user manual for the nihr crn industry costing … nihr crn industry costing template was the ......
TRANSCRIPT
User manual for the NIHR CRN
Industry Costing Template
Costing Industry Sponsored Studies
Version: May 2017
Guide to the NIHR CRN Industry Costing Template
May 2017 Page 2 of 32
Document Control
This document is issued and updated by the national CRN Coordinating Centre.
Readers should ensure that the latest version is being viewed which is available on the Life
Sciences Industry pages of the CRN website www.supportmystudy.nihr.ac.uk.
Document Information
Document Title User manual for the NIHR CRN Industry Costing Template
Version May 2017
Supersedes Version: April 2017
Function To support the use of the NIHR CRN Industry Costing Template
Effective Date May 2017
Audience All users and reviewers of the NIHR CRN Industry Costing Template
Category For Information
Expectation Operational
Purpose Supplementary information to support users understand the NIHR CRN Industry
Costing Template and facilitate the appropriate and efficient use of the templates
for Industry Sponsored (commercial contract) studies in the NHS.
Guide to the NIHR CRN Industry Costing Template
May 2017 Page 3 of 32
Contents
1. Executive Summary 4
2. Background 5
3. Format 7
4. Cost calculation 8
5. Worksheet Overview 12
6. Costing Completion and Agreement 16
7. Ongoing review and contacts 18
8. Annex 1 – Extract from the NHS Financial Manual 19
9. Annex 2 - NIHR CRN Industry Costing Group Membership 21
10. Annex 3 Frequently Asked Questions 22
11. Abbreviations 31

1. Executive Summary
The Industry Costing Templates were developed in 2008 to provide a single, standardised
structure for the display and calculation of NHS costs associated with the delivery of Industry
Sponsored clinical trials. By providing a standard format with greater cost transparency and
consistency for research costs the aim was to minimising the time required for cost
negotiations which impacts on study set-up time.
The fit-for-purpose templates have been developed in a collaborative process involving the
NHS and Life Science Industry representatives for use in trials of pharmaceutical and
biotechnology agents in secondary care or primary care settings and medical device studies
in secondary care or primary care settings eligible for the NIHR CRN portfolio.
As dynamic templates, they are updated annually and frequently reviewed to ensure they
remain accurate and fit-for-purpose for both the NHS and the Life Science Industry. The
templates do include guidance costs for an ‘average’ clinical trial which are designed to be
transparently adjusted where relevant with accompanying justification to support the
adaptation. The templates do not reflect a national tariff which would anti-completive for the
NHS Organisations involved.
This novel approach to national research costing provides the NHS with a unique selling
point in the global market of commercial clinical trials and this guidance document is design
to support the effective use of these templates to minimise the time required for cost
negotiations during study set-up. For the most effective approach to commercial research in
the NHS, the NIHR CRN Industry Costing Template should be used in conjunction with the
national model agreements for study contracts.
The latest version of the NIHR CRN Industry Costing Templates can only be accessed on
the dedicated NIHR website.

2. Background
The NIHR CRN lead a Costing Project to address a specific recommendation made in the
Cooksey Report 2006, which highlighted the need for a transparent and consistent national
costing system. The NIHR CRN Industry Costing template was the output of this group.
With 233 1 NHS Trusts in England, all taking responsibility for their own finances as
independent legal entities, the range in methodology of research cost calculation and display
had the ability to adversely affect study set-up time. Sponsors would review numerous cost
formats to compare values and ensure a ‘fair market value’ was represented for the service
delivered.
As publically funded bodies, each NHS Organisation needs to ensure that commercial
research is not subsided with tax payer money and in line with the Health Service Guidelines
(HSG) 97-32 ‘Responsibilities for meeting patient care costs associated with research and
development in the NHS’ ensure that “All Costs Associated with Commercial R&D to be met
by company concerned”. The template methodology enables the NHS Organisations to be
confident that the cost structure can reflect this requirement while fulfilling the Life Sciences
Industry requirement for cost transparency under Anti-bribery and Anti-corruption legislation.
The resulting commercial cost approach provides:
Clarity Clear methodology and standard rates to calculate consistent and transparent prices associated with industry-sponsored studies to support both the Life Sciences Industry and the NIHR CRN
Guidance For Industry and the public sector
Full reimbursement To NHS Trusts for any activities associated with commercial studies, in accordance with the requirements of the NHS Finance Manual (Annex 1)
Supports research in the NHS
Support a swift, transparent cost negotiation and value for money environment for clinical research
Development Groups
The templates were developed in conjunction with three key groups:
Industry Road Map Group
Steers the development of the overall NIHR CRN agenda for commercial research
National Pharmacy Clinical Trials Advisory Group (NPCTAG)
Dedicated support service group who also provide input and recommendations for the pharmacy costing worksheet and associated tasks.
NIHR CRN Industry Costing Group
formed specifically to provide expertise in the development and ongoing management the costing template for industry-sponsored studies. The group membership (Annex 2) includes
1 https://improvement.nhs.uk/resources/national-tariff-1719/

