use of pharmacoeconomics in prescribing research part 3 cea a technique for decision making the...
TRANSCRIPT

8/10/2019 Use of Pharmacoeconomics in Prescribing Research Part 3 CEA a Technique for Decision Making the Margin (MITH…
http://slidepdf.com/reader/full/use-of-pharmacoeconomics-in-prescribing-research-part-3-cea-a-technique-for 1/7
RESEARCH NOTE
Use of pharmacoeconomics in prescribing research.Part 3: cost-effectiveness analysis – a techniquefor decision-making at the margin
R. Lopert* BSc BMed MMedSc, D. L. Lang BMath BEc PostgradDipHlthEcEv
and S. R. Hill BMed PhD FAFPHM
*Pharmaceutical Benefits Branch, Department of Health and Ageing, Canberra, ACT, Australia and
Discipline of Clinical Pharmacology, Faculty of Health, University of Newcastle, NSW, Australia
SU M M A RY
This is the third Research Note addressing phar-
macoeconomics in prescribing research, reflecting
the increasing use of economic evaluation in drug
purchasing decisions in a variety of settings. Inthis segment we provide an overview of the the-
oretical basis, practical application and meth-
odological limitations of cost-effectiveness
analysis (CEA).
Keywords: allocative efficiency, cost-effective-
ness analysis, economic evaluation, opportunity
cost, pharmacoeconomics, technical efficiency
INT RODU CT ION
Economics is fundamentally about optimizing the
distribution of limited resources – making choices,
recognizing opportunity costs and maximizing
efficiency. Choosing to direct resources to (i.e.spend money on) a particular health care inter-
vention means that other interventions may need to
be modified, delayed or even abandoned. In max-
imizing efficiency the benefit to be derived from
the expenditure decision should exceed the benefit
to be gained by any alternative (1). Although eco-
nomic evaluation is an aid to making rational
decisions in health care, it cannot be regarded as a
panacea for making difficult choices. Other factors
apart from efficiency, such as access to drugs,
clinical need and who benefits will also influence
resource allocation decisions.
The term cost-effectiveness analysis (CEA) is often
used generically to refer to all forms of economic
evaluation, but is in fact only one of several tech-
niques that may be applied to the evaluation of the
benefits and costs of drugs and other health tech-
nologies. Other techniques of economic evaluation –
cost benefit analysis (CBA), cost minimization
analysis (CMA) and cost utility analysis (CUA) –
may also be applied in the context of drug selection
(hence pharmacoeconomic evaluation) to help make
explicit the costs and consequences of resourceallocation decisions. These are discussed in other
articles in this series.
The various techniques all share a common,
overarching objective – to relate the outcomes of
health care interventions to the costs associated
with their use. Where they differ is in the way in
which the outcomes are measured and valued, and
Box 1.
Key message box
Cost-effectiveness analysis is a technique to aid
decision-making at the margin.
Cost-effectiveness analysis is most readily applicable toquestions of technical efficiency – questions of
allocative efficiency can only be addressed where
there is a common outcome measure.
Difficulties of interpretation can occur when
cost-effectiveness ratios are presented in terms of
surrogate or intermediate endpoints.
Series Editor: Paramjit Gill, University of Birmingham
Received 27 November 2002, Accepted 3 January 2003
Correspondence: Dr Ruth Lopert, Pharmaceutical Benefits
Branch, Department of Health and Ageing, Canberra ACT,
Australia. Tel.: +612 6289 4111; fax: +612 8289 8633; e-mail:
Journal of Clinical Pharmacy and Therapeutics (2003) 28, 243–249
2003 Blackwell Publishing Ltd 243

8/10/2019 Use of Pharmacoeconomics in Prescribing Research Part 3 CEA a Technique for Decision Making the Margin (MITH…
http://slidepdf.com/reader/full/use-of-pharmacoeconomics-in-prescribing-research-part-3-cea-a-technique-for 2/7
whether the resource allocation issue in question is
one of allocative efficiency or technical efficiency (2).
