· web viewaccording to a.s.p.e.n. guidelines, protein should not be restricted as a...
TRANSCRIPT

ALCOHOLIC LIVER DISEASE: Medical Nutrition Therapy
Sarah TefftSodexo Philadelphia Dietetic InternshipFall 2012-Spring 2013
(1)

Table of ContentsI. Abstract………………………………………………………………………………3
II. Introduction………………………………………………………………………….5
III. The Liver……………………………………………………………………………...6
Anatomy
Metabolic Functions
IV. Alcoholic Liver Disease……………………………………………………………..10
Risk Factors
Alcohol Metabolism
Maldigestion and Malabsorption
Inflammation and Oxidative Stress
Diagnosis
V. Medical Nutrition Therapy………………………………………………………...32
Role of the Registered Dietitian
Completing the Nutrition Assessment
Nutrition Intervention
Recommendations
VI. Presentation of the Patient…………………………………………………………43
Description of the Patient
Timeline
Initial Assessment
1st Follow-Up
2nd Follow-Up
3rd Follow-Up
4th Follow-Up
VII. Critical Comments……………………………………………………………….…60
VIII. Summary…………………………………………………………………………….63
IX. Medical Term Glossary……………………...……………………………………..65
X. Medication Bibliography…………………………...………………………………68
XI. Index A: Subjective Global Assessment…………………………………………..72
XII. References………………………………………………………………………...…73
2

I. Abstract
Alcoholic liver disease (ALD) is sometimes referred to as liver disease due to alcohol,
alcoholic cirrhosis, alcoholic hepatitis, or Laennec’s cirrhosis (2). It is the most common liver
disease in the United States (3). About 2 million people in the U.S. are affected by ALD (4).
Approximately two-thirds of the adult American population drinks alcohol and more than 10%
of people abuse or are dependent on alcohol (20, 6,). More men than women abuse alcohol at a
ratio of approximately 2:1 (6). The typical age range of patients, with a diagnosis of ALD, is
between 40 and 50 years with the majority occurring before the age of 60 (7). Though this
disease can have devastating effects on the human body, there are treatments and therapies
available to remedy the complications and damages caused by ALD. Among these, nutrition
plays an important and integral role in managing and even reversing this disease process.
In this case study, a 62 year old woman with a long history of alcohol abuse was brought
in to the Emergency Department for complaints of chest pain. She was diagnosed as having
alcoholic ketoacidosis and alcoholic cirrhosis. She was sent to the Intensive Care Unit (ICU)
where they began more comprehensive treatment. During her 22 day hospital stay she also
contracted a urinary tract infection (UTI), sustained an iatrogenic pneumothorax, and developed
acute kidney injury. The patient also suffered from multiple complications that often accompany
alcoholic liver disease including hepatic encephalopathy which resulted in altered mental status.
An initial nutrition assessment was completed on December 12, 2012. This was one day
after the patient’s admission to the hospital. The assessment included anthropometric
measurements, biochemical data, physical exam findings, medical history, list of current
medications, and calculations for nutrients and fluids needed. Along with the information
gathered, the Nutrition Care Practice Guidelines were followed to establish a nutrition diagnosis,
3

implement interventions, and establish monitoring and evaluation plans. Four follow-up nutrition
assessments were completed on December 10th, 13th, 18, and 24th throughout the patients stay at
the hospital. She was discharged on December 28. 2012.
The patient was ordered an NPO diet on admission. After the placement of a small bore
feeding tube, she started on a tube feedings of Nepro 1.8 at 35 mm/hour for 20 hours per day.
She was then advanced to a Dysphagia 2 diet after a swallow evaluation by the speech language
pathologist (SLP). Her diet was then advanced to mechanical soft as her mental status improved.
At discharge the patient was clinically and hemodynamically stable.
4

II. Introduction
I chose alcoholic liver disease as the focus for my case study for a number of reasons.
First, I wanted to know more about liver disease and it’s affects on the body in greater detail.
Alcohol liver disease can go undetected for a long period of time and frequently the patient will
be asymptomatic during the early stages of the disease. The disease process can continue to
progress for years before a patient show any signs or symptoms resulting from complications of
the disease. It is difficult for clinicians to make a definitive and accurate diagnosis because of the
nature of the disease. The disease is also a result of addiction and for this reason, both the
diagnosis and treatment of ALD requires an interdisciplinary approach. The disease is directly
linked to behavior, lifestyle choices, and other environmental factors. For this reason, the
primary treatment, which is cessation from drinking, is a difficult one to achieve.
The liver is one of the most complex organs in the body. Resulting damage stemming
from the diseased liver, is widespread, detrimental, and often times irreversible. Fortunately, if
the patient is able to stop drinking, there are medical treatments and nutritional interventions that
can help to restore healthy functioning of the liver and essentially the body as a whole. I hope
through researching the disease process, examining the current treatments, available
interventions, and information gathered through the study of this patient, to gain a better
understanding of ALD and the implications for nutrition therapy.
5

III. The Liver
Anatomy:
The liver is the largest organ in the abdominal cavity and the most metabolically complex
(3). The liver also has the unique ability to regenerate itself. Only 10 to 20% of a functioning
liver is needed to sustain life, however complete removal of the liver would result in death within
24 hours (3). It consists of individual microscopic functional units called lobules. The liver
weighs approximately 1800 grams in men and 1400 grams in women. The surfaces of the liver
are smooth and convex in the superior, anterior and right lateral regions. Indentations from the
colon, right kidney, duodenum and stomach are apparent on the posterior surface (8).
It is located in the right upper quadrant of the body. The line between the vena cava and
gallbladder divides the liver into right and left lobes. The Falciform ligament divides the liver in
to the right and left atomic lobes. Each lobe has an independent vascular and duct supply. The
lobes are divided into eight segments each containing portal vessels, ducts, and hepatic veins (8).
The portal venous system extends from the intestinal capillaries to the hepatic sinusoids.
This system carries blood from the abdominal gastrointestinal tract, the pancreas, the gallbladder
and the spleen back to the heart, flowing through the liver. The largest vessel in this system is the
portal vein (8).
The portal vein supplies 70% of the blood flow to the normal liver, but only 40% of the
liver’s oxygen supply. The remainder of the blood comes from the hepatic artery, and blood from
both vessels mixes in the sinusoids. The liver receives an extraordinary volume of blood;
approximately 1.5 liters per minute (8).
6

It is also part of the biliary system along with the gallbladder and associated ducts. This
system is sometimes referred to as the biliary tree. The liver, along with the pancreas, is essential
to digestion (9).
Metabolic Functions
There are more than 500 functions the liver performs in the body. Hepatocytes, cells in the
liver, are responsible for these metabolic functions (3). A selection of the liver’s many functions
will be discussed in the following section.
One highly important role of the liver is the regulation of carbohydrate homeostasis in the
body. Galactose and fructose, products of carbohydrate digestion, are converted into glucose.
Glucose is then stored in the liver as glycogen and returned to the blood when glucose levels are
low (3). Hepatocytes also contain enzymes that allow for the synthesis of glucose from
precursors such as amino acids, pyruvate, and lactate through the process of gluconeogenesis (6).
The liver is involved in lipid metabolism as well, where fatty acids are broken down and
triglycerides are synthesized. Triglyceride synthesis occurs when carbohydrate intake exceeds
energy needs. Triglycerides in adipose tissue are hydrolyzed to release fatty acids. In the blood,
the fatty acids are bound to albumin and removed by the hepatocyte (10).
As an important contributor to the digestive system, the liver secretes bile salts which are
necessary for fat digestion and absorption (9). The liver is also responsible for cholesterol
metabolism by synthesizing bile salts from cholesterol, which are secreted in bile and mixed with
intestinal contents after a meal. Triglycerides enter the duodenum in the form of an emulsion, the
7
Figure 1. Anatomy of the portal venous system (8).

surface of which is covered by a layer of phospholipids and proteins that must be removed by
bile salts in order for lipolysis to take place. The products of lipolysis form micelles with bile
salts and promote the intestinal uptake of long-chain fatty acids. In the absence of bile, however,
the absorption of short- and medium-chain fatty acids occurs. After the uptake of fatty acids, the
bile salts are recycled through enterohepatic circulation. Some bile salts are reabsorbed from the
distal small bowel by an active, sodium-dependent process. Other bile salts are absorbed by
passive diffusion from the proximal small bowel. The liver extracts these reabsorbed bile salts
from the portal vein blood and returns them to the biliary tree. The biliary tree is made up of the
bile ducts and the gallbladder. Hepatic synthesis of bile salts replenishes the amount of bile salts
that are not reabsorbed or are excreted in the feces (10).
The liver is central to the breakdown and synthesis of protein. Plasma proteins such as
albumin, transferrin, and coagulation factors make up approximately half of the protein
synthesized in the liver. The secretion of plasma proteins called thrombopoietin which are
involved in platelet formation and hepcidin which inhibits intestinal iron uptake as well as the
production of enzymes and insulin-like growth factor-I which stimulates growth are all functions
of the liver. Protein synthesis in the liver is affected by nutritional status as well as hormones,
and alcohol. Insulin and steroids stimulate protein synthesis whereas glucagon promotes their
degradation.
8

The liver is involved in the
storage, activation, and transport of
many vitamins and minerals. All fat
soluble vitamins, vitamin B12,
minerals, including zinc, iron, copper,
and magnesium are stored in the liver
(3). Vitamin D is activated by the liver
as well as by the kidneys.
Bilirubin, which is the
metabolic end product from the
destruction of red blood cells, is also
excreted by the liver (3). Detoxifying
the body of drugs, alcohol, hormones,
removing bacteria and debris from the blood is another function of the liver (12,9). Hepatocytes
detoxify ammonia by converting it to urea which is then mostly excreted by the kidneys (3).
IV. Alcoholic Liver Disease
Risk Factors
Several variables predispose a person to alcoholic liver disease. The main factors that
contribute to ALD are quantity and duration, usually more than eight years of use, gender,
genetic and metabolic traits, and nutritional status. The amount of alcohol ingested, independent
from the type of alcoholic beverage that is consumed, is the most important risk factor for the
9
Figure 2. The liver and associated biliary tree (11)

development of alcoholic liver disease (5). Women are more susceptible to ALD even when
adjustments for body size are accounted for (6). It takes less time and lower doses of alcohol
exposure to cause liver damage in females than in males (4). One reason for the increased
susceptibility may be that women have less alcohol dehydrogenase in their gastric mucosa.
Alcohol dehydrogenase is an enzyme necessary for the oxidation of alcohol and therefore the
rate of alcohol metabolism is decreased in females (6). Although the majority of patients are
males, men are twice as likely as women to abuse alcohol (7).
Protein-energy malnutrition increases susceptibility as well as a diet high in unsaturated fat
and obesity (6). Other factors include type of alcohol consumed, drinking pattern, ethnicity, iron
overload, simultaneous exposure to other drugs, immunologic factors, and infections such as
viral hepatitis (5). Hispanics, more than any other ethnicity, have an increased risk of developing
ALD (7).
Genetic alterations to alcohol-metabolizing enzymes, including alcohol dehydrogenase
and acetaldehyde dehydrogenase, can affect the likelihood of developing ALD as well (5).
Environmental factors such as availability of alcohol and social acceptability of alcohol use can
also increase the prevalence of ALD (13).
However, not all heavy drinkers develop ALD and a person does not have to get drunk in
order for the disease to develop (2). Up to 40% of individuals with modest alcohol intake, that is
less than or equal to 10 grams per day, exhibit fatty changes to their liver (6).
Alcohol content is estimated by multiplying the beverage volume in milliliters times the
percentage of alcohol. Therefore 40 mL of an 80 proof beverage, or 40% alcohol contents, is 16
mL. Each mL contains about 0.79 grams of alcohol (6). Based on an autopsy series of men, 40
grams of alcohol per day is necessary to produce pathologic changes of ALD. This would be
10

equivalent to three to six cans of beer, three to six shots of hard liquor, or four to eight glasses of
wine per day (6). One in five heavy drinkers develops alcoholic hepatitis, and one in four heavy
drinkers develops cirrhosis. A daily dose of more than 60 grams of alcohol in men and 20 grams
in women significantly increases the risk of cirrhosis (13). In practice most patients with
alcoholic hepatitis drink more than 100 grams per day with 150-200 grams per day being
common (7).
Table 1. Alcohol Content of Some Common Beverages (3)Drink Amount (oz) Absolute Alcohol (g)Beer 12 12Wine 5 12Liquor (80 proof) 1.5 12
Alcohol Metabolism
The liver and the gastrointestinal tract are the main sites of ethanol metabolism. Ethanol
is the type of alcohol in alcoholic beverages. It is easily absorbed from the stomach but the
majority is absorbed by the small intestine and cannot be stored in the body. A fraction of the
alcohol ingested is degraded as it passes through the gastric mucosa, but most is metabolized by
the liver (6).
Within the liver there are two main oxidative pathways of alcohol metabolism. One is
through the use of alcohol dehydrogenase (ADH) and the second is with cytochrome P-450
(CYP) 2E1. To a lesser degree, alcohol is also catabolized by a third pathway, the microsomal
enzyme oxidation system (MEOS) (6).
The major oxidative pathway for alcohol metabolism in the liver involves ADH (14).
Alcohol dehydrogenase is a hepatocyte enzyme that converts alcohol to acetaldehyde.
Acetaldehyde is a toxic byproduct of alcohol metabolism that causes damage to the structure and
function of mitochondrial membranes (3). Acetaldehyde is produced with the transfer of
11

hydrogen to nicotinamide adenine dinucleotide (NAD), reducing it by two electrons to form
(NADH). This altered proportion of NAD to NADH inhibits gluconeogenesis and fatty acid
oxidation, therefore contributing to fatty liver (13).
CYP 2E1 is the main enzyme involved in ethanol metabolism when there are elevated
concentrations of ethanol. Through this oxidative pathway, ethanol is also converted to
alcetaldehyde. Through this pathway, free radicals are generated by the oxidation of
nicotinamide adenine dinucleotide phosphate (NADPH) which is the reduced form to NADP
which is the oxidized form (3).
The alternative pathway for ethanol metabolism is the MEOS. This pathway also
oxidizes ethanol to form acetaldehyde and requires the oxidation of NADPH to NADP. In most
individuals this pathway only plays a minor role but in chronic alcohol consumption the activity
of this pathway is increased (14). When induced, the MEOS pathway can account for 20% of
alcohol metabolism (6). This pathway generates harmful reactive oxygen species which increases
oxidative stress and the formation of oxygen free radicals (6). Due to the oxidation of NADPH to
NADP, adenosine triphosphate (ATP) is used and heat dissipated. Some researchers believe this
contributes to increased resting energy expenditure in chronic alcohol drinkers (14).
Alcetaldehyde, formed from these pathways, is then metabolized mainly by aldehyde
dehydrogenase 2 (ALDH2) to form acetate which is released into the blood and NADH. Reactive
oxygen species are also produced which contribute to oxidative stress (13, 14).
Many metabolic disturbances occur because of this excess NADH. These include
increased lactic acid in the blood, acidosis, hyperuricemia, ketonemia, and hyperlipidemia. The
tricarboxylic acid (TCA) cycle is also depressed as it requires NAD. The mitochondria in turn,
use hydrogen from ethanol rather than from the oxidation of fatty acids to produce energy via the
12

