urinary tract infection chishti - uk healthcare cecentral tract infection_chishti.pdf · finding...
TRANSCRIPT
5/15/2012
1
AFTABAFTAB S. CHISHTI, MD., FAAP., CCSTS. CHISHTI, MD., FAAP., CCSTUKUK
Department of PediatricsDepartment of PediatricsDivision of Pediatric Nephrology, Division of Pediatric Nephrology,
Hypertension & Renal TransplantationHypertension & Renal TransplantationUniversity of Kentucky, University of Kentucky, KY Children’s HospitalKY Children’s Hospital
Lexington, KYLexington, KY
•• No Financial conflict of interests to DeclareNo Financial conflict of interests to Declare
Scope, Aims & ObjectivesScope, Aims & Objectives
• Diagnosis of urinary tract infections {UTI}
• Risk Factors for UTI
• Management of UTI
• Post UTI Evaluation
• Imaging strategies
• Antibiotic Prophylaxis
5/15/2012
2
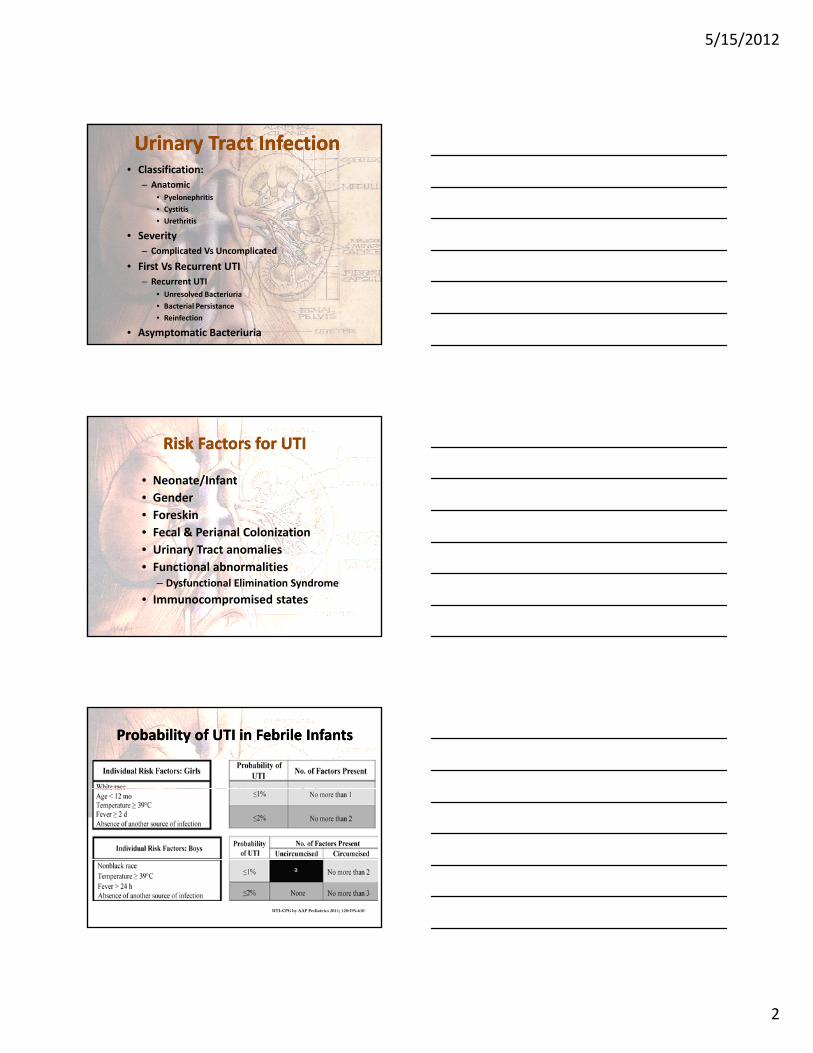
Urinary Tract InfectionUrinary Tract Infection• Classification:
– Anatomic• Pyelonephritis
• Cystitis
• Urethritis
• Severity• Severity
– Complicated Vs Uncomplicated
• First Vs Recurrent UTI
– Recurrent UTI
• Unresolved Bacteriuria
• Bacterial Persistance
• Reinfection
• Asymptomatic Bacteriuria
Risk Factors for UTIRisk Factors for UTI
• Neonate/Infant
• Gender
• Foreskin
• Fecal & Perianal Colonization
• Urinary Tract anomalies
• Functional abnormalities– Dysfunctional Elimination Syndrome
• Immunocompromised states
Probability of UTI in Febrile InfantsProbability of UTI in Febrile Infants
UTI-CPG by AAP Pediatrics 2011; 128:595-610

