vha innovation program innovation #104 pre-procedural checklist tool (ppct) vha isb business case...
TRANSCRIPT

VHA INNOVATION PROGRAMInnovation #104 Pre-Procedural Checklist Tool (PPCT)VHA ISB Business Case
September 25, 2013

VETERANS HEALTH ADMINISTRATION
Project Background• Problem Statement – Healthcare requires coordination of multiple people and many pieces of information,
completing a series of proscribed steps, over time, in preparation for procedural events, such as a major surgical operation or in the care of critical events such as a heart attack or stroke.
– Healthcare requires coordination of multiple people and many pieces of information over time– Medical work ups consist of a series of essential steps that must be completed over time – VistA/CPRS records are limited to single author, are invisible to others prior to completion, and cannot be
filled out over time, as a work up progresses– CPRS records document a single point in time and can not be used to follow a prolonged clinical workup or
process over time • Description of Solution - The Pre-Procedural Checklist Tool (PPCT) integrates and analyzes multiple different
types of information from disparate sources over time. – PPCT allows the creation and editing of checklists for medical or surgical care– PPCT extracts data such as labs, tests, notes, medications, etc. from VistA/CPRS and writes back using the
Class I Medical Domain Web Services (MDWS) interface– PPCT stores work up data so the checklist can be filled out as work-up progresses managing work flow– Single patient view is used to document and follow the work-up of a single patient– Multi-patient view which allows managing panels of patients, such as all patients scheduled for hip
replacement– Logic editor identifies issues that are incomplete or out of range, identifying problems.
2
VETERANS HEALTH ADMINISTRATION
Execution Status
• Fully developed and functional prototype successfully completed May 2013 in the Innovation Sandbox– Includes:
• Checklist Editor, Single-Patient View, Multi-Patient View, and Logic Editor• Database for storage of work-ups in progress• Uses Class I MDWS interface and can extract, analyze, and write data to and from VistA/CPRS• Systems Based Medicine Resource Group (SBMRG) plan of validated checklists is complete
• Systems Based Medicine Resource Group (SBMRG) won first place for LVA 2012 Innovation Prize.• PPCT has been presented to NCPS, MWM VERC, CAC, VA Quality Scholars, Kaiser Permanente, VA
Anesthesia FAC, PACT, CHF QUERI, IHD QUERI, San Francisco VA Medical Center (VAMC) Performance Improvement for comments and suggested improvements
• Final code and documentation submitted to OSEHRA• Approved for production environment by OI&T Region 1• On schedule for clinical testing in Region 1 starting with San Francisco VAMC • High level, project specific, tasks required for enterprise deployment:
– MDWS enhancements may be necessary for pharmacy data, order entry, etc.– Oracle database may need to be converted over to SQL if Oracle support not available – Refine functionality/improvements identified during prototype testing during pilot and C&A – Pilot at approximately twelve (12) and Class III to Class I verification prior to national release
3

VETERANS HEALTH ADMINISTRATION
ISB Selection Criteria
4
Criteria See… Self-Assigned Score
Compliance Slide 4 1
Five-Year Net Operational Cost Change Slide 5 10
Implementation Cost Slide 6 -7
Clinical Impact (Broadness) Slide 7 10
Clinical Impact (Degree) Slide 8 10
Business Impact (Broadness) Slide 7 10
Business Impact (Degree) Slide 8 10
Patient Safety Slide 9 10
Patient Value Slide 10 15
Healthcare Disparity Slide 11 3
Summary Value = 1 * (23+48) = 71
Business Value = 10 + (-7) + 10 + 10 = 23
Clinical Value = 10 + 10 + 15 + 3 + 10 = 48
VETERANS HEALTH ADMINISTRATION
Business Case – Compliance
• PPCT is compliant with regulations, including patient safety
– A fundamental goal of the PPCT is to improve, monitor, and document compliance with approved standards of care. Standards of care can be built into checklists. Required tests, procedures, checks, notes, tests can be required elements in checklist. Checklist elements that are not completed or are out of date or range are flagged red by the logic
editor. Overriding or checklist elements is allowed but all over ride decisions are documented to time,
data, and author.
– PPCT has been approved for production testing by OI&T Region 1
– Uses Class I MDWS interface for data exchange with VistA/CPRS
– PPCT complies with patient safety requirements
5
Self Assigned Score: 1

