vascular assessment and intervention in the wound care setting
TRANSCRIPT

Vascular Assessment and Intervention
in the Wound Care Setting
Roger Walcott MD, FACS, RPVI Associate Director, Vascular Surgery Services, Catholic Health
Partner, Vascular and Endovascular Center of WNY
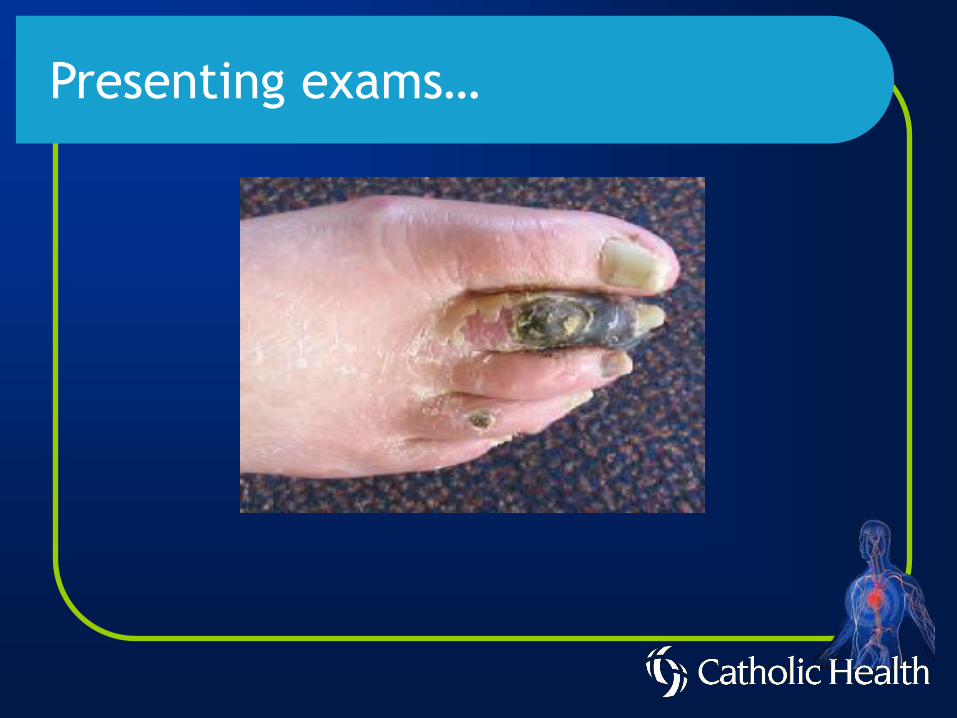
Presenting exams…
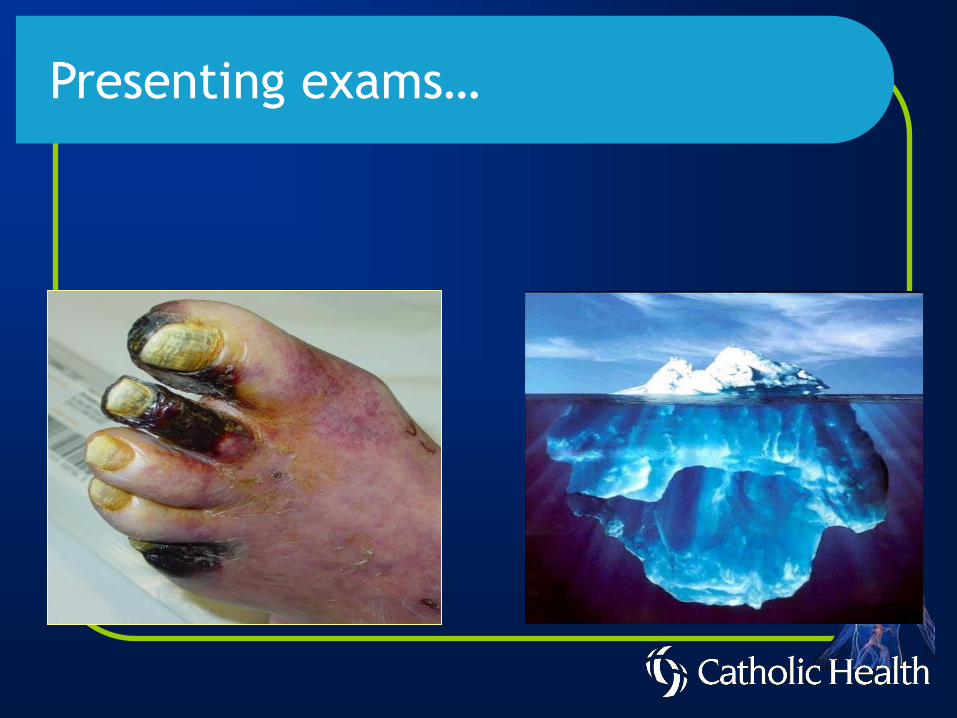
Presenting exams…