5/15/2012
3
Common Urinary PathogenCommon Urinary Pathogen• Gm Negative Rods
E coliPseudomonasKlebsiella sppCitrobacterEnterobacter cloacaeMorganella morgagniiProteus MirabilisProteus Mirabilis
• Gm Negative CocciNeisseria gonorrhea
• Gm Positive CocciEnterococcus sppStreptococcus Group B/ Group D/ faecalisStaphlococcus aureus/epidermidis/saprophyticus
• Candida sp.• Adenovirus
Chang SL, Shorliffe LD, Pediatr Clin N Am 53(2006)379-400
Clinical PresentationClinical Presentation
• Based on Age– Birth ‐ 90 days of age– 3 months – 2 years of age– 2 – 5 years of age– More than 5 years of age
• Pertinent Physical findings– Anthropometric measures– Blood Pressure– Genitourinary exam
UTIUTI‐‐SymptomsSymptoms
• Lower Tract
– Frequency
– Urgency
• Upper Tract
– Fever
– Lethargy Urgency
– Wetting
– Gross Hematuria
– Non Specific Abd. Pain
Lethargy
– Vomiting
– Malaise
– Loin Pain
Nonspecific Symptoms more likely in children < 2 years

5/15/2012
4
DiagnosisDiagnosis
• Urinalysis
– Dipstick
– Microscopic Analysis
Enhanced Urinalysis– Enhanced Urinalysis
• Urine Culture
– Catheterized
– Supra‐pubic Aspiration
UrinalysisUrinalysis
Bell et al. Seminars in Nephrology, Vol. 29, No. 4, July 2009. pp 349-359

5/15/2012
5
Urine CultureUrine Culture
Hallerstein S. Pediatric Infectious Disease journal. 1982; 1: 271-81
Sermin A Saadeh, Tej K. Mattoo Pediatr Nephrol (2011) 26: 1967-1976
UTI CPG by AAP Action Statement # 3UTI CPG by AAP Action Statement # 3
• To Establish the diagnosis of UTI clinician should require both
– UA suggestive of infection
• Pyuria &/or BacteriuriaPyuria &/or Bacteriuria
– Urine Culture with > 50000 colony forming units per ml of uropathogen cultured from a urine specimen obtained through Catheterization or Suprapubic aspiration
{Evidence Quality: C; Recommendation}
UTI-CPG by AAP Pediatrics 2011; 128:595-610
Management of UTIManagement of UTI
Avoid Constipation Scheduled VoidingAntibiotics
Si l Simple Broad Spectrum Step down after sensitivities are available Oral Vs Intravenous Avoid Nephrotoxic antibiotoics Duration Prophylaxis