representatives of the pharmaceutical industry, Contract Research Organisations, NHS R&D Forum, NHS R&D staff, Department of Health, University/ academic sector, NIHR Clinical Research Network and NHS Pharmacy Services.
3. Format
The Industry Costing Templates are Microsoft Excel based tools providing an accessible,
easy-to-use spreadsheet based method of calculating the contract price of an individual
industry-sponsored study. The template values are based on standardised staff rates to
enable input of study specific staff time required, specific investigations required and their
frequency as well as any set-up or additional charges. The format ensures that the costs of
all activities undertaken at the site are included in the final price agreed with the Sponsor.
Worksheets
There are seven or eight separate cost sections on individual worksheets depending on which
template is required:
Cover sheet
Study information
Per Patient Costs
Additional Itemised Investigation Costs
Device/Supply Management (Medical Technology templates only)
Pharmacy Costs (termed NHS Trust Pharmacy for Primary Care templates)
Set-up and Other Costs
Summary
Completion
It is the responsibility of the Sponsor Company to select the appropriate template and enter
the protocol or clinical investigation plan activities into the relevant sections. The template will
automatically calculate the total chargeable price consisting of:
full cost i.e. the cost to the NHS inclusive of direct costs and indirect costs
capacity building element
local cost adjustment for each Trust involved, via the National Tariff Market Forces
Factor (MFF).
Detailed information regarding how to complete the templates to ensure the automatic
calculations are maintained can be sought from the step-by-step completion guide on the
website.
4. Cost calculation
To get the most from the Industry Costing Templates, the cost calculation methodology used
is important to understand.
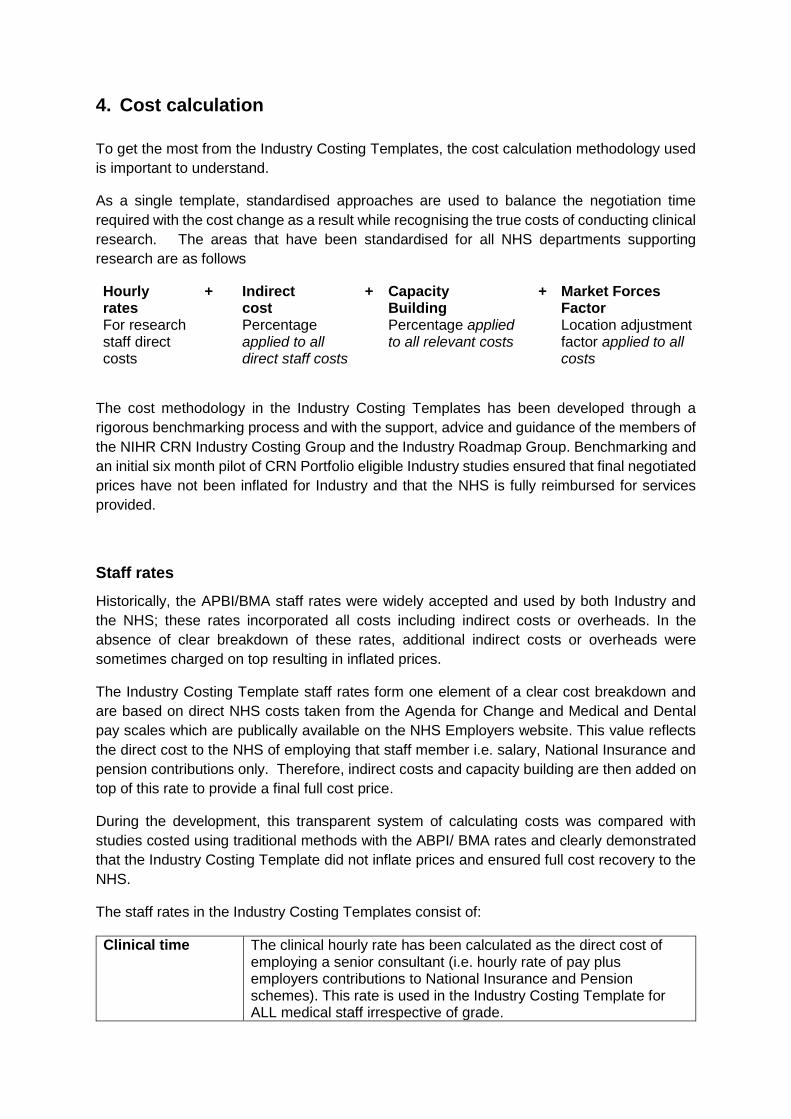
As a single template, standardised approaches are used to balance the negotiation time
required with the cost change as a result while recognising the true costs of conducting clinical
research. The areas that have been standardised for all NHS departments supporting
research are as follows
Hourly rates
+ Indirect cost
+ Capacity Building
+ Market Forces Factor
For research staff direct costs
Percentage applied to all direct staff costs
Percentage applied to all relevant costs
Location adjustment factor applied to all costs
The cost methodology in the Industry Costing Templates has been developed through a
rigorous benchmarking process and with the support, advice and guidance of the members of
the NIHR CRN Industry Costing Group and the Industry Roadmap Group. Benchmarking and
an initial six month pilot of CRN Portfolio eligible Industry studies ensured that final negotiated
prices have not been inflated for Industry and that the NHS is fully reimbursed for services
provided.
Staff rates
Historically, the APBI/BMA staff rates were widely accepted and used by both Industry and
the NHS; these rates incorporated all costs including indirect costs or overheads. In the
absence of clear breakdown of these rates, additional indirect costs or overheads were
sometimes charged on top resulting in inflated prices.
The Industry Costing Template staff rates form one element of a clear cost breakdown and
are based on direct NHS costs taken from the Agenda for Change and Medical and Dental
pay scales which are publically available on the NHS Employers website. This value reflects
the direct cost to the NHS of employing that staff member i.e. salary, National Insurance and
pension contributions only. Therefore, indirect costs and capacity building are then added on
top of this rate to provide a final full cost price.
During the development, this transparent system of calculating costs was compared with
studies costed using traditional methods with the ABPI/ BMA rates and clearly demonstrated
that the Industry Costing Template did not inflate prices and ensured full cost recovery to the
NHS.
The staff rates in the Industry Costing Templates consist of:
Clinical time The clinical hourly rate has been calculated as the direct cost of employing a senior consultant (i.e. hourly rate of pay plus employers contributions to National Insurance and Pension schemes). This rate is used in the Industry Costing Template for ALL medical staff irrespective of grade.

Nurse time & other professional staff (e.g. pharmacists)
The hourly staff rate has been agreed at the top of Agenda for Change band 7 which includes only the hourly rate of pay plus employers contributions to National Insurance and Pension schemes.
Administration time
The NIHR CRN hourly administration rate is set at the top of Agenda for Change band 3 which includes only the hourly rate of pay plus employers contributions to National Insurance and Pension schemes. The admin rate will only be used for studies which require specific data entry or other discrete/defined tasks, by an admin assistant. It is not to be used for calculating general admin duties such as clinician’s secretarial costs which are included in the Indirect Costs rates described below.
GP and Practice Manager time
As employed by independent providers, a specific GP rate has been develop in consultation with Primary Care representatives during the template development. The Practice Manager rate has been tethered to equivalent NHS Agenda for Change pay band for other professional staff. This approach has given a consistent methodology for the primary care site costs in the absence of alternatives sources of pay structure for these staff, variability and transparency of staff pay in general medicine.
Annual changes to staff pay
Staff rates in the templates are adjusted in accordance with NHS salaries, National Insurance
and Superannuation contributions at the beginning of each financial year (April for the NHS).
The application of staff rate changes should be agreed between the site and company and
detailed in the model agreement as required.
Indirect Costs
Indirect running costs are incurred by the organisation conducting research and reflect the
‘true’ cost of conducting clinical research. They cover the NHS Costing Manual ‘overhead’
categorised elements such as heating, lighting, building maintenance and corporate
management as well as the ‘indirect’ costs such as security staff, finance, general
administration, human resources, and other support functions. This term in the Industry
Costing Template is designed to cover all these aspects and enable potential activity based
allocation to cost centres when related to research income through the income distribution
model methodology.
The indirect cost rate is also used to cover the cost of the infrastructure, which allows clinical
trial activity to take place. It provides recognition and potential reimbursement of those tasks
which cannot always be attributed to a specific study procedure such as general organisation
or communication with the Sponsor such as teleconferences or individual telephone calls. The
indirect cost percentage is fixed in the Industry Costing Template and it is important to
recognise that indirect costs are only added to direct staff costs. This approach indirectly
relates the value, which may be incurred by a number of cost centres in different proportions,

to level of patient activity on the study. The templates are formulated to include this
automatically.
Following consultation and extensive benchmarking, using both retrospective and real time
studies to ensure that overall costs were acceptable to both NHS and industry, the Indirect
Costs rate has been set at 70% for secondary care and medical device studies. The Primary
Care setting is a different facility environment and as such the indirect costs are reduced to
25% for studies conducted in this setting and is reflect in the relevant Industry Costing
Templates.
The Industry Costing Templates ensure that NHS organisations and or Primary Care facilities
are properly reimbursed for their direct and indirect costs and that indirect costs are only added
once. This element has a direct impact on the sustainability of the individual research activity
and the research environment as a whole.
Capacity building
Investment in the research offering of the NHS requires the long term commitment of all
stakeholders and following consultation with key stakeholders, agreement was reached that a
capacity building margin should be incorporated into the final price to support this. The
element is intended to build sustainable research and innovation capacity to the benefit of all
research partners, but this requires significant commitment and resources from all research
partners to utilise for the best effect.
This rate has been set at 20% and is added to direct staff and investigation costs and the
income raised through this element is intended to be ring-fenced within NHS Trusts to build
research capacity.
Location Adjustment Factor – Market Forces Factor
The delivery of healthcare across the nation is recognised as having an uncontrollable variable
cost components indices: Staff, Medical & Dental (London only), Land and Buildings. NHS
England commissioned by the Department of Health annually publishes a ‘Market Forces
Factor’ tariff via the group ‘Monitor’ as part the National Tariff. This factor provides an
adjustment value to accommodate these unavoidable cost differences of providing healthcare
across the country.
In the Industry Costing Templates the MFF is applied to localise the national rates for the
geographical location in which the research is being conducted. This approach better reflects
the ‘actual’ cost of delivery while maintaining a national charge-out rate for staff to minimise
negotiation required when agreeing costs at each location.
The final price calculated within the Industry Costing Template is multiplied by the MFF rating
for each individual participating Trust, including those in the devolved nations who have a
country specific MFF:
For example, a calculated fee per patient of £2500 becomes:

