vegf gene and phenotype relation with alzheimer's disease and mild cognitive impairment
TRANSCRIPT

REJUVENATION RESEARCHVolume 9, Number 4, 2006© Mary Ann Liebert, Inc.
VEGF Gene and Phenotype Relation with Alzheimer’sDisease and Mild Cognitive Impairment
MARTINA CHIAPPELLI,1 BARBARA BORRONI,2 SILVANA ARCHETTI,2ELENA CALABRESE,3 MASSIMILIANO M. CORSI,4 MASSIMO FRANCESCHI,5
ALESSANDRO PADOVANI,2 and FEDERICO LICASTRO1
ABSTRACT
Background: The expression of vascular endothelial growth factor (VEGF) represents one po-tential mechanism whereby vascular and Alzheimer’s disease (AD) pathologies are related.The authors investigated whether AD cases, especially those having a rapid cognitive decline,more commonly carried a functional promoter gene variant for VEGF (�2578C/A) and showedelevated plasma levels of Vegf. In addition, the authors investigated whether patterns of as-sociation also were found for mild cognitive impairment (MCI) and conversion from MCI toAD. Methods: Group 1 included 317 AD cases and 320 unaffected control subjects. Group 2included 113 MCI patients and 130 control subjects. Plasma levels of Vegf were measured bychemiluminescence for a subset of group 1. Genotype determinations were made for all sub-jects. Findings: The VEGF AA genotype was associated with an increased risk of developingAD (OR � 1.616, p � 0.046). This genotype also was associated with an accelerated cognitivedecline in APOE �4 positive patients with AD (AA vs. CC OR � 6.5, p � 0.04). The VEGF AAgenotype was a risk factor for MCI (OR � 2.5, p � 0.037) and MCI conversion to AD in APOE�4� (OR � 6.5, CI � 2.014–20.980; p � 0.002). Vegf plasma levels were higher in patients withAD than controls (230 pg/mL vs. 42 pg/mL), and were even higher in those patients with afast cognitive decline and the APOE �4 allele. Interpretation: Modulation of VEGF expressionis a potential mechanism associated with the risk of developing AD and its clinical deterio-ration.
485
INTRODUCTION
ALZHEIMER’S DISEASE (AD) is a chronic neu-rodegenerative disease, characterized by a
progressive impairment of cognitive functionsand memory loss.1 Neurofibrillary tangles,
�-amyloid plaques, neuron loss, and astroglio-sis2 are major pathologic hallmarks of the ADbrain.
Mild cognitive impairment (MCI), defined asmemory deficits with preservation of othercognitive and functional brain activities, may
1Department of Experimental Pathology, School of Medicine, University of Bologna, Bologna, Italy.2Neurology Unit, Center for Brain Aging and Neurodegenerative Disorders, University of Brescia, Brescia, Italy.3Neurology Department, Don Gnocchi Foundation, Milan, Italy.4Institute of General Pathology, Laboratory of Clinical Pathology, University of Milan, Milan, Italy.5Department of Neurology, University of Castellanza, Milan, Italy.

be the initial clinical stage of the disease;3 how-ever, not all individuals with MCI progress toAD.4 Etiopathogenetic mechanisms associatedwith age-related cognitive decline and AD arecomplex and still largely unclear. Probablyboth genetic and environmental factors are im-plicated in the pathogenesis of the disease.5
Findings from a population study suggestedthat vascular risk factors are associated with in-cidence of AD.6 A recent report showed thatcoronary artery disease was associated withAD neuropathology.7 Moreover, cerebrovascu-lar alterations also are often observed in pa-tients with MCI.8
It has been suggested recently that AD couldbe an angiogenesis-dependent disorder, andabnormal endothelium activation might lead toamyloid deposition and neuronal death.9 Animpairment of neurovascular mechanismsleading to brain ipoperfusion, vessel regres-sion, and neurovascular inflammation alsohave been suggested to be involved in AD.10 Arecently emerging body of evidence shows thatabnormalities in vascular functions are presentin patients with AD. In fact, significant cerebralmicrovascular pathology,11 deficient clearanceof A� across the blood–brain barrier12 and in-creased density of microvessels in the patho-logic lesions13 are frequent neuropathologicfeatures of AD. In addition, gene array analy-sis has shown marked upregulation of angio-genesis-relevant genes in the brain with AD.14
Vegf, a major angiogenic factor and primeregulator of endothelial cell proliferation, hasbeen implicated recently in neuronal survival,neuroprotection, regeneration, growth, differ-entiation, and axonal outgrowth.15 EnhancedVegf immunoreactivity has been found in theneurocortex of patients with AD, and the ex-pression of this compound has been shown inreactive astrocytes and endothelial cells sur-rounding amyloid deposits in brains withAD.16
The human VEGF gene is located on chromo-some 6p21.3, and consists of eight exons and fivepolymorphisms in the promoter region of thegene have been described.17 A polymorphism(C-2578A) within the VEGF promoter recentlywas correlated with the risk of developing AD.18
However, two independent investigations didnot confirm these findings.19,20
The present authors report data showing thatthe promoter C-2578A SNP in the VEGF geneis associated with increased risk of developingAD, cognitive deterioration during its clinicalcourse, and MCI conversion to AD. The rate ofcognitive decline was influenced by an appar-ent interaction between the VEGF A allele andAPOE �4 allele in both AD and MCI patients.Vegf plasma levels in patients with AD werehigher than controls. Elevated plasma Vegf waspresent in patients with AD with the APOE �4allele and a high rate of cognitive decline.
SUBJECTS AND METHODS
Subjects
Clinical diagnosis of probable AD was per-formed according to standard clinical proce-dures and followed the NINCDS/ADRDA21
and DSM-III-R22 criteria. Diagnoses of proba-ble AD were performed after patient evalua-tion by two independent physicians accordingto brain computed tomography scans. Cogni-tive performances and alterations were mea-sured by the mini-mental state examination(MMSE) and the global deterioration scale(GDS). Longitudinal cognitive performancesduring a 2-year follow-up of patients with ADwere assessed by MMSE scores as described.23
Patients with AD were divided into two groupsaccording to MMSE scores; that is, those withslow decline (�4.9 points/year), and thosewith fast decline (�5 points/year).