Allocative efficiency is concerned with whether to
allocate scarce resources to a programme or whe-
ther to allocate more or less resources to it. Allocative
efficiency addresses the mix and type of services
that maximize the health gain of a society. Tech-
nical efficiency is concerned with how best to deliver
a programme or to achieve a given objective in
circumstances where a decision has already been
made to allocate resources for a new or existing
programme (Table 1).
Where the expected health benefits of two drugs
(or other health technologies) are similar, then
attention may be focused on the comparative costs
in order to identify the least cost option. This
technique – CMA – was described in a previous
article in this series [Newby D and Hill S (2003) Use
of pharmacoeconomics in prescribing research.Part 2: cost minimization analysis – when are two
therapies equal? Journal of Clinical Pharmacy and
Therapeutics 28, 145–150]. If, however, the outcomes
are not expected to be the same, then both costs and
consequences of alternative options need to be
considered. CEA, CBA and CUA are all techniques
that enable us to do this (Table 2).
W HA T IS CEA ?
Generally speaking CEA is a technique that is most
appropriately applied when a choice must be made
between two or more competing options for which
the expected health gains can be expressed in terms
of a common outcome measure. CEA has been
described as a technique for making decisions at the
margin, in situations where the question may be
framed as, ‘Is it worth spending an additional $x or
£y to achieve the additional benefits offered by the
new drug compared to existing therapy?’ It istherefore primarily a technique for addressing
Table 1. Questions of efficiency and economic evaluation technique
Efficiency Example Appropriate technique
Allocative efficiency Cox-2 inhibitors for arthritis vs. HmG-CoA reductase inhibitors
(‘statins’) for prevention of coronary heart disease
Cost benefit analysis
Cost utility analysis
Technical efficiency Cox-2 inhibitors vs. NSAIDs for the management
of rheumatoid arthritis
Cost minimization analysis
(if no difference in benefit)
Cost-effectiveness analysis
Cox-2, cyclooxygenase-2; NSAIDS, non-steroidal anti-inflammatory drugs; HmG-CoA, hydroxy-methyl-glutaryl coenzyme.
Table 2. Types of economic evaluation
Method Example of an appropriate question Outcomes Measure
Cost minimization
analysis
Of two Cox-2 inhibitor drugs with
equal effectiveness, which is the least expensive?
Equivalent None
Cost effectiveness
analysis
Streptokinase has different costs and effects
to tissue plasminogen activator in thrombolysis
for acute myocardial infarction
What is the incremental cost per life
year gained of SK compared with TPA?
Unidimensional Natural units
(life-years gained)
Cost utility
analysis
A low molecular weight heparin offers survival and
quality of life gains but at a higher cost than
unfractionated heparin in patients with
unstable coronary artery disease.
What is the cost per quality adjusted life year gained
of therapy with LMWH compared with UFH?
Multidimensional Health index
(quality adjusted
life years – QALYs)
Cost benefit
analysis
What is the ratio of cost to benefit for SK vs. LMWH? Multidimensional Commensurate
($, 2, ¥)
2003 Blackwell Publishing Ltd, Journal of Clinical Pharmacy and Therapeutics, 28 , 243–249
244 R. Lopert et al.
8/10/2019 Use of Pharmacoeconomics in Prescribing Research Part 3 CEA a Technique for Decision Making the Margin (MITH…
http://slidepdf.com/reader/full/use-of-pharmacoeconomics-in-prescribing-research-part-3-cea-a-technique-for 3/7
questions of technical efficiency (how best to deliver a
programme or to achieve a given objective).
SOM E DEF INIT IONS ( A ND F ORM U LA E)
To appreciate the role of CEA within economic
evaluation more generally, some definitions are
helpful. First, a cost-effectiveness ratio (CER) is a
method of calculating the cost per unit of benefit of
a drug or other therapeutic intervention. It is the
ratio of the resources used per unit of benefit of the
drug or intervention in question and implies that
the calculation has been made relative to ‘no
treatment’ – although no treatment usually has
costs and effects that should be taken into account
in the CEA (3). This ratio, when calculated relative
to no treatment, is sometimes referred to as an
‘average’ or ‘absolute’ CER:
Average CER ¼ CostA=EffectA
However, an average CER calculated in isolation
may be of limited usefulness. In most cases we are
interested in establishing the net cost-effectiveness of
an intervention – its costs and health outcomes,
compared with some alternative, such as the treat-
ment most likely to be replaced by the intervention.