TCA cycle, which leads to decreased fatty acid oxidation and the accumulation of triglycerides.
Hypoglycemia can also occur in early alcoholic liver disease secondary to the suppression of the
TCA cycle along with decreased gluconeogenesis (3). However, it is still not completely
understood how alcohol metabolism itself is linked to the genesis of ALD (15). It is also not
understood why only a minority of alcoholics develop alcoholic hepatitis (7).
Maldigestion/Malabsorption
Alcoholics are malnourished because they either eat poorly or alcohol metabolism
prevents them from properly absorbing, digesting, and using nutrients (4). Portal hypertension, a
common complication of chronic alcoholism, also leads to impaired absorption of nutrients (16).
Classic effects of malnutrition from alcoholism include Wernicke’s encephalopathy, Korsakoff
psychosis, muscle wasting, weight loss, and liver disease (4).
Fat or triglycerides accumulate throughout the hypatocytes for a number of reasons. First,
the export of fat from the liver is compromised. This is because hepatic fatty acid oxidation and
lipoprotein production is decreased. Second, due to the decreased export of fat from the liver,
peripheral lipolysis is increased and the input of fat is increased. This, in turn, increases
triglyceride synthesis and results in hyperlipidemia (6). Glucose tolerance is usually abnormal in
these patients and has been linked to insulin resistance. During fasting, fatty acid oxidation
appears to supplement glucose due to depleted glycogen stores found in a fatty liver (10).
Another reason is acetyl CoA, a product of glycolysis, may not be needed for oxidative
phosphorylation and therefore is converted to fatty acids and ultimately triglycerides. These
triglycerides are then transported to the adipose tissues as part of very-low-density lipoproteins
(VLDLs) (10). In summary, hepatic steatosis is caused by the following metabolic disturbances:
increased mobilization of fatty acids from adipose tissue; increased hepatic synthesis of fatty
13

acids; decreased fatty acid oxidation; increased triglyceride production; and trapping of
triglycerides in the liver (3).
Bile salts involved in fat digestion are decreased resulting in impaired micelle formation
which leads to fat absorption abnormalities. This is exacerbated in patients with underlying
pancreatic insufficiency and can result in steatorrhea and poor absorption of fat-soluble vitamins,
thiamin, folic acid, vitamin B12, and zinc (J, K). Thiamin deficiency is the most common
vitamin deficiency in alcoholics and is responsible for both Wernicke’s encephalopathy and
Korsakoff psychosis (3).
Heavy alcohol consumption leads to decreased levels of hepatic vitamin A. Defects have
also been noted in the phosphorylation of thiamin, the synthesis of retinol-binding protein, and
the conversion of vitamin D to its active form. Induced hepatic microsomes may enhance the
breakdown of both retinol and retinoic acid related to vitamin A (10).
Protein loss in patients with ALD is common and can be attributed to the following:
diuretic use or the procedure of paracentesis both commonly indicated for the treatment ascites,
the use of lactulose which is prescribed in to alter intestinal flora, blood loss from esophageal
and gastric varices, and ulcerations in the intestinal lumen (16). Glycogen stores are depleted in
cirrhotic liver and therefore peripheral muscle will provide amino acids for gluconeogenesis.
Therefore patients with alcoholic cirrhosis go into an early starvation mode after only 12 hours
of fasting while normally it takes 2 days in normal subjects (17).
Metabolism of protein is also defective in patients with ALD and contributes to loss of
protein stores. Metabolic processes affected include hepatic synthesis of export proteins,
decreased urea synthesis, and decreased metabolism of aromatic amino acids. A decrease in
plasma proteins may cause lower levels of albumin and can exacerbate ascites in patients who
14

have portal hypertension. Lower levels of coagulation factors may predispose patients to risk of
gastrointestinal bleed. The liver’s inability to detoxify ammonia and the imbalanced amino acid
levels could increase the risk for hepatic encephalopathy (10).
The effect of ethanol on protein metabolism, measured as nitrogen balance, is nitrogen
sparing when ethanol is given as additional calories but causes increased urea when given as a
substitute for carbohydrates. Ethanol interfers with amino acid absorption in the gut. It causes
impaired hepatic amino acid uptake, decreased gluconeogenesis, impaired synthesis of
lipoproteins, albumin, and fibrinogen. Over time ethanol impairs protein secretion from the liver
(10).
Inflammation and Oxidative Stress
Alcohol-induced liver injury is an immunological response of the liver; neutrophils
damage liver cells through cytotoxicity (4). Inflammation results from the formation of
neoantigiens, resulting from the binding of alcohol oxidation products, such as acetaldehyde, to
liver cell proteins. There is also an accumulation of neutrophils and other white blood cells that
are attracted by lipid perioxidative damage and these neoantigens. The white blood cells then
secrete inflammatory cytokines causing inflammation (6).
Worsening inflammation leads to cell necrosis and apoptosis which results in hepatocyte
loss. Stellate cells in the liver proliferate and transform into myofibroblasts which produce
excess collagen. As a result the sinusoids narrow limiting blood flow within the liver. Fibrosis
narrows the terminal hepatic venules or central veins, compromising distribution of blood within
the liver, which contributes to portal hypertension. Extensive fibrosis is associated with an
attempt at regeneration, resulting in liver nodules. This process culminates into cirrhosis (6).
15

Chronic alcohol intake also activates hepatic macrophages which then produce tumor
necrosis factor-alpha (TNF-alpha). TNF-alpha induces mitochondria to increase production of
reactive oxygen species or peroxides. This oxidative stress promotes hepatocyte necrosis which
is exacerbated by probable lack of antioxidants, particularly in the protective antioxidants
glutathione, vitamins A and E. Free radicals initiate lipid perioxidation which causes
inflammation and fibrosis (13).
Bacteria in the gut produce endotoxins which are normally detoxified by the liver but the
impaired liver function increases the presence of these endotoxins. In response, liver
macrophages release free radicals, increasing oxidative damage (6). If there is an accumulation
of iron in the liver, this can also contribute to oxidative damage.
Diagnosis
The diagnosis of ALD is based on a combination of factors including history of alcohol
intake, clinical evidence of liver disease, and laboratory abnormalities (5). No single laboratory
marker definitively establishes alcohol as the cause of liver disease (5).
A variety of scoring systems have been used to assess the severity of ALD. Patients can
be screened for alcoholism using the CAGE questionnaire which stands for need to Cut down,
Annoyed by criticism, Guilty about drinking, and need for a morning Eye-opener (6).
16
The CAGE questionnaire 1. Have you ever felt you should cut down on your drinking?2. Have people annoyed you by criticizing your drinking?3. Have you ever felt bad or guilty about your drinking?4. Have you ever had a drink first thing in the morning to steady yournerves or to get rid of a hangover (eye-opener)?Scoring: Each response is scored as 0 or 1, with a higher score indicative of alcohol-related problems, and a total of greater than or equal to 2 being clinically significant.
Table 2. CAGE Questionnaire (18).

Both the Maddrey discriminant function and the Model for End-Stage Liver Disease
(MELD) score can be useful in predicting short-term mortality in patients with alcoholic
hepatitis (13). The MELD score predicts short-term survival in patients with cirrhosis and is used
to select patients for liver transplantation. The MELD classification is more difficult to apply for
every patient but is widely used and is generally accepted among physicians. This method also
excludes undernutrition as a contributor to the score (7).
The Maddrey’s discriminant function is calculated as total bilirubin (in mg/dL) + 4.6 x
prothrombin time in seconds prolonged. This tool was published in 1978 based on laboratory and
clinical data collected from studies in the 1960’s and 1970’s. It was then modified in 1989 so that
a discriminant function score of greater than 32 signified severe alcoholic hepatitis and the need
for drug treatment (7). The Lille model is another prognostic scoring system that is more
accurate than the MELD score for predicting death at six months in patients with severe
alcoholic hepatitis. The Lille score is based on pretreatment data and serum levels of bilirubin as
compared to a seven day course of corticosteroids. This score is designed to help the clinician
decide whether to stop corticosteroids after the one week of administration or to continue the
treatment. A Lille score of greater than 0.45 indicates a lack of response to corticosteroids and
predicts a six month survival rate of less than 25% (15).
To identify patients at risk of early mortality from alcoholic hepatitis clinicians also use
the Glasgow Alcoholic Hepatitis score (4). In 2005 investigators from Glasgow reported the
results of an analysis involving a large cohort of patients with ALD identifying variables related
to survival at 28 days and 84 days after hospital admission. From the results of this study they
developed the Glasgow alcoholic assessment (15). The Glasgow Alcoholic Scale is a five-item
scale using four laboratory values, bilirubin blood urea, nitrogen, prothrombin time and WBC
17

count along with patient age to score the severity of alcoholic hepatitis. The study based on 200
people showed that a score of 9 or higher on the Glasgow alcoholic hepatitis scale indicated
having an increased mortality rate; these patients had improved survival rate with corticosteroid
therapy (7).
The easiest and most globally recognized methods for assessing clinical status and
severity of disease in patients with liver cirrhosis are the Child-Plugh classification and the
model for end stage liver disease (MELD). The Child-Plugh classification was derived from the
Child-Turcotte classification which was used up to the early seventies and recognized five
factors that affect prognosis and survival. These five factors are ascites, hepatic encephalopathy,
and levels of bilirubin, albumin and prothrombin time. Unfortunately this classification system
does not evaluate for nutrition status. It is the most common and feasible method in categorizing
cirrhotic patients (16).
Name Derivation set
Elements Test characteristics
1. Maddrey (modified) discriminant function (1989) (158)
n=66 MDF=4.6 (patient's PT−control PT) + total bilirubin (mg/dl)
Poor prognosis if score 32
2. MELD score (2001)a (160) n × 1,179MELD score × 3.8 × loge(bilirubin in mg/dl)+11.2 × loge(INR)+9.6 × loge
(creatinine mg/dl)+6.4Poor prognosis if >18
3. Glasgow alcoholic hepatitis score (2005) (161) n=241 Score 1 2 3
18
Table 3. Prognostic Scoring System used for patients with alcoholic hepatitis (19).

Name Derivation set
Elements Test characteristics
Age WCC Urea (mmol/l) PT ratio Bilirubin (mg/dl)
<50 <15 <5 <1.5 <7.3
≥50 ≥15 ≥5 1.5–2.0 7.3–14.6
— — — ≥2 >14.6
Poor prognosis if score >8 (for score calculated on hospital day 1 or day 7)
Signs and Symptoms:
Findings from a physical examination may range from normal to those suggesting
advanced cirrhosis. The presence of certain features may help to include advanced liver disease
as a possibility but indicators specific to ALD are more difficult to identify. Just as no single lab
value is definitive for diagnosing ALD, neither is any single physical finding or collection of
findings. It is important for physicians to recognize that ALD does not exist on its own. Other
organ dysfunctions related to alcohol abuse may coexist with ALD including: cardiomyopathy,
skeletal muscle wasting, pancreatic dysfunction, and alcoholic neurotoxicity (5).
General symptoms vary based on the severity of the disease. Alcoholic liver disease
progresses in three stages: hepatic steatosis, alcoholic hepatitis, and lastly cirrhosis. Hepatic
steatosis, occurs in more than 90% of patients, alcoholic hepatitis seen in 10 to 35%, and lastly
cirrhosis is prevalent in 10 to 20% of patients seen (6).
Physical examination usually reveals a malnourished patient with a fever, low blood
pressure and tachycardia. There is a high prevalence of jaundice and ascites and a significant
number who present with hepatic encephalopathy (7).
Symptoms can include: abdominal pain and tenderness, dry mouth, increased thirst,
fatigue, jaundice, loss of appetite, nausea, swelling or edema in the legs or ascites in the presence
of cirrhosis, and weight loss. Changes in skin include: abnormal darkening or lightening of the
19

skin, redness of feet or hands, and spider angiomas which are spider-like blood vessels on the
face, back or belly (2, 4). Abnormal bleeding can occur as well. This can appear as melena,
nosebleeds, bleeding gums and vomiting blood or material that looks like coffee grounds (2).
In the brain and nervous system symptoms such as agitation, mood changes, confusion,
poor judgment, shortened attention span, or encephalopathy can occur. This can result in periods
of decreased alertness or awareness of one’s surroundings, hallucination and impaired memory,
including both short-term and long-term memory. Pain, numbness, or tingling in the extremities
can occur as well as slow or sluggish movements. In men, altered hair patterns and gynecomastia
or breast development in males, may occur (4).
The first stage hepatic steatosis, also called fatty liver and is often asymptomatic. In one
third of patients the liver is enlarged and smooth but not usually tender (6). Hepatic steatosis is
reversible if abstinence from alcohol is achieved for approximately 4 to 6 weeks (5).
Alcoholic hepatitis is the second stage and is generally characterized by an enlarged liver
(3). This stage is considered an acute form of alcohol-induced liver injury that occurs with a
large intake of alcohol over a prolonged period of time. Alcoholic hepatitis encompasses
spectrum of severity ranging from alterations in biochemical factors to sudden and severe liver
failure as well as death (13). Labs specific to this stage of ALD include an elevation of
transaminase levels, increased serum bilirubin concentrations, normal or low serum albumin
concentrations, or anemia (3). AST is greater than the ALT and usually less than 400 IU/mL.
Total and direct bilirubin levels are elevated, with bilirubin exceeding 15 mg/dL. In severe cases,
serum sodium and albumin are low, while INR is elevated. WBC count is elevated sometimes to
>1500/mm3 (7). Signs and symptoms that patients may experience are abdominal pain,
anorexia, nausea, vomiting, weakness, diarrhea, weight loss or fever. If alcohol consumption is
20

