volume 11 number 3 summer 2002 a short history of … · volume 11 number 3 summer 2002 the renal...
TRANSCRIPT

This publication is a part of the K/DOQI Learning System (KLS)™ and is made
possible in part through an educational grant from
the Title and Founding Sponsor of K/DOQI
in this issue
VOLUME 11 NUMBER 3 SUMMER 2002
The Renal Community’s Newspaper
Good Nutrition
page 4
Fitness
page 5
Choices
page 9
Transplant Column
page 13
National KidneyFoundation®
Chronic dialysis became a reali-ty in the mid to late 1960sbasically due to the pioneering
work of Belding Scribner, MD inSeattle. Dr. Scribner showed that onceyou had a reusable vascular accesspeople could not only dialyze chroni-cally in the hospital setting but for thefirst time they could also perform theprocedure at home. This first groupselected to initiate home dialysis werehighly motivated individuals.
Many of these initial home patientswere supported by a Public HealthService (PHS) grant that from 1968to 1972 made it possible to acceptpeople even when they had no insur-ance. Those on home hemodialysisdialyzed eight to 11 hours, three timesa week on Kiil dialyzers that they“built” themselves from sheets ofcuprophane that were sterilized withformaldehyde once they were pressuretested. No blood pumps were neces-sary as the patients’ own arterial sys-tems pushed the blood through thelow-pressure system.
By the early 1970s, it hadbecome evident that morepeople could be dialyzed in-center and for a shorter peri-od of time using commercialdialysis coils. This alsoallowed people to dialyzewho had no “helper” forhome hemodialysis or whosehome situation was not suit-able for dialysis. In 1972,with passage by Congress ofHR1, Medicare was expand-ed to those with chronic kid-ney failure of any age. Medicare beganpaying for most dialysis and kidneytransplantation as of July 1, 1973.Following this event, in-center dialysisbegan to grow and soon passed thehome as the favored site of chronicdialysis. The rest of the 1970s sawtremendous growth in size and numberof dialysis units to meet the increasingdemand. In addition, the time requiredfor dialysis was reduced, which allowedtwo patient dialysis shifts to occur in a10-hour period.
In the 1980s, Jack Moncrieff, MDand his colleagues in Austin, Texasdeveloped chronic ambulatory peri-toneal dialysis (CAPD). CAPD providedpeople with another dialysis option andthe opportunity to dialyze independent-ly in the home setting. CAPD used theperitoneal membrane of the abdomenin place of cuprophane. The Austingroup’s initial dialysis was based onfive-two liter exchanges each day.
CAPD initially captured a significantpart of the United States (U.S.) market,with15-20 percent of those on dialysisselecting this modality. CAPD has sincetapered off to 10 or 11 percent for anumber of reasons. A majority of thosein the U.S. on peritoneal dialysis (PD)now use a cycler and dialyze at night inthe same way early home hemodialysispatients did.
By the mid 1980s, many nephrol-ogists in the U.S. further reducedpatient time on hemodialysis usinghigh-flux dialysis treatments. Thispractice was based on a study by theNational Institutes of Health (NIH). Itwas not until after the InternationalAdequacy Meeting was held in Dallasin 1989 and its proceedings werereported in the May 1990 AmericanJournal of Kidney Diseases thatnephrologists began to realize howhigh the U.S. ESRD mortality rate was (24 percent) in comparison to the much lower rates in Europe (12-15 percent) and in Japan (nine percent).
A Short History of Dialysisin the United States
By Alan Hull, MD
CHOICES I: BASICS OF KIDNEY DISEASE
continued on page 3
“ In 1972, with passage
by Congress of HR1,
Medicare was expanded
to those with chronic
kidney failure of
any age.”
UNDERSTANDING YOUR CHOICES
2
Family Focus Volume 11, Number 3
In this issue of Family Focus yourEditorial Board wanted to informyou as to what dialysis and kid-
ney transplantation are like today, aswell as touch on what they used to bein the not so distant “good ole’ days.” I began my career in the field ofnephrology in 1979, which was nottoo long after Medicare was expandedto cover most of those in need of dialy-sis and kidney transplantation. Thiseliminated the need for the “selection”committees for dialysis treatmentsthat Dale Ester referred to in the lastissue of Family Focus. I am trulyamazed and encouraged by all of thechanges that have taken place in thepast 23 years. At that time, there wasonly one type of chronic dialysismodality—hemodialysis. Blood trans-fusions were commonplace becausethere was no such medication as ery-thropoeitin (EPO), and transplant
rejection rates and post-transplanthospital stays were considerably higherand longer due to less sophisticatedmedications. Imagine what enhance-ments we can expect in the next 23years.
In the next and final issue of FamilyFocus for this year, we will focus onthe future, specifically what we canexpect treatment to look like down theroad. There are many exciting possibil-ities on the horizon, and we will besharing those with you.
Many of you, our readers, also sharewith us. We have received many arti-cles, cartoons and poems. Readingthem is often inspirational and enlight-ening, and always educational. Weattempt to use as many of them as possible but please know that ourspace is limited and it may take as longas one year to actually see your workpublished. Additionally, we will soon behaving a Family Focus Editorial Boardmeeting where we will plan the themesof the four 2003 Family Focus issues.Help us select topics by sharing withus the areas that you and your lovedones think are important for those withchronic kidney disease. We appreciatehearing from you, so please keep yourletters and stories coming.
Karren King, MSW, ACSW, LCSWFor the Editorial Board
Karren King
NKF Family Focus is published quarterly by the National Kidney Foundation
Editorial Office:National Kidney Foundation30 E. 33rd Street, New York, NY 10016(800) 622-9010 • (212) 889-2210http://www.kidney.org
Editor-in-Chief:Karren King, MSW,ACSW, LCSWKansas City, MO
Fitness Editor:Tiffany Shubert, MS, PTSan Francisco, CA
Medical Editor:Wendy W. Brown, MD St. Louis, MO
Nursing Editor:Bobbie Knotek, RN, BSN Plano, TX
Nutrition Editor:Lori Fedje, RD, LD Portland, OR
Patient Editor:Dale EsterGlendale, AZ
Pediatric Editor: Barbara Fivush, MDBaltimore, MD
Social Work Editor:Mary Beth Callahan,ACSW/LMSW-ACPDallas, TX
Transplant Editor:Linda Harte, RN,BSN, MA, CNN, CCTKansas City, MO
Opinions expressed in this newspaper do not necessarily represent the position of the National Kidney Foundation
Editorial Director: Gigi Politoski
Editorial Manager:Sheila Weiner, MSW, CSW
Executive Editor: Sara Kosowsky
Managing Editor: Danielle Slade
Production Manager: Sunil Vyas
Design Director: Oumaya Abi Saab
FROM THE EDITOR
Another way to con-
tribute to the National
Kidney Foundation
is to visit
our Web site at
www.kidney.org or call
(800) 622-9010to make your
donation as a
Family Focus reader.
FF
and the National Kidney Foundation
want to help you show all thespecial people in your life exact-ly how much they mean to youand help support the National
Kidney Foundation in theprocess!
Order today on-line at
www.1800flowers.comor call
1-800-356-9377 and 1-800-FLOWERS.COM® will give10 percent* of the net proceeds fromyour purchase to the National Kidney
Foundation, just use the code KIDNEY when ordering.
©2002 1-800-FLOWERS.COM, INC.
*Items may vary and are subject todelivery rules and times. Offer validonline and by phone. Offers can notbe combined, and are not availableon all products, and are subject torestrictions and limitations. Offervalid through 6/01/03. Void where
prohibited.
1-800-FLOWERS.COM® uses Secure Socket Layer(SSL) encryption technology to secure its Web site.
Family Focus Volume 11, Number 3
3
A Short History of Dialysis in the United Statescontinued from page 1
The 1990s were spent increasingthe measured adequacy of hemodialy-sis (Kt/V) from .8 to 1.0 to 1.2, with a resulting slight decrease in patientmortality from above 24 percent toalmost 22 percent. This decreasingtrend in lowering mortality has nowstopped and mortality has actuallyincreased slightly according to prelim-inary results over the last two years.There are many reasons suggested for this trend but it can probably beattributed to the U.S. dialyzing thosewho are older and sicker, and theinability to routinely increase theamount of dialysis delivered in-centerhemodialysis or by peritoneal dialysis(PD) due to such things as paymentrate and nursing shortage.
In the new millennium (2000-2002), studies to see how much dialysis is necessary have been com-pleted and the results are somewhatsurprising.
1.The Ademex study, reported in theJournal of the American Society ofNephrology in June 2002, utilizingPD in Mexico, showed that increas-ing the amount of dialysis deliv-ered (Kt/V) did NOT improve mortality.
2.The HEMO study, supported bythe NIH and not yet published butreported at the National KidneyFoundation Clinical NephrologyMeetings in Chicago in April 2002,again showed that increasing thedose (Kt/V) in hemodialysis didNOT improve survival.
SOLUTIONIn my opinion, it would appear that
we must either increase the dialysisfrequency (once daily, six days a week)or the dialysis duration (longovernight, three to four times a week)in order to increase the amount ofdialysis delivered and apparentlyrequired to decrease mortality inAmerican chronic kidney failurepatients. I believe that in the future we will move to daily hemodialysis athome, long overnight hemodialysis athome or daily in-center for some peo-ple. As these increases in dialysisbecome available (payment by Medicareand insurance is the greatest obstacleat present), I believe we will see a signif-icant improvement in mortality forthose patients utilizing these approach-es. At this time, there are about 500patients doing more frequent and/orlonger dialysis. I believe the responseseen to date in these patients has beenimpressive and suggests that this is thedirection in which we should move.