A marginal CER refers to the change in costs and
health benefits from a one-unit expansion or con-
traction of service from a particular health care
intervention (2).
Marginal CER ¼ CostnA Costð
n
1Þ
AEffectnA Effectðn1ÞA
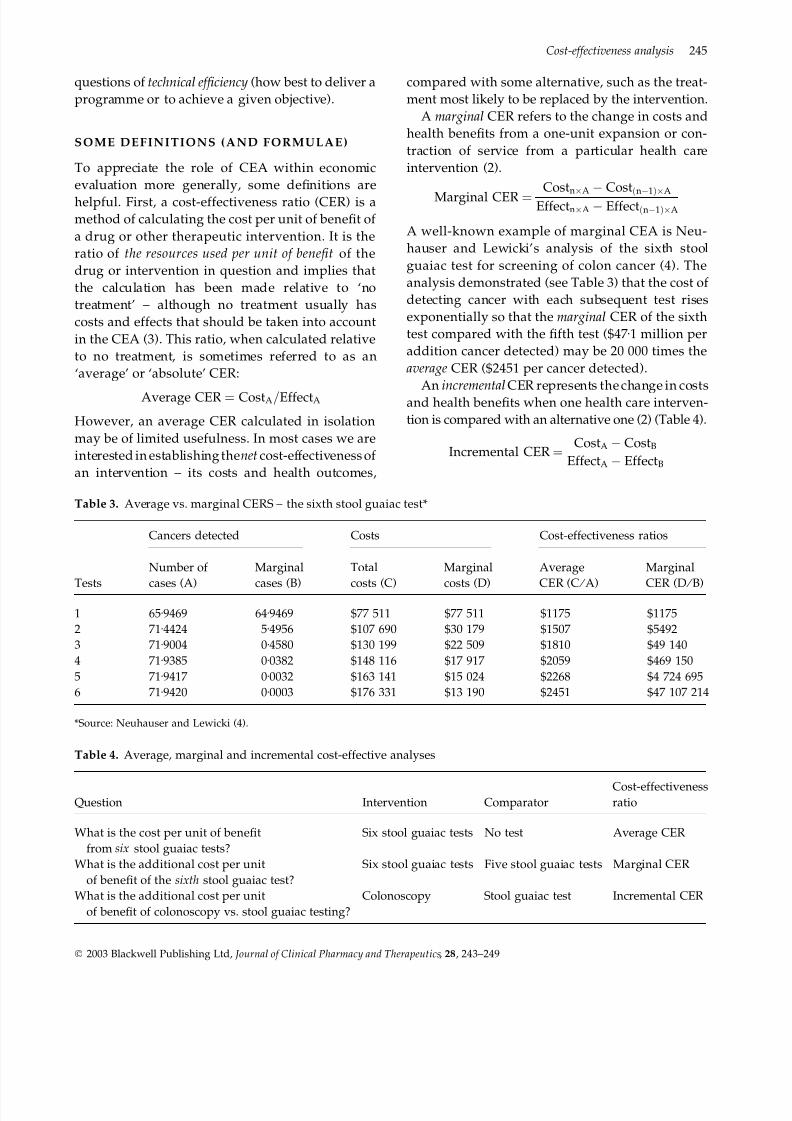
A well-known example of marginal CEA is Neu-
hauser and Lewicki’s analysis of the sixth stool
guaiac test for screening of colon cancer (4). The
analysis demonstrated (see Table 3) that the cost of
detecting cancer with each subsequent test rises
exponentially so that the marginal CER of the sixth
test compared with the fifth test ($47Æ1 million per
addition cancer detected) may be 20 000 times the
average CER ($2451 per cancer detected).
An incremental CER represents the change in costsand health benefits when one health care interven-
tion is compared with an alternative one (2) (Table 4).