discontinued, this condition could improve. However, more frequently, it will progress to the
third and final stage (3).
Alcoholic cirrhosis is the third stage and can present with varying symptoms as well. In
some patients, the symptoms are similar to those of alcoholic hepatitis. For other patients,
symptoms can be more severe and include gastrointestinal bleeding, hepatic encephalopathy, or
elevated blood pressure in the portal venous system or portal hypertension (3). The elevated
blood pressure is caused by the obstruction of blood flow through the liver (3). Portal
hypertension may lead to cyanosis and nail clubbing (6).
Ascites is often times present as well. Ascites is the accumulation of fluid, serum protein,
and electrolytes within the peritoneal cavity. It is caused by the increased pressure from the
portal hypertension and decreased production of albumin. Albumin maintains serum colloidal
osmotic pressure or the osmotic balance between the cells and the blood in the body (3).
During alcoholic cirrhosis, there is a replacement of normal hepatic parenchyma with
extensive thick bands of fibrous connective which result in the clinical manifestations of portal
hypertension and liver failure (13). There are many complications of cirrhosis including:
malnutrition, hyponatremia, hepatic encephalopathy, glucose alterations, fat malabsorption,
hepatorenal syndrome, and osteopenia.
21
Figure 3. Stages of Liver Damage (20).

If the patient remains abstinent, fatty liver resolves within six weeks (6). If the disease
had not progressed to cirrhosis, the liver can heal with the cessation of drinking. Fibrosis and
cirrhosis are irreversible. Once cirrhosis has developed, the complications of this advanced stage
will require management and a liver transplant may be needed (2).
There are two stages of cirrhosis, compensated and decompensated. Compensated
cirrhosis indicates that despite the scarring the liver tissue, the body still functions and the patient
has few symptoms or is asymptomatic. When there is severe scarring of liver and body functions
are disrupted, this is classified as decompensated cirrhosis. Patients at this stage may develop
serious and even lethal symptoms and complications (21).
Biochemical Markers:
Biochemical markers are used to evaluate and monitor patients having or suspected of
having liver disease. Enzyme assays measure the release of liver enzymes and other tests
measure liver function. Screening tests include: serum levels of bilirubin, alkaline phosphatase,
aspartate aminotransferase (AST), and alanine aminotransferase (ALT) (3). Serum AST is
typically elevated to a level of 2 to 6 times the upper limits of normal in severe alcoholic
hepatitis (5). Ratios of AST/ALT which are greater than 3 are highly suggestive of ALD (5).
22

Typically the ratio of AST to ALT is approximately 2:1 (13). The basis for low ALT is a dietary
deficiency of pyridoxal phosphate or vitamin B6, which is needed for ALT to function (6).
Serum y-glutamyl transpeptidase (GGT) increases due to ethanol which induces this
enzyme. Serum albumin may be low, usually reflecting undernutrition but sometimes is
representative of liver failure with deficient synthesis. Macrocytosis with Mean Corpuscular
Volume (MCV) greater than 100 fL reflects the direct effort of alcohol on bone marrow as well
as macrocytic anemia resulting from folate deficiency. Indexes of the severity of liver disease are
serum bilirubin which represents secretory function and Prothrombin Time (PT) or International
Normalized Ratio (INR) which reflects synthetic ability (6). Other common laboratory
abnormalities include anemia and leukocytosis (13). Serum tests for ferritin and iron are often
unreliable due to hepatic inflammation and hepatocyte death (7).
Table 4. Common Laboratory Tests Used to Treat Liver Function (3)Hepatic Excretion CommentTotal serum bilirubin When ^ may indicate bilirubin overproduction or
defect in hepatic uptake or conjugation; increased with jaundice, cirrhosis, biliary obstruction, and hemolysis (3, 26)
Indirect serum bilirubin Unconjugated bilirubin; ^ with excessive bilirubin production, immaturity of enzyme systems, inherited defects, drug effects (3)
Direct serum bilirubin Conjugated bilirubin; ^ with depressed bilirubin excretion, hepatobiliary disease, intrahepatic or postoperative jaundice and sepsis, and congenital conjugated hyperbilirubinemia; increased with jaundice, cirrhosis, biliary obstruction, and hemolysis (3, 26)
Urine bilirubin More sensitive than total serum bilirubin; confirms if liver disease is cause of jaundice (3)
Urine urobilirubin Used when obstructive jaundice is expected; rarely used (3)
Serum bile acids Reflects efficacy of ileal resorption and hepatic
23

extraction of bile acids from portal circulation; levels increase with liver disease; little clinical use (3)
CholestasisSerum alkaline phosphatase Enzyme widely distributed in liver, bone,
placenta, intestine, kidney, leukocytes; increased levels suggest cholestasis but can be ^ with other conditions; ^ levels with hepatic disease (3, 26)
Hepatic EnzymesALT Located in cytosol of hepatocyte; found in some
other body tissues but highest in liver; ^ with liver cell damage, jaundice, cirrhosis, hepatitis, and pancreatitis (3,26)
AST Located in cytosol and mitochondria of hepatocyte; also in cardiac and skeletal muscle, brain, pancreas, kidney, and leukocytes; ^ with liver cell damage, acute cirrhosis, hepatitis, pancreatitis, alcoholism, or renal injury (3, 26)
Serum lactic dehydrogenase Located in liver, RBCs, and leukocytes; ^ with liver disease but lack sensitivity and specificity because it is found in other body tissues (3)
Serum ProteinsProthrombin time (PT) Most blood coagulation factors are synthesized
in the liver; vit. K deficiency and decreased synthesis of clotting factors increase prothrombin time and risk of bleeding (3)
Partial thromboplastin time (PTT) Assesses the “intrinsic” clotting mechanism; reflects activity of most clotting factors; complimentary to PT (3)
Serum albumin Main export protein synthesized in the liver and most important factor in maintaining plasma oncotic pressure; decreased synthesis with liver dysfunction, thyroid and glucocorticoid hormone dysfunction, abnormal plasma colloid osmotic pressure, and toxins; ^ losses occur with protein-losing enteropathy, nephrotic syndrome, GI bleeding; values can be low with edema, hepatic disease, malabsorption, end stage renal disease, malnutrition, low protein intake, over-hydration
24

and stress (3, 26)Ammonia Liver converts ammonia to urea; may ^ with
hepatic failure and portal-systemic shunts (3)
Imaging:
Hepatic imaging is used to diagnose the presence of liver disease but does not establish
alcohol as the cause of the liver disease. Instead, these tests are used to rule out other causes of
abnormal tests in a patient who abuses alcohol. These imaging tests include: ultrasound, CT
scan, or magnetic resonance imaging (MRI). Magnetic resonance imaging has been used to
diagnose cirrhosis and to distinguish end-stage liver disease that is related to a viral hepatitis
infection from ALD (5).
Biopsy:
A liver biopsy is sometimes needed to secure the diagnosis. A clinical suspicion of
alcoholic hepatitis may be inaccurate in up to 30% of patients (13). If the disease is not
decompensated, clinical and biochemical markers are not reliable for determining the severity of
the disease and a biopsy is needed in establishing the stage and severity of the disease (5). In
addition to confirming the diagnosis, a liver biopsy may help to rule out any other possible
causes of liver disease. A liver biopsy aids in assessing the extent of the damage, making a
prognosis, and offering appropriate therapies (13). However sometimes the risks involved with
doing a biopsy may influence the incentive to make a histological diagnosis (5).
Treatment:
The most important part of treatment is to stop using alcohol completely and as soon as
possible. Compliance to abstinence is difficult and therefore a team approach is key. This
approach includes incorporating services from behavioral and psychological therapies as well as
25

integrating rehabilitation programs and support groups. Brief interventions by primary care
physicians may also be a component to treatment (6).
Patients with alcoholic hepatitis, who discontinue drinking alcohol, live significantly
longer than those who continue to drink. Three year survival nears 90% in those who sustain
from drinking alcohol and less than 70% in those who continue to drink (13). The 28 day
mortality for alcoholic hepatitis ranges from 30% to 50% (7). Clinical and laboratory features are
powerful prognostic indicators for short-term mortality. Hepatic encephalopathy, alterations in
renal function, hyperbilirubinemia, and prolonged prothrombin time are seen more often in
patients who die from the illness than in those who survive (13).
Part of the therapy for ALD is treating the complications of the disease. Generally ascites
can be decreased through the use of diuretics and a salt-restricted diet. The use of lactulose and
antibiotics to kill bacteria in the gut are treatments for hepatic encephalopathy. Any outside
infections should be addressed and treated with the recommended antibiotics. Hepatorenal
syndrome should be treated with albumin and vasoconstrictors (15).
Medications:
Medications may be prescribed to aid in maintaining abstinence but are only
recommended along with the other healthcare interventions, as mentioned above. Disulfiram
(Antabuse) is given with patients’ consent. It causes the patient to vomit after ingesting alcohol
and could be dangerous (4). Naltrexone was approved in 1995 however it has also been shown to
cause hepatocellular damage. However, in a systematic review of the medication, the risk of
relapse was lowered with short-term use (5). Short-term abstinence is improved by the use of
naltrexone at 100 mg per day (7). Baclofen has been proven safe in clinical trials, whereas the
26

safety of naltrexone or acamprosate in the treatments of patients with alcohol-related liver failure
has not been established (15).
Supportive care is at the core of managing the disease and the complications involved.
Alcohol withdrawal requires the use of benzodiazepines except in patients with advanced ALD,
as excessive sedation can contribute to hepatic encephalopathy (6). Opioid antagonists, such as
naltrexone, or nalmefene and drugs that modulate y-aminobutyric acid (GABA) receptors,
including baclofen or acamprosate, may have a short-term benefit by reducing withdrawal
symptoms and cravings (6). Naltrexone is more effective in some individuals than in others.
Delirium tremens can also be treated with benzodiazepines (15).
Severe acute alcoholic hepatitis commonly requires hospitalization and often an intensive
care unit. Here enteral feeds can be initiated to help manage nutritional deficiencies and certain
complications can be monitored more carefully. These complications can include infections,
bleeding esophageal varices, electrolyte imbalances, ascites, and hepatic encephalopathy (6).
Beta-blockers such as propranolol or nadolol or octreotide, brand named Sandostatin, may be
used to reduce portal hypertension when varices occur. Insulin may be necessary to regulate
blood sugars but should not be mixed with ethanol and therefore is not recommended for patients
who continue to drink alcohol. Alcohol intake may cause severe hypoglycemia in patients taking
insulin. Metformin should be avoided with patients with liver disease as well (4).
Corticosteroids have become the standard of care in patients with severe alcoholic
hepatitis. The concept behind this pharmaceutical therapy is the suppression of the immune
system to prevent further hepatic damage. Practice guidelines support the use of corticosteroids
in those who have a diagnosis of severe alcoholic hepatitis with no signs of infection,
gastrointestinal bleeding, renal failure, or pancreatitis (13, 6). The most common corticosteroid
27

therapy for ALD is prednisolone at 40 mg per day for 28 days. The patient will either be taken
off the medication all at once or slowly tapered off over a three week period. Unfortunately
alcoholic hepatitis is unresponsive to corticosteroid treatment in approximately 40% of patients.
The mechanism of action is believed to decrease transcription of pro-inflammatory
cytokines such as TNF-alpha. Indications include discriminant function (DF) > 32, MELD score
> 20, Glasgow score > 8 or the presence of hepatic encephalopathy (7). No other treatment has
been shown to be more effective with this group of patients (15). Methylprednisolone, a
corticosteroid, improves the ability to produce albumin and to normalize prothrombin time (PT)
and bilirubin levels. Side effects of this treatment may include negative nitrogen balance,
hypocalcemia, or hyperglycemia (4).
Research into pentoxifylline, an inhibitor of TNF-alpha synthesis, has been used in
studies as a possible treatment since increased levels of TNF-alpha have been found to be linked
to a higher mortality from alcoholic hepatitis (13). Pentoxifylline is a nonselective
phosphodiesterase inhibitor which indirectly decreases expression of cytokines such as TNF-
alpha, interleukin 8 (IL-8) and macrophage inflammation (7). Pentoxifylline at 400 mg three
times per day for 28 days is an alternative treatment of alcoholic hepatitis; indications for
treatment are similar to corticosteroids. A potential benefit is that it can be used in patients with
infection and patients with renal insufficiency (7).
Anabolic steroids such as oxandralone and testosterone have been tested in attempts to
increase the incorporation of nutrients into muscle mass in alcoholic hepatitis but there has not
been enough supporting data to put into practice. Also colchicine, an anti-fibrotic, anti-
inflammatory, often used to treat gout, has been tried but failed as well (7). Neither oral
28