VETERANS HEALTH ADMINISTRATION
Business Case – 5 Year Net Operational Cost Change
• This innovation creates two major sources of benefit totaling more than $700 million in net savings over five years:
– Cost savings associated with reductions in surgical cancellations: $41.6 million over the first five years of deployment and $30.25 million annually thereafter
– Cost savings from reductions in surgical morbidity and mortality: $850 million over the first five years of deployment and $400 million annually thereafter
6
Data Element Amount
Approx. number of surgical cancellations in FY12 (national) 60,500 (13%)
Cost of surgical cancellation $2,000-$10,000
Anticipated reduction in cancellation rate 25%
Annual cost savings from reduced surgical cancellations $30.25 million
Data Element Amount
Approx. number of morbidity or mortality events in FY12 (national) 41,140 (9%)
Cost of morbidity or mortality event $28,00-$60,000Anticipated reduction in rate of morbidity/mortality 35-50%
Annual cost savings from reduced reductions in morbidity/mortality $400 million
Self Assigned Score: 10
Cost Savings from Reduced Surgical Cancellations Cost Savings from Reduced Surgical Morbidity/Mortality

VETERANS HEALTH ADMINISTRATION
Business Case - Implementation Costs
7
Year 1 Year 2 Year 3 Year 4 Year 5
Pilot Phase $1,000,000 $1,000,000 $0 $0 $0
Deployment Phase $0 $1,000,000 $3,000,000 $3,000,000 $3,000,000
Annual Total $1,000,000 $2,000,000 $3,000,000 $3,000,000 $3,000,000
Cumulative Costs $1,000,000 $3,000,000 $6,000,000 $9,000,000 $12,000,000
Self Assigned Score: -7

VETERANS HEALTH ADMINISTRATION
Business Case – Clinical Impact
• Broadness: PPCT positively impacts many clinical performance metrics. PPCT is designed to improve compliance.
8
Self Assigned Score, Broadness: 10Self Assigned Score, Degree: 10
Clinical Performance Metric Degree of Impact
Surgery (SIP1a, SIP3an, SIP14, SIP8, SIP10a, SIP12, SIP25, SIP26, SIP13, SIP90) 25% improvement
Diabetes (DMG90, 25hs, 23h, 31h, 32h, 27h, 34h, c9h) 25% improvement
Clinical Practice Guideline Index (CPGI4) 25% improvement
AMI (IHI90, 1, 6, 7, 9, 47, 61), HF (CHI70, 7, 10, 19,), HTN9h, 25% improvement
Getting Care Quickly (OP) WTM53 25% improvement
Access list 14 days- Specialty Care 25% improvement
• Degree: PPCT positively impacts these metrics in the following ways- Allows coordination of multiple team members, referring physicians, nurses, surgeons, internists- Standardizes surgical and medical works ups and follows standards of care- Reduces surgical mortality by 35 to 50%- Reduces surgical morbidity by 35 to 50%- Reduces cost from surgical cancellations, morbidity, mortality, and medical errors- Reduces surgical cancellations from inadequate or incomplete work ups- Reduces time for surgical work ups and prevents delays- Reduces inappropriate clinical testing- Identifies critical work up elements that are incomplete or abnormal or out of date

VETERANS HEALTH ADMINISTRATION
Business Case – Business Impact
• Broadness: PPCT positively impacts six (6) business performance metrics
9
Self Assigned Score, Broadness: 10Self Assigned Score, Degree: 10
• Degree: PPCT positively impacts these metrics in the following ways- Allows coordination of multiple team members, referring physicians, nurses, surgeons, internists- Standardizes surgical and medical works ups and follows standards of care- Reduces surgical mortality by 35 to 50%- Reduces surgical morbidity by 35 to 50%- Reduces cost from surgical cancellations, morbidity, mortality, and medical errors- Reduces surgical cancellations from inadequate or incomplete work ups- Reduces time for surgical work ups and prevents delays- Reduces inappropriate clinical testing- Identifies critical work up elements that are incomplete or abnormal or out of date
Business Performance Metric Degree of Impact
Improved accuracy of decision making (quality of work) 25% improvement
Standardization of best practices (quality of work) 25% improvement
Enhanced data access, integrity, or aggregation (quality of work) 25% improvement
Reduces program or organizational risk (quality of work) 25% improvement
Reduces costs (VA staff efficiency or workflow) 25% improvement
Improves the environment of care (Veteran/beneficiary’s experience) 25% improvement

