomen. As soonas possible whenvisual disturbancesand hemostaticdisorders exist
Mode of delivery According to clinicalcircumstancesand women'spreferences
Not discussed Not discussed Individual decision Not discussed
Corticosteroidsand magnesiumsulfate
Only if early deliveryis planned
Steroids recommendedfor planned deliveries<34 wk andmagnesium for <30 wk
Not discussed Steroids for deliverybetween 24 and34 wk (up to 38 wkif planned cesarean)Multiple courses notrecommended.Magnesium fordeliveries <32 wk
Not discussed
Intrapartum care Continueantihypertensivetreatment. BPmeasurementhourly or every 15–30 min if BP ≥160/110 mm Hg. Noextra IV fluids. Donot routinely limitthe duration ofsecond stage oflabor. Offer OVD incase of severeuncontrolledhypertension
Not discussed Not discussed Continueantihypertensivetreatment. 60–80mL/hfluid intake
Not discussed
Epidural or spinalanesthesia
Not discussed Acceptable if PLT >50–75 × 109/L, nocoagulopathy orsepsis. Regionalpreferred over generalanesthesia
Not discussed Not discussed Not discussed
620 Obstetrical and Gynecological Survey
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.

. (Continued)
FIGO SOGC ACOG ISUOG WHO USPSTF
International CanadaUnitedStates International International United States
2016/2019 2014 2020 2018 2011 2017
DBP <85 mm Hg. Lowertargets whencomorbidities exist. <130/80 for diabetic patients
SBP = 130–155 andDBP = 80–105 mm Hg.Lower targets whencomorbidities exist(<140/90 mm Hg)
Not discussed Not discussed Not discussed Not discussed
≤36+6 wk: expectantmanagement≥37 wk: deliverywithin days
After 37 wk in theabsence ofcomplications
At ≥37 wk in theabsence ofcomplications or≥34 wk when severefeatures exist
Not discussed Not discussed Not discussed
If preeclampsia occurs>37 wk: delivery. Ifnonsevere preeclampsiaat 24–33+6 wk: expectantmanagement in a tertiarycenter. If nonseverepreeclampsia at 34–36+6 wk:expectant management.HELLP syndrome <35 wk:delay for steroidsadministration≥35 wk: delivery
If preeclampsia occurs>37 wk: delivery. If
If 24–33+6 wk: expectantmanagement in atertiary center. If34–36+6 wk: paucity ofdata. HELLPsyndrome <35 wk:delay for steroids'administration≥35 wk: delivery
If diagnosed after37 wk, delivery.Preeclampsia withsevere features >34 wk:delivery, without severefeatures: expectantmanagement. <34 wkexpectantmanagementwith increasedsurveillance. Deliveryat any time if maternalor fetal deterioration
Not discussed If preeclampsiaoccurs >37 wk:delivery. Between34 and 36+6 and<34 wk: expectantmanagementif no maternalor fetalcomplicationsexist (closemonitoring)
At 37 wk in theabsence ofcomplications
Vaginal delivery unlessobstetric indications forcesarean or pretermdelivery with fetalcompromise
Vaginal delivery unlessobstetric indicationsfor cesarean orpreterm delivery withfetal compromise
Vaginal delivery unlessobstetric indicationsfor cesarean delivery
Not discussed Not discussed Not discussed
For deliveries anticipatedwithin 7 d and ≤34+6 wk
Magnesium for deliveries<34 wk
Steroids if ≤34+6 wk anddelivery is expectedwithin the next 7 d.Consider for electivecesarean ≤38+6 wk.Magnesium fordelivery <32 wk
Not discussed Not discussed Not discussed Not discussed
Continue antihypertensivetreatment to maintainBP <160 /110 mm Hg.Avoid ergometrine.Active management ofthird stage of labor withoxytocin especially in caseof thrombocytopenia orcoagulopathy
Continueantihypertensivetreatment to keep BP<160 /110 mm Hg.Avoid ergometrine.Active managementof third stage of laborwith oxytocinespecially in case ofthrombocytopenia orcoagulopathy
Monitoring of BPand symptoms
Not discussed Not discussed Not discussed
Epidural catheter isrecommended for paincontrol in the absenceof contraindications
Acceptable ifPLT ≥75 × 109/L,without coagulopathy.Caution in case ofheparin use
Acceptable ifPLT >70 × 109/Land no othercontraindicationsexist
Not discussed Not discussed Not discussed
(Continued on next page)
621Gestational Hypertension and Preeclampsia • CME Review Article
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.

TABLE 1. (Continued)
Country
NICE SOMANZ ISH ISSHP ESC
United KingdomAustralia andNew Zealand International International European
Issued 2019 2015 2020 2018 2018
Postnatal BPmeasurements
Daily for the first 2 d,once between days3 and 5 and then asclinically indicatedfor gestationalhypertension;
4 times/day whileinpatient, oncebetween days 3 and5 and on alternatedays until normal forpreeclampsia
Not discussed Not discussed Every 4–6 h for the first3 d in preeclampsia
Not discussed
Postpartumantihypertensivetreatment
Continue if required.Reduce if BP <130/80 mm Hg. Starttreatment ifBP ≥150/100mmHg.Replace methyldopawith an alternative
Continue if required Continue if required.Replace methyldopawith an alternative.
Continue and tamperslowly after 3–6 dunless BP <110/70 mm Hg orsymptomatic
Replace methyldopawith an alternative
Reevaluation orappointment witha GP or specialist
At 2 wk postpartum(when treatment iscontinued) and at6–8 wk postpartumUrinary reagent striptest. If ≥1+, refer to aspecialist or GP at3 mo postpartum
Not discussed Not discussed At 1 wk postpartumwhen treatment iscontinued and3 mo postpartum
Not discussed
Prophylactic useof aspirin
To all pregnant womenwith 1 high or >1moderate RF,aspirin 75–150 mg/dfrom 12 wk until labor
To all pregnantwomen of moderateto high risk, ideallybefore 16 wkuntil 37 wk
To all pregnantwomen with 1 highor >1 moderateRF, aspirin75–162 mg/d from12 until 36 wk
To all pregnantwomen of high risk,aspirin 75–162 mg/ddaily starting before20 wk, ideallybefore 16 wk
To all pregnantwomen with 1 highor >1 moderate RF,100–150 mg ofaspirin daily from12 wk until36–37 wk
*Renal dysfunction, proteinuria, liver dysfunction (persistent right upper quadrant or epigastric pain, raised aspartate aminotransferase/ala-nine aminotransferase), low PLTs (<150 × 109/L [NICE, ISSHP, FIGO] or <100 × 109/L [SOMANZ, ACOG]), hemolysis, disseminated intravascu-lar coagulation, pulmonary edema, neurological signs (convulsions, headaches, hyperreflexia, visual disturbances, stroke), FGR/abnormal UADoppler wave/stillbirth.
†Full blood count, liver and kidney function, uric acid.‡Significant proteinuria = PCR ≥30 mg/mmol or ACR ≥8 mg/mmol or proteinuria ≥0.3 g/d in a 24-h urine collection.§Fetal growth and amniotic fluid volume assessment and umbilical artery Doppler velocimetry.BMI, bodymass index (in kg/m2); CTG, cardiotocography; DIC, disseminated intravascular coagulation; eGFR, estimated glomerular filtration
rate; Hb, hemoglobin; IV, intravenous; MAP,mean arterial pressure; OVD, operative vaginal delivery; UA, umbilical artery; UACR, urine albumin-to-creatinine ratio; US, ultrasound.
622 Obstetrical and Gynecological Survey
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.

. (Continued)
FIGO SOGC ACOG ISUOG WHO USPSTF
International CanadaUnitedStates International International United States
2016/2019 2014 2020 2018 2011 2017
At days 3 to 6 postpartum At days 3 to 6postpartum
Not discussed Not discussed Not discussed Not discussed
Continue so as to maintainBP <140/90 mm Hg and<130/80 for women withpregestational diabetes.Especially in case ofantenatal preeclampsiaand preterm delivery.Clonidine iscontraindicated.
Continue so as tomaintain BP <140/90 mm Hg for womenwith or withoutcomorbidities (exceptpregestationaldiabetes) and <130/80for those withpregestationaldiabetes. All drugs arecompatible withbreastfeeding
Not discussed Not discussed Continue or start ifrequired.