administration of colchicines or propylthiouracil or combined regimen of insulin and glucagon,
is effective in patients with alcoholic hepatitis (15).
In liver disease the activation of methionine to S-adenosylmethionine (SAMe) is
impaired. Folate deficiency accentuates abnormal methionine metabolism, lipid oxidation, and
liver injury. Trimethylglycine (TMG) or betaine is manufactured by the body. It helps to break
down homocysteine. Plasma homocysteine levels are altered in actively drinking patients casuing
brain atrophy and withdrawal seizures. Common recommendations for betaine range from 375 to
3,000 mg daily. Betaine may help to protect the liver against the effects of alcohol, perhaps by
stimulating the formation of SAMe. However betaine also seems to worsen cholesterol profile
and this may counteract any possible benefits (22). Betaine may lessen damage of ALD by
increasing synthesis of SAMe and glutathione, decreasing homocysteine (tHey) level. SAMe,
betaine, and folate decrease oxidative stress by upregulation of TNF-alpha however more
research is indicated (4).
Alternative Therapies:
Antioxidants are often recommended as part of the treatment of ALD due to the presence
of oxidative stress and the reduction in antioxidant capabilities. Also, N-acetylcysteine an
antioxidant, has been proven effective as a treatment for acetaminophen-induced acute liver
failure (7). Studies involving treatment with antioxidants however, including vitamin E and
silymarin, which is the active ingredient in milk thistle, have not shown any survival benefit in
either patients with alcoholic hepatitis or alcoholic cirrhosis (15).
Numerous double-blind, placebo-controlled studies enrolling a total of several hundred
people have evaluated whether the herb milk thistle can successfully counter alcohol-induced
liver damage. These studies have yielded inconsistent results. A 2007 review of published and
29
unpublished studies on milk thistle as a treatment for liver disease concluded that benefits were
seen only in low-quality trials and even in those milk thistle did not show more than a slight
benefit. A subsequent 2008 review of 19 randomized trials drew a similar conclusion for ALD
generally, although it did find a modest reduction in mortality for patients with severe liver
cirrhosis (22).
Curcuma longa or turmeric and Glycyrrhiza glabra which is licorice, have also been
evaluated for effectiveness but studies have been inconclusive. Tea polyphenols, especially green
tea, may alleviate liver damage but further testing is needed. Chaparral is especially toxic to the
liver and should be avoided. Aloe vera, has been evaluated but should not be administered orally
(13). Other herbs and supplements that may possess known or suspected liver-toxic properties
include: excessive doses of beta-carotene and vitamin A which might cause alcoholic liver
disease to develop more rapidly in people who abuse alcohol; coltsfoot, comfrey, germander,
greater celandine, kaya, kombucha, pennyroyal, and prepackaged Chinese herbal remedies (22).
Nutritional supplementation at the standard daily requirement level should not cause a problem.
Herbs and botanical supplements should only be used when discussed with a physician.
Transplant:
A patient is appropriate for transplant when the disease has advanced to decompensated
cirrhosis, evidenced by the presence of ascites, spontaneous bacterial peritonitis, hepatic
encephalopathy, and variceal bleeding. For patients with decompensated alcoholic cirrhosis who
undergo transplant, survival is comparable to that of patients with other causes of liver disease; 5
year survival rate is about 70% (13). Alcoholic hepatitis, the second stage of ALD, has been
considered an absolute contraindication to liver transplantation due to the fact that the patients
30

with this disorder have been drinking recently and a period of abstinence will allow many to
recover (15).
Most U.S. transplantation programs now require 6 months of abstinence before a patient
with alcoholic hepatitis can become eligible for transplant (15). There is always a concern that
the patient will return to alcoholism after transplantation. Also, recidivism depends on the
definition of alcohol use. Approximately 20-40% of alcoholics consume some degree of alcohol
after transplant with up to 25% returning to abusive drinking habits (7). There is a high cost and
limited availability of cadaveric livers associated with transplantations.
Support groups and therapy are a cornerstone to the treatment of ALD. Chemical
addiction is a disease. Self-help programs and follow-up with professionals can reduce
dependency (4). The dietitian or other healthcare providers need identify sources of assistance
for those who need help with meal preparation, access to food, medication, and post-discharge
medical care (4).
V. Medical Nutrition Therapy
Role of the Registered Dietitian
There are several components to the nutrition intervention for which the dietitian is
responsible. First, is to ensure adequate nutrients are provided in the meal plan and with
31

supplementation if needed. Second, is to provide enteral and/or parenteral support when
appropriate. Third, is to assess whether or not limitation of certain nutrients is needed to manage
cirrhotic complications. Lastly, the dietitian should provide education and information regarding
outside resources to aid in ongoing compliance with the medical and nutrition prescription.
The primary dietary recommendation is to remove alcohol from the diet in order to allow
the liver to function more effectively while protecting it from metabolic stress. The patient
should also avoid alcohol in food and medicinal products such as vinegar, sauces, and cough
syrup. The dietitian should also function to correct fluid and electrolyte imbalances, nutritional
deficits, such as iron deficiency anemia from chronic bloods loss in varices, ulcers, and vomiting
(4). In improving the health of the liver, it can better synthesize albumin and other important
serum proteins. This will help liver tissue regeneration, replenish lost plasma proteins, and
improve skeletal muscle synthesis.
Nutrition therapy should aim to correct metabolic syndrome, hyperglycemia,
hypertension, and hypertriglyceridemia. It should also target to mend damage from fatty liver
and diminished bile salt synthesis. Another important aspect is the repair of neural damage from
malnutrition and malabsorption (4).
Completing the Nutrition Assessment
All sources indicate a need to first identify the severity of the disease in order to better
assess the level of malnutrition and related nutrition implications. The methods which are
universally used to evaluate the nutritional status and to detect the presence of malnutrition, are
the Subjective Global Assessment (SGA) and anthropometric parameters (16). The SGA when
compared to anthropometry shows an agreement of 77% (23). SGA is recommended by
European Society for Clinical Nutrition and Metabolism (ESPEN) as a practical bedside method
32

in assessing undernourished patients (16). SGA collects clinical information through history and
physical examination. The SGA looks at variables including muscle wasting, loss of
subcutaneous fat, dietary intake, functional capacity, and physical activities (23). Apart from data
which are collected by the SGA questionnaire, the ESPEN guidelines recommend the use of
simple anthropometric parameters also which are not affected by the presence of ascites and
peripheral edema. These parameters consist of mid-arm muscle circumference (MAMC) or mid-
arm circumference (MAC) and triceps skin fold thickness (TST). It is suggested that they be
performed by experienced clinicians in order to avoid observer error. Diagnosis of malnutrition
is established on values of MAMC and/or TST below 5th percentile in patients aged 18-74 years,
or the 10th percentile in patients aged over 74 years (16).
According to the Nutrition Care Manual, the first step in the nutrition assessment for
cirrhosis, is physical observation. The following signs could be useful in determining the extent
of liver damage: ascites, edema, muscle wasting, and jaundice. A diet history, along with a 24-
hour food recall would also be useful when the registered dietitian selects recommendations for
the nutrition intervention. This will give the dietitian insight into the patient’s food preferences,
taste aversions, intolerances, and allergies (24).
Alcoholics tend to underestimate their consumption of alcohol. Therefore, discussions
with family members or close friends may help to provide a more accurate record of their intake
(13). Any weight changes or alterations in appetite should be noted here as well as the use of
nutritional supplements, vitamins, or minerals. Looking at the diagnostic tests, laboratory values
and anthropometrics would be the next step in the nutrition assessment (24). Cirrhosis usually
causes patients to have abnormal anthropometric measurements due to complications such as
33

ascites or muscle wasting (6). Therefore when looking at indicators such as changes in weight or
body mass index it is important to keep these complications in mind.
Information for completing the nutrition assessment should include as many of the
following criteria as possible for the most accurate evaluation:
Height Weight Body Mass Index (BMI Usual Body Weight (UBW)
o Inquire about recent weight loss or weight gain
Diet history Food intolerances or taste aversions Presence of anorexia, nausea,
vomiting or diarrhea Input and Output (I & O) Blood pressure Presence of mild, moderate or severe
fatigue
Presence of leg edema or ascites Poor wound healing Diagnostic Tests:
o CT scan or ultrasound of abdomen
o Dual energy x-ray absorptiometry (DEXA) scan
o Liver biopsy Lab work
o Glucose increased or decreased
o Glucose tolerance test o Aspartate Amino Transferase
(AST)
o Alanine Amino Transferase (ALT)
o International Normalized Ratio (INR)
o Bilirubin o Serum ammoniao Blood Urea Nitrogen (BUN) o Albumin o C-Reactive Protein (CRP)o Triglycerides (TG)o Cholesterolo White blood cell (WBC)
counto Serum B12o Serum Folateo Plasma homocysteine o Sodium (Na) o Potassium (K) o Hemoglobin (Hb) o Hematocrit (HCT)o Serum iron (Fe), Ferritin,
Transferrin o Uric acid (UA)o Globulino Alkaline Phosphatase (ALP
or alk phos) o Magnesium (Mg) o Calcium (Ca) o Phosphorus (Phosphate, PO4)
Nutrition Intervention
34

For the patient who has been actively drinking alcohol, it is first essential to correct any
electrolyte imbalances and to treat withdrawal symptoms (17). Malnutrition is by far considered
one of the most important prognostic factors in liver cirrhosis and should alert clinicians to the
same extent as the presence of other common complications of cirrhosis such as hepatic
encephalopathy or ascites (16). Among cirrhotic patients, 34% are considered hypermetaboilc
with resting energy expenditure 120% of the expected value. Elevated pro-inflammatory and
anti-inflammatory cytokine levels point to a cytokine-driven hypermetabolism in cirrhosis (16).
Those with advanced ALD may also suffer from alterations in mental status if they have
hepatic encephalopathy which can contribute to poor dietary decision making. If hospitalization
is required, these patients are at an even higher risk, as many diagnostic and therapeutic
interventions contribute to malnutrition. Many alcoholics replace nutrients and food with
alcohol. Food that is eaten tends to be richer in carbohydrates and low in protein (6).
Malnourished alcoholics should consume a diet rich in carbohydrates and protein
preferentially via oral or enteral routes. In hypertensive patients the Dietary Approaches to Stop
Hypertension or DASH diet may be implemented as it provides adequate nutrients without
excessive calories. All fasting or very low calorie diets should be avoided. Energy control is only
recommended for those who are obese (24). Obesity, diabetes, and hyperinsulinemia play a role
in the development of hepatic steatosis and weight loss is critical to protect liver against further
damage. Four to six feedings per day, including nutritional supplements and a fluid prescription
is recommended for patients with hyponatremia (24).
In a Veterans Administration Cooperative study of 363 patients with alcoholic hepatitis,
100% of patients were found to have protein and/or combined protein calorie malnutrition based
on anthropometric and laboratory testing (19). Due to inadequate dietary intake, maldigestion,
35

malabsorption and/or defective metabolism there are many nutritional deficiencies often found in
these patients (6).
The risk of death is closely related to the degree of malnutrition (15). A randomized,
controlled clinical trial compared enteral tube feedings of 2000 kcal per day with prednisolone
therapy of 40 mg per day in 71 patients for 28 days. The survival rate at 28 days and at one year
were similar between the two groups suggesting that nutritional support may be as effective as
corticosteroids in some patients (15).
Recommendations
Meals and Calories:
Small frequent meals are recommended in order to prevent hypoglycemia, which can
result from limited glycogen stores (4). Four to six multiple meals are recommended, containing
foods rich in carbohydrates (16). In end-stage liver disease, the liver has lost some of its ability
to synthesize and metabolize protein, glycogen, and very low-density lipoporoteins (VLDL).
Consequently, the liver cannot regulate metabolism and therefore a continuous offering of
nutrients is needed. Further nutritional support is needed in cirrhotic patients with ongoing
alcohol abuse because of the risk of hypoglycemia due to the alcohol induced restriction in
gluconeogenesis (16). Meals should be made make appealing to the patient in order to stimulate
appetite (4). According to ESPEN, patients with liver cirrhosis should receive 30-40 kcal/kg per
day (16).
Carbohydrates:
The plan should include sufficient carbohydrate and fat to spare protein. Overfeeding
glucose can result in hyperglycemia and fatty liver and therefore is not recommended. Prescribed
diets should recommend no carbohydrate intake restriction, even if the patient suffers from
36

diabetes mellitus or demonstrates insulin resistance. 40-50% of all patients with end-stage liver
disease (ESLD) suffer from insulin-resistant diabetes mellitus. When cirrhosis reaches level at
which 80% of hepatocytes are dysfunctional, hypoglycemia is frequent due to high levels of
insulin in the blood (4).
Protein:
Inadequate intake of protein is common in patients with alcoholism and cirrhosis, as
mentioned above (6). Patients with liver injury both acute and chronic are in negative nitrogen
balance, it is assumed that liver regeneration is delayed and muscle wasting is increased (10).
Despite abnormalities in metabolism the overall nitrogen balance can be maintained with protein
intake of 35-50 grams per day or with daily amounts of dietary protein (0.74 g/kg) similar to that
of a healthy person (10, 6). ESPEN recommends a protein intake of 1.2-1.6 g/kg (16).
The restriction of protein is often suggested in the presence of hepatic encephalopathy
and hyperammonemia. However, recommendations from different medical-based sources vary.
According to one source, the amount of protein intake that can be tolerated without altering
mental status can vary greatly. Sometimes only a small amount of protein can be tolerated and in
these cases, to minimize the breakdown of protein stores, supplementary calories from fats and
carbohydrates should be given (10).
According to ESPEN guidelines, when feeding protein or administering amino acids, the
balance between restoring protein and precipitating hepatic encephalopathy, must be considered.
The ESPEN consensus report, in 2006, concluded that low grade hepatic encephalopathy (grades
I and II) is not regarded as a reason for protein restriction and malnutrition is more of a negative
prognostic factor (16). According to A.S.P.E.N. Guidelines, protein should not be restricted as a
management strategy to reduce risk of developing hepatic encephalopathy. Protein requirements
37