Two populations of patients with a clinicaldiagnosis of AD were included in the study.The first AD population (n � 77; mean age �77 � 7, men � 32%) was enrolled from north-ern Italy at Don Gnocchi Foundation (Milan,Italy); the second one (n � 240; mean age �76 � 8, men � 33%), also from Northern Italy,was enrolled at the Department of Neuro-science of Castellanza University near the met-ropolitan Milan area.
Patients with AD were then followed up atthe Don Gnocchi Foundation and Departmentof Neuroscience of Castellanza University, re-spectively. Non-demented controls consistedof 320 elderly subjects from the same geo-graphic area (mean age � 73 � 5, men � 35%)
CHIAPPELLI ET AL.486
who were in good health and without cogni-tive impairment (MMSE � 26).
A second case-control population consistedof 113 MCI subjects (mean age � 71 � 8,men � 33%) and 130 controls (mean age �70 � 7, men � 39%) from the Department ofNeurology, University of Brescia, northernItaly. Diagnosis of MCI was performed ac-cording to current clinical criteria.24
Patients and controls were white, and in-formed consent from each subject or a relative
of each AD patient was obtained. This studywas approved by the Medical Ethical Commit-tee of the Don Gnocchi Foundation, Milan.
DNA extraction and polymorphism detection
DNA extraction from peripheral bloodleukocytes were assessed as described.25
The triallelic APOE �2-4 polymorphism wasassessed by a polymerase chain reaction(PCR)–based method as described.26
VEGF GENE IS ASSOCIATED WITH MCI AND AD 487
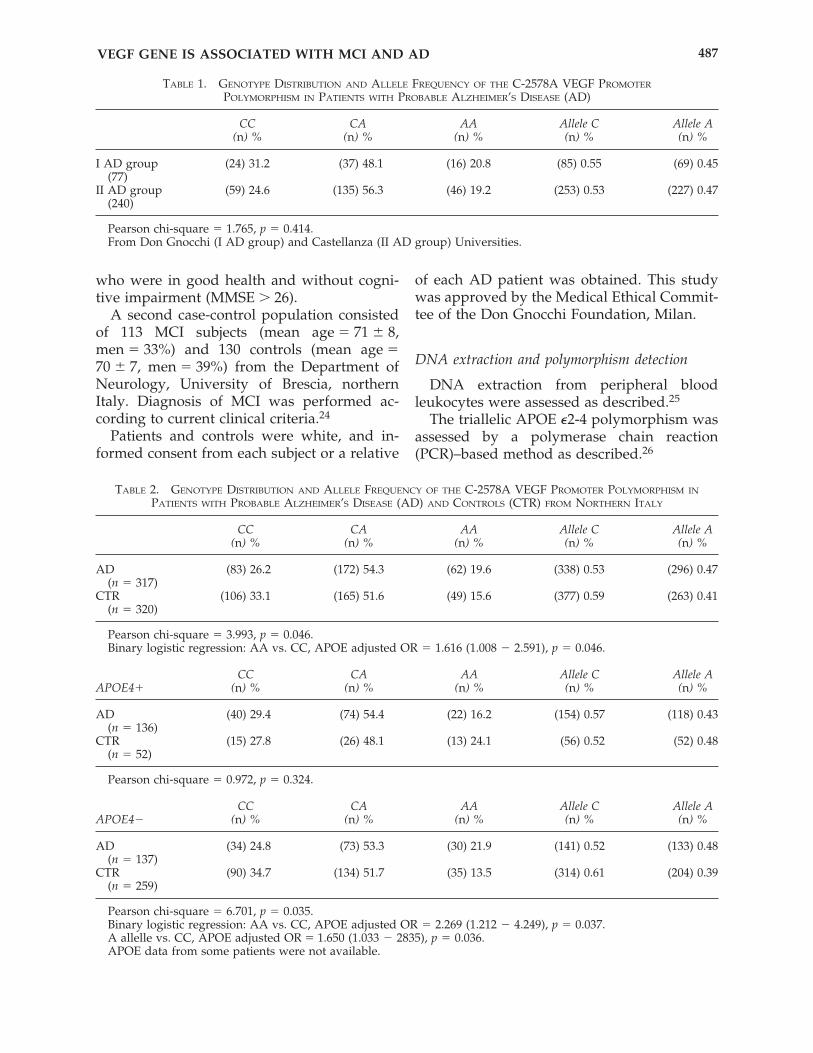
TABLE 1. GENOTYPE DISTRIBUTION AND ALLELE FREQUENCY OF THE C-2578A VEGF PROMOTER
POLYMORPHISM IN PATIENTS WITH PROBABLE ALZHEIMER’S DISEASE (AD)
CC CA AA Allele C Allele A(n) % (n) % (n) % (n) % (n) %
I AD group (24) 31.2 (37) 48.1 (16) 20.8 (85) 0.55 (69) 0.45(77)
II AD group (59) 24.6 (135) 56.3 (46) 19.2 (253) 0.53 (227) 0.47(240)
Pearson chi-square � 1.765, p � 0.414.From Don Gnocchi (I AD group) and Castellanza (II AD group) Universities.
TABLE 2. GENOTYPE DISTRIBUTION AND ALLELE FREQUENCY OF THE C-2578A VEGF PROMOTER POLYMORPHISM IN
PATIENTS WITH PROBABLE ALZHEIMER’S DISEASE (AD) AND CONTROLS (CTR) FROM NORTHERN ITALY
CC CA AA Allele C Allele A(n) % (n) % (n) % (n) % (n) %
AD (83) 26.2 (172) 54.3 (62) 19.6 (338) 0.53 (296) 0.47(n � 317)
CTR (106) 33.1 (165) 51.6 (49) 15.6 (377) 0.59 (263) 0.41(n � 320)
Pearson chi-square � 3.993, p � 0.046.Binary logistic regression: AA vs. CC, APOE adjusted OR � 1.616 (1.008 � 2.591), p � 0.046.
CC CA AA Allele C Allele AAPOE4� (n) % (n) % (n) % (n) % (n) %
AD (40) 29.4 (74) 54.4 (22) 16.2 (154) 0.57 (118) 0.43(n � 136)
CTR (15) 27.8 (26) 48.1 (13) 24.1 (56) 0.52 (52) 0.48(n � 52)
Pearson chi-square � 0.972, p � 0.324.