The next issue of Family Focus willfurther explore what treatments maybe ahead for those with chronic kidneyfailure. This issue should make each ofus realize and appreciate just how farwe have come.
About the Author:Alan Hull, MD is a transplant
nephrologist, who began dialyzingpatients in 1964. He was president ofDallas Nephrology from the mid to late1980's, the president of the RenalPhysicians of Transplantation since itsfounding, the president of the AmericanSociety of Transplant Physicians (nowthe American Transplant Society), andwas president of the National KidneyFoundation. He is a clinical professor ofmedicine at the University of Texas,Southwestern Medical Center at Dallas.
Both of these studies were prospec-tive (participants followed to see whatwill happen) and randomized (partici-pants chosen fairly for each form oftreatment) to remove research bias.
However, in a large observationalstudy of 50,000 patients, published inthe April 2002 issue of the AmericanSociety of Nephrology, Fritz Port, MDfound that more dialysis appeared toimprove survival. How then shouldnephrologists, and the kidney teamsthey lead, interpret these results, andmore importantly, what questionsshould those on dialysis be asking?
From my viewpoint of 35 years ofdialysis experience, I would make thefollowing summary statements:
1.Normal kidney function is approxi-mately 120 cc/minute. That meansthat every hour 8,200 cc of bloodis cleared of urea by a normal pairof kidneys. This occurs 24 hours aday, seven days a week.
2. In the better dialysis units withgood dialysis we may get an aver-age clearance up to 15 cc/minuteor slightly more than 10 percent of normal kidney function.
3.To increase beyond this figure, youmust either dialyze more or havesome remaining kidney function.However, as time passes, kidneyfunction will decrease towards zero on any form of dialysis.
FF
There are lots of reasons to donate a vehicle. Funding kidney research and patient care are only a few. Make your car a Kidney Car. Cars that save lives. For more information, call 1-800-488-CARS.

Family Focus Volume 11, Number 3
4
Following a diet that has beenplanned to meet your needscan help keep you healthy
and feeling well whether you are onhemodialysis, peritoneal dialysis orhave recently had a kidney transplant.If you are on dialysis, following yourmeal plan will prevent fluid and wasteproducts from building up in yourbody. If you have received a kidneytransplant, adhering to your diet willhelp prevent high blood sugars andfats, high blood pressure and somemedication side effects. The followingarticle will discuss each of these mealplans and help you discover whichdiet is right for you.
When your kidneys are workingwell, they are working continually. Formany of you, dialysis has now takenover the job of your kidneys. Betweendialysis treatments however, no filter-ing is occurring and your body cannotget rid of extra fluid and waste prod-ucts. This build-up can make you feelnauseated, tired, weak and bloated.Salt and potassium in your diet con-tribute to this build-up. Followingyour meal plan will help you stay feel-ing well until your next dialysis treat-ment. If you are on peritoneal dialysis,your allowances are usually greater.This is because your treatments aremore frequent, so less fluid and wasteproducts remain in your body.
Phosphorus is another dietary com-ponent that must be limited. Whenyour blood phosphorus level is toohigh, your bones may become weakand your arteries can narrow. You mayneed to take phosphorus “binders”when you eat to help control yourphosphorus level. These prevent muchof the phosphorus in your food frombeing absorbed into your blood.
Both meal plans for dialysis advise ahigh protein intake. More protein isrequired because each time you dia-lyze, you lose some protein duringyour treatment. In peritoneal dialysis(PD), these losses are greater, in partbecause your treatments are more fre-quent. This means that your proteinneeds will be slightly higher on PDthan on hemodialysis. Remember toinclude a good source of protein(meat, fish, fowl, eggs) at each meal to help meet these needs.
For those of you who have under-gone a kidney transplant, good nutrition is as important as ever.Immediately after your transplant,your body needs protein and energy(calories) to heal and rebuild. The diet you once followed will likely bechanged. Once your kidney is workingwell, most of the advised diet changesare to help prevent complicationsrelated to your immunosuppressantmedication (necessary medications tohelp keep your body from rejectingyour new kidney). Some of the sideeffects you may experience are: highblood sugars, high blood pressure, anincrease in blood fats (cholesterol andtriglycerides), weight gain and fluidretention. However, these commonside effects can be minimized by mak-ing healthy food choices limited inextra calories, salt and fat and byexercising regularly.
Most of you will require a specialvitamin supplement to make up forlosses during dialysis or to meet yourincreased requirements after trans-plant. Check with your doctor ordietitian to make sure you are nottaking a supplement or herbal reme-dies that may be harmful.
Regardless of the type of meal planyou follow, try to make healthy selec-tions and include a variety of foods.Having chronic kidney diseaseincreases your risk of developingheart disease. Aim to achieve andmaintain a desirable body weight and acceptable blood fat levels byincluding exercise in your daily routine and reducing fat intake, especially saturated fat.
Remember, nothing can replace theattention your renal dietitian can giveyou! Whenever you have questionsabout your meal plan or nutritionalhealth, contact your renal dietitian orhave your doctor refer you to one. Thedietary and lifestyle choices you makewill play a big role in keeping youhealthy.
About the Author:Holly Minor works with hemodialy-
sis patients at the Hollywood DialysisCenter in Portland, OR. She bringswith her 12 years of experience fromCanada working as a dietitian in avariety of settings including two and ahalf years working with a liver trans-plant program in Riyadh, SaudiArabia.
FF
Good NutritionWhich Diet is Right for You?
By Holly Minor, RD, LD

5
The last few fitness articleshave talked about why exer-cise is good for you, as well as
the best way to start exercising. Wethought you might like to get someideas about exercising from folks onhemodialysis and peritoneal dialysiswho exercise for LIFE!
AnnAnn is a 72 year-young lifelong exer-
ciser. “ I have always been a walker,”says Ann, and she decided to keep onwalking when she was told her kidneyswere failing. “It was tough, but I feltbetter after walking.” Ann walksbecause, “it gives me a lot of strength, I look forward to it—it is the way I startmy day.” She walks six blocks daily onher way to her volunteer work takingcare of young children of single moth-ers while they receive job training. Shemakes time to walk a mile three timesa week, and she recently started aweight lifting program. She participat-ed in a study that provided coachedweight training during dialysis, andwhen she was finished with the study,she decided to continue lifting weightsfor her arms and legs. Her advice todialysis patients is: “Just do it! Keepmoving, and you will feel better.”
RickRick is 42 years old. He is HIV posi-
tive, and has been dialyzing for twoand a half years. Rick lets his feet takehim around town to run errands, visitwith friends and “have fun.” He walksapproximately four miles a day. Bywalking for exercise and for pleasure,Rick feels he gets a chance to clear hismind and increase his endurance andflexibility. Rick had exercised all of hislife, and decided not to stop when hestarted dialysis. During his first threeweeks of hemodialysis treatment, hefelt “really tired” and “slept a lot.”However, he did not change his activitylevel. “It was important to keep ongoing, it helped me feel better.” Rickrecommends, “You definitely want tostart slow and easy. Try walking up aflight of stairs, one at a time. Keepgoing up the flight of stairs, once a dayfor a few weeks, and it will start to geteasier. Once it becomes easy, thenmake it harder and go up two flights ofstairs. Think of this as something fun,something that is good for you andsomething that you want to do.”
F I T N E S S
Exercisers for Life! By Tiffany Shubert, MS, PT
SteveSteve is a bit of a celebrity. He is an
accomplished tennis player and playsin the U.S. Tennis Association. He hasshared the court with Venus Williamsand other professional players. WhenSteve first started PD, he was quite ill,and he stopped playing tennis andexercising. When his health stabilized,he slowly began exercising again. Heshared, “It felt so great to start!” Stevediscovered that exercise was helping tokeep his muscles strong, and he wasfeeling better after working out. Heplays tennis six days a week and fiveto six times a week he works out at thegym using weights to strengthen hisarms and legs. He now plays tourna-ments usually one to two weekendseach month. A great benefit of being soactive is that he sweats which helps tocontrol his fluid, and he can drink abit more. Steve has not experiencedany problems with his PD treatmentsas a result of exercise. However, if he isnot feeling well, he limits his activitiesuntil he is feeling better.
Jophry“Exercising is the way that I deal
with stress,” states Jophry, who beganworking out in his mid-twenties, longbefore he started his PD treatments.The day after his catheter was placedsurgically, he decided that he had bet-ter keep exercising to help manage hisweight and to keep feeling good. “I doabout 30 minutes on the treadmill orstationary bike, then I drain out myPD solution to avoid any stress on myabdomen while doing sit ups, pushups, and weight lifting,” explainsJophry. He alternates his upper bodyand lower body weight lifting days.After Jophry started PD, he usedlighter weights, and slowed down his
workouts. “I concentrated on form,and doing things perfectly, so I would-n’t injure myself.” Jophry recommendstalking to your doctor about yourblood pressure medication schedule.“If you take your blood pressure med-ications way in advance of exercising,they will have less of an effect on yourexercise session. Also, it is a good ideato eat something light before exercis-ing so you don’t get too physicallydrained.”