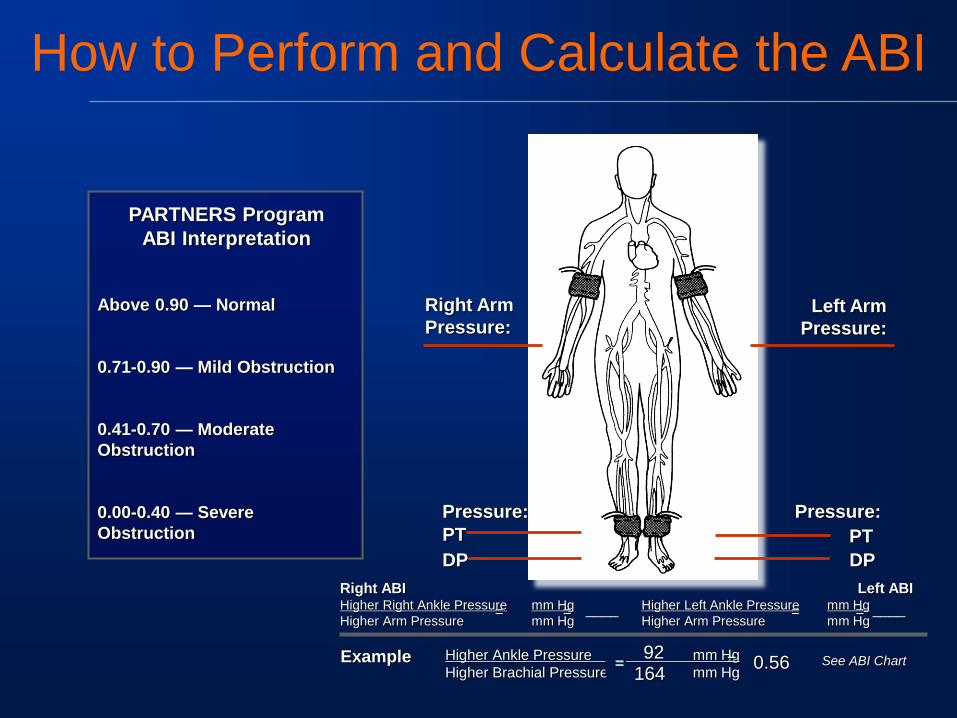
How to Perform and Calculate the ABI
Above 0.90 — Normal
0.71-0.90 — Mild Obstruction
0.41-0.70 — Moderate
Obstruction
0.00-0.40 — Severe
Obstruction
PARTNERS Program
ABI Interpretation
Right ABI Higher Right Ankle Pressure mm Hg
Higher Arm Pressure mm Hg = =
Left ABI Higher Left Ankle Pressure mm Hg
Higher Arm Pressure mm Hg = = ____