Not discussed
6 wk postpartum.Further investigation ifhypertension orproteinuria persist at6 mo postpartum, ifpreeclampsia occurred<34 wk or was severeor eGFR <60 mL/min orabnormal urinarysediment
6 wk postpartumFurther investigationif hypertension orproteinuria persistat 6 mo postpartum,if preeclampsiaoccurred <34 wk orwas severe oreGFR <60 mL/minor abnormal urinarysediment
Not discussed Not discussed Not discussed Not discussed
To all pregnant womenof high risk, 150 mg/dat bedtime. Start ideallyin the first trimesterscreening until 36 wkor delivery or diagnosisof preeclampsia
To all pregnant womenwith 1 high or >1moderate RF, aspirin75–162 mg/d ofdaily starting before16 wk until labor
To all pregnantwomen with 1 highor >1 moderate RF,aspirin 81 mg/d from12–28 wk, ideallybefore 16 wk,until labor.
To all pregnantwomen of highrisk, aspirin150 mg/d atbedtime. Startideally in thefirst trimesterscreening
To all women ofhigh risk, 75 mgof aspirin dailystarting before20 wk
To all women ofhigh risk, aspirin81 mg/d from12 wk
623Gestational Hypertension and Preeclampsia • CME Review Article
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.

624 Obstetrical and Gynecological Survey
that in case of multifetal gestations, the combined screen-ing algorithms for singletons may be used with similardetection rates.35 In addition, FIGO recommends themeasurement of PAPP-A, in case PlGF and UtA PI arenot available, based on a systematic review and meta-analysis, which indicated that low levels of PAPP-A dou-ble the risk of preeclampsia (odds ratio, 1.94; 95% confi-dence interval, 1.63–2.30).36 FIGO also proposes a 2-stepscreening procedure for low-income countries; that is, allpregnant women should be screened for maternal factorsand mean arterial pressure, and only those identified ashigh-risk should receive a UtA PI and PlGF evaluation.In contrast, the UtA PI and the use of combined
screening models are not supported by SOGC, ACOG,and USPSTF, mainly due to the lack of robust evidenceproving the effectiveness of this screening strategy. TheUSPSTF guideline strongly recommends the monitor-ing of maternal BP levels only at each antenatal visit,in order to detect early the development of gestationalhypertension or preeclampsia, based on a systematic re-view highlighting the inaccuracy of all the other predic-tive tests.37 USPSTF also discourages the routine use ofdipstick testing for proteinuria because no study hasassessed the value of repeat testing of urine protein forscreening,38 whereas FIGO, SOGC, and ESC supportthe performance of this test to all pregnant women
TABLE 2Summary of Risk Factors for Preeclampsia
NICE SOMANZ
High risk factorsfor preeclampsia
HD in a previouspregnancy,
CKD, autoimmunedisease, type 1 or 2diabetes, chronichypertension
Preeclampsia in aprevious pregnancy,
CKD, antiphospholipidsyndrome, autoimmunedisease, type 1 or 2diabetes, chronichypertension (nodiscrimination betweenhigh and moderate)
H
C
Moderate riskfactors forpreeclampsia
First pregnancy,age ≥40 y,pregnancy interval>10 y
BMI ≥35,FH of preeclampsia,multifetal pregnancy
First pregnancy,age ≥40 y, pregnancyinterval >10 y,
BMI ≥30,FH of preeclampsia,multifetal pregnancy,SBP >130 andDBP >80 mm Hgbefore 20 wk,fetal hydrops, GTD
F
B
*Lower maternal birth weight and/or preterm delivery; heritable thcocaine and methamphetamine use; maternal uterine abnormality; incAfro-Caribbean or South Asian race; short duration of sexual relation≥130 mm Hg or booking DBP ≥80 mm Hg; vaginal bleeding in early prebeta human chorionic gonadotropin; gestational hypertension; abnormaduring pregnancy; abnormal UtA Doppler; FGR; investigational laboratonancy complicated by preeclampsia with another partner.
BMI, body mass index; CKD, chronic kidney disease; FH, family historSLE, systematic lupus erythematosus.
Copyright © 2021 Wolters Kluwer
especially in the second trimester as a screening toolfor preeclampsia.
DIAGNOSTIC EVALUATION INGESTATIONAL HYPERTENSION
According to the majority of medical societies (ex-cept from WHO and USPSTF that make no relevantrecommendations), all pregnant women diagnosed withgestational hypertension, as well as those suspected forpreeclampsia, should undergo some further laboratorytests including full blood count (hemoglobin, PLTcount,white blood cells), liver and kidney function (liver en-zymes, serum creatinine), uric acid, and testing for protein-uria, in order to investigate the coexistence of end-organdamage and subsequently the development of preeclamp-sia. In particular, according to NICE, SOMANZ, andACOG, every pregnant woman diagnosed with gesta-tional hypertension should be tested for proteinuria 1to 2 times per week and undergo further weekly bloodtesting (full blood count, liver and kidney function). Ifsignificant proteinuria is confirmed, repeated assessmentsare not recommended by the NICE, FIGO, SOGC, andACOG guidelines. The SOMANZ guideline points outthat these women should also be physically examinedfor signs of preeclampsia since a study of 970 women
ISH ISSHP ESC
D in a previouspregnancy,KD, autoimmunedisease,type 1 or 2diabetes, chronichypertension
Preeclampsia in aprevious pregnancy,antiphospholipidsyndrome, type 1or 2 diabetes,chronic hypertension,BMI >30, assistedreproduction
HD in a previouspregnancy,
CKD, autoimmunedisease, type 1or 2 diabetes,chronichypertension
irst pregnancy,age ≥40 y, pregnancyinterval >10 y,MI ≥35,FH of preeclampsia,multifetal pregnancy
Advanced maternal age,FH of preeclampsia,sexual relationship<6 mo prior topregnancy,primipaternity,connective tissuediseases,FV Leiden
First pregnancy,age ≥40 y,pregnancyinterval >10 y,
BMI ≥35,FH of preeclampsia,multifetal pregnancy
rombophilias; increased prepregnancy triglycerides; nonsmoking;reased stress; mental health; short maternal stature; rural location;ship with current partner; reproductive technologies; booking SBPgnancy; gestational trophoblastic disease; abnormal PAPP-A or freel AFP, hCG, inhA, or E3; excessive weight gain in pregnancy; infectionry markers; anemia with low vitamins C and E intake; fathered preg-
y; GTD, gestational trophoblastic disease; HD, hypertensive disorder;
Health, Inc. All rights reserved.