How is your own exercise programgoing? Here is a checklist to makesure you are on track. Be certain tocheck first with your doctor to makesure it is safe for you to start an exer-cise program.
Steve’s recommendations:✦ Find an activity that you enjoy,
something that you look forward todoing.
✦ Start slowly, do about half of whatyou think you can do.
✦ Do not get discouraged, even if youhave a bad day, just keep on mov-ing.
✦ Choose a goal that you know youcan reach, and slowly build up tothat goal.
✦ Remember, reaching your goal maytake awhile, but it will get easier.
✔ Are you warming up (deep breath-ing, stretching your arms and legs)for 10-15 minutes?
✔ Are you able to do 10-15 minutesof exercise to get your heart rateup?
✔ If 10 minutes is too long, can youdo five minutes twice daily?
✔ Are you cooling down and doinggentle stretching?
✔ If 10 minutes feels ok, try increas-ing your exercise by two minutesevery week, until you get up to 20minutes. Maintain 20 minutesuntil the next newsletter.
✔ What type of exercise are youdoing? Write to Family Focus andfill us in. Also tell us if there isequipment at your unit, or if thereis access to physical therapists orexercise physiologists to help youachieve your goals.
Family Focus Volume 11, Number 3
6
Family Focus Volume 11, Number 3
U.S. Congress and TransplantationBy Dolph Chianchiano, JD, MPA
Payment for Anti-RejectionMedications
Often people on dialysis and thosewith chronic kidney disease are reluc-tant to consider transplantation as atreatment alternative because they areconcerned about paying for the medica-tions they will need to take to keep theirtransplant functioning. Because ofadvocacy by the NKF and other kidneyorganizations, Congress has graduallyextended the duration of the Medicarebenefit for immunosuppressive drugsso that some transplant recipients nowhave indefinite coverage for these med-ications. However, many people stillneed expanded coverage.
The following bills have been intro-duced in the 107th Congress to addressthe needs of those patients:
Immunosuppressive Drug CoverageAct of 2001 – HR 1839, introduced byRepresentatives Camp (R. MI) andThurman (D. FL), and S 880, intro-duced by Senators DeWine (R. OH) andLincoln (D. AR). This legislation wouldprovide indefinite coverage for anti-rejection medications for any kidneytransplant recipient who was eligible for Medicare benefits at the time of thetransplant and who doesn’t have suchcoverage through an employer’s healthinsurance program. You would have topay Medicare Part B premiums andwould be responsible for 20 percent of the cost of the drugs if this proposalbecomes law.
Comprehensive ImmunosuppressiveDrug Coverage for Transplant PatientsAct of 2001 – S 1204, introduced bySenator Durbin (D. IL). This legislationwould provide indefinite coverage forrecipients of heart, liver and lung trans-plants as well as kidney patients.
Financial Concerns of Living DonorsThe increase in the number of live
organ donors in the U.S. over the pastdecade has been the most encouragingdevelopment in the effort to close thegap between the number of transplantcandidates and the number of organsthat are donated annually for trans-plantation. Whereas there were 2,124live organ donors in 1990, the numberof live organ donors grew to 4,712 in1999 and this growth trend is expected
to continue because of the shortage ofcadaver organs. On the other hand,research supported by the NKF’sCouncil of Nephrology Social Workersindicates that a quarter of potential live organ donors are unable to pro-ceed with donation because of financial concerns.
Furthermore, the NKF has taken theposition that living donors should notpersonally bear any costs associatedwith donation. Provisions to create aprogram of grants to cover travel, hous-ing and other living donor relatedexpenses have been included in threemajor transplant bills that are makingtheir way through Congress. These are:the Organ Donation Improvement Act of 2001 – HR 624, introduced by Rep.Bilirakis (R. FL), the Donor Outreach,Network and Timely Exchange Act – S 1062, introduced by Senator Durbin(D. IL) and the Organ Donation andRecovery Improvement Act – S. 1949,introduced by Senators Frist (R. TN)and Dodd (D. CT). Representative Karen Thurman (D. FL), whose hus-band received a kidney transplant,introduced legislation on March 19,2002, designed to assure leave fromwork for living donors. This bill, HR4008, would amend the Family andMedical Leave Act of 1993. That statuteprotects workers from losing their jobsbecause of the need to take medicalleave and requires employers to provideunpaid time off from work when justi-fied for medical reasons.
Improving the Organ DonationRequest Process in Hospitals
HR 4086, introduced by Represent-ative Joe Wilson (R. SC), would providefor grants to organ procurement agen-cies so that they can carry out pro-grams to improve the organ donationrequest process in hospitals. The bill isnamed in memory of Rep. Floyd D.Spence who formerly representedCongressman Wilson’s district.Representative Spence was a lungtransplant recipient who later receiveda kidney transplant.
Financial Incentives for Non-LivingOrgan Donation
In February of 1991, the NationalKidney Foundation held a consensus
conference to seek input from trans-plant professionals, attorneys anddonor families to explore whether finan-cial incentives could offer a solution tothe organ donor shortage. The consen-sus conference was followed by fourregional public forums and a telephonepublic opinion survey that was con-ducted by the Southeastern Institute ofResearch. The kinds of financial incen-tives that were discussed included pay-ments for funeral or burial expenses,tax credits and charitable contribu-tions. Based on the findings from thisinitiative, the NKF recommended thatCongress permit one or more demon-stration projects which would revealwhether the American public wouldaccept the introduction of financialincentives for non-living organ donationand if such financial incentives wouldactually increase the supply of organsavailable for transplantation in thiscountry.
Congressional action is neededbecause of the concern that theNational Organ Transplant Act of 1984(NOTA) would thwart the planning andexecution of such demonstration pro-jects. That statute prohibits the pur-chase of organs for transplantation andimposes civil and criminal penalties onindividuals and organizations that vio-late this prohibition. The Frist/Doddbill mentioned above (S 1949), however,provides that, “notwithstanding” thissection in NOTA, the Secretary of theDepartment of Health and HumanServices may conduct up to threedemonstration projects similar to those NKF has advocated in the past.
If the proposals described in this arti-cle are not enacted this year, they willbe replaced by new bills during the108th Congress, convening in January2003. To learn more about the status ofthese bills and any new legislation thatmay be introduced to accomplish simi-lar goals, please call the NKF Office of Scientific and Public Policy at (800) 889-9559, or visit the NKFGovernment Relations Web site athttp://www.kidney.org/general/pubpol
S ince transplantation is the preferred treatment option for many people with kidneyfailure, the National Kidney Foundation (NKF) Office of Scientific and Public Policy is fighting to overturn the barriers which limit access to this modality. These include the
shortage of organs available for transplantation as well as economic and financial con-straints. Members of the U.S. Congress are crafting approaches to these problems, with inputfrom the NKF, and have introduced the bills described below. These bills offer hope andpromise, but advocacy by transplant candidates and recipients and their friends and lovedones will be necessary to turn these proposals into reality.
FF
Family Focus Volume 11, Number 3
7
You have kidney failure, and itneeds treatment.” Whenever Ispeak these words to some-
one, I ask the person to rememberthat many people are available to helpthem get through these tough times.There are no right or wrong choices;there are only roads to take. If theytake a road that does not take themwhere they want to go, there are otherroads to be traveled.
Kidney failure means that the level ofkidney function has fallen to less than15 percent of normal. The decision tostart dialysis is made by you and yourkidney doctor. It is not based just onnumbers, but whether the benefits ofdialysis outweigh the risks. Some peo-ple may feel that dialysis is not rightfor them. For whatever reason, theychoose non-dialysis treatment. Thismay include anemia-treating drugs,water pills, blood pressure medicineand diet changes. Many people livequite comfortably for a time withoutdialysis, but others may be quite ill.Hospice care may be considered forthose who choose not to dialyze. Yourdoctors should be able to prevent suf-fering and help you live with the bestquality of life possible if you select thisoption. It is important that peoplewith chronic kidney disease feel incontrol and able to make their owndecisions. You could change yourmind and start or stop dialysis at any time.
You may decide to do hemodialysis.It cleans your blood by pumping itthrough a machine with an artificialkidney that allows the blood to travelon one side of a filter and a cleaningsolution on the other side. Wasteproducts pass from the blood into thewashing solution through the filter.
This process takes time, each sessionis three to five hours, with most peo-ple having at least three sessions aweek. Blood is taken from an access,which can be a fistula, graft orcatheter. A fistula is a connectionbetween an artery and a vein that ismade by a surgeon. For a graft, thesurgeon places man-made tubingbetween an artery and a vein. Acatheter is a tube placed into a largevein in your neck or chest. Any ofthese accesses allow blood to bepumped at rates of about one-halfquart per minute through themachine and returned to you at thesame rate.
The most difficult problem withhemodialysis is access complications.Problems with catheters and fistulasmay include blood clots and the riskof infection. Hemodialysis is done in acenter or at home. If you dialyze athome, you must have a partner. Ittakes six to 12 weeks to teach youand your partner how to do homehemodialysis.
