· web viewafter complete assessment of the site of insertion, a three-dimensional guidance must...
TRANSCRIPT
ABSTRACT
Background: Replacement of tooth loss has been a topic of constant research in dentinstry,
given the challenges that dentists face during the treatment through dental implants. Amongst
such challenges is sinus lift surgery and controlling the stress encountered during the process.
Alternatives to the sinus lift surgery include the use of short straight implants and tilted implants
that allow dentists to control stress distribution and make a successful implant.
The Aim: The aim was to identify an alternative to sinus lift surgery in order to minimize its
drawbacks through a comparison between two alternatives to sinus lift surgery (short vs tilted)’
around the maxillary sinus.
Material and Methods: A human jaw model of cortical bone layer, trabecular bone layer and
commercially pure titanium implants was utilized in this regard and the analysis conducted on
the maxilla region through a MSC NASTRAN FEA model. A 3D simulation of a human adult
jaw was utilized to test the short and tilted implants using loads of 300N at a 25o inclination
(oblique occlusal) to the bucco-palatinal axis of the implants in both models. The FE model of
this study was derived from a C.T scan of an adult male patient to simulate the maxilla,
maxillary sinus and alveolar bone.
Results: Through the simulation, Von Mises principal stress distribution was charted along with
Cortical bone and Trabecular bone minimum and maximum principal stress distribution for both
the models i.e. short straight implants and tilted dental implants. The use of the oblique occlusal
loads increased the stress on the Trabecular bone, and had lower stress in the Cortical bone
during the simulation of the tilted implants in the maxilla region.
Conclusion: It was found that the use of tilted implants is a better alternative over short
implants, given its success rate in stress distribution as alternative to sinus lift surgery in the
maxillary region given the simulation results. It is recommended that future research within this
research area through the application of FE analysis be supported with a qualitative modelling
for better and more reliable results.

Introduction to Tooth Loss & its Effect
The replacement of missing teeth has been one of the most important aspects of dentistry in the
past decades (Irish, 2004). In order to reach a proper treatment plan, one must have a full
understanding of dental anatomy; the science that studies appearance, development and
morphology of teeth. Teeth are bone like structures composed of two parts, a root that is
implanted in the jawbone and a crown that is exposed to the oral cavity (Saber et al., 2015).
Jawbones are composed of two parts, a fixed part; the maxilla responsible for stability and a
lower mobile jaw; the mandible. The two jaws perform the action of mastication. (American
Dental Association, 2010). The alveolar bone is the part that surrounds the roots and it forms the
socket, similar to all bones in the body they are continuously undergoing through cyclic
resorption and reformation. (Linkow and Chercheve, 1970)
Tooth loss is multi-factorial and is mainly encountered in older patients. The case of complete
loss of the dentition is called edentoulism, while the loss of a few numbers of teeth is called
partial edentoulism (Ruth et al, 2001). There are various causes of tooth loss which includes
Physical trauma or injury; Tooth decay; and Periodontal disease (Saber et al., 2015). The failure
in replacing missing teeth has many drawbacks. Patients may suffer from aesthetical as well as
functional problems (Shahrul et al, 2011). After the tooth loss, the alveolar bone undergoes a
continuous regeneration. There is continuous osteoblastic (bone forming) and osteoclastic (bone
resorbing) activity (Saber et al., 2015). However, this cycle is affected by the force transmitted
by teeth from the mechanical action of chewing. After tooth loss this stimulus is absent, leading
to a disturbed equilibrium. Bone loss becomes more prominent, which eventually decreases bone
height and width leading to deformation (Verri et al., 2015).
The occlusion harmony is also disturbed by the movement of neighbouring teeth into the empty
space; this action shifts the direction of force distribution from the long axis of the tooth. The
opposing teeth lose their function due to the absence of mastication, their periodontal ligament
becomes thinner and looser. Hence, these teeth will gradually creep into the empty space.
(Shahrul et al, 2011)
34

Replacing Missing Teeth and Applied Approaches
To replace the tooth loss and the missing teeth, there are different approaches that are practiced
by dentists. While the approaches have evolved over the years, there are two commonly used
methods practiced widely: Fixed Denture and Removable Denture. As the name indicates, a
fixed denture or a fixed bridge is cemented or bonded to the surface while a removable denture
allows removability.
Dental Implants
Dental implants are applied to solutions for total or partial tooth loss, however, given the varying
anatomy of positions as well as structures, they cannot be placed in the most appropriate position
as analysed (Sarfaraz et al., 2015). Sometimes, they are used in a titled position and sometime in
a straight position. The straight implants are commonly used in tiled position considering the
effect of the anatomy (often referred to as the maxillary sinus). The application of dental
implants has been and is subjected to numerous studies examining the most suitable methods to
investigate the distribution of stress and the logical effects that arise of the treatment.
Research conducted earlier highlight on the point that there is no clinical difference in the use of
tilted and straight implants (Rammelsberg et al., 2012; Guven et al., 2015). In those studies, the
biomechanical characteristics were considered for evaluation and used in comparison against the
design for straight implants (7, 8). Past research also indicates that the survival rates vary based
on the type of implants applied in clinical studies (Guven et al., 2015; Saleh Saber et al., 2015;
Verri et al., 2015). One of the most widely applied framework for analysis pertaining to dental
implant stress effects is the finite element analysis (Verri et al., 2015). Given the lower
availability of data on the stress distribution on the maxillary posterior region through short or
titled implants, this research area was identified.
In the past few years, an increase in the use of FEA tool has been found to predict dental
implants stress level within the implant as well as the surrounding area of the bone. Using the
FEA, more realistic and accurate structures can be assessed, with the models further being
divided parts that are mathematically accurate (Geng et al., 2008). With the simulation process,
the aspects covering strain, stress as well as displacement can be studied and calculated in detail
(Beer, 1981). The use of oblique and vertical loads apply a mastication affect leading to actions

such as bending leading to stress within the bone as well as the implant. In dental implants,
success of the implants is tested in the form of gradient of stress that is transferred to the bone
(Guven et al., 2015; Geng et al., 2008). The impact or density of the stress relates to the interface
between the bone and the implant structure, the applied location (oblique or vertical), the type of
prosthesis, implant length/diameter, shape and also, the implant surface characteristics. Another
important factor is the quality /quantity of the bone area (Beer, 1981). To measure the stress, von
Mises stress metric is utilized which combines shear and normal stress in all directions.
LITERATURE REVIEW:
Background on Dental Implants
History
Dental implants date back to ancient Egypt; wherein sea shells and stones were used to replace
missing teeth, while noble metals were used by others to act like the natural roots (Abraham,
2014). In the 1930's, some archaeological excavations discovered that the Mayans used curved
stones, shells, and gold to replace missing teeth over 2000 years ago (Jemat et al., 2015). In more
recent times, teeth from the same individual (autograft), and teeth from a different individual of
the same species (allograft) were used. However, its use was limited as a result of infectious
diseases that sometimes led even to death. (Lee JH et al, 2005)
In 1957, a Swedish orthopaedic surgeon by the name Peringor Branemark discovered that bone
could grow in proximity with Ti, without being rejected. This phenomenon was called
“osseointegration’’ (Searson, 2005; Sullivan, 2001). The first dental implant was placed in 1965
by Branemark into a 34 year old male patient; it served for more than 40 years until the patient
passed away. Branemark presented his 15 years of research in 1982 at the Toronto conference.
The US Food and Drug Administration (FDA) approved the use of Titanium (Ti) dental implants
in the same year. Ever since, there has been continuous development and different types of
dental implant have been used.
The history of Ti dental implants began in 1940 (Adelle et al, 1981), Bothe et al. implanted a
mix of Ti and other metals into laboratory animals, Ti was well tolerated due to its high

corrosion resistance. In the early 1970’s, Ti and its alloys have been gradually accepted in the
U.S, after the development of pre-fabricated Ti blade implants (Hiroshi and Toru, 1996). Grade
four commercially pure Ti is typically used in dental implants because of its great strength and
resistance to corrosion. However, recently Ti alloys, mainly Ti6A14V, has become popular
because of its strength and fatigue resistance. (Le Guéhennec et al, 2007)
Abutment
They are made of Ti in different sizes and angulations specific to each case.. As seen in the
figure 11, the classification of abutments is into three types: Rotational, manufacture version and
retention of prosthesis. These are further classified into seven types.
Figure 1: Classification of Abutments
classification of abutments
Rotational device
one piece abutment
two piece abutment
Form obtained from the
manufacurer
machined form
custom cast using gold or plastic components
Retention of prothesis to abutment
screw retained
cement retained
attachments

