use of adhd medication during pregnancy from 1999 to 2010: a danish register-based study
TRANSCRIPT
ORIGINAL REPORT
Use of ADHD medication during pregnancy from 1999 to 2010:a Danish register-based study
Katia Buch Hærvig, Laust Hvas Mortensen, Anne Vinkel Hansen and Katrine Strandberg-Larsen*
Section of Social Medicine, Department of Public Health, University of Copenhagen, Copenhagen K, Denmark
ABSTRACTObjective This study aimed to describe the trends in use of Attention Deficit Hyperactivity Disorders (ADHD) medication during preg-nancy in Denmark from 1999 to 2010, as well as to explore characteristics of women who use ADHD medication during pregnancy andwhether exposure is associated with outcome of pregnancy.Method A linkage between various Danish national health registries was performed to identify all recorded pregnancies from 1999 to2010. Use of ADHD medication was defined as a redeemed prescription on methylphenidate, modafinil, or atomoxetine from 28 days priorto the first day of the last menstrual period until the end of pregnancy.Results Of the 1 054 494 registered pregnancies, 480 were exposed to ADHD medication. From 2003 to the first quarter of 2010, use ofADHD medication during pregnancy increased from 5 to 533 per 100 000 person-years. A similar increase was observed among Danishwomen of childbearing age. Compared with unexposed, women who used ADHD medication during pregnancy were more often younger,single, lower educated, received social security benefits, and used other psychopharmaca. Exposed pregnancies were more likely to result ininduced abortions on maternal request (odds ratio = 4.70, 95%CI = 3.77–5.85), induced abortions on special indication (odds ratio = 2.99,95%CI = 1.34–6.67), and miscarriage (odds ratio = 2.07, 95%CI = 1.51–2.84) compared with unexposed pregnancies.Conclusions The number of pregnancies exposed to ADHD medication has increased similarly to the increase in use of ADHD medicationamong women of childbearing age. Use of ADHD medication in pregnancy was associated with different indicators of maternaldisadvantage and with increased risk of induced abortion and miscarriage. Copyright © 2014 John Wiley & Sons, Ltd.
key words—pregnancy; pregnancy outcome; attention deficit/hyperactivity disorder; ADHD; psychostimulants; ADHD medication;pharmacoepidemiology
Received 25 June 2013; Revised 22 January 2014; Accepted 23 January 2014
INTRODUCTION
During the last decade, there has been a notableincrease in the number of adults treated with ADHDmedication.1–3 As cohorts of girls treated for ADHDduring childhood reach an age where they becomesexually active, the number of pregnancies exposedto ADHD medication will likely increase, and this isperhaps particularly true for pregnancies that areunplanned.4 The safety of use during pregnancy isunknown, and all kinds of ADHD medication aretherefore contraindicated in pregnancy.5
First trimester exposure to methylphenidate, whichis the most common type of ADHD medication, was
not associated with increased risk of congenitalmalformations in a recently published review.4 Never-theless, it still seems plausible that exposure to ADHDmedication during pregnancy may be detrimental, asthe pharmacological actions of ADHD medicationare similar to those of amphetamine and cocaine,6,7
both of which are known to be detrimental to thefetus.8 Animal studies show that amphetamines aretransferred across the placenta, but there is nosupporting data on humans concerning ADHDmedication.9 It is thus important to monitor the useof ADHD medication during pregnancy.We describe the trends in use of ADHD medication
during pregnancy in Denmark from 1999 to 2010.Moreover, we explore characteristics of women whouse ADHD medication during pregnancy and whetherexposure to ADHD medication is associated withoutcome of pregnancy.
*Correspondence to: Katrine Strandberg-Larsen, Section of Social Medicine,Department of Public Health, University of Copenhagen, Øster Farimagsgade5, DK-1014 Copenhagen K, Denmark. E-mail: [email protected]
Copyright © 2014 John Wiley & Sons, Ltd.
pharmacoepidemiology and drug safety 2014; 23: 526–533Published online 4 March 2014 in Wiley Online Library (wileyonlinelibrary.com) DOI: 10.1002/pds.3600

METHOD
For the period of interest, we identified all pregnanciesending in either a live birth or stillbirth registered inthe Medical Birth Registry, miscarriage or pregnancytermination registered in the National Patient Registryor the Register of Legal Induced Abortions. All ofthese registries have nationwide and universal cover-age. We identified a total of 1 054 494 pregnanciesstarting later than 1 April 1998 and ending before 31December 2010, as these pregnancies were at risk ofbeing exposed to ADHD medication between 1999to the first quarter of 2010. In Denmark, we have acivil registration system tracking all persons aliveand living in Denmark using a unique personalidentification number that is assigned to every Danishcitizen at time of birth or when getting permanentresidency.10 The personal identification number forevery women registered with a pregnancy was usedto link information from, for example, the NationalPrescription Registry,11 the Psychiatric CentralResearch Registry,12 and Statistics Denmark.