Peritoneal dialysis (PD) is donethrough a catheter placed surgicallyin your abdomen. The blood iscleansed by using the membrane thatlines your abdomen. PD is done man-ually or by a machine at night, or by acombination of the two. Several timesa day, solution is drained into yourabdomen, where it is allowed to cleanthe blood and afterwards is drainedout. Then the process begins anewwhen clean solution is once againdrained into the abdomen. Each ofthese exchanges takes about 30 min-utes, and must be done every day. Itusually takes less than one week tolearn how to do this dialysis. (It isimportant to note that there is no“typical” PD exchange becauseaccording to Kidney DialysisOutcomes Quality Initiative (K/DOQI)standards, every dialysis treatmentprogram is customized to eachpatient.) You return to the kidney cen-ter only to review your treatment withthe dialysis team and make any nec-essary changes. Blood work is doneregularly to check for adequate bloodcleansing.
The main advantage of peritonealdialysis is it can be done at home. Thedisadvantages are risk of infection(called peritonitis) and difficulty get-ting enough fluid into the abdomen to
provide ade-quate clean-ing.Peritonealdialysis isoften used inearly stagesof kidney failure and may not be goodenough later, depending on the level ofremaining kidney function. Some also“burn out” from the daily treatments.Peritoneal dialysis, however, gives thegreatest degree of independence andself-control.
The best replacement for lost kidneyfunction is a new kidney, but transplan-tation is not for everyone and there arenot enough kidneys for those who needone. Thousands of people are on thewaiting list to receive a kidney trans-plant. Kidneys can be donated from peo-ple who have died (non-living donors) ormay be donated by family or other lovedones (living donors). People who donatewithout having any attachment to therecipient (living non-related donors), arerarer. The kidney is attached to a bloodvessel in your groin (not in the backwhere they are naturally). After thetransplant, you have to take medicationfor the rest of your life to keep the kid-ney functioning. The risks of transplantinclude the risk of anesthesia andsurgery, infection, rejection and compli-cations related to medicines that mustbe taken to keep the kidney working.The benefits are obvious.
Others have traveled the many roadsthat must be traveled to successfullytreat kidney disease. Perhaps the mostimportant support you will get on yourway is from other people who have suc-cessfully traveled those roads. Thissupport can be found in your localNational Kidney Foundation (NKF) affil-iate or in your local dialysis unit. Somekidney centers or NKF affiliates offereducation prior to beginning dialysisthat can be very helpful. Remember,professional staff are available to helpguide you on your journey; you are notin this alone.
About the Author:Leslie Spry is a nephrologist in private
practice with the Dialysis Center ofLincoln and Lincoln Nephrology &Hypertension in Lincoln, Nebraska. Hehas been active with the NationalKidney Foundation since 1981, and hasgreat interest in public education bothlocally and nationally.
Choices: Which Road to Travel?By Leslie Spry, MD, FACP
“
FF
Family Focus Volume 11, Number 3
8
Our MuseumBy Lee Deuell
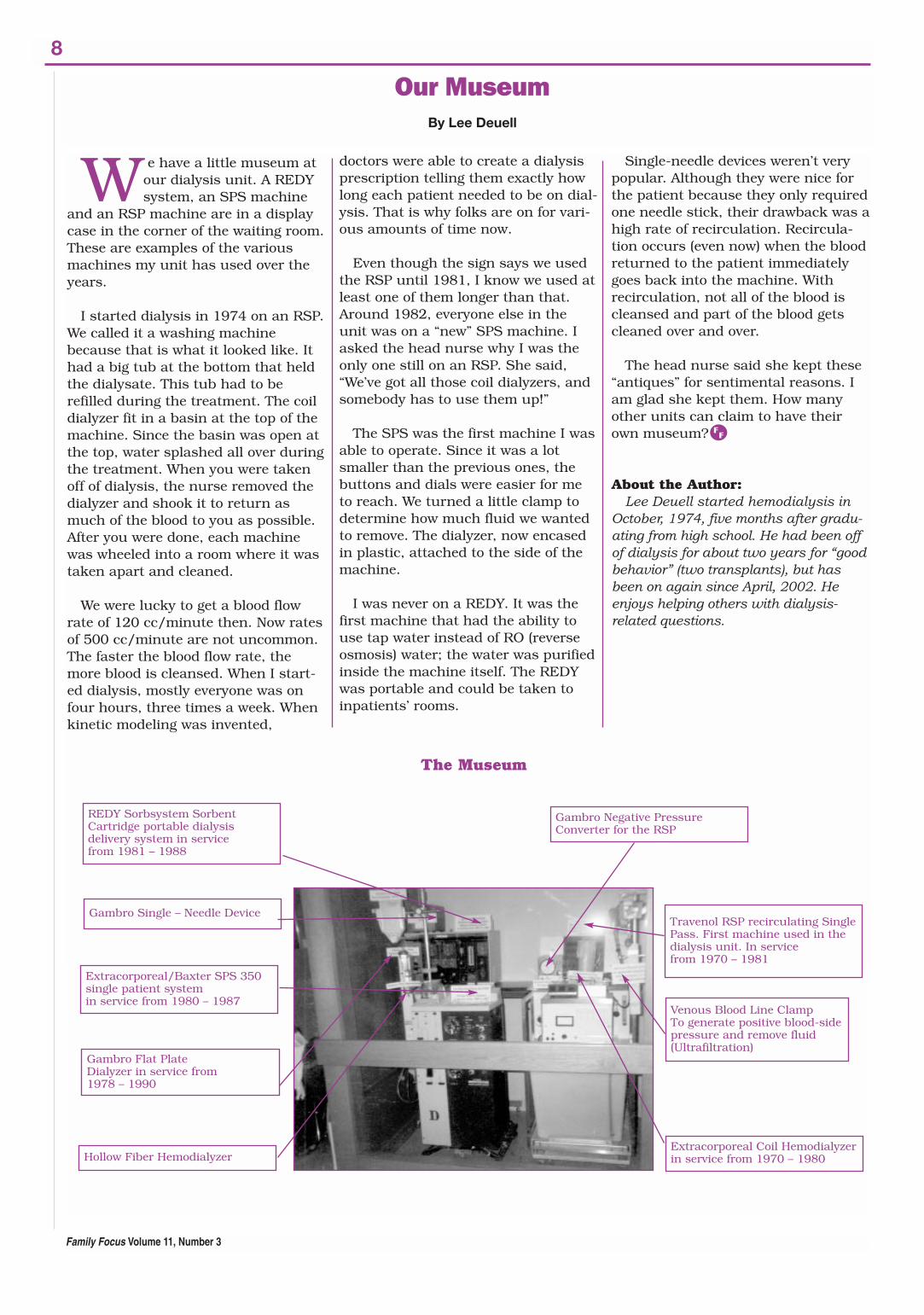
We have a little museum atour dialysis unit. A REDYsystem, an SPS machine
and an RSP machine are in a displaycase in the corner of the waiting room.These are examples of the variousmachines my unit has used over theyears.
I started dialysis in 1974 on an RSP.We called it a washing machinebecause that is what it looked like. Ithad a big tub at the bottom that heldthe dialysate. This tub had to berefilled during the treatment. The coildialyzer fit in a basin at the top of themachine. Since the basin was open atthe top, water splashed all over duringthe treatment. When you were takenoff of dialysis, the nurse removed thedialyzer and shook it to return asmuch of the blood to you as possible.After you were done, each machinewas wheeled into a room where it wastaken apart and cleaned.
We were lucky to get a blood flowrate of 120 cc/minute then. Now ratesof 500 cc/minute are not uncommon.The faster the blood flow rate, themore blood is cleansed. When I start-ed dialysis, mostly everyone was onfour hours, three times a week. Whenkinetic modeling was invented,
doctors were able to create a dialysisprescription telling them exactly howlong each patient needed to be on dial-ysis. That is why folks are on for vari-ous amounts of time now.
Even though the sign says we usedthe RSP until 1981, I know we used atleast one of them longer than that.Around 1982, everyone else in theunit was on a “new” SPS machine. Iasked the head nurse why I was theonly one still on an RSP. She said,“We’ve got all those coil dialyzers, andsomebody has to use them up!”
The SPS was the first machine I wasable to operate. Since it was a lotsmaller than the previous ones, thebuttons and dials were easier for meto reach. We turned a little clamp todetermine how much fluid we wantedto remove. The dialyzer, now encasedin plastic, attached to the side of themachine.
I was never on a REDY. It was thefirst machine that had the ability touse tap water instead of RO (reverseosmosis) water; the water was purifiedinside the machine itself. The REDYwas portable and could be taken toinpatients’ rooms.
Single-needle devices weren’t verypopular. Although they were nice forthe patient because they only requiredone needle stick, their drawback was ahigh rate of recirculation. Recircula-tion occurs (even now) when the bloodreturned to the patient immediatelygoes back into the machine. Withrecirculation, not all of the blood iscleansed and part of the blood getscleaned over and over.
The head nurse said she kept these“antiques” for sentimental reasons. Iam glad she kept them. How manyother units can claim to have theirown museum?
About the Author:Lee Deuell started hemodialysis in
October, 1974, five months after gradu-ating from high school. He had been offof dialysis for about two years for “goodbehavior” (two transplants), but hasbeen on again since April, 2002. Heenjoys helping others with dialysis-related questions.