Nottingham MFF 1.07 x £2500 = £2681 (price for Nottingham)
London MFF 1.25 x £2500 = £3125 (price for London)
Further information about MFF can be found on the gov.uk website.
5. Worksheet Overview
5.1 Cover sheet
The cover sheet provides information regarding the template i.e. the type of template which
has been downloaded and for which study types it can be used for.
It includes information regarding contact details for the research site and the Sponsor
contact. These are used to ensure that anyone working with the template will have access
to the relevant contact information to support a swift agreement of costs. This is especially
important for example if a staff member is on leave and the discussions must continue in
their absence.
The last section forms part of the CRN quality check ‘validation’ and Trust sign-off of the
costs. There are three sections completed by the 1) CRN staff to confirm completion of the
quality review for the master version (a requirement for HRA approval submission), 2) the
Sponsor to confirm any changes prior to sharing with sites as part of the minimum document
set and 3) final agreement by the Trust.
5.2 Study Info
The study information sheet requires the inclusion of the study specific information to enable
clear identification of the study when completing or reviewing the associated costs. The two
key components included are:
The ‘patient total’ box enables various auto-calculations within the template to run correctly and provided a representative total value
The ‘market forces factor’ drop-down menu selection
ensures the relevant uplift factor can be applied to the costs.
This worksheet also includes questions regarding the study requirements to provide relevant
guidance responses to ensure the correct sections are completed initially which minimises
review comments.
5.3 Per Patient Budget
One of the key objectives of the NIHR CRN Industry Costing Project was to establish clarity
about the method of calculation of the prices charged to Industry by the NHS, for industry-
sponsored studies. The Per Patient Budget page in the Industry Costing Templates enables
automatic calculation of a per patient price for individual clinical studies based on the time
taken to perform each procedure required by the protocol or clinical investigation plan.
This worksheet requires the identification of all per patient activities conducted within the
study, establishing which member of staff would be most likely to perform the activity and the
time required to complete each task. Guidance is provided within the Industry Costing
Template by providing pre-populated staff times and additional considerations for the common
procedures in the ‘About this template’ worksheet that may help understand when adjustments
to these recommended times are required. All parties can then see a clear breakdown of the
costs and negotiation should be based around the time to perform a procedure rather than the
resultant cost value.
Investigation Pricing Index
The Investigation Pricing Index captures the research investigations commonly used in
Industry studies using Provider to Provider data-sets from NHS organisations i.e. the prices
an NHS host organisation charges another NHS organisation for a specific investigation. Any
outlying data points were removed by subtracting any prices greater than one standard
deviation from the mean and the MFF was removed from each individual Trust price to
generate data from which a mean cost for each investigation could be established. The prices
will have 20% capacity building and the MFF added by the Industry Costing Template. Indirect
costs will not be added as they have already been included by Trusts as it is hard to separate
the indirect costs of performing an investigation from the direct staff costs and thus are
concluded to already be included in the cost.
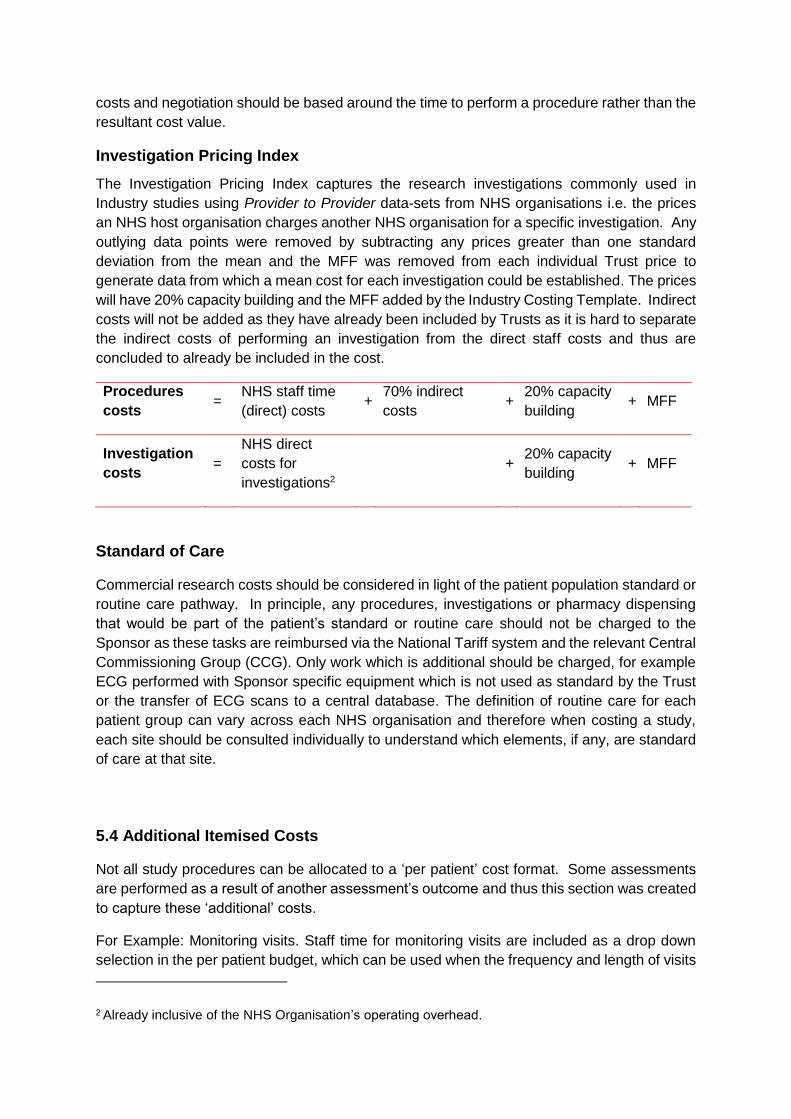
Procedures
costs =
NHS staff time
(direct) costs +
70% indirect
costs +
20% capacity
building + MFF
Investigation
costs =
NHS direct
costs for
investigations2
+ 20% capacity
building + MFF
Standard of Care
Commercial research costs should be considered in light of the patient population standard or
routine care pathway. In principle, any procedures, investigations or pharmacy dispensing
that would be part of the patient’s standard or routine care should not be charged to the
Sponsor as these tasks are reimbursed via the National Tariff system and the relevant Central
Commissioning Group (CCG). Only work which is additional should be charged, for example
ECG performed with Sponsor specific equipment which is not used as standard by the Trust
or the transfer of ECG scans to a central database. The definition of routine care for each
patient group can vary across each NHS organisation and therefore when costing a study,
each site should be consulted individually to understand which elements, if any, are standard
of care at that site.
5.4 Additional Itemised Costs
Not all study procedures can be allocated to a ‘per patient’ cost format. Some assessments
are performed as a result of another assessment’s outcome and thus this section was created
to capture these ‘additional’ costs.
For Example: Monitoring visits. Staff time for monitoring visits are included as a drop down
selection in the per patient budget, which can be used when the frequency and length of visits
2 Already inclusive of the NHS Organisation’s operating overhead.