Incremental CER ¼ CostA CostB
EffectA EffectB
Table 3. Average vs. marginal CERS – the sixth stool guaiac test*
Tests
Cancers detected Costs Cost-effectiveness ratios
Number of
cases (A)
Marginal
cases (B)
Total
costs (C)
Marginal
costs (D)
Average
CER (C ⁄
A)
Marginal
CER (D ⁄
B)
1 65Æ9469 64Æ9469 $77 511 $77 511 $1175 $1175
2 71Æ4424 5Æ4956 $107 690 $30 179 $1507 $5492
3 71Æ9004 0Æ4580 $130 199 $22 509 $1810 $49 140
4 71Æ9385 0Æ0382 $148 116 $17 917 $2059 $469 150
5 71Æ9417 0Æ0032 $163 141 $15 024 $2268 $4 724 695
6 71Æ9420 0Æ0003 $176 331 $13 190 $2451 $47 107 214
*Source: Neuhauser and Lewicki (4).
Table 4. Average, marginal and incremental cost-effective analyses
Question Intervention ComparatorCost-effectivenessratio
What is the cost per unit of benefit
from six stool guaiac tests?
Six stool guaiac tests No test Average CER
What is the additional cost per unit
of benefit of the sixth stool guaiac test?
Six stool guaiac tests Five stool guaiac tests Marginal CER
What is the additional cost per unit
of benefit of colonoscopy vs. stool guaiac testing?
Colonoscopy Stool guaiac test Incremental CER
2003 Blackwell Publishing Ltd, Journal of Clinical Pharmacy and Therapeutics, 28, 243–249
Cost-effectiveness analysis 245
8/10/2019 Use of Pharmacoeconomics in Prescribing Research Part 3 CEA a Technique for Decision Making the Margin (MITH…
http://slidepdf.com/reader/full/use-of-pharmacoeconomics-in-prescribing-research-part-3-cea-a-technique-for 4/7
If drug A is clearly superior to drug B and costs
less, then the decision is relatively straightforward.
In this case, drug A is said to be dominant over drug
B. If drug A offers less benefit at greater cost then the
choice is again straightforward – why pay more if
you expect to derive less benefit? If drug A offers
additional benefit at a higher cost then our calcu-
lation of an incremental cost-effectiveness ratio
(ICER) comes into play. The question is then: Are
the extra benefits to be gained from using this drug
worth the additional costs? This involves a difficult
value judgement; what is an acceptable CER for
one person, or in one setting or at one time, may be
unacceptable in another (3). In order to attempt to
answer this question we calculate the ICER – a
means of expressing the additional cost (or
expenditure required) to deliver each incremental
unit of benefit (Table 5).
COM PONENT S OF A CEA
Several guidelines exist for reviewing a published
or submitted CEA, or for preparing your own (2, 5,
6). The key components of a CEA are summarized
below.
Context
A description of the intervention, the population
and setting in which it is to be used, and the
appropriate comparator should be identified and
justified. The population in the CEA may be
identified by, for example, age, gender and ⁄ or
clinical history (6). The description of the setting
may include the location and type of institution
(hospital or primary care) (6). Appropriate com-
parators for the CEA may be the most cost-
effective alternative currently available, or the
therapy most likely to be replaced by the new
intervention (5). For a new drug, this may be a
drug in the same therapeutic class, a drug
belonging to a different therapeutic class or a non-
drug therapy where this represents standard
medical management of the condition in question
(7). The choice of an appropriate comparator is
critical in CEA (8). The nomination of an expen-
sive comparator may make the new intervention
appear more cost-effective than it should, leading
to an underestimate of the true opportunity costof its adoption.
Evidence of comparative efficacy
It is important to include the search strategies and
inclusion criteria used to identify studies that pro-
vide evidence of treatment efficacy for incorpor-
ation into the CEA, and to consider the design and
evidentiary quality that these studies represent (9).