Abutments are available in two types: Angulated and Straight, as seen in the figure 12. The
angulated abutments are further divided into 30˚Cad-cam milled structure, 6˚ is indicated for
overdenture and bridges; Upto 20˚for immediate provisional prosthesis and 25˚ for narrow
platforms and 28˚ for the rest of the platforms.
Figure 2: Types of Angulations
Abutment selection criteria
There is a particular selection criterion on which dental implants are planted. Due to the
advancement in medical field, it has opened many doors for performing a dental implant in a
variety of ways. The dental surgeon can specifically choose what material is to be used and what
exact method of implants is going to be implemented during the dental surgery. The dental
implants are also very stable in the long term if the procedure is done accurately (Cavallaro and
Greenstein, 2011). Aesthetics is quite a difficult field and a lot of challenges are present in a
successful restoration through aesthetics. It has been seen that anterior teeth are very hard to
restore through aesthetics. The tissue and bone loss determine the success of the process and if
these losses are kept at a minimum the procedure is considered successful. However it is even
more difficult to replace multiple teeth instead of a single tooth through aesthetics. A lot of
planning is needed and also a lot of emphasis is to be put on the overall betterment of the patient.
Angulation
Angulated
upto 30˚Cad-cam milled structure for
individual prosthesis
6˚ is indicated for overdenture and
bridges
Upto 20˚for immediate provisional prosthesis
25˚ for narrow platforms and 28˚ for the rest of the
platforms
Straight
Some of the commonly used abutment selection criteria include it being bio-compatible, accurate
fit to prevent loosening, long-term stability and aesthetics.
Angulated Implant placement
It was first used by Dr: Paulo Malo in 1933, when he placed two vertical implants in the anterior
and two in the posterior region at an angulation of 35˚-40˚ and named it “all in four”.
A two-dimensional safe distance between the vertical and tilted implant must be obtained, by
multiplying the known length of each implant by a constant derived from the sine of the insertion
angle. After complete assessment of the site of insertion, a three-dimensional guidance must be
preformed. Extreme angulation must be avoided as it increases forces exerted at the bone-
implant interface. For easier construction of the final prosthesis, inter-implant angulation must be
confined to a single three-dimensional plane. Single tooth restoration should be avoided on
angulated abutments (Geramipanah et al, 2010).
Maxillary sinus lift surgery
Sinus lift is a well-accepted technique to treat the loss of the VBH (vertical bone height) inside
posterior maxilla either performed through a lateral window (Summers 1994) or by an osteotome
sinus floor elevation technique with bone-graft material located within maxillary sinus region in
order to enhance the width and height of the bone available.
Table 1: A guideline towards sinus floor elevation

Alternatives to sinus lift surgery
There is an alternative present to the sinus augmentation technique, short implants have some
potential as they are brought forward by some researchers (Renouard et al, 2006). The implants
with a relatively small length of 5-8 mm are known as short implants. Although there is some
ongoing discussion on this topic as some authors also claim that 7-10 mm are the short implants
(Das et al, 2006). It has been seen through Finite element (FEA) that the occlusal forces are
distributed mainly to the crestal bone, they are not evenly spread over the surface area of an
implant. Therefore the short implants are viable and can be used (Lum et al, 1999).
The short implants faced a lot of questions as the implants previously used had a lot of history
and research behind them although over the years short implants have proven to be more
successful. The success rates of short implants have steadily climbed and in 2004 it was 95.1% to
be exact (Renouard et al, 2006). The patients with missing teeth have benefitted from this as the
survival rate of normal implants is somewhat similar to the survival rate of short implants.
The earlier writings and researches stated the short implants had low survival rate when
compared to standard ones and they failed more often than them. However in recent times where
the textured-surfaced implants are more common, the survival rate has climbed and is almost the
same to the standard implants. Research from different sources has determined that implants with
a length of 6 mm have had the same survival rate as the standard ones (Bruggenkate et al, 1998).
Although it is still recommended to not use shorter implants on their own but to synergize them
with the longer ones to make them more stable.
A system review was conducted where a total of 16344 implants were reviewed and the failure
rate was 4.8%. Implants that were 3.75 mm wide and 7 mm long failed more often as they had
the failure rate of 9.7% while the failure rate of 3.75-10mm implants was at 6.3% (Das et al,
2006). The difference in the failure rates can be noted as the 4 mm implant in diameter proved to
be more successful and had little failures. The long term effects of short implants as opposed to
bone augmentation are not known at this time. The residual bone was about 6 to 7 mm with a
standard implant while it was placed there at the same time with the sinus augmentation
procedure (Pieri et al, 2012). Outcome of both of these techniques were similar. The clinical and
radiographic review therefore proved the short implants are viable too.

Implants can also be placed in a disto-angulated direction as an alternative to the sinus surgery
which can in turn avoid disturbing maxillary sinus. Pterygomaxilla can also be used as a location
to place implants. Zygoma implants are another alternative to sinus augmentation procedure.
(Graves et al, 1994)
Finite Element analysis
Many methods were implemented in the study of stress distribution around dental implants eg:
strain gauge, two and three dimensional photo elasticity and finite element analysis (FEA) (Shen
et al, 2010). FEA is a computer analysis that involves numerical techniques in order to calculate
the strength as well as the behaviour of the structures engineered. It was developed in 1956 in the
aircraft industry and was then introduced in the field of dentistry in the1970’s, when W. Farah,
Thresher R.W, and Yattran A.L studied the stress in a tooth structure they modelled.
In the year 2000, Zhang L, et al conducted a study on the correlation between implant length and
diameter, with proper stress distribution using three- dimensional FEA. The uses of three
dimensional FEA can assess biomechanical problems before they occur. Each element is
assigned with the properties of the material being modelled. The model should mimic the exact
physical properties of the actual structure or as close as possible to ensure the quality of FEA.
The most difficult part of the simulation is to mimic the properties of a living tissue. Mostly the
properties are either drawn from a detailed anatomy book or a cone beam C.T scan of the jaws.
CBCT offers not only the anatomical structure, but also can give a better idea about the material
properties in relation to different bone density. Depending on the study intended, different bone
modelling is initiated, in some studies bone is modelled as simple rectangle ellipsoids, or u-
shaped (Sagat et al, 2010; Gröning et al, 2012).
As natural bone density occurs in different densities, specific density is modelled according to
the study conducted, a more detailed geometric might be required sometimes like in cancellous
bone, especially in the posterior maxilla as it has a wide variety of densities in the same jaw
(Georgiopoulos et al, 2007). As for implants, many ways were used to simulate both implants
and abutment materials, but the two main ways were well studied in the literature. One way is to
obtain all required information from the manufacturer eg: length, diameter, macro- micro thread
configuration, the second way is by obtaining a digital scan of the used implant and abutment

and to use the scanned model. While crowns are modeled relying on the morphology of the
natural tooth to be replaced after calculation of both mesiodistal and buccolingual dimensions
(Wheeler, 1963).
After completion of bone and implant simulation, masticatory forces are simulated and applied.
Masticatory forces are defined 1. Compressive forces that attempt to push materials towards each
other. 2. Tensile forces that pull objects apart. 3. Shear forces which cause sliding. Tensile and
shear forces are the forces that can increase stress around implant-bone interface and prosthetics.
In actual mastication two different types of forces are present, cyclic and static. Most of FEA
studies use static forces as they are more accurate to simulate (Misch et al, 2005). The stress is
then measured in a cross sectional area in neuton (force) per square meter (unit area), that’s
N/m2. Usually different colour figures are used to illustrate the amount of stress around the
implant and prosthetic structures (Geng et al, 2001).
MATERIALS AND METHODS
In this study a 3D finite element model was used to examine and compare the force distribution
on the bone-implant interface between short and tilted dental implants around the maxillary
sinus. The FE model of this study was derived from a C.T scan of an adult male patient to
simulate the maxilla, maxillary sinus and alveolar bone. Using I-DEAS Artisan 4.0 CAD-CAM
software (World Head quarters 200 East man drive, Milford, Ohio 45150).
General overview
The effect of implant tilting on stress distribution was studied in model 1 for a single cylindrical
Ti implant placed in the posterior maxilla. The implant was placed in the upper left second pre-
molar area (#25) with an angulation of 20o in respect to the occlusal plane (Fig 16). Another
single short cylindrical Ti implant was inserted in model 2. The implant was inserted in area of
#25 with 0 angulation in respect to the occlusal plane (Fig 17). In the present study two different
implant configurations (diameter/length) were modelled (Fig 18).
A detailed description of the models used in this study varying according to implant diameter,
length and inclination are given in table 4. Implant and abutment dimension was based on the

dimensions of commercially available Straumann implant system, but the geometry of both
components was simplified to that of a cylinder. A 20o angulated abutment by Struman was used
with implant in model 1 whereas a straight one used with the implant in model 2, (Fig 17 and Fig
18).
Table 2: Configuration and inclination of the implants used in this study.
Model Dimensions ConfigurationModel 1 4.1mm/12mm 20 tiltedModel 2 4.1mm/6mm Perpendicular to the
horizontal plane
Figure 3: Model 1: 25o tilted dental implant at area of #25
Figure 4: model 2 short dental implant 00 inclination

