ekibbey.weebly.comekibbey.weebly.com/.../clinical_practicum_paper.docx · web viewgaining...
TRANSCRIPT

Running head: CLINICAL PRACTICUM 1
Nurse Educator and NPD Specialist Clinical Practicum Paper
Erin Kibbey
Ferris State University
CLINICAL PRACTICUM 2
Abstract
Gaining competency in the role of the nurse educator and nursing professional development
specialist can be obtained through the utilization of a practicum experience. This paper describes
a practicum experience designed to gain experience and practical knowledge related to the
educational process utilized by both of these specialty roles. The three standards of practice this
practicum experience focused on included: a) facilitation of learning, b) participation in
curriculum design and evaluation of program outcomes, and c) use of assessment and evaluation
strategies. Based on these competencies and guided by Kolb’s experiential learning theory,
several key objectives and activities were completed during this experience. This paper
describes challenges related to the application of these roles, strategies applied to address the
challenges, description and analysis of clinical projects completed during the project, and an
evaluation of the practicum.
Keywords: competency, nurse educator, nursing professional development specialist,
standards of practice

CLINICAL PRACTICUM 3
Nurse Educator and NPD Specialist Clinical Practicum Paper
According to the American Nurses Association and National Nursing Staff Development
Organization (ANA & NNSDO, 2010) the nursing professional development (NPD) specialist
uses their expertise in nursing education to help other nurses develop their competence in various
settings. They support continuous learning and help create an environment that supports the
adult learning process. Competencies related to the educational process including assessment,
planning, implementation, and evaluation are the same for both NPD specialists and academic
nurse educators (Brunt, 2007). This practicum was designed to gain confidence and skills related
to the educational process within both of these specialty roles. The purpose of this paper is to
describe the clinical practicum experience, including role issues and challenges, strategies
utilized to address role challenges, clinical projects completed, and evaluation of the practicum.
The importance of obtaining hands-on, practical experience prior to taking on a new role
cannot be underestimated. As a future academic nurse educator or NPD specialist, fulfillment of
a 300 hour clinical practicum experience provided the opportunity to gain competency towards
these roles. The following paper describes the clinical practicum intended to provide experience
in the educational process similar to both of these specialty roles.
Practicum Overview
The overall goal of the clinical practicum was to gain competency in the specialty roles
of the NPD specialist and nurse educator as based on my previous background and clinical
experience and future career goals. Since the educational process utilized by these roles is a
competency area I had little experience in, this practicum was designed to specifically focus on
growth in this area. As such, this practicum focused on three particular National League for
Nursing (NLN, 2012) standards of practice. These three standards included: the facilitation of

CLINICAL PRACTICUM 4
learning, participation in curriculum design and evaluation of program outcomes, and the use of
assessment and evaluation strategies (2012). Although these standards are specific to the nurse
educator role, the NPD specialist has several responsibilities related to these education based
standards. Some of the key responsibilities for NPD specialists related to educational
competency include: assessing and validating competency, assessing educational needs,
participating in on-the-job activities, orienting, assisting in role transition, and developing
curricula (ANA & NNSDO, 2010). Thus, several of these responsibilities were integrated into
the clinical practicum experience. Finally, the practicum experience provided several additional
opportunities for growth in the ANA and NNSDO (2010) standards of leadership, collegiality,
and collaboration.
In order to gain competency in the educational process as an NPD specialist and nurse
educator, this practicum took place at Munson Medical Center (MMC) in Traverse City,
Michigan. Within this setting, I gained experience in the educational process by working closely
with the program coordinator for the critical care internship program as well as the transition to
practice program. The coordinator for both of these programs, Ms. Hresko, was also my
preceptor for the clinical practicum experience.
Foundational Theory
Progression of competency within the three nurse educator standards of practice were
designed based on Kolb’s experiential learning theory. From this theory comes the notion that
ideas are not fixed, they are shaped and reshaped through experience (Kolb, 1984). Thus,
learning is a process that continually changes through experience. Also central to this theory is
the idea that learning involves the environment and real-world experience. In addition, learning

CLINICAL PRACTICUM 5
is a cyclical, adaptive process occurring in all human settings and all life stages. This practicum
amplified these ideas and provided the foundation for the clinical practicum.
Objectives for the practicum were based on Kolb’s (1984) idea that the experiential
learning cycle is a continuous process. The first objective for the practicum was to become
acclimated to the educator role and educational process through observation. The second
objective was to reflect on the observational experiences and the third objective was to apply
knowledge and actively participate in the educational process. This is similar to Kolb’s (1984)
idea that individuals have a concrete experience, they reflect on that experience, they derive
meaning from it, and they try out the meaning they’ve constructed (Jeffries & Clochesy, 2012).
Additional objectives for the practicum were based on the desire to further apply the proposed
concrete experiences, as Kolb’s theory suggests.
Issues, Challenges, and Strategies
In retrospect, five main challenges related to implementation of the NPD specialist and
educator roles were encountered during the practicum experience. These issues related to role
clarity, assessing learning needs, anxiety about teaching, organizing and planning, and
communication. Several strategies and approaches were applied in order to gain further
experience in these roles and to ultimately allow for a successful practicum experience.
Congruence of Role Expectations
Since this practicum was completed at MMC, where I am also a staff nurse employee,
one of the first issues of concern was the congruence of expectations to individuals encountered
while immersed in the practicum. Since I was also working with Ms. Hresko for completion of
another Ferris course, I had similar concerns about the need to clarify and differentiate
expectations and practicum goals compared to the other course. In addition, as I progressed
CLINICAL PRACTICUM 6
within the practicum experience, there were various individuals that requested my help with
projects or endeavors that they felt would be mutually beneficial. Some of the time I was able to
help with these requests and still work towards my own practicum goals. However, I did feel
that I had to continually ensure the expectations of others still met the practicum goals for
development in the NPD specialist and educator roles. According to McKinley (2008),
expectations of nursing administration, management, and staff may not be mutually exclusive,
which can result in educators feeling frustrated and spread too thin. There were a few times
throughout the practicum where Ms. Hresko and I were involved in several different projects,
roles, and responsibilities, occasionally resulting in an inability to complete some of the tasks we
had planned on completing for the day. Similarly, it was a challenge to keep in mind that there
are limitations to the role. As McKinley (2008) notes, the clinical educator cannot fix every
problem, nor do they have the answer to every question.
Strategies. One of the main strategies evoked at the beginning of the practicum was to
share with Ms. Hresko the practicum planning guide I had previously created (see Appendix A).
By sharing the goals and objectives for the practicum with Ms. Hresko, she was able to have a
clearer picture of what the practicum experience intended to focus on. From the beginning,
providing clarity about expectations is essential to implementation of the educator role
(McKinley, 2008). In addition, establishment of goals and an outline of specific activities and
responsibilities for a defined time frame can assist the educator in establishing successful
implementation of the educator role (2008).
Another strategy employed to clarify my role outside of my normal job at MMC was to
dress differently than I do as a staff nurse. On the unit I typically work, I wear burgundy colored
scrubs. Once I was visiting units as a student instructor, I wore blue hospital scrubs. This

CLINICAL PRACTICUM 7
usually caused those that I typically work with to question why I was wearing something
different, resulting in a conversation that clarified my role as a student instructor for the critical
care interns. Outside of the hospital units, Ms. Hresko also announced my presence at meetings
and clarified my role.
A similar approach was taken with individuals that approached me about helping them
with various projects. I carefully consulted with the individuals and clarified what my role
would be and considered how the activity would be beneficial to my own goals and whether it
was appropriate to take part. For example, I was able to help on several occasions in the
simulation lab, allowing valuable experience in the facilitator and operator roles. However,
before taking part in these opportunities, achieving clarity about expectations, time commitment,
and goals, were key to these being successful experiences for all parties involved.
Assessing Learning Needs
At the onset of the practicum, I was unsure as to how Ms. Hresko had obtained her
insight into what the course learning needs may be for the next class of critical care interns. She
had several ideas about what needed to be included in the next class, but it was not until I saw
the stacks of folders with raw evaluation in her filing cabinet that I began to understand some of
the ways she had assessed learning needs. I was surprised and overwhelmed with the amount of
evaluation data pertaining to the internship that had been collected over the years. Accordingly,
needs assessments for clinical educators can be both formal and informal (McKinley, 2008).
Although Ms. Hresko had clearly looked at feedback, test results, and worked closely
with the past interns, I was concerned about the lack of compilation of the data that could have
been further analyzed to assess learning gaps. For instance, the written tests that had been given
to past interns could have been used to identify areas of education that needed strengthening in

CLINICAL PRACTICUM 8
order to achieve program outcomes (McKinley, 2008). However, the raw evaluations, as well as
the pre and post internship knowledge tests were in a filing cabinet but had never been placed
into a usable form. According to Avillion, Brunt, and Ferrell (2007), a needs assessment can
identify specific needs, validate the needs to key stakeholders, and document the identified needs
into a format that can be developed. Because these items were never placed into a format where
the data could be meaningfully interpreted, it was difficult for me to assess the potential learning
needs for the next class of critical care interns.
Strategies. In order to fix the issue of unclear needs assessment data, I compiled the pre
and post test results from the Basic Knowledge Assessment Tool for Critical Care (BKAT). This
tool is an example of a test that can be used to assess the knowledge level of staff and are
available for various nursing care specialties (Toth, 2008). The BKAT-7 or the BKAT-8 were
given to all the previous classes of interns at the start of the critical care internship program and
then again at the end of the internship program. Since the results of how the interns had
improved and what content areas they were still having difficulty with were never placed into
any kind of spreadsheet and analyzed, I spent a great deal of time completing this process. In
scoring the BKAT’s there is an answer sheet and score sheet that tells what content area the
question pertains to (such as emergency situations, electrocardiogram interpretation, monitoring
of lines, ventilators, etc.). Toth (2008), the author of the BKAT, noted that the BKAT can be
useful for identifying needed content and as a measure of learning. Content areas were tabulated
across each of the interns. In total, I tabulated results from 28 interns that completed the BKAT-
8. All 90 questions were examined on both the pre-test and post-test, so this was quite a bit of
data to record.

CLINICAL PRACTICUM 9
Once I was able to interview and spend more time with the new class of interns I was also
able to begin less formally assessing learning needs. Gaberson and Oermann (2010) note that the
first area of assessment involves understanding the learner’s current level of knowledge, skill,
and attitude. Interactions with interns while on the various critical care units were utilized as an
opportunity to assess the current level of knowledge and skill and other characteristics that could
influence achievement of the internships learning outcomes. In addition, e-journals and post
conferences were helpful for assessing learning gaps and identifying accomplishments in clinical
practice. A second assessment area should consider individual characteristics that could
potentially influence performance (Gaberson & Oermann, 2010). “Understanding the
background, experience, and style of learners, determining the number of learners, and focusing
on the desired outcome must all be a part of the assessment for the educator to select the best
approach to learning” (McKinley, 2008, p. 392). Finally, another strategy for assessing learning
needs is to assess possible barriers to learning (2008). Time, motivation, lack of resources, lack
of support, and resistance to change are potential roadblocks to learning. Thus, all of these
considerations were utilized in the assessment of learning needs and planning of clinical learning
approaches, as well as the development of the first clinical project (see Appendix B).
Anxiety about Teaching
As a novice to the nurse educator role, one of the biggest concerns I had going into this
practicum was worrying about my ability to help new nurses, new critical care nurses, and the
critical care interns learn the essential knowledge and skills to become a competent nurse. As
Penn, Wilson, and Rosseter (2008) point out, “many nurses who have spent years in the practice
setting are only vaguely aware of what is involved in teaching…” (p. 6). This was true in my
case. Although, I have been a preceptor, spent the last six years as a bedside nurse, and was
CLINICAL PRACTICUM 10
starting my last semester of graduate school, I had never been immersed in the educator role
outside of the unit I worked. Moving out of my comfort zone and teaching in other areas with
nurses I did not know, was a new experience that definitely evoked some concern at the start of
the practicum. Research has identified effective teachers as knowing how to teach, being
clinically competent, supportive, patient, friendly, and having the ability to maintain collegial
relationships with students and staff (Stokes & Kost, 2012). Educators must also have the ability
to deliver knowledge in an effective manner (2012). Since I was new to the role, I was
concerned about my ability to portray these qualities and actually be an effective teacher.
Strategies. Consequently, the ability to help students’ master essential skills and
knowledge in order to become professional nurses is so paramount that the need for preparation
and development of individuals taking on teaching roles is an important issue (Stokes & Kost,
2012). Therefore, through a variety of experiences, both observational and experimental, my
learning and knowledge about facilitation grew, allowing me to become more comfortable with
teaching. As previously mentioned, the proposed practicum was designed based on Kolb’s
experiential learning theory and cycle of learning. Within Kolb’s cycle of learning the various
learning processes can include concrete experience, reflective observation, abstract
conceptualization, or active experimentation (Ullrich & Haffer, 2009). Thus, in this practicum I
utilized this process in order to gain confidence and ease my fears about teaching. I began by
watching and carefully observing my preceptor and the speaker at the first role transition class,
then reflected on the experiences, and finally I began refining and improving my comfort level
with teaching through active experimentation.
Imperative to Kolb’s cycle of learning framework was the opportunity to interact with
Ms. Hresko, several other educators, and my graduate degree program peers that I got to know