for the patient with hepatic failure should be determined in the same manner as for the general
ICU patient (25).
If the patient develops portal-systemic encephalopathy (PSE) and there is no evidence of
other precipitating disorders such as gastrointestinal bleeding, sedative use, hypoxia, electrolyte
or acid-base disturbances, volume depletion, or infections then protein can be restricted to as low
as 20 g/day for only 1-2 days (17). However proteins restriction is used too often and for too
long in most clinical situations and can further exacerbate catabolism (17). A daily protein intake
of 1.5 g/kg of body weight is recommended even in patients with hepatic encephalopathy
according to the New England Journal of Medicine (15).
Branched Chain Amino Acids (BCAA):
Effectiveness of using BCAA therapeutically is controversial but the majority studies
indicate that BCAA can improve outcomes if given to patients with nutritional deficits.
Branched-chain amino acids have a specialized role in energy metabolism. Most amino acid
catabolism occurs in the liver however branched chain amino acids are catabolized mainly in the
muscle, adipose, kidney and the brain. They are not only used as substrates for protein synthesis
but regulate protein synthesis and consequently keep skeletal muscles intact. In liver cirrhosis the
increased prevalence of hyperinsulinemia leads to an increased uptake of BCAA by skeletal
muscle for use as energy. Branched-chain amino acids (BCAA) are used in attempts to reduce
blood ammonia in patients with cirrhosis and intermittent hepatic encephalopathy based on the
idea that BCAA stimulate muscle ammonia detoxification. Therefore, lower levels of circulating
BCAA results in the destruction of skeletal muscle of these patients (16). The long-term use of
BCAAs in liver cirrhosis leads to an increase in serum proteins of approximately 10% if given
before bedtime (16). The ratio of the BCAAs isoleucine, leucine, valine, and lysine to aromatic
38

amino acids, phenylalanine, tryptophan, and tyrosine is abnormally low in these patients,
especially when malnourished (10).
Lipids:
According to the Nutrition Care Manual, for alcoholism requiring parenteral nutrition,
intravenous fat intake should not exceed 2.5 grams/kg body weight per day to avoid fat overload
syndrome. Fat emulsion should be used cautiously in patients with severe liver disease because
of their decreased capacity to clear the infused fat (24). Fat content should include a mix of from
omega-3 fish oils, omega-6 fatty acids, and medium-chain fatty acids (4). A fat restriction of less
than 30% of calories, with or without medium-chain triglyceride supplements, is recommended
in patients with steatorrhea (24). Increased absorption of fat can aggravate hepatic inflammation
and fibrogenesis contributing to the dysfunction of the liver. Also, a diet rich in fat in
combination with the impaired VLDL release can result in increased hepatic fat storage and
therefore should be avoided (16).
Vitamins/Minerals:
The diet should include adequate amounts of vitamins C, E, and K, phosphorus,
potassium, selenium, magnesium, zinc, and calcium (4). It is not generally advised to provide
supplementation of vitamins and minerals in patients with ESLD but at times complications of
deficiencies in various mineral and vitamins justify individualized nutritional support.
Prescription of supplements in the presence of clinical symptoms of various deficiencies is
indicated (16).
Circulating levels of both fat-soluble and water-soluble vitamins tend to be low in many
patients with ALD (6). Deficiencies in a number of vitamins and minerals is common including
vitamin A, vitamin D, thiamine, folate, pyridoxine, and zinc and therefore may need to be
39

supplemented (19). A diet low in sodium of less than 2-3 grams is generally advised in ESLD
among patients with ascites and fluid retention (NCM).
One of the most common complications of ESLD is osteoporosis. Patients, particularly
with risk factors such as previous smoking habits, older age, and a history of fractures are
candidates for supplements. The recommendation is 1200-1500 mg of calcium with 400-800 IU
vitamin D (16). For vitamin A, 100,000-200,000 IU every 4 weeks is advisable (16).
Supplementing vitamin K in conditions with a high risk of bleeding such as impaired
prothrombin time and esophageal varices is common. Parenteral administration of 10 mg vitamin
K every four weeks is recommended (16). It is common to provide B-vitamins, folic acid and
vitamin K intravenously for the first few days (7). Iron intake needs to be monitored to avoid
excess from the diet and/or supplements, especially if there is possibility of iron storage disease
(4).
Zinc is a common deficiency due to poor intake and/or increased urination (7). Alcohol
dehydrogenase is made with zinc and this too may contribute to a deficiency (4). Zinc deficiency
impairs would healing, immune reaction, protein metabolism and alters appetite and taste so it is
important to recognize any deficiency (16). Zinc replacement of approximately 220 mg/day
should be adequate. The optimal duration of vitamin and mineral support is not established but is
reasonable to continue for at least six months and oral zinc for 12 months (7).
Enteral and Parenteral Nutrition:
Enteral nutrition via a nasogastric tube, parenteral feeding, and oral intake are used in
severely ill patients with ESLD. Supplemental enteral nutrition is advisable for severely ill
cirrhotic patients who are hospitalized as the method of feeding. Based on clinical trials, nutrition
support results in a more rapid improvement in liver disease but does not improve survival (7).
40

When deciding between enteral or parenteral nutrition in critically ill patients, the risk of
repeated vomiting, diarrhea and aspiration during feeding through a nasogastric tube must be
weighed against the complications of parenteral feeding which include fluid overload and septic
complications (16). According to ESPEN guidelines, patients that cannot meet their caloric needs
though oral dietary intake, despite adequate nutrition support, are candidates for supplemental
enteral nutrition. Early placement of a fine-bore feeding should be considered in patients who do
not eat sufficient calories (7).
One clinical trial comparing nutrition support with prednisolone gave randomized
patients with alcoholic hepatitis 28 days of treatments with either 2,000 calories or treatment
with prednisolone and a standard hospital diet. The patients were followed for 12 months and the
improvement in survival with nutrition support compared to the corticosteroid treatment was
substantial, though not statistically significant due to the small study size. Survival during the
first 28 days was similar between the two groups however several patients receiving
corticosteroids developed infections after day 28. This began a survival advantage in the
nutrition support group which was seen starting at month six and continued through to the 12
month end point (7).
The majority of attending physicians do not initiate enteral feeding promptly with the
idea that many patients will spontaneously start oral dietary intake when general health returns.
Giving supplements with oral feedings is the standard for many hospitals (16).
One study showed that oral dietary intake improved after a long hospital stay with oral
nutrition support and the help of a dietitian in a 2 to 3 week period in the majority of the patients
(16). However, in severely ill patients, supplemental enteral nutrition is advisable. Tube feeds,
even with esophageal varices, is recommended (16). If enteral nutrition is needed, it is advised
41

to avoid glutamine-enriched formulas which may increase ammonia levels (4). In patients with
ascites the use of whole protein formulas and concentrated high energy formula is recommended.
BCAA-enriched formulas are used in patients with hepatic encephalopathy arising during enteral
nutrition feeds (10).
In acute liver injury where the focus has been on the role of protein and amino acids on
the outcome of alcoholic hepatitis, enteral and parenteral nutrition have been examined (10). In
studies, patients with acute hepatitis have shown that hepatic encephalopathy can be avoided by
judicious titration of dietary protein; low amounts of protein can contribute to a positive nitrogen
balance, and both biochemical and symptomatic improvements have been seen (10).
VI. Presentation of the patientDescription of the Patient
Initials: P.W.Gender: FemaleAge: 62Race: African American
42

Social History: Ms. W. lives alone with a son that lives nearby. Patient presents with long history
of tobacco use at a pack per day for about 35 years. She also has a history of heavy alcohol use
of three to six beers per day for 35 years. She denies any illegal drug use.
Date of Admission: 12/06/2012
Admitting Diagnosis: Metabolic Acidosis, Alcoholic Cirrhosis
Past Medical History:
Hypertension (HTN), chronic obstructive pulmonary disease (COPD), alcoholic cirrhosis,
alcoholism, primary metabolic acidosis, chronic kidney disease (CKD) stage III-IV, chronic
pancreatitis, hepatic encephalopathy (no stage mentioned), anemia of chronic disease, falls,
diaphragmatic hernia, gastritis, heparin-induced thrombocytopenia, pleural effusions, type II
diabetes mellitus.
Patient reports having falls in the yard outside of her house for the previous two weeks.
According to the emergency department (ED), family and friends reported that patient has been
have increased weakness and falls. She continues to consume alcoholic beverages on a daily
basis despite multiple warnings in the past not to drink anymore because of her underlying
cirrhosis and other areas of organ failure.
She has been admitted to this hospital and others multiple times because of her
alcoholism and alcohol-related complications. Per patient report, she was admitted to another
hospital 5-6 days prior for a fall. There, she was treated for a laceration on her head and was
given six stitches resulting from the fall. On December 6, 2012 the day of her current admission,
she fell again at home and hit her head.
Previous hospital admissions to this hospital: June 20, 2012 [Length of stay (LOS): 3 days] August 27, 2012 (LOS: 18 days)
43

October 2, 2012 (LOS: 3 days)October 9, 2012 (ED)October 14, 2012 (LOS: 2 days)
History with this hospital includes: chronic renal insufficiency, alcohol abuse, chronic obstructive pulmonary disease (COPD), and hypertension (HTN)
ALLERGIES: Heparin, penicillin, and aspirin; no known food allergies
Medications taken at home: Lasix 40 mg daily, Pepcid 20 mg daily, Tylenol as needed for pain, Propranolol 10 g three times daily, Thiamine 100 mg daily
Admission weight: 86 poundsAdmission height: 60 inches
Previous Weight RecordDate Weight Lbs. Weight Kg06/21/12 90 Lbs. 40.9 Kg10/02/12 96.8 Lbs. 44 Kg
Current Medications: Medications: Propranolol, Labetalol, Lactulose, Oxepam, Omeprazole, Hydralazine, Aztreonam/Dextrose, Hydromorphone, Amlodipine Besylate, Insulin Human Lispro (HumaLOG), Dextrose, Dextrose/Water,
Vitamins/Minerals: Thiamine, Folic Acid, Calcium Acetate, Sodium Chloride
Lab Summary I: 12/06-12/27
12/061:04 P.M.
12/06 3:00 P.M.
12/07 12/104:30 A.M.
12/1311:00 A.M.
12/146:20 A.M.
pH 7.14Bicarbonate 6
44

Total Bilirubin 0.6 0.6 0.4Direct Bilirubin 0.4 H 0.4 0.3AST 34 34 27ALT 16 16 16Alkaline Phosphatase 514 H 514 H 413 HAmmonia 119 H *
Reflective of underlying
hepatic encephalopathy 21
Total Creatine Kinase 80CK-MB 4.3Troponin T 0.10 HTotal Protein 8.1 5.6 LAlbumin 3.4 L 2.3 LGlobulin 4.7 HAlbumin/Globulin Ratio 0.7 LWBC 31.3 HHemoglobin 7.0 LHematocrit 21.2 LIron 78TIBC 138 LTransferrin 110 LFerritin 930 HBeta-Hydroxyburtic Acid
1.5 H (9:00 P.M.)
Date pH Arterial Normal Range12/06 at 3:00 p.m. 7.14 L 7.35-7.45
Low arterial pH or acedemia can occurs with metabolic acidosis, as well as renal failure, diarrhea, shock, and congestive heart failure (26).
Date Bicarbonate Normal Range12/06/12 at 3:00 p.m. 6 L 22-29 mmol/L
This lab value is decreased with metabolic acidosis, renal failure, and starvation (26).
Date Anion Gap Normal Range
45

12/06/12 at 3:00 p.m. 23 H 7-15 mmol/L
This value can be increased with renal failure, ketoacidosis, or lactic acidosis (26).
Lab Summary II: 12/06 through 12/27Chemistry
12/6 1:04 P.M.
12/6 9:00 P.M.
12/7 5:15 A.M.
12/8 5:37 A.M.
12/9 6:04 A.M.
12/104:30 p.m.
12/11 4:00 a.m.
Sodium 140 142 142 142 143 142 142Potassium 4.3 2.5 L 3.8 3.8 4 3.3 L 3.2 LChloride 107 106 104 102 106 106 106Carbon Dioxide 6 L 13 L 19 L 23L 22 L 22 L 22 LAnion Gap 27 H 22 H 19 H 17 H 15 14 14BUN 57 H 56 H 53 H 50 H 50 H 52 H 55 HCreatinine 4.6 H 4.6 H 4.0 H 3.6 H 3.4 H 3.1 H 2.8 HEst GFR A.A. 12 L 12 L 14 L 16 L 17 L 18 L 21 LBUN/Cr ratio 12.4 12. 13.3 13.9 14.7 16.8 19.6Glucose 83 264 H 65 L 132 H 157 H 159 H 142 HCalcium 6.9 L 6.3 L 7.1 L 8.3 L 8.4 L 8.2 L 8.4 LPhosphorus 14.1 H 10.9 H 9.8 H 7.8 H 6.4 H 5.3 H 4.3Magnesium 1.5 L 3.5 H 2.7 H 2.2 2.2 2.1
Chemistry 12/128:40 A.M.
12/1311:00 A.M.
12/146:20 A.M.
12/159:55 A.M.
12/169:00 A.M.
Sodium 148 143 145 143 141Potassium 3.9 3.8 3.5 3.7 3.8Chloride 114 H 111 H 112 H 111 H 112 HCarbon Dioxide 22 L 20 L 19 L 20 L 19 L
Anion Gap 12.0 12.0 14.0 12.0 10.0BUN 54 H 52 H 48 H 40 H 34 HCreatinine 2.6 H 2.4 H 2.3 H 2.1 H 1.9 HEst GFR A.A. 23 L 25 L 26 L 29 L 32 L
BUN/Cr ratio 20.8 21.7 20.9 19.0 17.9Glucose 112 H 100 H 80 154 H 108 HCalcium 9.1 8.7 L 8.6 L 8.2 L 8.3 LPhosphorus 4.7 H 5.3 H 5.0 H 5.0 HMagnesium 2.1 1.9 1.7 L 1.7 L
46

