upper airway and thoracic surgery - vet-ecpd · obstruction or collapse of the pharynx, larynx or...
TRANSCRIPT

1/36
Upper airway and Thoracic Surgery
Laurent Findji DMV MS DECVS MRCVS

2/36
DAY 1
Upper airway surgery

3/36
Upper airway surgery Laurent Findji DMV MS MRCVS DiplECVS Fitzpatrick Referrals, United Kingdom
Brachycephalic syndrome
The canine brachycephalic syndrome (BS) consists of a number of anatomical abnormalities of brachycephalic dogs which lead to obstructive dyspnea and digestive disorders. These abnormalities include stenotic nares, tortuous nasal cavities, aberrant conchae, elongated soft palate, laryngeal collapse and tracheal hypoplasia. It is classically understood that upper obstructions (nares, conchae, soft palate) aggravate, if not cause, deeper obstructions (laryngeal, tracheal and bronchial collapses) and digestive disorders. One study showed that 97% of brachycephalic dogs presented for BS had concurrent gastrointestinal diseases1. Early surgical correction of these upper airway abnormalities is therefore recommended and most commonly include treatment of stenotic nares and elongated soft palate. Other abnormalities occasionally require to be addressed surgically (e.g. laryngeal collapse2), but rarely in first intention.
My approach to BS treatment therefore consists of correcting the stenotic nares and elongated soft palate (ESP) first and almost systematically, which in most instances improve dogs enough to obviate the need for subsequent laryngeal surgery. In rare cases, markedly enlarged and everted laryngeal saccules will justify laryngeal sacculectomy.
Surgical techniques
Elongated soft palate Elongated soft palate is the most consistent anatomical abnormality encountered in dogs with BS, being reported in up to 100% of cases3, 4. Initially, it was mostly described as a mere excessive length of the soft palate, which causes an obstruction of the rima glottidis on inspiration. However, it has long been observed5-11 and recently demonstrated12-14 that in a significant proportion of brachycephalic dogs, the soft palate is also excessively thick, adding nasopharyngeal and oropharyngeal components to the airway obstruction. Most surgical techniques described for correction of ESP consist of a simple resection of the redundant portion of the soft palate, using different devices and various resection landmarks15-27. These techniques address the laryngeal component of the obstruction but address partially, or not at all, the nasopharyngeal and oropharyngeal obstructions. A technique, called folded flap palatoplasty (FFP) was developed to address the 3 components of the obstruction caused by the soft palate by making it both thinner and shorter5, 9-11. This technique will be the one described here as it is our current technique of choice.
Prior to surgery, the animal is premedicated and stress is avoided. Premedication can include acepromazine (0.01-0.03 mg/kg), dexamethasone (0.1-0.2 mg/kg) and an opioid analgesic (e.g. methadone, 0.1-0.3 mg/kg). Glycopyrrolate (2-10 µg/kg) can also be administered if the patient is bradycardic. Before induction of anesthesia, oxygen can be supplied as required by mask or flow-by. Induction must be swift to allow prompt control of the airway by tracheal intubation. The pharynx is examined and the larynx assessed for signs of laryngeal collapse.

4/36
The dog is placed in sternal recumbency. The head is restrained with the mouth kept open and the tongue gently pulled and fixed rostrally (Figure 1a, Figure 1b, Figure 2a, Schema 1).
a b FIGURE 1
The oral cavity is prepped for surgery. The deep portion of the pharynx is packed with swabs to prevent blood from reaching the glottis. Stay sutures are placed on each side of the caudal most part of the soft palate. The caudal border of the soft palate is retracted rostrally, until the caudal opening of the nasopharynx is directly visible (Schema 2). The retracted caudal edge is applied on the ventral mucosa of the soft palate and the point where the contact is made is marked with an electrocautery cut. The ventral mucosa of the soft palate is then incised in a trapezoidal shape from this mark rostrally to the free edge of the soft palate caudally. Laterally, the sides of the trapezoid pass just medially to the tonsils (Figure 2b, Schema 3). Using blunt dissection with fine scissors, most of the soft tissues contained between the nasopharyngeal and oropharyngeal mucosae of the soft palate (ventral mucosa, connective tissues, part of the palatinus and levator veli palatini muscles) are resected (Figure 2c, Figure 2d, Figure 2e, Figure 2f, Schema 4). Bleeding of the palatine vessels can be anticipated on the rostrolateral corners of the resection area. Hemostasis is achieved with electrocautery, preferably with bipolar forceps. With experience, these vessels can be identified and cauterized before section, which avoids any significant bleeding. The border of the free end of the palate, consisting of the reflection of the mucosa, is trimmed. To avoid losing the holding effect of the stay sutures, this can be done progressively in sequences alternating cutting and suturing (Figure 2g, Figure 2h, Figure 2i). The soft palate is then sutured folded on itself with monofilament absorbable sutures in an interrupted pattern (Figure 2j, Schema 5).