Exposure to ADHD medication during pregnancy
The exposure of interest was redeemed prescription ofADHD medication from 28 days before the first day ofthe last menstrual period (LMP), estimated from thegestational age recorded in the National PatientRegistry, until the end of pregnancy. The NationalPrescription Registry contains information of all pre-scriptions dispensed for Danish residents at outpatientpharmacies from 1995 and onwards. The prescriptionsare recorded according to the Anatomic TherapeuticChemical (ATC) classification system by the WorldHealth Organization.13 We defined ADHD medicationas the following chemical substances: methylpheni-date (ATC-code: N06BA04), modafinil (ATC-code:N06BA07), and atomoxetin (ATC-code: N06BA09).
Demographic characteristics
Data on demographic characteristics were identifiedthrough Statistics Denmark. Maternal age at time ofconception was calculated by subtracting the day ofconception, defined as LMP plus 14 days, from thewoman’s day of birth. The maternal age was catego-rized as follows: <18, 18–24, 25–29, 30–34, 35–39,and >40. Civil status was categorized as follows:married or in a registered relationship, single, anddivorced/widow. The very low number of widowedwomen and none among the pregnancies exposed toADHD medication did not allow us to distinguishbetween divorced and widowed women. Ethnicity
was defined as country of origin of the pregnantwoman’s mother. When we were unable to identifythe mother in the registries, ethnicity was defined fromthe woman’s own country of origin. Ethnicity wasdivided into the following: native born, western originand non-western origin.14 Different regions ofDenmark were defined by the municipal code andcategorized into the following: the Capital Region,Zealand, Central Denmark, Southern Denmark, andNorthern Denmark.2 Data on educational level,occupational status, and personal income wereobtained from the same year as the estimated LMP.Educational level was defined as the last terminatedor currently ongoing education categorized into thefollowing: primary/lower secondary school, uppersecondary school, vocational, and bachelor/master orhigher education. Data on occupational status werecategorized as belonging to one of the followinggroups: a student, receiver of social security benefits,early retired, part of the workforce, and others. Thewoman’s own annual disposable income was dividedinto quintiles. The division was carried out by yearto allow for inflation and changes in income levels.
Other characteristics
Parous was categorized as never given birth before andgiven birth one or more times before: 0 and 1+. Birthsincluded both live births and stillbirths. Information onpreviously induced abortions was obtained from theNational Patient Registry and the Register of LegalInduced Abortions. This included both inducedabortions on maternal request and induced abortionson special indication. Data on redeemed prescriptionsof anxiety medication (ATC-code: N05B) and SelectiveSerotonin Reuptake Inhibitor (SSRI) (ATC-code:N06AB) were identified through the National Prescrip-tion Registry. Use of these medications was defined asone or more redeemed prescriptions from 28 days beforeLMP to end of pregnancy. Moreover, information onADHD diagnosis, given any time before LMP, wasderived from the Psychiatric Central Research Registryand divided into the following categories: yes and no.Patients are only registered in the Psychiatric CentralResearch Registry when psychiatric hospitals or depart-ments are involved. Patients only in contact with generalpractitioners are thus not recorded in the register.
Outcome of pregnancy and congenital malformations
Information on outcome of pregnancy was obtainedfrom the Medical Birth Registry, the National PatientRegistry, and the Register of Legal Induced Abortions.The outcome was categorized as induced abortion on
use of adhd medication during pregnancy 527
Copyright © 2014 John Wiley & Sons, Ltd. Pharmacoepidemiology and Drug Safety, 2014; 23: 526–533DOI: 10.1002/pds

maternal request (<12 completed week), inducedabortion on special indication (≥12 completed weeks),miscarriage (fetal loss <22 completed weeks), still-birth (fetal loss ≥22 completed weeks), and live birth(child with any signs of life ≥22 completed week).In Denmark, it is legal and covered by the universalhealth care system to request an abortion before 12completed weeks of gestation. Terminating a preg-nancy in week 12 or later requires medical or serioussocial circumstances.15 Multiple gestation pregnancies(n= 16 432) were handled as one observation, bywhich only one outcome was possible. In case amultiple gestation pregnancy resulted in both livebirths and stillbirths (n= 71), it was counted as a livebirth. Congenital malformations in the child weredefined as any Q-diagnosis on live-born singletons inthe National Patient Registry within the first 12monthsof the infant’s life.