625Gestational Hypertension and Preeclampsia • CME Review Article
found a strong association between the presence of clini-cal symptoms, abnormal laboratory values, and increasedmaternal morbidity.39 Moreover, according to FIGO andSOGC, the investigation of hypertension should includeurine analysis, pulse oximetry, and coagulation tests,whereas SOMANZ recommends these tests only if fea-tures of preeclampsia are present.Regarding proteinuria, the 24-hour urine collection,
although considered as the criterion-standard methodfor the quantification of proteinuria by the majority ofguidelines, it is impractical and frequently inaccurate40;therefore, it may be replaced by the easier dipstick test-ing (automated or visual). Hence, if dipstick screeningis ≥1+, it should be followed by the evaluation of spoturine protein-to-creatinine ratio (PCR) or albumin-to-creatinine ratio (ACR) (NICE, SOMANZ, ISH, ISSHP,ESC, FIGO, SOGC). Whereas ISH and ESC supportthat a urine ACR below 30 mg/mmol reliably excludesproteinuria in pregnancy, ISSHP and FIGO claim thatthere is lack of evidence on the accuracy of this testand thus recommend the PCR, based on the results of ameta-analysis.41 In contrast, ACOG recommends usingthe quantitative methods (ie, 24-hour urine collectionor PCR) first and, if not available, then utilizing the dip-stick test with a discriminant value of ≥2+. A prospectivestudy showed that a cutoff value of 2+ in dipstick test
FIGO SOGC ACOG
Preeclampsia in aprevious pregnancy,
CKD, antiphospholipidsyndrome, type 1 or2 diabetes, SLE,chronic hypertension,multiple pregnancy,booking proteinuria
Preeclampsia in aprevious pregnancy,
CKD, antiphospholipidsyndrome, type 1or 2 diabetes,chronic hypertension
Preeclampsia in aprevious pregnancy,
CKD, antiphospholipidsyndrome or SLE, type2 or gestational diabetemultifetal gestation,chronic hypertension,assisted reproduction
First pregnancy, age≥35–40 y, obesity,pregnancy interval >4 y,
FH of preeclampsia orearly onset CVD,previous miscarriage at≤10 wk with the samepartner or FGR, newpartner, other factors*
First pregnancy, multiplepregnancy, age ≥40 y,obesity, pregnancyinterval >10 y,
FH of preeclampsia orearly onset CVD,previous miscarriageat ≤10 wk with thesame partner, newpartner, other factors*
First pregnancy,age ≥35 y, BMI ≥30,
FH of preeclampsia,sociodemographiccharacteristics, personahistory factors (sleepapnea, thrombophilia)
Copyright © 2021 Wolters Kluwer
improves the overall diagnostic accuracy of preeclamp-sia, although having a higher false-negative rate.42 Nota-bly, USPSTF avoided any recommendation regardingthe preferred testing for proteinuria, due to the inconclu-sive results of a systematic review.38
In addition, for women with suspected preeclampsia,NICE recommends the performance of PlGF-basedtesting between 20 and 35 weeks of gestation, whereasSOMANZ and ISSHP highlight that the implementationof this test should be deferred until further supportingevidence is available. Moreover, the ESC guidelineacknowledges the ability of soluble fms-like tyrosinekinase-1 (sFlt-1) to PlGF ratio ≤38 to exclude an upcom-ing preeclampsia within the following 7 days. However,it does not make any further recommendations regard-ing a specific screening approach. Evidence from aprospective, multicenter, observational study demon-strated that a sFlt-1–to–PlGF ratio of 38 or lower hada negative predictive value (no preeclampsia in the sub-sequent week) of 99.3%, with 80.0% sensitivity and78.3% specificity.43
In addition, an ultrasound assessment of fetal well-beingat diagnosis is recommended by the NICE, SOMANZ,ISSHP, FIGO, SOGC, and ACOG guidelines. In con-trast, biophysical profile should not be part of the fetalmonitoring in hypertensive pregnancies, due to its poor
ISUOG WHO USPSTF
1 ors,
History,demographics,cardiovascularand metabolicprofile
Preeclampsia ina previouspregnancy,
CKD, autoimmunedisease, type 1 or2 diabetes,chronic hypertension
Preeclampsia oradverse outcomein a previouspregnancy, type 1,type 2, or gestationaldiabetes, chronichypertension, CKD,autoimmune disease,multiple pregnancy
l
Not discussed Obesity, first pregnancy,adolescent or multiplepregnancy
First pregnancy, obesity,advanced maternal age,African American, lowsocioeconomic status
Health, Inc. All rights reserved.

626 Obstetrical and Gynecological Survey
predictability on perinatal outcomes confirmed by a sec-ondary analysis of a cohort study.44
Finally, SOMANZ, ISH, and ESC report that ultrasoundof the kidneys and adrenals, as well as measurement offree plasma metanephrines, should only be consideredin case of clinically suspected pheochromocytoma.
ANTENATAL CARE
Regarding hospital admission, there is a consensusamong the reviewed guidelines that women with anonsevere gestational hypertension can be managed asoutpatients, taking into consideration that this strategyhas been shown to be both efficient and cost-effective.45
Hospital admission is recommended in cases of severehypertension, severe preeclampsia, and compromising fe-tal or maternal status. However, the ISSHP and FIGOstate that a pregnant woman should also be admitted tothe hospital at the time of preeclampsia diagnosis in orderto undergo appropriate assessment.In cases of diagnosed preeclampsia, NICE, SOMANZ,
and ISSHP recommend blood testing twice weekly, re-peated proteinuria assessment if not present at diagno-sis or if clinically indicated (NICE), and frequent BPmeasurements.Moreover, plasma volume expansion is not recom-
mended in preeclamptic women by SOMANZ, ISSHP,FIGO, SOGC, and ACOG, as a randomized controlledtrial (RCT) in 216 pregnant women depicted no clearmaternal or fetal benefit.46 Fluid administration shouldbe restricted to 80 mL/h (NICE, FIGO) unless ongoingfluid losses exist, in order to minimize the risk of pulmo-nary edema.18 Notably, the SOMANZ guideline suggeststhe bolus injection of extra fluid only in cases of hydral-azine treatment, regional anesthesia, immediate delivery,and oliguria with suspected or confirmed intravascularvolume deficit.Regarding the need for thromboprophylaxis, the
SOMANZ, FIGO, and SOGC guidelines point out thatalthough preeclampsia is an independent major risk factorfor venous thromboembolism in pregnancy and puerpe-rium, additional risk factors are required for the admin-istration of pharmacological prophylaxis.
FETAL SURVEILLANCE
The NICE and the SOMANZ guidelines recommendthe ultrasound assessment of fetal growth and amnioticfluid volume, as well as the UA Doppler velocimetry atthe time of gestational hypertension diagnosis and every 2to 4 weeks. They also recommend fetal heart auscultation(NICE) and assessment of fetal well-being (SOMANZ)at each antenatal visit. ACOG, while agreeing on fetalgrowth measurement every 3 to 4 weeks, supports the
Copyright © 2021 Wolters Kluwer
monitoring of amniotic fluid volume at shorter intervals(ie, at least once weekly). Moreover, ISSHP points outthat in cases of elevated uric acid levels, a detailed eval-uation of fetal growth is required since a retrospectivecohort study found that this finding is associated withadverse fetal outcomes even in women with gestationalhypertension without any preeclamptic features.47
To date, the optimal frequency and type of fetal eval-uation in pregnancies complicated by hypertensive dis-orders are not well determined, although HDPs areassociated with increased risk of adverse perinatal out-comes, as proven by a study including 8623 women.48
A meta-analysis of 12 RCTs proved that clinical actionguided by ultrasonographic findings of UAwaveformscan reduce perinatal deaths in high-risk pregnanciesby 38%.49
For cases complicated with preeclampsia, NICE,SOMANZ, and ISSHP suggest a more frequent ultraso-nographic assessment of the fetus, that is, at diagnosisand then every 2 weeks. In case of absent end-diastolicflow in the UA prior to 34 weeks, ISSHP recommendsdaily cardiotocography and UA Doppler and amnioticfluid volume assessment twice per week, whereas in caseof reversed end-diastolic flow prior to 30 weeks, hospitaladmission is required together with daily cardiotocographyand UADoppler and amniotic fluid volume assessment3 times per week. According to the SOMANZ guide-line, cardiotocography is recommended twice weekly,whereas NICE states that it should only be performedat diagnosis and repeated if maternal status is deteriorat-ing or the woman reports changes in fetal movements,vaginal bleeding, or abdominal pain.
MEDICALTREATMENT
Nonsevere Hypertension
Antihypertensive treatment is recommended whenBP levels are persistently higher than 140/90 mm Hg,according to the NICE, ISH, ISSHP, ESC, and FIGOguidelines since CHIPS (Control of Hypertension InPregnancy Study) confirmed that this strategy reducesthe adverse maternal outcomes without affecting theperinatal ones.50,51 On the other hand, the SOMANZ,SOGC, ACOG, andWHOguidelines, despite acknowl-edging the need for medical treatment to all womenwith severe hypertension (SBP ≥160 mm Hg and/or aDBP ≥110 mm Hg), point out that there are controver-sial data regarding the treatment of nonsevere hypertension.A Cochrane review concluded that medical treatmentof nonsevere HDPs neither prevents preeclampsia norimproves perinatal outcomes.52 Thus, no clear recom-mendation about the treatment of BP levels between
Health, Inc. All rights reserved.

