vaginal repair of apical prolapse mesh kit vs. vaginal suture repair marie fidela r. paraiso, m.d....
TRANSCRIPT
Vaginal Repair of Apical Prolapse Vaginal Repair of Apical Prolapse
Mesh Kit vs. Vaginal Suture RepairMesh Kit vs. Vaginal Suture Repair
Marie Fidela R. Paraiso, M.D.Marie Fidela R. Paraiso, M.D.
Head, Division of UrogynecologyHead, Division of Urogynecology
Professor of SurgeryProfessor of Surgery
Cleveland Clinic Lerner College of Medicine at Cleveland Clinic Lerner College of Medicine at
Case Western Reserve UniversityCase Western Reserve University
Cleveland, OHCleveland, OH
DisclosuresDisclosures
NoneNone
Food for ThoughtFood for Thought
Best practices are difficult to define when Best practices are difficult to define when discussing innovation because of lack of discussing innovation because of lack of data to support newer kit procedures.data to support newer kit procedures.
However, quality data are lacking with However, quality data are lacking with respect to traditional suture repair respect to traditional suture repair procedures as well.procedures as well.
Comparative data show that synthetic mesh Comparative data show that synthetic mesh implantation in the anterior wall results in implantation in the anterior wall results in better anatomic cure rates.better anatomic cure rates.
ICUD Modification of Oxford SystemICUD Modification of Oxford System
Levels of Evidence Levels of Evidence
1.1. RCTsRCTs
2.2. Prospective cohortProspective cohort
3.3. Retrospective case controlRetrospective case control
4.4. Case seriesCase series
5.5. Expert opinion without evidenceExpert opinion without evidence