Data analysis
The incidence rate of use of ADHD medication duringpregnancy was estimated as the number of pregnan-cies, in which a prescription was redeemed, dividedby the sum of times at risk in weeks, in each calendaryear. The women were at risk from 28 days beforeLMP until the woman’s first redemption of a prescrip-tion of ADHD medication or end of pregnancy, which-ever occurred first. To have the annualized incidenceper person-year at risk, we multiplied by 52.2, as aweek is 1/52.2 of a year. The incidence rate wascompared with the incidence rate of redeemed pre-scription on any ADHD medication (ATC-code:N06BA) among Danish women of childbearing age(15–19 and 20–39 years old). These estimates werederived from a public resource provided by theDanish Health and Medicine Authority and estimatedas the number of women redeeming a prescription onany ADHD medication per 100 000 person-years.16
Thus, this estimate also includes pregnant women.Simple crosstabs and logistic regression models wereused to compare the characteristics of pregnanciesexposed to ADHD medication with unexposedpregnancies. To avoid confounding from potentialdifferences in the age distribution age-adjusted oddsratios were estimated. The association between useof ADHD medication and outcome of pregnancywas estimated in a logistic regression model. Thisanalysis was conducted on the whole study popula-tion and restricted to women with an ADHD diagno-sis. In the restricted study population, we were onlyable to estimate odds of induced abortion on maternalrequest and miscarriage. A separate analysis on live-
born singletons surviving the first year of life wasperformed, to examine the prevalence of congenitalmalformations diagnosed within the first 12months ofthe infants’ life. This analysis was restricted to pregnan-cies ending before the first quarter of 2009 to be able tofollow the infant in the first 12months of the infants’life. Analyses were adjusted for the following potentialconfounders: ethnicity, age, and region. To adjust fordependence between pregnancies of the same woman,robust standard error estimates were calculated in allanalysis. Finally, we conducted a case-crossover analy-sis, where we compared exposed pregnancies tounexposed pregnancies of the same woman. The case-crossover analysis is feasible because many womenexperience more than one pregnancy, but they may nothave the same exposure to ADHD medication in allpregnancies. Using this method is similar to matchingall maternal characteristics that are unchanged frompregnancy to pregnancy (e.g., genes, early life expo-sures, and early onset chronic diseases).17 We usedconditional logistic regression for the cases-crossoveranalysis. Few women in our data contributed with bothADHD exposed and unexposed pregnancies, and thuswe only estimated odds ratios for induced abortion onmaternal request and miscarriage in the case-crossoveranalysis.
RESULTS
Of the 1 054 494 registered pregnancies, a total of 480were exposed to ADHD medication. Methylphenidate(81.88%) was the most common type of ADHDmedication used during pregnancy followed byatomoxetin (9.38%) and modafinil (8.75%). Thewomen who used ADHD medication were aged 14to 47 years old and redeemed between 1 and 26prescriptions during pregnancy, though only ninewomen redeemed more than 10 prescriptions. Themedian time between the redeemed prescriptions were1.8weeks. Redeemed prescriptions of, for example,methylphenidate on average covered 20 defined dailydoses, and one defined daily dose of methylphenidateis 30mg; that is, prescriptions of methylphenidateon average is equivalent to 600mg.13 Only 150(29.70%) of the exposed pregnancies had been incontact with a psychiatric hospital or department andthereby had an ADHD diagnosis in the PsychiatricCentral Research Registry.
Incidence
The incidence of use of ADHD medication duringpregnancy was very low and stable from 1999 to
k. b. hærvig et al.528
Copyright © 2014 John Wiley & Sons, Ltd. Pharmacoepidemiology and Drug Safety, 2014; 23: 526–533DOI: 10.1002/pds

2002. Between 2003 and the first quarter of 2010, theincidence of pregnancies exposed to ADHDmedicationincreased from 5 to 533 per 100 000 person-years. Thissubstantial increase was also observed among Danishwomen of childbearing age, especially among womenbelow 20years (Figure 1). From the first quarter 2009to the first quarter 2010, the incidence of pregnanciesexposed to ADHD medication increased with 48%.During the same period, a similar increase was foundamong Danish women of childbearing age; thus, the in-crease was 28% for women aged 15–19years and 38%for women aged 20–39 years.16
Characteristics
Women using ADHD medication during pregnancywere more often young, single, and had not givenbirth before. However, having experienced a previouspregnancy resulting in an induced abortion onmaternal request and/or an induced abortion onspecial indication was associated with use of ADHDmedication in a subsequent pregnancy. A large partof the women who used ADHD medication duringpregnancy had only finished or were currentlyenrolled in primary/lower secondary school or uppersecondary school, were receiving social securitybenefits, and had a low annual income. Furthermore,women who used ADHD medication were morecommonly native born and lived in Central Denmark.Compared with unexposed women, women who used
ADHD medication during pregnancy were morelikely to use anxiety medicine and SSRI. Whenadjusted for age, the same tendencies in the character-istics were found (Table 1).