CLINICAL PRACTICUM 11
throughout the practicum. Not only did these individuals serve as mentors and guides to the
educator role, but they helped me feel welcome and encouraged throughout the process. In a
study by Schoening (2013) it was found that peer mentors provided beneficial emotional support
during the role transition process from nurse to nurse educator. According to Penn et al. (2008),
faculty mentors and professional development opportunities that promote learning about the
teaching environment and opportunities to enhance teaching skills should be encouraged for
novice educators.
Participating as a facilitator in a role transition class was my first attempt at teaching in
this practicum. The first and main focus during this time was on creating the right tone for
students to feel comfortable sharing, especially with the difficult topics that were presented in the
class. According to the NLN (2012), facilitation of learning can be accomplished by creating an
environment conducive for students to learn the desired outcomes. In addition, I knew it was
also important, as noted by the NLN (2012), to display interest and respect for the learners. I
shared stories that demonstrated patience, caring, and integrity.
Attending the simulation facilitator class was another strategy utilized to become more
comfortable with teaching and facilitating. It was extremely useful to utilize the information
learned from the beginning of the facilitator class and apply it when assigned to act as a
facilitator. I essentially practiced being a facilitator, without having real students. This
opportunity provided individualized attention in both the operator and facilitator roles. In
addition, I was able to obtain feedback from the other learner and the class instructor on my
facilitator techniques. Finally, I had the opportunity to practice debriefing and to discuss
effective ways to debrief. This approach was very helpful in decreasing my anxiety related to
facilitation and debriefing.
CLINICAL PRACTICUM 12
According to Shellenbarger and Edwards (2012), simulation activities can benefit
graduate nurse educator students. Accordingly, simulation activities can be a useful way for
novice nurse educators to create scenarios for simulation so they can practice the skills of
planning, implementing, and evaluating teaching and learning skills. Thus, not only was it
beneficial to learn this technology for future use, but the process of learning and practicing using
it throughout this practicum helped me gain experience in feeling more comfortable with
teaching as well as planning, which was another challenge as described in the following section.
Organizing and Planning
Throughout the clinical practicum experience, there were several hours spent planning
and organizing. McDonald (2010), notes that many educators take work home with them and
that an excessive workload for educators is often a factor in faculty retention. From the
beginning, I realized this was a potential issue for the success of my practicum experience. Since
Ms. Hresko’s educator position was only a 24 hour a week position this was a concern from the
start and one that felt like we had to frequently come to terms with. Duties that included
teaching, preparation, administrative meetings, and other committee meetings often times left us
both with the added burden of planning and organizing outside of MMC. Educators must also
prepare students for orienting to the clinical environment, be familiar with the clinical setting,
and know the knowledge and skill level needed in the practice area where teaching will take
place (Gaberson & Oermann, 2010).
During the transition stage from nurse to nurse educator, one of tendencies for novice
educators is to over prepare for student encounters (Schoening, 2013). This was a real challenge
at the onset of this practicum. Before facilitating in skills sessions, I often spent several hours
preparing myself for teaching content that I was already very familiar with. This concern

CLINICAL PRACTICUM 13
seemed to coincide with my anxiety of teaching. According to Schoening (2013), novice
educators that over prepare may fear failure due to a lack of experience. In planning my first
clinical project, the physical assessment simulation, I also spent several hours not only in
creating the lesson plan but playing the facilitation over in my head and researching how to
perform a proper head-to-toe assessment. As a critical care nurse of nearly six years, I am very
comfortable performing head-to-toe assessments, but I felt the need to prepare and plan for the
learning activity more than what I believe would be required for an educator that is more
confident in their role.
Strategies. One strategy I utilized to deal with organizational and planning issues was to
frequently consult my calendar and carve out time for necessary tasks. Utilizing the practicum
planning guide (see Appendix A), I placed all of the activities and responsibilities Ms. Hresko
and I had committed to into a calendar. I frequently consulted my calendar and estimated the
length of time it would take to carry out various tasks and plugged those in as necessary. Ms.
Hresko and I frequently communicated via email and telephone in order to ensure we were
prepared for the planned activities. Planning for the lessons also became easier with practice. In
addition, when I came to the realization that I would never be completely prepared for every
single question that could be asked or for every contingency that could occur, I began to lighten
up on my planning. According to Schoening (2013), faculty that successfully transitioned from
nurse to nurse educator identified the strategy of focusing on the learning process, rather than the
product. Thus, teaching became more learner focused than content-focused. This was
something I still need practice with, but was a mindset I tried to utilize as I continued in my
practicum experience.

CLINICAL PRACTICUM 14
Communication
One of the biggest issues and concerns encountered during this practicum experience was
related to the topic of communication. According to McKinley (2008), communication is
essential to the success of any role but even more so for that of an educator. Moreover,
McKinley (2008) notes that unclear, indirect, inefficient, and poor communication techniques
can result in frustration and failure. Finally, the NLN (2012) notes that an important competency
for the nurse educator is to practice skilled oral, written, and electronic communication. In
addition, communication should reflect awareness about one’s self and others as well as convey
ideas in a range of situations (2012).
This concern was important in my interactions with the critical care interns. Emphasis on
the lines of communication on clinical units, who to go to for help, and under what
circumstances they should seek help were important issues that needed to be communicated to
students, or in this case the interns, before they entered the critical care units (Gaberson &
Oermann, 2012). Providing feedback that is constructive and respectful was another concern I
had during the practicum experience, due to my lack of experience in this area. Often evaluation
is one of the most intimating skills for new educators (Penn et al., 2008). Another example of a
communication concern that occurred earlier in the practicum was when the last class of interns
were working on their case study presentations. This was the final component to the internship
program and was scheduled for March 14. An issue that came about in relation to
communication was the lack of guidelines about Ms. Hresko’s expectations for the presentations.
In talking with some of the past interns, as well as Ms. Hresko, there was no description of what
the presentation should entail or identification of how the interns would be evaluated based on
the presentation.
CLINICAL PRACTICUM 15
Another important consideration when communicating with learners is that too much
information can result in overload and shutting down communication (McKinley, 2008).
According to Penn et al. (2008), the ability to differentiate between critical content and logically
sequencing the information to maximize learning is an important communication consideration.
On the first day of the internship, the interns were given a huge binder of unit specific articles,
the syllabus I developed, the electrocardiogram course book, and the skills lab book. It was very
apparent that this approach resulted in overload and a portrayal of being overwhelmed.
Finally, promoting clear communication with internship preceptors, unit managers, and
others encountered throughout the practicum was another important concern related to
communication. During one of the meetings I attended about the development of the
professional practice model, I was called on to voice my opinion about the idea of back rubs
being part of the model. Knowing that this topic was a source of contention amongst the group,
it was a concern that poor communication about my thoughts on this subject could result in a
poor outcome. Lastly, there was an issue with an intern feeling unwelcomed on one of the
critical care units and proper communication in handling this problem was critical for all parties
involved.
Strategies. One strategy utilized to promote communication to the interns related to the
issue about the case presentations was to provide clear, written expectations for the assignment
as well as a copy of the tool that would be utilized to evaluate the interns on. As such, rubrics
are a type of rating scale and can be used to help provide a clear direction for grading and
assignment criteria (Bonnel, 2012). Since the case presentations by the interns are an important
evaluation component to the internship program, it was deemed necessary by myself and Ms.
Hresko that a rubric could be utilized to help facilitate a clearer understanding of the

CLINICAL PRACTICUM 16
expectations for the presentation. Rubrics can be a convenient form for providing feedback and
allows for more discrimination in judging than checklists (Bonnel, 2012). While a rubric worked
well for the case study presentation, a checklist was utilized for the physical assessment
simulation learning activity. The use of a checklist, in this instance, provided me, the observer,
with clear criteria for evaluation resulting in feedback that was viewed as fair, direct,
constructive, and respectful.
Another strategy utilized to combat communication challenges was my promotion of
credibility. McKinley (2008) has said that real-world credibility is an essential component that
needs to be portrayed by the educator. Hence, having appropriate credentials, experience, and
knowledge can communicate a message of credibility (2008). In meeting with the interns it was
conveyed by both Ms. Hresko and myself that we were both still critical care staff nurses, had
obtained critical care certification, and had several years of experience at the bedside. Similarly,
another strategy that is important to communicating credibility is just being available, dressing
the part, and bringing forth a positive attitude (2008). When working with the interns, I met with
them on a daily basis, wore scrubs, lent a hand with patient care, and was available throughout
the day.
Additional communication strategies utilized throughout the practicum focused on the
use of personal attributes. Accordingly, the NLN (2012) facilitation of learning competency
notes the importance of using personal attributes such as caring, confidence, patience, integrity
and flexibility. This strategy is also supported by studies that have found faculty considered the
most successful by students when they possessed attributes such as enthusiasm, flexibility, a
sense of humor, approachability, and respectfulness (Penn et al., 2008). Key to promoting a
positive learning environment is the fostering of collegial working relationships with the

CLINICAL PRACTICUM 17
personnel in the clinical learning environment (NLN, 2012; Gaberson & Oermann, 2010). Thus,
Ms. Hresko and I had several discussions with preceptors, unit educators, unit managers, and unit
coordinators in order to keep communication open and foster trusting relationships with staff
members.
Clinical Project
The fourth competency for the nurse educator, or the ability to participate in curriculum
design and evaluate program outcomes, should reflect today’s health care and educate graduates
to be effective nurses in the modern day health care milieu (NLN, 2012). In light of current
health care trends such as the increasing critical nature of patient illness, increasing emphasis on
high quality care, and decreased spending, it is important for curriculum to keep pace (Boland,
2012). In order to help accomplish the goal of developing competency in curriculum design and
evaluation of program outcomes, I originally planned to develop two didactic lessons that could
be incorporated into the critical care internship program. However, after developing the first
lesson, outlined in the following section, the opportunity to develop a program syllabus became a
second clinical project.
Clinical Project 1: Lesson Plan
After careful consideration of learning needs as previously discussed, Ms. Hresko
suggested I plan a simulation activity focused on how to conduct a proper physical assessment
and the differences encountered on the critical care patient. This learning topic was one Ms.
Hresko had identified as an area for potential growth based on feedback from preceptors and
interns in previous classes. In addition, according to Gaberson and Oermann (2010), clinical
instructors are responsible for assessing the level of skill development prior to entrance in to the
clinical setting. Thus, utilization of simulation settings or skills labs can provide this opportunity

CLINICAL PRACTICUM 18
before being expected to do so in a fast-paced, demanding environment like critical care
(Gaberson & Oermann, 2010). Once a time and date were established, I coordinated the
reservations for the simulation lab where the learning activity would take place. I also obtained
materials to help in not only designing the simulation activity, but also in evaluation of the
activity and learning outcomes. I utilized a teaching outline the staff development and
simulation coordinator sent to me, in order to begin writing the teaching plan for the simulation.
This project utilized adult learning theory as well as evidence based practice for
developing lesson plans, needs assessments and learning objectives. According to Knowles
(1980) theory of adult learning, adults prefer learning that is practical, promotes self-esteem,
utilizes past experiences, demonstrates respect and allows self-direction, and synthesizes new
ideas with previous knowledge. In looking at the development of a teaching lesson for
simulation, I first focused on the objectives, outcomes, and competencies of what the desired
outcome was for the simulation activity (see Appendix B). Identification of the learners and
their level of expertise, including knowledge gaps, was an essential step in creating the learning
activity with adult learning theory in mind. According to Billings (2012), each lesson should
state the purpose, outcomes, assignments, learning activities, and evaluation being used. Since
the identified learning gap was performing a physical assessment on a critically ill, hospitalized
patient, the learning outcomes focused on improving clinical performance and self-confidence.
The introduction of the critically ill patient in the simulation lab, early in the orientation
period, was felt to be a safe and less threatening way of learning how to perform a complete
physical assessment and become familiar with some of the equipment that would be seen
throughout the orientation period. In addition, the design of this activity considered potential
past knowledge with a plan to integrate new knowledge related to critical care, as adult learning
CLINICAL PRACTICUM 19
theory suggests. According to Jeffries and Clochesy (2012), simulation can provide a safe
environment conducive to learning skills that require practicing a number of times. The learning
outcomes and placement of this particular simulation learning activity at the beginning of critical
care orientation was also in line with the idea that learning activities should build from level to
level and be threaded throughout the course as they fit with the program outcomes (Billings,
2012). Moreover, the simulation activity could assist with a more effective method of measuring
the skill and level of comfort the interns possessed before allowing them on the critical care units
(Billings, 2012).
The last stage in developing the lesson plan was determining evaluation methods.
According to Saunders (2003), this should be a twofold evaluation, considering evaluation of
learning or outcomes and evaluation of the instruction or the process. Primary strategies for
evaluating and measuring learning in a clinical setting is through observation, written
communication, oral communication, simulation, and self-evaluation (Bonnel, 2012).
Accordingly, Bonnel (2012) notes the importance of creating a checklist of behaviors and skills
to be observed during the simulation or performance so the potential for direct visualization and
confirmation of student performance is easier to evaluate. In working on the competencies and
evaluation for the simulation activity MMC’s intranet and information from the Lippincott
reference manual were utilized. Thus, organizational and nursing standards were followed and
considered throughout the development of this activity. Since structured observational tools can
contribute to a more objective and fair evaluation, I created an evaluation checklist based on
information from the previously mentioned sources. An analysis of the evaluations for this
project will be discussed further in the evaluation section of this paper.