Figure 5: Struman dental implants
Figure 6: 20o angulated Struman abutment and Struman straight abutment
The maxilla was represented as a combination of cortical and cancellous bone. The cortical plate
(see above, Fig 16, 17 colour coded purple) was assumed around a cancellous core (see above
Figure 16, 17 colour coded blue). For implant longevity in the posterior region, it is important to
maintain at least 2mm of bone between the sinus wall and the implant. In this study, therefore
bone plate of 2mm was modelled in this region. The residual ridge height in the posterior region
was identical in both models.
The focus of this study was on the stress distribution of tilted vs straight implants in the bone-
implant interface. Therefore, only half of the maxilla was analysed. Inclusion of the entire
maxilla in the analysis would have resulted in a FE model that consists of a great number of
elements and nodes. By analysing only half of the maxilla, a finer FE mesh was obtained, which
probably led to a higher accuracy of the results.
Material Properties
All materials used in this study were considered to be isotropic, homogeneous and linearly
elastic. The material properties of all the materials used in this study are given in table 6.
Table 3: materials parameter
Elastic Modulus (MPa) Poisson’s Ratio
Cortical Bone 14800 0.30
Type 4 Trabecular Bone 1100 0.30
Implant 105000 0.33
Abutment 105000 0.33
Crown 68900 0.28
Interface conditions
In a continuous bond, the interfacing between the bone and the implant was modelled, which
leads to an ideal osseoitegration minus any relativity. It can be said that the implants were rigid
to the bone in terms of position with similar bonding applied at all interfaces.
Elements and nodes
Generally the total number of elements and nodes used in this study sum up to 865,276. All
structures were meshed using First order Tetrahedron free meshing. (Fig 20)
Figure 7: meshing of the model.
Number of Elements: 329303 (Short Implant Model)
Number of Nodes: 66309 (Short Implant Model)
Number of Elements: 392529 (Long Implant Model)
Number of Nodes: 77135 (Long Implant Model)
Loading conditions and Boundary conditions
The direction and magnitude of masticatory forces vary greatly between individuals and location
of force application in the mouth. In this study the models were restored with a crown cemented
on the abutment, the crown to implant ratio is 1.5: 1. An oblique occlusal bite force on 300N was
applied at a 25o inclination to the bucco-palatinal axis of the implants in both models. The
boundary conditions applied to both models are shown in Fig 21 and. As restraint condition, the
top of the maxilla was totally fixed.

Figure 8: Figure 20: boundary conditions.
Software and evaluation
MSC NASTRAN/PATRAN Version FE, software was used.

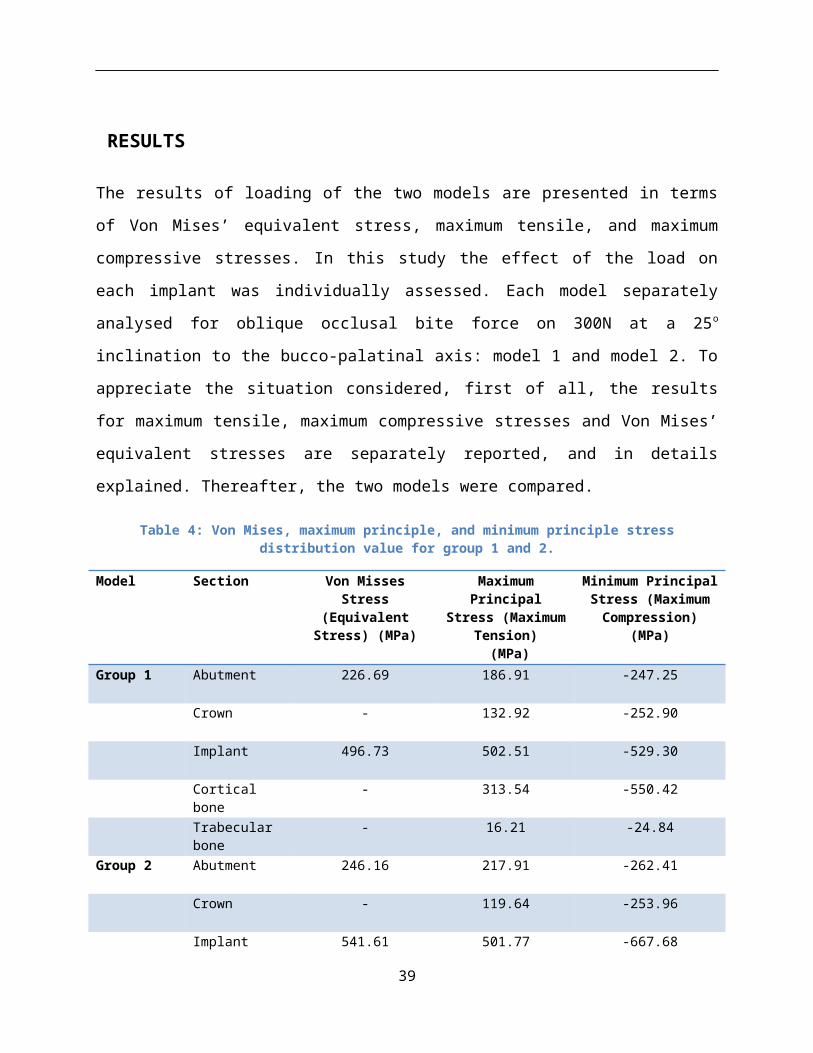
RESULTS
The results of loading of the two models are presented in terms of Von Mises’ equivalent stress,
maximum tensile, and maximum compressive stresses. In this study the effect of the load on
each implant was individually assessed. Each model separately analysed for oblique occlusal bite
force on 300N at a 25o inclination to the bucco-palatinal axis: model 1 and model 2. To
appreciate the situation considered, first of all, the results for maximum tensile, maximum
compressive stresses and Von Mises’ equivalent stresses are separately reported, and in details
explained. Thereafter, the two models were compared.
Table 4: Von Mises, maximum principle, and minimum principle stress distribution value for group 1 and 2.
Model Section Von Misses Stress (Equivalent Stress)
(MPa)
Maximum Principal Stress (Maximum
Tension) (MPa)
Minimum Principal Stress (Maximum
Compression) (MPa)
Group 1 Abutment 226.69 186.91 -247.25
Crown - 132.92 -252.90
Implant 496.73 502.51 -529.30
Cortical bone - 313.54 -550.42
Trabecular bone - 16.21 -24.84
Group 2 Abutment 246.16 217.91 -262.41
Crown - 119.64 -253.96
Implant 541.61 501.77 -667.68
Cortical bone - 382.95 -526.61
Trabecular bone - 57.54 -44.67
The Von Mises stress distribution computed for the dental implants evaluated under oblique load
were 496.73 MPa for group 1 and 541.61 MPa for group 2 (Table 7; Figure 22 and 23). For the
cortical bone-implant interface on the side of the stress concentration under oblique load, the
maximum principle stress values were 313.54 and 382.95 MPa and the minimum principle stress
values were -550.42 and -526.61 MPa for groups 1 and 2, respectively (Table 7; Figure 24to 27).
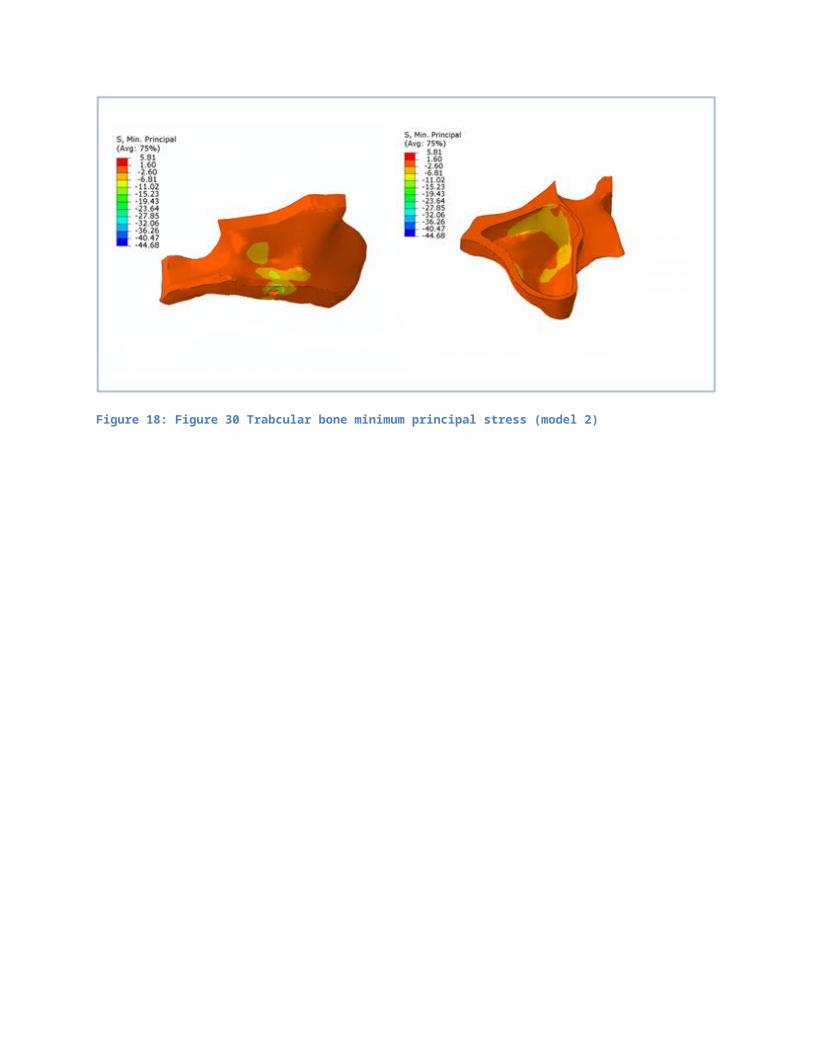
For trabecular bone, the maximum principle stress, and minimum principle stress values of
39