Outcome of pregnancy
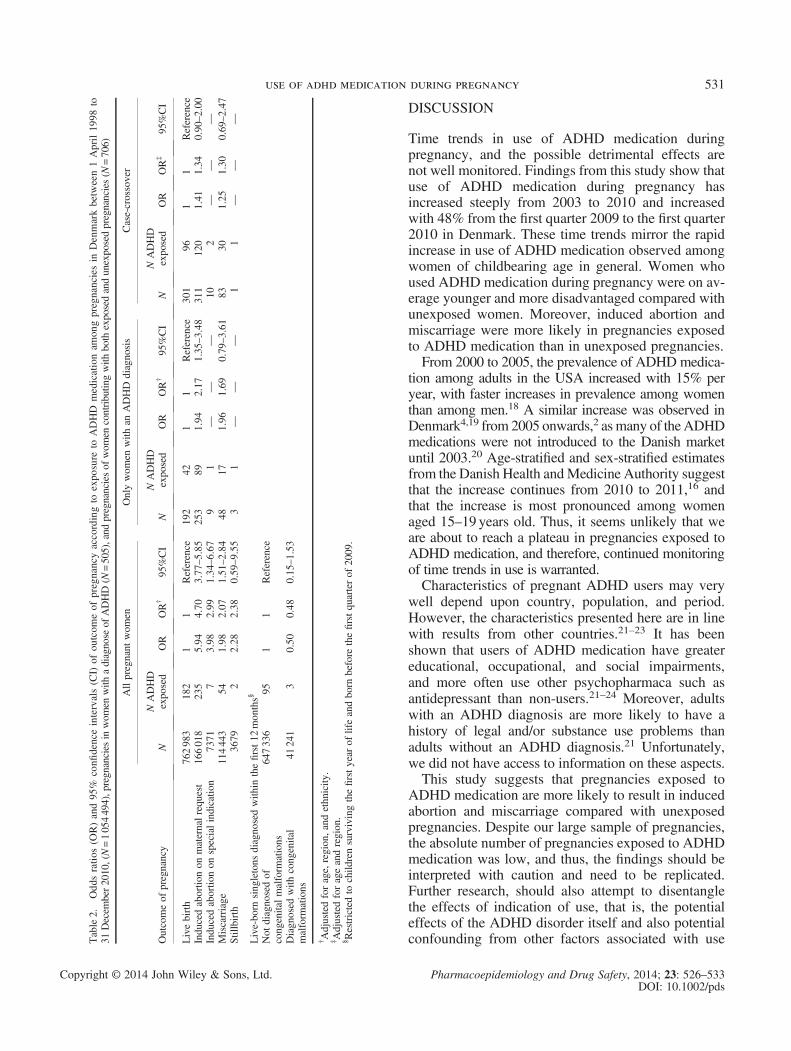
The associations between exposure to ADHDmedicationduring pregnancy and outcome of pregnancy are shownin Table 2. Induced abortions on maternal request andinduced abortions on special indication were morefrequent in pregnancies exposed to ADHD medicationduring pregnancy compared with unexposed pregnan-cies. Moreover, miscarriage was more likely among theexposed pregnancies odds ratio (OR)=2.07, 95% confi-dence interval (CI) = (1.51–2.84) than in unexposed preg-nancies. Among women with an ADHD diagnosis,induced abortion on maternal request (OR=2.17, 95%CI=1.35–3.48) and miscarriage (OR=1.69, 95%CI=0.79–3.61) occurred more frequent in the pregnanciesexposed to ADHDmedication comparedwith unexposedpregnancies. The case-crossover analysis indicated thatinduced abortion on maternal request (OR=1.34, 95%CI=0.90–2.00) and miscarriage (OR=1.30, 95%CI=0.69–2.47) was not more likely to occur in pregnanciesexposed to ADHD medication than in otherpregnancies of the same woman. Only three pregnanciesexposed to ADHD medication resulted in a child with acongenital malformation within the first year of life(prevalence of 3.1%, 95%CI=0.6%–8.7%), and thesedata did not support any association between use ofADHD medication during pregnancy and congenitalmalformations (Table 2). Among all included pregnan-cies, the prevalence of congenital malformation was6.4% with a 95%CI=6.3–6.4%.
Figure 1. Incidence rate of women redeeming a prescription on ADHD medications from 1999 to 2010. The incidence rate is shown per 100 000 person-years.Data on women of childbearing age is drawn from MEDSTAT†.16 *We only have the incidence rate for the first quarter of 2010 among pregnant women.
†MEDSTAT includes all types of medication within the ATC-group N06BA;thus, dexo-amphetamine (ATC-code: N06BA02) and amphetamine (ATC-code: N06BA01) were also included. Note that the population of pregnantwomen is nested within these statistics.