REDY Sorbsystem SorbentCartridge portable dialysis delivery system in service from 1981 – 1988
Extracorporeal/Baxter SPS 350single patient systemin service from 1980 – 1987
Gambro Negative PressureConverter for the RSP
Travenol RSP recirculating SinglePass. First machine used in thedialysis unit. In servicefrom 1970 – 1981
Extracorporeal Coil Hemodialyzerin service from 1970 – 1980
Venous Blood Line ClampTo generate positive blood-sidepressure and remove fluid(Ultrafiltration)
Gambro Single – Needle Device
Gambro Flat PlateDialyzer in service from 1978 – 1990
Hollow Fiber Hemodialyzer
The Museum
FF
9
Family Focus Volume 11, Number 3
C H O I C E S
S elf-determination is your rightto decide what happens toyou. In medical terms, it is
your right to choose the level of med-ical care that you receive and tochange your wishes about medicalcare as your situation changes overtime. Learning that you have chronickidney disease can create anxiety,stress, feelings of loss and the need to make many decisions. There arefour main treatment choices for kid-ney failure. They are, hemodialysis,peritoneal dialysis, transplantationand no treatment.
Many times when a person is firsttold about having kidney failure andneeding dialysis, there is little time tothink, learn and mull over decisions.Starting dialysis is a big decision; it isgoing into the unknown. Do not forgetthat there are many caring andinformed health care professionalswho can help you choose the treat-ment that is best for you.
Can dialysis be tried and later stopped?While you may decide not to begin
dialysis, you should also know thattrying dialysis does not mean that youare forced to stay on it forever. If youare uncertain whether to begin dialy-sis, a trial of dialysis treatment mighthelp you make the decision. Also, afterdialyzing for any length of time, someindividuals may decide that the bur-dens of dialysis simply outweigh thebenefits for them. If you are consider-ing stopping dialysis, you should dis-cuss this important decision with yourdoctor, social worker and loved ones.You may wish to have members ofyour health care team present whenyou speak to your family about stop-ping dialysis so that your family canask questions and gain an under-standing of what would happen if youchose to end treatment. The membersof your health care team and yourloved ones will want to understandwhy you are considering this decision.They will probably want to know if it isbecause your health is getting worse,if you are having specific treatmentproblems or if you are depressed.
If you are experiencing depression,you may not be able to think as clearlyas you might have before. Depressioncan often be treated successfully withmedication, counseling or a combina-tion of both. If depression is a part ofyour situation, you can rethink yourdecision to stop dialysis after yourdepression is treated. Although youmay arrive at the same decision, you,your family and your health care teamwill know that you are making thedecision with a clear mind. No matterwhat your thoughts are, it is impor-tant to discuss your feelings openly sothat these people can help you andkeep you from feeling all alone.
Is stopping dialysis suicide?Dialysis is considered a life-sustain-
ing treatment because, without it, aperson with kidney failure would die.Many Western religions support thebelief that individuals have the rightto stop treatment if they feel it is nothelping. You may wish to speak withyour religious adviser if you havequestions about this. Ultimately, how-ever, this is a decision that individu-als must answer for themselves.
What if I am too sick to tellsomeone else about my wishes? Advance directives are a way of
telling someone what you would likedone about your medical care if youcannot speak for yourself. There aregenerally two types of advance direc-tives: a durable power of attorney forhealth care, which allows you toappoint someone to make health caredecisions for you if you are unable tocommunicate them, and a living will,which allows you to specify whatmedical treatments you want or donot want. Completing advance direc-tives and discussing them with yourfamily will give them peace of mind inknowing that they are helping you toget the type of health care you wouldwant. You can change or cancel anadvance directive at any time. Yoursocial worker can give you informa-tion about advance directives.
Can anyone help me and my family if I decide not tostart dialysis or, later, decide to stop dialysis?Your dialysis health care team
should continue to be available to pro-vide information and support. Also,hospice services may be available foryou. Hospice services will allow manypeople (social workers, nurses, homehealth aides, chaplains, doctors) tohelp you and your family by providingmedical, counseling, emotional andspiritual support.
How can I help as a family member?It is difficult to see someone you love
struggle with issues of life and death.They need your support now morethan ever. You can listen, hold theirhand, help them think through deci-sions about business matters andmemorial or funeral services and letthem know you love them and supporttheir decisions, remembering that thefinal decision must be that of the per-son with kidney disease. Your supportand understanding will help yourloved one achieve self-determinationand peace. This will be a stressful timefor you, too. Let your support systemknow how they can help you throughthis difficult time.
Readers may want to refer to the fol-lowing National Kidney Foundation(NKF) educational booklets:• When Stopping Dialysis Treatment
is Your Choice• If You Choose Not to Start Dialysis
Treatment • Advance Directives: A Guide for
Patients and their Families.Contact the NKF at (800) 622–9010
or e-mail [email protected] to requesta copy.
FF
Making the Choices That are Right for YouBy Mary Beth Callahan, ACSW, LMSW-ACP
☞ Family Focus is available on the Web. To findthis issue or back issues of the newspaper, go to
www.kidney.org/patients/backissues.cfm
Family Focus Volume 11, Number 3
10
From Head to ToeBy Bobbie Knotek, RN, BSN, CNN
Eyes need tobe checkedby an eyedoctor everyyear. Youmay needmore fre-quent eyeexams if youhave dia-betes or highblood pres-sure. Your
eye doctor will:• test for vision changes• look at blood vessels inside
your eyes • check for glaucoma, an eye disease
in which pressure builds up insidethe eye, causing blindness if nottreated.
Teeth & Gums need extra care whenyou have kidney failure. This is espe-cially true if you have diabetes. Also, ifyou are interested in being evaluatedfor a kidney transplant (now or in thefuture), healthy teeth and gums are amust! Surgeons will not perform kid-ney transplant operations on a personwith infected gums or an infectedtooth.
To keep YOUR teeth and gumshealthy:• See a dentist at least once a year
(two to three times a year is best)for exams and cleaning.
• Tell your dentist:1) You have kidney failure and howyou are treated—hemodialysis,peritoneal dialysis or a kidneytransplant.2) About other medical problems(heart disease, high blood pressure,hepatitis B or C, etc.)3) ALL medicines you take.If you do hemodialysis:- Make dentist appointments for
the day after dialysis1.
- Heparin, the blood thinner usedto keep your blood from clottingduring dialysis, makes youbleed easier for several hoursafter dialysis. Schedulingappointments for the day afterdialysis helps to prevent excessbleeding during teeth cleaningor dental work by:
a) letting the heparin wear off and
b) giving any bleeding from dental work time to clot before your next dose of heparin.
• Do not have dental work donewhen you have an active vascularaccess problem (like clotting orinfection)
1. It is possible for germs
from a clotted or infected graft, fis-tula or catheter to spread to yourteeth and gums, or your blood-stream during dental procedures.
• If you are on peritonealdialysis—do not have dental workdone when you have an activeinfection at your exit site or haveperitonitis. Wait for 30 days afterthe infection has cleared up beforehaving dental work done
1. This will
help prevent the spread of germsfrom an exit site infection or peri-tonitis to your teeth and gums, oryour bloodstream.
• Brush/floss twice a day. Use a softtoothbrush. If flossing makes yourgums bleed, try a dental floss likeGlide™ (GORE) or SATINfloss™(Oral-B). Use a fluoride toothpasteand mouth rinse.
• Ask your dentist or dietitian aboutsaliva substitutes for dry mouth.Many dentists recommendBiotene™.
• Do not use mouthwashes or salivasubstitutes made with alcohol. Thealcohol in the mouthwash willmake your mouth even drier.
• Call your dentist if you get sores orwhite patches in your mouth.
• For dental work that could causebleeding(includingcleaning),ask yournephrolo-gist if youneed totake pro-phylacticantibioticsbefore theappoint-ment
2.
Vaccinations help your body fight off germs. People with kidney failureshould have these vaccinations:1) Flu shot every year in the fall or
winter. 2) Pneumonia shot—ask your
nephrologist how often you needthis shot.
3) Hepatitis B vaccinations (especiallyif you do hemodialysis).
Most dialysis and transplant clinicsoffer these vaccinations:
Screening tests look for signs of can-cer. Medicare knows the importance of screening tests and will help pay for these tests.Prostate cancer screening tests for men.
a) A digital rectal exam every year.b) A Prostate Specific Antigen or
PSA test every year (ask yournephrologist if you need thistest).
Breast and cervical cancer screeningtests for women: a) pap smear, pelvic exam and clinical
breast exam at least every twoyears.
b) screening mammogram every yearfor women 40 and older.
Screening tests everyone should have: a) Fecal Occult Blood Test (FOBE)
every year and Flexible Sigmoidos-copy every four years to check forcolorectal cancer.
b) skin cancer screening with a der-matologist once a year.
Many people on dialysis have circula-tion problems in their feet from dia-betes or poor blood supply. If you havecirculation problems in your feet, readthe “foot care habits” below to learn howto help prevent serious problems thatcan lead to the loss of toes or a foot.
NEVER:• Wear shoes with an open toe or
heel. • Hold socks/nylons up with rubber
bands or garters.
ALWAYS:• Wash feet every day with mild soap
and warm (not hot) water. • Dry your feet well.
Dry between each toe.
continued on last page
J ust like a car needs a “tune up” to run smoothly, your body needs a “tune up” to stay healthy. In addition to takingcare of dialysis or transplant needs, you cannot neglect the needs of the rest of your body. Your body may need a“tune up” as well! Follow these important steps to keep the rest of your body as healthy as possible.