directly relates to the number of patients enrolled in the study. Alternatively, monitoring visits
that do not correlate with the number of patients enrolled can be captured in the additional
itemised cost section and only charged as they are performed.
5.5 Pharmacy Costs (NHS Trust Pharmacy in Primary Care Template)
The method of calculating IMP-related costs for an NHS Trust Pharmacy utilises as dedicated
worksheet within the Industry Costing Template that has been specially developed and
updated in conjunction with the NIHR CRN Industry Costing Group and a pharmacy working
group from the National Pharmacy Clinical Trials Advisory Group (NPCTAG).
A breakdown of Pharmacy activities was identified and average recommended times allocated
for each. While included in a separate worksheet, the structure of the remaining template is
maintained with separate areas for set-up, per patient and other costs with full descriptions of
the tasks contained in the Pharmacy section in the costing template.
Set up activities Categorised into three bands, which are complexity-based and range from a simple dispensing study to a complex study involving aseptic technique. Timing required for individual activities within these bands were agreed within the initial working group, leading to the proposed prices included in the Industry Costing Templates for set up.
Per patient costs Driven by the number of dispensing per patient per study drug and includes costs for NHS prescription charges
IMP management Fee is included to cover all non–patient associated IMP-Management-based Pharmacy tasks when taking part in research studies
Additional work Charged by using the additional or variable cost sections as necessary.
Where IMP related costs need to be included for other locations, such as IMP management
within a General Practice. These should be included as procedures within the per patient or
additional itemised costs worksheets in the template.
5.5 Set-up & Other Costs
Additional legitimate study costs are captured in the Industry Costing Template, such as set-
up costs for a department providing services for a trial or payments which may be deemed as
‘pass-through’ costs.
Set-up costs
The set-up total is displayed with a task breakdown for each of the various departments and
services in relation to conducting clinical research studies along with guidance values for
inclusion when applicable. Details of various elements can be found in the fee definition area
at the bottom of the ‘Set-up and other costs’ worksheet.
Primary Care Referrals
General Practices that refer patients for clinical trials need to be reimbursed for performing
database searches and contacting their relevant patients via post or telephone which incurs
costs for the practice. They also need to be reimbursed for the follow-up work if the patient
chooses to participate, such as source data verification. As such a recommended payment
structure is included in the Industry Costing Template which was developed with the CRN
Primary Care specialists to reflect the best working practice.
Refreshment Costs
Patients (and their carers where appropriate) who are required to remain at the site for more
than three hours or have fasted prior to their visit should be offered appropriate refreshments
and sustenance. These costs should be included in the Industry Costing Template on the Set-
up and other costs tab.
Inconvenience Payments
Reimbursement for patient inconvenience due to taking part in a clinical trial can be captured
in this section as applicable. The Sponsor should decide when this may be applicable for a
study and the costs include should be approved by the ethics committee.
Travel Costs
It is often difficult to estimate the reimbursement costs for patient travel at the beginning of a
study. A maximum amount per patient per visit should be established with the Sponsor to
support reflective budget generation. A number of approaches can be used to manage these
costs and some examples are provided in the model agreement financial appendix template
on the NIHR website.
Chief Investigator Expenses
The expenses associated with the Chief Investigator attending an ethics meeting should be
outlined in the costing template to support transparency of payments.
5.6 Summary Page of Total Costs
A total value is provided on the summary page to enable all parties to understand the total
costs involved. However, due to the nature of the clinical research these ‘total’ values should
be treated as guidance only as the actual total will depend on recruitment levels and the
progress of the study.
Tables providing summaries of per visit costs and investigation costs can be generated using
the programmed buttons to the right of the summary table.

6. Costing Completion and Agreement
Further information regarding the process below can be found in the effective costing and
contracting leaflet on the CRN website or obtained through the NIHR CRN Support My Study
helpdesk via [email protected] or by telephoning 0113 34 34 555.
Step 1 Submit study for CRN portfolio eligibility Sponsor or CRO applies for CRN Portfolio status via CRN feasibility and eligibility services using the CRN system accessed via https://cpms.nihr.ac.uk prior to HRA approval submission.
NOTE: This is separate to the IRAS submission
Step 2 Download templates and guidance documents The Sponsor or CRO downloads the latest copy of the relevant Industry Costing Template according to their study requirements from the NIHR Website Costing Section. The relevant guidance documents can be accessed from this same location to support accurate completion of the template.
Step 3 Input study specific information for cost calculation The Sponsor or CRO populates the Industry Costing Template to reflect the study requirements of the latest protocol or study design
Step 4 CRN provided with completed template for validation Sponsor provides Local CRN industry team contact with the completed template for validation along with the protocol/schedule of events prior to submission for HRA approval. This is provided to the Local CRN supporting the site where the Chief Investigator is located.
Step 5 CRN undertake study wide validation The Local CRN are responsible for validating the costing template and returning the validated template along with any comments to the Sponsor or CRO within 3 working days. The checklist used to validate the template is available on the NIHR Website Costing Section where the templates are provided.
Step 6 HRA approval submission Following the completion of the template validation, the Sponsor or CRO includes the validated template with the HRA approval submission.
Step 7 Local cost negotiation with each site HRA ‘initial assessment’ letter confirms the validated template as an information source for participating site assessment, arrangement and confirmation of local capacity and capability. Cost negotiations are an activity undertaken as part of the confirmation of local capacity and capability.
Step 8 Inclusion in model agreement financial appendix The final agreed costing template should be included in the model agreement along with any necessary invoicing or payment information in Appendix 5: Financial Arrangements. A template is available on the NIHR Website Costing Section

Cost negotiations with individual sites
The Industry Costing Template supports the clear documentation and display of study tasks
and associated times to support swift local negotiations with each site involved. The templates
do not constitute a set national tariff and agreement with each site will need to be sought as
each site is responsible for their own contract and thus costs.
While the templates are intended to minimise the scope for local negotiation if all time and
requirements have been captured appropriately within the final price, there may occasionally
be specific local issues to address. These can include the timing of activities or delivery of
investigations for example, procedures in frail or vulnerable populations may require more
time or access to equipment may vary between sites. A cost adjustment may be required as
a result and that will need to be discussed and agreed between the site and Sponsor or CRO
directly.
The NIHR CRN can support these negotiations by acting as a mediator between the parties
to reach an agreement. However, it is important to recognise that the NIHR CRN does not
have the authority to set a fixed price for research activities within the NHS and a fixed price
for NHS research could also create an anti-competitive environment.
7. Ongoing review and contacts
The methodology, rates, investigation pricing index, template format and costing process
described in this guidance document are monitored and reviewed periodically by NIHR CRN
Costing Group. Adjustments may be made as deemed appropriate to ensure they remain fit-
for-purpose.
Any issues experienced should be sent to the CRN Study Support Service Helpdesk at
[email protected] or proposed changes can be submitted via the online feedback
form at the bottom of the NIHR Website Costing Section to be reviewed for the next template
revision.
As updates to the Industry Costing Template will be made on a regular basis, users are
advised to download a new version of the Industry Costing Template from the NIHR CRN
website for each new study to avoid potential re-work at a later stage.

8. Annex 1 – Extract from the NHS Financial Manual
Research and Development (R&D) 30.47 The Prime Minister’s Pharmaceutical Industry Competitiveness Task Force (PICTF,
March 2001) reported an inconsistent approach to costing for commercial R&D activity in the NHS. The Department agreed to clarify guidance to promote a more consistent and transparent approach to pricing.
30.48 The current policy for commercial R&D in the NHS is in two guidance documents:
HSG (97) 32 Responsibilities for meeting patient care costs associated with research and development in the NHS), http://www.dh.gov.uk/PublicationsAndStatistics/LettersAndCirculars/HealthServiceGuidelines/HealthServiceGuidelinesArticle/fs/en?CONTENT_ID=4018353&chk=ZUXc1q and
Commercial sponsorship: ethical standards for the NHS, November 2000) http://www.dh.gov.uk/PublicationsAndStatistics/Publications/PublicationsPolicyAndGuidance/PublicationsPolicyAndGuidanceArticle/fs/en?CONTENT_ID=4005135&chk=2dVlTD
30.49 This section supplements that guidance and should be read in conjunction with it. All
NHS income derived from commercial R&D activity is raised through Income Generation powers. NHS bodies engaged in this activity should make arrangements to ensure they comply fully with this guidance, including the accounting requirements. The guidance requires income generation activity to be profit making but does not specify target levels.
30.50 The Department has assured the pharmaceutical industry that it wishes to support and
encourage R&D in the NHS. The creation of UK Clinical Research Collaboration in 2004 is one of the measures introduced to facilitate this. The NHS should not subsidise commercial R&D. That would divert resources from patient care. On the other hand, the Government does not wish the NHS to take advantage of market conditions to maximize profits, because of the wider benefits of conducting R&D activity to NHS patients in this country.
30.51 Paragraph 30.20 states that where an item or service is considered an integral part of
a patient’s treatment (treatment in this context includes diagnostic procedures) then a charge should not be made. Income generation powers must not be used to carry out the delivery of core functions. Therefore, when costing out commercial studies, NHS bodies may not seek to recover from industry the costs of standard treatment that would otherwise have been incurred in treating patients in the NHS. NHS bodies’ costing may include only activities, tests, treatments, etc which are in addition to normal treatment of the condition concerned. The exception is that, in accordance with the normal conventions for commercial clinical trials, the company sponsoring the trial is expected to supply free the medicine that is the subject of the trial.
30.52 In discussions on pricing with companies proposing to undertake commercial studies,
NHS bodies should seek to disaggregate costs, with appropriate Indirect Costs related to each separately identified item, to avoid the use of general Indirect Costs. This approach is in line with Government policy to improve transparent pricing in selling government services into wider markets. Guidance is provided in the document “Guidance to Facilitate the Conduct of Commercially Funded Research in the National