CLINICAL PRACTICUM 20
Clinical Project 2: Program Syllabus
Prior to the start of the critical care internship on March 13, I learned that there was no
program syllabus. A syllabus can be seen as an important component to student understanding
of what is expected of them throughout a course. According to Sauter, Nightingale Gillespie,
and Knepp (2012), the syllabus can also be used during review of instructors and effectiveness in
teaching. Furthermore, the syllabus should be reviewed for expectations that are clear and
evaluation methods that are detailed. I found that Ms. Hresko did have written program goals
but there was really nothing formal, written, and given out to the interns that described all the
things that a normal program syllabus would contain.
Since I was still working toward gaining experience in the competency of curriculum
design and evaluation of program outcomes, I believed working on the components of a program
syllabus and putting them all together would provide me with additional growth in this area.
According to Billings (2012), the syllabus sets the tone for the course and should start off by
being written in a welcoming style. In addition she says a title, purpose, description,
prerequisites, corequisites, outcomes, teaching-learning strategies, learning activities, topical
outline, policies and procedures, assessment and evaluation strategies, as well as the grading plan
should be standard and essential components in a syllabus. Keeping this information in mind
and the difference between creating the program’s syllabus I needed to create for the internship
to one that would be created for an academic course, I set out to the task of creating a program
syllabus (see Appendix C). In doing this, I also had to email the electrocardiogram class
instructor and request course information to add to the syllabus about this program component.
The first step to creating the internship syllabus was to figure out the course outcomes.
Although, my preceptor had already created some broader program objectives, I felt the syllabus

CLINICAL PRACTICUM 21
needed to have more specific intern learning outcomes. Objectives and outcomes specify what
students should know, do, value, and determine how they will be graded (Billings, 2012).
Dillard and Siktberg (2012) also note that objectives and outcomes provide the framework for
the curriculum. In addition, learning activities and course objectives should focus on the three
main domains of learning, the cognitive, affective, and psychomotor domain. By matching
objectives with learning activities students are better able to make connections between what the
content is and why it is important, thus, promoting learning. One resource I utilized for this
component was the American Association of Critical-Care Nurse’s website for information about
the learning objectives related to the online modules that the internship utilizes for didactic
learning. According to Dillard and Siktberg (2012), one way to demonstrate that learning
objectives match the assignments is to use an evaluation grid or matrix. Therefore, I did create a
grid to demonstrate how the learning objectives would be assessed. One observation noted after
creating the grid was that in looking at all the various learning activities utilized in the internship
program, there was a great mix of active and passive learning approaches.
Evaluation
According to Saunders (2003), instructional evaluation can be done formally or
informally. Informal examples could include remarks from learners during the class session.
Thus, the evaluation of the first clinical project, the simulation activity, was completed using
both of these methods. Informal examples included remarks from the group during the
simulation activity. Comments made by the interns during the simulation activity itself were
very positive. In addition, the interns were all very engaged throughout the learning session,
each taking on the role of the nurse performing the physical assessment. An evaluation form for
the simulation learning activity was also created (see Appendix D). The beginning of the

CLINICAL PRACTICUM 22
evaluation form was created based on the learning objectives for the simulation. It has been
shown that student ratings are considered highly reliable as well as positively correlated with
student achievement, however, there remains challenges with the validity and reliability of the
instrument used to evaluate teaching effectiveness (Hayes, 2011).
The rest of the evaluation form utilized for the simulation activity was a standard form
created and used by MMC for the simulation lab. The evaluation consisted of a Likert five point
scale, asking the learner to rate how they felt about various evaluation criteria. Likert scales are
the most widely used scaling technique (Polit & Beck, 2012). A Likert scale allows the
evaluator the opportunity to express an opinion on a particular issue through indicating the
degree to which they agree or disagree (Bourke & Ihrke, 2012). Overall, each of the intern’s
evaluations reflected strong, positive feelings towards the learning activity. All responses were
marked “strongly agree” related to their feeling of whether or not they were able to achieve the
learning objectives for the activity. In addition, one of the comments made on the evaluation
noted that hands on learning was a preferred learning method. Lastly, no remarks were made on
the evaluations suggesting recommendations for future simulations.
An evaluation tool was also created as a means of assessing how well the goals for the
entire practicum were met (see Appendix E). The evaluation was completed by myself and Ms.
Hresko. The evaluations were based on the standards of practices for the academic nurse
educator as outlined by the NLN (2012). Both of these evaluations also utilized a Likert five
point scale. Overall, I believe this was a successful practicum experience. Significant
experience was gained in not only the specified areas outlined on the evaluation, but also in
learning more about the nurse educator and NPD specialist roles related to leadership and change
in an organization. Ms. Hresko’s evaluation was also highly rated.

CLINICAL PRACTICUM 23
Formal evaluation forms administered to students are often used by institutions at the end
of a course in order to solicit feedback on various criteria and are another way to receive
feedback (Saunders, 2003). Thus, at the end of this practicum I created an evaluation form that
once again utilized a Likert five point scale (see Appendix F). The evaluation form was given to
the interns on April 25, 2014 by Ms. Hresko when I was not present. The evaluations were
collected and given back to me by Ms. Hresko in order to provide the interns with an opportunity
to submit the evaluations anonymously. Evaluations from the interns were overall very positive.
On each of the 21 questions, all interns rated me as “excellent”, which was at the top of the scale
provided. Additional comments provided were also positive in nature. Lastly, in telling the
interns that I would not be working with them anymore, I received several informal comments
that they were going to miss me and that they were really grateful for my help.
Conclusion
Obtaining experience and knowledge in the educational process is an important goal in
the development of the academic nurse educator and NPD specialist roles. Competency in the
educational process can be gained through the utilization of a practicum experience. This paper
described a practicum experience designed to expand competency related to the educational
process utilized by both of these roles. Kolb’s experiential learning theory was described as the
foundation for the practicum experience. Challenges encountered in implementing these roles as
well as the strategies applied to meet these challenges were also detailed. Lastly, this paper
described and analyzed the clinical projects undertaken during the practicum and provided an
evaluation of the practicum experience.
CLINICAL PRACTICUM 24
References
American Nurses Association and National Nursing Staff Development Organization [ANA &
NNSDO]. (2010). Nursing professional development: Scope and standards of practice.
Silver Spring, MD: Nursesbooks.org.
Avillion, A., Brunt, B., & Ferrell, M. J. (2007). Nursing professional development: Nursing
review and resource manual (1st ed.). Silver Spring, MD: American Nurses Credentialing
Center.
Boland, D. (2012). Developing curriculum: Frameworks, outcomes, and competencies. In D.
Billings & J. Halstead (Eds.), Teaching in nursing: A guide for faculty (4th ed.). (pp. 138-
159). St. Louis, MO: Elsevier Saunders.
Bonnel, W. (2012). Clinical performance evaluation. In D. Billings & J. Halstead (Eds.),
Teaching in nursing: A guide for faculty (4th ed.). (pp. 485-502). St. Louis, MO: Elsevier
Saunders.
Bourke, M. P. & Ihrke, B. A. (2012). The evaluation process: An overview. In D. Billings & J.
Halstead (Eds.), Teaching in nursing: A guide for faculty (4th ed.). (pp. 422-440). St.
Louis, MO: Elsevier Saunders.
Brunt, B. A. (2007). Competencies for staff educators: Tools to evaluate and enhance nursing
professional development. Danvers, MA: HCPro, Inc.
Gaberson, K. & Oermann, M. (2010). Clinical teaching strategies in nursing (3rd ed.). NY:
Springer Publishing Company.
Hayes, J. (2011). Student evaluation of teaching. In M. Bradshaw & A. Lowenstein (Eds.),
Innovative teaching strategies in nursing and related health professions (5th ed.). (pp.
563-574). Sudbury, MA: Jones & Bartlett Publishers.

CLINICAL PRACTICUM 25
Jeffries, P. R. & Clochesy, J. M. (2012). Clinical simulations: An experiential, student-centered
pedagogical approach. In D. Billings & J. Halstead (Eds.), Teaching in nursing: A guide
for faculty (4th ed.). (pp. 352-368). St. Louis, MO: Elsevier Saunders.
Knowles, M.S. (1980). The modern practice of adult learning. Chicago, IL: Follett.
Kolb, D. (1984). Experiential learning: Experience as the source of learning and development.
Englewood Cliffs, NJ: Prentice Hall. Retrieved from
http://academic.regis.edu/ed205/kolb.pdf
McDonald, P. (2009). Transitioning from clinical practice to nursing faculty: Lessons learned.
Journal of Nursing Education, 49(3), 126-131. doi:10.3928/01484834-20091022-02
McKinley, M. (2008). Walking on water and other lessons learned as a clinical educator. AACN
Advanced Critical Care, 19(4), 388-395.
National League for Nursing [NLN]. (2012). The scope of practice for academic nurse educators
2012 revision. NY: author.
Penn, B., Wilson, L., & Rosseter, R. (2008). Transitioning from nursing practice to a teaching
role. OJIN: The Online Journal of Issues in Nursing, 13(3), 1-14.
Polit, D. F. & Beck, C. T. (2012). Nursing research: Generating and assessing evidence for
nursing practice (9th ed.). Philadelphia, PA: Lippincott Williams & Wilkins.
Saunders, R. (2003). Constructing a lesson plan. Journal for Nurses in Staff Development, 19(2),
70-80.
Schoening, A. M. (2013). From bedside to classroom: The nurse educator transition model.
Nursing Educator Research, 34(3), 167-172.
CLINICAL PRACTICUM 26
Shellenbarger, T. & Edwards, T. (2012). Nurse educator simulation: Preparing faculty for
clinical nurse educator roles. Clinical Simulation in Nursing, 8(6), 249-255.
doi:10.1016/j.ecns.2010.12.006
Stokes, L. G. & Kost, G. C. (2012). Teaching in the clinical setting. In D. Billings & J. Halstead
(Eds.), Teaching in nursing: A guide for faculty (4th ed.). (pp. 311-334). St. Louis, MO:
Elsevier Saunders.
Toth, J. (2008). The basic knowledge assessment tool, version eight (BKAT-8): For adult critical
care nursing. Retrieved from http://www.bkat-toth.org/BKAT-8.html.
Ullrich, S. & Haffer, A. (2009). Precepting in nursing: Developing an effective workforce.
Sudbury, MA: Jones and Bartlett Publishers.

CLINICAL PRACTICUM 27
Appendix A
Project Planning Guide
Title of Project: Practicum Proposal for Nurse Educator or NPD Specialist
Goals Objectives Activities TimelineGoal 1:Develop knowledge and experience in the standards of practice for both the education domain of the advanced specialty role of the NPD specialist and competencies I – Facilitate Learning & III – Use Assessment & Evaluation Strategies for the advanced specialty role of the nurse educator (ANA & NNSDO, 2010; NLN, 2012)
1.1Orient to the clinical educator/staff development role at MMC through multiple observation experiences focused on facilitation of learning and the use of assessment and evaluation strategies
1.2Use reflective observation to gain knowledge in facilitation of learning techniques and evaluation strategies
1.1aObserve preceptor facilitation in one role transition class & review class evaluations
1.1bParticipate in interviews and selection process of candidates for internship program
1.1cObserve facilitator and preparation of EKG course for new nurses
1.1dShadow preceptor and her interactions, facilitation of learning, and use of assessment and evaluation techniques with the interns, unit educators, and managers
1.1eMeet with preceptor and interns during any scheduled learning sessions
1.2aEngage in weekly to bi-weekly reflection and journaling of experiences
1.2bMeet regularly with preceptor to discuss, evaluate, and plan experiences for professional growth
1.1aJan. 16
1.1bJanuary
1.1cFeb. 20, 27, Mar. 6, Mar. 13, Mar. 20
1.1dMar. 10 – May 2
1.1eInternship starts Mar. 10
1.2aJan. 13- May 2, 2014
1.2bJan. 13-May 2, 2014

CLINICAL PRACTICUM 28
1.3Take on an active role as a facilitator of learning in the clinical setting
1.4Implement assessment and evaluation strategies into active facilitation experiences
1.5Use simulation technology for facilitation of learning in at least one lab session
1.3aHelp preceptor with preparation for start of internship program (preparing program materials, schedules, coordination with unit educators/managers)
1.3bTeach stations at skills labs
1.3cParticipate as facilitator in transition classes
1.3dSelect meetings with interns and preceptor to focus the planning and leading of
1.3eFacilitate agreed upon topics in March EKG course
1.4aUse evaluation strategies and review outcomes from facilitation at skills labs
1.4bUse evaluation strategies and review outcomes from facilitation in role transition classes
1.5aAttend 4 hour simulation operator class
1.5bAttend 4 hour simulation
1.3aJan. 13- Mar. 9
1.3bFeb. 26 & Mar. 20
1.3cFeb., Mar., Apr. (1 day month for 3 hrs.)
1.3dSelect 1-2 Fridays in April
1.3eMar. 27, Apr. 10, Apr. 17, Apr. 24, May 1
1.4aFebruary 26& March 20
1.4bFeb., Mar., Apr. (1 day month for 3 hrs.)
1.5aBy end of February
1.5bBy end of

CLINICAL PRACTICUM 29
Goal 2:Gain knowledge and experience in the NLN (2012) nurse educator competency IV – Participation in Curriculum Design and Evaluation of Program Outcomes
2.1Implement at least two didactic lessons into existing educational materials for the critical care interns
facilitator class
1.5cFacilitate simulation scenario(s) at skills lab(s) and with interns, use debriefing and evaluation strategies
2.1aMeet with preceptor to determine gaps in program learning outcomes
2.1bCreate an outline of education needs
2.1cReview the literature on topics that need additional educational facilitation of learning
2.1dRevise curricula and write learning objectives and select appropriate learning activities to fulfill needs
2.1eDetermine and implement evaluation strategies appropriate to the interns and learning goals for new curricula
February
1.5cApril 30 & various date(s) once internship program starts in March
2.1aJan. 13 – Jan 27
2.1bJan.27 – Feb. 10
2.1cFeb. 10 – Feb. 17
2.1dFeb. 17 – Mar. 3
2.1eMar. 3 – Mar. 10
CLINICAL PRACTICUM 30
Appendix B
Clinical Project 1
High-fidelity Simulation Case Planning
Munson Medical Center
Scenario name: Critical Care Physical Assessment Simulation
Estimated scenario run time: 20 minutes each intern
Estimated debriefing time: 40 minutes
Target audience: Critical Care Interns
Location of simulation: Simulation Lab
Learning gap: Physical assessment of critically ill hospitalized patient
What outcome/s are you measuring?
Clinical performance
Self-confidence
Brief overview: Fran York is a 75-year-old Caucasian female that lives alone. Her husband Jack passed away a year ago. She has a cat, Pumpkin, who is very important to her. Fran has one daughter, Phoebe Miller, who is 52, lives nearby, and is Fran's major support system.
Her current medical problems include: hypertension, atrial fibrillation, glaucoma, osteoarthritis of the knee, stress incontinence, osteoporosis, and hypercholesterolemia.
Fran is taking several anti-hypertensive medications, diuretics, Coumadin, and analgesics.
She was admitted to the hospital last night with a diagnosis of urinary tract infection, dehydration, and change in mental status.
The scenario takes place at 7:00 AM shift change. Fran has been in her room on A2 for about six hours. Due to her confusion, Fran did not take her medications properly in the

CLINICAL PRACTICUM 31
days prior to admission and as a result, her blood pressure is very elevated. Fran's daughter, Phoebe is at the bedside and is quite concerned about the confusion and elevated blood pressure.
The learner receives handoff report from the previous nurse and is expected to perform and document a general assessment.
Learning objectives:
At the end of the simulation, the participant will be able to:
Perform a complete systematic head to toe assessment of a simulated patient.
Identify major alterations in assessment findings: elevated blood pressure, confusion, rhonchi, murmur
- Evaluate the data
Respect and maintain patient privacy within the context of the examination.
Implement patient safety standards throughout the assessment.
Communicate clearly to patient, family member and all members of the healthcare team.
Simulation outcome checklist
(Lippincott skills checklist, ACLS, NRP or other
See attached
Monitor Layout List parameters that you want to show:
Initially just the ECG, once student assesses then add as they assess the BP, temp, SpO2
Patient Description
Name
Age
Weight and Height
Gender
Fran York
75 years old
48 kg, 61 inches
Female
History of present complaint Fran’s daughter became concerned yesterday when she stopped over to check on her and found her still in her