Family Focus Volume 11, Number 3
11
In 1972, Medicare coverage wasincreased to provide financialsupport to people with End Stage
Renal Disease (ESRD), or kidney fail-ure, who require dialysis or a kidneytransplant to maintain life. TheCenters for Medicare and MedicaidServices (CMS) oversee the Medicareprogram for people with kidney fail-ure. CMS also oversees the 18 ESRDNetworks (http://www.esrdnetworks.org) in the United States, and one ofthe Networks’ jobs is to make surethat those with kidney failure who areMedicare eligible receive quality care.
Over the last decade there has beena great deal of effort by CMS toimprove the care of those withMedicare due to ESRD. In 1999, CMSdeveloped a program to measure andreport on the quality of kidney dialysisservices provided to those in theMedicare program. This program iscalled The ESRD Clinical PerformanceMeasures (CPM) Project. The ESRDCPM Project is now a national effortled by CMS and the 18 ESRDNetworks. The goal of the ESRD CPMproject is to improve patient care andoutcomes. To reach this goal, theESRD CPM project identified 15 clini-cal performance measures for adultson dialysis based on input from theNational Kidney Foundation, and inaccordance with the Kidney DiseaseOutcome Quality Initiative (K/DOQI).These 15 measures were developed inthe areas of hemodialysis and peri-toneal dialysis adequacy, vascularaccess and anemia management.These measures only apply to adultdialysis patients. Very briefly, the 15measures are described below:
➤ HEMODIALYSIS
1. Those who are maintained onchronic hemodialysis, the deliv-ered dose of hemodialysis shouldbe measured once a month.
2. The delivered dose of hemodialy-sis received should be deter-mined by calculating a Kt/Vnumber.
3. People on hemodialysis shouldhave a Kt/V number greater thanor equal to 1.2.
4. Blood urea values are needed tocalculate the Kt/V, and they needto be drawn in a standard way.
5. If a person is dialyzed using ahollow fiber dialyzer (a commonlyused dialyzer), and there is dia-lyzer reuse, the blood volume ofthe dialyzer has to be calculated.
➤ PERITONEAL DIALYSIS
6. If a person is maintained onchronic peritoneal dialysis, theclearance of urea and creatinineshould be measured.
7. The clearance of urea and creati-nine should be determined bycalculating a weekly Kt/V num-ber and a weekly creatinineclearance number.
8. For those on continuous ambula-tory peritoneal dialysis (CAPD),the weekly Kt/V number shouldbe greater than or equal to 2.0.For those on continuous cyclingperitoneal dialysis (CCPD) theweekly Kt/V number should begreater than or equal to 2.1.
➤ VASCULAR ACCESS
9. A primary arterial venous fistula(access) should be made in atleast half of the people beforethey start hemodialysis.
10. Less than 10 percent of allthose receiving chronichemodialysis should have anexternal catheter as theirhemodialysis access.
11. If a person has an AV graft asan access, it should be moni-tored for narrowing
➤ ANEMIA
12. The target range for hemoglobinfor those on dialysis should be 11-12.
13. The iron stores in a person onchronic dialysis should be moni-tored and adequate.
14.The transfer in saturation levelshould be greater than or equalto 20 and the ferritin levelshould be greater than or equalto 100.
15. Extra iron should be given tothose on chronic dialysis if needed to keep their iron storesnormal.
Since 1999, data has been collectedfrom a sample of people on dialysisaround the United States to see if theclinical performance measures arebeing met. The results of the data collection are reported yearly in anannual report which is available tothe public. CMS and the 18 ESRDNetworks are committed to improvingmedical care for those with kidneyfailure by using these clinical perfor-mance measures as guidelines.
Due to the small number of chil-dren with ESRD, there is a lack ofinformation to scientifically defineclinical performance measures forchildren. However, despite the factthat there are no measures, data isbeing collected on all children onhemodialysis in the United States. Itis hoped that this data collection willallow the development of clinical per-formance measures for children ondialysis in the next few years. Thiswill ultimately help improve the quali-ty of care that these children receivein the United States. F
F
Improved Patient Care and OutcomesBy Barbara Fivush, MD
12
Family Focus Volume 11, Number 3
Dear Editor,
First, let me thank you andyour staff very much for sending
me the quarterly Family Focus news-paper. I enjoy reading them immensely,
and I share the information with my fellowrenal patients at the John Hayes Kidney
Foundation in Port of Spain, Trinidad.
In the last issue of Family Focus, (Vol. 11, No. l –Winter 2002), I was very pleased that your very firstarticle dealt with high blood pressure and chronickidney disease. High blood pressure is a problem thataffects most of us patients in Trinidad. We are havinga lot of problems controlling it, mainly because ofignorance. I am reading leaflets and booklets on thesubject, and I have even bought a pressure gauge sothat I can monitor my pressure on a daily basis.
The other articles on high blood pressure are veryinteresting and informative; I enjoy them all. I mustthank you and your staff for emphasizing theimportance of controlling one’s blood pressure soas to avoid heart disease and stroke.
I am eagerly awaiting my next copy of FamilyFocus so that I can share it with my fellow
patients. Thanks once again.
I am yours respectfully, Cambdon Elder
Dear Editor,
My name is Pamela Ivery. I enjoy read-ing your newsletter, and it has been an
inspiration to me while I was going through myillness. I would like to tell my story so that it may be
able to help someone else.
At the age of two, the doctors discovered that one of my kid-neys was not fully developed. It had to be surgically removed.
Because of my illness, the doctors told my mother that I wouldnot survive to be six years old. I am now 32 years old. I was blessed
to complete high school and go on to college. I obtained a Bachelor’sDegree from Augusta State University and a Master’s Degree from the
University of Georgia.
My health started declining in December 1998, and I was diagnosed withEnd Stage Renal Disease. The doctors told my mother that someone couldbe tested to be a possible kidney donor. My mother wanted to be testedfirst. During this time, I had to go on dialysis, a fear of mine because of themyths I had heard from other people. I was blessed to go to the OutpatientDialysis Center at the Medical College of Georgia in Augusta. The staff waswonderful to me; they helped me get through my fears of dialysis. Somedays I would not be feeling my best, but once I got there, I had to smile.They kept my spirits up and provided my family and me with encouragingwords.
My mother became my kidney donor, and on June 23, 1999, I had mykidney transplant. I think God for her because she gave me the “Gift ofLife”. I also thank God for the transplant team at the Medical Collegeof Georgia, because they gave me a second chance at life.
Even though you may be going through something difficult inyour life, keep a positive attitude and have faith that God is
going to work it out. Although you may go through sometrials and tribulations, just
remember,
THERE’S A BLESSING IN THE STORM!Pamela Ivery
Dear Editor,
I am writing in regards to Pat Donnelly’sarticle, You Can Be Whole, which appeared in
the Summer 2001 edition of Family Focus. If youwould please pass on my compliments, I would
appreciate it. I very much enjoyed her article. It waswell written and about subjects that I could definitelyrelate to. Although I shared her thinking before I readthe article, it was helpful to have her words to rein-force my attitude. Thank you for passing this on.
I found several other articles very informative aswell. Thank you for putting out such a helpful
newspaper.
Sincerely, Jeannette A. Samuels
Dear Friends,
Thank you for the summeredition of Family Focus. While
I gained encouragement andenlightenment from every page,You Can Be Whole by PatDonnelly was immensely helpful.
Thanks Sincerely, Harry Lansman
MAILBOX

13
T R A N S P L A N TRAANSP
N
LA
TN
RT R A N S P L A N T
SPLANT
Transplantation became anacceptable treatment forkidney failure almost 40
years ago. Numerous improve-ments have made this therapymore successful and an option formany people. One of the primaryreasons for the success of trans-plantation is the availability of bet-ter immunosuppressive medica-tions, the drugs that keep the bodyfrom rejecting the new kidney. Thebody’s rejection of the new kidneyis a normal reaction to any neworgan. Each class of drugs works in a different way to help block the rejection. As medical scienceunderstood the rejection processbetter, they were able to changeand improve the medications thatprevent and treat rejection.
Cyclosporin became available in the early 1980s and made atremendous impact on the successof transplantation. Rejection rateswent from 50 percent to less that20 percent with its introduction.Some of the even newer medica-tions are now able to more effec-tively target the specific types ofwhite cells that attack the neworgan. Rejection rates are now aslow as 10 percent or less, and mostrejection episodes are reversible.
Each transplant program uses acombination of these and otherdrugs and each transplant recipienthas his or her own tailored medica-tion formula. Changes are made asphysicians review the patient’sresults, rejection rates, infections,side effects and cost, as well as theresults of other larger programsthat do clinical studies. The drugmanufacturers conduct medicationtrials with large transplant pro-grams which then publish theirresults for the transplant communi-ty to review and learn from.
Much work is being done withone of the oldest medications intransplantation, prednisone. The side effects of this drug are the most bothersome to patientslong-term and include weight gain,acne, bruising easily and bone dis-ease. However, it remains a verygood immunosuppressive medica-tion because it reduces the inflam-mation caused by rejection.Because the newer drugs work sowell in preventing rejection, mostprograms are using much lowerdoses of prednisone, which helps
prevent some of the negative sideeffects. Some programs are taper-ing patients off completely.