Example Higher Ankle Pressure mm Hg
Higher Brachial Pressure mm Hg =
92 164
0.56 = See ABI Chart
Right Arm
Pressure: Left Arm
Pressure:
Pressure:
PT
DP
Pressure:
PT
DP
____
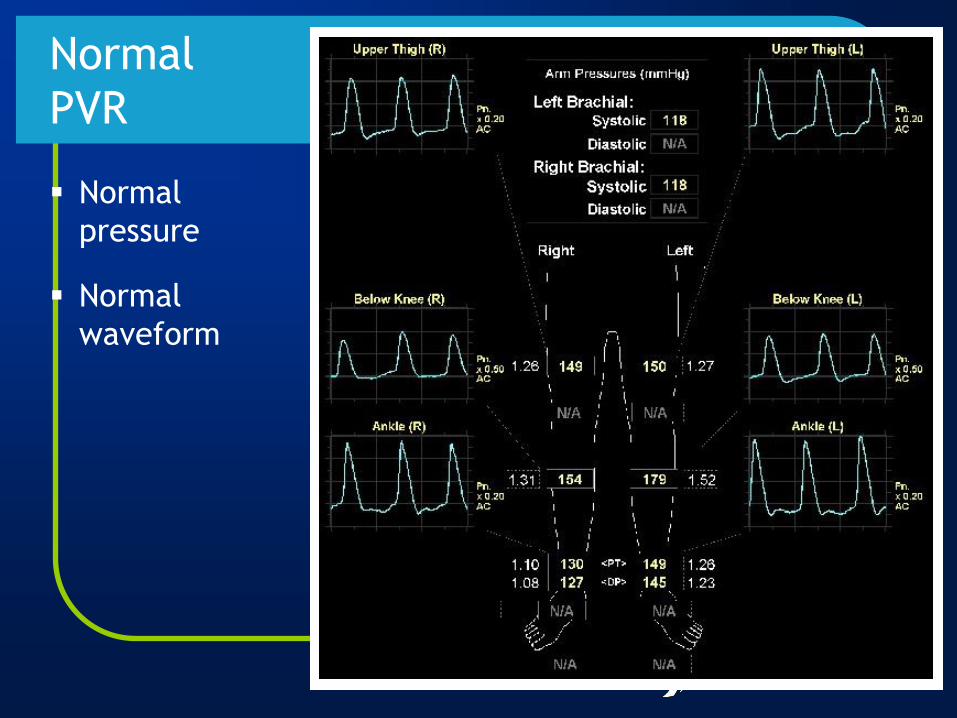
Normal
pressure
Normal
waveform
Normal
PVR
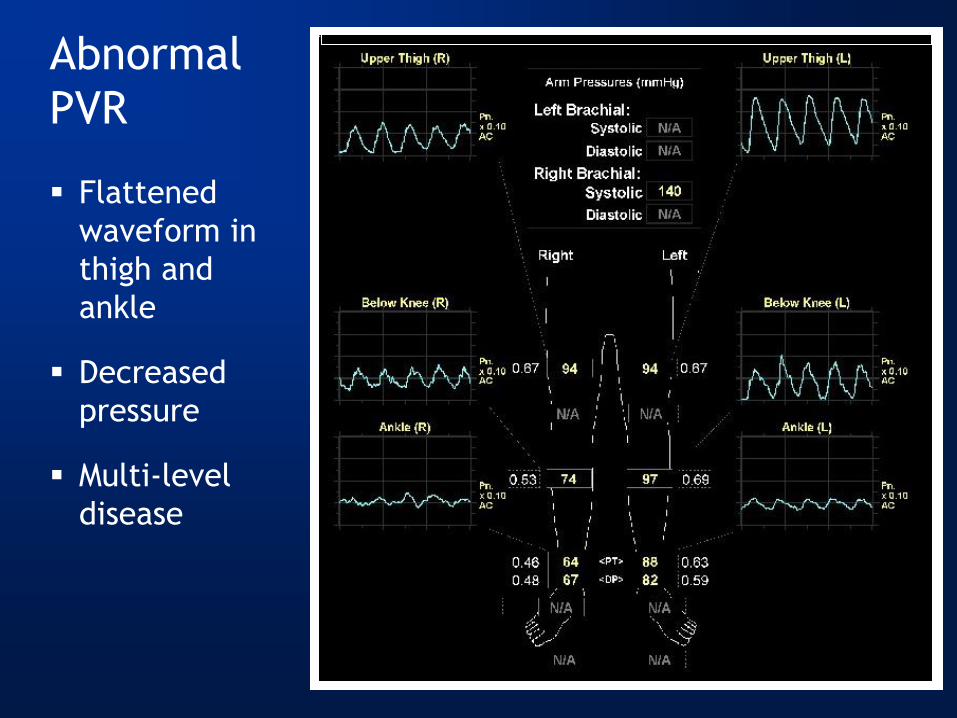
Flattened
waveform in
thigh and
ankle
Decreased
pressure
Multi-level
disease
Abnormal
PVR