627Gestational Hypertension and Preeclampsia • CME Review Article
140 and 160/90 and 110 mm Hg is provided by theseguidelines.There is an overall agreement among all reviewed
guidelines (ACOG makes recommendations only forthe urgent control of hypertension) that methyldopa,labetalol, and nifedipine should be the antihypertensivedrugs of choice. However, some discrepancies havebeen identified; NICE reports that methyldopa shouldbe administered only if the other 2 antihypertensivedrugs are not suitable, whereas SOMANZ supports thatnifedipine should be considered as a second-line agent.The latter, along with the ISSHP guideline, recommendthe use of oxprenolol as first-line medication for hyper-tension in pregnancy and prazosin and hydralazine assecond-line ones. This recommendation was based onan RCT including 183 pregnant women, which showedsuperiority of oxprenolol over methyldopa.53 On theother hand, FIGO discourages the use of prazosin dur-ing pregnancy since an RCT found an increase in still-births associated with the use of this medication.54 ACochrane meta-analysis of 22 trials found no clear dif-ference between any class of antihypertensive drugs inavoiding adverse maternal and perinatal outcomes.However, a reduction in the overall risk of developingproteinuria/preeclampsia was detected, when β-blockersand calcium-channel blockers, considered together, werecompared with methyldopa (relative risk, 0.73; 95%confidence interval, 0.54–0.99).52 Of note, angiotensin-converting enzyme inhibitors and angiotensin receptorblockers are contraindicated in pregnancy as they areassociated with significant fetal and neonatal complica-tions, such as low birth weight, preterm birth, miscar-riages, and renal malformations.55,56
With regard to the treatment targets, discrepanciesalso exist. More specifically, the DBP should be keptless than 85 mm Hg according to NICE, ISSHP, andFIGO, whereas SOGC supports that a DBP between80 and 105 mm Hg is acceptable for women withoutcomorbidities. The argument for “tight” control is basedon the results of the CHIPS trial, which showed thatkeeping the DBP at <85 mm Hg is associated withfewer cases of severe hypertension.51 Moreover, theideal levels for SBP recommended by NICE, ISSHP,and SOGC are ≤135 mm Hg, 110 to 140 mm Hg, and130 to 155 mm Hg, respectively. Notably, the FIGOand the SOGC guidelines highlight the need for lowertreatment targets in cases of severe comorbidities, suchas diabetes.
Severe Hypertension
Urgent admission to hospital and initiation of antihy-pertensives are required in cases of severe hypertension,
Copyright © 2021 Wolters Kluwer
as recommended by all guidelines except from ISUOGand USPSTF that lack relevant recommendations; oral ni-fedipine, intravenous hydralazine, and oral or intravenouslabetalol are the most common drugs of choice. A recentmeta-analysis proved that oral nifedipine can effectivelyand safely treat cases of severe hypertension in preg-nancy.57Moreover, anRCTcomparing intravenous hydral-azine and oral nifedipine found them equally effective inmanaging acute hypertensive emergencies in pregnancy.58
Alternative agents include methyldopa (ISH, ESC,and SOGC), diazoxide (SOMANZ), nicardipine andesmolol (ISH), urapidil (ISH, ESC), and clonidine(FIGO, SOGC). A Cochrane Database systematic re-view comparing these medications did not find signifi-cant differences in their safety and efficacy, except fromdiazoxide, which should better be avoided.59 Nitroglyc-erine infusion is the indicated medication in case of pre-eclampsia and pulmonary edema, according to the ESCguidelines. Of note, the NICE and the SOMANZ guide-lines highlight the importance of coadministration of250 to 500 mL of crystalloid fluid with hydralazine,so as to prevent a precipitous fall in BP levels and sub-sequent fetal distress due to placental hypoperfusion.Importantly, SOMANZ, FIGO, and SOGC recommendcontinuous fetal heart rate monitoring while treating se-vere hypertension until BP is stabilized.
Prevention and Treatment of Eclampsia
Magnesium sulfate should not be used solely as a an-tihypertensive medication; according to NICE, SOMANZ,ESC, FIGO, and ACOG, it should be the agent of choicefor the prevention of eclampsia and treatment of eclampticseizures, as Cochrane reviews confirmed its superiorityover other medications.60,61 Moreover, all guidelines(except ISUOG that does not provide any relevant rec-ommendation) recommend the administration of magne-sium sulfate in case of severe preeclampsia or severegestational hypertension with persistent neurologicalsymptoms, deterioration of laboratory tests (PLT count,liver or renal function), right upper quadrant/epigastricpain, proteinuria, or oliguria, in order to prevent the de-velopment of eclampsia. TheMagpie trial (MAGnesiumsulfate for PreventIon of Eclampsia), a randomizedplacebo-controlled trial including 10,141women, showedthat magnesium sulfate halves the risk of eclampsia andreduces maternal mortality without compromising theperinatal outcomes.62 Of note, the ISSHP supports theuse of this agent to all women with preeclampsia inlow-resource settings for convulsion prophylaxis dueto the favorable cost-benefit ratio.Regarding the appropriate dosage of magnesium sul-
fate, the NICE, SOMANZ, ISSHP, FIGO, SOGC, and
Health, Inc. All rights reserved.

628 Obstetrical and Gynecological Survey
ACOGguidelines agree on an intravenous loading doseof 4 g over 5 to 20 minutes followed by an infusion of1 g/h, based on the protocol used in the Magpie trial.62
NICE and SOMANZ recommend the continuation ofthe infusion for 24 hours after the last seizure or at leastfor 24 hours, whereas the ISSHP and the ACOG supportthat magnesium sulfate should continue to be adminis-tered for 24 hours postpartum, although the postnatalrole of this agent has not been fully elucidated yet be-cause of lack of adequately powered RCTs.63 Of note,intramuscular administration is also acceptable for theloading dose (10 g) and the maintenance regimen (5 gintramuscular every 4 hours for 24 hours), as well asin combination with the intravenous injection (ISSHP,FIGO, ACOG, WHO).
HELLP Syndrome
There is a consensus among the reviewed guidelinesthat HELLP (hemolysis, elevated liver enzymes, lowplatelets) syndrome (ie, hemolysis, elevated liver en-zymes, and low PLTs) should not be treated with corti-costeroids, as a Cochrane review demonstrated noimprovement in clinical outcomes.64 Platelet transfu-sion is indicated when PLTs are less than 20 � 109/Lor between 20 and 49 � 109/L, prior to cesarean deliv-ery or in case of excessive bleeding, known PLT dys-function, coagulopathy, or rapid fall in PLTs (FIGOand SOGC). SOMANZ also states that PLT transfusionshould be considered in cases of postpartum hemor-rhage, wound, or vulvar hematoma.
DELIVERY
Timing of Delivery
Most of the reviewed guidelines (NICE, SOMANZ,ISH, ESC, FIGO, SOGC, ACOG) agree regarding thetiming of delivery of pregnant women with uncompli-cated gestational hypertension, which should be at orbeyond 37 weeks of gestation. This recommendationis based on evidence from the HYPITAT trial (HYper-tension and Preeclampsia Intervention Trial At Term),a multicenter RCT, which showed that induction of la-bor for women with mild hypertensive disease beyond37 weeks of gestation is associated with improved ma-ternal outcomes.65 The ISSHP alone suggests expectantmanagement up to 39+6 weeks of gestation for pregnan-cies with well-controlled BP, reassuring fetal status, andno signs of preeclampsia, based on a multicenter obser-vational study, which found that induction of labor be-tween 38 and 39 weeks balances the lowest maternaland neonatal morbidity and mortality.66
Copyright © 2021 Wolters Kluwer
In terms of preeclampsia, there is a consensus for im-mediate delivery if it occurs after 37 weeks of gestation,according to the HYPITAT trial.65 Moreover, accordingto NICE, SOMANZ, ISSHP, FIGO, SOGC, ACOG, andWHO, although delivery is the definite treatment of pre-eclampsia, expectant management should be consideredin cases of preeclampsia without severe clinical featuresoccurring between 24 and 36+6 weeks of gestation, ide-ally in a tertiary center that can provide increased fetaland maternal surveillance and appropriate neonatal care.Two systematic reviews comparing expectant versus in-terventional care of early-onset preeclampsia found thatthe former is associated with improved neonatal out-comes; however, they report that the trials included wereunderpowered and provided insufficient evidence onmaternal morbidity.67,68 The HYPITAT-II trial provedthat expectant management should also be preferred forwomen with nonsevere HDP at 34 to 37 weeks of ges-tation, as the rate of maternal adverse outcomes is low,and immediate delivery increases the risk of neonatal re-spiratory distress syndrome.69 SOMANZ, ISSHP, FIGO,ACOG, and WHO consider termination of pregnancywhen preeclampsia develops before 24 weeks, that is,before reaching fetal viability. Expectant managementwas found to be associated with increased maternalcomplications and extremely low perinatal survival.70
RegardingHELLP syndrome, FIGO and SOGC recom-mend immediate delivery when it is diagnosed after35 weeks of gestation and delay of labor for steroids ad-ministration when it is diagnosed earlier.Importantly, all guidelines (except from WHO and
USPSTF that do not provide any relevant recommenda-tion) highlight that planned preterm delivery should beoffered to women with uncontrollable BP despite using3 antihypertensive drugs or severe complications suchas deterioration of liver or kidney function, hemostaticdisorders, pulmonary edema, maternal pulse oximetry<90%, neurological signs, myocardial infarction, stroke,placental abruption, abnormal UA Doppler waveforms,severe FGR, nonreassuring fetal status, and fetal death.