Health Service (Secondary Care)”, January 2005, produced by the NHS Research and Development Forum, ABPI and the Institute of Clinical Research (www.rdforum.nhs.uk).
30.53 NHS bodies should consider in the context of all their functions how they propose to
utilise funds generated through commercial R&D activity. It is acceptable to plan for profit to be used within the NHS body’s own managed R&D programme, but this is a matter for agreement with the NHS body’s Board and Chief Executive.
30.54 Guidance on contract research and on collaborative or co-funded research related
activity is given in the Clinical Research Report of the Pharmaceutical Industry Competitive Task Force which was published in March 2002 (www.advisorybodies.doh.gov.uk/pictf).

9. Annex 2 - NIHR CRN Industry Costing Group Membership
Group membership list – April 2017
NIHR CRN
NIHR CRN CC representatives
Local CRN representatives
Devolved Nations Networks
NHS Research Scotland
National Institute for Social Care and Health Care Research (NISCHR) (Wales)
NHS Trusts
University Hospitals Bristol NHS Trust
Kings Health Partnership and Imperial College London
Southampton University Hospitals NHS Trust
NHS Trust Finance
Newcastle Upon Tyne Hospitals NHS Foundation Trust
Primary Care
Primary Care Speciality Group representation being considered by Speciality Group
members, current feedback mechanism via CRN CC
R&D Forum
R&D Forum Manager
UK CRF Network
UK CRF Network Member
Pharmacy (NPCTAG)
Costing Sub-group representative from either Southampton University Hospitals NHS
Trust, Royal Free NHS Foundation Trust or Newcastle Upon Tyne Hospitals NHS
Foundation Trust
Department of Health
Finance and Performance, Department of Health
Health Research Authority
Policy Lead
Industry
Boehringer Ingelheim (cCOG and CREN representative)
Novartis
MSD
Sanofi
Industry (Medical Technology)
Medtronic
Industry (CRO)
Quintiles
The CRN would also like to acknowledge the advice and support of the many other individuals
and organisations who have contributed to the development and refinement of the NIHR CRN
Industry Costing process.
10. Annex 3 Frequently Asked Questions
1. Template use
Can the Industry Costing Template be used for studies which are not run via NIHR CRN?
Yes. Some NHS Trusts request a completed Industry Costing Template for those studies not conducted via the Network, in order to support local costing negotiations. The NIHR CRN supports this approach, as it ensures that the site is taking into account its full cost recovery responsibilities and providing an efficient and consistent methodology to do so.
Can devolved nations use the NIHR CRN Industry Costing Template?
The Costing Template is approved for use within the Devolved Administration of Scotland, Wales and Northern Ireland, by utilising a country specific MFFs from the drop down menu selection.
Does the template affect the incentive for researchers to take part in Industry sponsored studies?
The NIHR CRN Industry Costing Template provides a tool to support NHS R&D and finance departments in their allocation and reimbursement of funds to researchers and departments supporting research. The Income Distribution Guidance document has been issued by the NIHR CRN to provide a suggested framework for funding flow between researchers and the Trust, which must be reviewed and agreed at a local level.
Does the Network receive any of the template fees?
Trusts contract directly with Companies as per the financial arrangements documented within the model agreement and all fees will go directly to the Trust. Local agreements between Trusts and Local Clinical Research Networks ensure the cost reimbursement for Network staff time where applicable.
Should the template be used for commercial non-clinical trials?
Yes. The Industry Costing Template provides consistent methodology to calculate transparent prices which clearly represent the activities required to deliver the study and this includes activities to deliver non-clinical trials. The template supports the parties involved to clarify what activity and resources is required in a consistent manner. As such the template can be amended to reflect a one off activity or multiple activities as required within the 'additional itemised costs' worksheet and/or revision of the 'set-up and other fees' worksheet content.
2. Template completion
Who should complete the Industry Costing Template?
The Industry Costing Template will be completed by the company (either Sponsor or CRO) which should be quality checked by the CRN prior to sharing with any study sites.
The template looks complicated, is it difficult to use?
No. The Industry Costing Template is based in excel with pre-populated formulas to ensure the format is familiar and easy to complete. Completion instructions are provided within the template step by step guide available on the CRN website
where the templates are downloaded. Users only need to populate certain cells and all prices will be automatically calculated based on the data entered. The NIHR CRN support my study team or your local CRN team offers a support facility to answer any questions or difficulties you may be having when using the template. This can be accessed through your local contact or via [email protected] or please call 0113 34
34 555.
Why are the indirect costs set at 70%?
It is essential to understand that a 70% for indirect costs is only added to the DIRECT STAFF COST NOT to a commercial price. Previous costing methods have traditionally added 30-40% ‘overheads’ onto the Trust commercial rate, whereas the Industry Costing Template bases its calculations on the direct cost to the Trust. This rate has been chosen as a result of extensive benchmarking to select an appropriate multiplier which did not inflate prices. In practice this means that one hour of clinical time (direct staff costs + overheads + capacity building rate of 20%) with the MFF compares favourably with the ABPI/BMA medical hourly rate.
Why are the 70% indirect costs not added to the Investigation Pricing Index?
The price of investigations in the Pricing Index was derived through a benchmarking process from more than 25 Trusts, using provider to provider prices for NHS services which include elements of staff time and equipment. Thus these prices already include Trust indirect costs for that investigation and inclusion of an additional charge for indirect costs would be duplication.
How are the staff rates calculated?
The hourly rates have been calculated using the salary at the top of each staff band in the Agenda for Change Pay scale available on the NHS employer website and updated each year, which takes into account annual leave. As the rate is based on the highest salary for the pay grade it provides assurance that all salary costs are covered regardless of the pay scale of the staff member performing the task, which may not be the case if using an average pay value. It also automatically builds in some flexibility when negotiating times for procedures (as not all staff will be paid at this highest scale) without the need for prolonged negotiations with Sponsors to adjust the procedure times allocated. The time required to reach an agreement on a revised time may not also represent value for money in terms of the cost difference. The hourly rates do include National Insurance contributions and NHS superannuation scheme costs in the calculations and confirmation is detailed beneath the hourly rate table at the base of the study info tab in the costing template.
Are the University full Economic Costs (fEC) incorporated?
In September 2005, the UK Research Councils incorporated the fEC methodology for funding research projects, but this is different to the NHS cost structure applied in the Industry Costing template. There has been growing concern from the Life-Sciences Industry regarding cost when Universities are
involved in clinical research, which has been raised at forums such as the NIHR NHS Biopharmaceutical Industry R&D Leadership Forum led by the Department of Health. As a result there is ongoing work with the Association of UK Universities and Hospitals (AUKUH) to better understand the two cost approaches. Further information about fEC and funding based on these principles can be found on the Research Councils UK website under the Grant Terms and Conditions section www.rcuk.ac.uk/research/Pages/grantstcs.aspx
How do companies calculate the time that each study specific activity takes?
It is recognised that companies completing the Industry Costing Template may not know how long a specific assessment may take. There is a drop down box in the procedures column with a list of common study activities and any outside of this list will need to be negotiated with each site based on the company’s and site’s previous experience. It is often helpful to contact the lead or a participating site for the study in order to get advice regarding an appropriate time or cost to include on the initial completion of the template. An additional list of therapy area specific procedures developed by the NIHR CRN Costing Group may provide supporting information and is available at www.supportmystudy.nihr.ac.uk
My procedure isn’t listed?
Procedures are provided as guidance, based on consultation with NHS research staff. There are numerous instances where the times referenced may need to be adjusted such as Informed Consent for certain patient populations (mental health, children) or blood samples in different populations. The template includes guidance regarding these timings in the ‘Rate Card’ worksheet and the relevant section can be accessed directly via the hyperlink in the template under the procedure table. If there are no guide timings or price included in the template, please contact your Lead or a participating site for an estimate value that can be included. If a procedure is not listed, please populate the template to include this as per the protocol to avoid missing procedures from the template no matter how insignificant it may seem. Time spent communicating and adding missing procedures during negotiation is often more than the marginal cost of the actual procedure.
Where can I find out more about the investigations listed?
Definitions of the investigations listed in the template are provided in the ‘rate card’ section of the costing template. For Laboratory tests conducted in the NHS, the website http://labtestsonline.org.uk/ provides peer-reviewed information regarding the test and the sample requirements.
How were the prices of investigations reached?
To create the template guidance price list, twenty-five Provider to Provider datasets from NHS organisations were collected and assessed in 2008 when the template was first created. These data contain the prices that an NHS host organisation charges another NHS organisation for a specific investigation
(NHS provider to provider prices). Any outlying data points were removed by subtracting any prices greater than one standard deviation from the mean and the MFF was removed from each individual Trust price. These data were then used to establish a national mean cost for each investigation.
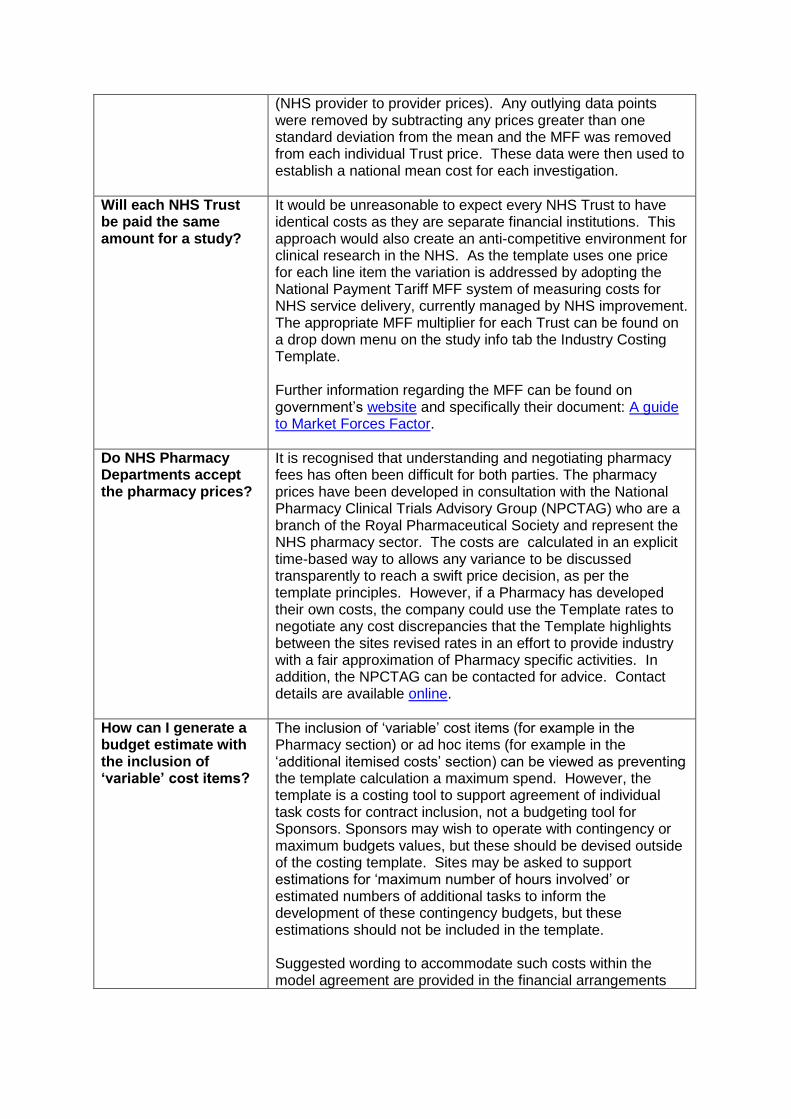
Will each NHS Trust be paid the same amount for a study?
It would be unreasonable to expect every NHS Trust to have identical costs as they are separate financial institutions. This approach would also create an anti-competitive environment for clinical research in the NHS. As the template uses one price for each line item the variation is addressed by adopting the National Payment Tariff MFF system of measuring costs for NHS service delivery, currently managed by NHS improvement. The appropriate MFF multiplier for each Trust can be found on a drop down menu on the study info tab the Industry Costing Template. Further information regarding the MFF can be found on government’s website and specifically their document: A guide to Market Forces Factor.
Do NHS Pharmacy Departments accept the pharmacy prices?
It is recognised that understanding and negotiating pharmacy fees has often been difficult for both parties. The pharmacy prices have been developed in consultation with the National Pharmacy Clinical Trials Advisory Group (NPCTAG) who are a branch of the Royal Pharmaceutical Society and represent the NHS pharmacy sector. The costs are calculated in an explicit time-based way to allows any variance to be discussed transparently to reach a swift price decision, as per the template principles. However, if a Pharmacy has developed their own costs, the company could use the Template rates to negotiate any cost discrepancies that the Template highlights between the sites revised rates in an effort to provide industry with a fair approximation of Pharmacy specific activities. In addition, the NPCTAG can be contacted for advice. Contact details are available online.
How can I generate a budget estimate with the inclusion of ‘variable’ cost items?
The inclusion of ‘variable’ cost items (for example in the Pharmacy section) or ad hoc items (for example in the ‘additional itemised costs’ section) can be viewed as preventing the template calculation a maximum spend. However, the template is a costing tool to support agreement of individual task costs for contract inclusion, not a budgeting tool for Sponsors. Sponsors may wish to operate with contingency or maximum budgets values, but these should be devised outside of the costing template. Sites may be asked to support estimations for ‘maximum number of hours involved’ or estimated numbers of additional tasks to inform the development of these contingency budgets, but these estimations should not be included in the template. Suggested wording to accommodate such costs within the model agreement are provided in the financial arrangements