Chemistry 12/1811:07 A.M.
12/198:15 A.M.
12/208:40 A.M. 12/21 12/23 12/24 12/27
Sodium 139 140 141 140 139 138 136Potassium 4.4 4.3 4.3 4.3 4.8 4.8 4.5Chloride 110 H 110 H 111 H 110 H 109 H 107 H 104Carbon Dioxide 21 L 21 L 19 L 21 L 19 L 23 L 22 L
Anion Gap 8.0 9.0 11.0 9.0 11.0 8.0 10.0BUN 28 H 24 21 18 14 15 12Creatinine 1.7 H 1.7 H 1.6 H 1.5 H 1.5 H 1.5 H 1.6 HEst GFR A.A. 37 37 L 40 L 43 L 43 L 43 L 40 L
BUN/Cr ratio 16.5 14.1 13.1 12.0 9.3 10.0 7.5
Glucose 81 87 115 H 74 L 120 H 96 159 HCalcium 8.4 L 8.5 LPhosphorus 4.5 4.4Magnesium 1.5 L 1.5 L
Timeline
Admission to Emergency Department (ED):
In the ED she was noted to be extremely acidemic and was diagnosed with alcoholic
ketoacidosis for which they gave her thiamine and started her on dextrose containing IV fluids.
The ED staff attempted to place an internal jugular (IJ) catheter on the patient’s left, side but
were unsuccessful due to patient’s resistance. She was noted to be noncompliant and “thrashing
around somewhat”. They were then able to place the catheter on the right side successfully.
A chest x-ray taken in the ED showed a left pneumothorax. She was then sent to surgery
where they placed a large bore thoracostomy tube for the iatrogenic pneumothorax. Patient was
in increased pain because of this procedure and was given sedatives. The following is a timeline
of the events that occurred during Ms. W’s stay:
12/06/12 at 4:30 p.m.: It was noted that left thoracostomy tube was in place and left lung completely re-inflated
47
- Patient was treated with IV bicarbonate infusion; treated for alcohol withdrawal with oxazepam, and given thiamine
12/06/12 at 5:11 p.m.: Admitted to the Intensive Care Unit (ICU) with metabolic acidosis, alcoholic cirrhosis, and acute on chronic kidney disease
12/06/12:-Critical Care consultation for Alcoholic ketoacidosis and iatrogenic pneumothorax --In the ICU, patient was somnolent but arousable; was receiving IV bicarbonate fluids continuously-Patient would not respond to questions or provide any history-Noted that left chest tube was in place with suction-Right lung well inflated, left lung with notable pneumothorax; no evidence of pleural effusion-Enlarged liver border noted on physical examination-Abdomen was non-distended-No cyanosis or clubbing of fingers-Grossly cachectic; mostly in arms and legs as noted by physician-Mild asterixis-No seizure like activity while observed- Placement of KEO feeding tube-Head CT no acute findings-Computed Radiography (CR) Chest Portable ordered to evaluate central venous catheter (CVC) and source of chest pain: Right jugular catheter in good position without evidence of pneumothorax-Computed Tomography (CT) scan of brain ordered due to fall
12/07/12:-Nephrology consultation for elevated creatinine and metabolic acidosis-CR Chest Portable ordered for recurrent pneumothorax: No change since last exam
12/10/12-CR Chest Portable to evaluate pneumothorax in left lung: Findings indicate small bilateral pleural effusions; heart enlarged; no pneumothorax; bones are osteopenic- Electroencephalogram (EEG): EEG is abnormal suggestive of diffuse cerebral dysfunction, which can be seen in the setting of toxic or metabolic encephalopathies
12/11/12
48

-Patient presents as lethargic but arousable, responds to painful stimuli; not oriented to date; continues to fall asleep during exam by neurologist-Positive for upper B/L extremity tremors -No evidence of seizure-Lethargic during this admission despite improvement in her acidosis, resolution of her acute on chronic renal insufficiency, and decrease in her ammonia level-altered mental status-Noted that EEG on 12/11/12 consistent with toxic metabolic encephalopathy-Infection with WBC count which remains elevated-Suspected underlying thiamine deficiency noted-CR Chest portable showed that left chest tube was removed, no pneumothorax; bilateral pleural effusions-CT Brain without contrast showed atrophy and nonspecific white matter change; bilateral otomastoiditis
12/12/12-CR Chet Portable to verify position of KEO feeding tube; left pneumothorax identified-Per speech: advance diet to mechanical soft and thin liquids-CR Chest Portable to evaluate pneumothorax: large left pneumothorax; CHF with B/L effusions
12/13/12-Re-inserted chest tube-CR Chest Portable: small to moderate pleural effusions with associated deflating of the lung; cardiomegaly-Left pneumothorax nearly completely resolved with tiny pneumothorax. Small hiatal hernia-Per speech language pathologist (SLP), mild-moderate dysphagia due to weakness and mental status; moderate cognitive-linguistic deficits related to encephalopathy per neurology
12/14 6:20 A.M.: Iron 78, Total iron binding capacity (TIBC) 138 L, Transferrin 110 L, Ferritin 930 H
For iron, the normal ranges for females are 30-60 µg/dL and the patient’s value fell within this range. Iron can be low with iron deficient anemia, infection, and hepatitis. Total iron binding capacity (TIBC) can be low with chronic inflammatory states, iron overload and hemochromatosis. The normal ranges are between 240-250 µg/dL. Transferrin can be low with infection, hepatic disease, malnutrition and nephritic syndrome. Moderate depletion is considered 100-150 mg/dL. Normal range is 212-360 mg/dL. Ferritin can be increased with inflammatory diseases, chronic renal disease, and hepatitis. The normal ranges for females is 12-150 ng/mL (26).
49

12/15/12-Chest tube removal; small apical pneumothorax noted
12/16/12: -Left apical pneumothorax is not evident
12/17/12-Small bilateral pleural effusions; per SLP patient having difficulty with mastication and swallowing related to complaints of pain on back side; reports improved cognition but difficulty participating due to pain; per nursing patient tolerating Dysphagia 2 diet without difficulty; patient ready for diet upgrade
12/18/12-Diet changed to Dysphagia 2
12/19/12: SLP reports diet advanced to mechanical soft; no overt signs or symptoms of aspiration; cognition improving but not to patient’s baseline status
Initial Assessment (12/07/2012) – Patient screened for poor oral intake since admission
Anthropometrics:Date Height Weight BMI IBW12/07/12 5’0” (152.4 cm) 86 lbs. (39.1 kg) 16.8 100 Lbs +/- 10 lbs.
Weight History: UnknownCurrent Diet: NPO (Nothing orally)Diet History: Unable to obtain at this time due to patient’s mental status.
Nutritional Needs: Based on Total amount
Kcals per day 30-35 kcals/kg (actual weight) 1524-1780 kcals
Protein grams 1.0 g/kg (actual weight) 40 grams
Fluid mL 20-25 mL/kg(actual weight)
1010-1270 mLs
50

Nutrition Related Medications: Lactulose, Prilosec, hydralazine, insulin Vitamins/Minerals: Thiamine, folic acid, and PhosLo (calcium acetate)
Assessment: Patient is currently NPO status. No longer on propofol, but not alert enough for PO intake. Patient with elevated ammonia levels therefore protein restricted to 1.0 g/kg until ammonia levels decrease. KEO feeding tube in place for lactulose administration. If unable to safely tolerate PO within the next 48-72 hours, consider feeding via KEO tube. Monitor patient for possible refeeding syndrome.
Nutrition Diagnosis: Underweight related to inadequate energy intake, history of alcoholism, and altered mental status as evidenced by BMI of 16.8.
Intervention: Nutrition Prescription: When medically feasible, advance to oral diet. If unable to initiate within 24-28 hours consider enteral nutrition through KEO feeding tube.
Intervention #1: General/healthful dietGoal: If PO diet is initiated, meet >75% of estimated needs within 48 hours
Intervention #2: Protein-modified dietGoal: Provide 1.0 grams protein per kg until ammonia levels normalize
Nutrition Monitoring & Evaluation:Indicators Criteria1. Energy intake Meeting 100% of needs within 48 hours
2. Weight Prevent weight loss and promote weight gain of 1-2 lbs. per week
3. Electrolyte and renal profile Potassium: remaining WNLPhosphorus: trending downMagnesium: trending downBUN: trending downCreatinine: trending downGFR: trending up
51

4. Gastrointestinal profile Ammonia: trending down
1 st Follow-Up (12/10/12)
AnthropometricsDate Height Weight BMI Weight Change12/07/12 5’0” (152.4 cm) 86 lbs. (39.1 kg) 16.812/10/12 112 lbs. (50.8 kg) 21.9 Gain: 26 lbs. (11.8 kg)*
Laboratory Values: POC 145, 80, 168,
123, 148High
Current Diet: Nepro 1.8 at 35 mL/hr
-Feed runs for 20 hours for a TV of 700 mL per dayDiet History: NPO on admit. Diet prior to admission unknown.
Nutrition Needs: Based on Total amount TF provides
Kcals per day 25-30 kcals/kg (actual weight)
1270-1524 kcals 1260 kcals
Protein grams 1.0-1.2 g/kg (actual weight)
50-60 grams 57 grams
Fluid mL 20-25 mL/kg(actual weight)
1010-1270 mLs 508 mLs free water
Assessment: Current rate is not sufficient to meet patient’s estimated needs. Patient was seen at bedside this morning. She was unarousable currently receiving Nepro 1.8 at 35 mL per hour over 20 hours. KEO feeding tube in place. At this rate, the patient is not meeting estimated needs and she remains at high risk for malnutrition. Current feed provides 1260 kcals, 57 grams protein and 508 mL of free water.
Nutrition Diagnosis: Previous: Underweight related to inadequate energy intake, history of alcoholism and altered mental status as evidenced by BMI of 16.8--resolved as patient now weight 112 lbs. with a BMI of 21.9
Current: Inadequate enteral infusion rate related to current rate of feed proving less than estimated needs as evidenced by Nepro 1.8 infusing at 35 mL/hr
52

Intervention: Nutrition Prescription: Increase enteral feed rate to 40 mL/hr within 24 hours to meet 100% of estimated needs.
Intervention #1: Enteral nutrition rateGoal: Increase rate to 40 mL/hr with 50 mL flush every 4 hours
Nutrition Monitoring & Evaluation: Indicators Criteria1. Energy intake Meeting 100% of estimated needs
through enteral feeds within 48 hours2. Weight Prevent weight loss and maintain BMI
WNL
3. Electrolyte and renal profile Potassium: remain WNL Phosphorus: trending downMagnesium: trending downBUN: trending downCreatinine: trending downGFR: trending up
2 nd Follow-Up (12/13/12)
AnthropometricsDate Height Weight BMI Weight Change12/07/12 5’0” (152.4 cm) 86 lbs. (39.1 kg) 16.812/10/12 5’0” (152.4 cm) 112 lbs. (50.8 kg) 21.9 Gain: 26 lbs. (11.8 kg)*12/13/13 5’0” (152.4 cm) 112 lbs. (50.8 kg) 21.9 No change
Current Diet: NPODiet History: Patient was NPO on admit; put on Nepro 1.8 @ 35 mL/hr through KEO feeding tube
Nutrition Needs: Based on Total amount
Kcals per day 25-30 kcals/kg 1270-1524 kcals
53

(actual weight)Protein grams 1.0-1.2 g/kg
(actual weight)50-60 grams
Fluid mL 20-25 mL/kg(actual weight)
1010-1270 mLs
Assessment: Since last visit patient pulled out her KEO tube and SLP is now recommending to advance her diet to Dysphagia 2 diet. Patient is NPO and no longer receiving tube feeds. She is not currently meeting nutritional needs. Speech continues to follow patient for chewing and swallowing difficulties.
Note: Dysphagia level II diet consists of foods that are mechanically altered by blending, chopping, grinding or mashing so that they are easy to chew and swallow. Foods in large chunks or foods that are too hard to be chewed thoroughly should be avoided (6).
Nutrition Diagnosis: Previous: Underweight related to inadequate energy intake, history of alcoholism and altered mental status as evidenced by BMI of 16.8--resolved as patient now weight 112 lbs. with a BMI of 21.9
Previous: Inadequate enteral infusion rate related to current rate of feed providing less than estimated needs as evidenced by Nepro 1.8 infusing at 35 mL/hr—resolved; patient not longer receiving EN
Current: Inadequate oral intake related to no PO intake and discontinuation of enteral feeds as evidenced by current NPO status
Intervention: Nutrition Prescription: Advance diet as medically appropriate per SLP to Dysphagia 2 diet. Introduce Glucerna supplement TID to aid in meeting 100% of estimated needs within 48 hours.
Intervention #1: Texture modified dietGoal: Advance diet per SLP recommendations to Dysphagia 2 diet
Intervention #2: Commercial BeverageGoal: Consume Glucerna TID
Nutrition Monitoring & Evaluation: Indicators Criteria1. Energy intake Meeting 100% of estimated needs
within 48 hours through meals consumption and oral supplement TID
54

2. Weight Prevent weight loss and maintain BMI WNL
3. Electrolyte and renal profile Potassium: remain WNL Phosphorus: trending downMagnesium: trending downBUN: trending downCreatinine: trending downGFR: trending up
3 rd Follow Up (12/18/12)
AnthropometricsDate Height Weight BMI Weight Change12/07/12 5’0” (152.4 cm) 86 lbs. (39.1 kg) 16.812/10/12 5’0” (152.4 cm) 112 lbs. (50.8 kg) 21.9 Gain: 26 lbs. (11.8 kg)*12/13/13 5’0” (152.4 cm) 112 lbs. (50.8 kg) 21.9 No change12/18/13 5’0” (152.4 cm) 115 lbs. (52.2 kg) 22.5 Gain: 3 lbs. (1.4 kg)
Current Diet: Mechanical softDiet History: Patient was NPO on admit; started on Nepro 1.8 at a rate of 35 mL/hr ; Dysphagia 2 diet (12/12-12/18) with intake at 25-50% advanced this morning to mechanical soft per SLP evaluation
Nutrition Needs: Based on Total amount
Kcals per day 25-30 kcals/kg (actual weight)
1270-1524 kcals
Protein grams 1.0-1.2 g/kg (actual weight)
50-60 grams
Fluid mL 20-25 mL/kg(actual weight)
1010-1270 mLs
Assessment: Diet is appropriate but not meeting estimated nutrient needs. Suggest adding oral supplements and advancing diet per SLP recommendations. Patient has difficulty swallowing and chewing and pain is affecting intake per nursing.
Nutrition Diagnosis: Previous: Underweight related to inadequate energy intake, history of alcoholism and altered mental status as evidenced by BMI of 16.8--resolved as patient now weight 112 lbs. with a BMI of 21.9
55