Mode of Delivery
The FIGO, SOGC, and ACOG guidelines highlightthat hypertension is not an absolute indication for cesar-ean delivery; vaginal birth should be offered unless spe-cific obstetric indications for cesarean delivery exist orpreterm birth is planned due to fetal compromise. NICEand ISSHP acknowledge that the decision should be in-dividualized based on the clinical circumstances and thewoman's preference. Hence, gestational hypertensionand preeclampsia are indications for induction of labor,whereas preeclampsia may be associated with reduced
Health, Inc. All rights reserved.

629Gestational Hypertension and Preeclampsia • CME Review Article
success rates of vaginal birth after previous cesarean de-livery.71,72 Published data reported that induction of la-bor does not worsen neonatal outcomes even in cases ofsevere early-onset preeclampsia, although it is rarelysuccessful before 28 weeks of gestation.73 Of note, pre-eclampsia is considered as a contraindication for exter-nal cephalic version in cases of breech presentation.74
Intrapartum Care
Regarding BPmonitoring during labor in women withgestational hypertension or preeclampsia, NICE recom-mends measurements every hour for mild hypertensionand every 15 to 30 minutes for severe hypertension. Italso supports that the second stage of labor should notbe accelerated routinely; however, operative vaginal de-livery should be offered in case of severe uncontrolledhypertension.75 Moreover, the SOMANZ, FIGO, SOGC,and ACOG guidelines suggest the use of epidural anal-gesia in the absence of contraindications, as it has beenproven to be both safe and beneficial for the fetus.76
FIGO and SOGC also support the active managementof the third stage of labor using oxytocin, especially incases of thrombocytopenia or coagulopathy, but discour-age the administration of ergometrine given its potentialto precipitate severe hypertension. Asmentioned byNICE,ISSHP, FIGO, and SOGC, antenatal antihypertensive treat-ment should be continued intrapartum. Finally, ISSHPpoints out that, when FGR is detected, cord arterial and ve-nous pH should be recorded. Moreover, intrapartum mon-itoring with continuous cardiotocography during labor, forpregnancies complicated by HDP, is a reasonable option.
Corticosteroids and Magnesium Sulfate forPreterm Delivery
In general, there is an agreement between the NICE,SOMANZ, ISSHP, FIGO, and SOGC guidelines, con-cerning the administration of corticosteroids for fetal lungmaturation for planned deliveries, before 34+0 weeks ofgestation, in pregnancies complicated by any hyperten-sive disorder.77,78 However, these medical societies havenot adopted a common strategy regarding the use of ste-roids after 34+0 weeks of gestation. In particular, NICEmentions that antenatal steroids may be considered up to36+0 weeks, FIGO and SOGC suggest an upper limit of34+0 weeks, whereas ISSHP and SOMANZ recommendsteroids' administration for up to 38 weeks in case of elec-tive cesarean section. However, SOMANZ and ACOGpoint out that urgent delivery after 34 weeks of gestationfor pregnancies complicated with gestational hyperten-sion or preeclampsia should not be delayed to allow ad-ministration of corticosteroids.
Copyright © 2021 Wolters Kluwer
NICE, SOMANZ, ISSHP, FIGO, and SOGC supportthe use of magnesium sulfate for fetal neuroprotection incase of preterm delivery before 30 (SOMANZ), 32 (ISSHP,SOGC), or 34 (FIGO, NICE) weeks of gestation.77 ACochrane review indicated that the administration ofmagnesium sulfate to women requiring preterm deliv-ery reduces significantly the risk of neonatal cerebralpalsy.79
POSTNATAL CARE
There is no consensus regarding postpartummonitoringof women with gestational hypertension or preeclampsia;hypertension usually resolves after birth, but it can alsopresent for the first time in the early puerperium. Thus,FIGO and SOGC recommend, for cases with gestationalhypertension, 1 BP measurement at days 3 to 6 after de-livery, as this is the time of anticipated peak postpartumBP elevation; if hypertension is detected, investigation forpostpartum preeclampsia is required. Moreover, in casesof antenatal preeclampsia, the resolution of end-organdysfunction should be confirmed, according to thesemed-ical societies. On the other hand, the NICE and the ISSHPguidelines state that, in preeclamptic women, BP shouldbemeasured at least 4 times per day during the first 3 dayspostpartum, and blood tests including hemoglobin, PLTcount, creatinine, and liver enzymes should be performed24 (ISSHP) or 48 to 72 (NICE) hours after birth. Repe-tition of these blood tests is recommended only if theyhave been abnormal according to NICE or every 2 daysuntil normalization according to ISSHP. Moreover, NICEstates that for gestational hypertension, BP should bemeasured once daily for the first 2 days postpartumand once between days 3 and 5. If BP does not nor-malize until then, serial measurements on alternate daysare needed.Seven guidelines (NICE, SOMANZ, ISH, ISSHP, FIGO,
SOGC, and WHO) agree that antihypertensive treatmentshould be continued after birth if BP remains elevated, al-though a Cochrane review concluded that there are no re-liable data to guide clinical practice on this matter.80 Thetarget is to maintain BP levels at less than 130/80 mmHgfor women with pregestational diabetes mellitus and lessthan 140/90 mm Hg for the rest of the women, with orwithout comorbidities (FIGO, SOGC). NICE suggests re-ducing treatment if BP falls less than 130/80 mm Hg andinitiating treatment (to women who did not receive anti-hypertensive drugs during pregnancy) if postpartum BPlevels exceed 150/100 mm Hg. Moreover, methyldopashould be replaced by an alternative agent as a recentreview proved its association with the emergence ofpostnatal depression.81 All the other agents can safely be
Health, Inc. All rights reserved.

630 Obstetrical and Gynecological Survey
administered in the puerperium, and they are compatiblewith breastfeeding, according to a systematic review.82
SOMANZ, ISSHP, FIGO, and SOGC discourage theuse of nonsteroidal anti-inflammatory drugs for postpar-tum analgesia in womenwith HDP, especially in cases ofpoorly controlled hypertension, acute or chronic kidneydisease, and thrombocytopenia, because these drugs canincrease BP, reduce renal perfusion, and cause anti-PLTeffects.83 In contrast, ACOG supports their use over opi-oid analgesics based on a retrospective study demon-strating that nonsteroidal anti-inflammatory drugs donot increase the average postpartum BP levels, the re-quirement for antihypertensive medications, or the rateof adverse postpartum events.84
FOLLOW-UP
In cases of persistent hypertension in the puerperium,NICE and ISSHP recommend a medical review 1 to2 weeks after delivery for those women who remain onantihypertensive treatment. Moreover, all women whoexperience gestational hypertension or preeclampsiashould be reevaluated at 6 weeks postpartum, accordingto NICE, FIGO, and SOGC. The former suggests theperformance of a urinary dipstick test at that time, soas to identify women with persistent proteinuria (≥1+)and offer them a renal function assessment 3 monthslater. On the other hand, ISSHP suggests a reevaluation3 months after delivery for all women with gestationalhypertension or preeclampsia so as to confirm resolutionof hypertension and laboratory abnormalities and then anannual review. Appropriate specialist referral is requiredfor severe preeclampsia or preeclampsia presenting before34 weeks of gestation, poorly controlled hypertension,ongoing proteinuria, decreased estimated glomerular fil-tration rate, or another indication of renal disease at 3 to6 months postpartum (FIGO, SOGC). Assessment of car-diovascular risk and advice on healthy diet and lifestylemodifications are also recommended by all the aforemen-tioned medical societies. Women should also be informedabout their increased risk of developing preeclampsia orgestational hypertension in future pregnancies.