groups 1 and 2 were estimated as 16.21 and 57.54 MPa, -24.84 and -44.67 MPa, respectively
(Table 7; Figure 28 to 31).
Figure 9: Model 1Von Mises stress distribution On implant (group 1)
Figure 10: Model 2 Von Mises stress distribution On the implant (group 2)
Figure 11: Cortical bone maximum principal stress (model1)

Figure 12: Figure 24 Cortical bone maximum principal stress (model 2)
Figure 13: Figure 25 Cortical bone minimum principal stress ( model 1)
Figure 14: Figure 26 Cortical bone minimum principal stress (model 2)

Figure 15: Figure 27 Trabecular bone maximum principal stress (model1)
Figure 16: Figure 28 Trabecular bone maximum principal stress (model2)
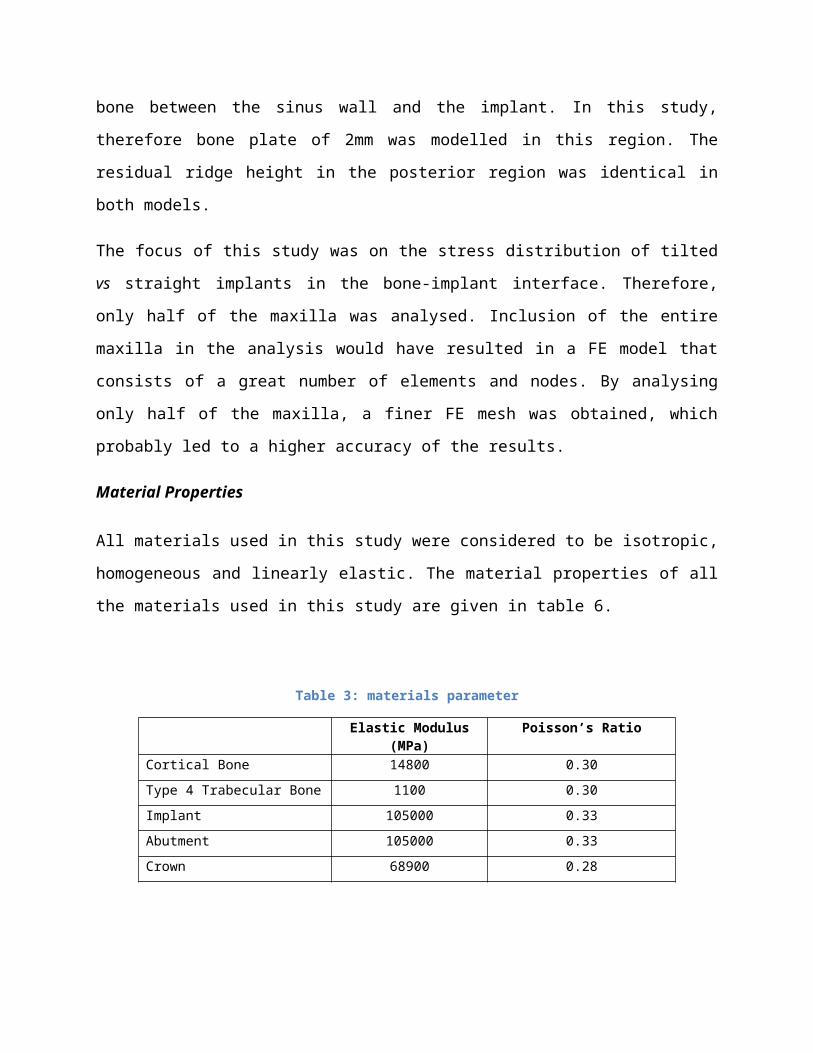
Figure 17: Figure 29 Trabecular bone minimum principal stress (model 1)
Figure 18: Figure 30 Trabcular bone minimum principal stress (model 2)

DISCUSSION
Overview
In recent years, field of implant dentistry has benefited from the computer-aided designs with
associated finite element analysis in achieving the proper implant and prosthesis design. Finite
element analysis (FEA) method is used in many biomechanical studies to investigate the stress
distributions in implant- bone complex (Akca et al., 2001, Menicucci et al., 2002, Mailath et al.,
1991). This method can precisely model the complex geometries mathematically and stress and
stain distributions may be obtained from a solution of equilibrium equations. Compared with the
other techniques (photo elastic model studies, strain gauge analysis on physical models) FEA
seems to be a superior tool in evaluating biomechanical loads on implants because it is capable
of simulating both isolated vertical and horizontal forces, as well as combined oblique loads
(Tepper et al., 2002).
The accuracy of a finite element study relies on the simulation of the model which represents the
natural tissues. In a finite element study, a two dimensional or a three dimensional model can be
used for an accurate prediction. Different patterns of stress values and magnitude were calculated
around the maxillary implants when an anatomic and a non-anatomic model are used (Simon et
al., 1977, Ismail et al., 1987). In 2-D system, it is assumed that out-of-plane deformations, strains
and stresses are negligible (DeTolla et al., 2000). Such models may lead to inconclusive data
with numerical failure. Therefore in this study a complex 3-D anatomical finite element model is
used to investigate the effect of tilted Vs short implants on stress distributions in edentulous
maxilla in the area of maxillary sinus. The complexity of the model in the study depends on two
factors: the spatially complex geometry of the maxilla, and oblique loads applied.
Findings
The model of the present study is derived from a model whose geometrical data are based on the
C.T scan of an adult male patient. The anatomical model of this study consists of the entire
maxilla, maxillary sinus, and cylindrical implants. However the reality is too complex to be
simulated completely in a numerical model (McElhaney et all., 1970, Carter & Spengler, 1978).
45