VETERANS HEALTH ADMINISTRATION
Business Case - Patient Safety
• PPCT demonstratively improves patient safety
- Standardizes surgical and medical work ups reducing iatrogenic injury.- Identifies critical lab values and incomplete work ups.- Reminds staff of critical steps in processes. - Improves communication and coordination of staff during work ups.- Improves compliance with, and adoption of, standards of care.- Reduces surgical mortality by 35-50%- Reduces surgical morbidity by 35-50%
Evaluation CriteriaScored -10 to 10 where -10 is severe decrease in patient safety, 0 is no change in patient safety and +10 is very strong impact in patient safety
1. Demonstratively reduces preventative harm in this population: 102. Reduces mortality and morbidity in this population: 103. Improves patient safety by demonstratively reducing the chance of human error: 10
10
Self Assigned Score: 10

VETERANS HEALTH ADMINISTRATION
Business Case – Patient Value
• This solution significantly increases patient satisfaction and it is anticipated VA would be contacted with written accolades
- Decreases surgical cancellation rates
- Reduces time for surgical work ups and prevents delays
- Decreases waiting time for surgery by better management of pre surgical work ups
- Reduces unnecessary preoperative testing and iatrogenic injury
- Improves compliance with, and adoption of, standards of care.
- Reduces disparity in VHA healthcare by standardizes work ups throughout VHA
- Reduces surgical mortality by 35-50%
- Reduces surgical morbidity by 35-50%
11
Self Assigned Score: 15
VETERANS HEALTH ADMINISTRATION
Business Case – Healthcare Disparity
• PPCT addresses a healthcare disparity with regard to standardization of care
– PPCT is designed to standardize medical and surgical pre-procedural work ups
– Patients will receive standardized care driven by checklists thus reducing the disparity
in healthcare
– Best practice checklists from each VAMC will be shared across the VHA system reducing
healthcare disparity between VAMCs
– VAMCs with special expertise will develop checklists that can then be used by all VAMCs
thus reducing system-wide disparities in specialty healthcare
– Increased adoption of and compliance with standards of care across VHA system will
reduce the disparity in healthcare
– Care will be uniform and the best care possible regardless of the VAMC location
12
Self Assigned Score: 3
VETERANS HEALTH ADMINISTRATION
Back Up Slides
13