PREVENTION OF PREECLAMPSIA
After evaluating the individual risk of developingpreeclampsia based on maternal factors alone (NICE,SOMANZ, ISH, ISSHP, ESC, SOGC, ACOG, WHO, andUSPSTF) or on the combined screening test (FIGO,ISUOG), the reviewed guidelines unanimously recommendthe daily administration of low-dose aspirin to high-riskpregnant women starting from 12 weeks of gestation,ideally before 16weeks, until 36 to 37weeks (SOMANZ,ISH, ESC) or until delivery (NICE, SOGC, ACOG). This
Copyright © 2021 Wolters Kluwer
recommendation is based on the ASPRE trial, whichproved that 150 mg of daily aspirin reduces the risk ofpreterm preeclampsia by 62%.85 According to NICE,ISH, ESC, SOGC, and ACOG, women at high risk areconsidered those with at least 1 high or more than 1moderate risk factor. The optimal time of aspirin ad-ministration is at bedtime, as proven by a prospective,randomized trial, which found that bedtime ingestionof aspirin (compared with ingestion upon awakeningor 8 hours later) best regulates BP and reduces the inci-dence of preeclampsia.86 However, the appropriate dos-age is an issue of controversy; the suggested dose variesfrom 75 to 162 mg/d (NICE: 75–150 mg/d; ISH, ISSHP,SOGC: 75–162 mg/d; ESC: 100–150 mg/d; FIGO,ISUOG: 150 mg/d; ACOG, USPSTF: 81 mg/d; WHO:75 mg/d). Notably, evidence from a systematic reviewand meta-analysis showed that a dose of less than 100 mgdoes not improve pregnancy outcomes,87 while a trialfound that 2.5 to 3.5 mg/kg is the required dosage to pro-duce statistically significant improvement.88 Moreover,a prospective cohort study demonstrated that 10% to30% of patients present resistance to 81 mg/d.89
Calcium supplementation to prevent preeclampsia inpregnant women with a low dietary calcium intake, es-pecially those at high risk for preeclampsia, has beensuggested by several medical societies (SOMANZ,ISH, ISSHP, ESC, FIGO, SOGC, ACOG, and WHO).This recommendation is mainly based on a Cochrane re-view, which showed that calcium supplementation re-duces the risk of preeclampsia by approximately 50%.90
The proposed dosage is 1.5 to 2 g οf elemental calciumper day orally.91 On the other hand, interventions suchas salt restriction, bed rest, and administration of antioxi-dants (vitamins C and E) are not recommended, as severalstudies argue against their effectiveness.92–95 The use offolic acid (SOMANZ, FIGO, SOGC, ACOG), progester-one (NICE), diuretics (NICE, SOGC, WHO), and nitricoxide donors (NICE, FIGO) is currently discouraged be-cause of scarce and conflicting data. Finally, the administra-tion of heparin is discouraged by NICE, SOMANZ, andISSHP as 2 RCTs showed no benefit.96,97 However,SOGC and FIGO state that the use of low-molecular-weight heparin should be considered for women with pre-vious placental complications, based on ameta-analysis.98
CONCLUSIONS
There is an overall consensus among the reviewedguidelines for the need of screening for preeclampsia,the required diagnostic investigations, the managementof preeclampsia, the optimal timing and mode of deliv-ery for gestational hypertension and preeclampsia, andthe indications for the administration of corticosteroids
Health, Inc. All rights reserved.

631Gestational Hypertension and Preeclampsia • CME Review Article
and magnesium sulfate, with some discrepancies re-garding the prompt gestational age to administer theseagents. In addition, they all agree on the type of appro-priate medical treatment for gestational hypertension/preeclampsia, although there are minor inconsistenceson the choice of first- and second-line medications.On the other hand, the main issues of controversy
among the reviewed guidelines lie in the definition ofpreeclampsia, the optimal BP treatment targets, thepostnatal BP monitoring, and the appropriate screeningtools for preeclampsia. ISSHP, FIGO, and ISUOG arein favor of the combined screening strategy (ie, usingmaternal factors, maternal arterial BP, UtA Doppler,and PlGF levels), whereas the USPSTF, ESC, and theSOGC guidelines do not support it. Finally, althoughNICE, ISH, ISSHP, ESC, and FIGO recommend medi-cal treatment of nonsevere hypertension, SOMANZ,ACOG, andWHO recommend treatment only for casesof severe hypertension.Gestational hypertension and preeclampsia are major
contributors of maternal and perinatal morbidity andmortality worldwide, especially when left untreated ormanaged in a suboptimal way, with their incidence ris-ing in high-income countries due to the increasing ma-ternal age and obesity. The multifactorial pathogenesisof different preeclampsia phenotypes has not been fullyelucidated yet, rendering its accurate prediction anduniform prevention difficult. These facts underline theimportance of adopting consistent international proto-cols in all areas of controversy, in order to achieve earlyassessment and intervention and subsequently improvethe outcomes of such pregnancies. Further large-scalewell-designed studies are required to adopt a commonoptimal screening and management strategy amongvarious medical societies and physicians.
REFERENCES1. Unger T, Borghi C, Charchar F, et al. 2020 International Society of
Hypertension global hypertension practice guidelines. JHypertens.2020;38:982–1004.
2. Cunningham FG, Leveno KJ, Bloom SL, et al. Pregnancy hyper-tension. In: Cunningham FG, ed. Williams Obstetrics. 23rd ed.New York: McGraw-Hill Professional; 2009.
3. Khan KS, Wojdyla D, Say L, et al. WHO analysis of causes of ma-ternal death: a systematic review. Lancet. 2006;367:1066–1074.
4. Ghulmiyyah L, Sibai B. Maternal mortality from preeclampsia/eclampsia. Semin Perinatol. 2012;36:56–59.
5. Tsakiridis I, Arvanitaki A, Zintzaras E. Assessing the reportingquality of systematic reviews of observational studies in pre-eclampsia. Arch Gynecol Obstet. 2019;299:689–694.
6. Brown MC, Best KE, Pearce MS, et al. Cardiovascular diseaserisk in women with pre-eclampsia: systematic review and meta-analysis. Eur J Epidemiol. 2013;28:1–19.
7. Williams D. Long-term complications of preeclampsia. SeminNephrol. 2011;31:111–122.
Copyright © 2021 Wolters Kluwer
8. Tsakiridis I, Mamopoulos A, Athanasiadis A, et al. Management ofpregestational diabetes mellitus: a comparison of guidelines.J Matern Fetal Neonatal Med. 2020;1–10.
9. Tsakiridis I, Giouleka S, Mamopoulos A, et al. Diagnosis andmanagement of gestational diabetes mellitus: an overview ofnational and international guidelines. Obstet Gynecol Surv.2021;76:367–381.
10. Gruslin A, Lemyre B. Pre-eclampsia: fetal assessment andneonatal outcomes. Best Pract Res Clin Obstet Gynaecol. 2011;25:491–507.
11. Olusanya BO, Solanke OA. Perinatal outcomes associated withmaternal hypertensive disorders of pregnancy in a developingcountry. Hypertens Pregnancy. 2012;31:120–130.
12. NICE. NICE guideline. Hypertension in pregnancy: diagnosis andmanagement. Published June 25, 2019. Available at: https://www.nice.org.uk/guidance/ng133. Accessed January 3, 2021.
13. Lowe SA, Bowyer L, Lust K, et al. The SOMANZ guidelines for themanagement of hypertensive disorders of pregnancy 2014. AustN Z J Obstet Gynaecol. 2015;55:11–16.
14. Brown MA, Magee LA, Kenny LC, et al. The hypertensive disor-ders of pregnancy: ISSHP classification, diagnosis & manage-ment recommendations for international practice. PregnancyHypertens. 2018;13:291–310.
15. Regitz-Zagrosek V, Roos-Hesselink JW, Bauersachs J, et al.2018 ESC guidelines for the management of cardiovascular dis-eases during pregnancy. Eur Heart J. 2018;39:3165–3241.
16. Magee LA, von Dadelszen P, StonesW, et al. The FIGO Textbookof Pregnancy Hypertension: An Evidence-Based Guide to Moni-toring, Prevention and Management. London: The Global Libraryof Women’s Medicine; 2016.
17. Poon LC, Shennan A, Hyett JA, et al. The International Federationof Gynecology and Obstetrics (FIGO) initiative on pre-eclampsia:a pragmatic guide for first-trimester screening and prevention. IntJ Gynaecol Obstet. 2019;145(suppl 1):1–33.
18. Magee LA, Pels A, Helewa M, et al. Diagnosis, evaluation, andmanagement of the hypertensive disorders of pregnancy: execu-tive summary. J Obstet Gynaecol Can. 2014;36:416–441.
19. American College of Obstetricians and Gynecologists' Commit-tee on Practice Bulletins—Obstetrics. Gestational hypertensionand preeclampsia: ACOG practice bulletin, number 222. ObstetGynecol. 2020;135:e237–e260.
20. Sotiriadis A, Hernandez-Andrade E, da Silva Costa F, et al.ISUOG practice guidelines: role of ultrasound in screening forand follow-up of pre-eclampsia. Ultrasound Obstet Gynecol.2019;53:7–22.
21. World Health Organization.WHO Recommendations for Pre-vention and Treatment of Pre-eclampsia and Eclampsia.2011. Available at: http://apps.who.int/iris/bitstream/handle/10665/44703/9789241548335_eng.pdf?sequence=1. AccessedJanuary 3, 2021.