Comparison
of the
extremities
Abnormal
PVR Left/
Normal
PVR Right
Duplex vs. Physiologic testing
Graft surveillance post distal bypass procedures.
Segmental pressures vs. Peak Systolic Velocities
PVR’s vs. spectral Doppler evaluation
ABI’s must be documented with duplex imaging
To be accurate, duplex imaging is time intensive

Lower Extremity Anatomy

SFA Occlusion / Duplex

DUPLEX / SFA STENT
Left: Normal velocities with flow reversal
consistent with distal stenosis. Right: Elevated
velocities consistent with in stent stenosis
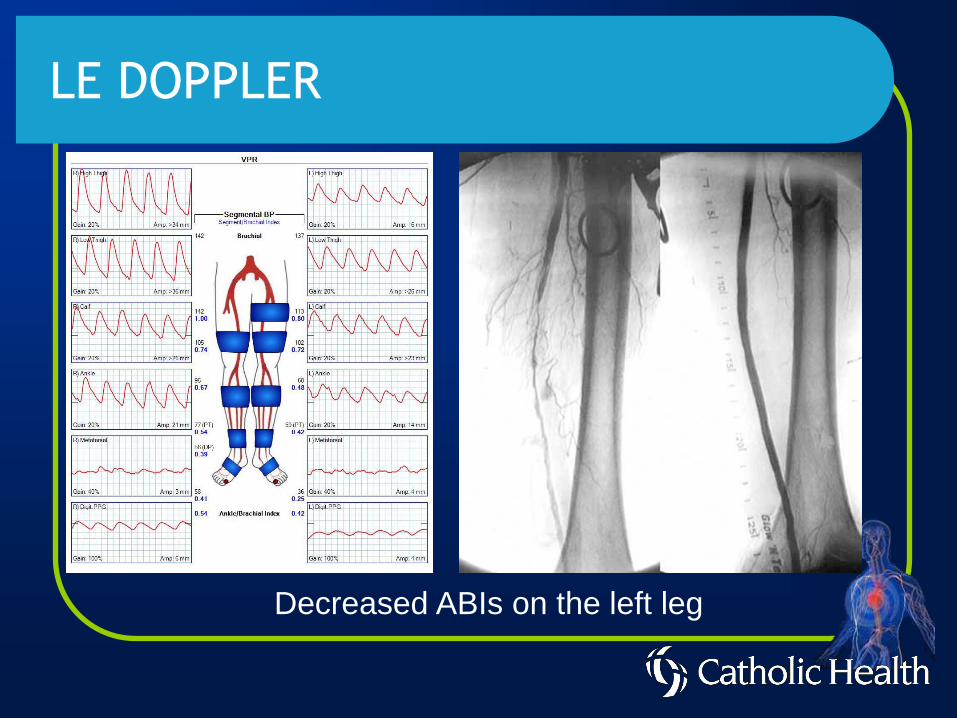
LE DOPPLER
Decreased ABIs on the left leg

LE DOPPLER
Normal post intervention ABIs on the left

Gangrene of the forefoot
83 yo female
Smoker
Presented for wound
care
Vascular evaluation
performed in
multidisciplinary clinic

Severe Tibial Disease

PTA Tibial Vessels

Runoff into foot

Extensive Debridement


Deep Vein Thrombosis
Duplex is the primary noninvasive diagnostic
method for DVT
The sensitivity/specificity of venous
ultrasound for the diagnosis of DVT is 97%.