**Pelvic Organ ProlapsePelvic Organ Prolapse
Approximately half of women 50 and older Approximately half of women 50 and older are affected. are affected.
Women feel their pelvic organs bulging or Women feel their pelvic organs bulging or protruding out of the vaginal opening and protruding out of the vaginal opening and may experience pelvic pain.may experience pelvic pain.
Urination and/or bowel movements may Urination and/or bowel movements may be difficult.be difficult.
Women may also experience pain with Women may also experience pain with intercourse and decreased body image.intercourse and decreased body image.
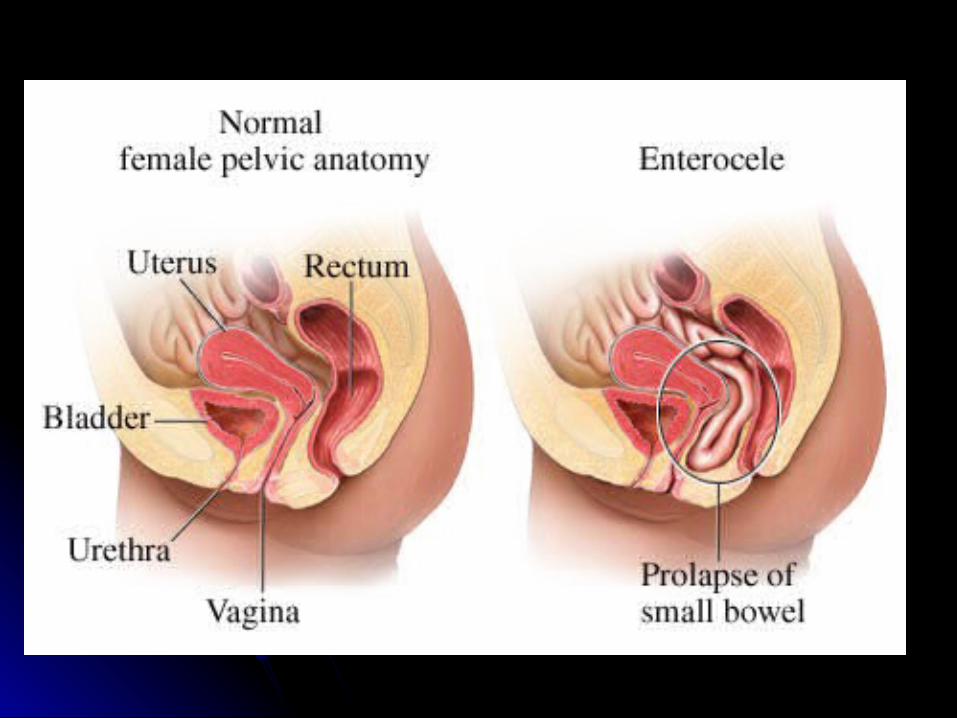
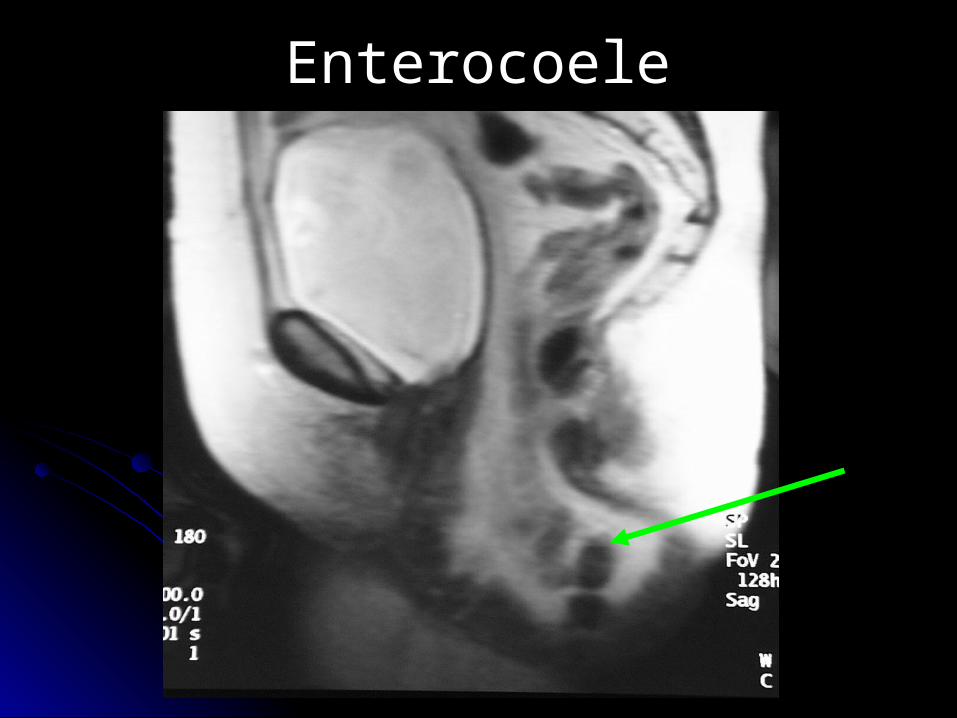
EnterocoeleEnterocoele

Repairs Requiring Graft Repairs Requiring Graft Augmentation or “Kits” for Augmentation or “Kits” for
Pelvic Organ ProlapsePelvic Organ Prolapse

Current Vaginal Mesh Kits with TrocarsCurrent Vaginal Mesh Kits with Trocars
Prolift® System Avaulta® System
Perigee® Sling /Apogee® Sling
Apogee and Perigee are registered trademarks of AMS Research Corporation. | Avaulta is a registered trademark of C.R. Bard, Inc. | Gynecare Prolift is a registered trademark of Johnson & Johnson Corporation
Potential LimitationsPotential Limitations• Blind pass of needles Blind pass of needles
through unfamiliar anatomythrough unfamiliar anatomy• Proximity to neurovascular Proximity to neurovascular
structuresstructures
• Vaginal apex support• Extent of anterior vaginal
wall support unless modified
• Gap failure
Many surgeons have switched to trocarless kits without any data!