22. US Preventive Services Task Force, Bibbins-Domingo K, GrossmanDC, et al. Screening for preeclampsia: US Preventive ServicesTask Force recommendation statement. JAMA. 2017;317:1661–1667.
23. Davis GK, Roberts LM, Mangos GJ, et al. Comparisons of aus-cultatory hybrid and automated sphygmomanometers withmercury sphygmomanometry in hypertensive and normoten-sive pregnant women: parallel validation studies. J Hypertens.2015;33:499–505 discussion 506.
24. Ogedegbe G, Pickering T. Principles and techniques of bloodpressure measurement. Cardiol Clin. 2010;28:571–586.
25. Bergel E, Carroli G, Althabe F. Ambulatory versus conventionalmethods for monitoring blood pressure during pregnancy.Cochrane Database Syst Rev. 2002;2:CD001231.
26. Bellomo G, Narducci PL, Rondoni F, et al. Prognostic valueof 24-hour blood pressure in pregnancy. JAMA. 1999;282:1447–1452.
27. Brown MA, Robinson A, Bowyer L, et al. Ambulatory blood pres-sure monitoring in pregnancy: what is normal? Am J ObstetGynecol. 1998;178:836–842.
Health, Inc. All rights reserved.

632 Obstetrical and Gynecological Survey
28. Homer CS, Brown MA, Mangos G, et al. Non-proteinuric pre-eclampsia: a novel risk indicator in women with gestational hy-pertension. J Hypertens. 2008;26:295–302.
29. Tsakiridis I, Giouleka S, Arvanitaki A, et al. Chronic hypertensionin pregnancy: synthesis of influential guidelines. J Perinat Med.2021;49:859–872.
30. Tsakiridis I, Giouleka S, Mamopoulos A, et al. Management oftwin pregnancies: a comparative review of national and interna-tional guidelines. Obstet Gynecol Surv. 2020;75:419–430.
31. Tsakiridis I, Giouleka S, Kalogiannidis I, et al. Diagnosis andman-agement of gestational trophoblastic disease: a comparative re-view of national and international guidelines. Obstet GynecolSurv. 2020;75:747–756.
32. O'Gorman N, Wright D, Syngelaki A, et al. Competing risksmodel in screening for preeclampsia by maternal factors andbiomarkers at 11–13 weeks gestation. Am J Obstet Gynecol.2016;214:103.e1–103.e12.
33. Rolnik DL, Wright D, Poon LC, et al. Aspirin versus placebo inpregnancies at high risk for preterm preeclampsia. N Engl JMed. 2017;377:613–622.
34. Dagklis T, Tsakiridis I, Zavlanos A, et al. The effect of placentallaterality at 20–24 gestational weeks on uterine artery Doppler in-dices, fetal growth and preeclampsia. J Matern Fetal NeonatalMed. 2020;1–6.
35. Francisco C, Wright D, Benko Z, et al. Competing-risks model inscreening for pre-eclampsia in twin pregnancy according to ma-ternal factors and biomarkers at 11–13 weeks' gestation. Ultra-sound Obstet Gynecol. 2017;50:589–595.
36. Morris RK, Bilagi A, Devani P, et al. Association of serumPAPP-Alevels in first trimester with small for gestational age and adversepregnancy outcomes: systematic review and meta-analysis.Prenat Diagn. 2017;37:253–265.
37. Meads CA, Cnossen JS, Meher S, et al. Methods of predictionand prevention of pre-eclampsia: systematic reviews of accuracyand effectiveness literature with economic modelling. HealthTechnol Assess. 2008;12:iii–iv 1–270.
38. Henderson JT, Thompson JH, Burda BU, et al.Screening for Pre-eclampsia: A Systematic Evidence Review for the US PreventiveServices Task Force. US Preventive Services Task Force EvidenceSyntheses, Formerly Systematic Evidence Reviews. Rockville, MD:Agency for Healthcare Research and Quality (US); 2017.
39. Martin JN Jr., May WL, Magann EF, et al. Early risk assessmentof severe preeclampsia: admission battery of symptoms and labora-tory tests to predict likelihood of subsequent significant maternalmorbidity. Am J Obstet Gynecol. 1999;180(6 pt 1):1407–1414.
40. Cote AM, Firoz T, Mattman A, et al. The 24-hour urine collection:gold standard or historical practice? Am J Obstet Gynecol.2008;199:625.e1–625.e6.
41. Morris RK, Riley RD, Doug M, et al. Diagnostic accuracy of spoturinary protein and albumin to creatinine ratios for detection ofsignificant proteinuria or adverse pregnancy outcome in patientswith suspected pre-eclampsia: systematic review and meta-analysis. BMJ. 2012;345:e4342.
42. Phelan LK, BrownMA, Davis GK, et al. A prospective study of theimpact of automated dipstick urinalysis on the diagnosis of pre-eclampsia. Hypertens Pregnancy. 2004;23:135–142.
43. Zeisler H, Llurba E, Chantraine F, et al. Predictive value of thesFlt-1:PlGF ratio in women with suspected preeclampsia. N EnglJ Med. 2016;374:13–22.
44. Payne BA, Kyle PM, Lim K, et al. An assessment of predictivevalueof thebiophysical profile inwomenwithpreeclampsia usingdatafrom the fullPIERS database. Pregnancy Hypertens. 2013;3:166–171.
45. Barton JR, Istwan NB, Rhea D, et al. Cost-savings analysis of anoutpatientmanagement program forwomenwith pregnancy-relatedhypertensive conditions. Dis Manag. 2006;9:236–241.
46. Ganzevoort W, Rep A, Bonsel GJ, et al. A randomised controlledtrial comparing two temporising management strategies, onewith and one without plasma volume expansion, for severe andearly onset pre-eclampsia. BJOG. 2005;112:1358–1368.
Copyright © 2021 Wolters Kluwer
47. Hawkins TL, Roberts JM, Mangos GJ, et al. Plasma uric acid re-mains a marker of poor outcome in hypertensive pregnancy: aretrospective cohort study. BJOG. 2012;119:484–492.
48. Bakker R, Steegers EA, Hofman A, et al. Blood pressure in differentgestational trimesters, fetal growth, and the risk of adverse birth out-comes: the Generation R study. Am J Epidemiol. 2011;174:797–806.
49. Alfirevic Z,Neilson JP. Doppler ultrasonography in high-risk preg-nancies: systematic review with meta-analysis. Am J ObstetGynecol. 1995;172:1379–1387.
50. Magee LA, von Dadelszen P, Singer J, et al. The CHIPS random-ized controlled trial (control of hypertension in pregnancy study):is severe hypertension just an elevated blood pressure? Hyper-tension. 2016;68:1153–1159.
51. Magee LA, vonDadelszenP, ReyE, et al. Less-tight versus tight controlof hypertension in pregnancy.N Engl J Med. 2015;372:407–417.
52. Abalos E, Duley L, Steyn DW. Antihypertensive drug therapy formild to moderate hypertension during pregnancy. Cochrane Da-tabase Syst Rev. 2014;2:CD002252.
53. Gallery ED, Ross MR, Gyory AZ. Antihypertensive treatment inpregnancy: analysis of different responses to oxprenolol andmethyldopa. Br Med J (Clin Res Ed). 1985;291:563–566.
54. Hall DR, Odendaal HJ, Steyn DW, et al. Nifedipine or prazosin asa second agent to control early severe hypertension in preg-nancy: a randomised controlled trial. BJOG. 2000;107:759–765.
55. Ratnapalan S, Koren G. Taking ACE inhibitors during pregnancy.Is it safe? Can Fam Physician. 2002;48:1047–1049.
56. Moretti ME, Caprara D, Drehuta I, et al. The fetal safety of angio-tensin converting enzyme inhibitors and angiotensin II receptorblockers. Obstet Gynecol Int. 2012;2012:658310.
57. Shekhar S, Gupta N, Kirubakaran R, et al. Oral nifedipine versusintravenous labetalol for severe hypertension during pregnancy:a systematic review and meta-analysis. BJOG. 2016;123:40–47.
58. Sharma C, Soni A, Gupta A, et al. Hydralazine vs nifedipine foracute hypertensive emergency in pregnancy: a randomized con-trolled trial. Am J Obstet Gynecol. 2017;217:687.e1–687.e6.