5/15/2012
6
UTI CPG by AAP Action Statement # 4UTI CPG by AAP Action Statement # 4
• 4B
– The Clinician should choose 7‐14 days as duration of antimicrobial therapy
{Evidence Quality: B; Recommendation}{Evidence Quality: B; Recommendation}
Empiric Oral AntibioticsEmpiric Oral Antibiotics
UTI-CPG by AAP Pediatrics 2011; 128:595-610
Empiric Empiric ParenteralParenteral AntibioticsAntibiotics
UTI-CPG by AAP Pediatrics 2011; 128:595-610
5/15/2012
7
Post UTI ImagingPost UTI Imaging
• Renal and Bladder Ultrasound – RBUS
• Voiding Cystouretherogram – VCUGg y g
– Conventional VS Radionuclide
• Dimercaptosuccinic Acid Scan – DMSA Scan
UTI CPG by AAP UTI CPG by AAP Action Statement # 5 & 6Action Statement # 5 & 6
• Febrile Infants with UTIs should undergo Renal & Bladder Ultrasonography (RBUS)
{Evidence Quality: C; Recommendation}• 6A
– VCUG should not be performed after first Febrile UTI; Its indicated if RBUS reveals Hydronephrosis scarring or otherindicated if RBUS reveals Hydronephrosis, scarring, or other finding either suggestive of high grade reflux or obstructive uropathy, as well as in other atypical or complex clinical circumstances.
{Evidence Quality: B; Recommendation}
• 6B– Further Evaluation should be conducted if there is recurrence
of febrile UTIs{Evidence Quality: X; Recommendation}
United Kingdom’s NICE GuidelinesUnited Kingdom’s NICE Guidelines
• All children with atypical UTI need Renal Sonogram in acute stage
• Infant younger than 6 months with first UTI – do sonogram within 6 weeks of infectiong
• Children younger than 3 with atypical or recurrent UTI do DMSA scan 4-6 months after the acute infection to detect scarring
• No routine imaging to detect VURMori R et al BMJ 2007;335:395-397

5/15/2012
8
European GuidelinesEuropean Guidelines
• European Association of Urology/European Society of Pediatric Urology– RBUS – VCUG
• Initial Febrile or Recurrent UTI in girls• Initial Febrile or Recurrent UTI in girls• Initial UTI in Boys
– DMSA• Initial Febrile UTI
• European Society of Pediatric Research– RBUS & DMSA– VCUG only if DMSA positive
European Urology 61(2012) 773-782
ProphylaxProphylax or NOT to or NOT to ProphylaxProphylax
Effect of Prophylaxis on the recurrence of symptomatic UTIEffect of Prophylaxis on the recurrence of symptomatic UTI
Bing et al. Arch Dis Child 2010, 95: 499-508
Prophylaxis or NO ProphylaxisProphylaxis or NO Prophylaxis
Effect of Antibiotic Prophylaxis on repeat positive CulturesEffect of Antibiotic Prophylaxis on repeat positive Cultures
Bing et al. Arch Dis Child 2010, 95: 499-508

5/15/2012
9
Prophylaxis or NO to ProphylaxisProphylaxis or NO to Prophylaxis
The Effect of Antibiotic Prophylaxis on the rate of renal scarsThe Effect of Antibiotic Prophylaxis on the rate of renal scars
Bing et al. Arch Dis Child 2010, 95: 499-508
Relationship between Renal Scarring and Relationship between Renal Scarring and repeated bouts of repeated bouts of PyelonephritisPyelonephritis
Jodal U Infect Dis Clin North Am 1987:1:(4) 713-729
Antibiotic Prophylaxis & Rec. UTIAntibiotic Prophylaxis & Rec. UTI
Time to Symptomatic UTITime to Symptomatic UTI Time to Febrile UTITime to Febrile UTI
19%
13%
Craig JC et al. NEJM 361:18, 1748-59
13%
7%

5/15/2012
10
Antibiotic Prophylaxis in preventing Antibiotic Prophylaxis in preventing APN or ScarAPN or Scar
Marco Pennesi et al. Pediatrics Vol 121, # 6, June 08
Antibiotic Prophylaxis in preventing Antibiotic Prophylaxis in preventing APN or ScarAPN or Scar
Marco Pennesi et al. Pediatrics Vol 121, # 6, June 08
Take Home MessageTake Home Message• High Index of suspicion• Prompt treatment of UTI/Pyelonephritis
– Oral Antibiotics are as good as Intravenous– Rx for 7‐10 days
• Individualize work up post UTI– RUS in almost all with Febrile UTI– VCUG should still be considered
• After second febrile UTI• Atypical UTI
– DMSA still may be helpful but should be done by specialist
• Consider Dysfunctional Elimination • Antibiotic Prophylaxis in high grade reflux patients

5/15/2012
11