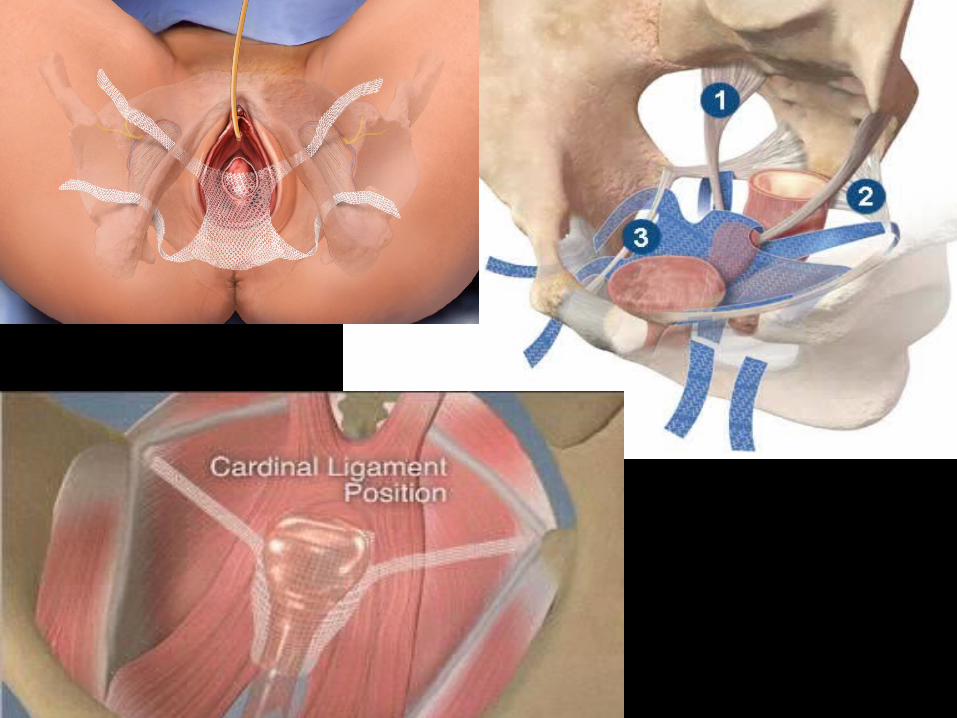
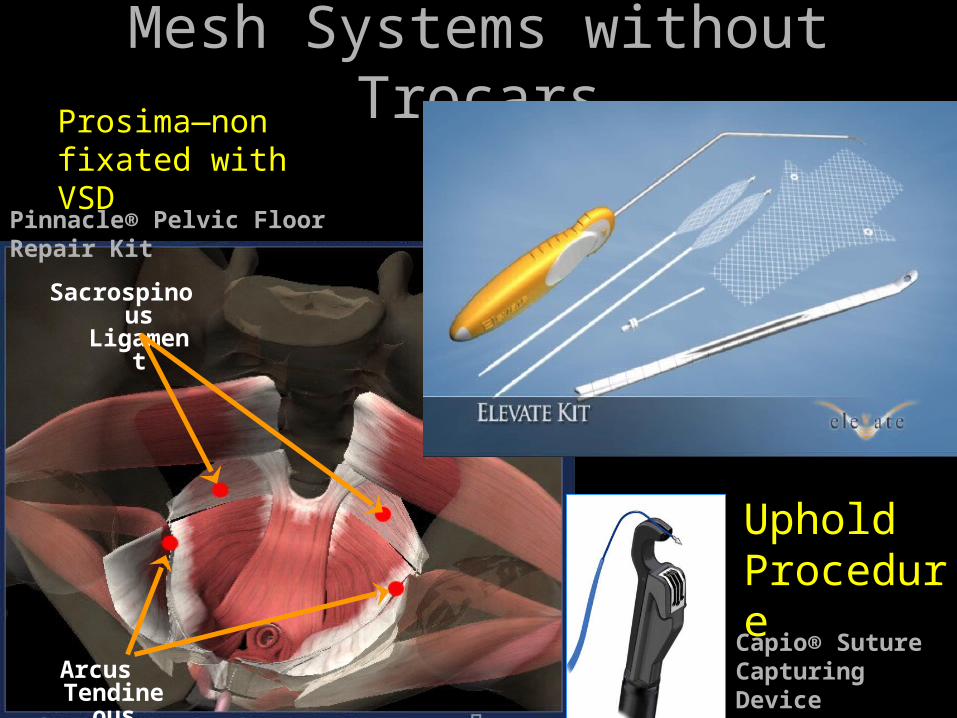
Mesh Systems without TrocarsMesh Systems without Trocars
Sacrospinous Ligament
Arcus Tendineous
Pinnacle® Pelvic Floor Repair Kit
Capio® Suture Capturing Device
Uphold Procedure
Prosima—non fixated with VSD
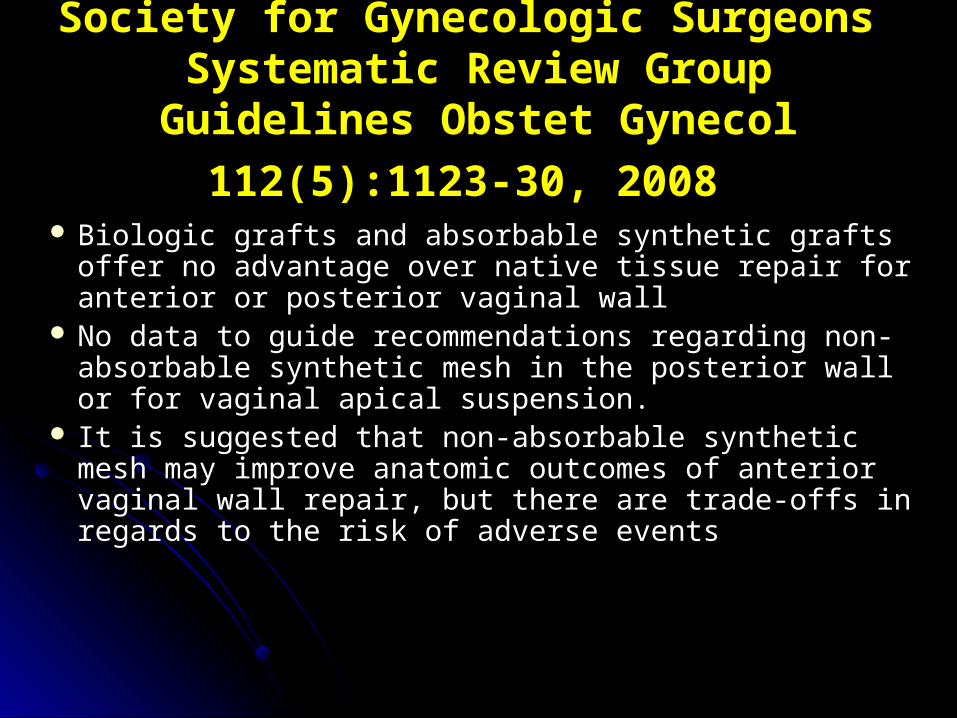
Society for Gynecologic Surgeons Society for Gynecologic Surgeons Systematic Review Group Guidelines Systematic Review Group Guidelines
Obstet Gynecol 112(5):1123-30, 2008Obstet Gynecol 112(5):1123-30, 2008 Biologic grafts and absorbable synthetic grafts offer Biologic grafts and absorbable synthetic grafts offer
no advantage over native tissue repair for anterior no advantage over native tissue repair for anterior or posterior vaginal wallor posterior vaginal wall
No data to guide recommendations regarding non-No data to guide recommendations regarding non-absorbable synthetic mesh in the posterior wall or absorbable synthetic mesh in the posterior wall or for vaginal apical suspension.for vaginal apical suspension.