Therefore, in a finite element study several assumptions are made. The early attempts at
modelling dental implants resulted in unrealistic assumptions (DeTolla et al., 2000). Complex
reality is simplified assuming that proportion and relative effects reflect reality. For the
convenience of the study, material properties, loads, boundary and interface conditions are
simplified in the models. The structures are all assumed to be homogeneous and isotropic and to
possess linear elasticity. However in fact, the maxilla is inhomogeneous and subjected to
functional elastic deformations originating from masticatory forces, like other living tissues. In
reality the loads from mastication are dynamic and oblique relative to the occlusal surface of the
implants. The approximation of masticatory forces, loads and bone properties of bone has been
attributed to insufficient computer capacities (Ladd & Kinney, 1998). But recent improvement in
computer programming methods, computational power and digital imaging techniques have
allowed FEM to better analyse the biological structures (Ulrich et al, 1998).
The implants in the present study are simulated so that they are rigidly bounded to bone over the
entire surface and fully (100 %) osseointegrated, as in many other studies (Tepper et al., 2002,
Kawasaki et al. 2001, Van Oosterwyck et al 2002). However histomorphometric studies have
demonstrated that there is never 100 % osseointegration in bone. Simulating such an interface
would cause redistribution of the strains in the models. All these assumptions imply a certain
degree of uncertainty in all FE studies (del Valle et al, 1997). For this reason, only larger changes
in the strain levels are the interest of the study.
In the present study loads are applied to the occlusal surfaces of the superstructure in order to
simulate real masticatory movements. But with a finite element analysis, precise calculations
cannot be made, because there is great variation in the magnitude of the mechanical factors for
bone. And in addition, masticatory movements and their magnitude vary enormously between
the individuals (Glantz & Nilner, 1998). Theoretically, the problem of predicting loads on the
implants is a statistically indeterminate problem in mechanics. In most cases occlusal loads lie
between 100 N and 2400 N. Furthermore the masticatory loads are dynamic and oblique relative
to occlusal surfaces of the implants. However, in this study a static load of 300 N is applied with
250 inclinations (representing oblique loads). Simulating such a loading condition can be
considered as a realistic masticatory pattern. But when this is compared with the natural
mastication pattern, loads with inclinations relative to implants axis and sagittal plane may be
insufficient for complete simulation of oblique masticatory forces (Yaicioglu et al, 2015).
These variations in important biomechanical factors may lead to imprecise calculations.
Although the results of some other finite element studies (Holmes & Loftus 1997, Hoshaw et al,
1994; Spiekermann, 1994) demonstrated that the areas of higher stress concentrations (such as
implant neck) coincided with stress analysis predictions, the exact stress values causing
biological changes are not known (Lanyon, 1984).
In this study, similar to other studies using simplified models of human jaw, the model
compromises a cortical bone layer, trabecular bone layer and commercially pure titanium
implants. It is assumed that a homogeneous external layer of 0.75 mm cortical layer exists
around the cancellous bone. However, in reality the spatial distribution of the cortical and
trabecular bone is very different and inhomogeneous. The inhomogeneity of the cancellous bone
influences strongly the local elastic parameters. It is very important to choose the proper
parameters in stress analysis with FEM (Rong, 2002). The elastic modulus of cortical and
trabecular bone shows considerable variability. Therefore the elastic modulus of cortical and
trabecular bone are taken as an average of the several values cited in literature. These data are
either gained from mechanical testing or ultrasonic testing from human and bovine material.
However, even such a model may lead to failures in numerical data. Therefore, the inherent
limitations of the finite element stress analysis must be acknowledged. Since the reality is more
complex than the simulated models, a qualitative comparison among the models is advisable
rather than focusing on quantitative data from the finite element analysis (Stegaroiu et al., 1998).
Tilting of implant
Patients suffering from hard and soft tissue deficiencies are invariably the most difficult group of
patients to treat with osseointegrated implants. Severe atrophy of the maxilla, insufficient bone
quality and quantity of the arches complicate the use of osseointegrated implants in the maxilla
and usually necessitates advanced surgical techniques. However complicated surgical techniques
are not always practical because of patient related factors and the increased risk of
complications. Based on these considerations, tilting of dental implants and commercially
available dental implants are suggested as an alternative treatment method.
The benefits of tilting dental implants can be summarized are as follows (Krekmanov, 2000).
Firstly, it provides an end- support for the prosthetical restoration. This additional distal
anchorage helps to withstand occlusal loads by distributing them throughout the arch. It allows
the use of longer implants and reduces the cantilever length and broadens the prosthetic base. It
improves the cortical anchorage, indirectly the primary stabilisation of the implant, because the
implant follows a dense, bony structure.
According to the results of the present study, placement of short implant in the maxillary sinus
area, will affect the success rate of the implant, as all the stress will be absorbed by the trabecular
bone around the dental implant, and less on the cortical bone. Bone resorbtion will occur in the
trabecular bone all around the dental implant, which will cause failure of the implant. Hence, the
success rate is affected. (minimum principle stress in cortical bone is -550.42 MPa, minimum
principal stress in trabecular bone is -24.84 MPa).
Another result that was obtained by this study is that the use tilted implants in the maxillary sinus
area, will affect the survival rate of the implant, as bone reorbtion will be more in the cortical
bone leading to exposure of some threads but the implant remain anchoroged to the bone, while
less amount of stress in absorbed by the trabeular bone. (minimum principle stress in cortical
bone is -526.61MPa, minimum principal stress in trabecular bone is -44.67 MPa).

Conclusion
In conclusion, it is identified that tilted implants are a better alternative over straight implants in
the maxillary sinus area. The simulation of the model indicates that the short straight implants
have a compromised success rate, while tilted implants may have a decreased survival rate. The
application of a FE analysis comes with its own limitative as the study is limited to a computer
based simulation. It is further limited with restriction imposed in terms of material properties,
models, application type and load values. These factors together alter the results and hence, are
of limited nature in comparison with those in clinical testing. While the use of the FE analysis
has allowed in comparing the simulation of the short straight implants vs the tilted implants in
the bone in various situation with biomechanical aspects, it will be much helpful if it is supported
by clinical tests performed with qualitative data.
49

REFERENCES

Abraham, C. (2014). A Brief Historical Perspective on Dental Implants, Their Surface Coatings
and Treatments. Open dental journal, 8(1), pp.50-55.
Adell, R., Lekholm, U., Rockler, B. and Branemark, P. (1981). A I5-year study ofosseointegrated
implants in the treatment of the edentulous jaw. International Journal of Oral Surgery. 10.
Pp:387-416.
Alca, k. and Iplikçioğlu, H. (2001). Finite element stress analysis of the influence of staggered
versus straight placement of dental implants. International Journal of Oral Maxillofac Implants,
16(5), pp.722-30.
Anderson, L., Kosinski, T. and Mentag, P. (1991). Review of the intraosseous course of the
nerves of the mandible. Journal of Oral Implantology, 17(4), pp.394-403.
Annibali, S., Cristalli, M., Dell'Aquila, D., Bignozzi, I., La Monaca, G. and Pilloni, A. (2011).
Short Dental Implants: A Systematic Review. Journal of Dental Research, 9(1), pp.25-32.
Ardekian, L., Oved-Peleg, E., Mactei, E. and Peled, M. (2006). The clinical significance of sinus
membrane perforation during augmentation of the maxillary sinus. Journal of Oral Maxillofac
Surgery, 64(1), pp.277-282.
Ariji, Y., Kuroki, T., Moriguchi, S., Ariji, E. and Kanda, S. (1994). Age changes in the volume
of the human maxillary sinus: a study using computed tomography. Dentomaxillofac Radiol,
23(1), pp.163-168.
Baloh, R., Honrubia, V. and Jacobson, K. (1987). Benign positional vertigo: clinical and
oculographic features in 240 cases. Neurology, 37(1), pp.371-378.
Beer, F. P., (1981) Johnston ER. Mechanics of materials. New York (NY): McGraw-Hill.
Bilhan, H. (2008). An Alternative Method to Treat a Case With Severe Maxillary Atrophy by the
Use of Angled Implants Instead of Complicated Augmentation Procedures: A Case
Report. Journal of Oral Implantology, 34(1), pp.47-51.
Boyne, P. J., and James, R. A. (1980) Grafting of the maxillary sinus floor with autogenous
marrow and bone. Journal of Oral Surgery. 38. pp:613-616