use of adhd medication during pregnancy 529
Copyright © 2014 John Wiley & Sons, Ltd. Pharmacoepidemiology and Drug Safety, 2014; 23: 526–533DOI: 10.1002/pds
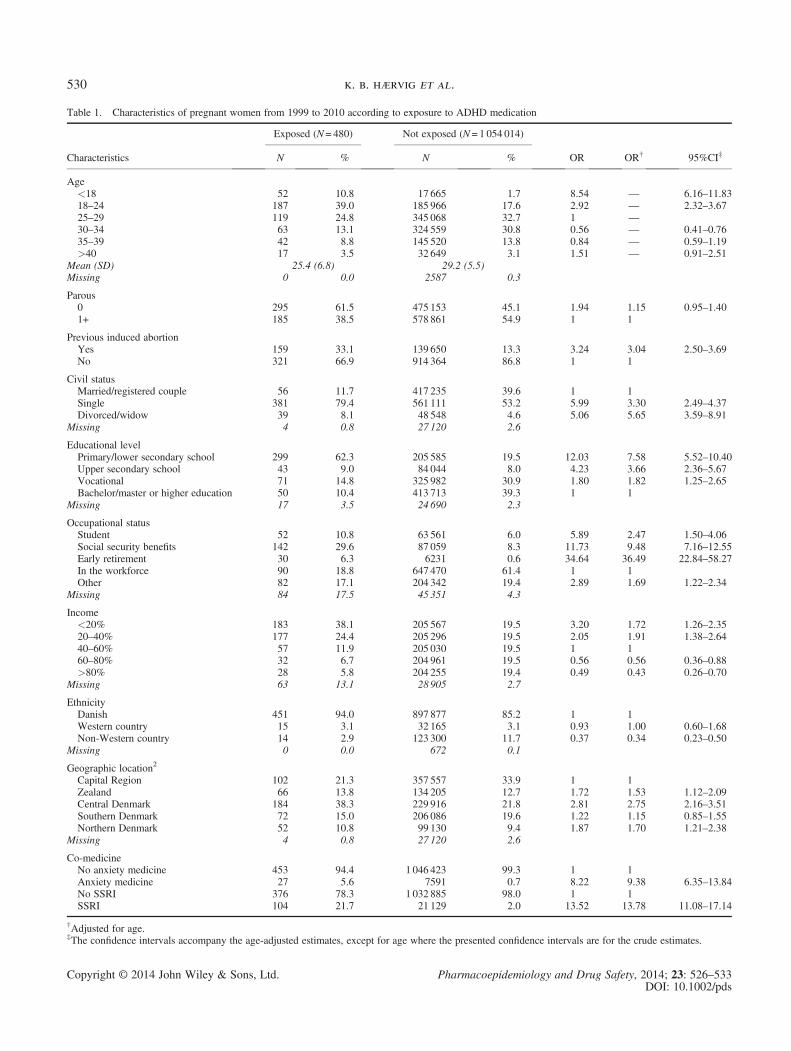
Table 1. Characteristics of pregnant women from 1999 to 2010 according to exposure to ADHD medication
Exposed (N= 480) Not exposed (N= 1 054 014)
Characteristics N % N % OR OR† 95%CI‡
Age<18 52 10.8 17 665 1.7 8.54 — 6.16–11.8318–24 187 39.0 185 966 17.6 2.92 — 2.32–3.6725–29 119 24.8 345 068 32.7 1 —30–34 63 13.1 324 559 30.8 0.56 — 0.41–0.7635–39 42 8.8 145 520 13.8 0.84 — 0.59–1.19>40 17 3.5 32 649 3.1 1.51 — 0.91–2.51
Mean (SD) 25.4 (6.8) 29.2 (5.5)Missing 0 0.0 2587 0.3
Parous0 295 61.5 475 153 45.1 1.94 1.15 0.95–1.401+ 185 38.5 578 861 54.9 1 1
Previous induced abortionYes 159 33.1 139 650 13.3 3.24 3.04 2.50–3.69No 321 66.9 914 364 86.8 1 1
Civil statusMarried/registered couple 56 11.7 417 235 39.6 1 1Single 381 79.4 561 111 53.2 5.99 3.30 2.49–4.37Divorced/widow 39 8.1 48 548 4.6 5.06 5.65 3.59–8.91
Missing 4 0.8 27 120 2.6
Educational levelPrimary/lower secondary school 299 62.3 205 585 19.5 12.03 7.58 5.52–10.40Upper secondary school 43 9.0 84 044 8.0 4.23 3.66 2.36–5.67Vocational 71 14.8 325 982 30.9 1.80 1.82 1.25–2.65Bachelor/master or higher education 50 10.4 413 713 39.3 1 1
Missing 17 3.5 24 690 2.3
Occupational statusStudent 52 10.8 63 561 6.0 5.89 2.47 1.50–4.06Social security benefits 142 29.6 87 059 8.3 11.73 9.48 7.16–12.55Early retirement 30 6.3 6231 0.6 34.64 36.49 22.84–58.27In the workforce 90 18.8 647 470 61.4 1 1Other 82 17.1 204 342 19.4 2.89 1.69 1.22–2.34
Missing 84 17.5 45 351 4.3
Income<20% 183 38.1 205 567 19.5 3.20 1.72 1.26–2.3520–40% 177 24.4 205 296 19.5 2.05 1.91 1.38–2.6440–60% 57 11.9 205 030 19.5 1 160–80% 32 6.7 204 961 19.5 0.56 0.56 0.36–0.88>80% 28 5.8 204 255 19.4 0.49 0.43 0.26–0.70
Missing 63 13.1 28 905 2.7
EthnicityDanish 451 94.0 897 877 85.2 1 1Western country 15 3.1 32 165 3.1 0.93 1.00 0.60–1.68Non-Western country 14 2.9 123 300 11.7 0.37 0.34 0.23–0.50
Missing 0 0.0 672 0.1
Geographic location2
Capital Region 102 21.3 357 557 33.9 1 1Zealand 66 13.8 134 205 12.7 1.72 1.53 1.12–2.09Central Denmark 184 38.3 229 916 21.8 2.81 2.75 2.16–3.51Southern Denmark 72 15.0 206 086 19.6 1.22 1.15 0.85–1.55Northern Denmark 52 10.8 99 130 9.4 1.87 1.70 1.21–2.38
Missing 4 0.8 27 120 2.6
Co-medicineNo anxiety medicine 453 94.4 1 046 423 99.3 1 1Anxiety medicine 27 5.6 7591 0.7 8.22 9.38 6.35–13.84No SSRI 376 78.3 1 032 885 98.0 1 1SSRI 104 21.7 21 129 2.0 13.52 13.78 11.08–17.14
†Adjusted for age.‡The confidence intervals accompany the age-adjusted estimates, except for age where the presented confidence intervals are for the crude estimates.