VETERANS HEALTH ADMINISTRATION
Other Considerations – Data Sources Used to Estimate Cost Savings Resulting from PPCT
14
• Number of surgical cancellations in FY12: VASQIP 2012• Cost associated with surgical morbidity and mortality: VASQIP 2012, NSQIP 2004, • Costs associated with surgical cancellation:
– Data pulled from SF VAMC; costs associated with surgical cancellation include cost of un-used OR time, wasted equipment, contract employees, etc.
• Anticipated reduction in cancellation rate: – Observed reduction in cancellation rate with simple checklist was 75%. Model used 25% reduction to increase aplicability.
• Approximate number of morbidity and mortality events in FY12: VASQIP 2012– Mortality 4,571– Morbidity 36,569
• Costs associated with morbidity or mortality event:– $28,000 Veterans Affairs Surgical Quality Improvement Program (NSQIP) 2004 data– $37,000 - $45,000: Veterans Affairs Surgical Quality Improvement Program (VASQIP) 2012 data. Wakefield H, Vaughan-Sarrazin
M, Cullen JJ. Am J Surg. 2012 Oct;204(4):434-40.• Anticipated reduction in rate of morbidity/mortality:
– 35% Reduction in mortality.: Wallace, AW, Selwyn Au, S. Cason, BA. Association of the Pattern of Use of Perioperative b-Blockade and Postoperative Mortality. Anesthesiology 2010 113:794-805.
– 50% Reduction in mortality: Mangano D.T., Layug E.L., Wallace A., Tateo I., and the Multicenter Study of Perioperative Ischemia (McSPI) Research Group.
– 50% Reduction: Effect of Atenolol on Mortality and Cardiovascular Morbidity after Noncardiac Surgery. N. Engl. J. Med. 335(23): 1713-1720, 1996.
– 50% Reduction Weisner et al Effect of a 19-item surgical safety checklist during urgent operations in a global patient population. Ann Surg. 2010 May;251(5):976-80.
VETERANS HEALTH ADMINISTRATION
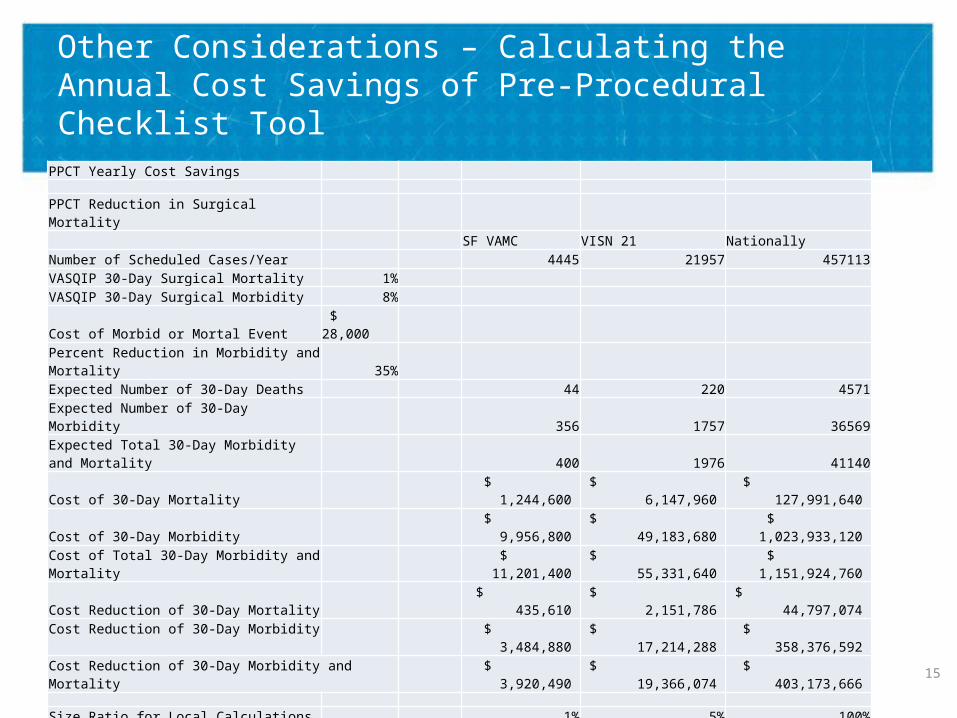
Other Considerations – Calculating the Annual Cost Savings of Pre-Procedural Checklist Tool
15
PPCT Yearly Cost Savings
PPCT Reduction in Surgical MortalitySF VAMC VISN 21 Nationally
Number of Scheduled Cases/Year 4445 21957 457113VASQIP 30-Day Surgical Mortality 1%VASQIP 30-Day Surgical Morbidity 8%Cost of Morbid or Mortal Event $ 28,000 Percent Reduction in Morbidity and Mortality 35%Expected Number of 30-Day Deaths 44 220 4571Expected Number of 30-Day Morbidity 356 1757 36569Expected Total 30-Day Morbidity and Mortality 400 1976 41140Cost of 30-Day Mortality $ 1,244,600 $ 6,147,960 $ 127,991,640 Cost of 30-Day Morbidity $ 9,956,800 $ 49,183,680 $ 1,023,933,120 Cost of Total 30-Day Morbidity and Mortality $ 11,201,400 $ 55,331,640 $ 1,151,924,760 Cost Reduction of 30-Day Mortality $ 435,610 $ 2,151,786 $ 44,797,074 Cost Reduction of 30-Day Morbidity $ 3,484,880 $ 17,214,288 $ 358,376,592 Cost Reduction of 30-Day Morbidity and Mortality $ 3,920,490 $ 19,366,074 $ 403,173,666