The results (together with appropriate confidence
intervals for the estimates of effect) should be
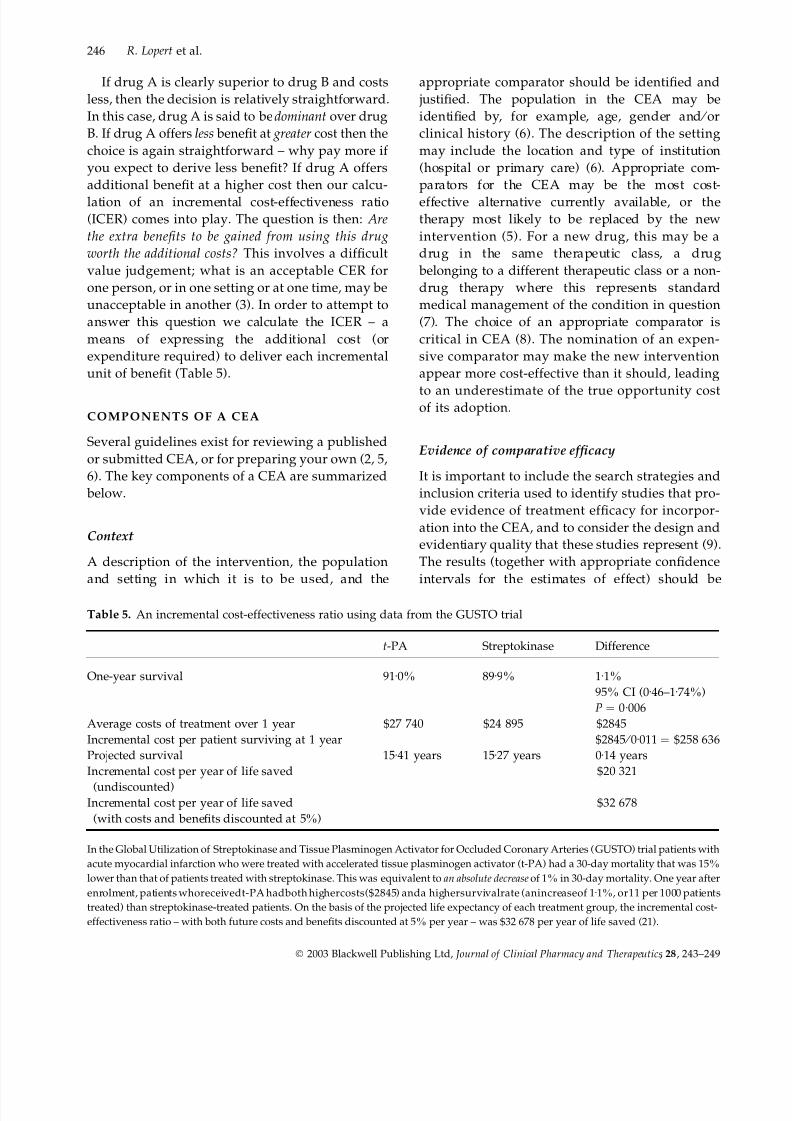
Table 5. An incremental cost-effectiveness ratio using data from the GUSTO trial
t-PA Streptokinase Difference
One-year survival 91Æ0% 89Æ9% 1Æ1%
95% CI (0Æ46–1Æ74%)
P ¼ 0Æ006
Average costs of treatment over 1 year $27 740 $24 895 $2845
Incremental cost per patient surviving at 1 year $2845 ⁄ 0Æ011 ¼ $258 636
Projected survival 15Æ41 years 15Æ27 years 0Æ14 years
Incremental cost per year of life saved
(undiscounted)
$20 321
Incremental cost per year of life saved
(with costs and benefits discounted at 5%)
$32 678
In the Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries (GUSTO) trial patients with
acute myocardial infarction who were treated with accelerated tissue plasminogen activator (t-PA) had a 30-day mortality that was 15%
lower than that of patients treated with streptokinase. This was equivalent to an absolute decrease of 1% in 30-day mortality. One year after
enrolment, patients whoreceivedt-PA hadboth highercosts($2845) anda highersurvivalrate (anincreaseof 1Æ1%, or11 per 1000 patients
treated) than streptokinase-treated patients. On the basis of the projected life expectancy of each treatment group, the incremental cost-
effectiveness ratio – with both future costs and benefits discounted at 5% per year – was $32 678 per year of life saved (21).