k. b. hærvig et al.530
Copyright © 2014 John Wiley & Sons, Ltd. Pharmacoepidemiology and Drug Safety, 2014; 23: 526–533DOI: 10.1002/pds
DISCUSSION
Time trends in use of ADHD medication duringpregnancy, and the possible detrimental effects arenot well monitored. Findings from this study show thatuse of ADHD medication during pregnancy hasincreased steeply from 2003 to 2010 and increasedwith 48% from the first quarter 2009 to the first quarter2010 in Denmark. These time trends mirror the rapidincrease in use of ADHD medication observed amongwomen of childbearing age in general. Women whoused ADHD medication during pregnancy were on av-erage younger and more disadvantaged compared withunexposed women. Moreover, induced abortion andmiscarriage were more likely in pregnancies exposedto ADHD medication than in unexposed pregnancies.From 2000 to 2005, the prevalence of ADHDmedica-
tion among adults in the USA increased with 15% peryear, with faster increases in prevalence among womenthan among men.18 A similar increase was observed inDenmark4,19 from 2005 onwards,2 as many of theADHDmedications were not introduced to the Danish marketuntil 2003.20 Age-stratified and sex-stratified estimatesfrom the Danish Health andMedicine Authority suggestthat the increase continues from 2010 to 2011,16 andthat the increase is most pronounced among womenaged 15–19 years old. Thus, it seems unlikely that weare about to reach a plateau in pregnancies exposed toADHD medication, and therefore, continued monitoringof time trends in use is warranted.Characteristics of pregnant ADHD users may very
well depend upon country, population, and period.However, the characteristics presented here are in linewith results from other countries.21–23 It has beenshown that users of ADHD medication have greatereducational, occupational, and social impairments,and more often use other psychopharmaca such asantidepressant than non-users.21–24 Moreover, adultswith an ADHD diagnosis are more likely to have ahistory of legal and/or substance use problems thanadults without an ADHD diagnosis.21 Unfortunately,we did not have access to information on these aspects.This study suggests that pregnancies exposed to
ADHD medication are more likely to result in inducedabortion and miscarriage compared with unexposedpregnancies. Despite our large sample of pregnancies,the absolute number of pregnancies exposed to ADHDmedication was low, and thus, the findings should beinterpreted with caution and need to be replicated.Further research, should also attempt to disentanglethe effects of indication of use, that is, the potentialeffects of the ADHD disorder itself and also potentialconfounding from other factors associated with useT
able2.
Odd
sratios
(OR)and95
%confi
denceintervals(C
I)of
outcom
eof
pregnancyaccordingto
expo
sure
toADHD
medicationam
ongpregnanciesin
Denmarkbetw
een1April19
98to
31Decem
ber2010,(N=1054494),pregnancies
inwom
enwith
adiagnose
ofADHD(N
=505),and
pregnanciesof
wom
encontributin
gwith
both
exposedandunexposedpregnancies(N
=706)
Outcomeof
pregnancy
Allpregnant
wom
enOnlywom
enwith
anADHD
diagnosis
Case-crossover
NNADHD
exposed
OR
OR†
95%CI
NNADHD
exposed
OR
OR†
95%CI
NNADHD
exposed
OR
OR‡
95%CI
Livebirth
762983
182
11
Reference
192
421
1Reference
301
961
1Reference
Inducedabortio
non
maternalrequest
166018
235
5.94
4.70
3.77
–5.85
253
891.94
2.17
1.35–3.48
311
120
1.41
1.34
0.90–2.00
Inducedabortio
non
specialindicatio
n7371
73.98
2.99
1.34
–6.67
91
——
—10
2—
——
Miscarriage
114443
541.98
2.07
1.51
–2.84
4817
1.96
1.69
0.79–3.61
8330
1.25
1.30
0.69–2.47
Stillbirth
3679
22.28
2.38
0.59
–9.55
31
——
—1
1—
——
Live-born
singletons
diagnosedwith
inthefirst12
months§
Not
diagnosedof
congenitalmalform
ations
647336
951
1Reference
Diagnosed
with
congenital
malform
ations
41241
30.50
0.48
0.15
–1.53
†Adjustedforage,region,and
ethnicity
.‡Adjustedforageandregion.