Size Ratio for Local Calculations 1% 5% 100%
PPCT Reduction in Cost of Medical AdmissionsNumber of Medical Admissions 6,729 33,240 692,000 Cost of Medical Care $ 442,652,423 $ 2,186,573,508 $ 45,521,299,625 Number of Unique Patients 54,119 267,330 5,565,427 Cost of Medical Care per unique patient $ 8,179 $ 8,179 $ 8,179 Estimated Cost of Medical Admission $5,000 $ 33,645,291 $ 166,197,899 $ 3,460,000,000 Percent Reduction in Cost of Medical Admission 10% $ 3,364,529.1 $ 16,619,789.9 $ 346,000,000.0
Total Yearly Cost Savings for Reduction in Surigcal and Medical Morbidity and Mortality $ 7,285,019 $ 35,985,864 $ 749,173,666
VETERANS HEALTH ADMINISTRATION
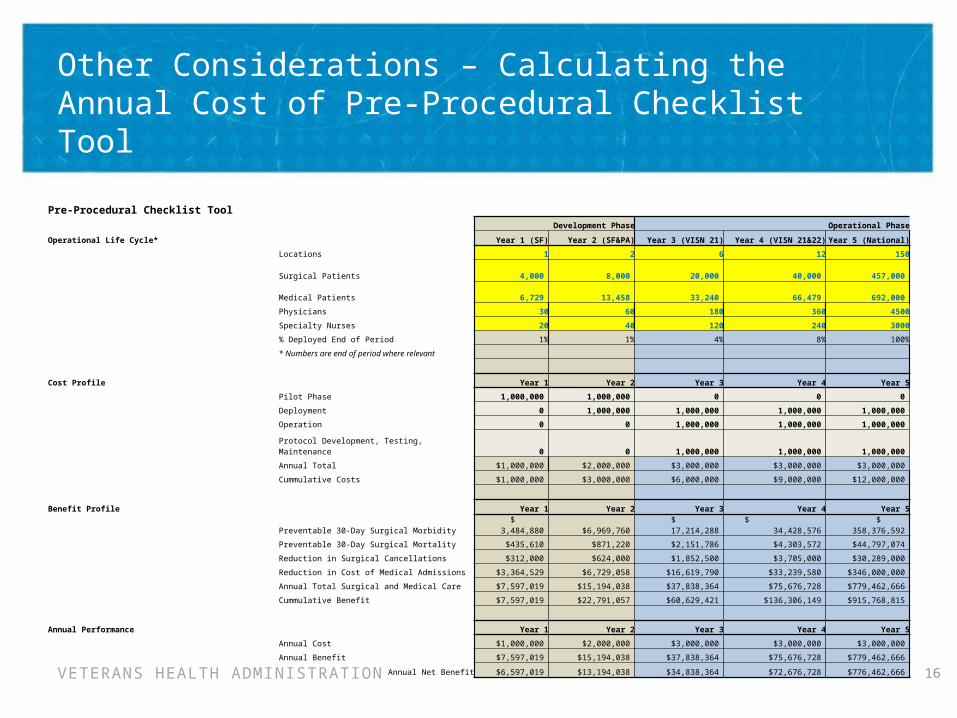
Other Considerations – Calculating the Annual Cost of Pre-Procedural Checklist Tool
16
Pre-Procedural Checklist ToolDevelopment Phase Operational Phase
Operational Life Cycle* Year 1 (SF) Year 2 (SF&PA) Year 3 (VISN 21) Year 4 (VISN 21&22) Year 5 (National)
Locations 1 2 6 12 150
Surgical Patients 4,000 8,000 20,000 40,000 457,000
Medical Patients 6,729 13,458 33,240 66,479 692,000
Physicians 30 60 180 360 4500
Specialty Nurses 20 40 120 240 3000
% Deployed End of Period 1% 1% 4% 8% 100%
* Numbers are end of period where relevant
Cost Profile Year 1 Year 2 Year 3 Year 4 Year 5
Pilot Phase 1,000,000 1,000,000 0 0 0
Deployment 0 1,000,000 1,000,000 1,000,000 1,000,000
Operation 0 0 1,000,000 1,000,000 1,000,000
Protocol Development, Testing, Maintenance 0 0 1,000,000 1,000,000 1,000,000
Annual Total $1,000,000 $2,000,000 $3,000,000 $3,000,000 $3,000,000
Cummulative Costs $1,000,000 $3,000,000 $6,000,000 $9,000,000 $12,000,000
Benefit Profile Year 1 Year 2 Year 3 Year 4 Year 5
Preventable 30-Day Surgical Morbidity $ 3,484,880 $6,969,760 $ 17,214,288 $ 34,428,576 $ 358,376,592
Preventable 30-Day Surgical Mortality $435,610 $871,220 $2,151,786 $4,303,572 $44,797,074
Reduction in Surgical Cancellations $312,000 $624,000 $1,852,500 $3,705,000 $30,289,000
Reduction in Cost of Medical Admissions $3,364,529 $6,729,058 $16,619,790 $33,239,580 $346,000,000
Annual Total Surgical and Medical Care $7,597,019 $15,194,038 $37,838,364 $75,676,728 $779,462,666
Cummulative Benefit $7,597,019 $22,791,057 $60,629,421 $136,306,149 $915,768,815
Annual Performance Year 1 Year 2 Year 3 Year 4 Year 5
Annual Cost $1,000,000 $2,000,000 $3,000,000 $3,000,000 $3,000,000
Annual Benefit $7,597,019 $15,194,038 $37,838,364 $75,676,728 $779,462,666
Annual Net Benefit $6,597,019 $13,194,038 $34,838,364 $72,676,728 $776,462,666

