upper airways research laboratory department of otorhinolaryngology advanced treatments of nasal...
TRANSCRIPT

Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
Advanced treatments of nasal
polyposis: Anti-IL-5 and Anti-IgE
Which for whom?
Prof. Dr. Philippe Gevaert
Department of Otorhinolaryngology
Ghent University Hospital, Belgium

Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
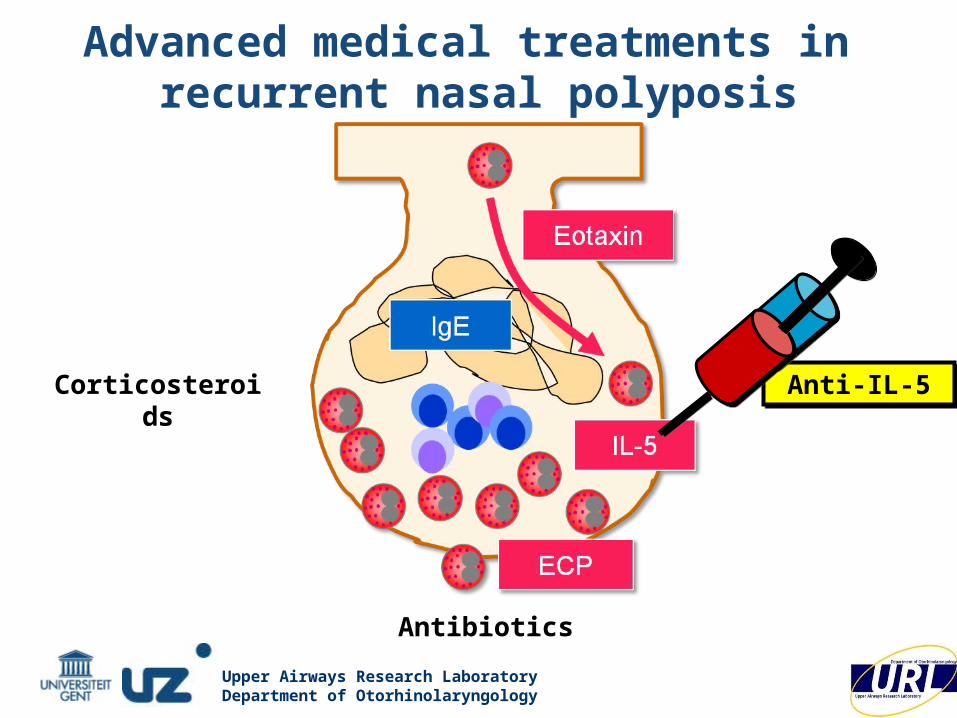
Advanced medical treatments in recurrent nasal polyposis
Surgery = removing
immunological memory

Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
Antibiotics
Anti IL
-5
Anti-IL-5Corticosteroids
IL-5IL-5
ECPECP
EotaxinEotaxin
IgE
Anti IL
-5
Advanced medical treatments in recurrent nasal polyposis

Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
N=354J Allergy Clin Immunol 2005;116:1275-81

Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
Nasal corticosteroid DROPS in nasal polyps
double-blind, placebo-controlled study with nasal GCS dropsAfter 12-weeks: nasal blockage, peak nasal inspiratory flow
polyp volume (CT score) need for sinus surgery
Aukema, Mulder, Fokkens; JACI 2005

Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
Participating centers: ENT Dept: University Hospital Ghent, Belgium, University Hospital St. Rafael Leuven Belgium; University Hospital Erlangen, Germany, Adelaide University Hospital, Australia, Academic Medical Center, Amsterdam, the Netherlands
T Van Zele, Gevaert P (in preparation)
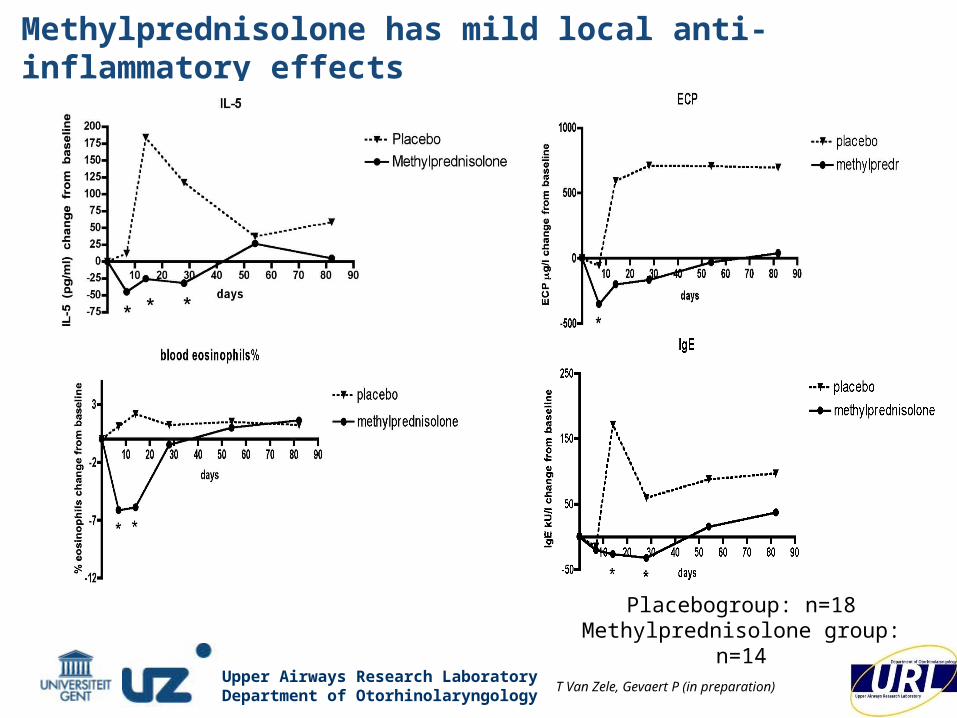
Oral steroids in nasal polyps: a 3-month double blind, randomized, placebo-controlled trialDBPC in 32 patient with nasal polyps, 20days methylprednisolon(Day 1-5 32 mg, day 6-10 16 mg, day 11-20 8 mg)
Primary endpoint: endoscopic scoring with a five grade system
Secoundary endpoints
symptoms
evaluation of local and systemical biological activity and efficacy
measurement of IgE, IL-5 and ECP on nasal secretions (merocell)
measurement of blood eosinophilia
daily measurement of nasal peak inspiratory flow
grade 0 1 2 3 4

Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
Thibaut Van Zele, Philippe Gevaert, Gabriele Holtappels, Achim Beule, Peter John Wormald, Susanne Mayr, Greet Hens, Peter Hellings, Fenna A Ebbens, Paul Van Cauwenberge, Claus Bachert
Oral steroids in nasal polyps: a 3-month double blind, randomized, placebo-controlled trialDBPC in 32 patient with nasal polyps, 20days methylprednisolon(Day 1-5 32 mg, day 6-10 16 mg, day 11-20 8 mg)
Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
Methylprednisolone has mild local anti-inflammatory effects
Placebogroup: n=18Methylprednisolone group:
n=14T Van Zele, Gevaert P (in preparation)

Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
Antibiotics
Anti IL
-5Anti-IL-5Corticosteroids
IL-5
ECP
Eotaxin
IgE
Advanced medical treatments in recurrent nasal polyposis

Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
Long term antibiotic treatment in NP
• DBPC study in 90 patients:
• 3m low-dose erythromycin, nasal douche,
nasal GCS vs. sinus surgery• 50% Improvement of symptoms• no difference vs sinus surgery