Boyne, P.J. (1993) Analysis of performance of root-form endosseous implants placed in the
maxillary sinus. Journal of Long Term Efficiency in Medical Implants. 3. pp:143-159.
Bruggenkate, T., Asikainen, P., Foitzik, C., Krekeler, G. and Sutter, F. (1998). Short (6-mm)
nonsubmerged dental implants: results of a Multicenter clinical trial of 1 to 7 years. International
Journal of Oral Maxillofac Implants, 13(1), pp.791-798.
Carranza, F., Newan, M. and Takei, H. (2002). Carranza's clinical periodontology. 9th ed.
Philadelphia.
Carter, D. R. and Spengler, D. M. (1978) Mechanical properties and composition of cortical
bone. Clinical Orthop Related Research. 135. pp:192-264
Chanavaz, M. (1990). Maxillary sinus: anatomy, physiology, surgery, and bone grafting related
to implantology-eleven years of surgical experience (1979-1990). Journal of Oral Implantology,
16(1), pp.199-209.
Christopher, C. (2012). Implant rehabilitation in the edentulous jaw: the “All-on-4” immediate
function concept. Australasian Dental Practice, pp.138-148.
Das Neves, F.D, Fones, D., Bernardes, S.R, do Prado, C.J, and Neto, A.J. (2006) Short
implants--an analysis of longitudinal studies. International Journal of Oral Maxillofac Implants.
21. pp:86-93.
DeTolle, D. H., Andreana, S., Patra, A., Buhite, R., and Comella, B. (2000) The role of the finite
element model in dental implants. Journal of Oral Implantology. 2(26) pp:77- 81
Elian, N., Wallace, S., Cho, S.C., Jalbout, Z.N., and Froum, S. (2005) Distribution of the
maxillary artery as it relates to sinus floor augmentation. International Journal of Oral
Maxillofac Implants. 20. pp:784-787.
Ellegaard, B., Kolsen-Petersen, J., and Baelum, V. (1997) Implant therapy involving maxillary
sinus lift in periodontally compromised patients. Clinical Oral Implants Research. 8. pp:305-
315.
Esposito, M., et al. (2010) Effectiveness of sinus lift procedures for dental implant rehabilitation:
a Cochrane systematic review. European Journal of Implantology. 3(1). pp:7–26.
Fabbro, M.D., Bellini, C.M., Romeo, D., and Francetti, L. (2012) Tilted Implants for the
Rehabilitation of Edentulous Jaws: A Systematic Review. Clinical Implant Dentistry and Related
Research. 14(4). pp:612-21.
Fredholm, U., Bolin, A., and Andersson, L. (1993) Pre-implant radiographic assessment of
available maxillary bone support: Comparison of tomographic and panoramic technique.
Swedish Dental Journal. 17. pp:103-109.
Geng, J., Yan, W., and Xu, W. (2008) Application of the finite element method in ımplant
dentistry. Zhejiang: Springer.
Geng, J.P, Tan, K.B, and Liu, G.R. (2001) Application of finite element analysis in implant
dentistry: a review of the literature. Journal of Prosthetic Dentistry. 85(6). pp:585-98.
Georgiopoulos, B., Kalioras, K., Provatidis, C., Manda, M., and Koidis, P. (2007) The effects of
implant length and diameter prior to and after osseointegration: a 2-D finite element analysis.
Journal of Oral Implantology. 33(5). pp:243-56.
Geramipanah, F., and Sadighpour, L. (2012) Estimation of the safe distance between the implant
and an adjacent ttilted implant using trigonometry. Journal of Oral Implantology. 38(3). pp:289-
90.
Glesia, M. A. (2012) Anteriorly Tilted Implants in Maxillary Tuberosity: Avoiding the Maxillary
Sinus. CPOI. 3(1). pp:6-16.
Graves, S.L. (1994) The pterygoid plate implant: a solution for restoring the posterior maxilla.
International Journal of Periodontics Restorative Dentistry. 14. pp:512-523.
Greenstein, G., Cavallaro, J., Romanos, G. and Tarnow, D. (2008) Clinical recommendations for
avoiding and managing surgical complications associated with implant dentistry: a review.
Journal of Perio. 79(8). pp:1317-1329.

Gröning, F., Fagan, M., and O'higgins, P. (2012) Modeling the Human Mandible under
Masticatory Loads: Which Input Variables are Important? Anat Rec (Hoboken). doi:
10.1002/ar.22455.
Guan, H., van Staden, R., Loo, Y. C., Johnson, N., Ivanovski, S., and Meredith, N. (2009)
Influence of bone and dental implant parameters on stress distribution in the mandible: a finite
element study. International Journal of Oral Maxillofac Implants. 24. pp:866–876.
Guven, S., Atalay, Y., Asutay, F., Ucan, M., Dundar, S., Karaman, T. and Gunes, N. (2015).
Comparison of the effects of different loading locations on stresses transferred to straight and
angled implant-supported zirconia frameworks: a finite element method study. Biotechnology &
Biotechnological Equipment, 29(4), pp.766-772.
Handschel, J. et al. (2009) A histomorphometric meta-analysis of sinus elevation with various
grafting materials. Head Face Medicine. 5. pp:12
Himmlová, L., Dostálová, T., Kácovský, A., and Konvicková, S. (2004) Influence of implant
length and diameter on stress distribution: a finite element analysis. Journal of Prosthetic
Dentals. 91. pp:20–25.
Hiroshi, N and Toru, O. (1996) Titanium in Dentistry: Development and Research in the U.S.A.
Dental Materials Journal. 15(2). pp: 77-90.
Holmes, D.C. & Loftus, J.T. (1997) Influence of bone quality of stress distribution for
endosseous implants. Journal of Oral Implantology. 23(3).pp:104-111
Irish, J.D. (2004) A 5,500 year old artificial human tooth from a historical note. Journal of Oral
Maxillofac Implant, 19(5), pp. 645-647.
Ismail, Y.H., Pahountis, L.N. & Fleming, J.F. (1987) Comparison of two-dimensional and three-
dimensional finite element analysis of a blade implant. International Journal of Oral
Implantology. 4(2). pp:25-31
Jemat, A., Ghazali, M., Razali, M. and Otsuka, Y. (2015). Surface Modifications and Their
Effects on Titanium Dental Implants. BioMed Research International, 2015, pp.1-11.

John, C. Jr. and Gary, G. (2011) Angled Implant Abutments: A Practical Application of
Available Knowledge. Journal of American Dental Association.142. pp;150-158.
Juodzbalys, G., Kubilius, R., Eidukynas, V. and Raustia, A.M., (2005). Stress distribution in
bone: single-unit implant prostheses veneered with porcelain or a new composite material.
Implant dentistry, 14(2), 166-175.
Kawasaki, T., Takayaam, T., Yamada, T., and Notani, K. (2001) Relationship between stress
distribution and the shape of the alveolar residual ridge - three-dimensional behaviour of a
complete denture. Journal of Oral Rehabilitation. 28(10). pp:950-957.
Kenney, R., and Richards, M. W (1998) Photoelastic stress patterns produced by implant-
retained overdentures. Journal of Prosthet Dent. 80(5). pp: 559-64
Le Guéhennec, L., Soueidan, A., Layrolle, P., and Amouriq, Y. (2007) Surface treatments of
titanium dental implants for rapid osseointegration. Dental Mater. 23. pp:844–854.
Lee, C.Y, et al, (2011). The correlation of bone mineral density and histologic data in the early
grafted maxillary sinus: A preliminary report. Implant dentistry, 20(3), 202-214.
Lee, J. H, Frias, V., Lee, K.W., and Wright, R.F. (2005) Effect of implant size and shape on
implant success rates: a literature review. Journal of Prothet Dental. 94. pp:377-381.
Linkow, L. I. and Chercheve, R. (1970) Theories and Techniques of Oral Implantology, 1(2).
Saint Louis: The C. V Mosby Company.
Listl, S., and Faggion, C. M, Jr. (2010) An economic evaluation of different sinus lift techniques.
Journal of Clinical Periodontol. 37. pp:777-787.
Lum, L.B. (19991) A biomechanical rationale for the use of short implants. Journal of Oral
Implantol. 17. pp:126-131.
Lundgren, S., Andersson, S., Gualini, F., and Sennerby, L. (2004) Bone reformation with sinus
membrane elevation: a new surgical technique for maxillary sinus floor augmentation. Clinical
Implant Dental Relationship Research. 6. pp:165-173