VETERANS HEALTH ADMINISTRATION
PPCT: Multi-Patient View allows review of all patients scheduled for a procedure, or all patients with a common problem such as diabetes.
17
VETERANS HEALTH ADMINISTRATION
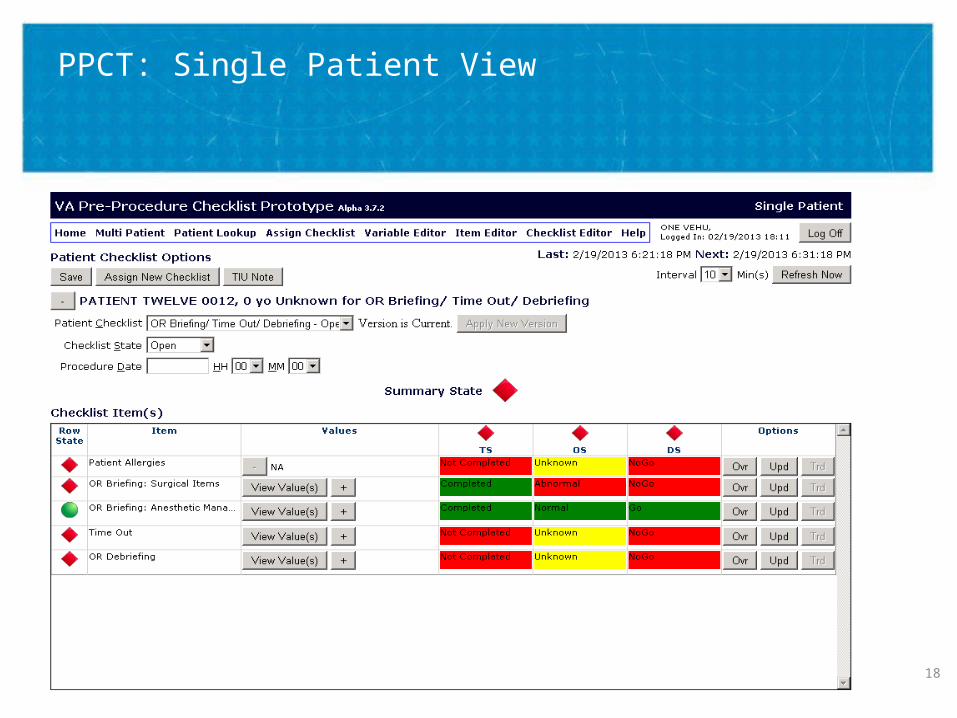
PPCT: Single Patient View
18
VETERANS HEALTH ADMINISTRATION
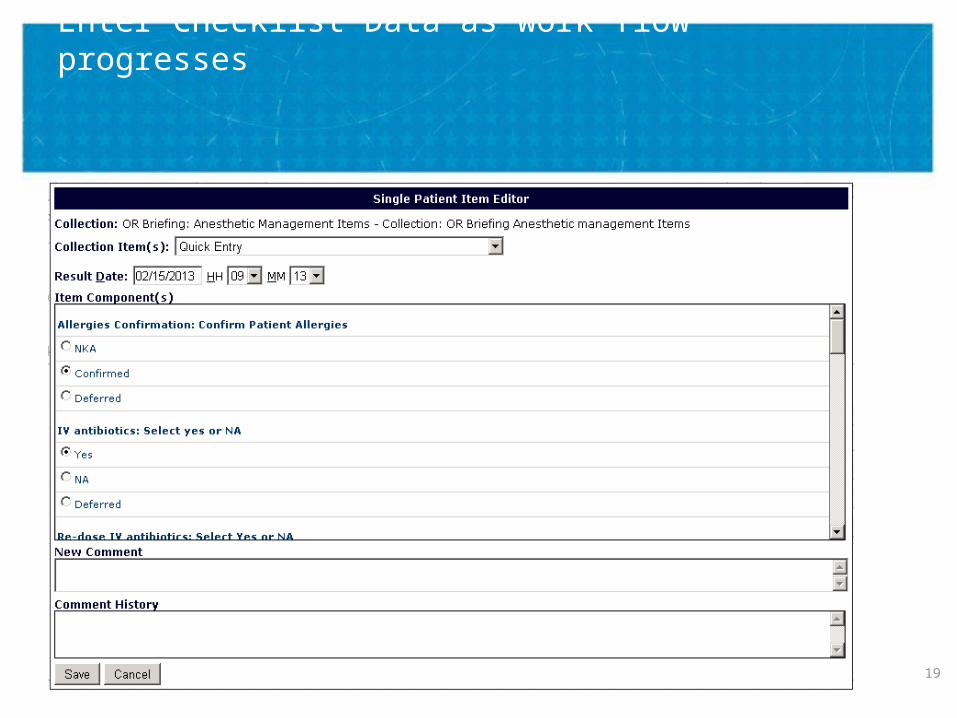
Enter Checklist Data as work flow progresses
19