Surgical techniques have notchanged too much in recent yearsfor the recipient, but living donorsmay benefit from a procedure forremoving the kidney that allows forquicker recovery. Using a laparo-scopic procedure, the kidney isremoved through much smallerincisions. A scope is inserted intothe abdominal space and a gas is“pumped in” to expand the areaaround the organs. Then, throughsmaller incisions, other instru-ments are used to carefully removethe kidney. As a result, the donormay be in the hospital for only twoor three days and return to work intwo weeks. This technique is beingperfected and adopted by more andmore transplant centers. As withany surgery, there are risks, suchas a reaction to the anesthesia,bleeding, infection or even death.Studies are being done to comparethe laparoscopic technique with theopen technique. Not all patientsmay be candidates for the laparo-scopic surgery—this depends onbody size, previous surgery and thekidney blood vessels.
Many on the waiting list wait along time for kidneys because theyhave a high antibody count. Thiscan be caused by blood transfu-sions, previous transplants or preg-nancies. It can be very frustratingfor those who have been on the listfor years to see others who havebeen on the list for a shorter time— yet do not have high antibodies— receive a kidney transplant whilethey continue to wait for a compati-ble kidney. However, there are newmethods to remove antibodies. Oneexample is through a combinationof medication and plasmapheresis(a blood cleansing process similarto hemodialysis). Your transplantcenter can discuss this option with
you and recommend a center thatis doing this technique.
Of course, all of these new med-ications and techniques are excit-ing and promising, but there stillremains a severe shortage of donororgans. Living donors are oneanswer. Early in transplantation,living donors had to be someonewho was blood related (living relat-ed donor) and a good tissue match.However, about 10 years ago, therewas a movement to use donors whohad a compatible blood type and aclose emotional relationship withthe recipient, usually a spouse, in-law or close friend (living non-relat-ed donor). With the newer immuno-suppressive drugs, a close tissuematch may not be as important asa kidney from a healthy livingdonor. As the public becomes moreaware of the need for donors, peo-ple are expressing interest indonating to a stranger. Some cen-ters are participating in joint effortswith organ procurement organiza-tions to closely evaluate these gen-erous people for possible donation.Transplants have been performedusing living anonymous donorsvery successfully. This is a newanswer to the shortage of kidneysthat may become more popular.
People are also now being referredfor transplantation who have morecomplicated illnesses. For example,in the early days of transplantation,people with diabetes were notaccepted for transplantationbecause of the fear of developingmore infections and heart complica-tions. Now, with diabetes being oneof the main causes of kidney fail-ure, many diabetics are successful-ly being transplanted, as are peoplewho may have already had a heartor liver transplant.
Still, transplantation is not thetreatment of choice for everyoneand it is an individual decision thatshould be made after consultationwith your family and health careteam. Dialysis techniques haveimproved so much that somechoose this option over transplan-tation. It is important to discuss allof the treatment options with yourhealth care team early in the man-agement of kidney failure and thenmake a decision that is the rightone for you.
What’s New in Transplantation?By Linda Harte
FF
Family Focus Volume 11, Number 3
“Transplants have been
performed using living
anonymous donors very
successfully. This is a
new answer to the short-
age of kidneys that may
become more popular.”
14
Family Focus Volume 11, Number 3
How To Partner With your Dialysis By
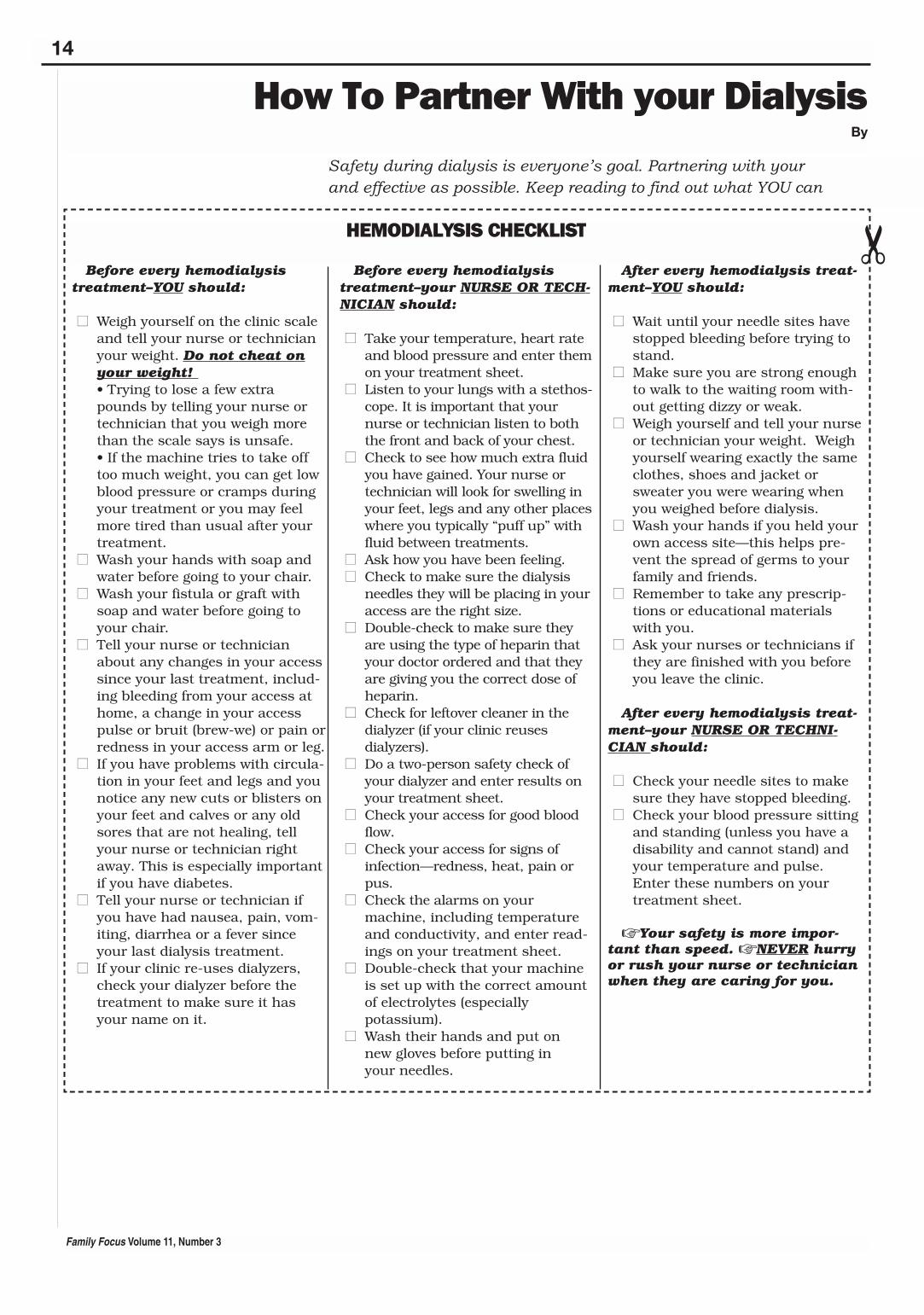
Before every hemodialysistreatment–YOU should:
■■ Weigh yourself on the clinic scaleand tell your nurse or technicianyour weight. Do not cheat onyour weight! • Trying to lose a few extrapounds by telling your nurse ortechnician that you weigh morethan the scale says is unsafe. • If the machine tries to take offtoo much weight, you can get lowblood pressure or cramps duringyour treatment or you may feelmore tired than usual after yourtreatment.
■■ Wash your hands with soap andwater before going to your chair.
■■ Wash your fistula or graft withsoap and water before going toyour chair.
■■ Tell your nurse or technicianabout any changes in your accesssince your last treatment, includ-ing bleeding from your access athome, a change in your accesspulse or bruit (brew-we) or pain orredness in your access arm or leg.
■■ If you have problems with circula-tion in your feet and legs and younotice any new cuts or blisters onyour feet and calves or any oldsores that are not healing, tellyour nurse or technician rightaway. This is especially importantif you have diabetes.
■■ Tell your nurse or technician ifyou have had nausea, pain, vom-iting, diarrhea or a fever sinceyour last dialysis treatment.
■■ If your clinic re-uses dialyzers,check your dialyzer before thetreatment to make sure it hasyour name on it.
Before every hemodialysistreatment–your NURSE OR TECH-NICIAN should:
■■ Take your temperature, heart rateand blood pressure and enter themon your treatment sheet.
■■ Listen to your lungs with a stethos-cope. It is important that yournurse or technician listen to boththe front and back of your chest.
■■ Check to see how much extra fluidyou have gained. Your nurse ortechnician will look for swelling inyour feet, legs and any other placeswhere you typically “puff up” withfluid between treatments.
■■ Ask how you have been feeling.■■ Check to make sure the dialysis
needles they will be placing in youraccess are the right size.
■■ Double-check to make sure theyare using the type of heparin thatyour doctor ordered and that theyare giving you the correct dose ofheparin.
■■ Check for leftover cleaner in thedialyzer (if your clinic reuses dialyzers).
■■ Do a two-person safety check ofyour dialyzer and enter results onyour treatment sheet.
■■ Check your access for good bloodflow.
■■ Check your access for signs ofinfection—redness, heat, pain orpus.
■■ Check the alarms on yourmachine, including temperatureand conductivity, and enter read-ings on your treatment sheet.
■■ Double-check that your machineis set up with the correct amountof electrolytes (especially potassium).