CLINICAL PRACTICUM 32
bathrobe at 3:00 PM. The house was very unkempt, and Fran couldn’t remember her daughter’s name. Fran was brought to the emergency department by her daughter and she was admitted to A2 around midnight. U/A, CBC, and basic metabolic panel labs have been completed and sent to the lab. Results are available.
Setting A2 - Acute care hospital unit
Patient Info:
History, Meds, Allergies and
Physician/s
Religion: Lutheran
Emergency Contact: Phoebe (daughter). Phone: 555-1210
Allergies: No known allergies
Immunizations: Influenza & pneumonia
(2 years ago)
Attending Physician/Team:
Dr. Yost
Past Medical History: Glaucoma, hypertension, atrial fibrillation, osteoarthritis, stress incontinence, hypercholesterolemia
Social History: Widow for one year; involved in church activities and gardening. Daughter and grandchildren live nearby.
Primary Medical Diagnosis: Dehydration; UTI
Surgeries/Procedures & Dates: Cholecystectomy at age 30

CLINICAL PRACTICUM 33
Show this information on the monitor before starting the simulation.
Initially just the ECG, once student assesses then add as they assess the BP, temp, SpO2
Make this information available throughout the simulation.
Significant Lab Values:
Urine Analysis:
Color: dark amber, cloudy
Specific gravity: 1.050 (normal 1.005-1.035)
ph 6.0 (normal 4.5-8.0)
RBC - 9 (normal 0-2)
WBC - 150,000 (normal 0-5)
Basic Metabolic Panel
Na - 149
K - 3.5
Glucose - 105
CBC
H/H - 9.9/32 WBC 12,000
Physician Orders:
Bedrest
Bathroom privileges with assistance
Regular, low fat diet
I & 0
Home Medications:
captopril, metoprolol, furosemide, Coumadin, Lipitor,

CLINICAL PRACTICUM 34
pilocarpine eye drops, Fosamax, Celebrex, Tramodol for arthritis pain prn
Continue home medications and add:
ciprofloxacin 200 mg IV q 12 hours
acetaminophen prn
IV fluids D5 .45 NaCl 20 mEq KCL at 60ml/hr
List equipment needed:
A. SimMan and equipment & SimMan 3G and equipmentB. Ventilator (not used in the simulation but will be used after)C. Central lineD. TelemetryE. WoundF. Chest tube G. Stage I pressure ulcerH. FoleyI. IV pole, pump, with IV solutions, bags with expiration datesJ. Computer with Powerchart training modeK. Checklist for evaluationL. Facilitator cards
Prep of the simulator:
I. Content outline
A. Introduce students to expectations of simulationa. Treat SimMan as you would a real patient.
i. Manikin talks (unless vented), blinks, has pulses, heart sounds, breath sounds, etc.
b. Student learning objectives include:i. Conduct a head-to-toe assessment of the patient
ii. Identify critical assessment findings (will be outlined on outcome checklist)
iii. Evaluate patient dataiv. Use SBAR techniques when communicating with other members of
the health care teamv. Document patient assessment
c. Facilitator will be a family member and observe, will be given a role cardd. Facilitator can answer questions about what manikin can do.e. After the simulation you will be charting your assessment in Powerchartf. At the end, the team will debrief.

CLINICAL PRACTICUM 35
B. Intro. To SimMana. Capabilities: pulse oxygen can be applied, take BPb. Gather all of your assessment data is if it was a real live patientc. Check IV and medications
C. Simulationa. Physical Assessment on non-vented pt with SimMan software
i. Receive report1. FY is a 75-year-old female admitted from home with
confusion. Her daughter noticed she wasn’t making sense or acting right when she stopped in to visit her yesterday evening. Her daughter brought her in to the ED yesterday afternoon; she was in the ED until about midnight. FY has a history of hypertension, atrial fibrillation, glaucoma, osteoporosis, arthritis, elevated cholesterol, and stress incontinence. It is unclear whether she has taken her medications properly the past few days, her daughter couldn't tell from looking at her medication box. Labs just came back, I haven’t had a chance to look at them. She has medications ordered, but they just came up from pharmacy and they all need to be given. She has not had any pain.
Number of roles and participants per scenario: 2
Primary nurse - Intern Family member - Facilitator
Timing Patient Patient/Manikin Student Cue/Prompt What

CLINICAL PRACTICUM 36
(approximate) and
Frame Name
Monitor Settings
(Actions)
(Actions) Expected Interventions
(Events)
advances frame to next frame?
Initial:
0-5 minutes
Initial State:
Vital Signs
Only initial display is heart rhythm/rate (pt is on a tele monitored floor)
Once interns takes vitals then display BP, spO2, temp
BP 180/110, P – 100, A-fib
R – 25 (do not display, want to check accuracy of intern’s assessment); T - 98.4
Vocal Sounds:
“My daughter dropped me off and left me here. I’m not quite sure where I am or why I’m here. I feel ok. I can’t believe how my life has changed in the past couple of weeks now. Howard died a couple of weeks, no months ago. I can’t remember. Why can’t I remember? Things have changed. I don’t like that; I’ve always been a strong woman. I feel ok and I take a lot of pills – not sure what they all are you can look on the kitchen counter or ask my daughter what they are. Where is Phoebe? I haven’t seen her in 6 years; no one ever comes to see me.”
Heart, lung
Wash hands
Introduce self
Identify patient
Take vital signs
Begins head-to-toe assessment
Role member providing cue:
Daughter
Cue: “I don't think she's been taking her medicine.”

CLINICAL PRACTICUM 37
sounds etc.
Murmur
Rhonchi
5-10 minutes
Complains of headache
“Has anyone checked on Pumpkin lately?"
Continues assessment
Notice elevated BP
Role member providing cue:
Daughter – 7-8 minutes into scenario
Cue: “Isn’t her blood pressure too high?”
10-20 minutes
(If student asks about medications)
“I don't remember when I took my Lopressor last.” Continues to complains of headache
Calls Dr. Yost to notify of BP using SBAR communication tool
Completes physical assessment
Role member providing cue:
Dr. Yost
Cue:
“Has she taken her antihypertensive? I’ll be there shortly”
Debriefing outline/questions:
A. What do you think went well?B. How did you feel throughout the simulation experience?C. Did you have the knowledge and skills to meet objectives?D. What were the key assessment findings and interventions?E. What would you do differently if we repeated the simulation?F. How can you apply this to your clinical practice?G. Differences in assessment techniques with a vented pt.
a. Demonstrate on other manikin H. Discuss areas for improvement.
Physical Assessment Evaluation Criteria

CLINICAL PRACTICUM 38
GeneralGather appropriate equipmentPerforms hand hygienePuts on gloves, if necessaryIntroduce selfIdentify the ptProvide privacy and maintain pt dignityExplain your purposeChecks patient concerns (chief complaint) prior to start of assessmentPhysical environment (temp, cleanliness, equipment in use or in room)
Inspection - using senses of vision, smell, and hearing to observe condition of various body parts, including any deviations from normal
Visually surveys the patient (details of appearance, overall condition, body habitus)Makes sure body area being inspected is sufficiently exposed and adequately lit, noting overall condition, color, shape, texture, odor, sound, and sizeLOCDisposition (facial expressions, mood, behavior)Note tubes, drains, IV's, etc. (include amount, color, odor, etc.)Always looks before touchingPerforms Vital Signs
Palpation - touching and feeling body parts with hands to determine the following characteristics
Texture (roughness, smoothness)Temperature (warm/hot/cold)Moisture (dry/wet/moist)Motion (stillness/vibration)Consistency of structures (solid/fluid filled)Tender areas are palpated last
Auscultation - Listening for various breath, heart, vasculature, and bowel sounds using a stethoscope
LungsHeartBowelsVasculature
Additional ConsiderationsProvide opportunity for patient to ask questions, express concerns, etc.Pt bed in lowest position once completeLock bed wheels if necessaryCall light within reach and pt is aware of how to useBedside table and personal items are within reachPerforms appropriate documentation of nursing assessment
References:

CLINICAL PRACTICUM 39
Lippincott Procedures – Assessment techniques, Ventilator management; Lippincott Skills Checklist – Assessment techniques, Cardiac Assessment
Weber, J. (2010). Nurses’ handbook of health assessment (7th ed.). Philadelphia, PA: Lippincott Williams & Wilkins
Appendix C

CLINICAL PRACTICUM 40
Clinical Project 2
Critical Care Internship Program
Program Description
The purpose of the Critical care Internship program is to provide the novice nurse with the essential foundation to safely care for patients and their families with in the critical care environment. The program consists of five months of clinical and didactic training.
Program Objectives
1. Provide a consistent approach for critical care orientation.2. Reduce nurse turnover and attrition in the critical care units.3. Establish a supportive environment to promote nurse maturation, acceptance and
successful transition from academia to the RN role.4. Provide a sustained approach for addressing the critical care shortage and current
vacancy rates.5. Attract new critical care recruits through an internship-marketing program.6. Promote overall job satisfaction for program participants and existing staff.7. Foster an educational environment that supports critical thinking and evidenced
based practice.8. Maintain AACN practice standards and healthy work environment
initiatives.9. Endorse Relationship Based Care principles.10. Establish preceptoring and mentoring role components to support skill acquisition
and position integration.11. Facilitate competency through AACN’s ECCO module test scores, Skills lab
competencies, Simulation competencies, EKG class exercises, blended learning activities, self-evaluation, and unit Educator, preceptor and program coordinator evaluations.
12. Provide safe, quality, critical care to fulfill the community need.
Program Teaching Strategies
Clinical Practicum with Preceptor(s) Computer based modules via Essentials of Critical Care Orientation (ECCO) by the
American Association of Critical-Care Nurses (AACN) Hands-on Skills Labs High Fidelity Simulation Articles

CLINICAL PRACTICUM 41
Basic ECG Interpretation Classroom Course Case Studies/Clinical Reasoning Activities Guided Self-Reflection Conferences/Face-to-Face Meetings
Program Schedule
Please see the program calendar for information on specific dates of required labs, classes, meeting times, etc. Interns will be notified of changes to the schedule via email. It is the intern’s responsibility to check his/her outlook email to be aware of schedule changes.
Program Coordinator Information
Patti Hresko, MSN, RN, CCRN Critical Care Internship Coordinator Office: South One (Offices past payroll)Phone: O: (231) 392-0193 H: (231) 264-9193 C: (231) [email protected] method of contact: Email
Participating Clinical Units
Emergency Department (ED)o Offers state-of-the-art design and technology with 43 private rooms,
including three full service trauma bays. Accredited through The American College of Surgeons as a Level II Trauma Center, the only one in northern Michigan.
o Manager: Kristi Johnsono Resource Clinician/Unit Educator: Rachel Blanchard
Intensive Care Unit (ICU)o 20-bed unit that serves a combined medical/surgical, trauma, and
neurological population. The Progressive Care Unit is housed in the ICU and is responsible for caring for a variety of patients with multisystem complexity.
o Manager: Jerry Hurono Resource Clinician/Unit Educator: Cathy Mowbry
Cardiothoracic Unit (A2)o 30-bed unit which encourages open visitation. The innovative acuity
adaptable rooms are designed to provide efficient care to cardiac surgical patients, immediately post-op until patient discharge.
o Manager: Eva Voisino Resource Clinician/Unit Educator: Jeanette Reynolds
Cardiac Care Unit (A3)o 30-bed unit in the Webber Heart Center is also acuity-adaptable. A3 serves a
patient population that includes adult cardiac critically ill and cardiac interventional patients.

CLINICAL PRACTICUM 42
o Manager: Lori Kirkeyo Resource Clinician/Unit Educator: Julie Bergsma
Program Materials
The following materials will be provided for you: Critical Care Internship binder with research articles and relevant critical care
nursing information ECCO skills lab book
Policies
You are accountable for your own learning which includes keeping track of changes to the program syllabus and calendar made by the coordinator and unit schedulers throughout the program.
It is the intern’s responsibility to contact the program coordinator with any issues, concerns, or questions related to the internship program.
The Internship covers a large amount of material. It is imperative to keep up with assigned ECCO modules. Professional conduct is expected at all times including dress code and social media policies. Please review Munson’s employee handbook.
Program Learning Outcomes
By the end of the internship program, the critical care intern will be able to:
1. Identify and implement evidence-based care strategies to prevent hospital-associated infections and complications.
2. Evaluate assessment data and develop a plan of care for patients with critical illness.
3. Understand basic hemodynamic monitoring concepts.4. Identify the clinical consequences of basic cardiac arrhythmias and choose
interventions that are appropriate for basic cardiac arrhythmias.5. Demonstrate knowledge of common conditions experienced by acutely ill patients
requiring critical care nursing. 6. Develop a treatment plan for patients experiencing critical illness.7. Evaluate the effectiveness of the treatment plan for patients experiencing critical
illness.8. Analyze and evaluate the role of the critical care nurse and seek to improve the
quality and effectiveness of nursing practice.Program Learning Activities & Assessment Methods
Assessment Activity Outcome(s) Due Date

CLINICAL PRACTICUM 43
Assessed
Clinical Competency Orientation Tool & Weekly Goal Sheets
1, 2, 3, 4, 5, 6, 7, 8 Weekly
Basic Knowledge Assessment Test (BKAT) 3, 5Start of internship & end of
internship
ECCO Module Exams 1, 2, 3, 5, 6, 76 modules must be completed
prior to skills labs, rest must be completed by end of internship
Skills Lab & Simulation Competency Tools 2, 3, 4, 5, 6, 7, 8 See course calendar
ECG Exam 4 May 1, 2014
Case Study Presentation 1, 2, 5, 6, 7, 8 End of internship
Case Studies/Clinical Reasoning Activities 1, 2, 3, 4, 5, 6, 7, 8 Throughout orientation program
Reflection Journals 8 Weekly
Description of Required Learning Activities
Clinical Practicum with Preceptor(s)A. Goal: To provide opportunities for the student to gain knowledge and participate in
patient care. B. Description: Upon completion of hospital orientation, the intern will rotate on each
of the four participating critical care units for approximately one week per unit. This is considered the familiarization period. After familiarization, the intern will be assigned to one of the critical care units. The intern will spend the next 4 months of their clinical practicum on their assigned unit to complete critical care orientation.
C. Objectivesa. During familiarization the critical care intern will:
i. Have an understanding of the various patient diagnoses treated on the participating critical care units
ii. Meet interdisciplinary team members on participating units.iii.
b. At the end of the clinical practicum the critical care intern will:i. Become aware of the various aspects of nursing care as an
interdisciplinary component of patient care. ii. Identify the operation of the department, i.e.
1. Duties and functions of the various personnel2. Equipment 3. Role-play with the interdisciplinary team using SBAR
Communication 4. Use information and patient care technology to communicate
effectively with members of the healthcare team