59. Duley L, Meher S, Jones L. Drugs for treatment of very high bloodpressure during pregnancy. Cochrane Database Syst Rev. 2013;7:CD001449.
60. Duley L, Gulmezoglu AM, Chou D. Magnesium sulphate versuslytic cocktail for eclampsia. Cochrane Database Syst Rev.2010;9:CD002960.
61. Duley L, Henderson-Smart DJ, Walker GJ, et al. Magnesium sul-phate versus diazepam for eclampsia. Cochrane Database SystRev. 2010;12:CD000127.
62. AltmanD,Carroli G, Duley L, et al. Dowomenwith pre-eclampsia, andtheir babies, benefit from magnesium sulphate? The Magpie Trial: arandomised placebo-controlled trial. Lancet. 2002;359:1877–1890.
63. Vigil-DeGracia P, Ludmir J. The use ofmagnesium sulfate for womenwith severe preeclampsia or eclampsia diagnosed during the postpar-tum period. J Matern Fetal Neonatal Med. 2015;28:2207–2209.
64. Woudstra DM, Chandra S, Hofmeyr GJ, et al. Corticosteroids forHELLP (hemolysis, elevated liver enzymes, low platelets) syndromein pregnancy. Cochrane Database Syst Rev. 2010;9:CD008148.
65. Koopmans CM, Bijlenga D, Groen H, et al. Induction of labourversus expectant monitoring for gestational hypertension or mildpre-eclampsia after 36 weeks' gestation (HYPITAT): a multicentre,open-label randomised controlled trial. Lancet. 2009;374:979–988.
66. Cruz MO, GaoW, Hibbard JU. What is the optimal time for deliv-ery in women with gestational hypertension? Am J ObstetGynecol. 2012;207:214.e1–214.e6.
67. Churchill D, Duley L. Interventionist versus expectant care for se-vere pre-eclampsia before term. Cochrane Database Syst Rev.2002;3:CD003106.
68. Magee LA, Yong PJ, Espinosa V, et al. Expectant management ofsevere preeclampsia remote from term: a structured systematicreview. Hypertens Pregnancy. 2009;28:312–347.
69. Broekhuijsen K, van Baaren GJ, van Pampus MG, et al. Immedi-ate delivery versus expectant monitoring for hypertensive disor-ders of pregnancy between 34 and 37 weeks of gestation
Health, Inc. All rights reserved.

633Gestational Hypertension and Preeclampsia • CME Review Article
(HYPITAT-II): an open-label, randomised controlled trial. Lancet.2015;385:2492–2501.
70. Sibai BM, Barton JR. Expectant management of severe preeclamp-sia remote from term: patient selection, treatment, and delivery indi-cations. Am J Obstet Gynecol. 2007;196:514.e1–514.e9.
71. Tsakiridis I, Mamopoulos A, Athanasiadis A, et al. Induction of la-bor: anoverviewof guidelines.ObstetGynecol Surv. 2020;75:61–72.
72. Tsakiridis I, Mamopoulos A, Athanasiadis A, et al. Vaginal birth af-ter previous cesarean birth: a comparison of 3 national guide-lines. Obstet Gynecol Surv. 2018;73:537–543.
73. Alanis MC, Robinson CJ, Hulsey TC, et al. Early-onset severe pre-eclampsia: induction of labor vs elective cesarean delivery and neo-natal outcomes. Am J Obstet Gynecol. 2008;199:262.e1–262.e6.
74. Tsakiridis I,Mamopoulos A, Athanasiadis A, et al. Management ofbreech presentation: a comparison of four national evidence-basedguidelines. Am J Perinatol. 2020;37:1102–1109.
75. Tsakiridis I, Giouleka S, Mamopoulos A, et al. Operative vaginaldelivery: a review of four national guidelines. J Perinat Med.2020;48:189–198.
76. Reynolds F. Labour analgesia and the baby: good news is nonews. Int J Obstet Anesth. 2011;20:38–50.
77. Tsakiridis I, Mamopoulos A, Athanasiadis A, et al. Antenatalcorticosteroids and magnesium sulfate for improved pretermneonatal outcomes: a review of guidelines.Obstet Gynecol Surv.2020;75:298–307.
78. Dagklis T, Tsakiridis I, Papazisis G, et al. Efficacy and safety ofcorticosteroids' administration for pulmonary immaturity in an-ticipated preterm delivery. Curr Pharm Des. 2020. doi: 10.2174/1381612826666201207102910.
79. Doyle LW, Crowther CA, Middleton P, et al. Magnesium sulphatefor women at risk of preterm birth for neuroprotection of the fetus.Cochrane Database Syst Rev. 2009;1:CD004661.
80. Magee L, von Dadelszen P. Prevention and treatment of postpar-tum hypertension.Cochrane Database Syst Rev. 2013;CD004351.
81. Wiciński M, Malinowski B, Puk O, et al. Methyldopa as an induc-tor of postpartum depression and maternal blues: a review.Biomed Pharmacother. 2020;127:110196.
82. Beardmore KS, Morris JM, Gallery ED. Excretion of antihyperten-sive medication into human breast milk: a systematic review.Hypertens Pregnancy. 2002;21:85–95.
83. Makris A, ThorntonC, Hennessy A. Postpartum hypertension andnonsteroidal analgesia. Am J Obstet Gynecol. 2004;190:577–578.
84. Wasden SW, Ragsdale ES, Chasen ST, et al. Impact ofnon-steroidal anti-inflammatory drugs on hypertensive disordersof pregnancy. Pregnancy Hypertens. 2014;4:259–263.
Copyright © 2021 Wolters Kluwer
85. RolnikDL,Wright D, Poon LCY, et al. ASPRE trial: performance ofscreening for preterm pre-eclampsia. Ultrasound Obstet Gynecol.2017;50:492–495.
86. Ayala DE, Ucieda R, Hermida RC. Chronotherapy with low-doseaspirin for prevention of complications in pregnancy. ChronobiolInt. 2013;30(1–2):260–279.
87. Roberge S, Bujold E, Nicolaides KH. Aspirin for the prevention ofpreterm and term preeclampsia: systematic review and metaanalysis.Am J Obstet Gynecol. 2018;218:287–293.e1.
88. Masotti G, Galanti G, Poggesi L, et al. Differential inhibition ofprostacyclin production and platelet aggregation by aspirin. Lan-cet. 1979;2:1213–1217.
89. Caron N, Rivard GE, Michon N, et al. Low-dose ASA responseusing the PFA-100 in women with high-risk pregnancy. J ObstetGynaecol Can. 2009;31:1022–1027.
90. HofmeyrGJ, Lawrie TA,AtallahAN, et al. Calciumsupplementationdur-ing pregnancy for preventing hypertensive disorders and related prob-lems. Cochrane Database Syst Rev. 2010;8:CD001059.
91. Tsakiridis I, Kasapidou E, Dagklis T, et al. Nutrition in pregnancy:a comparative review of major guidelines. Obstet Gynecol Surv.2020;75:692–702.
92. Villar J, Purwar M, Merialdi M, et al. World Health Organisationmulticentre randomised trial of supplementation with vitamins Cand E among pregnant women at high risk for pre-eclampsia inpopulations of low nutritional status from developing countries.BJOG. 2009;116:780–788.
93. Rumbold A, Duley L, Crowther CA, et al. Antioxidants forpreventing pre-eclampsia.Cochrane Database Syst Rev. 2008;1:CD004227.
94. Gulmezoglu AM, Hofmeyr GJ. Bed rest in hospital for suspectedimpaired fetal growth.CochraneDatabaseSyst Rev. 2000;2:CD000034.
95. Meher S, Duley L. Rest during pregnancy for preventingpre-eclampsia and its complications in womenwith normal bloodpressure. Cochrane Database Syst Rev. 2006;2:CD005939.
96. Martinelli I, Ruggenenti P, Cetin I, et al. Heparin in pregnantwomen with previous placenta-mediated pregnancy complica-tions: a prospective, randomized, multicenter, controlled clinicaltrial. Blood. 2012;119:3269–3275.
97. Groom KM, McCowan LM, Mackay LK, et al. Enoxaparin for theprevention of preeclampsia and intrauterine growth restriction inwomen with a history: a randomized trial. Am J Obstet Gynecol.2017;216:296.e1–296.e14.
98. Rodger MA, Carrier M, Le Gal G, et al. Meta-analysis of low-molecular-weight heparin to prevent recurrent placenta-mediatedpregnancy complications. Blood. 2014;123:822–828.
Health, Inc. All rights reserved.