§Restrictedto
child
rensurvivingthefirstyear
oflifeandborn
before
thefirstquarterof
2009.
use of adhd medication during pregnancy 531
Copyright © 2014 John Wiley & Sons, Ltd. Pharmacoepidemiology and Drug Safety, 2014; 23: 526–533DOI: 10.1002/pds
of ADHD medication. The analyses on women with anADHD diagnosis and the case-crossover analysessuggested that the apparent risk of induced abortion onmaternal request and miscarriage conferred by ADHDmedication may, at least to some extent, be attributableto the ADHD user rather than the medication itself.However, few pregnancies contributed to these analyses,and the findings should be interpreted with caution. Like-wise, our findings on congenital malformations are basedon very few cases, and even though it does not supportan association, it adds very little to the sparse quantityof data on the potential association between prenatalexposure to ADHDmedication and the risk of congenitalmalformations.4 The higher frequency of induced abor-tion on maternal request among pregnancies exposed toADHD medication may reflect a higher frequency ofunwanted pregnancies and thereby implies that womenusing ADHD medication need more information oncontraceptive methods.However, there are some limitations in this study.
One limitation is that our measure of use of ADHDmedication is based on redeemed prescriptions, butwe do not know if the women actually ingested theredeemed medication. This issue has been the subjectof much debate and has been handled differently indifferent studies. We chose the definition we foundto be most indicative of actual use during preg-nancy.25 It is possible that drugs prescribed forchildren under 16 years of age may have been regis-tered as dispensed for their mother, as this was theregistration practice until 1996.11 However, medica-tion prescribed for children should have been regis-tered under the child’s own personal identificationnumber for the period in the present study. Data fromnational registries (as all other data) are prone toregistrations errors, which might be the case for thesingle pregnancy with 26 redeemed prescriptions onADHD medication. Moreover, the Psychiatric CentralResearch Registry does not record all diagnoses ofADHD, as mild to moderate cases are most oftendiagnosed and treated by the general practitioner inDenmark.12 We think that this means that only therelatively severe or comorbid cases of ADHD will havea diagnosis in our study. Finally, our treating of multi-ple gestation pregnancies in our analysis as live birthsin case of resulting in both a live born and stillborncould imply underestimation of stillbirths. However,we only had 71 multiple gestation pregnancies endingin live born and stillborn(s), none among exposed,and changing the outcome definition into stillborninstead of live born had no impact on the conclusions.In conclusion, our findings suggest that use of
ADHD medication during pregnancy has increased
notably since 2003. Furthermore, it seems likely thatit has not reached a plateau yet as the use of ADHDmedication has increased most rapidly among womenaged 15–19 years old, who are only about to enteringtheir childbearing years. Compared with unexposed,women who used ADHD medication during preg-nancy were often younger, single, and more disadvan-taged, even when adjusted for age. Pregnanciesexposed to ADHD medication are more likely to resultin induced abortion and miscarriage than unexposedpregnancies. Whether this is caused by harmful effectsof the medication itself, confounding by indication orfactors associated with use of ADHD medicationremains to be examined.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
KEY POINTS• Between 2003 and the first quarter of 2010, theincidence of pregnancies exposed to ADHDmedication increased from 5 to 533 per 100 000person-years. This substantial increase was alsoobserved among Danish women of childbearingage.
• Women who used ADHD medication duringpregnancy were more often younger, single,lower educated, received social security benefits,and used other psychopharmaca compared withunexposed women.
• Induced abortion on maternal request andinduced abortion on special indication andmiscarriage occurred more frequently in preg-nancies exposed to ADHD medication than inunexposed pregnancies.
ETHICS STATEMENT
The use of data was approved by the Danish DataProtection Agency. Since the study used routineregister data, no ethical approval or informed consentwas acquired.
ACKNOWLEDGEMENTS
This project was supported by the Lundbeck Foundation(grant number R112-A9178). Katrine Strandberg-Larsenwas funded by the Danish Council for IndependentResearch / Medical Sciences (grant number 09-066049).
k. b. hærvig et al.532
Copyright © 2014 John Wiley & Sons, Ltd. Pharmacoepidemiology and Drug Safety, 2014; 23: 526–533DOI: 10.1002/pds
REFERENCES
1. Pottegård A, Bjerregaard BK, Glintborg D, Kortegaard LS, Hallas J, Moreno SI.The use of medication against attention deficit/hyperactivity disorder inDenmark: a drug use study from a patient perspective. Eur J Clin Pharmacol2013; 69(3): 589–598.
2. Pottegård A, Bjerregaard BK, Glintborg D, Hallas J, Moreno SI. The use of med-ication against attention deficit hyperactivity disorder in Denmark: a drug use studyfrom a national perspective. Eur J Clin Pharmacol 2012; 68(10): 1443–1450.
3. Zoëga H, Furu K, Halldórsson M, Thomsen PH, Sourander A, Martikainen JE.Use of ADHD drugs in the Nordic countries: a population-based comparisonstudy. Acta Psychiatr Scand 2011; 123(5): 360–367.