CLINICAL PRACTICUM 44
iii. Observe and/or assist with the use of treatments and therapeutic measures related to the department.
1. Administer and document administration of medications in the critical care environment
2. For assigned patients, compare observed practices with published standards.
iv. Identify the need for skills in assessment based on all body systems. 1. Perform patient assessment and evaluation of patient’s
response to pharmacological agents v. Identify the skills needed in patient and family teaching.
1. Address end-of-life decision making vi. Provide emotional support for the client, family members as needed.
1. Provide evidence-based, patient-centered end-of-life care to a dying patient and their significant others.
vii. Infection control 1. Reporting communicable diseases required 2. Universal Precautions
D. Evaluation: Clinical Competency Orientation Tool & Weekly Goal Sheets
Basic Knowledge Assessment Test (BKAT)A. The BKAT is a 90-item paper and pencil test that measures basic knowledge in
critical care nursing. These items measure content related to the following areas of critical care nursing practice: cardiovascular, pulmonary, monitoring lines, neurology, endocrine, renal, gastrointestinal/parenteral, infection control, hypothermia, burns, and spiritual care.
B. The BKAT will be taken once at the beginning of the internship program and once at the completion of the program to assess knowledge attainment.
ECCO Module ExamsA. ECCO is comprised of 10 critical care training modules; each containing multiple
lessons that provide in-depth, interactive content. Each module addresses the anatomy and physiology of a distinct body system, relevant diagnostic information and the clinical presentation and management of common disorders for each of the body systems.
B. A variety of media formats are used in the modules including: text, audio, video, animation, and tests.
C. Interns will be paid 62 hours of educational time for completion of the ECCO modules. Modules that correlate with the skills lab topics should be completed PRIOR to attending skills lab. All other modules are required to be completed by the end of the orientation program.
D. Module content includes:a. Introduction to Care of the Critically Illb. Care of the Patient with Cardiovascular Disordersc. Care of the Patient with Pulmonary Disordersd. Basic Hemodynamic Monitoringe. Care of the Patient with Neurological Disorders

CLINICAL PRACTICUM 45
f. Care of the Patient with Gastrointestinal Disordersg. Care of the Patient with Renal Disordersh. Care of the Patient with Endocrine Disordersi. Care of the Patient with Hematological Disordersj. Care of the Patient with Multisystem Disorders
ECCO Skills Labs, Simulation, & Case StudiesA. There will be four skills labs tailored for “hands-on” learning to take place over five
major content areas that correlate with ECCO learning modules including: cardiovascular, pulmonary, hemodynamics, and neuro/multisystem (neuro and multisystem are combined into one skills lab).
B. See ECCO skills lab description sheet on the next page for information about meeting locations, times, and topics covered for each of the four skills labs.
C. Simulation and unfolding case studies, as well as written case studies will be also be utilized throughout the orientation program. The purpose of these learning opportunities is to promote critical thinking, clinical reasoning, and adherence to internal and external standards of care. During simulation, the interns will often work together to care for a patient (simulated by a manikin) as a specified scenario unfolds. The intern is expected to fully engage and participate in the simulation session.
ECCO Skills Lab: January 2014 – April 2014All Skills Labs Are Located In Meeting Room 11 & 12
Time: 0800-1230 Pulmonary: Cardiovascular: Hemodynamics: Neuro & Multi-System:

CLINICAL PRACTICUM 46
May 28, 2014 June 25, 2014 July 30, 2014 April 30, 2014
Estimated pre-assignment completion time:
12.75 hours
ECCO modules which must be completed prior to attending skills lab:
Introduction to Critical Care Nursing (4.5)
Pulmonary (8.25)
o Respiratory distress & Intubation
o Ventilators/CPAP/ BiPAP
o Trach care & suctioning
o ABG’s
Estimated pre-assignment completion time:
15.5 hours
ECCO modules which must be completed prior to attending skills lab:
Cardiovascular (15.5)
o Cardiac assessmento Groin managemento Heart soundso Temporary
pacemakerso Permanent
pacemakerso Arterial lines
Estimated pre-assignment completion time:
12.75 hours
ECCO modules which must be completed prior to attending skills lab:
Hemodynamics (8.75)
PA Catheter Modules (4)
o PA Caths: Insertion & SVO2
o PA Caths: Waveforms and Trouble-Shooting
o PA Caths: Blood draws & Removal
o PA Caths: Cardiac Output
o Mega Codeo CVP
Estimated pre-assignment completion time:
13.25 hours
ECCO modules which must be completed prior to attending skills lab:
Neurologic (8.75) Multi-System (4.5)
o Neurological Assessment
o Multi-system/Sepsis Simulation
o Neuro Simulation/ICP
o Neuro Case Studieso Organ Donation
Clinical Experience:
Patient care with preceptor relevant to ECCO topics covered
Adjunct Learning Activities:
Policy/procedure review/case review (on unit)
Don’t forget to complete all other ECCO modules by the end of the internship program
Renal, GI, Endocrine, and HematologyBasic ECG Interpretation Course
A. Focus of Course Content: The content of the course will focus on basic ECG interpretation skills for cardiac monitoring that a nurse needs to utilize in the care of critically ill patients.

CLINICAL PRACTICUM 47
B. Hours and Length of Course: Basic ECG Interpretation classroom time occurs once a week for five weeks. The classroom time total is 9 hours. Class time per day varies according to the week. The education may have nursing contact hours. Participants will spend at least 6 hours outside of class reading, studying and completing homework.
C. Rationale of the Course: Most critically ill patients will be on a cardiac monitor. Cardiac monitoring takes place in areas like telemetry units, acute critical care, the emergency room, recovery room, outpatient and procedural areas, obstetric units, pediatric units and interventional radiology. Basic ECG interpretation is a valuable skill to have. This course provides the opportunity to practice and learn the skills of interpreting cardiac rhythms that will help the critically ill patient. Nurses need to take the interpretation in context with the patient, and make a decision for interventions and education.
D. Course Description: The Basic ECG Interpretation education is a blended learning experience. Students are expected to complete the assigned reading and review prior to each class. During the class time, an instructor will review the key points. Learning activities will include interpreting strips and case studies to strengthen concepts and skills.
E. Course Outcomes: At the completion of the Basic ECG Interpretation course, the participant will be able to:
a. Interpret basic cardiac rhythms using a standard process.b. Identify the clinical consequences of basic cardiac rhythms.c. Choose interventions that are appropriate for basic cardiac rhythms.d. Identify key points for patient education regarding basic cardiac rhythms and
their interventions. F. Course Delivery Method: This education will be presented weekly in a classroom
setting. The course provides an opportunity for the learner to practice and develop the basic ECG Interpretation skills needed in the critical care environment. This delivery format follows adult learning principles and experiential learning. The learning activities will engage visual, auditory, verbal, social and physical learners. The use of technology will engage the millennial generation.
G. Attendance Policy: Interns are expected to attend all sessions as this learning activity is required for their position in the critical care department. If an interns is ill or unable to attend, they must call the Basic ECG Interpretation course instructor and also the internship program coordinator. The session content will need to be completed either on the nursing unit with their preceptor or educator, or during the next cycle of Basic ECG Interpretation.
H. Course Instructors:a. Nancy Irish, MSN, RN-BC has taught Basic ECG Interpretation since 1997.
She has over 20 years of critical care experience in cardiac, surgical and emergency critical care. She also performed 12 lead ECGs and interpretation for home care cardiac patients. She graduated with an ADN from Northwestern Michigan College in 1979, a BSN from Ferris State University in 1993, and an MSN from Walden University in 2012. Email is the best method of contact: [email protected] or phone: 935-7275.

CLINICAL PRACTICUM 48
b. Debra Hart, MSN, BS, RN has been one of the primary and/or substitute teachers of Basic ECG Interpretation since 1988. She has over 15 years of cardiovascular patient care experience in acute and critical care settings. Deb graduated with an ADN from Northwestern Michigan College in 1974, a BS in Allied Health Education from Ferris State University in 1987, and an MSN from Walden University in 1012. Email is the best method of contact: [email protected] or phone: 935-6498.
I. Course Resources: a. Aehlert, B. (2013). ECG’s made easy (5th ed.). St. Louis: Mosby Year Book, Inc.b. Atwood, S., Stanton, C., & Storey-Davenport, J. (2009). Introduction to basic
cardiac dysrhythmias (4th ed.). China: Mosby Jems Elsevierc. Dubin, D. (2011) Rapid interpretation of ECG’s (6th ed.). Hong Kong:COVER
Inc.d. Wolters Kluwer, & Lippincott, Williams & Wilkins. (2011). ECG interpretation
made incredibly easy (5th ed.). Philadelphia: Wolters Kluwer/Lippincott, Williams & Wilkins.
e. Wolters Kluwer, & Lippincott, Williams & Wilkins. (2013, July 12) Cardiac Monitoring. Retrieved from http://procedures.lww.com/lnp/view.do?pId=656349&s=p&fromSearch=true&searchQuery=cardiac+monitoring
f. www.skillstat.com J. Special Requirements: Interns will need to borrow the “Basic ECG Interpretation
made Incredibly Easy,” 5th ed. book. This book can be signed out in Staff Development, Monday through Friday 0700-1630.
K. Please see the following Basic ECG Interpretation Schedule for details regarding class dates and times, expected learning to complete prior to class, class topics, and class locations.
L. Evaluationa. Participants must pass the written ECG exam with 84% and all mandatory
rhythms identified correctly.b. If participants score between 80-84% on the written ECG exam and have all
mandatory rhythms correctly identified, they must meet and review their exam with their unit educator. The unit educator will verify that they have passed the exam after the meeting.
c. If participants incorrectly identify a mandatory rhythm (VFib, VTach, AFib, Asystole and 3 degree AV block) and/or score less than 80%, they will need to do a retake exam, after they have practiced more.
d. An education activity evaluation will be administered at each class date and at the end of the course.
e. Learning outcomes will be measured via a brief online rhythm quiz at 3 months and 6 months after passing the written ECG exam.
Basic ECG Interpretation Schedule
Start Date: March 27th Schedule
CLINICAL PRACTICUM 49
Date Time Complete Prior to Class Class Topics Location
Day 1
ThursdayMarch 27
4:00-7:00 p.m.
Read chapters 1-4 prior to the 1st class, filling in the Sinus Node Arrhythmia note sheets as you read chapter 4. Complete all of the chapter quizzes.
A & P, Basic Interpretation, Sinus
Rhythms
14
Day 2
ThursdayApril 10
4:00–5:30 p.m. Read chapters 5 – 6,chapter quizzes,
and complete homework
Atrial and Junctional Rhythms
D6 meeting room 1
Day 3
ThursdayApril 17
4:00 – 5:30 p.m. Read chapters 7-8,chapter quizzes,
and complete homework
Ventricular Rhythms, and AV Blocks
14
Day 4
ThursdayApril 24
4:00-6:00 p.m. Read chapters 9 and 10,chapter quizzes,
and complete homework
Pacemakers, Interventions and Review
14
Day 5
ThursdayMay 1
4:00-5:00 p.m.Rhythm Review
1. Read “Brushing up on Interpretation Skills”
2. Read “Look Alike Challenge”
3. www.skillstat.com
Written Test 14
Case Study PresentationA. Objective: Presentation of an evolving case study appropriate for your peers.
Choose a Critical Care topic. Follow the format of the educational planning table worksheet on the following page to create your outline. Choose and/or develop
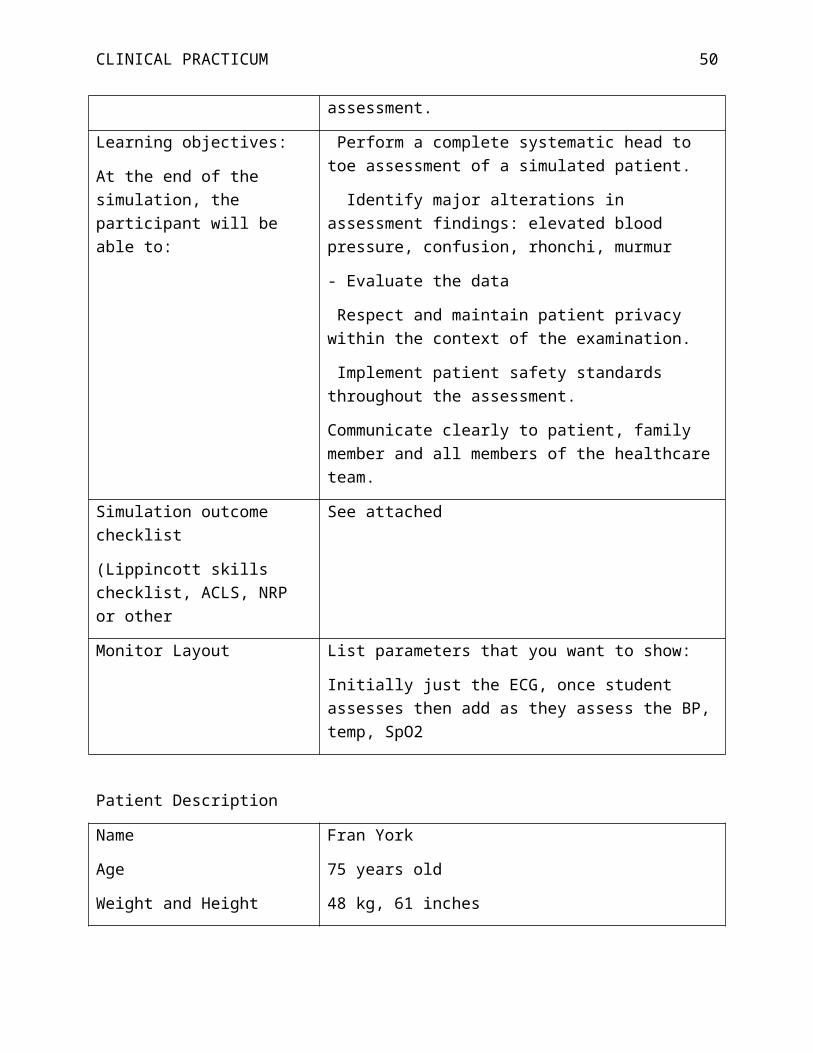
CLINICAL PRACTICUM 50
audiovisual aides for presentation of the case study. Review project with program coordinator prior to presentation. Deliver the presentation. Evaluate the effectiveness of the presentation.
B. Instructionsa. Each individual will select a topic of interest.b. Selected topic must be approved by program coordinator before you begin
working on the project. c. Develop evolving case study that shows progression of patient’s disease
process, with complications.d. Case study must be higher level learning geared toward nursing peers
utilizing Evidence Based Practice. Case study may include experiences on your particular clinical unit.
e. Presentation should be developed using the attached worksheet.f. Presentation should be scholarly, well researched utilizing current scholarly
journal articles, appropriate websites, and AV/media/PowerPoint.g. Time frame for each presentation is approximately 1 hour.h. A copy of the presentation worksheet should be emailed to
[email protected] by date on program calendar and must include references in APA format.
C. The presentation must include the following information:a. Introduction: Section consists of introducing/presenting the patient.
Required elements: Patient initials, date of birth, age, race and gender, current ht & wt, and date of admission.
i. Chief complaint: (why the pt came into the hospital) and primary admitting diagnosis.
ii. HPI: history of present illness (length of illness and signs and symptoms on admission). Provide a detailed course of illness and his or her present health state (are they better, worse or the same).
b. Overview of patient: History, bio-psycho-social assessments, diagnostic tests (and why they were ordered), pharmacological interventions (including reason it was prescribed, therapeutic effects expected, and adverse effects to monitor), EKG interpretation, hemodynamics, nutritional measures, and genomic considerations.
c. Pathophysiology: Review pathophysiology of the condition including etiologies, clinical manifestations, expected outcomes, current research, demographics, and relating this information to the assigned patient.
d. Plan of Carei. Part 1: Generate and discuss nursing diagnosis in planning care for
the patient. ii. Part 2: Priorities of care, plan, and evaluation of outcomes.
e. Research-based Interventions: Evaluate the care this patient received related to your research of the condition.
f. References: Cite all references used in the paper. The references must include at least one peer-reviewed journal article. The article must be less than 5 years old, and must be longer than 2 printed pages to count. Your
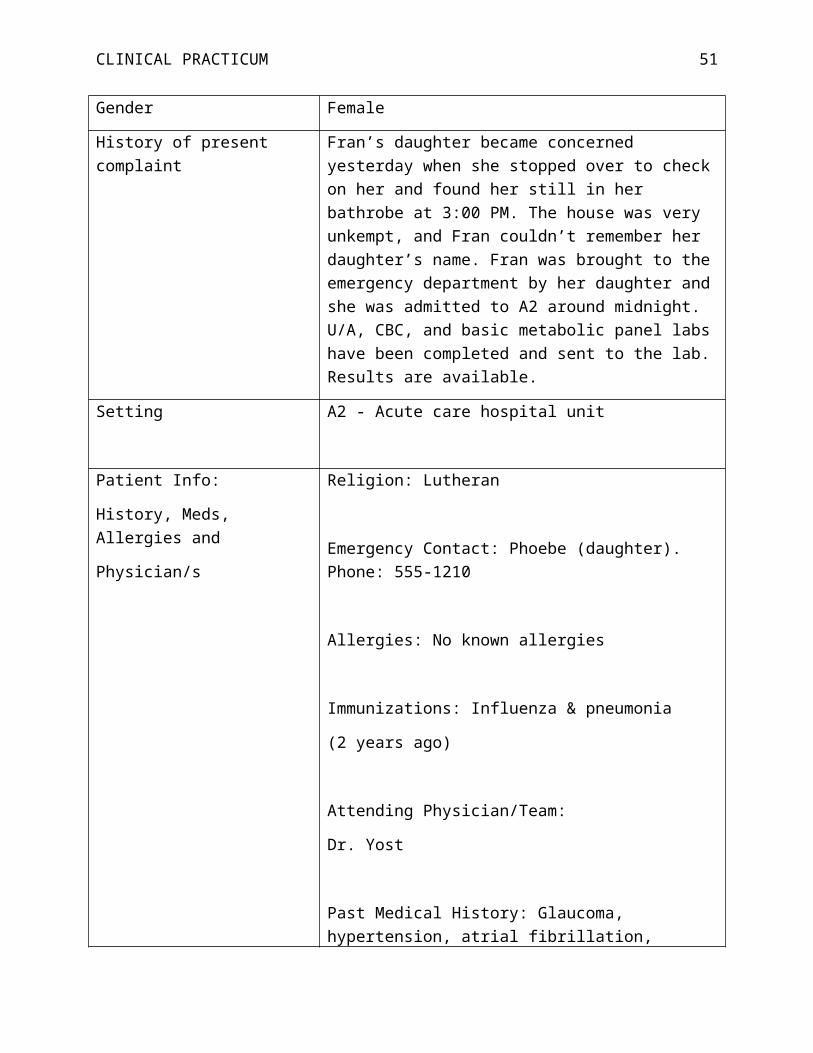
CLINICAL PRACTICUM 51
other references can be textbooks and internet sites. The reference section must follow APA 6th edition format
D. Evaluation of Presentationa. Please see rubric on the following page for evaluation criteria.