Mailath, G., Schmid, M., Lill, W., and Miller J. (1991) 3D-Finite Element Analyse der
Biomechanik von rein implantatgetragenen Extensionsbrücken. 7. pp: 205-211.
Malo, P, Rangert, B, and Nobre, M. (2003) All-on-Four Immediate- with Brånemark System®
Implants for Completely Edentulous Mandibles: A Retrospective Clinical Study. Clinical
Implant Dentistry and Related Research. 5(1). pp:2-9.
Mandhane, S.S., and More, A.P. (2014) A review: evaluation of design parameters of dental
implant abutment. International Journal of Emerging Science and Engineering. 2. pp:64–67.
Mardinger, O., Abba, M., Hirshberg, A., and Schwartz-Arad, D. (2007) Prevalence, diameter and
course of the maxillary intraosseous vascular canal with relation to sinus augmentation
procedure: a radiographic study. International Journal of Oral Maxillofac Surgery. 36. pp:735-
738.
Marquezan, M., Osório, A., Sant' Anna, E., Souza, M.M., and Maia, L. (2012) Does bone
mineral density influence the primary stability of dental implants? A systematic review. Clinical
Oral Implants Research. 23. pp:767–774.
McCord, F. and Smales, R. (2012). Oral diagnosis and treatment planning: part 7. Treatment
planning for missing teeth. British Dental Journal, 213(7), pp.341-351.
McCord, F., and Smales, R. (2012) Oral diagnosis and treatment planning : part 7- Treatment
planning for missing teeth. British Dental Journal. 213. pp: 341-351.
McElhaney, J.H., Fogle, J.L., Melvin, J.W., Haynes, R.R., Roberts, V.L., and Alem NM. (1970).
Mechanical properties of cranial bone. Journal of Biomechanics. 3(5). pp:495-511
Mendonça, J. A, et al. (2013) A Retrospective Evaluation of the Survival Rates of Splinted and
Nonsplinted Short Dental Implants in Posterior Partially Edentulous Jaws. Journal of
Periodontol. 85(6) pp: 787-94
Menicucci, G., Mossolav, A., Mozzati, M., Lornzetti, M., and Preti, G. (2002) Tooth-implant
connection: some biomechanical aspects based on finite element analysis. Clinical Oral Implants
Research. 13(3). pp:334-341.
Mijiritsky, E., Mazor, Z., Lorean, A., and Levin, L. (2013) Implant diameter and length influence
on survival: interim results during the first 2 years of function of implants by a single
manufacturer. Implant Dent. 22. pp:394–398.
Misch, C. E, Suzuki, J.B., Misch-Dietsh, F.M., and Bidez, M.W. (2005) A positive correlation
between occlusal trauma and peri-implant bone loss: literature support. Implant Dental. 1(2).
pp:108-16.
Misch, C.E., Steigenga, J., Barboza, E., Misch-Dietsh, F., Cianciola, L.J., and Kazor, C. (2006)
Short Dental Implants in Posterior Partial Edentulism: A Multicenter Retrospective 6-Year Case
Series Study. Journal of Periodontol. 77(8). pp:1340–1347.
Monje, A., et al. (2013). A systematic review on marginal bone loss around short dental
implants. Clinical Oral Implant Research. pp:1-6.
Nedir, R. et al. (2010) Osteotome sinus floor elevation technique without grafting: a 5-year
prospective study. Journal of Clinical Periodontol. 37. pp:1023-1028
Oh, E, and Kraut, R.A. (2011) Effect of sinus membrane perforation on dental implant
integration: a retrospective study on 128 patients. Implant Dentology. 20. pp:13-19.
Oral Health Topics - Tooth, (2010) ADA: American Dental Association. [Online]. Available:
http://www.ada.org/2751.aspx?currentTab=2. [Accessed: 26-Oct-2016].
Paget’s Disease of Bone - Your Orthopaedic Connection, (2010) American Academy of
Orthopaedic Surgeons. [Online]. Available: http://orthoinfo.aaos.org/topic.cfm?
topic=A00076&return_link=0. [Accessed: 08-Nov-2016].
Park, Y.B, Jeon, H.S., Shim, J.S., Lee, K.W., and Moon, H.S. (2011) Analysis of the anatomy of
the maxillary sinus septum using 3-dimensional computed tomography. Journal of Oral
Maxillofac Surgery. 69. pp:1070-1078.
Pessoa, R.S., et al. (2010). Biomechanical Evaluation of Platform Switching in Different Implant
Protocols: Computed Tomography--Based Three-Dimensional Finite Element Analysis. Journal
of Oral & Maxillofacial Implants, 25(5).

Pieri, F., Aldini, N.N, Fini, M., Marchetti, C., and Corinaldesi, G. (2012) Rehabilitation of the
Atrophic Posterior Maxilla Using Short Implants or Sinus Augmentation with Simultaneous
Standard-Length Implant Placement: A 3-Year Randomized Clinical Trial. Clinical Implant
Dental Relationship Research. 14(6). DOI: 10.1111/j.1708-8208.2012.00451.
Pjetursson, B. E, Tan, W. C., Zwahlen, M., and Lang, N. P. (2008) A systematic review of the
success of sinus floor elevation and survival of implants inserted in combination with sinus floor
elevation. Journal of Clinical Periodontol. 35. pp:216-240.
Pjetursson, B. E. (2009) Transalveolar maxillary sinus floor elevation using osteotomes with or
without grafting material: Part II: Radiographic tissue remodeling. Clinical Oral Implants
Research. 20. pp:677-683.
Pommer, B. et al. (2012) Effect of maxillary sinus floor augmentation on sinus membrane
thickness in computed tomography. Journal of Periodontol. 83. pp:551-556.
Pommer, B., et al. (2012) Prevalence, location and morphology of maxillary sinus septa:
systematic review and meta-analysis. Journal of Clinical Periodontol.39. pp:769-773.
Raghoebar, G. M, and Vissink, A. (2003) Treatment for an endosseous implant migrated into the
maxillary sinus not causing maxillary sinusitis: case report. International Journal of Oral
Maxillofac Implants.18. pp:745749.
Rammelsberg, P., Schwarz, S., Schroeder, C., Bermejo, J. and Gabbert, O. (2012). Short-term
complications of implant-supported and combined tooth-implant-supported fixed dental
prostheses. Clinical Oral Implants Research, 24(7), pp.758-762.
Reich, K. M, Huber, C. D., Lippnig, W. R., Ulm, C., Watzek, G., and Tangl, S. (2011) Atrophy
of the residual alveolar ridge following tooth loss in an historical population. Oral Dis. 17.
pp:33-44
Renouard, F., and Nisand, D. (2006) Impact of implant length and diameter on survival rates.
Clinical Oral Implants Research. 17(2). pp:35-51.

Riben, C., and Thor, A. (2012) The Maxillary Sinus Membrane Elevation Procedure:
Augmentation of Bone around Dental Implants without Grafts-A Review of a Surgical
Technique. International Journal of Dentists. pp:105-483.
Rosano, G., Taschieri, S., Gaudy, J.F, and Del Fabbro, M. (2009) Maxillary sinus
vascularization: a cadaveric study. Journal of Craniofac Surgery. 20. pp:940-943.
Rosano, G., Taschieri, S., Gaudy, J.F., Weinstein, T., and Del Fabbro, M. (2011) Maxillary sinus
vascular anatomy and its relation to sinus lift surgery. Clinical Oral Implants Research. 22(7).
pp:711-715.
Rosen, A., and Gynther, G. (2007) Implant Treatment without Bone Grafting in Edentulous
Severely Resorbed Maxillas: A Long-Term Follow-Up Study. Journal of Oral and Maxillofacial
Surgery. 65(5). pp:1010-16.
Saber, S., Ghasemi, S., Koodaryan, R., Babaloo, A. and Abolfazli, N. (2015). The Comparison of
Stress Distribution with Different Implant Numbers and Inclination Angles In All-on-four and
Conventional Methods in Maxilla: A Finite Element Analysis. Journal of Dental Research,
Dental Clinics, Dental Prospects, 9(4), pp.246-253.
Sagat, G., Yalcin, S., Gultekin, B.A, and Mijiritsky, E. (2010) Influence of arch shape and
implant position on stress distribution around implants supporting fixed full-arch prosthesis in
edentulous maxilla. Implant Dental Research. 19(6). pp:498-508.
Sarfaraz, H., Shenoy, K., Hussain, A. and Sucheta, P. (2015). A Comparison of Four Implant
Abutment Connection Designs on the Stress Distribution Pattern using 3D Finite Element
Analysis. International Journal of Oral Implantology & Clinical Research, 6, pp.1-8.
Scala, A., Botticelli, D., Faeda, R. S., Garcia-Rangel, I, Jr., Americo de Oliveira, J., and Lang, N.
P. (2012) Lack of influence of the Schneiderian membrane in forming new bone apical to
implants simultaneously installed with sinus floor elevation: an experimental study in monkeys.
Clinical Oral Implants Research. 23. pp:175-181.
Schwarz, M.S. Rothman, S.L. Chafetz, N. and Stauts, B. (1990) Pre-operative diagnostic
radiology for the tissueintegrated prosthesis. In: Laney, W.R, and Tolman, D.E, eds. Tissue