CC CA AA Allele C Allele AAPOE4� (n) % (n) % (n) % (n) % (n) %
AD (34) 24.8 (73) 53.3 (30) 21.9 (141) 0.52 (133) 0.48(n � 137)
CTR (90) 34.7 (134) 51.7 (35) 13.5 (314) 0.61 (204) 0.39(n � 259)
Pearson chi-square � 6.701, p � 0.035.Binary logistic regression: AA vs. CC, APOE adjusted OR � 2.269 (1.212 � 4.249), p � 0.037.A allelle vs. CC, APOE adjusted OR � 1.650 (1.033 � 2835), p � 0.036.APOE data from some patients were not available.
The VEGF C-2578A promoter polymorphism(rs699947) was detected by electrophoresedPCR fragments on 3% MS agarose gel. The Aallele consisted of an 18–nucleotide insertionalways associated with the –2578A allele,whereas CC homozygous did not show this in-sertion.
Vegf plasma level measurement
Biochip array technology was used for si-multaneously quantitative detection of multi-ple analytes from a single patient sample.
The technology was based on the RandoxBiochip (Randox Laboratories), a (9 mm2) solidsubstrate containing an array of discrete test re-gions with immobilized antibodies specific fordifferent antigens. Multiple cytokine levelswere detected by this method.
After antibody activation with assay buffer,standards and samples were added and incu-bated at 37°C for 60 minutes. Then membraneswere placed in the thermoshaker at 370 rpm for60 minutes.
Conjugates, anti-Vegf antibodies, and horse-radish peroxidase (HRP) were added to mem-branes and samples were incubated in the ther-moshaker at 370 rpm for 60 minutes.
The chemiluminescence signal formed afterthe addition of luminol (1:1 ratio with HRP)was detected.
The light signal generated from each of thetest regions on the biochip was detected usingdigital imaging technology and compared withthat from a stored calibration curve; then con-centrations were calculated. The functionalsensitivity of the biochip was 13.3 pg/mL andthe intra-assay precision was 6.3%.
Statistical analysis
The Hardy-Weinberg equilibrium was veri-fied for the two control groups. Two-tailed Pear-son’s chi-square exact test was used to comparegenotype and allele frequencies. The level of sta-tistical significance was set at �5%. Odds ratio(OR) and confidence intervals (CI) for AD riskalso were calculated. A logistic regression model,
CHIAPPELLI ET AL.488
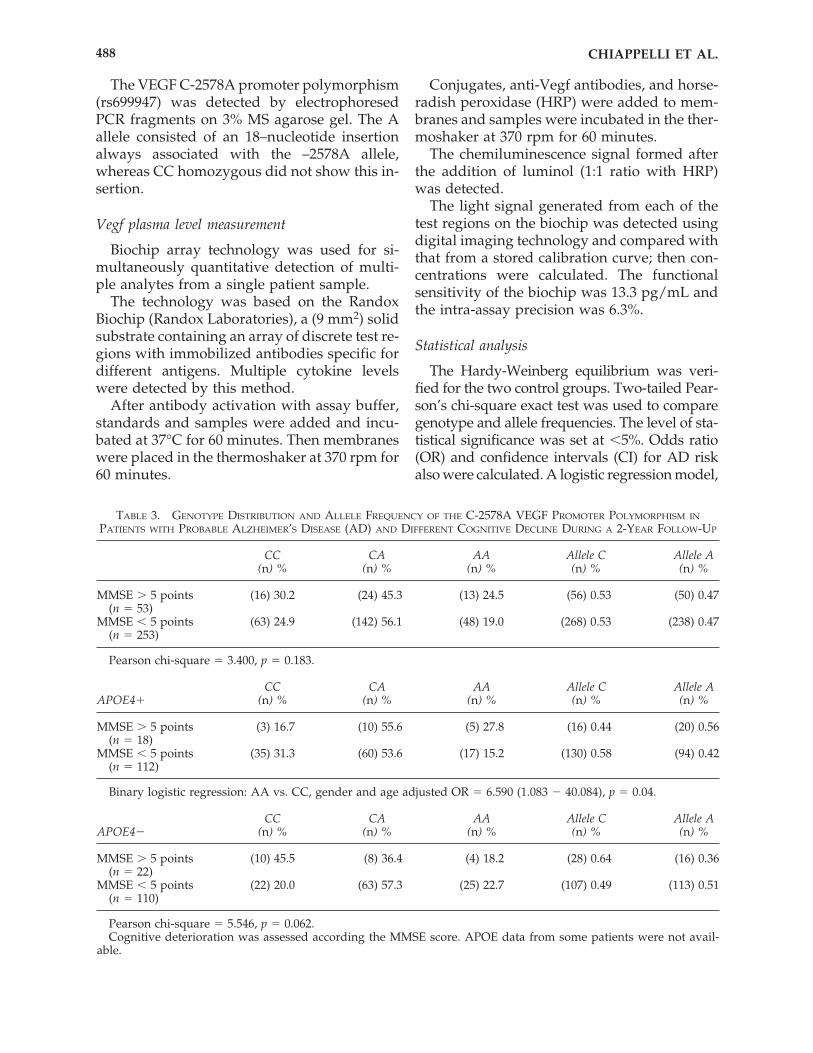
TABLE 3. GENOTYPE DISTRIBUTION AND ALLELE FREQUENCY OF THE C-2578A VEGF PROMOTER POLYMORPHISM IN
PATIENTS WITH PROBABLE ALZHEIMER’S DISEASE (AD) AND DIFFERENT COGNITIVE DECLINE DURING A 2-YEAR FOLLOW-UP
CC CA AA Allele C Allele A(n) % (n) % (n) % (n) % (n) %
MMSE � 5 points (16) 30.2 (24) 45.3 (13) 24.5 (56) 0.53 (50) 0.47(n � 53)
MMSE � 5 points (63) 24.9 (142) 56.1 (48) 19.0 (268) 0.53 (238) 0.47(n � 253)
Pearson chi-square � 3.400, p � 0.183.