CLINICAL PRACTICUM 52
EDUCATIONAL PLANNING TABLELIVE EVENT
Educational Activity:
Purpose of Activity: To improve the knowledge of nurses caring for patients with cardiac tamponadeInstructions: Type directly into blank cells of the tables.
OBJECTIVESList learner’s objectives in behavioral terms. (After completing this activity, the learner will be able to…)
CONTENTProvide an outline of the content for each objective. It must be more than a restatement of the objective.
TIME FRAMEState the time frame for each objective.
PRESENTERList the faculty for each objective.
TEACHING METHODSList the teaching methods, strategies, materials & resources for each objective.

CLINICAL PRACTICUM 53
(Add more rows as needed by placing cursor outside of last row and clicking ‘Enter’ key.)
Total minutes for this activity/session (including time spent evaluating the activity) =List the evidence-based reference(s) used for developing the content of this educational activity/session next to the appropriate category.
Information from organization/website:(may be published or unpublished content. Examples – Centers for Disease Control, National Institutes of Health)
Peer –reviewed journal/resource:(reference should be within past 5-7 years)
Clinical guidelines:(published or online. Example -www.guidelines.gov)
Expert resource:(individual, organization, or educational institution - book, article, website)
Textbook reference:Other:

Running head: PRACTICUM PAPER 54
Case Study Presentation RubricBelow Expectations Needs Improvement Meets Expectations Exceptional Comments
Organization
Below Expectations Needs Improvement Meets Expectations Exceptional Comments
The presentation was not clearly organized and was difficult to follow.
There was no introduction or
conclusion.
The presentation was somewhat organized, but it
may be a little difficult to follow. The presentation
was missing an introduction or summary.
The presentation was organized, but clear
learning objectives and summary may be
missing. An introduction provided sufficient
background on topic and preview of major points.
The presentation was well organized with clear objectives, introduction
of topic and major points, and summary.
Content
Below Expectations Needs Improvement Meets Expectations Exceptional Comments
Presentation content lacks depth and breadth. Major points are unclear.
Objectives are incomplete and not clearly supported by appropriate sources.
Presentation content is somewhat developed.
Major points are somewhat clear. Objectives may not be complete and
may not be clearly supported by appropriate
sources.
Presentation content is developed. Major points
are stated clearly. Objectives are mostly
complete and supported by appropriate sources.
Presentation content is thoughtfully developed
and supported by appropriate and current sources (< 5 years unless
a classical resource). Major points are stated
clearly and supported by specific examples.
Subject Knowledge
Below Expectations Needs Improvement Meets Expectations Exceptional Comments
Presenter does not have grasp of information;
presenter cannot answer questions about subject.
Presenter is uncomfortable with information and is
able to answer only rudimentary questions.
Presenter is at ease with expected answers to all questions, but fails to
elaborate.
Presenter demonstrates knowledge by answering
questions with explanation.
Audio/Visual
Below Expectations Needs Improvement Meets Expectations Exceptional Comments
Presenter uses no audio/visual aids.
Presenter use audiovisual aids to read out the
material.
Presenter's A/V relates to text and presentation.
Presenter's A/V explains and reinforces topic and
presentation.
Eye Contact
Below Expectations Needs Improvement Meets Expectations Exceptional Comments
Presenter reads all of report with no eye
contact.
Presenter occasionally uses eye contact, but still reads
most of report.
Presenter maintains eye contact most of the time but frequently returns to
notes.
Presenter maintains eye contact with audience,
seldom returning to notes.
Elocution
Below Expectations Needs Improvement Meets Expectations Exceptional Comments
Presenter mumbles, incorrectly pronounces terms, and speaks too quietly for audience to
hear.
Presenter's voice is low. Presenter incorrectly pronounces terms.
Audience members have difficulty hearing
presentation.
Presenter's voice is clear. Presenter pronounces most words correctly.
Most audience members can hear presentation.
Presenter uses a clear voice and correct,
precise pronunciation of terms so that all
audience members can hear presentation.
Enthusiasm
Below Expectations Needs Improvement Meets Expectations Exceptional Comments
Shows absolutely no interest in topic
presented.
Showed some negativity toward topic presented.
Occasionally showed positive feelings about
the topic.
Demonstrated a strong positive feeling about
topic during entire presentation.
CreativityBelow Expectations Needs Improvement Meets Expectations Exceptional CommentsNo creativity/information
appears to be taken be directly from a book.
Lacks creativity. Shows some creativity. Creative.

PRACTICUM PAPER 55
Reflection JournalsA. Reflecting on one’s practice is considered an important part of the
learning process. Thus, each week interns will make a journal entry of observations, insights, and discoveries encountered that week. Personal reflections should be related to clinical tasks, activities, and/or experiences.
B. Examination of progress, identification of strengths and weaknesses, and goals for improvement should also be included in your journal entries.
C. Journals should be approximately one page in length. Please date each entry by the week and place all entries into one ongoing document.
D. Journals should be emailed to the program coordinator at the end of the intern’s clinical week.
Intern Evaluation of Program
Interns are provided the opportunity, and are strongly encouraged to participate in a program evaluation at the end of the internship.
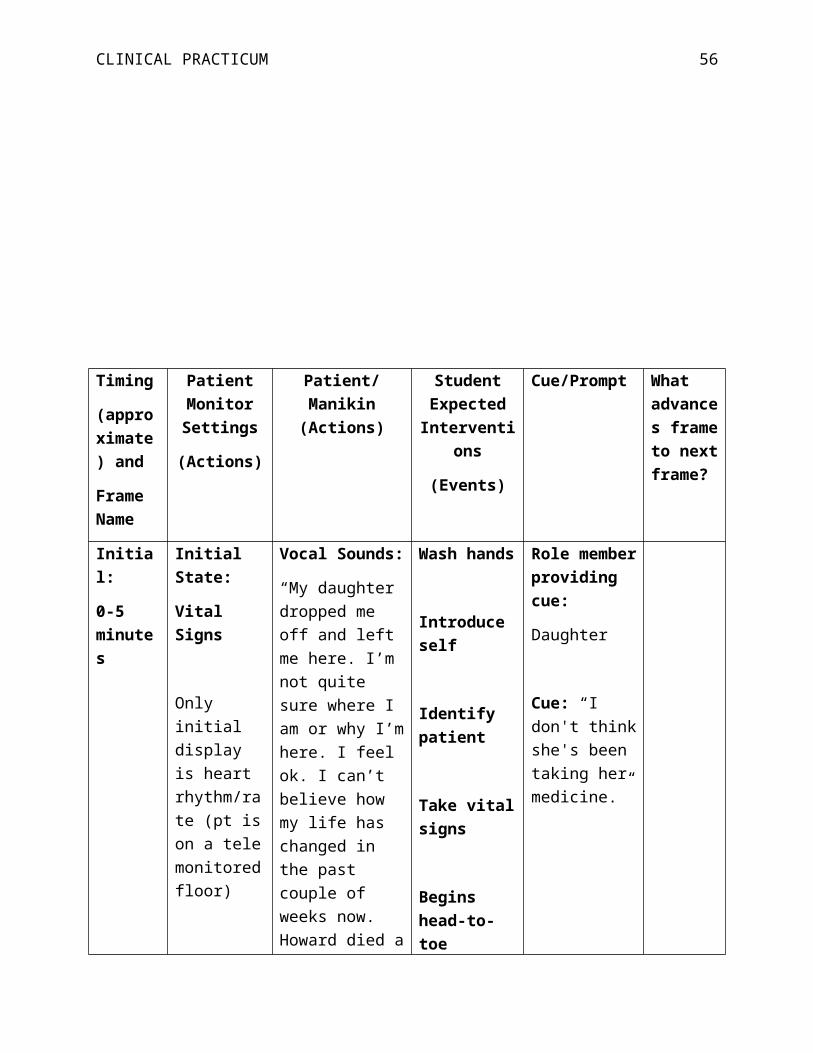
PRACTICUM PAPER 56
Appendix D
Simulation Evaluation
Munson Medical Center - Simulation Evaluation FormTitle of Presentation: Critical Care Physical Assessment Simulation
Date: 3/21/14 Location: Sim Lab
Please complete the evaluation form below by placing an “X” in the box that best fits your evaluation of the educational activity. Completion of this form is required to successfully complete this conference and be awarded contact hours for the program.
Purpose/Goal of this Simulation:
At the end of this program, I was able to:
Strongly Agree
Agree Neutral Disagree Strongly Disagree
1. Perform a full systematic head-to-toe physical assessment on a simulated patient
4
2. Identify major alterations in the assessment
4
3. Evaluate patient data 44. Communicate clearly to patient,
family and healthcare team4
I clearly understood the purpose and objectives for the simulation.
4
The scenario resembled a real-life situation.
3
Did the scenario allow you to use your critical thinking and decision making skills?
4
Did the scenario allow you to use your communication skills?
4
The simulation provided a variety of ways in which to learn the material.
4
The prep material provided to review before the simulation was valuable.
4
The debriefing session was well-organized.
4
The facilitator, _Erin , demonstrated expertise in the content area.
4
Feedback provided during the 4

PRACTICUM PAPER 57
debriefing was constructive.The simulation activity reinforced my knowledge base.
4
After participating in the simulation activity, do you feel more confident in a similar situation in the clinical environment?
4
What did you find most valuable participating in the simulation?Hands on training is always the best for me
What would you like to see done differently in the next simulation?None
How will you apply the information from the simulation activity into clinical practice?All of it I will apply