2003 Blackwell Publishing Ltd, Journal of Clinical Pharmacy and Therapeutics, 28 , 243–249
246 R. Lopert et al.

8/10/2019 Use of Pharmacoeconomics in Prescribing Research Part 3 CEA a Technique for Decision Making the Margin (MITH…
http://slidepdf.com/reader/full/use-of-pharmacoeconomics-in-prescribing-research-part-3-cea-a-technique-for 5/7
presented clearly. In calculating any incremental
CER, we are interested in the absolute difference in
benefit (EffectA – EffectB) of the interventions being
compared. This will be given by the absolute risk
difference for binary outcomes and the difference in
mean values for continuous data (Table 6).
The cost-effectiveness of a treatment will vary
with the degree of benefit that treatment offers. Thegreater the degree of benefit for a given cost,
the more cost-effective an intervention will be. The
degree of benefit offered by an intervention will in
turn depend on the baseline risk; those at higher
risk of an event have greater capacity to benefit
from treatment. To illustrate this point consider the
cost-effectiveness of ‘statin’ treatment of hyper-
cholesterolaemia. Pharoah and Hollingworth (10)
estimated the average cost-effectiveness of statin
therapy ranged from £15 000 to £70 000 in men
with pre-existing coronary heart disease. For men
without coronary heart disease, average cost-
effectiveness ranged from £70 000 to £424 000 (10).
Costs
For the numerator of the CER, we are interested
in the relevant differences in costs between the
two treatments under consideration (CostA –
CostB). There are three steps in determining the
costs: identification, measurement and valuation.
The perspective of the analysis determines the
range of costs to be included (identification). Thesocietal perspective is the most comprehensive
perspective, but often more limited perspectives
(patient, health care programme, government, or
other third party payer) are adopted. The num-
ber of units consumed (measurement) of each
resource for the intervention and its comparator
should be totalled and the unit costs for each
resource (valuation) identified separately. The
currency and year of the unit cost data should
also be provided in the report of the CEA, and
the sources of data on resource used and unit
costs. A comprehensive review of identifying,
measuring and valuing costs in CEA, is the
subject of the first paper in the series (11).
Resource utilization data for incorporation into
CEAs are increasingly being collected prospec-tively in clinical trials. This raises the issues of trial
design, in particular whether sample size calcula-
tions should take into account the requirements of
the economic and the clinical evaluation (12). There
is as yet no consensus on the correct method for the
calculation of an appropriate sample size or
determining the power of a trial of a given size if
economic endpoints are to be taken into account
(13, 14).
Appropriate time horizon ⁄ discounting
The analysis should state clearly the timespan or
time horizon of the CEA, and this should cover the
time period over which the health benefits and
resource utilization will accrue. When costs and
benefits extend over a number of years, discount-
ing should be used to reflect the fact that values
from today’s perspective depend on when costs are
incurred and benefits accrue (11). Typical discount
rates range from 3 to 6%. The effect of using dis-
count rates may be explored in sensitivity analyses.
Incremental analysis
The results of the incremental or marginal CEA
should be provided in both disaggregated and
aggregated form. That is, the costs and benefits of
each alternative should be presented, along with
the incremental costs and incremental benefits, and
the incremental CER.
Table 6. Unfractionated heparin vs. low molecular weight heparin
Outcome
Low molecular
weight heparin
Unfractionated
heparin Relative risk
Absolute risk
difference
Combined risk of death,
AMI or unstable angina
318 ⁄ 1607 (19Æ8%) 364 ⁄ 1564 (23Æ3%) 19Æ8% ⁄ 23Æ3% ¼ 0Æ85 23Æ3 ) 19Æ8% ¼ 3Æ5%
Source: Cohen et al. (22).
AMI, acute myocardial infarction.
2003 Blackwell Publishing Ltd, Journal of Clinical Pharmacy and Therapeutics, 28, 243–249
Cost-effectiveness analysis 247

8/10/2019 Use of Pharmacoeconomics in Prescribing Research Part 3 CEA a Technique for Decision Making the Margin (MITH…
http://slidepdf.com/reader/full/use-of-pharmacoeconomics-in-prescribing-research-part-3-cea-a-technique-for 6/7
The interpretation of incremental CERs can be
difficult. Clinical trials often measure and report
surrogate or short-term endpoint data rather than
results measured against major clinical endpoints
such as death, survival, disability or cure. A sur-
rogate endpoint is a laboratory measure or disease
marker which is relatively easily measured and
which is thought to predict the clinically relevant
outcome(s) of a therapeutic intervention (15, 16).