Inadequate enteral infusion rate related to current rate of feed providing less than estimated needs as evidenced by Nepro 1.8 infusing at 35 mL/hr (no longer relevant)
Inadequate oral intake r/t diet not advanced as evidenced by NPO status—resolved; patient no longer NPO status
Current: Inadequate oral intake related to poor appetite as evidenced by PO intake of 25-50% x 5 days per nursing.
Intervention:
56
Nutrition Prescription: Advance diet per SLP recommendations. Add Glucerna TID. Suggest daily MVI. Continue to monitor phosphorus levels and evaluate for possible restriction in the diet.
Intervention #1: Texture-modified dietGoal: Mechanical soft or per SLP intake at greater than 50% of meals daily
Intervention #2: Commercial BeverageGoal: Consume Glucerna TID
Intervention #3: MultivitaminGoal: Suggest multivitamin given daily
Nutrition Monitoring & Evaluation: Indicators Criteria1. Energy intake Completing > 50% of meals daily and
oral supplement TID within 24 hours2. Weight Prevent weight loss and maintain BMI
WNL
3. Electrolyte and renal profile Potassium: remain WNL Phosphorus: trending downMagnesium: trending downBUN: trending downCreatinine: trending downGFR: trending up
4. Glucose profile Accuchecks maintained < 150 mg/dLGlucose, casual < 150 mg/dL
4 th Follow-Up (12/24/12)
AnthropometricsDate Height Weight BMI Weight Change12/07/12 5’0” (152.4 cm) 86 lbs. (39.1 kg) 16.812/10/12 5’0” (152.4 cm) 112 lbs. (50.8 kg) 21.9 Gain: 26 lbs. (11.8 kg)*12/13/13 5’0” (152.4 cm) 112 lbs. (50.8 kg) 21.9 No change12/18/13 5’0” (152.4 cm) 115 lbs. (52.2 kg) 22.5 Gain: 3 lbs. (1.4 kg)12/24/12 5’0” (152.4 cm) 115 lbs. (52.2 kg) 22.5 No change
Current Diet: Mechanical soft
57

Diet History: Patient was NPO on admit; put on enteral feeds of Nepro 1.8 through KEO feeding tube; Dysphagia 2 diet (12/12-12/18) with intake at 25-50% advanced mechanical soft per SLP evaluation on 12/18/12
Nutrition Needs: Based on Total amount
Kcals per day 25-30 kcals/kg (actual weight)
1270-1524 kcals
Protein grams 1.0-1.2 g/kg (actual weight)
50-60 grams
Fluid mL 20-25 mL/kg(actual weight)
1010-1270 mLs
Indicators Criteria1. Energy intake Completing > 50% of meals daily and
oral supplement TID within 24 hours2. Weight Prevent weight loss and maintain BMI
WNL
3. Electrolyte and renal profile Potassium: remain WNL Phosphorus: trending downMagnesium: trending downBUN: trending downCreatinine: trending downGFR: trending up
4. Glucose profile Accuchecks maintained < 150 mg/dLGlucose, casual < 150 mg/dL
Secondary Diagnoses:1. Alcoholic cirrhosis2. Anemia of chronic disease3. Chronic pancreatitis4. Chronic renal impairment5. Hypertension6. Diabetes mellitus type 27. Chronic obstructive pulmonary disease
58

VIII. Critical Comments:
Evaluation of the situation:
Throughout the research of this topic, it became evident that monitoring other
biochemical markers would have beneficial from a nutritional standpoint. To indicate acid base
balance, carbon dioxide (CO2) levels could have been tracked. This lab value is decreased with
metabolic acidosis, renal failure, and starvation (26). Normal ranges are between 23-29 mmol/L.
The patient started with a CO2 level at 6 mmol/L on 12/06/12 and on 12/27/12 the CO2 level had
increased to 22 mmol/L which is just within the normal range and a significant improvement
from admission. The patient remained with a CO2 level below 23 mmol/L up until 12/24/12.
For gastrointestinal profile total bilirubin, direct bilirubin, AST, ALT, and alkaline
phosphatase would have been valuable indicators of liver function. The chart below indicated the
lab values for these markers on admission on 12/06/12 and again on 12/13/12.
12/06 1:04 P.M.
12/1311:00 A.M.
Normal Ranges
Total Bilirubin0.6 0.4
0.3-1.9 mg/dL (27)
Direct Bilirubin0.4 H 0.3
< or = to 0.3 mg/dL
AST 34 27 F: 10-31 U/LALT 16 16 F: 4-31 U/LAlkaline Phosphatase 514 H 413 H 40-120 U/L
Recommendations for improvement:
59

Protein was initially limited due to the extremely high blood ammonia levels the patient
presented with. As discussed previously, there are contradicting recommendations on limiting
protein to aid in the normalizing ammonia levels. This may or may not have been necessary.
A re-weight on a different scale on admission would have been beneficial to evaluate fluid
weight gain and eliminate discrepancies from observer or different scales used. A usual body
weight would have been useful as well as a history of recent weight loss or weight gain; within
the past 30 days. The two previous weights from previous admissions were 90 lbs. on June 2,
2012 and 96.8 lbs. on October 2, 2012.
The patient was a poor historian and unable to communicate diet history due to altered
mental status during her admission at the hospital. Additional diet related history from family
and friends could have helped to obtain more information about the patient’s diet before
admission. It would have offered background regarding pattern of eating including: number of
meals per day, average calorie and fluid intake amounts, intake of both macro- and
micronutrients, taste aversions and preferences.
Glucerna TID and a daily multivitamin we both recommended but not ordered for the
patient. In addition to the multivitamin that was requested, vitamin D should have been added as
osteopenia noted in bones on a CR chest portable on 12/10/12. In addition, zinc and vitamin A
are recommended for chronic alcohol abusers as they are often depleted.
Validation of Treatment Received:
On admission, the patient was given thiamine immediately in the ED along with dextrose
containing IV fluids. This helped to replenish her of electrolytes, fluid, and thiamine. In the ICU
the patient was given IV bicarbonate fluids for alcoholic ketoacidosis to improve her acidemic
state.
60

Also, in the ICU, a KEO feeding tube was placed for administering medications. This
was a good choice for a feeding tube versus an oral gastric tube which is often placed for short-
term use in hospitals as it allows for medications and feeds to be given as well as suction if
needed. The KEO feeding tube is small bore so usually better tolerated by patients and is
intended for more long-term use which would allow for on-going enteral feeds if needed. The
placement of the KEO feeding tube was verified with CR chest portable which is viable as
sometimes the feeding tubes are misplaced and can even end up in the patient’s lung. It is
important to verify that the feed is going into stomach.
Speech was consulted and followed the patient throughout her stay; SLP is an important
part of the care team especially when dysphagia and altered mental status are present. It is
important to ensure that the patient is being fed appropriately and without harm. This can
eliminate additional illness from infections such as pneumonia resulting from aspiration of food
or fluid into the lungs. The prescribed diets were discussed with speech and necessary advances
were initiated when medically appropriate.
61

IX. Summary
Due to the complex nature of the disease and its involvement with virtually every system
in the body, ALD is complicated to both diagnose and treat effectively. It truly takes the effort
and collaboration of a number of healthcare professionals to insure that the patient is receiving
the most accurate and effective care available. As with many other on-going health problems,
recovery takes commitment and effort on the part of the patient as well. Unfortunately without
the necessary behavior and lifestyle changes to stop consuming alcohol, the disease will only
progress. Once the disease has progressed to the third and final stage of decompensated cirrhosis,
liver transplant is the only available treatment. Without the cessation of drinking, the possibility
of receiving a donor liver is not likely.
Nutrition plays an integral role in the treatment of ALD. Evaluation of the degree to
which the disease has progressed is the first step in the nutrition assessment. From here, the
dietitian can determine the level of malnutrition present and calculate recommended amounts of
macro and micronutrients to replenish deficits and promote healing.
In this case study, the patient suffered from ALD as well as many of the complications
often seen with the disease including hepatic encephalopathy. Through medical and nutritional
interventions the patient became stable and suitable discharge after 22-day stay at the hospital.
The patient arrived to the hospital and was made NPO status. She was then started on an enteral
62

feed of Nepro 1.8 by way of a KEO feeding tube. After speech consulted with the patient, she
was advanced to a dysphagia 2 diet and then to a mechanical soft diet. The patient was given
thiamine, folic acid and calcium acetate throughout her stay at the hospital. Additional vitamins
and minerals were recommended in the form of a daily multivitamin but this along with the
recommendation of Glucerna TID was not carried out in the physician’s order.
After the patient had last been assessed on December 24, 2012, she was discharged on
December 28, 2012. Home care services with physical therapy were arranged. She was sent
home with medications and outpatient follow-up and referrals. The patient was hemodynamically
and clinically stable at time of discharge according to the hospital’s discharge summary. The
total length of stay at the hospital was 22 days. To date, the patient has had no new admissions to
this hospital since discharge.
63
IX. MEDICAL TERMINOLOGY GLOSSARY
Apoptosis: programmed cell death; deletion of individual cells by fragmentation into membrane-bound particles, which are phagocytized by other cells.
Ascites: a distended abdomen due to pathological fluid in the peritoneal cavity.
Asterixis: involuntary jerking movements, especially in the hands, best elicited by having the patient extend the upper limb, dorsiflex the wrists, and spread the fingers; results from lapses of sustained posture; seen primarily with various metabolic and toxic encephalopathies, especially hepatic encephalopathy. Alternate names: flapping tremor
Clubbing of fingers: occurs most often in people who have heart or lung disorders that decrease the amount of oxygen in their blood. This causes the fingertips and fingernails to spread out and become rounder.
Colloidal osmotic pressure: (COP) important determinant of the appearance of edema; osmotic pressure exerted by the tissues in the body
Cyanosis: A dark bluish or purplish discoloration of the skin and mucous membrane due to deficient oxygenation of the blood, evident when reduced hemoglobin in the blood exceeds 5 g/100 mL.
Cytokine: Any of several nonantibody proteins, such as lymphokines, that are released by a cell population on contact with a specific antigen and act as intercellular mediators, as in the generation of an immune response.
Edema: fluid buildup in the extremities
Electroencephologram (EEG): A painless procedure that uses small, flat metal discs (electrodes) attached to your scalp to detect electrical activity in your brain. Your brain cells communicate via electrical impulses and are active all the time, even when you're asleep. This activity shows up as wavy lines on an EEG recording.
64
Encephalopathy: Any disorder of the brain. Alternate names: cerebropathia, cerebropathy, cerebropathy, encephalopathia, encephalosis
Enterohepatic circulation: circulation of substances such as bile salts that are absorbed from the intestine and carried to the liver, where they are secreted into the bile and again enter the intestine.
Hepatic encephalopathy: A potentially fatal brain disorder that results when prolonged liver dysfunction caused by excessive alcohol consumption leads to the accumulation of toxic substances in the brain.
Hepatorenal syndrome: the occurrence of acute renal failure in people with disease of the liver or biliary tract, apparently due to decreased renal blood flow and conditions that damage both organs, such as carbon tetrachloride poisoning and leptospirosis.
Iatrogenic pneumothroax: pneumothorax caused by a medical procedure, most often central venous catheter insertion, thoracentesis, or transbronchial and transthoracic lung biopsy.
Jaundice: yellow color in the skin, mucus membranes, or eyes
KEO feed tube: small bore nasogastric feeding tube
Klebsiella: a group of bacteria normally living in the intestinal tract and frequently the cause of nosocomial infections (infections acquired in the hospital). Named for Dr. Klebs.
Macrophages: type of white blood that takes in (ingests) foreign material. Macrophages are key players in the immune response to foreign invaders of the body, such as infectious microorganisms.
Melena: bloody, dark black, or tary bowel movements
Myofibroblasts: spindle-shaped cells with characteristic contractile and structures that contribute to the wound healing process. They occur in granulation tissue and also in pathological processes such as fibrosis.
Neoantigen: antigenic proteins formed by metabolic pathways (drug metabolism).
Otomastoiditis: is the result of an infection that extends to the air cells of the skull behind the ear
Osteopenic: showing signs of osteopenia which is a condition where bone mineral density is lower than normal.
Parenchyma: he distinguishing or specific cells of a gland or organ, contained in and supported by the connective tissue framework, or stroma. The endoplasm of a protozoan cell. In the lung, consists of the gas-exchanging portion, excluding the radiographically visible blood vessels and bronchi.
65

Pleural effusions: outpouring of fluid between the two layers of the pleural membranes that cover the lungs. The term "effusion" comes from the Latin "effusio" meaning a pouring out. A pleural effusion is thus, literally, a pouring out of fluid into the pleural space. By comparison, a pericardial effusion is an outpouring of fluid within the fibrous sac (the pericardium) that surrounds the heart.
Pneumothroax: free air in the chest outside the lung. Pneumothorax can occur spontaneously ("out of the blue"), follow a fractured rib, occur in the wake of chest surgery, or be deliberately induced in order to collapse the lung.
Portal hypertension: abnormally high blood pressure in the portal vein (the large vein that brings blood from the intestine to the liver) and its branches.
Sinusoid: Resembling a sinus. Sinusoidal capillary; a thin-walled terminal blood vessel having an irregular and larger caliber than an ordinary capillary; its endothelial cells have large gaps and the basal lamina is either discontinuous or absent.
Stellate cell: cell that is vital to hepatocellular function and the liver's response to injury. Indeed, the paradigm of stellate cell activation into contractile myofibroblasts as the major pathway in hepatic fibrogenesis associated with liver injury
Thoracostomy tube: a tube placed through the chest wall that drains the pleural space.
Varices (gastric or esophageal): extremely dilated sub-mucosal veins result of portal hypertension; they are superficial and liable to ulceration and massive bleeding.
Wernicke’s encephalopathy and Korsakoff psychosis: Different conditions that are both due to brain damage caused by a lack of vitamin B1 (thiamine).
Korsakoff syndrome, or Korsakoff psychosis, tends to develop as Wernicke's symptoms go away. Wernicke's encephalopathy causes brain damage in lower parts of the brain called the thalamus and hypothalamus. Korsakoff psychosis results from damage to areas of the brain involved with memory.
66