■■ Wash their hands and put on new gloves before putting in your needles.
After every hemodialysis treat-ment–YOU should:
■■ Wait until your needle sites havestopped bleeding before trying tostand.
■■ Make sure you are strong enoughto walk to the waiting room with-out getting dizzy or weak.
■■ Weigh yourself and tell your nurseor technician your weight. Weighyourself wearing exactly the sameclothes, shoes and jacket orsweater you were wearing whenyou weighed before dialysis.
■■ Wash your hands if you held yourown access site—this helps pre-vent the spread of germs to yourfamily and friends.
■■ Remember to take any prescrip-tions or educational materialswith you.
■■ Ask your nurses or technicians ifthey are finished with you beforeyou leave the clinic.
After every hemodialysis treat-ment–your NURSE OR TECHNI-CIAN should:
■■ Check your needle sites to makesure they have stopped bleeding.
■■ Check your blood pressure sittingand standing (unless you have adisability and cannot stand) andyour temperature and pulse.Enter these numbers on yourtreatment sheet.
☞ Your safety is more impor-tant than speed. ☞ NEVER hurryor rush your nurse or technicianwhen they are caring for you.
Safety during dialysis is everyone’s goal. Partnering with your and effective as possible. Keep reading to find out what YOU can
HEMODIALYSIS CHECKLIST
✂

15
Family Focus Volume 11, Number 3
FF
Staff for A Safer TreatmentBobbie Knotek, RN, BSN
To stay as safe as possible whendoing YOUR peritoneal dialysis (PD),follow these “words of wisdom” from fel-low peritoneal dialysis patients:
■■ Do ALL your continuous ambula-tory peritoneal dialysis (CAPD)exchanges or cycler treatments.
✔ Many people think it is okay to skiptreatments or exchanges, especiallyif they are feeling good. Unfortunat-ely, how you are feeling from day today is not a good way to tell if youare getting enough dialysis to stayhealthy. When you miss or shortenyour dialysis treatments you arehurting your body in ways you cannot see. You may not feel bad rightaway, but sooner or later you willget sick. You may even die an earlydeath because of the damagecaused by too little dialysis.
✔ If you have trouble doing all yourCAPD exchanges or cycler treat-ments, talk to your home dialysisnurse right away.
■■ Always do your peritoneal dialysissteps the way you were taught.
✔ Never take short cuts or skip steps.If you take short cuts, change orskip steps, you could get peritonitis(an infection of the peritoneal dialysis membrane).
■■ Remember to:• Always wear your mask when
making a CAPD or cycler connection.
• Anyone in the room with youshould also wear a mask whenyou are making a CAPD or cyclerconnection.
• Do your dialysis in a clean area.• Turn off fans and keep windows
closed in the room while you aremaking a CAPD or cycler connection.
• Keep pets out of the room whileyou are making a CAPD or cycler connection.
■■ Wash your hands before every peri-toneal dialysis procedure!
✔ Put your mask on before you washyour hands. When you put yourmask on after you wash yourhands, your clean hands touch thegerms on your face and hair.
✔ Use the soap that comes with yoursupply order.
✔ Do NOT shorten your hand wash-ing time, even if you are in a hurry.Time yourself to make sure you arespending enough time washingyour hands. To keep track of howlong you are washing your hands,try one of these tricks: 1. Put a clock by the sink and
watch to make sure you arewashing for as long as you were taught.
2. Count out loud (1000, 1001,1002, etc.) while you watch theclock. See how high you cancount until your hand-washingtime is up. Then, every time youwash your hands, count to thatnumber before you stop.
3. Sing a song out loud while youwatch the clock. Repeat the songas many times as you need tountil your hand-washing time isup. Then, every time you washyour hands, sing this song outloud to yourself.
■■ Check your dialysis drain bags. Ifyou see cloudy fluid—call yournurse or doctor immediately!
✔ Normal drain bags should be clearand light yellow or straw colored.
✔ Cloudy drain bags are a sign ofinfection. They may start out hazyor cloudy, or they may look likemilk.
✔ Watch for other signs of infectionlike fever or belly pain. The bellypain may be a sharp ache or it mayfeel like gas pains. If you get a feveror belly pain between exchanges,drain your dialysis fluid right awayand check the fluid to see if it iscloudy. If your drain fluid is cloudyor hazy, call your nurse or doctorright away.
■■ Take care of your catheter and exitsite. An infected exit site can causeperitonitis!
✔ Daily exit site care helps preventexit site infections and peritonitis.
✔ Check your exit site and tunnelevery day for these signs of infection:• Redness of the skin around the
catheter.• Green, brown or white “stuff”
or pus at the exit site.• An exit site that hurts or is
tender.• Fever
✔ Never change the way you do exitsite care, unless your nurse or doc-tor says it is okay.
✔ Try to keep your catheter frombeing tugged on or moving around.Your catheter can be taped orsecured to the skin to keep it frombeing pulled or twisted. If you thinkyou would like to tape yourcatheter, but taping is not part ofyour catheter care steps, talk withyour nurse.
✔ Always get permission from yourdoctor and nurse before you swimanywhere! Some peritoneal dialysisunits let people on PD swim in theocean or in a private pool or spathat is heavily chlorinated, but youmany need to take extra precau-tions or do special exit site care toprevent infection.
✔ Do NOT swim in lakes, rivers andponds. Hard-to-kill germs in lakes,rivers and ponds can cause exit siteinfections, catheter tunnel infec-tions and peritonitis.
■■ Stay in touch with your home dialy-sis nurse in between clinic visits.Be sure to call your nurse if you:
✔ Make a mistake in your dialysissteps that could cause peritonitis.
✔ Start feeling bad between clinic vis-its (dizzy, headaches, feeling likeyou have the flu, trouble breathing,don’t feel like eating, vomiting, etc.)
✔ Have a new or continuing problemwith your exit site. For example, ifyour catheter gets tugged on, if youhave redness, pain or clear fluidaround the exit site or if you see“pus” at the exit site.
✔ Have a new or continuing problemwith your catheter or with dialysis.For example, you find a hole in thecatheter, you have slow drains orno fluid drains out or if your drainbag is hazy or cloudy.
☞ When you do dialysis at home— YOU are responsible for YOURsafety, so . . .
☞ Be smart — do your dialysisand do it safely!
dialysis staff will help make YOUR dialysis treatments as safe do to make your dialysis treatments safer and more effective.
PERITONEAL DIALYSIS CHECKLIST
✂
16
NON-PROFIT ORG.U.S. POSTAGE
PAIDNew York, NY
Permit No. 532730 East 33rd StreetNew York, NY 10016
• Check the top and bottom of your feet every day, lookingfor cracks, dry skin, cuts, blisters, sores and redness. Tocheck the soles of your feet, hold your foot over a magni-fying mirror placed on the floor and look in the mirror.Feel both feet to see if they are the same temperature. Ifone foot starts to become colder or warmer than theother, ask your dialysis or transplant nurse to do a “footcheck” on both your feet.
• Put lotion on your feet and legs every day (Vaselineworks well). Do NOT put lotion between your toes.Putting lotion between your toes makes the skin toomoist and can lead to fungus growth between your toes.A fungus can turn into a serious infection with possibleloss of toes or a foot.
• Cut toenails straight across, even with the top of toe.File sides down to prevent ingrown toenails.
• Wear white socks so any injury, bleeding or drainage willbe easily seen.
• Wear “tie” shoes. Slide-in shoes put too much pressureon your foot.
• Buy shoes with a finger’s width between the top of yourlongest toe and the end of the shoe and room for yourtoes to wiggle.
• Feel inside shoes for small objects or torn linings beforeputting on shoes. Foot ulcers from poor fitting shoes or aforeign object can form in eight hours.
• Wear slippers or shoes at all times, even athome—NEVER go barefoot. Keep feet away from heatingpads, hot water bottles, car heaters and fireplaces.
• Tell your nurse or nephrologist right away if you notice asore on your foot.
• Change position often. Do not cross your legs or sit for along time in one position.
• Keep toenails unpolished—ulcers can hide under yourpolished toenails.
• Go to a foot doctor to have corns or calluses trimmed.
It is up to you—make the decision today to “Tune Up” yourbody for better health tomorrow!
References:
1DeRossi, S.S., Glick, M., (1996). “Dental considerations
for the patient with renal disease receiving hemodialy-sis”. Journal of American Dental Association, 127 (2).p.211-219.
2Robinson, Tim., (2002). Interview with Tim Robinson,
D.D.S. February 20, 2002.
From Head to Toe continued from page 10
FF
NEW RESEARCH STUDY AT BOSTON COLLEGEFOCUSING ON OLDER COUPLES AND HEMODIALYSIS
The National Institutes of Health are conducting a new study concerning end-of-life treatment preferences and outcomes for hemodialysis patients and theirspouses. The OPTIONS study will aim to extend knowledge on the ways inwhich people with End Stage Renal Disease (ESRD) and their spouses makedecisions about continuing their life-sustaining treatment. Patients who are eli-gible are those 55 years of age and older, have been on hemodialysis for at leastsix months and have been married or partnered for at least five years.
If you would like to learn more about this study and find out how to participate,please go to this link on the NKF Web site: www.kidney.org/professionals/resstudy.cfm or contact Jennifer Rosenbaum, Recruitment Manager for theOPTIONS study, at the national, toll-free number (866) 772-3387.