The use of surrogate endpoints can considerably
reduce the sample size, duration, and cost of clin-
ical trials, and can allow treatments to be assessed
in situations where the use of clinical endpoints
might be considered excessively invasive or
unethical (15).
Where outcomes are presented in terms of
surrogate or intermediate endpoints, the results
of CEAs may be difficult to interpret. Even where
a surrogate endpoint is considered to be well-validated, the interpretation of its value may yet
be difficult. How, for example, should we inter-
pret an incremental cost per additional mm of Hg
of systolic blood pressure lowered, or per 1%
reduction in HbA1c? Furthermore a difference in
treatment effect demonstrated within a clinical
trial may be statistically significant, and may be
achievable at a modest increment in cost, but
may not necessarily be clinically meaningful or
worthwhile.
Even where a CEA presents results in terms of
clinically meaningful endpoints, the decision may
not be straightforward. CEA is highly context
dependent. An ICER of £10 000 per death averted,
for example, may seem reasonable in developed
country setting, but it nevertheless implies an
underlying judgement as to the value of avoiding a
death within the context in which the analysis takes
place.
Sensitivity analyses
It is important when considering estimates of cost-effectiveness to determine the sensitivity of the
estimates to variations in both costs and treatment
effects. At a minimum, CERs should be varied
around the confidence interval of the point esti-
mate of treatment effect. For each sensitivity ana-
lysis, the choice of variables to be varied, and the
range over which each variable is varied, should be
provided, with justification.
In recent years, considerable effort has been
expended in developing methods for addressing
uncertainty in CEA. This has encompassed meth-
ods for estimating confidence intervals for CERs,
and other, broader approaches to analysing
uncertainty in CEA (17, 18).
Financial implications
The adoption of a therapy with even a modest
ICER may involve expenditure which exceeds a
given budget (and is therefore unaffordable) or
which precludes expenditure within other pro-
grammes. It is therefore important, when con-
ducting CEAs, to also include the financial
implications of the introduction of the new drug or
other health care intervention.
LIM IT A T IONS OF CEA
Cost-effectiveness analysis is the most frequently
used economic evaluation technique; it is concep-
tually straightforward, perhaps deceptively so.
CERs are generally simple to calculate and are
often expressed in terms of outcomes routinely
collected in clinical trials (19).
Cost-effectiveness analysis nevertheless has a
number of limitations. As has already been noted,
it may useful in determining expenditure priorities
for different treatments for the same condition
(technical efficiency) but it is much less easily
applied to decisions involving treatments for dif-
ferent diseases. Comparisons are not possible be-
tween programmes (or even within the same
programme) where there is no common metric. We
cannot compute comparative cost-effectiveness for
an antihypertensive therapy and an asthma medi-
cation where the treatment effects are reported in
terms of reduction in blood pressure in the first
instance and percentage increase in forced expira-
tory volume (FEV1) for the second.
Even where it is possible to measure and incor-porate final clinical outcomes such as life years
gained, or deaths averted, into the assessment of
cost-effectiveness we are still left with a unidi-
mensional measure that cannot combine reductions
in morbidity or improvement in quality of life with
survival gains into a single index, which is neces-
sary if we are to be able to compare treatments that
vary on both dimensions. In order to incorporate
2003 Blackwell Publishing Ltd, Journal of Clinical Pharmacy and Therapeutics, 28 , 243–249
248 R. Lopert et al.

8/10/2019 Use of Pharmacoeconomics in Prescribing Research Part 3 CEA a Technique for Decision Making the Margin (MITH…
http://slidepdf.com/reader/full/use-of-pharmacoeconomics-in-prescribing-research-part-3-cea-a-technique-for 7/7
this multidimensionality the more appropriate
technique is CUA (20). CUA takes into account not
just the number of years (survival) gained but the
quality of life of those years. CUA can be used to
assess technical efficiency but also allocative effi-
ciency within the health care sector. The technique
is discussed in more detail in Part 4 of this series.