VETERANS HEALTH ADMINISTRATION
PPCT: Review checklist data for completeness and problems.
20

VETERANS HEALTH ADMINISTRATION
PPCT: Checklist work up stored in CPRS as a text note and in database for analysis.
21

VETERANS HEALTH ADMINISTRATION
PPCT: Can extract data from Vista/CPRS, analyze, and write notes back to CPRS. Lab data example.
22
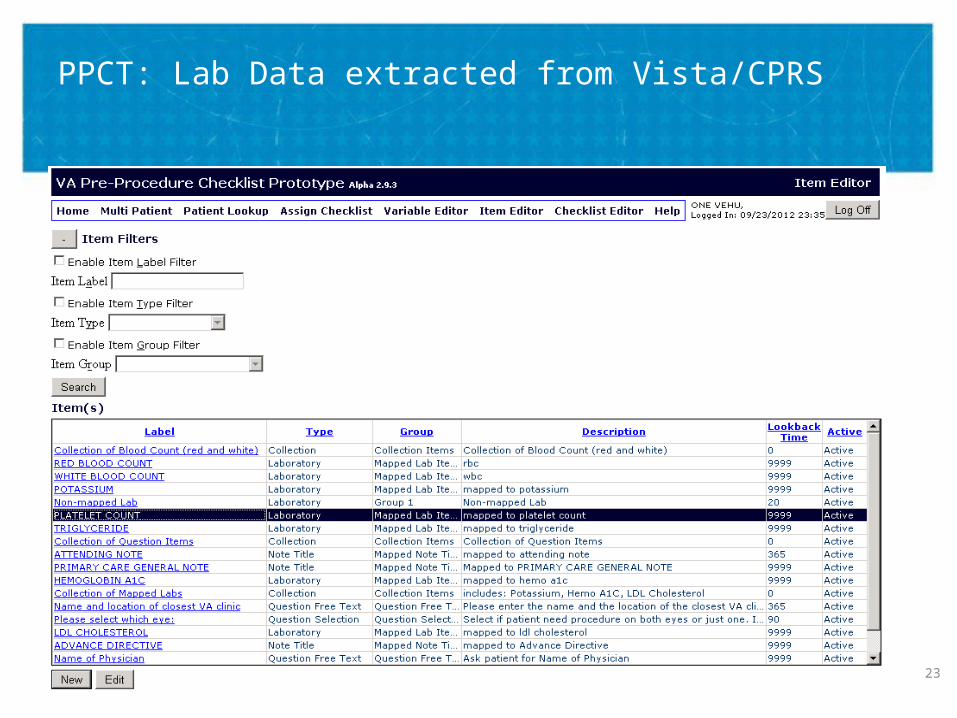
VETERANS HEALTH ADMINISTRATION
PPCT: Lab Data extracted from Vista/CPRS
23

VETERANS HEALTH ADMINISTRATION
PPCT: Editor allows creation and editing of checklist – Add items
24