CC CA AA Allele C Allele AAPOE4� (n) % (n) % (n) % (n) % (n) %
MMSE � 5 points (3) 16.7 (10) 55.6 (5) 27.8 (16) 0.44 (20) 0.56(n � 18)
MMSE � 5 points (35) 31.3 (60) 53.6 (17) 15.2 (130) 0.58 (94) 0.42(n � 112)
Binary logistic regression: AA vs. CC, gender and age adjusted OR � 6.590 (1.083 � 40.084), p � 0.04.
CC CA AA Allele C Allele AAPOE4� (n) % (n) % (n) % (n) % (n) %
MMSE � 5 points (10) 45.5 (8) 36.4 (4) 18.2 (28) 0.64 (16) 0.36(n � 22)
MMSE � 5 points (22) 20.0 (63) 57.3 (25) 22.7 (107) 0.49 (113) 0.51(n � 110)
Pearson chi-square � 5.546, p � 0.062.Cognitive deterioration was assessed according the MMSE score. APOE data from some patients were not avail-
able.
adjusted for age and gender, or APOE �4 allele,was used to evaluate the effect of C-2578A SNPand the interaction between polymorphisms onthe risk of AD, its clinical progression, the riskof MCI, and the risk of MCI progression to AD.A Kruskal-Wallis non-parametric test was usedto compare the Vegf plasma levels in the testedgroups.
RESULTS
As expected, the percentage of patients withAD carrying one APOE �4 allele was greaterthan that of controls (49.8% vs. 17.3%; adjustedOR � 4.4, CI � 3.3–6.9, p � 0.0001). No differ-ence between VEGF genotype distribution andallele frequency between the two populationsof patients with AD was observed (Table 1);therefore, data from patients were pooled.
As reported in Table 2, the distribution ofVEGF genotype was slightly different betweenpatients with AD and the control population(chi-square � 3.993, p � 0.046). The VEGF AA
genotype was associated with an increased riskof developing AD as assessed by binary logis-tic regression adjusted for APOE (OR � 1.616,CI � 1.008–2.591, p � 0.046).
Then patients with AD and controls were di-vided according to the presence or absence ofthe APOE �4 allele; only patients with AD neg-ative for the APOE �4 allele showed an in-creased frequency of the VEGF AA genotypeor A allele (p � 0.035). These results were con-firmed by logistic regression analysis showingthat OR for the disease was 2.269 for AD withthe VEGF AA genotype.
Patients with AD were followed up for 2years and cognitive performances were as-sessed by MMSE scores. Patients were furtherdivided in two groups: The first one showedan accelerated decline (MMSE � 5 points), andthe second one a slower cognitive deterioration(MMSE � 5 points). APOE �4 status also wastaken into consideration. As shown in Table 3,the AA VEGF genotype was associated with anaccelerated cognitive decline in APOE �4–pos-itive patients with AD. Patients with the VEGF
VEGF GENE IS ASSOCIATED WITH MCI AND AD 489
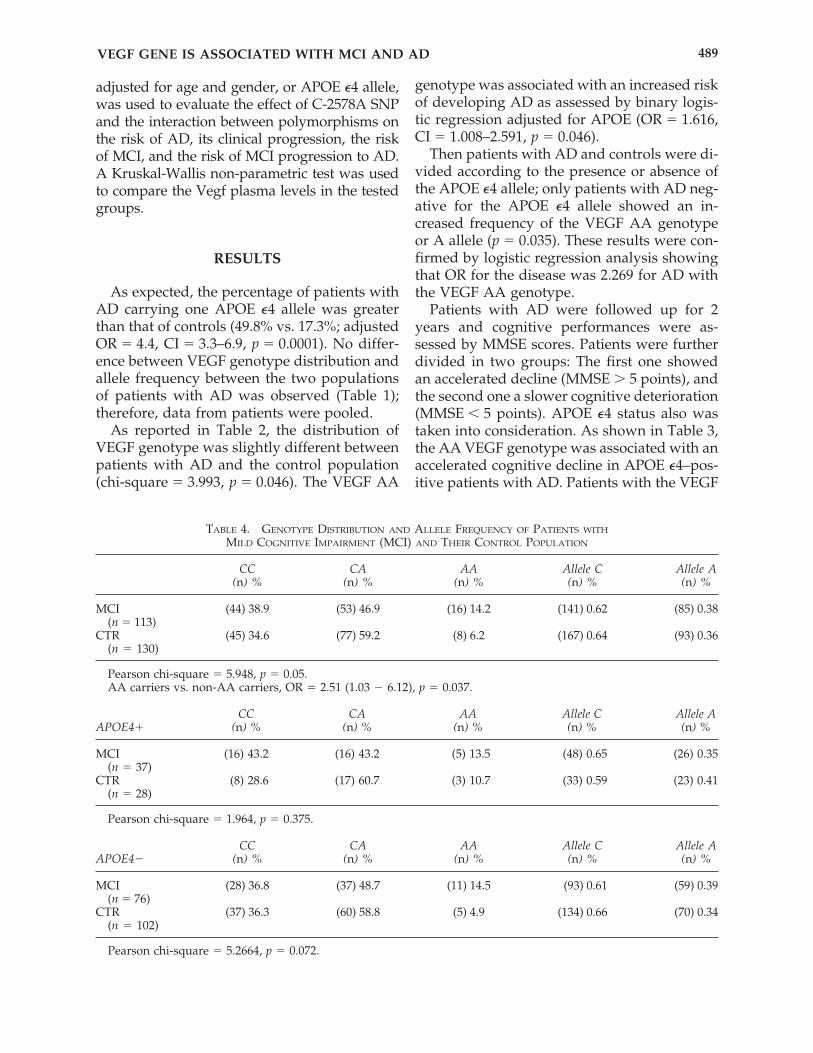
TABLE 4. GENOTYPE DISTRIBUTION AND ALLELE FREQUENCY OF PATIENTS WITH
MILD COGNITIVE IMPAIRMENT (MCI) AND THEIR CONTROL POPULATION
CC CA AA Allele C Allele A(n) % (n) % (n) % (n) % (n) %
MCI (44) 38.9 (53) 46.9 (16) 14.2 (141) 0.62 (85) 0.38(n � 113)
CTR (45) 34.6 (77) 59.2 (8) 6.20 (167) 0.64 (93) 0.36(n � 130)
Pearson chi-square � 5.948, p � 0.05.AA carriers vs. non-AA carriers, OR � 2.51 (1.03 � 6.12), p � 0.037.