X. MEDICATION BILIOGRAPHY
Pertinent Medications:Brand Name Generic Name Indication Contraindication Side Effects Food
interaction/patient education
Inderal propanolol Management of HTN, angina, arrhythmias
Uncompensated HF; pulmonary edema; cardiogenic shock; bradycardia, sick sinus syndrome or heart block
Arrhythmias, bradycardia, HF, pulmonary edema, fatigue, weakness
Lower sodium and lower calorie diet may be recommended; avoid natural licorice
Trandate labetalol Management of HTN
Uncompensated HF; pulmonary edema; cardiogenic shock; bradycardia or heart block
Fatigue, weakness, dizziness
Lower sodium and lower calorie diet may be recommended; avoid natural licorice
Cholac, Constulose
lactulose Treatment of chronic constipation; adjunct in the management of portal hepatic encephalopathy
Patients on low-galactose diets
Belching, cramps, distention, flatulence
Take with milk, juice, water or mix with sweet food to improve taste; follow with 8 oz water; high fiber diet with 1500-2000 mL fluid per day to prevent
67

constipation; Increases the absorption of calcium and magnesium; not to be used with a lactose or galactose restricted diet;
Serax oxepam Management of anxiety; anxiety associated with depression. Symptomatic treatment of alcohol withdrawal
Hypersensitivity; comatose patients or those with pre-existing CNS depression; uncontrolled severe pain; pregnancy; lactation
Dizziness, drowsiness, confusion, headache
May take with food if GI distress occurs; limit caffeine to < 400-500 mg/day; increased appetite may occur
Prilosec omeprazole GERD/maintenance of healing in erosive esophagitis. Duodenal ulcers. Reduction of GI bleeding in critically ill patients
Hypersensitivity; breastfeeding
Abdominal pain, dizziness, drowsiness, fatigue, headache
Avoid ginko or St. Johnn’s Wart
Formerly Apresoline
hydralazine Moderate to severe hypertension. Unlabeled use: HF unresponsive to conventional therapy with digoxin and diuretics
Hypersensitivity
Tachycardia, sodium retention, anorexia, dizziness, drowsiness, headache, N/V/D
Lower sodium and lower calorie diet may be recommended; avoid natural licorice; food increases bioavailability so take consistently with or without food
68

Azactam, Cayston
aztreonam Treatment of serious gram-negative infections including urinary tract infections
hypersensitivity
(with inhalation): nasal congestion, abdominal pain, cough, wheezing fever
Altered taste could occur
Dilaudid hydromorphone Moderate to severe pain
Hypersensitivity; severe respiratory depression; paralytic ileus; prior GI surgery; pregnancy and lactation
Confusion, sedation hypotension, constipation
May take with food to reduce GI distress; may cause dry mouth; avoid alcohol
Norvasc Amlodipine Besylate
Alone or with other agents in the management of hypertension, angina pectoris, and vasospastic angina
Hypersensitivity; systolic BP < 90 mm Hg
Headache, peripheral edema
Lower sodium and lower calorie diet may be recommended; avoid natural licorice; may take with food to decrease GI distress; grapefruit juice increases serum levels and effect;
Humolog Insulin Human Lispro
Control of hyperglycemia in patients with type 1 or type 2 diabetes mellitus
Hypoglycemia; allergy or hypersensitivity to a particular type of insulin
Hypoglycemia; allergic reaction
Diabetic meal plan to balance carbohydrate with insulin; use alcohol with caution as alcohol increases hypoglycemic effect of insulin; increased needs with exercise, large weight
69

gain, stress, or illness
Vitamin B1 thiamine Treatment of thiamine deficiencies; prevention of Wernicke’s encephalopathy; dietary supplement in patients with alcoholism or cirrhosis
Hypersensitivity; known alcohol intolerance
Extremely rare and usually associated with IV administration or extremely large doses
Increased requirement with carbohydrate intake; alcohol inhibits absorption
Folate, Folvite
folic acid Prevention and treatment of megaloblastic and microcytic anemias.
Uncorrected pernicious, aplastic, or normocytic anemias
Rash, irritability, difficulty sleeping, malaise, confusion, fever
None
PhosLo, Phoslyra, Eliphos
Calcium acetate
Treatment and prevention of hypocalcemia. emergency treatment of hyperkalemia and hypermag-nesemia and adjunct in cardiac arrest or calcium channel blocking agent toxicity; control of hyperphosphatemia in end-stage renal disease
Hyper-calcemia; ventricular fibrillation; concurrent use of calcium supplements
Arrhythmias, hypercalcemia, constipation; phlebitis (IV only)
Cereals, spinach, or rhubarb may decrease the absorption of calcium supplements
Slo-Salt sodium chloride
Hydration and provision of
Hypertonic solutions;
HF; pulmonary edema
70
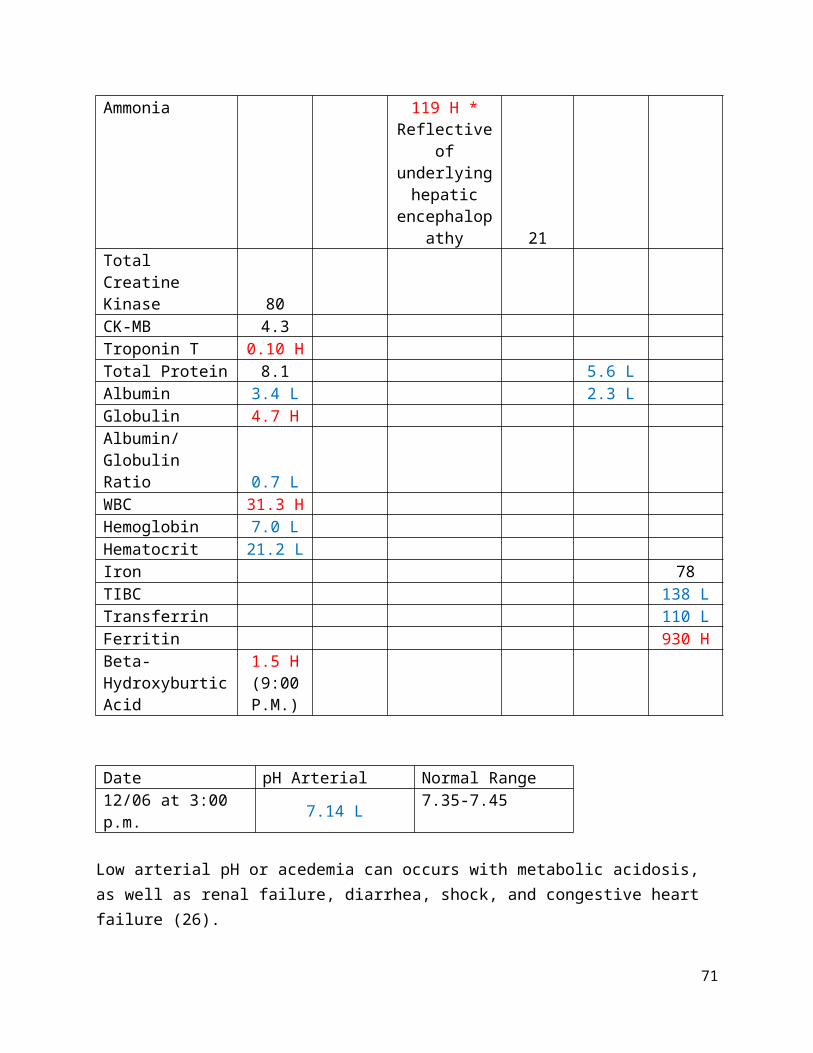
NaCl in deficiency; maintenance of fluid and electrolyte status
fluid retention or hyper-natremia
71

XI. APPENDIX: Subjective Global Assessment
72

XII. REFERENCES
1. Symptoms of Alcohol Liver Damage. Treatment4Addiction.com.2011. Available at: http://www.treatment4addiction.com/addiction/alcohol/liver-damage/. Accessed February 10, 2012.
2. Longstreth G. MedlinePlus Medical Encyclopedia: Alcoholic Liver Disease. 2010. http://www.nig.gov/medlineplus/ency/article/000281.htm. Accessed December 12, 2012.
3. Mahan K, Escott-Stump S, Raymond J. Krause's Food and the Nutrition Care Process. 13th ed. St. Louis, Missouri: Saunders 2012.
4. Escott-Stump S. Nutrition and Diagnosis-Related Care. 7th ed. Baltimore, Md: Lippincott Williams & Wilkins; 2012.
5. O'Shea Robert DS, McCullough A. ACG Practice Guidelines: Alcoholic Liver Disease. Am J Gastroenterol. 2010;105:14-32.
6. Shaffer E. Alcoholic Liver Disease. Merck Manual Professional Website. 2011. Available at: http://merckmanuals.com/professional/print/hepatic_billary_disorders/ alcoholic_liver_disease/alcoholic_liver_disease.html. Accessed December 29, 2012.
7. Cohen SM, Ahn J. Review article: the diagnosis and management of alcoholic hepatitis. Aliment Pharmacol Ther. 2009;30:3-13. Available from EBSCO Nursing Reference Center. Accessed January 22, 2013.
8. Liver Transplant Workup: Anatomy. Johns Hopkins Medicine Gastroenterology & Hepatology. 2013. Available at: http://www.hopkins-gi.org/GDL_Disease.aspx?Current UDV=31&GDL_Cat_ID=BB532D8A-43CB-416C-9FD2-A07AC6426961&GDL_ Disease_ID=9ED2FD73-51A1-49E1-B77A-D4B753B384AD. Accessed December 14, 2012.
9. Sherwood L. Human Physiology From Cells to Systems. 7th ed. Belmont, California: Brooks/Cole; 2010.
10. Shils ME, Shike M, Ross CA, et al. Modern Nutrition in Health and Disease. 10th ed. Baltimore, Md: Lippincott Williams & Wilkins; 2006.
11. Health Topics: About the Liver. Arizona Transplant Associates, PC. 2012. Available at: http://www.arizonatransplant.com/images/liver_large_2.jpg. Accessed February 10, 2012.
12. Herrine S. Liver Structure and Function: Approach to the Patient with Liver Disease. Merck Manual Professional. 2012. http://www.merckmanuals.com/professional/hepatic_and_biliary_disorders/approach_to_the_patient_with_liver_disease/liver_structure_and_function.html. Accessed January 22, 2013.
13. Fairbanks KD. Alcoholic Liver Disease. The Cleveland Clinic: Center for Continuing Education Website. 2012. Available at: http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement/hepatology/alcoholic-liver-disease/.Accessed December 19, 2012.
14. Zakhari S. Overview: How is Alcohol Metabolized by the Body? Alc Res Health. 2006; 29(4): 245-54.
15. Lucey MR, Mathurin P, Morgan TR. Alcoholic Hepatitis. New Eng J Med. 2009;360:1533-4406. Available from: EBSCOhost Web. Accessed January 21, 2013.
73

16. Tsiaousi E, Hatzitolios A, Trygonis S, Savopoulos C. Malnutrition in end stage liver disease: Recommendations and nutritional support. J Gastroen Hepatol. 2008;23:725-533. Available from EBSCO Nursing Reference Center. Accessed January 22, 2013.
17. McClain C, Barve S, Barve A, Marsano L. Alcoholic Liver Disease and Malnutrition. Alcoholic Clin Exp Res. 2011;35:815-820. Available from EBSCO Nursing Reference Center. Accessed January 18, 2013.
18. Steinweg DL, Worth H. Alcoholism: The Keys to the CAGE. Am J Med. 1993;94: 520-523.
19. O’Shea R, Dasarathy S, McCullough A. AASLD Practice Guidelines: Alcoholic Liver Disease. Hematol. 2010;51:307-322. Available from EBSCO Nursing Reference Center. Accessed January 22, 2013.
20. Stages of liver damage. National Institute of Diabetes and Digestive and Kidney Diseases. http://www.news-medical.net/health/Fatty-Liver-What-is-Fatty-Liver.aspx. Accessed January 22, 2013.
21. Cirrhosis – Symptoms. The University of Maryland Medical Center website. Available at: http://www.umm.edu/patiented/articles/who_gets_cirrhosis_000075_3.htm. Accessed January 10, 2013.
22. Alcoholic Hepatitis (Alternative Therapy). 2012. Nursing Reference Center, EBSCO Publishing. Accessed January 12, 2013.
23. Plauth M, Merli M, Kondrup J, Weimann A, Ferenci P, Muller MJ. Consensus Statement: ESPEN Guidelines for Nutriton in Liver Disease and Transplantation. Clin Nutr. 1997(16):43-55.
24. Nutrition Care Manual. Academy of Nutrition and Dietetics Website. Available at http://nutritioncaremanual.org. Accessed January 24, 2013.
25. A.S.P.E.N. Guidelines and Standards. American Society for Parenteral and Enteral Nutrition website. 2011. Available at: https://www.nutritioncare.org/library.aspx. Accessed January 12, 2013.
26. Pronsky ZM, Crowe J. Food-Medication Interactions. 17th ed. Birchrunville, Pa: Food Medication Interactions; 2012.
27. Dugdale D. MedlinePlus Medical Encyclopedia: Bilirubin-blood. 2011. http://www.nlm.nih.gov/medlineplus/ency/article/003479.htm. Accessed December 12, 2012.
28. Pocket Guide for International Dietetics & Nutrition Terminology (IDNT) Reference Manual: Standardized Language for the Nutriton Care Process. 4th ed. Chicago,Il: Academy of Nutrition and Dietetics; 2013.
29. Steiber A, Kalantar_Zadeh K, Secker D, McCarthy M, Sehgal A, McCann L. Sujective Global Assessment in Chronic Kidney Disease: A Review. J Ren Nutr. 2004;14(4):191-200.
74