integration in oral, orthopedic, and maxillofacial reconstruction. Chicago: Quintessence: pp. 68-
79.
Searson, L.J. (2005) History and development of dental implants. In: Narim L, Wilson HF,
editors. Implantology in general dental practice. Chicago: Quintessence Publishing Co. pp. 19–
41.
Seoane, J. et al. (2012) Membrane Perforation in Sinus Floor Elevation - Piezoelectric Device
versus Conventional Rotary Instruments for Osteotomy: An Experimental Study. Clinical
Implant Dental Relationship Research. 15(6). pp: 867-873. DOI: 10.1111/j.1708-
8208.2012.00447.
Shahrul, H. et al. (2011) Cellular and Molecular Changes in Orthodontic Tooth Movement. The
Scientific World Journal. 11, pp:1788–1803
Sharan, A, and Madjar, D. (2008) Maxillary sinus pneumatization following extractions: a
radiographic study. International Journal of Oral Maxillofac Implants. 23(1). pp:48-56.
Shen, W. L, Chen, C. S, and Hsu, M. L. (2010) Influence of implant collar design on stress and
strain distribution in the crestal compact bone: a three-dimensional finite element analysis.
International Journal of Oral Maxillofac Implants. 25(5). pp:901-910.
Simon, B. R, et al. (1977) Evaluation of one, two, three-dimensional finite element and
experimental models of international fixation plates. University of Arizona. pp.79-86.
Sohn, D. S, Lee, J. S, An, K. M, and Choi, B. J. (2009) Piezoelectric internal sinus elevation
(PISE) technique: a new method for internal sinus elevation. Implant Dental. 18(1). pp:458-463.
Srinivasan, M, Vazquez, L, Rieder, P, Moraguez, O, Bernard, J-P, and Belser, U. C. (2013)
Survival rates of short (6 mm) micro-rough surface implants: a review of literature and meta-
analysis. Clinical Oral Implants Research. 25(5). pp:539–545.
Stanford, C. M. (2008) Surface modifications of dental implants. Australasian Dental Journal.
53(Suppl 1). pp:S26–S33
Stegaroiu, R., Sato, T., Kusakari, H., and Miyakawa, O. (1998) Influence of restoration type on
stress distribution in bone around implants: a three-dimensional finite element analysis,
International Journal of Oral Maxillofac Implants. 13(1). pp:82-90
Strid, K. G. (1985) Radiographic results. In Branemark, P.I, Zarb, G., and Albrektsson, T. eds.
Tissue-integrated prostheses: Osseointegration in dentistry. Chicago: Quintessence, pp. 187-98.
Sullivan, R.M. (2001) Implant dentistry and the concept of osseointegration: a historical
perspective. Journal of California Dental Association. 29(11). pp:737–745.
Telleman, G., Raghoebar, G. M., Vissink, A., Hartog den, L., Huddleston Slater, J., and Meijer
HJA. (2011) A systematic review of the prognosis of short. Journal of Clinical Clin
Periodontol.38(7). pp:667–676.
Tepper, G., Haas, R., Zechner, W., Krach, W., and Watzek, G. (2002) Three-dimensional finite
element analysis of implant stability in the atrophic posterior maxilla. Clinical Oral Implants
Research.13(6). pp.657-665
Testori, T., Rosano, G., Taschieri, S., and Del Fabbro, M. (2010) Ligation of an unusually large
vessel during maxillary sinus floor augmentation. A case report. European Journal of Oral
Implantology. 3. pp.255-258.
Timmenga, N. M, Raghoebar, G. M, Boering, G., and Van-Weissenbruch, R. (1997) Maxillary
sinus function after sinus lifts for the insertion of dental implants. Journal of Oral Maxillofac
Surgery. 55(9). pp:936-939.
Tong, D. C., Rioux, K., Drangsholt, M., and Beirne, O. R. (1998) A review of survival rates for
implants placed in grafted maxillary sinuses using meta-analysis. International Journal of Oral
Maxillofac Implants. 13. pp:175-182
Toscano, N.J., Holtzclaw, D., and Rosen, P. S. (2010) The effect of piezoelectric use on open
sinus lift perforation: a retrospective evaluation of 56 consecutively treated cases from private
practices. Journal of Periodontol. 81(1). pp.167-171. doi: 10.1902/jop.2009.090190.

Truedsson, A., Hjalte, K., Sunzel, B., and Warfvinge, G. (2012) Maxillary sinus augmentation
with iliac autograft - a health-economic analysis. Clinical Oral Implants Research. 24(10).
pp.1088-1093. DOI: 10.1111/j.16000501.2012.02515.
Ulm, C. W., Solar, P., Krennmair, G., Matejka, M., and Watzek, G. (1995) Incidence and
suggested surgical management of septa in sinus-lift procedures. International Journal of Oral
Maxillofac Implants. 10. pp.462465.
Vanden-Bergh, J. P, Ten-Bruggenkate, C. M, Disch, F. J, and Tuinzing, D. B. (2000) Anatomical
aspects of sinus floor elevations. Clinical Oral Implants Research.11. pp.256-265.
Van-Oosterwyck, H., Duyck, J., Vander-Sloten, J., Van der Perre, G., and Naert, I. (2002) Peri-
implant bone strains in cases of dehinscence: a finite element study. Clinical Oral Implants
Research. 13. pp.327-333.
Verri, F., Santiago Júnior, J., Almeida, D., Verri, A., de Souza Batista, V., Lemos, C., Noritomi,
P. and Pellizzer, E. (2015). Three-Dimensional Finite Element Analysis of Anterior Single
Implant-Supported Prostheses with Different Bone Anchorages. The Scientific World Journal,
2015, pp.1-10.
Vina-Almunia, J, Penarrocha-Diago, M. (2009) Influence of perforation of the sinus membrane
on the survival rate of implants placed after direct sinus lift: Literature update. Medicina Oral
Patologia Oral y Cirugia Bucal. 14. pp:133-136.
Wallace, S. S., and Froum, S. J. (2003) Effect of maxillary sinus augmentation on the survival of
endosseous dental implants: A systematic review. Ann Periodontol.8. pp:328-343.
Wheeler, R. (1963). Wheeler's atlas of tooth form. 1st ed. Philadelphia and London:
W.B.Saunders, p.26.
White, S., Heslop, E., Hollender, L., Mosier, K., Ruprecht, A. and Shrout, M. (2001). Official
report of the American Academy of Oral and Maxillofacial Radiology. Oral Surgery, Oral
Medicine, Oral Pathology, Oral Radiology.
Wishan, M., Bahat, O. and Krane, M. (1988). Computed tomography as an adjunct in dental
implant surgery. International Journal of Periodontics Restorative Dentistry, 8, pp.30-47.

Yazicioglu, D., Bayram, B., oguz, y., Cinar, D. and Uckan, S. (2015). Stress Distribution on
Short Implants at Maxillary Posterior Alveolar Bone Model with Different Bone-to-Implant
Contact Ratio: Finite Element Analysis. Journal of Oral Implantology.
Yeshwante, B., Patil, S., Baig, N., Gaikwad, S., Swami, A. and Doiphode, M. (2015). Dental
Implants- Classification, Success and Failure –An Overview. IOSR Journal of Dental and
Medical Sciences (IOSR-JDMS), 14(5), pp.01-08.
Zampelis, A., Rangert, B. and Heijl, L. (2007). Tilting of splinted implants for improved
prosthodontic support: A two-dimensional finite element analysis. The Journal of Prosthetic
Dentistry, 97(6), pp.S35-S43.