CC CA AA Allele C Allele AAPOE4� (n) % (n) % (n) % (n) % (n) %
MCI (16) 43.2 (16) 43.2 (5) 13.5 (48) 0.65 (26) 0.35(n � 37)0
CTR (8) 28.6 (17) 60.7 (3) 10.7 (33) 0.59 (23) 0.41(n � 28)0
Pearson chi-square � 1.964, p � 0.375.
CC CA AA Allele C Allele AAPOE4� (n) % (n) % (n) % (n) % (n) %
MCI (28) 36.8 (37) 48.7 (11) 14.5 (93) 0.61 (59) 0.39(n � 76)
CTR (37) 36.3 (60) 58.8 (5) 4.90 (134) 0.66 (70) 0.34(n � 102)
Pearson chi-square � 5.2664, p � 0.072.
AA genotype showed a sixfold higher risk thanCC carriers of losing more than five points ofMMSE score per year during the 2-year follow-up, as assessed by logistic regression analysisadjusted for gender and age. The APOE �4 al-lele alone was not associated with differentialcognitive deterioration in AD during the 2-yearfollow-up period (data not shown).
The VEGF AA genotype was representedmore in the MCI group than controls (chi-square � 5.948, p � 0.05; OR � 2.5, C.I. �1.03–6.12, p � 0.037) (Table 4). MCI and con-trols were further divided according to APOE�4 status and the AA genotype was over-rep-resented only in MCI APOE �4-negative pa-tients (chi-square � 5.264, p � 0.072; Table 4).
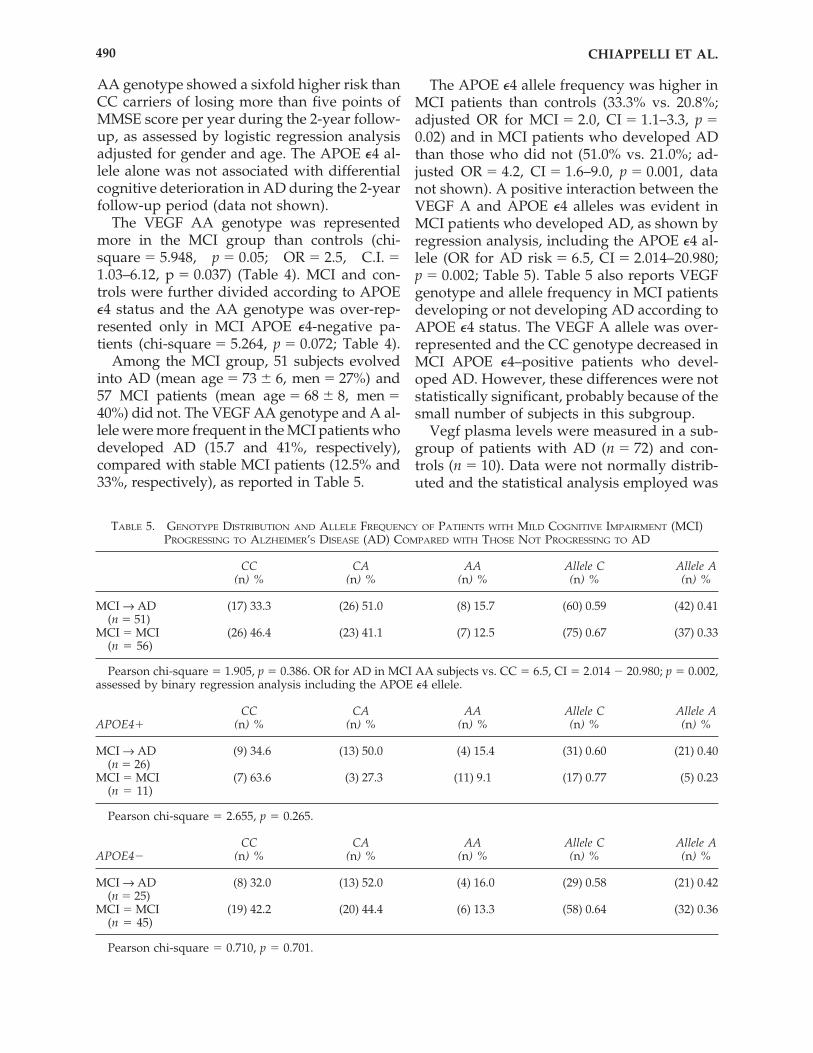
Among the MCI group, 51 subjects evolvedinto AD (mean age � 73 � 6, men � 27%) and57 MCI patients (mean age � 68 � 8, men �40%) did not. The VEGF AA genotype and A al-lele were more frequent in the MCI patients whodeveloped AD (15.7 and 41%, respectively),compared with stable MCI patients (12.5% and33%, respectively), as reported in Table 5.
The APOE �4 allele frequency was higher inMCI patients than controls (33.3% vs. 20.8%;adjusted OR for MCI � 2.0, CI � 1.1–3.3, p �0.02) and in MCI patients who developed ADthan those who did not (51.0% vs. 21.0%; ad-justed OR � 4.2, CI � 1.6–9.0, p � 0.001, datanot shown). A positive interaction between theVEGF A and APOE �4 alleles was evident inMCI patients who developed AD, as shown byregression analysis, including the APOE �4 al-lele (OR for AD risk � 6.5, CI � 2.014–20.980;p � 0.002; Table 5). Table 5 also reports VEGFgenotype and allele frequency in MCI patientsdeveloping or not developing AD according toAPOE �4 status. The VEGF A allele was over-represented and the CC genotype decreased inMCI APOE �4–positive patients who devel-oped AD. However, these differences were notstatistically significant, probably because of thesmall number of subjects in this subgroup.