Post Thrombotic Syndrome
29-79% of all patients with DVT Will develop post
thrombotic syndrome
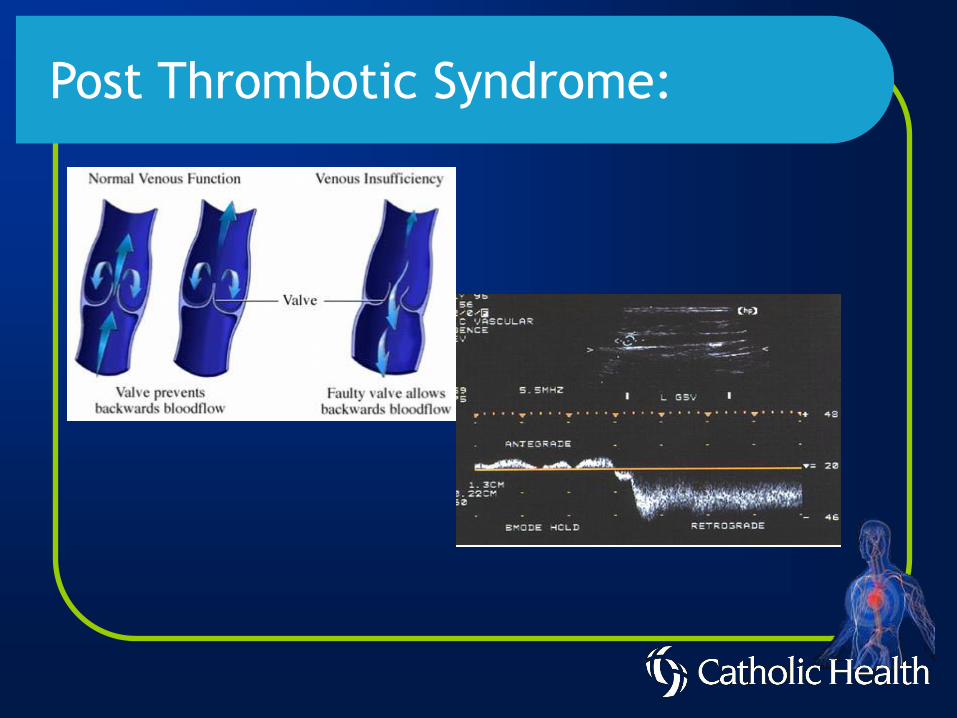
Post Thrombotic Syndrome:

Venous Reflux Disease
Perforators
• Communicating veins between the deep and superficial
venous system
• Incompetent perforating veins are usually present with
ulcers.