PRACTICUM PAPER 58
Appendix E
Practicum Evaluations
Student name: Erin Kibbey________________________________________________________
Evaluated by: Erin Kibbey________________________________________________________
Goal/Objective Strongly Disagree
Disagree Neutral Agree Strongly Agree
Comments
Standard of Practice: Facilitation of Learning
Shows enthusiasm for teaching,
learning, and nursing
X
Demonstrates interest and respect for
learners
X
Uses personal attributes such as caring, patience,
integrity, flexibility, etc. to facilitate
learning
X
Serves as a role model of
professional nursing
X
Models critical and reflective thinking
X
Creates opportunities for learners to
develop critical thinking skills
X
Uses information technologies
skillfully to support the teaching-learning
X
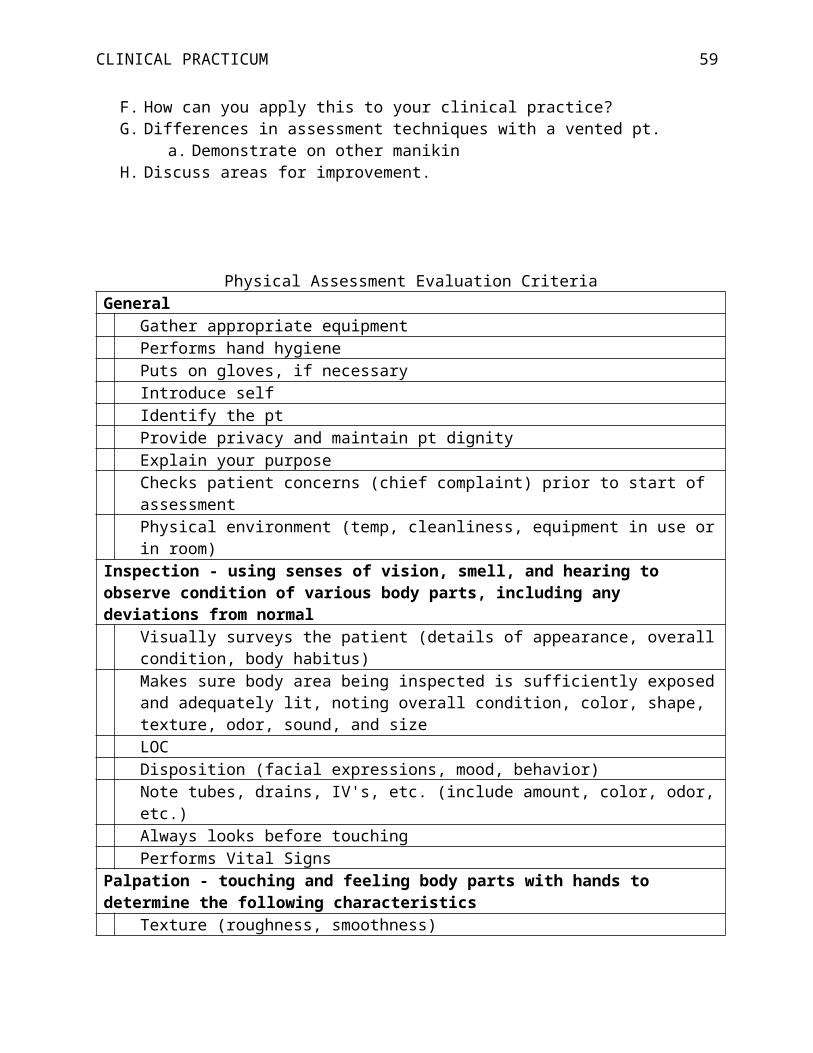
PRACTICUM PAPER 59
process
Practices communication that reflects awareness of
self and others
X
Ability to convey ideas in a variety of
contexts
X
Demonstrates recognition of
multicultural, gender, and experiential
influences on teaching and learning
X
Implements a variety of teaching strategies
X
Teaching strategies are appropriate to learner, outcomes,
context, content, etc.
X
Engages in self-reflection and
continued learning to improve teaching
X
Standard of Practice: Use Assessment & Evaluation Strategies
Uses literature to develop evidence-
based assessment and evaluation practices
X
Uses a variety of strategies to assess
and evaluate learning
X
Provides timely feedback to learners
X
Provides constructive feedback to learners
X
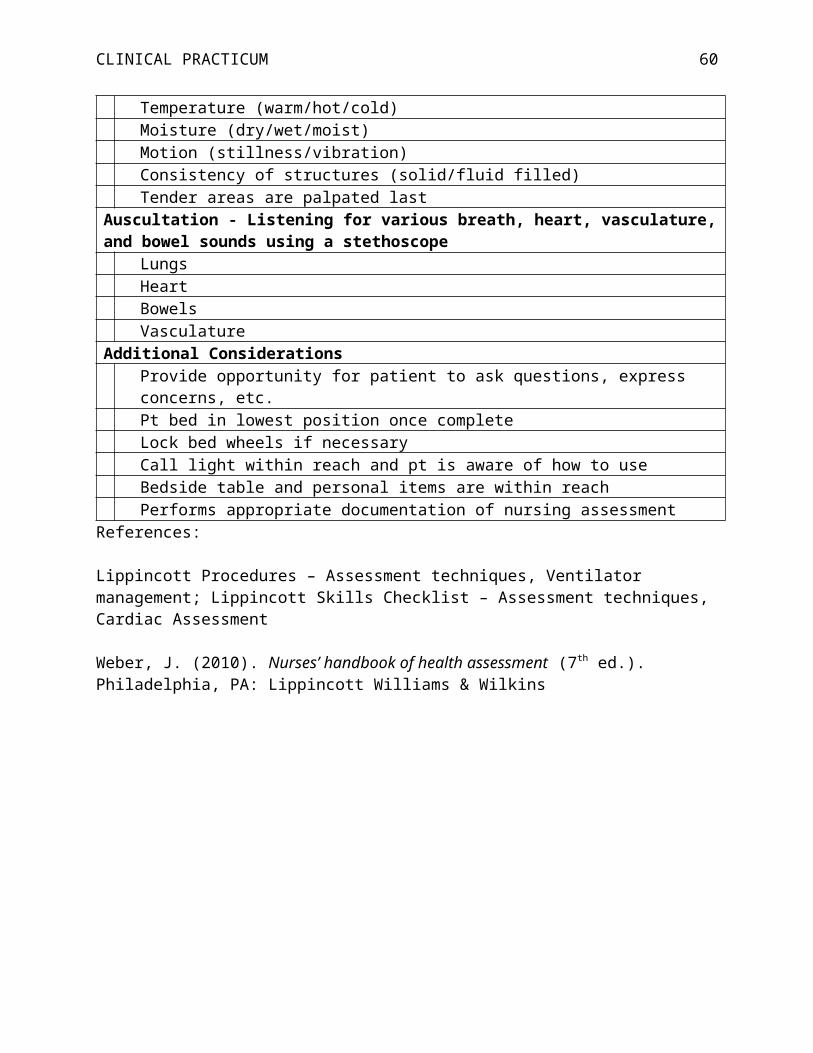
PRACTICUM PAPER 60
Uses evaluation data to enhance the
teaching-learning process
X
Standard of Practice: Participate in Curriculum Design and Evaluation of Program Outcomes
Ensures curriculum reflects current
nursing and health care trends
X
Identifies program outcomes
X
Identifies learner needs
X
Writes appropriate learning objectives
X
Selects appropriate learning activities
X
Implements appropriate
evaluation strategies for new curricula
X
Bases curriculum design on
educational principles, theory,
and research
X
Demonstrates overall knowledge of
curriculum development
X
Comments:

PRACTICUM PAPER 61

PRACTICUM PAPER 62
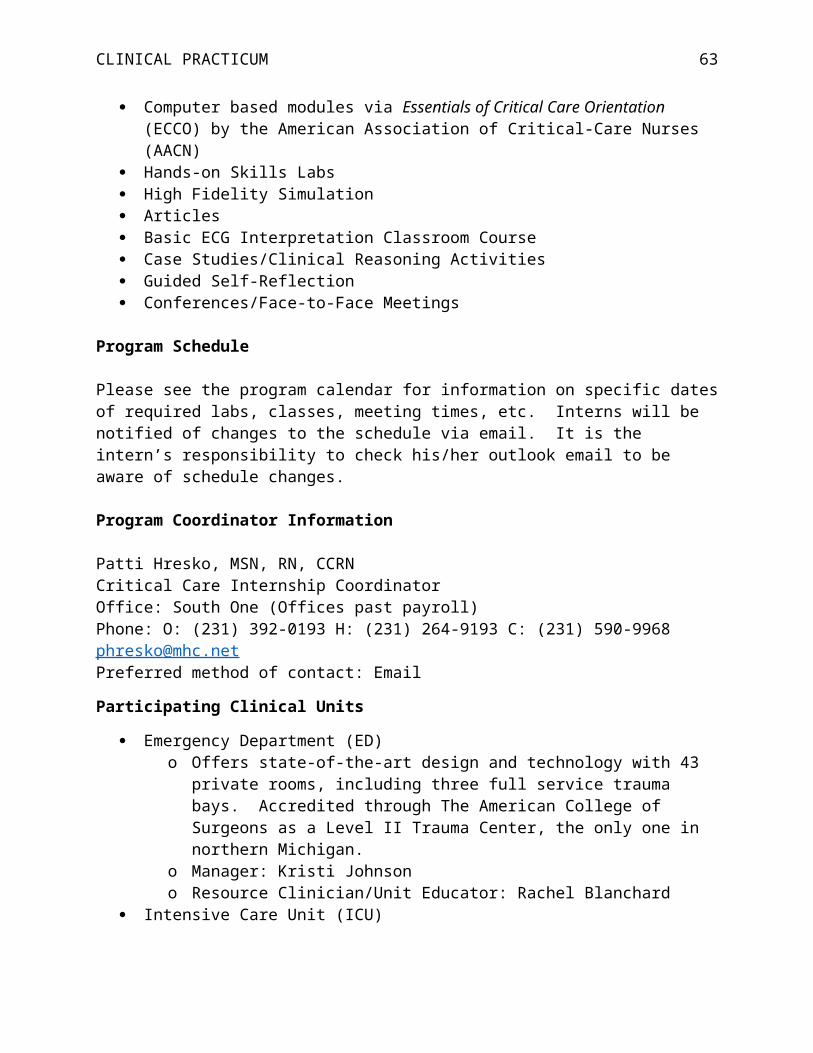
PRACTICUM PAPER 63

PRACTICUM PAPER 64
Appendix F
Evaluations from Interns
Evaluation 1

PRACTICUM PAPER 65
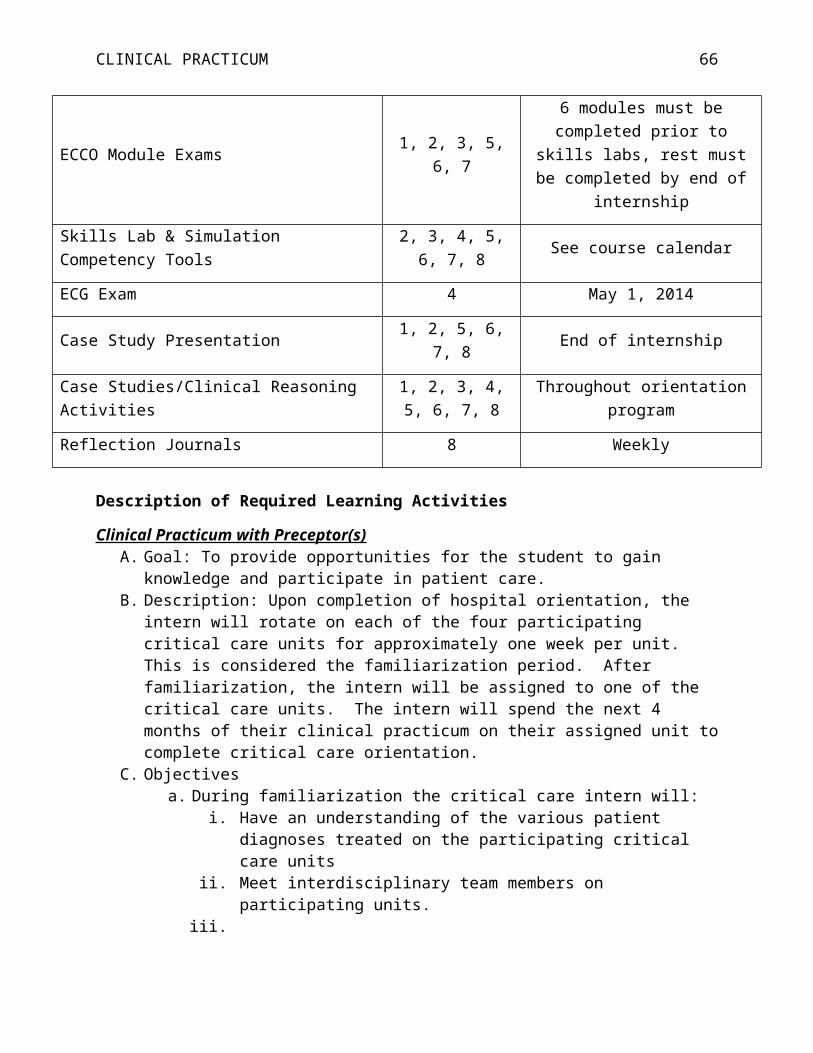
PRACTICUM PAPER 66
Evaluation 2