Vegf plasma levels were measured in a sub-group of patients with AD (n � 72) and con-trols (n � 10). Data were not normally distrib-uted and the statistical analysis employed was
CHIAPPELLI ET AL.490
TABLE 5. GENOTYPE DISTRIBUTION AND ALLELE FREQUENCY OF PATIENTS WITH MILD COGNITIVE IMPAIRMENT (MCI)PROGRESSING TO ALZHEIMER’S DISEASE (AD) COMPARED WITH THOSE NOT PROGRESSING TO AD
CC CA AA Allele C Allele A(n) % (n) % (n) % (n) % (n) %
MCI → AD (17) 33.3 (26) 51.0 (8) 15.7 (60) 0.59 (42) 0.41(n � 51)
MCI � MCI (26) 46.4 (23) 41.1 (7) 12.5 (75) 0.67 (37) 0.33(n � 56)
Pearson chi-square � 1.905, p � 0.386. OR for AD in MCI AA subjects vs. CC � 6.5, CI � 2.014 � 20.980; p � 0.002,assessed by binary regression analysis including the APOE �4 ellele.
CC CA AA Allele C Allele AAPOE4� (n) % (n) % (n) % (n) % (n) %
MCI → AD (9) 34.6 (13) 50.0 (4) 15.4 (31) 0.60 (21) 0.40(n � 26)
MCI � MCI (7) 63.6 (3) 27.3 (11) 9.1 (17) 0.77 (5) 0.23(n � 11)
Pearson chi-square � 2.655, p � 0.265.
CC CA AA Allele C Allele AAPOE4� (n) % (n) % (n) % (n) % (n) %
MCI → AD (8) 32.0 (13) 52.0 (4) 16.0 (29) 0.58 (21) 0.42(n � 25)
MCI � MCI (19) 42.2 (20) 44.4 (6) 13.3 (58) 0.64 (32) 0.36(n � 45)
Pearson chi-square � 0.710, p � 0.701.
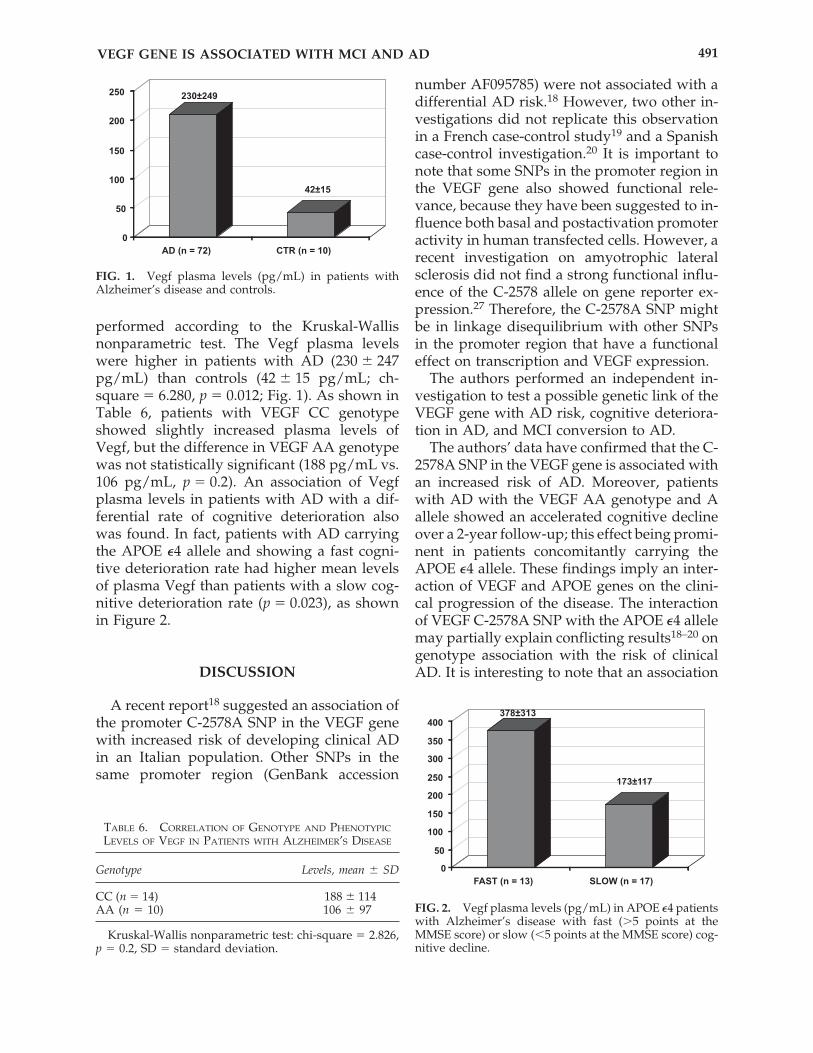
performed according to the Kruskal-Wallisnonparametric test. The Vegf plasma levelswere higher in patients with AD (230 � 247pg/mL) than controls (42 � 15 pg/mL; ch-square � 6.280, p � 0.012; Fig. 1). As shown inTable 6, patients with VEGF CC genotypeshowed slightly increased plasma levels ofVegf, but the difference in VEGF AA genotypewas not statistically significant (188 pg/mL vs.106 pg/mL, p � 0.2). An association of Vegfplasma levels in patients with AD with a dif-ferential rate of cognitive deterioration alsowas found. In fact, patients with AD carryingthe APOE �4 allele and showing a fast cogni-tive deterioration rate had higher mean levelsof plasma Vegf than patients with a slow cog-nitive deterioration rate (p � 0.023), as shownin Figure 2.
DISCUSSION
A recent report18 suggested an association ofthe promoter C-2578A SNP in the VEGF genewith increased risk of developing clinical ADin an Italian population. Other SNPs in thesame promoter region (GenBank accession
number AF095785) were not associated with adifferential AD risk.18 However, two other in-vestigations did not replicate this observationin a French case-control study19 and a Spanishcase-control investigation.20 It is important tonote that some SNPs in the promoter region inthe VEGF gene also showed functional rele-vance, because they have been suggested to in-fluence both basal and postactivation promoteractivity in human transfected cells. However, arecent investigation on amyotrophic lateralsclerosis did not find a strong functional influ-ence of the C-2578 allele on gene reporter ex-pression.27 Therefore, the C-2578A SNP mightbe in linkage disequilibrium with other SNPsin the promoter region that have a functionaleffect on transcription and VEGF expression.