Incompetent Perforator

Incompetent Perforator with scarring

Venous Doppler or Arterial Doppler
Many patients have risk factors for both PAD and Venous
disease.
If DVT is questionable, venous duplex must always be
performed first
When in doubt, order both
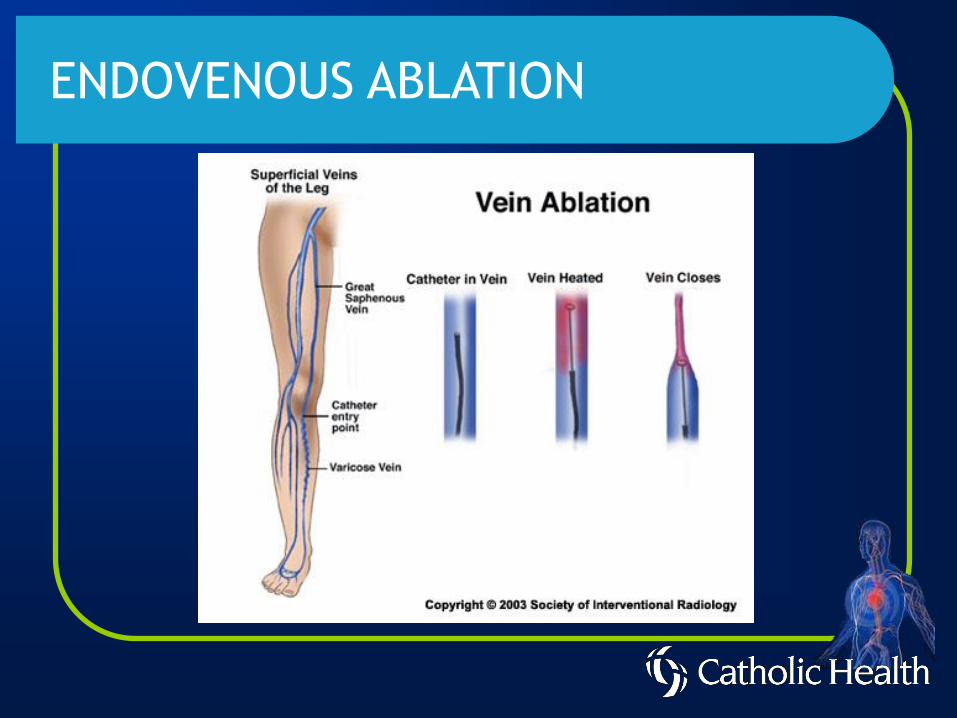
ENDOVENOUS ABLATION
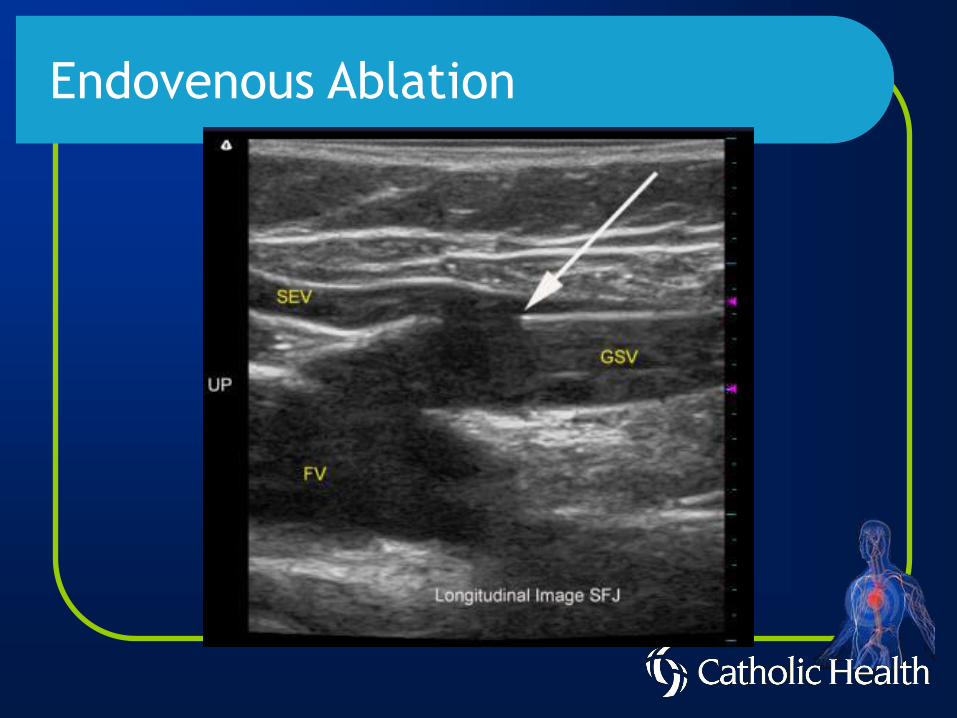
Endovenous Ablation

Endovenous Ablation

Efficacy of Compression Therapy
1. 22 trials comparing healing of venous ulcers using compression stockings
• Compressive therapy more effective than non-compression
• Higher pressure were more effective than lower
• Multilayer compression was better than single layer bandaging
2. 466 patients with a healed ulcer
• Continued use of compression stocking reduced reoccurrence within 3-5 year
3. 500 limb trial that compares surgery and compression vs. compression alone for ulcer treatment
• Combination therapy had lower rates of reoccurrence of ulcer at year 4 (24% vs. 52%)

EARLY DETECTION AND DIAGNOSIS IN
CONCERT WITH MEDICAL MANAGEMENT AND
VASCULAR INTERVENTION WILL PROVIDE
PATIENTS WITH THE HIGHEST QUALITY CARE.
ADDRESS VENOUS INSUFFICIENCY WITH
COMPRESSION AND ABLATION WHERE
INDICATED
IDENTIFY AND TREAT MIXED ARTERIAL AND
VENOUS DISEAS
In Conclusion
• Understanding PAD pathology
• Understanding who benefits from medical, interventional vs surgical bypass
• Treating venous insufficiency with ablation therapy
• Treating mixed arterial and venous disease
Conclusions