4. Dideriksen D, Pottegård A, Hallas J, Aagaard L, Damkier P. First trimester inutero exposure to methylphenidate. Basic Clin Pharmacol 2013; 112(2): 73–76.
5. Humphreys C, Garcia-Bounissen F, Ito S, Koren G. Motherisk Update Exposureto attention de cit hyperactivity disorder medications during pregnancy. CanFam Physician 2007; 53: 1153–1155.
6. Ashton H, Gallagher P, Moore B. The adult psychiatrist’s dilemma:psychostimulant use in attention deficit/hyperactivity disorder. J Psychopharmacol2006; 20(5): 602–610.
7. Ryan L, Ehrlich S, Finnegan L. Cocaine abuse in pregnancy: effects on the fetusand newborn. Neurotoxicol Teratol 1987; 9(4): 295–299.
8. Sithisarn T, Granger D, Bada H. Consequences of prenatal substance use. Int JAdolesc Med Health 2012; 24(2): 105–112.
9. Bolea-Alamanac BM, Green A, Verma G, Maxwell P, Davies SJC. Methylphe-nidate use in pregnancy and lactation, a systematic review of evidence. Br J ClinPharmacol [Internet] 2013 [cited 2013 Nov 26]; 1–20. Available from: http://www.ncbi.nlm.nih.gov/pubmed/23593966
10. Pedersen CB. The Danish Civil Registration System. Scand J Public Health2011; 39(7 Suppl): 22–25.
11. Kildemoes HW, Sørensen HT, Hallas J. The Danish National PrescriptionRegistry. Scand J Public Health 2011; 39(7 Suppl): 38–41.
12. Mors O, Perto GP, Mortensen PB. The Danish Psychiatric Central ResearchRegister. Scand J Public Health 2011; 39(7 Suppl): 54–57.
13. WHO. WHO Collaboration Centre for Drug Statistics Methodology [Internet].2012 [cited 2013 Apr 23]. Available from: http://www.whocc.no
14. Statistics Denmark. Immigrants and decendants [Indvandre og efterkommere][Internet]. [cited 2013 Mar 11]. Available from: http://www.dst.dk/da/Statistik/emner/indvandrere-og-efterkommere/indvandrere-og-efterkommere.aspx
15. Law. The Danish health law [Internet]. 2010 [cited 2013 Nov 26]. p. 140. Avail-able from: https://www.retsinformation.dk/forms/r0710.aspx?id=130455#K26
16. Center for Disease Control [Statens Serum Institut]. SSI Statistics: medstat.dk[Internet]. 2013 [cited 2013 Mar 14]. Available from: http://medstat.dk/
17. Maclure M, Mittleman M. Should we use a case-crossover design? Annu RevPublic Health 2000; 21: 193–221.
18. Castle L, Aubert RE, Verbrugge RR, Khalid M, Epstein RS. Trends inmedication treatment for ADHD. J Atten Disord 2007; 10(4): 335–342.
19. The National Board of Health [Sundhedsstyrelsen]. The sale of ADHD drugsfrom 2002-2011 in Denmark [Salget af ADHD-medicin fra 2002-2011].2011;1–6. Available from: http://www.ssi.dk/Sundhedsdataogit/Analyser ograpporter/Lagemiddelforbrugsanalyser/2012/~/media/Indhold/DK-dansk/Sundhedsdata og it/NSF/Analyser og rapporter/Laegemiddelforbrugsanalyser/2012/Salget af ADHD medicin fra 2002-2011.ashx
20. Danish Health and Medicines Authority. Registred medicine in Denmark[Internet]. 2012 [cited 2013 Nov 26]. Available from: http://sundhedsstyrelsen.dk/da/medicin/regulering/godkendelse-af-medicin/lister-over-godkendte-og-afregistrerede-laegemidler
21. Mao AR, Babcock T, BramsM.ADHD in adults: current treatment trends with con-sideration of abuse potential of medications. J Psychiatr Pract 2011; 17(4): 241–250.
22. Lensing MB, Zeiner P, Sandvik L, Opjordsmoen S. Four-year outcome inpsychopharmacologically treated adults with attention-deficit/hyperactivitydisorder: a questionnaire survey. J Clin Psychiatry 2013; 74(1): e87–e93.
23. Kessler RC, Adler L, Barkley R, et al. The prevalence and correlates of adultADHD in the United States: results from the National Comorbidity SurveyReplication. Am J Psychiatry 2006; 163(4): 716–723.
24. Lichtenstein P, Halldner L, Zetterqvist J, Sjölander A, et al. Medication forattention deficit-hyperactivity disorder and criminality. N Engl J Med 2012;367(21): 2006–2014.
25. Grzeskowiak LE, Gilbert AL, Morrison JL. Exposed or not exposed? Exploringexposure classification in studies using administrative data to investigateoutcomes following medication use during pregnancy. Eur J Clin Pharmacol2012; 68(5): 459–467.
use of adhd medication during pregnancy 533
Copyright © 2014 John Wiley & Sons, Ltd. Pharmacoepidemiology and Drug Safety, 2014; 23: 526–533DOI: 10.1002/pds