The authors performed an independent in-vestigation to test a possible genetic link of theVEGF gene with AD risk, cognitive deteriora-tion in AD, and MCI conversion to AD.
The authors’ data have confirmed that the C-2578A SNP in the VEGF gene is associated withan increased risk of AD. Moreover, patientswith AD with the VEGF AA genotype and Aallele showed an accelerated cognitive declineover a 2-year follow-up; this effect being promi-nent in patients concomitantly carrying theAPOE �4 allele. These findings imply an inter-action of VEGF and APOE genes on the clini-cal progression of the disease. The interactionof VEGF C-2578A SNP with the APOE �4 allelemay partially explain conflicting results18–20 ongenotype association with the risk of clinicalAD. It is interesting to note that an association
VEGF GENE IS ASSOCIATED WITH MCI AND AD 491
FIG. 1. Vegf plasma levels (pg/mL) in patients withAlzheimer’s disease and controls.
TABLE 6. CORRELATION OF GENOTYPE AND PHENOTYPIC
LEVELS OF VEGF IN PATIENTS WITH ALZHEIMER’S DISEASE
Genotype Levels, mean � SD
CC (n � 14) 188 � 114AA (n � 10) 106 � 970
Kruskal-Wallis nonparametric test: chi-square � 2.826,p � 0.2, SD � standard deviation.
FIG. 2. Vegf plasma levels (pg/mL) in APOE �4 patientswith Alzheimer’s disease with fast (�5 points at theMMSE score) or slow (�5 points at the MMSE score) cog-nitive decline.

between APOE �4 allele and calcific valvularheart diseases has been reported.28 Recently, aninvestigation that aimed to verify a possible as-sociation between postmortem AD neuro-pathology and autopsy-verified cardiovasculardisease showed that coronary heart diseasewas indeed associated with AD brain neu-ropathologic lesions in patients with the APOE�4 allele.7 The present findings implicate thatin patients with AD with the APOE �4 allelevascular factors further contributed to cogni-tive deterioration during the clinical history ofthe disease.
It is of interest that the AA genotype also wasoverrepresented among patients with MCIcompared with a control population. Finally,the frequency of the AA genotype and A allelewas higher in APOE �4–positive MCI patientswho developed AD than in those who did not.These data strongly support an interaction ofthese two genes in the deterioration rate of cog-nitive performances in both preclinical andclinical AD. Further investigations will clarifythe biologic significance of these two genes as-sociated with AD.
The present findings support the notionthat factors with regulatory function on brainvessels and neuronal survival, such as VEGF,are linked to the pathogenesis of age-relatedcognitive decline, and the clinical manifesta-tion of AD and its clinical progression. VEGFhas been implicated in neoangiogenesis, neu-rogenesis, and glial activation in the adultbrain.29 The functional significance of VEGF-induced adult neurogenesis is not fully un-derstood. However, the authors’ findingssuggest that VEGF is closely linked to patho-genetic mechanisms leading to cognitive im-pairment and AD. It is important to note thatVegf coaccumulated with �-amyloid depositsin AD brains,30 and this sequestration mayimpair Vegf availability in the central nervoussystem (CNS) and contribute to vascular dys-function and neurodegeneration. It is also im-portant to stress that Vegf influences glucoseuptake in the brain by modulating GLUT1 ex-pression,31 and glucose uptake is an early al-teration of brain areas developing the neu-rodegeneration in MCI and patients with AD.Increased levels of peripheral Vegf in AD andthe increasing levels of this factor with the
cognitive deterioration and clinical progres-sion of AD might reflect the progressive Vegfdeficiency in the AD brain that is insuffi-ciently compensated by a peripheral releaseof this compound. Therefore, the authors hy-pothesized that a Vegf-mediated uncouplingof neoangiogenesis, neurogenesis, and glialactivation is an early event in the brain dys-function leading to cognitive impairment.These data have important therapeutic impli-cations and suggest that several drugs withpositive regulatory effect on brain circulation,neurogenesis (neurotrophins), and glial acti-vation (antiinflammatory) might be used todelay the manifestation of age-related cogni-tive impairment and dementia.
ACKNOWLEDGMENTS
This research was supported by the ItalianMinistry for Technology Research (ex COFIN)and the Italian CURA. The authors thank Dr.E. Tumini for statistical assistance.
REFERENCES
1. Katzman RN. Medical progress: Alzheimer’s disease.N Engl J Med 1986;274:964–973.
2. Selkoe DJ. Alzheimer’s disease: genes, protein andtherapy. Physiol Rev 2001;81:741–766.
3. Nestor PJ, Scheltens P, Hodges JR. Advances in theearly detection of Alzheimer’s disease. Nat Med 2004;10:34–41.
4. Ritchie K, Altero S, Touchon J. Classification criteriafor mild cognitive impairment. A population-basedvalidation study. Neurology 2001;56:37–42.
5. Breteler MMB, Claus JJ, van Duijn CM, Launer LJ,Hofman A. Epidemiology of Alzheimer’s disease.Epidemiol Rev 1992;14:59–82.
6. Hayden KM, Zandi PP, Lyketsos CG, KhachaturianAS, Bastian LA, Charoonruk G, Tschanz JT, NortonMC, Pieper CF, Munger RG, Breitner JC, Welsh-Bohmer KA, Cache County Investigators. Vascularrisk factors for incident Alzheimer disease and vas-cular dementia: the Cache County study. AlzheimerDis Assoc Disord 2006;20:93–100.
7. Beeri MS, Rapp M, Silverman JM, Schmeidler J, Gross-man HT, Fallon JT, Purohit DP, Perl DP, Siddiqui A,Lesser G, Rosendorff C, Haroutunian V. Coronaryartery disease is associated with Alzheimer diseaseneuropathology in APOE4 carriers. Neurology 2006;66:1399–1404.
8. DeCarli C, Mungas D, Harvey D, Reed B, Weiner M,Chui H, Jagust W. Memory impairment, but not cere-
CHIAPPELLI ET AL.492

brovascular disease, predicts progression of MCI todementia. Neurology 2004;63:220–227.