REF ERENCES
1. Gafni A (1996) Economic evaluation of health care
interventions: an economist’s perspective. ACP Jour-
nal of Club, 124, A12.
2. Drummond MF, Stoddart GL, O’Brien BJ, Torrance
GW (1997) Methods for the Economic Evaluation of
Health Care Programmes. Oxford: Oxford University
Press.
3. Petitti D (2000) Meta-analysis, decision analysis and cost
effectiveness analysis. Methods for quantitative synthesis
in medicine, 2nd edn. Oxford: Oxford UniversityPress.
4. Neuhauser D, Lewicki AM (1975) What do we gain
from the sixth stool guaiac? NEJM, 293, 226–228.
5. Drummond MF, Jefferson TO (1996) Guidelines for
authors and peer reviewers of economic submissions
to the BMJ. British Medical Journal, 313, 275–283.
6. Gold MR, Siegel JE, Russell LB et al. (1996) Cost-ef-
fectiveness in health and medicine. New York: Oxford
University Press.
7. Commonwealth Department of Health and Ageing.
(2002) Guidelines for the Pharmaceutical Industry on
Preparation of Submissions to the Pharmaceutical
Benefits Advisory Committee: including major submis-
sions involving economic analyses. Available at http://
www.health.gov.au/pbs/pubs/pharmpac/gusubpac.htm
[Accessed November 30th 2002].
8. Palmer S, Raftery J (1999) Opportunity cost. BMJ ,
318, 1551–1552.
9. Landray MJ, Whitlock G (2002) Evaluating treatment
effects reliably. BMJ , 325, 1373–1374.
10. Pharoah PDP, Hollingworth W (1996) Cost effect-
iveness of lowering cholesterol concentration with
statins in patients with and without pre-existing
coronary heart disease: life table method applied to
health authority population. BMJ , 312, 1443–1448.
11. Robertson J, Lang DL, Hill S (2003) Use of pharma-
coeconomics in prescribing research. Part 1: Costs –
Moving beyond the acquisition price for drugs. J Clin
Pharmacy and Therapeutics, 28, 73–79.
12. Backhouse ME (2002) Use of Randomised Controlled
Trials for Producing Cost-Effectiveness Evidence:Potential Impact of Design Choices on Sample Size
and Study Duration. Pharmacoeconomics, 20, 1061–
1077.
13. Briggs A (2000) Economic evaluation and clinical
trials: size matters. BMJ , 321, 1362–1363.
14. Briggs AH, Gray AM (1998) Sample size and power
calculations for stochastic cost-effectiveness analysis.
Medical Decision Making, 18(Suppl.) , S81–S92.
15. Fleming TR (1994) Surrogate markers in AIDS and
cancer trials. Statistics in Medicine, 13, 1423–1435.
16. Food and Drug Administration Modernization Act
(1997). S11Z: Expediting Study and Approval of Fast
Track Drugs.
17. Briggs AH, Gray AM (1999) Handling uncertainty in
economic evaluations of healthcare interventions.
BMJ , 319, 635–638.
18. Stinnett AA, Mullahy J (1998) Net health benefits: a
new framework for the analysis of uncertainty in
cost effectiveness analysis. Medical Decision Making,
18(Suppl.) , S68–S80).
19. Oliver A, Healey A, Donaldson C (2002) Choosing
the method to match the perspective: economic
assessment and its implications for health-services
efficiency. Lancet, 359, 1771–1774.
20. Robinson R (1993) What does it mean? Economicevaluation and health care, Part 1. BMJ , 307, 670–674.
21. Mark DB, Hlatky M, Califf RM et al. (1995) Cost
effectiveness of thrombolytic therapy with Tissue
Plasminogen Activator as compared with streptok-
inase for acute myocardial infarction. NEJM, 332(21) ,
1418–1424.
22. Cohen M, Demers C, Gurfinkel EP et al. (1997) A
comparison of low-molecular-weight heparin with
unfractionated heparin for unstable coronary artery
disease. NEJM, 337(7) , 447–452.
Cost-effectiveness analysis 249
2003 Blackwell Publishing Ltd, Journal of Clinical Pharmacy and Therapeutics, 28, 243–249