Upper Airways Research LaboratoryDepartment of Otorhinolaryngology

Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
* *
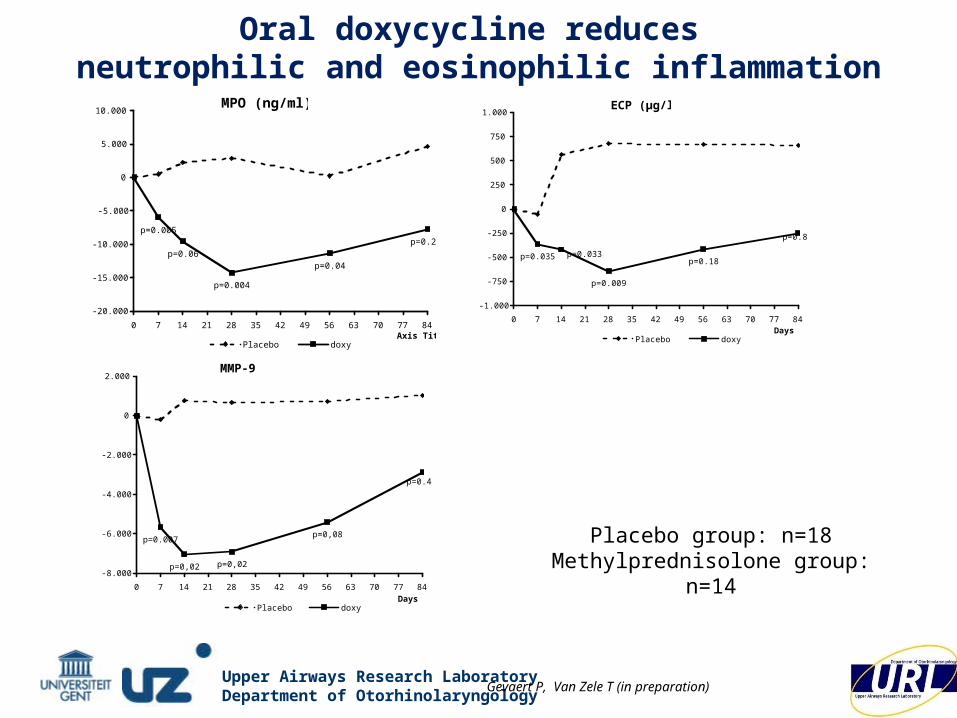
Doxycycline reduces MMP9, ECP, MPO and nasal polyp size, in a double-blind, randomized, placebo controlled, multicenter trial.20 days doxycycline (100mg/d) reduces PND
Philippe Gevaert, Thibaut Van Zele, Gabriele Holtappels, Achim Beule, Peter John Wormald, Susanne Mayr, Greet Hens, Peter Hellings, Fenna A Ebbens, Paul Van Cauwenberge, Claus Bachert
Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
ECP (µg/l)
p=0.035 p=0.033
p=0.009
p=0.18
p=0.8
-1.000
-750
-500
-250
0
250
500
750
1.000
0 7 14 21 28 35 42 49 56 63 70 77 84Days
EC
P (
µg
/l)
in n
asal
secre
tion
Placebo doxy
MPO (ng/ml)
p=0.005
p=0.06
p=0.004
p=0.04
p=0.2
-20.000
-15.000
-10.000
-5.000
0
5.000
10.000
0 7 14 21 28 35 42 49 56 63 70 77 84Axis Title
MP
O (
ng
/ml)
in
nasal
Placebo doxy
MMP-9
p=0.007
p=0,02 p=0,02
p=0,08
p=0.4
-8.000
-6.000
-4.000
-2.000
0
2.000
0 7 14 21 28 35 42 49 56 63 70 77 84Days
MM
P-9
(p
g/m
l) i
n n
asal
secre
tion
s (
Placebo doxy
Placebo group: n=18Methylprednisolone group:
n=14
Oral doxycycline reduces neutrophilic and eosinophilic inflammation
Gevaert P, Van Zele T (in preparation)

Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
First double blind placebo controlled trial with antibiotics in nasal polyps that shows:
a significant effect of doxycycline on nasal polyp sizeDoxycycline reduces local inflammation in terms of ECP and MPO
effect on eosinophilic inflammationeffect on neutrophilic (may be related to the effect on S. aureus)Doxycycline has a sigificant effect on remodeling (MMP-9)
Doxycycline
Gevaert P, Van Zele T (in preparation)

Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
Practical management of Nasal Polyposis• Nasal douche with saline • Nasal corticosteroids
• GCS sprays: 2x/d, symptoms↓, no resolution of NP• GCS drops: symptoms↓, surgery↓↓
• Oral corticoids: effective but fast recurrence• Antibiotics:
• Antibiotic ointment• Long-term antibiotics: macrolides 500mg/d ged 3m
doxycycline 100 mg/d ged 1mCombinations?
• Endoscopic sinus surgery: only chance for cure!!in NP: recurrencesin NP: recurrences

Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
Treatment of nasal polyposis following EP³OS
Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
Antibiotics
Anti IL
-5
Anti-IL-5Anti-IL-5Corticosteroids
Advanced medical treatments in recurrent nasal polyposis

Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
IL-5 and eosinophils in nasal polyposis
ECP
IL-5
IL-5
IL-5
Migration Homing
Survival
Activation
Maturation
Differentiation
Recruitement
IL5 + Eotaxin

Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
ECP
IL-5
IL-5
IL-5
Migration Homing
Survival
Activation
Maturation
Differentiation
Recruitement
IL5 + Eotaxin
Anti-interleukin 5 in nasal polyposis
Anti IL-5
xx x

Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
Objective and study design
30 SubjectsSevere nasal polyps
20 Subjects
10 Subjects
Weeks 0 1 4 128
*
MEPO 750mg IVPlacebo
Dosing
Follow up
* Primary endpoint
24 36 48

Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
EndpointsPrimary endpoint
• Endoscopic Nasal polyp score 8 weeks post 1st dosing
Secondary endpoints• CT scan assessment (blinded)
Difference <10% or 10-30% or 30-50% or >50%
• Symptom score• Peak nasal inspiratory flow• nasal (merocel) and systemic
Inflammatory mediators
0 1 2 3 4Score
0
1
4
3
2

Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
Endoscopic Nasal polyp score and improvement
**intranasal steroids permitted
10/20
12/20
13/20
Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
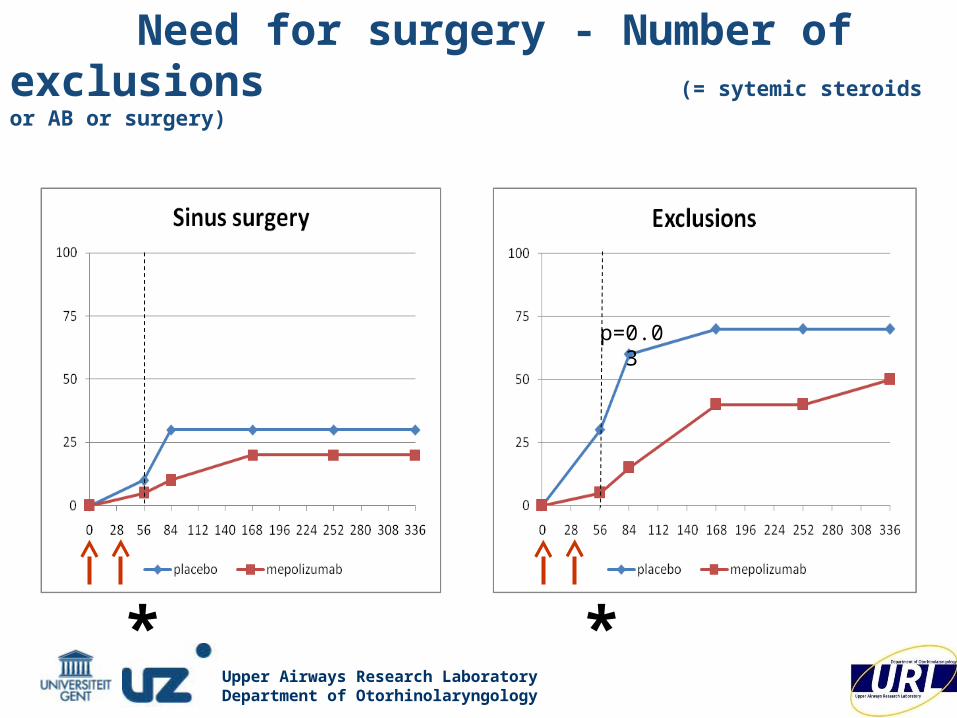
Need for surgery - Number of exclusions(= sytemic steroids or AB or surgery)
p=0.03
* *

Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
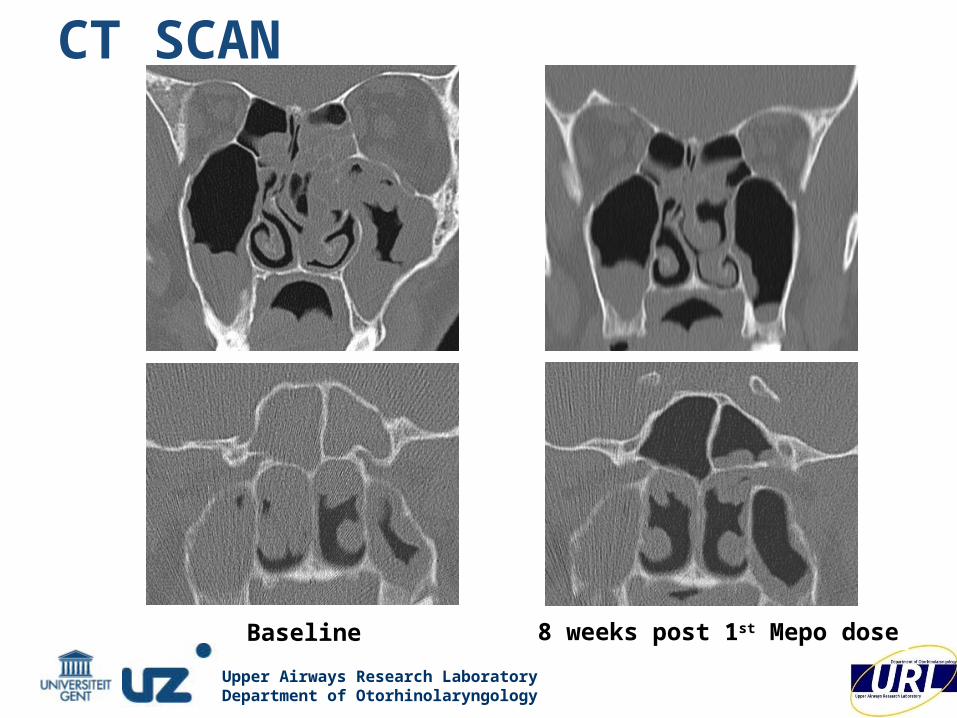
CT scores improvement from baseline at week 8
Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
8 weeks post 1st Mepo doseBaseline
CT SCAN

Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
Symptoms
intranasal steroids permitted intranasal steroids permitted
intranasal steroids permitted intranasal steroids permitted

Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
Peak nasal inspiratory flow (change from baseline)

Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
Anti IgE in nasal polyposis24 patients: 16 got anti-IgE
8 got placebo
4 (evt 8) Injections over 3 months
IgE
? Local Anti-IgE
Concentration?
Anti IgE
x IgEx
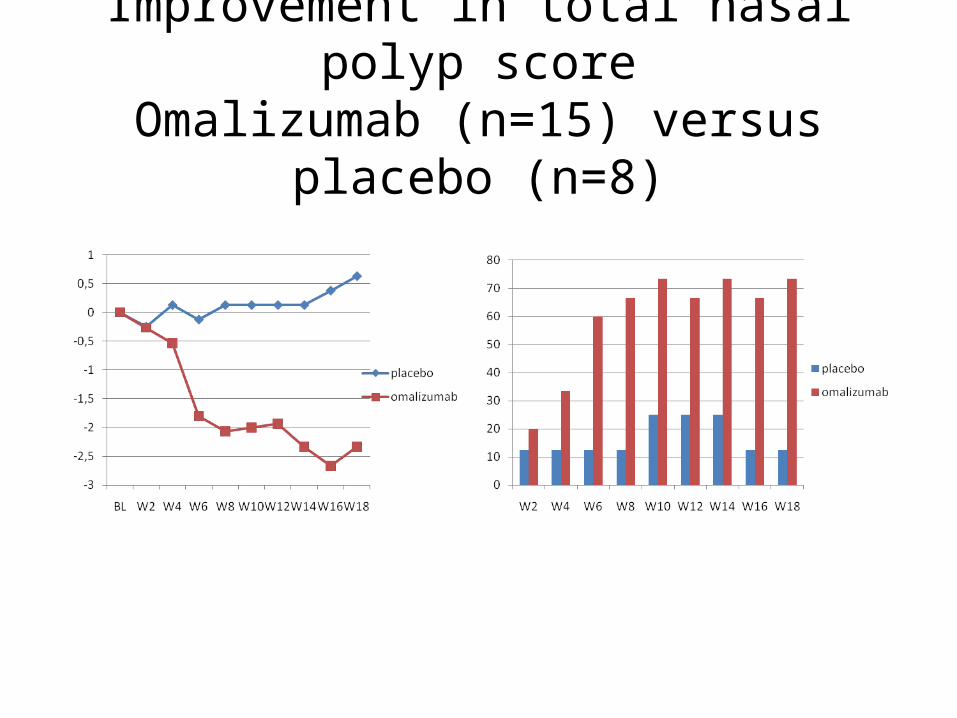
Improvement in total nasal polyp scoreOmalizumab (n=15) versus placebo (n=8)

Improvement in symptomsOmalizumab (n=15) versus placebo (n=8)

UPSIT smell test

Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
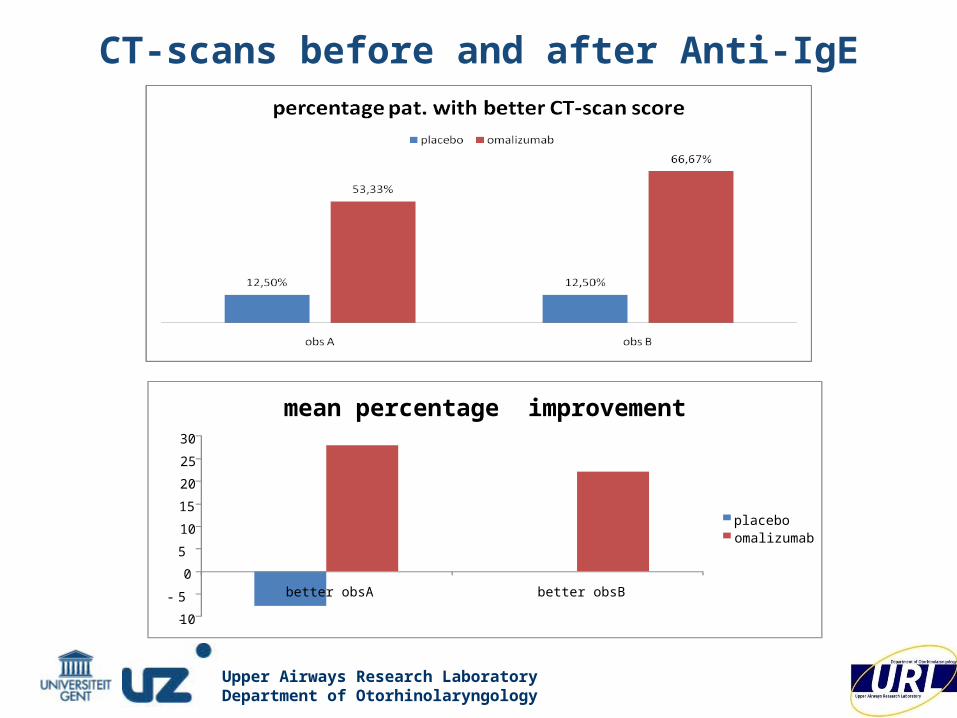
CT-scans before and after Anti-IgE

Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
CT-scans before and after Anti-IgE
Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
CT-scans before and after Anti-IgE
-10
- 5
0
5
10
15
20
25
30
better obsA better obsB
mean percentage improvement
placeboomalizumab

Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
Allergic versus non allergic patients
Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
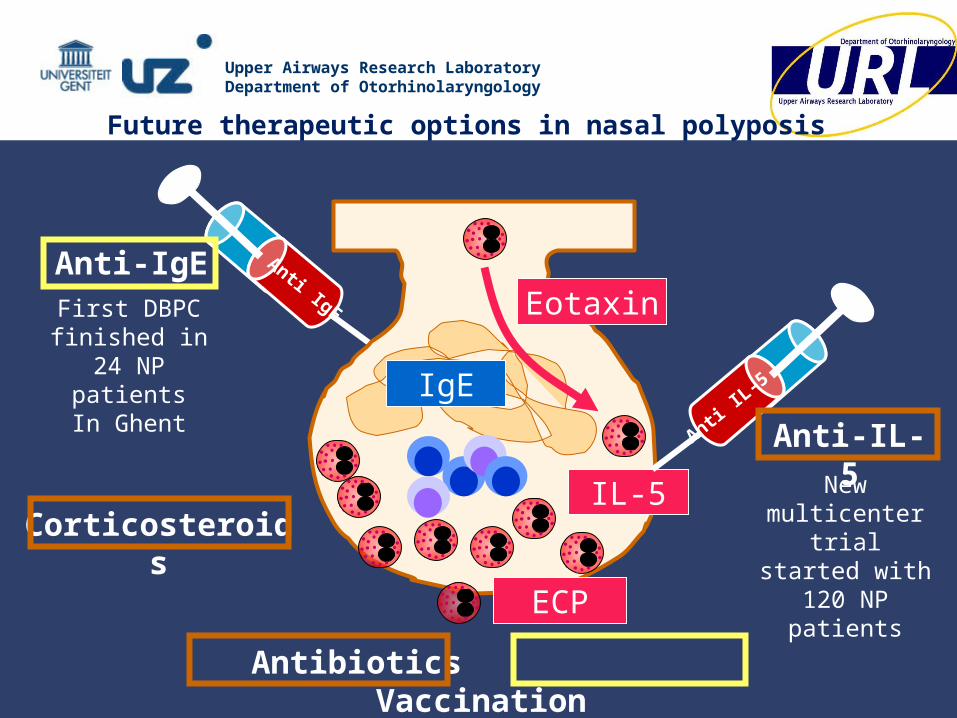
Anti IgE
Anti-IgE
Antibiotics Vaccination
IL-5
ECP
Eotaxin
IgEAnti
IL-5
Anti-IL-5
Corticosteroids
First DBPC finished in
24 NP patientsIn Ghent
New multicenter trial started with 120 NP patients
Future therapeutic options in nasal polyposis

Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
Practical management of Nasal Polyposis• Nasal douche with saline • Nasal corticosteroids
• GCS sprays: 2x/d, symptoms↓, no resolution of NP• GCS drops: symptoms↓, surgery↓↓
• Oral corticoids: effective but fast recurrence• Antibiotics:
• Antibiotic ointment• Long-term antibiotics: macrolides 500mg/d ged 3m
doxycycline 100 mg/d ged 1m• Future:
• Omalizumab (antiIgE) allergic 85% vs non allergic NP 55%
• Mepolizumab (anti-IL5): 2 injections in 65% better

Upper Airways Research LaboratoryDepartment of Otorhinolaryngology
Up
pe
r A
irw
ays
Res
ear
ch L
abo
rato
ry 2
009