PRACTICUM PAPER 67

PRACTICUM PAPER 68
Evaluation 3
PRACTICUM PAPER 69
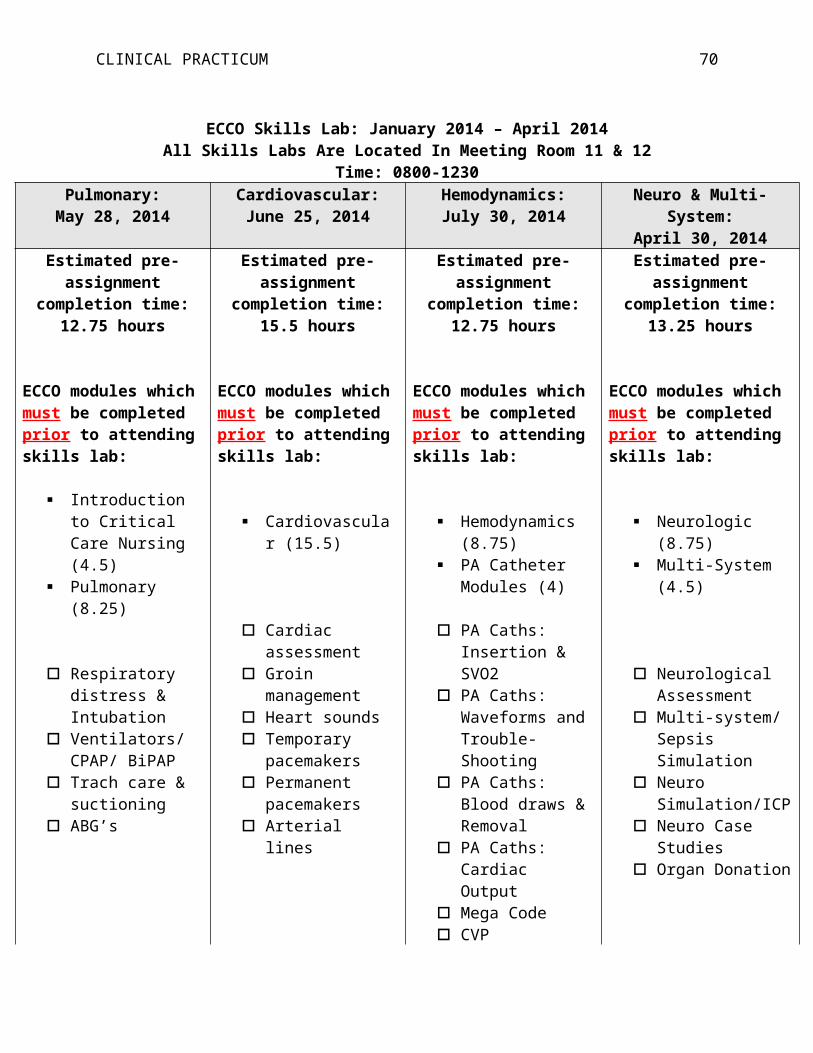
PRACTICUM PAPER 70
Evaluation 4

PRACTICUM PAPER 71
PRACTICUM PAPER 72
Bibliography
Alspach, J. G. (2000). The educational process in nursing staff development. Annapolis, MD:
American Association of Critical Care Nurses.
American Nurses Association and National Nursing Staff Development Organization [ANA &
NNSDO]. (2010). Nursing professional development: Scope and standards of practice.
Silver Spring, MD: Nursesbooks.org.
Avillion, A., Brunt, B., & Ferrell, M. J. (2007). Nursing professional development: Nursing
review and resource manual (1st ed.). Silver Spring, MD: American Nurses Credentialing
Center.
Baltimore, J. J. (2004). The hospital clinical preceptor: Essential preparation for success. Journal
of Continuing Education in Nursing, 35(3), 133-140.
Beyea, S. C., Slattery, M. J., & von Reyn, L. J. (2010). Outcomes of a simulation-based nurse
residency program. Clinical Simulation in Nursing, 6(5). doi:10.1016/j.ecns.2010.01.005
Billings, D. M. (2012). Developing leaner-centered courses. In D. Billings & J. Halstead (Eds.),
Teaching in nursing: A guide for faculty (4th ed.). (pp. 160-169). St. Louis, MO: Elsevier
Saunders.
Billings, D. M., & Halstead, J. A. (2012). Teaching in nursing: A guide for faculty (4th Ed.).
Philadelphia: W.B. Saunders.
Bjork, R., McDaniel, M., Pashler, H., & Rohrer, D. (2009). Learning styles: Concepts and
evidence. Psychological Science in the Public Interest, 9(3), 105-119.
Boland, D. (2012). Developing curriculum: Frameworks, outcomes, and competencies. In D.
Billings & J. Halstead (Eds.), Teaching in nursing: A guide for faculty (4th ed.). (pp. 138-
159). St. Louis, MO: Elsevier Saunders.

PRACTICUM PAPER 73
Bonnel, W. (2012). Clinical performance evaluation. In D. Billings & J. Halstead (Eds.),
Teaching in nursing: A guide for faculty (4th ed.). (pp. 485-502). St. Louis, MO: Elsevier
Saunders.
Bourke, M. P. & Ihrke, B. A. (2012). The evaluation process: An overview. In D. Billings & J.
Halstead (Eds.), Teaching in nursing: A guide for faculty (4th ed.). (pp. 422-440). St.
Louis, MO: Elsevier Saunders.
Bradshaw, M. (2011). Effective learning: What teachers need to know. In M. Bradshaw & A.
Lowenstein (Eds.), Innovative teaching strategies in nursing and related health
professions (5th ed.). (pp. 1-19). Sudbury, MA: Jones and Bartlett.
Bradshaw, M. & Lowenstein, A. (2011). Innovative teaching strategies in nursing and related
health professions (5th Ed.). Sudbury, MA: Jones & Bartlett Publishers.
Bratt, M. (2009). Retaining the next generation of nurses: the Wisconsin Nurse Residency
Program provides a continuum of support. Journal of Continuing Education in
Nursing, 40(9), 416-425. doi:10.3928/00220124-20090824-05
Brunt, B. A. (2007). Competencies for staff educators: Tools to evaluate and enhance nursing
professional development. Danvers, MA: HCPro, Inc.
Buruss, N. & Popkess, A. (2012). The diverse learning needs of students. In D. Billings & J.
Halstead (Eds.), Teaching in nursing: A guide for faculty (4th ed.). (pp. 15-33). St. Louis,
MO: Elsevier Saunders.
Center for Medical Simulation. (2013). Debriefing assessment for simulation in healthcare
(DASH): Rater’s handbook. Retrieved from
http://www.harvardmedsim.org/_media/DASH.handbook.2010.Final.Rev.2.pdf

PRACTICUM PAPER 74
Clynes, M., & Raftery, S. (2008). Feedback: An essential element of student learning in clinical
practice. Nurse Education in Practice, 8(6), 405-411.
Deck, M. L. (2012). Nursing professional development: Stories, tips, and techniques. Journal for
Nurses in Staff Development, 28(3), 143-149.
Dillard, N. & Siktberg, L. (2012). Curriculum development: An overview. In D. M. Billings & J.
A. Halstead (Eds.). Teaching in nursing a guide for faculty (4th ed.). (pp. 76-91). St.
Louis, MO: Elsevier Saunders.
Dyess, S. M., & Sherman, R. O. (2009). The first year of practice: New graduate nurses’
transition and learning needs. The Journal of Continuing Education in Nursing, 40(9),
403-410. http://dx.doi.org/10.3928/00220124-20090824-03
Flood, L., & Powers, M. (2012). Lessons learned from an accelerated post-master's nurse
educator certificate program: Teaching the practicum course. Nursing Education
Perspectives, 33(1), 40-44. doi:10.5480/1536-5026-33.1.40
Forneris, S., & Peden-McAlpine, C. (2007). Evaluation of a reflective learning intervention to
improve critical thinking in novice nurses. Journal of Advanced Nursing, 57(4), 410-421.
doi:http://0-dx.doi.org.libcat.ferris.edu/10.1111/j.1365-2648.2007.04120.x
French, B. & Greenspan, M. (2011). The preceptored clinical experience. In M. Bradshaw & A.
Lowenstein (Eds.), Innovative teaching strategies in nursing and related health
professions (5th ed.). (pp. 437-457). Sudbury, MA: Jones and Bartlett
Gaberson, K. & Oermann, M. (2010). Clinical teaching strategies in nursing (3rd ed.). NY:
Springer Publishing Company.

PRACTICUM PAPER 75
Goode, C. J., Lynn, M. R., Krsek, C., & Bednash, G. D. (2009). Nurse residency programs: An
essential requirement for nursing. Nursing Economics, 27(3), 142-147, 159. Retrieved
from https://www.nursingeconomics.net/ce/2011/article27142159.pdf
Happell, B. (2009). A model of preceptorship in nursing: Reflecting the complex functions of the
role. Nursing Education Perspectives, 30(6), 372-376.
Hayes, J. (2011). Student evaluation of teaching. In M. Bradshaw & A. Lowenstein (Eds.),
Innovative teaching strategies in nursing and related health professions (5th ed.). (pp.
563-574). Sudbury, MA: Jones & Bartlett Publishers.
Henderson, A., & Eaton, E. (2013). Assisting nurses to facilitate student and new graduate
learning in practice settings: What ’support’ do nurses at the bedside need? Nurse
Education in Practice, 13(3), 197-201.
Iwasiw, C, Goldenberg, D., & Andrusyszyn, M. (2005). Curriculum development in nursing
education. Sudbury, MA: Jones and Bartlett Publishers.
Jeffries, P. R. & Clochesy, J. M. (2012). Clinical simulations: An experiential, student-centered
pedagogical approach. In D. Billings & J. Halstead (Eds.), Teaching in nursing: A guide
for faculty (4th ed.). (pp. 352-368). St. Louis, MO: Elsevier Saunders.
Jewell, A. (2013). Supporting the novice nurse to fly: A literature review. Nurse Education in
Practice, 13(4), 323-327. doi:10.1016/j.nepr.2013.04.006
Kirkpatrick, J. M. & DeWitt, D. A. (2012). Strategies for assessing and evaluating learning
outcomes. In D. Billings & J. Halstead (Eds.), Teaching in nursing: A guide for faculty
(4th ed.). (pp. 441-463). St. Louis, MO: Elsevier Saunders.
Knowles, M.S. (1980). The modern practice of adult learning. Chicago, IL: Follett.

PRACTICUM PAPER 76
Kolb, D. (1984). Experiential learning: Experience as the source of learning and development.
Englewood Cliffs, NJ: Prentice Hall. Retrieved from
http://academic.regis.edu/ed205/kolb.pdf
Leighton, K. & Johnson-Russell, J. (2011). Innovations in facilitating learning using simulation.
In M. Bradshaw & A. Lowenstein (Eds.), Innovative teaching strategies in nursing and
related health professions (5th ed.). (pp. 239-264). Sudbury, MA: Jones and Bartlett.
Longo, A., & Tierney, C. (2012). Presentation skills for the nurse educator. Journal for Nurses in
Staff Development, 28(1), 16-23.
Lowenstein, A. J. (2011). Role play. In M. Bradshaw & A. Lowenstein (Eds.), Innovative
teaching strategies in nursing and related health professions (5th ed.). (pp. 187-205).
Sudbury, MA: Jones and Bartlett.
McDonald, P. (2010). Transitioning from clinical practice to nursing faculty: lessons
learned. Journal of Nursing Education, 49(3), 126-131. doi:10.3928/01484834-
20091022-02
McKinley, M. (2008). Walking on water and other lessons learned as a clinical educator. AACN
Advanced Critical Care, 19(4), 388-395.
Morris, L. L., Pfeifer, P. B., Catalano, R., Fortney, R., Hilton, E. L., McLaughlin, J., . . .
Goldstein, L. (2007). Designing a comprehensive model for critical care orientation.
Critical Care Nurse, 27(6), 37-60.
Myrick, F., Yonge, O., & Billay, D. (2010). Preceptorship and practical wisdom: A process of
engaging in authentic nursing practice. Nursing Education in Practice, 10(2), 82-87.
doi:10.1016/j.nepr.2009.03.018
PRACTICUM PAPER 77
National League for Nursing [NLN]. (2012). The scope of practice for academic nurse educators
2012 revision. NY: author.
Penn, B., Wilson, L., & Rosseter, R. (2008). Transitioning from nursing practice to a teaching
role. OJIN: The Online Journal of Issues in Nursing, 13(3), 1-14.
Polit, D. F. & Beck, C. T. (2012). Nursing research: Generating and assessing evidence for
nursing practice (9th ed.). Philadelphia, PA: Lippincott Williams & Wilkins.
Robinson, C. P. (2009). Teaching and clinical educator competency: Bringing two worlds
together. International Journal of Nursing Education Scholarship, 6(1), 1-14.
Rowles, C. J. (2012). Strategies to promote critical thinking and active learning. In D. Billings, &
J. Halstead (Eds.), Teaching in nursing: A guide for faculty (4th ed.). (pp. 258-284). St.
Louis, MO: Elsevier Saunders.
Saunders, R. (2003). Constructing a lesson plan. Journal for Nurses in Staff Development, 19(2),
70-80.
Sauter, M., Nightingale Gillespie, N., & Knepp, A. (2012). Educational program evaluation. In
D. M. Billings & J. A. Halstead (Eds.). Teaching in nursing a guide for faculty (4th ed.).
(pp. 503-549). St. Louis, MO: Elsevier Saunders.
Scanlan, J. (2001). Learning clinical teaching: Is it magic? Nursing & Health Care
Perspectives, 22(5), 240-246.
Scheckel, M. (2012). Selecting learning experiences to achieve curriculum outcomes. In D.
Billings & J. Halstead (Eds.), Teaching in nursing: A guide for faculty (4th ed.). (pp. 170-
187). St. Louis, MO: Elsevier Saunders.

PRACTICUM PAPER 78
Schipper, L. (2011). The socialization process of newly graduated nurses into a clinical setting:
role of the clinical nurse educator. Journal for Nurses in Staff Development, 27(5), 216-
219. doi:10.1097/NND.0b013e31822d68ba
Schoening, A. M. (2013). From bedside to classroom: The nurse educator transition model.
Nursing Educator Research, 34(3), 167-172.
Shellenbarger, T. & Edwards, T. (2012). Nurse educator simulation: Preparing faculty for
clinical nurse educator roles. Clinical Simulation in Nursing, 8(6), 249-255.
doi:10.1016/j.ecns.2010.12.006
Stokes, L. G. & Kost, G. C. (2012). Teaching in the clinical setting. In D. Billings & J. Halstead
(Eds.), Teaching in nursing: A guide for faculty (4th ed.). (pp. 311-334). St. Louis, MO:
Elsevier Saunders.
Tedesco-Schneck, M. (2013). Active learning as a path to critical thinking: Are competencies a
roadblock? Nurse Education in Practice, 13(1), 58-62.
Toth, J. (2008). The basic knowledge assessment tool, version eight (BKAT-8): For adult critical
care nursing. Retrieved from http://www.bkat-toth.org/BKAT-8.html.
Ullrich, S. & Haffer, A. (2009). Precepting in nursing: Developing an effective workforce.
Sudbury, MA: Jones and Bartlett Publishers.
Ulrich, B. (Ed.). (2012). Mastering precepting: A nurse’s handbook for success. Indianapolis,
IN: Sigma Theta Tau International.