vertebroplasty for osteoporotic crush fractures
TRANSCRIPT

Percutaneous vertebroplasty
Dr David Lisle
Brisbane Private Imaging Royal Brisbane Hospital University of Queensland

• 85 year old female • Severe acute mechanical back pain
– Pain not managed with high dose therapy – Can’t sleep – Limited walking to only a few steps
• Spontaneous onset • No known trauma • No known malignancy



Vertebral compression fracture
• Radiographic or symptomatic clinical event • Radiographic: 26% women >50 years • USA/year: 150,000 hospital admissions;
5,000,000 restricted days • ↓ VC and FEV • ↑ mortality
– ≥ 1 # : 1.23 x age adjusted – ≥ 5 # : >2 x age adjusted
Mathis AJNR 2001;22:373-381



Indications
• Painful crush fracture – Osteoporosis – Acute: 4-6 weeks
• Malignant crush fracture – +/- biopsy
• Haemangioma – Galibert Neurochirurgie 1987;33:166-8

Patient selection = key to success
• Back pain – Sudden onset – May radiate anteriorly – NOT sciatica – Mechanical – Restricted activity – Poor sleep
• Local tenderness • Imaging

Patient selection
• Purposes of pre-procedure imaging: – Confirm presence of crush fracture – Confirm that crush fracture is acute – Diagnose other acute levels – Integrity of spinal canal – Accurately localise level

Imaging techniques
• Plain films: – Confirm presence of crush fracture – Confirm that crush fracture is acute – Diagnose other acute levels – Integrity of spinal canal – Accurately localise level


24/3/2001
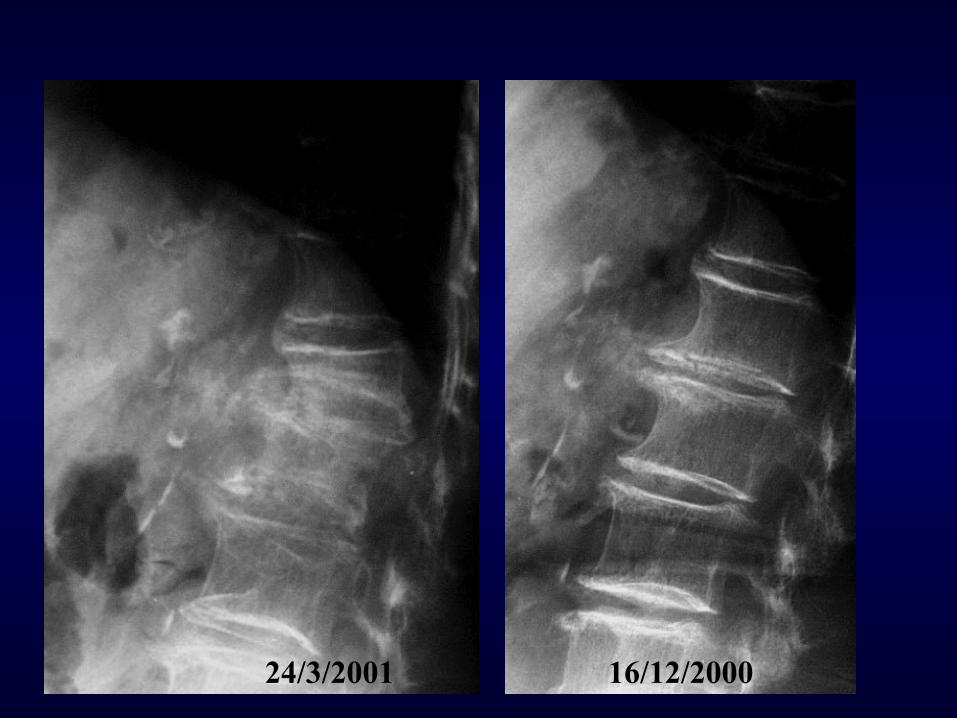
24/3/2001 16/12/2000

Imaging techniques
• MRI: – Confirm presence of crush fracture – Confirm that crush fracture is acute – Diagnose other acute levels – Integrity of spinal canal – Accurately localise level

MRI pre-vertebroplasty
• Sagittal plane • T1 for anatomy • T2 fat saturation or
STIR – Marrow black – Oedema white
STIR

MRI
2
3
2
3
T1 STIR

Procedure

Patient preparation
• Ensure MRI done and available • (Coagulation profile) • Pre-sedation fast • Sedation and pain relief
– iv cannula – Fentanyl + Midazolam
• Sterile swab and drape

Needle placement: Thoracic



Needle placement: Lumbar


Cement preparation





Cement injection

Post procedure care
• Lie prone for 20 minutes • Bed rest for 2-3 hours • CT to document cement placement • Discharge if well
– Post-sedation instructions – Rest 24 hours – Mobilize according to pain
• Advise re muscle pain • Follow-up phone call(s)

Complications: rare
• Mild fever; nausea for 24 hours • Rib fracture • Foraminal leak • Spinal canal leak • Venous emboli



Literature
• Amar Neurosurg 2001;49:1105 – 97 pat., 258 levels – ‘better life’ 74%
• Narcotic/analgesic use • Mobility • Better sleep
• Evans Radiology 2003;226:366 – 488 pat, 245 follow-up – Pain scale 8.9 → 3.4 – Impaired ambulation:
• 72% pre → 28% post
Literature
• Diamond MJA 2006;184:113-117 – Conservative Rx vs PCV (non-randomised) – Acute pain 1-6 weeks, not relieved analgesics – MRI: acute fracture(s) – 3 factors: pain (VAS); physical function;
hospital days – 24 hours and 6 weeks: 60% ↓ pain scores;
29% ↑ physical function; 43% ↓ hospital days – Similar clinical outcomes at 6/12, 12/12, 24/12.

My results
• Audit of first 250 patients, 2001 to 2006 • Complete or near complete response
– No or minimal pain – Good return of activity level – 83.0 %
• Moderate response – Still suffer pain, though noticeably reduced – Some return of activity, though still restricted – 12.0 %
• No response – 5.0 %

Percutaneous vertebroplasty Keys to success
• Patient selection – Early referral – MRI
• High quality fluoroscopy – Accurate needle placement – Cement injection
• Nursing care – Cement preparation – Patient care: pre and post

Percutaneous vertebroplasty
• Indications • Patient selection
– Clinical assessment – Imaging
• Technique – Needle placement – Post-procedure care
• Results

MBS funding September 2005

So, what happened?
• Buchbinder NEJM 2009;361:557-68 – Multicentre, randomized, double blind – Vertebroplasty vs placebo ‘sham’
procedure – N = 78: 38 vertebroplasty, 40 sham – No difference in pain scales or quality of
life • MJA (Editorial) 2009;191:476-7
– ‘Percutaneous vertebroplasty is not an effective treatment for acute osteoporotic vertebral fractures’

• Patient selection – Up to 12 months pain
• Recruitment – Majority of eligible
patients not recruited • Technique
– Up to 3ml cement – Stopped injection if
leaking

MBS funding withdrawn 2011

Where are we now? • Uncommon in most places • Ongoing studies
– eg randomised trial in Sydney for acute fractures; recruitment very slow
• Included in appropriateness guidelines in UK and USA – http://www.nice.org.uk/guidance/IPG12/chapter/1-
Guidance – http://www.acr.org/
• No Medicare rebate • Our cost: 1400 + day bed about 700


Thank you