suggested appendix text available on the NIHR website costing page.
What is the expectation for screen failure payments?
The template states that all screen failure work done will be charged as per the agreed costs in the template e.g. per patient procedure or investigation costs. Any assumptions regarding the portion of screen failures expected should be included in the protocol or agreed in conjunction with the PI and site expert input. Any estimation of screen failure rates that may affect the reimbursement of costs should be included in the model agreements financial appendix with wording to allow adjustment if the estimation is significantly different to reality.
How are travel costs covered?
The template has a dedicated section for including costs associated with patient travel in the ‘Set-up and Other costs’ worksheet. These may vary across sites due to location and transport links: for example rural based sites with minimal public transport access to city centre based hospitals with minimal parking availability. The patient population also needs consideration when developing the budget: for example some patient groups will require door to door transport or mobility support. In terms of payment for these costs there are several approaches taken by individual Trusts of which two common methods are detailed below: Use of a float – Within the financial arrangements appendix of the model agreement, wording is included to enable the Trust to obtain an upfront float of either a set value or a percentage of the total travel costs. The PI or research team nominee takes responsibility for maintaining the float and requesting additional funds when the value drops to an agreed minimum as per terms in the financial arrangements appendix. This float is used to reimburse the participants at the visits as per the agreed template values upon presentation of valid travel receipts/documentation which are retained to evidence the costs to the Sponsor/CRO. Wording is also included to cover the return of any un-used float fund to the Sponsor at the end of the study. Quarterly invoices – The Trust reimburses participants at the visits as per the agreed template values upon presentation of valid travel receipts/documentation which are retained to evidence the costs to the Sponsor. Each quarter the reimbursement value for that period in invoiced to the Sponsor/CRO for payment back to the Trust. Again, this approach is detailed in the financial arrangements appendix. Individual receipts are required for both options to evidence the values required and monies paid to patients. Additional wording should be included in the financial arrangements appendix to explain the procedure for agreeing travel costs higher than the maximum proposed in the template. This is usually the requirement for written approval from the
Sponsor/CRO prior to the participant incurring the higher travel costs.
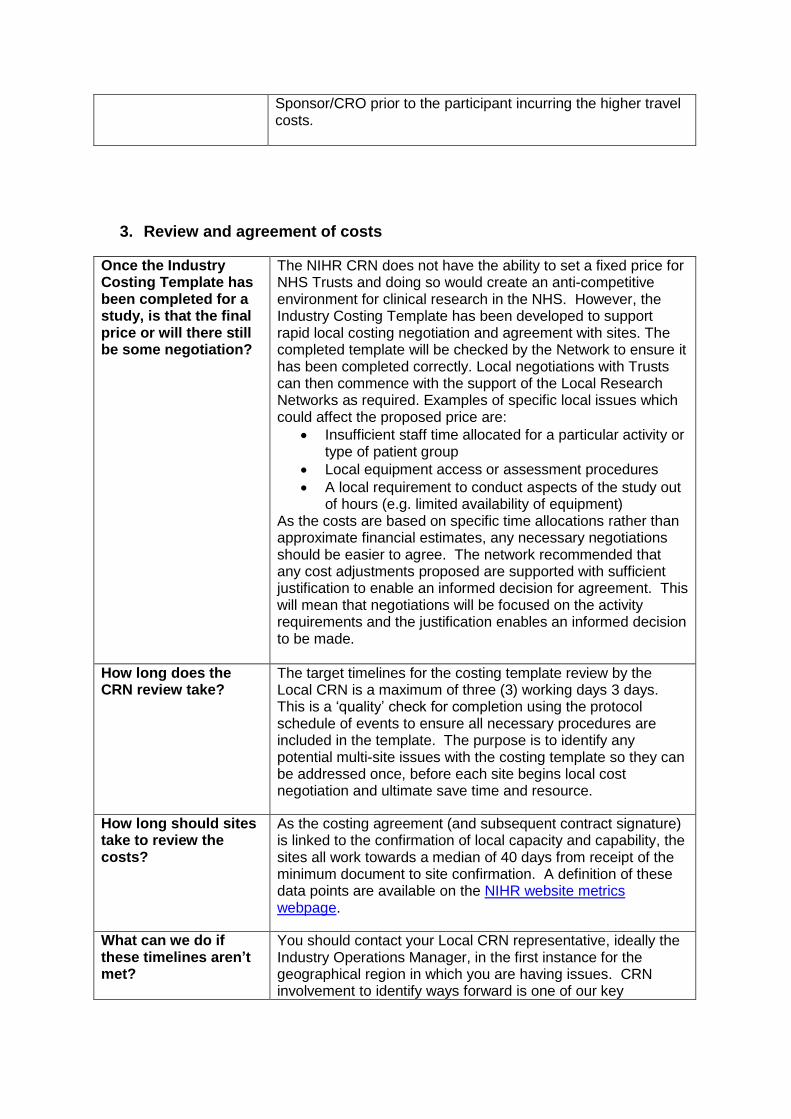
3. Review and agreement of costs
Once the Industry Costing Template has been completed for a study, is that the final price or will there still be some negotiation?
The NIHR CRN does not have the ability to set a fixed price for NHS Trusts and doing so would create an anti-competitive environment for clinical research in the NHS. However, the Industry Costing Template has been developed to support rapid local costing negotiation and agreement with sites. The completed template will be checked by the Network to ensure it has been completed correctly. Local negotiations with Trusts can then commence with the support of the Local Research Networks as required. Examples of specific local issues which could affect the proposed price are:
Insufficient staff time allocated for a particular activity or type of patient group
Local equipment access or assessment procedures
A local requirement to conduct aspects of the study out of hours (e.g. limited availability of equipment)
As the costs are based on specific time allocations rather than approximate financial estimates, any necessary negotiations should be easier to agree. The network recommended that any cost adjustments proposed are supported with sufficient justification to enable an informed decision for agreement. This will mean that negotiations will be focused on the activity requirements and the justification enables an informed decision to be made.
How long does the CRN review take?
The target timelines for the costing template review by the Local CRN is a maximum of three (3) working days 3 days. This is a ‘quality’ check for completion using the protocol schedule of events to ensure all necessary procedures are included in the template. The purpose is to identify any potential multi-site issues with the costing template so they can be addressed once, before each site begins local cost negotiation and ultimate save time and resource.
How long should sites take to review the costs?
As the costing agreement (and subsequent contract signature) is linked to the confirmation of local capacity and capability, the sites all work towards a median of 40 days from receipt of the minimum document to site confirmation. A definition of these data points are available on the NIHR website metrics webpage.
What can we do if these timelines aren’t met?
You should contact your Local CRN representative, ideally the Industry Operations Manager, in the first instance for the geographical region in which you are having issues. CRN involvement to identify ways forward is one of our key