9. Vagnucci AHJr, Li WW. Alzheimer’s disease and an-giogenesis. Lancet 2003;361:605–608.
10. Zlokovic BV. Neurovascular mechanisms of Alzhei-mer’s neurodegeneration. Trends Neurosci 2005;28:202–208.
11. de la Torre JC. Is Alzheimer’s disease a neurodegen-erative or a vascular disorder? Data, dogma, and di-alectics. Lancet Neurol 2004;3:184–190.
12. Zlokovic BV. Clearing Amyloid through the blood-brain barrier. J Neurochem 2004;89:807–811.
13. Carmeliet P, Jain RK. Angiogenesis in cancer andother diseases. Nature 2000;407:249–257.
14. Pogue AI, Lukiw WJ. Angiogenic signaling in Alz-heimer’s disease. Neuroreport 2004;15:1507–1510.
15. Sun Y, Jin K, Xie L, Childs J, Mao XO, Logvinova A,Greenberg DA. VEGF-induced neuroprotection, neu-rogenesis, and angiogenesis after focal cerebral isch-emia. J Clin Invest 2003;111:1843–1851.
16. Kalaria RN, Cohen DL, Premkumar DR, Nag S,LaManna JC, Lust WD. Vascular endothelial growthfactor in Alzheimer’s disease and experimental cere-bral ischemia. Brain Res Mol Brain Res 1998;62:101–105.
17. Brogan JI, Khan N, Isaac K, Hutchinson JA, PravicaV, Hutchinson IV. Novel polymorphisms in the pro-moter and 5� UTR regions of the Human Vascular En-dothelial Growth Factor gene. Hum Immunol 1999;60:1245–1249.
18. Del Bo R, Scarlato M, Ghezzi S, Martinelli BoneschiF, Fenoglio C, Galbiati S, Virgilio R, Galimberti D, Gal-imberti G, Crimi M, Ferrarese C, Scarpini E, BresolinN, Comi GP. Vascular endothelial growth factor genevariability is associated with increased risk for AD.Ann Neurol 2005;57:373–380.
19. Chapuis J, Tian J, Shi J, Bensemain F, Cottel D, LendonC, Amouyel P, Mann D, Lambert JC. Associationstudy of the vascular endothelial growth factor genewith the risk of developing Alzheimer’s disease. Neu-robiol Aging 2006;27:1212–1215.
20. Mateo I, Llorca J, Infante J, Rodriguez-Rodriguez E,Sanchez-Quintana C, Sanchez-Juan P, Berciano J,Combarros O. Case-control study of vascular endo-thelial growth factor (VEGF) genetic variability inAlzheimer’s disease. Neurosci Lett 2006;401:171–173.
21. McKhann G, Drachman D, Folstein M, Katzman R,Price D, Stadlan EM. Clinical diagnosis of Alzheimer’sdisease: report of the NINCDS-ADRDA Work Groupunder the auspices of Department of Health and Hu-man Service Task Force on Alzheimer’s Disease. Neu-rology 1984;34:939–944.
22. American Psychiatric Association: Diagnostic andStatistical Manual of Mental Disorders: DSM-III-R, 3drev ed. Washington, DC: American Psychiatric Asso-ciation 1987.
23. Doody RS, Massman P, Dunn K. A method for esti-mating progression rate in Alzheimer’s disease. ArchNeurol 2001;58:449–454.
24. Petersen RC, Doody R, Kurz A, Mohs RC, Morris JC,Rabins PV, Ritchie K, Rossor M, Thal L, Winblad B.Current concepts in mild cognitive impairment. ArchNeurol 2001;58:1985–1992.
25. Grimaldi LM, Casadei VM, Ferri C, Veglia F, LicastroF, Annoni G, Biunno I, De Bellis G, Sorbi S, MarianiC, Canal N, Griffin WS, Franceschi M. Association ofearly-onset Alzheimer’s disease with an interleukin-1 alpha gene polymorphism. Ann Neurol 2000;47:361–365.
26. Licastro F, Pedrini S, Govoni M, Pession A, Ferri C,Annoni G, Casadei V, Veglia F, Bertolini S, GrimaldiLM. Apolipoprotein E and �-1-antichymotrypsin allele polymorphism in sporadic and familial Alzhei-mer’s disease. Neurosci Letters 1999;270:129–132.
27. Storkebaum E, Lambrechts D, Dewerchin M, Moreno-Murciano MP, Appelmans S, Oh H, Wyns S, Thijs V,Andersson J, van Marion I, Al-Chalabi A, Bornes S,Musson R, Hansen V, Beckman L, Adolfsson R, PallHS, Prats H, Vermeire S, Rutgeerts P, Katayama S,Awata T, Leigh N, Lang-Lazdunski L, Dewerchin M,Shaw C, Moons L, Vlietinck R, Morrison KE, Rob-berecht W, Van Broeckhoven C, Collen D, AndersenPM, Carmeliet P. VEGF is a modifier of amyotrophiclateral sclerosis in mice and humans and protects mo-toneurons against ischemic death. Nat Genet 2003;34:383–394.
28. Novaro GM, Sachar R, Pearce GL, Sprecher DL, Grif-fin BP. Association between apolipoprotein E allelesand calcific valvular heart disease. Circulation 2003;108:1804–1808.
29. Greenberg DA, Jin K. From angiogenesis to neu-ropathology. Nature 2005;438:954–959.
30. Yang SP, Bae DG, Kang HJ, Gwag BJ, Gho YS, ChaeCB. Co-accumulation of vascular endothelial growthfactor with beta-amyloid in the brain of patients withAlzheimer’s disease. Neurobiol Aging 2004;25:283–290.
31. Mani N, Khaibullina A, Krum JM, Rosenstein JM. Ac-tivation of receptor-mediated angiogenesis and sig-naling pathways after VEGF administration in fetalrat CNS explants. J Cereb Blood Flow Metab 2003;23:1420–1429.
Address reprint requests to:Federico Licastro, M.D.
Department of Experimental PathologySchool of Medicine
University of BolognaVia S. Giacomo 14
40126 Bologna, Italy
E-mail: [email protected]
Received: July 10, 2006Accepted: August 12, 2006
VEGF GENE IS ASSOCIATED WITH MCI AND AD 493