VETERANS HEALTH ADMINISTRATION
PPCT: Checklists can have questions for completion. Checklist editor is flexible to allow many different types of checklists.
25
VETERANS HEALTH ADMINISTRATION
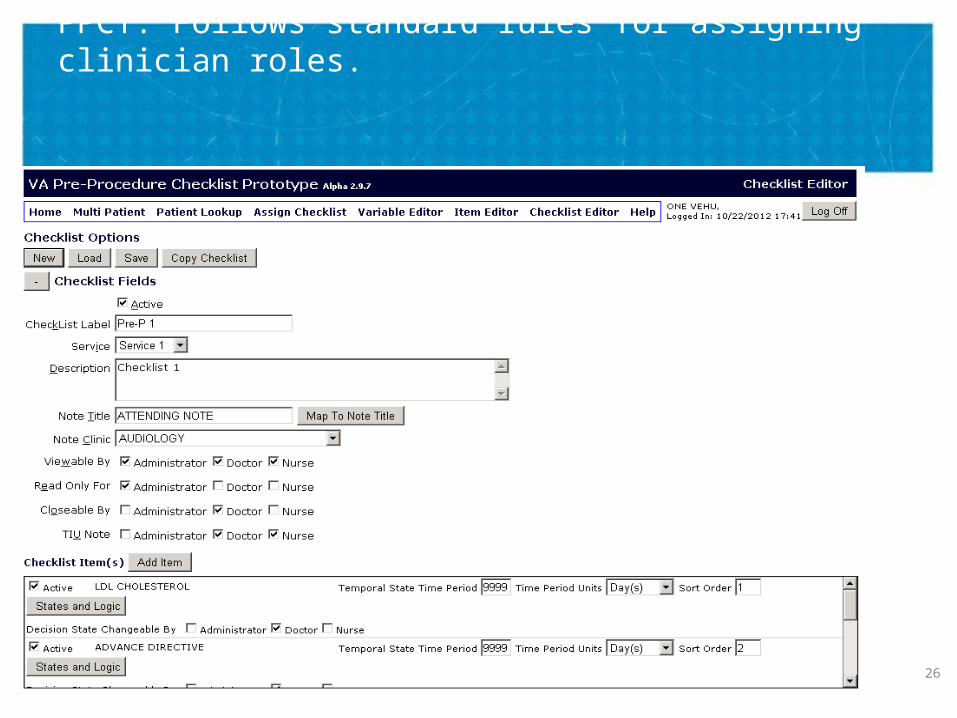
PPCT: Follows standard rules for assigning clinician roles.
26

VETERANS HEALTH ADMINISTRATION
PPCT: Logic editor allows validation of data and identification of problems.
27
VETERANS HEALTH ADMINISTRATION
PPCT: Possibilities for using Checklist for Quality Improvement
• Presurgical workup guidance (like SQWM)• Preoperative briefing-timeout-debriefing• Guidelines for acute MI, congestive heart
failure• Discharge planning• Managing panels of patients• PACT
28
VETERANS HEALTH ADMINISTRATION
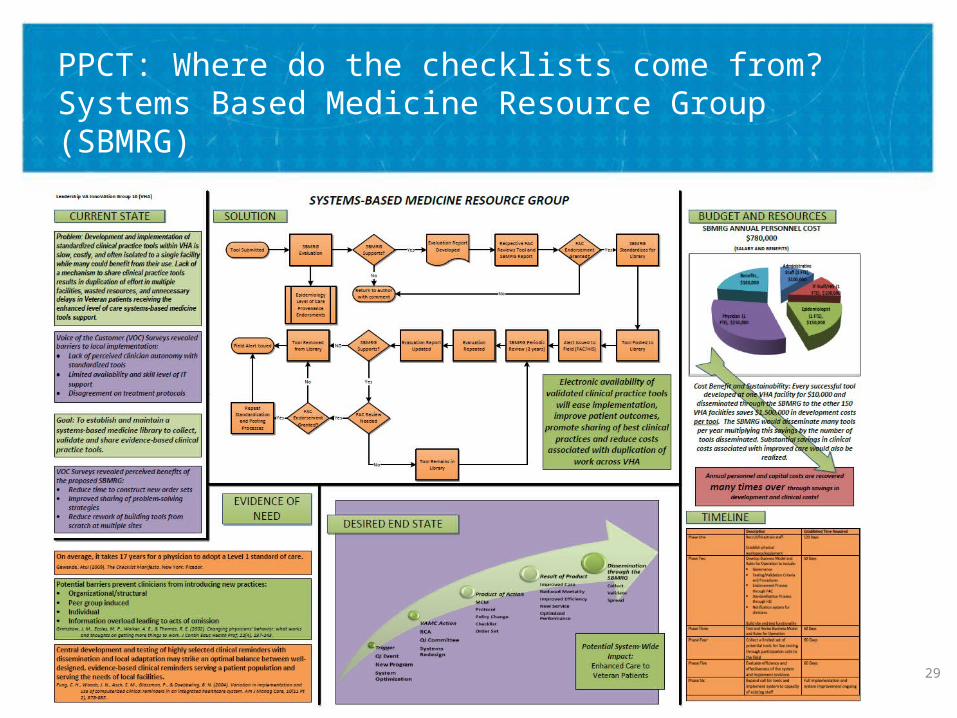
PPCT: Where do the checklists come from? Systems Based Medicine Resource Group (SBMRG)
29