responsibilities and a frontline resource for Industry to utilise. The contact details are on our website.
How can I check that all appropriate NHS costs are included?
The Industry Costing Template has been designed to identify every activity associated with an individual study. There is a full breakdown of all costs so you can identify both the direct costs and the final prices of individual activities at each patient visit, as well as the total per patient budget. There should be no hidden costs for either industry or the NHS. A list of the checks performed during the validation review by the Local CRN network are available on the NIHR website costing page which may help to identify all required costs.
How should the costs be referenced in the model agreements or study contract?
The NIHR CRN recommends that the template is at a minimum referenced in Appendix 5: Financial Arrangements of the model agreement or the full version is displayed. The template has been developed to work with the model agreement and the summary tab provides an overview of the costs with specific tables to provide visit cost summaries. This can be copied and pasted into the model agreement appendix. Any key figures required to make the financial arrangements with the site should be pulled out and transposed as needed, especially those that are variable costs e.g. ad hoc assessment costs or out of hours charge rates that may apply. A suggested format agreed by the NIHR CRN Costing Group for this appendix is available on the NIHR website costing page.
4. Formatting and technical issues (primary care template)
Reinstating the macros
Unfortunately there is no easy solution for this to ensure that all formulas and macros are working correctly. The least time consuming way around this is to copy the information into a new template downloaded from the website.
Why can’t I send the file to anyone?
When the costing template is downloaded, the file needs to be renamed before it can be distributed. If this is not done, a warning will appear that it will revert to the original i.e. non populated version from the website and all your inputs will be lost. Best practice is to download the template from the website and rename before inputting your costs.
Corrupted copied files
When lots of sites are involved it is tempting to generate one template and update it each time for a new site. This should not be a problem as long as one master template is used i.e. complete the template and use this to create individual site versions rather than copying each sequential version as this creates errors in the functionality that we are unable to trace to the source for correction.
Run time error on summary tab when
When an initial template is completed, the MFF is selected as ‘Blank – Sites to be determined’. This provides a text value where a numerical one would usually be located. As a result
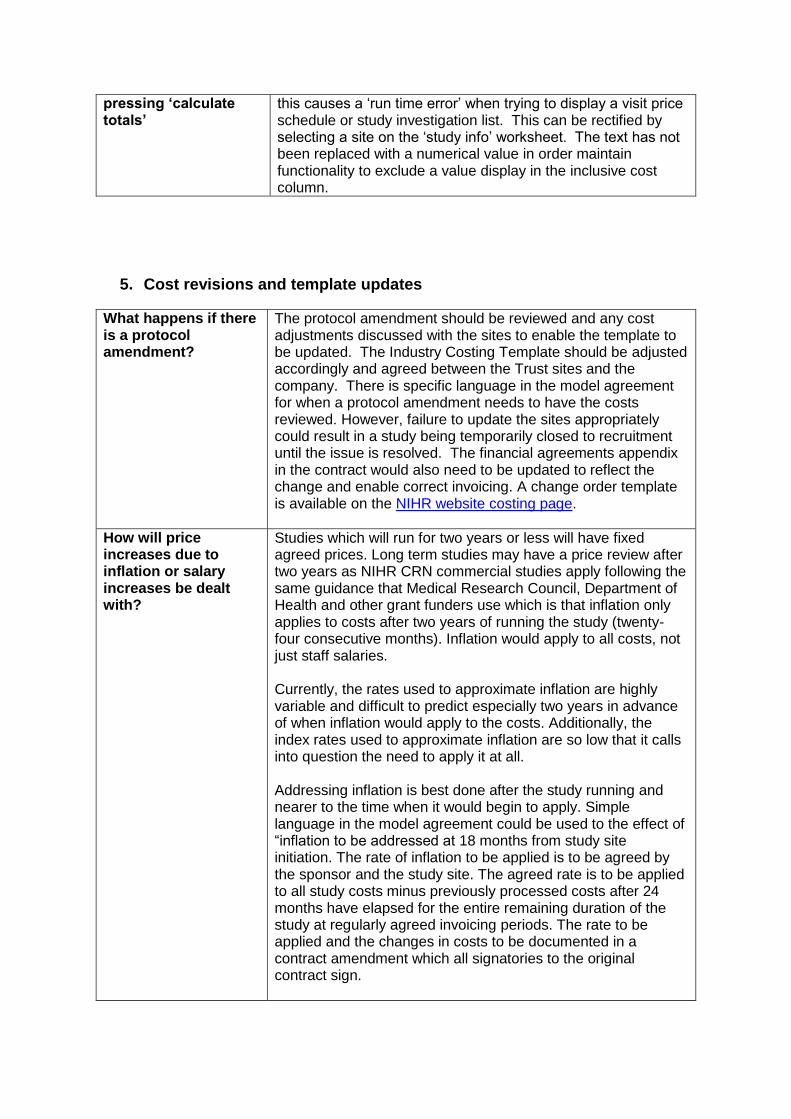
pressing ‘calculate totals’
this causes a ‘run time error’ when trying to display a visit price schedule or study investigation list. This can be rectified by selecting a site on the ‘study info’ worksheet. The text has not been replaced with a numerical value in order maintain functionality to exclude a value display in the inclusive cost column.
5. Cost revisions and template updates
What happens if there is a protocol amendment?
The protocol amendment should be reviewed and any cost adjustments discussed with the sites to enable the template to be updated. The Industry Costing Template should be adjusted accordingly and agreed between the Trust sites and the company. There is specific language in the model agreement for when a protocol amendment needs to have the costs reviewed. However, failure to update the sites appropriately could result in a study being temporarily closed to recruitment until the issue is resolved. The financial agreements appendix in the contract would also need to be updated to reflect the change and enable correct invoicing. A change order template is available on the NIHR website costing page.
How will price increases due to inflation or salary increases be dealt with?
Studies which will run for two years or less will have fixed agreed prices. Long term studies may have a price review after two years as NIHR CRN commercial studies apply following the same guidance that Medical Research Council, Department of Health and other grant funders use which is that inflation only applies to costs after two years of running the study (twenty-four consecutive months). Inflation would apply to all costs, not just staff salaries. Currently, the rates used to approximate inflation are highly variable and difficult to predict especially two years in advance of when inflation would apply to the costs. Additionally, the index rates used to approximate inflation are so low that it calls into question the need to apply it at all. Addressing inflation is best done after the study running and nearer to the time when it would begin to apply. Simple language in the model agreement could be used to the effect of “inflation to be addressed at 18 months from study site initiation. The rate of inflation to be applied is to be agreed by the sponsor and the study site. The agreed rate is to be applied to all study costs minus previously processed costs after 24 months have elapsed for the entire remaining duration of the study at regularly agreed invoicing periods. The rate to be applied and the changes in costs to be documented in a contract amendment which all signatories to the original contract sign.