It is suggested that non-absorbable synthetic mesh It is suggested that non-absorbable synthetic mesh may improve anatomic outcomes of anterior vaginal may improve anatomic outcomes of anterior vaginal wall repair, but there are trade-offs in regards to the wall repair, but there are trade-offs in regards to the risk of adverse eventsrisk of adverse events
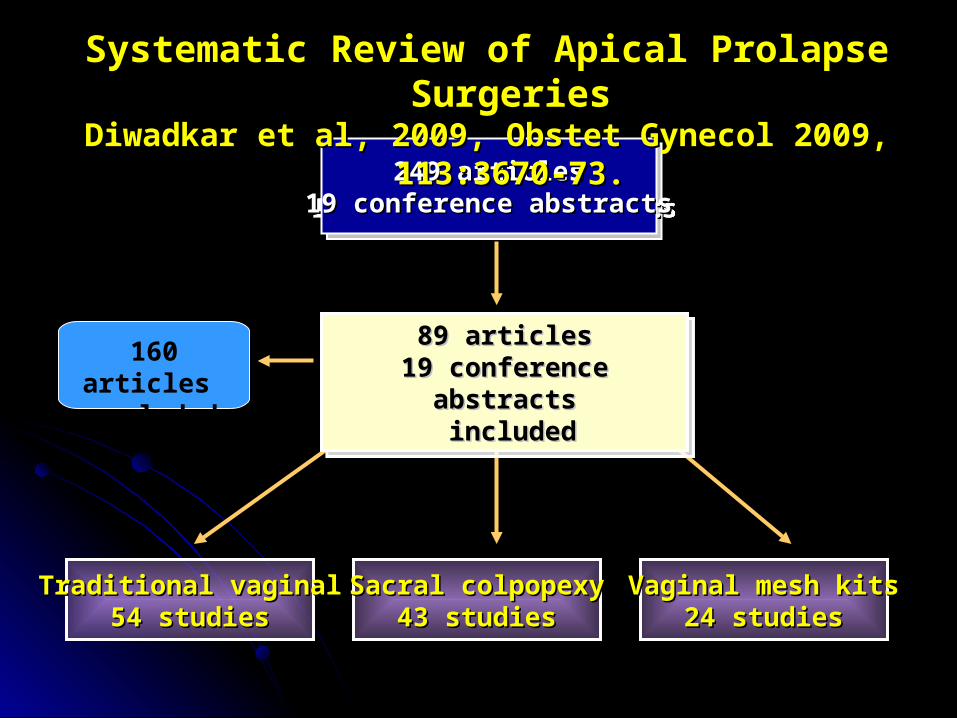
249 articles249 articles19 conference abstracts19 conference abstracts
249 articles249 articles19 conference abstracts19 conference abstracts
160 articles excluded
Traditional vaginalTraditional vaginal54 studies54 studies
Sacral colpopexySacral colpopexy43 studies43 studies
Vaginal mesh kitsVaginal mesh kits24 studies24 studies
89 articles89 articles19 conference abstracts19 conference abstracts
includedincluded
89 articles89 articles19 conference abstracts19 conference abstracts
includedincluded
Systematic Review of Apical Prolapse SurgeriesSystematic Review of Apical Prolapse SurgeriesDiwadkar et al, 2009, Obstet Gynecol 2009, 113:3670-73.Diwadkar et al, 2009, Obstet Gynecol 2009, 113:3670-73.
Conclusions of ReviewConclusions of ReviewTraditional vaginal procedures Traditional vaginal procedures
Highest reoperation rate for prolapse recurrenceHighest reoperation rate for prolapse recurrence
Lowest rates of complications that required surgical Lowest rates of complications that required surgical
intervention intervention
Lowest total reoperation rateLowest total reoperation rate
Vaginal mesh kits Vaginal mesh kits Shortest follow-up periodShortest follow-up period
Highest rate of complications that required surgical Highest rate of complications that required surgical
interventionintervention
Highest total reoperation rate (recurrence + complications)Highest total reoperation rate (recurrence + complications)
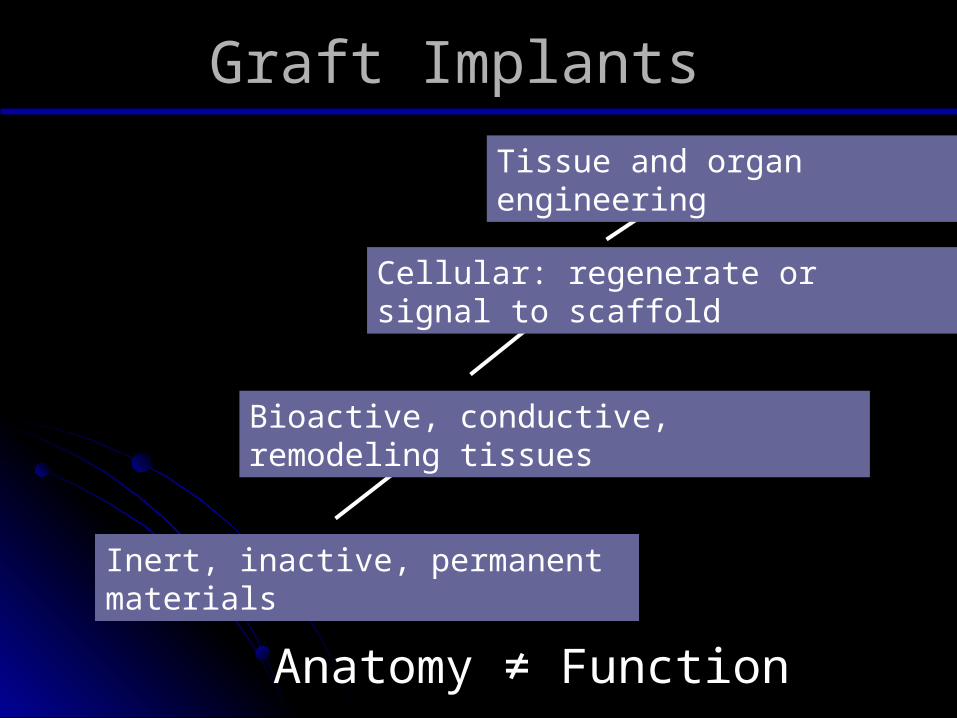
Graft ImplantsGraft Implants
Inert, inactive, permanent materials
Bioactive, conductive, remodeling tissues
Cellular: regenerate or signal to scaffold
Tissue and organ engineering
Anatomy ≠ Function
Vaginal Prolapse Surgery: Vaginal Prolapse Surgery: No Mesh or Mesh?No Mesh or Mesh?
Sacral colpopexy and mid-urethral slings are the most Sacral colpopexy and mid-urethral slings are the most
proven surgeries using meshproven surgeries using mesh
Grafts tend to improve anatomic success in most prolapse Grafts tend to improve anatomic success in most prolapse
repairs, but there is usually no significant difference in QOL repairs, but there is usually no significant difference in QOL
and sexual function after traditional vs. mesh surgeryand sexual function after traditional vs. mesh surgery
Grafts always increase complications and cost but many Grafts always increase complications and cost but many
surgeons use vaginal grafts routinely and with great successsurgeons use vaginal grafts routinely and with great success
Surgeons should use what is best in their hands Surgeons should use what is best in their hands
What are we doing at the What are we doing at the Cleveland Clinic?Cleveland Clinic?
Route of Surgery:Route of Surgery: Vaginal 65%, Laparoscopic 20%, Robotic 10%, Open 5%Vaginal 65%, Laparoscopic 20%, Robotic 10%, Open 5%
I do most kit procedures in our division: uterine I do most kit procedures in our division: uterine sparing, recurrent, non-sexually active, co-sparing, recurrent, non-sexually active, co-morbid, vaginal route indicated or preferredmorbid, vaginal route indicated or preferred
Referral center mesh removal (kits, Referral center mesh removal (kits, augmentation)augmentation)
We have been doing robotic surgery in Gyn since We have been doing robotic surgery in Gyn since 2000; for prolapse since 20062000; for prolapse since 2006
Tend to be “early adopters” but with a skeptical Tend to be “early adopters” but with a skeptical eye; “early studiers” so we can make eye; “early studiers” so we can make recommendations on “Best Practice”recommendations on “Best Practice”
Concluding CommentsConcluding Comments
I believe that augmented vaginal repairs and I believe that augmented vaginal repairs and robotic surgery will continue to be part of the robotic surgery will continue to be part of the future of pelvic reconstructive surgery but future of pelvic reconstructive surgery but not in their current form.not in their current form. New innovations in these technologies are already on New innovations in these technologies are already on
the way!the way! New biocompatible mesh, flexible-single port robots, New biocompatible mesh, flexible-single port robots,
stem cell therapy, gene therapy and biomarkers are in stem cell therapy, gene therapy and biomarkers are in development!development!
When adopting innovative techniques When adopting innovative techniques
into your surgical practice:into your surgical practice: Do your homework: Review the available literature Do your homework: Review the available literature
& package insert& package insert Go to a training sessionGo to a training session Have your first 5-10 procedures proctored by a Have your first 5-10 procedures proctored by a
surgeon experienced in the techniquesurgeon experienced in the technique Inform the patientInform the patient Critically reflect on your experienceCritically reflect on your experience
Track your outcomesTrack your outcomes Keep up on the new dataKeep up on the new data Talk to colleaguesTalk to colleagues

Thanks for your attention!