If you are already approaching the two year window for a study and need to estimate inflation, the standard approach is to use either the Consumer Price Index (CPI), averaged over the last 2-5 years to come up with a rate. This rate is then compound multiplied ([1 + decimal rate] ^ no. of years) to all the costs listed in appendix 5 of the model agreement. The National Office of Statistics is the default authority for CPI rates.
When are the templates updated?
A revised version is released each year in April for use in the new financial year. This version includes any annual updates to the pay rates, MFF and prescription charges as well as consideration of any other adjustments if deemed appropriate.
When should the new template be used?
When a new Template is launched all new studies should use the new template. Any templates which are currently being negotiated should be discussed between the Sponsor and the site to agree whether they wish to update the template prior to contract signature.
Example 1:
10 patients
12 month study
Non standard set-up cost used
Archiving fee agreed upfront on estimate number of boxes
Investigator meeting time charged at hourly rate in template if required
Task
Version 1.6.1
(intended
costs)
Version 1.6.1
(actual costs)
Version 2 (intended
cost) Considerations
Pharmacy £873.24 set-
up
£1,397.18
maintenance
£1,552.43
dispensing
TOTAL:
£3,822.82
£873.24 set-up
£698.59
maintenance
£1,552.43
dispensing
TOTAL:
£3,124.26
£873.24 set-up
£351.50 IMP
management
£1,552.43
dispensing
TOTAL: £2,777.17
Maintenance
fee negotiated
at half time (60
minutes not 120
minutes)
Set-up £700 R&D
TOTAL: £700
plus training
costs
£1000 R&D
£ Initiation and
training at cost
TOTAL: £1000
plus training
costs
£700 R&D
£400
Initiation/Training
£150 Support
Department (Labs)
TOTAL: £1,250
Archiving £ Blank fee £298 £300 Upfront
assumption

made to agree
costs
Example 2:
7 patients
24 month study
Standard set-up cost used
No archiving fee agreed
Investigator meeting time charged at hourly rate in template if required
Task Version 1.6.1
(intended costs)
Version 1.6.1
(actual costs)
Version 2 (intended
cost) Considerations
Pharmacy £873.24 set-up
£2,794.37
maintenance
£5,283.29
dispensing
TOTAL:
£8,950.90
£873.24 set-up
£2,794.37
maintenance
£5,283.29
dispensing
TOTAL:
£8,950.90
£873.24 set-up
£703 IMP
management
£5,283.29
dispensing
TOTAL: £6,859.53
Set-up £700 R&D
£ Initiation and
training at cost
TOTAL: £700
plus training
costs
£1200 R&D
£ Initiation and
training at cost
£180 Support
Department labs
set-up
£500 Radiology
set-up fee
TOTAL: £1,880
plus training
costs
£700 R&D
£400
Initiation/Training
£150 Support
Department labs set-
up
£150 Radiology set-
up fee
TOTAL: £1,400
Set-up fees for
support
departments are
inconsistently
charged and
variable in value
Archiving £ Blank fee £ Not agreed £300 Upfront
assumption
made to agree
costs
11. Abbreviations
Term Definition
ABPI Association of the British Pharmaceutical Industry

Term Definition
AUKUH Association of UK Universities and Hospitals
BMA British Medical Association
CCG Central Commissioning Group
CPI Consumer Price Index
CRN Clinical Research Network
CRO Contract Research Organisation
ECG Electrocardiogram
FAQ Frequently Asked Questions
FEC full Economic Costs
GP General Practitioner
HRA Health Research Authority
HSG Health Service Guidelines
IMP Investigational Medicinal Product
IVR/IWR Interactive Voice Recognition/ Interactive Web Recognition
IRAS Integrated Research Application System
LCRN Local Clinical Research Network
MMF Market Forces Factor
NHS National Health Service
NIMP Non-Investigational Medicinal Product
NPCTAG National Pharmacy Clinical Trials Advisory Group
NIHR National Institute for Health Research
R&D Research and Development