5/36
a b c d e
f g h i j FIGURE 2
Schema 1
Schema 2
Schema 3
Schema 4
Schema 5

6/36
Stenotic nares Stenotic nares, when present, are then corrected. Various techniques have been described, among which the vertical wedge alaplasty has our preference. It consists of the excision of a vertical wedge portion of the ala nasi. Incisions are made with a no. 11 scalpel blade and are started at the apex of the wedge, which is positioned slightly dorsolaterally to the dorsal limit of the slit-like opening of the stenotic naris (Figure 3a). The medial border of the wedge is parallel to the medial wall of the ala nasi. The lateral border of the wedge is made at an angle (40°-70°) from its medial border. The degree of postoperative opening of the naris will be grossly proportional to the angle chosen. It is important that incisions be deep enough and include a portion of the alar fold to fully relieve the obstruction and not limit the opening to the rostral part of the nostril (Figure 3b, Figure 3c). Hemorrhage is usually brisk on incision and may impair visibility of the surgical field to some extent, but it resolves quickly when the wound is sutured. Three or 4 sutures are placed in a simple interrupted pattern, using absorbable monofilament material. Starting with a suture placed at the ventrolateral corner of the naris (Figure 3d, Figure 3e) helps in obtaining a satisfactory cosmetic result. Another of these sutures is placed in depth from medial to lateral and exits through the skin, just laterally to the caudal end of the alar notch (Figure 3f, Figure 3g). When gently tied, this suture aims at keeping the deep portion of the naris widely open during the wound healing period (Figure 3h). The procedure is repeated on the other side with a new scalpel blade. Care must be taken to obtain a symmetrical opening on both sides. We find that starting with the side of the surgeon’s dominant hand (e.g. right nostril for a right-handed surgeon) helps in controlling symmetry.
a b c d
e f g h
FIGURE 3
When deemed necessary, a nasotracheal tube for postoperative oxygen supplementation can be placed before the dog is let to recover from anesthesia.

7/36
Tracheostomies
When presented with a case of upper airway obstruction as an emergency, the surgeon must first evaluate if it is life-threatening or not. In the first case, immediate action must be taken to gain control of the airway. Unless the animal is already unconscious or deeply shocked, this requires promptly induced general anaesthesia. In most cases, endotracheal intubation is possible, with a smaller than normal tube if necessary, and will provide the clinician with time to investigate the cause of the affection and make therapeutic decisions. In rare cases, a tracheostomy will need to be performed in emergency, in non-sterile conditions, to gain access to the trachea, but this procedure can most often be performed under sterile and settled conditions after an endotracheal tube has been placed. It is indicated whenever obstruction or collapse of the pharynx, larynx or proximal trachea is a risk during and after recovery from anaesthesia. Once the access to the lower airway is secured, oxygen supplementation can be provided.
Depending on the origin, type and size of the tumour responsible for the obstruction, the surgeon must choose between temporary or palliative measures (mainly tracheostomy), either temporary or definitive, or immediate causative treatment.
Temporary tracheostomy
Choice of the tube Tracheostomy tubes can be cuffed or non-cuffed, simple or with interchangeable cannulas and made of different materials.
Metallic tracheostomy tubes have little indications in small animals. They are the most rigid tubes and are still occasionally used for mechanical support after tracheal reconstruction. Most tubes used in veterinary medicine are made of polyvinyl chloride. They are of intermediate rigidity and fit most purposes. Lastly, silicone tubes are now more widely available and are the softer type of tubes. They are better tolerated but more expensive, and their flexibility can be useful whenever the tracheal conformation does not match well with polyvinyl chloride tubes.
The tube can be cuffed or non-cuffed. Cuffed tubes have few indications in small animals. The only rationale for using a cuffed tube is the need to provide assisted ventilation. Cuffed tubes can also be used for tracheostomies which are part of a surgical procedure, so that no leaking is present between the anaesthetic circuit and the airways. If needed, only high volume low pressure chuff should be used. Cuffed tubes occlude the portion of the trachea they do not fill and therefore narrow the functional airway and carry a higher risk of airway obstruction. Non-cuffed tubes are therefore most commonly used.
Tubes can have inner cannulae or not. Inner cannulas make cleaning of the tube easier, as they can be removed and either changed or clean, without the need to remove the tracheostomy tube itself. Disposable inner cannulas are also available. When using tubes without inner cannula, cleaning the tube involves taking the actual tube out, and either changing it or cleaning it. It is however important to note that even when using inner cannulas, the tube should be taken out regularly to be checked and cleaned. The cannulas only decrease the frequency with which the entire tube has to be removed and replaced.

8/36
Placement Whenever possible, a endotracheal tube is placed, securing access to the airway and bypassing the obstruction site. The patient can then be prepared aseptically as for any other surgery. In rare cases, the tracheostomy will have to be a life-saving emergency procedure on a patient which cannot be conventionally intubated. In these latter instances, the amount of preparation prior to performance of the tracheostomy has to be evaluated against the degree of respiratory obstruction and can go from none (imminent death) to complete (partial obstruction and oxygen supplemented via nasotracheal, orotracheal or tracheal catheter).
The patient is placed in dorsal recumbency. The entire ventral aspect of the neck is clipped and aseptically prepared. A midline longitudinal incision is made centred over the 4th or 5th tracheal ring. Blunt dissection between the sternohyoid muscles gives access to the trachea. The trachea is dissected as required to gain sufficient exposure, and care is taken not to damage the recurrent laryngeal nerves or extend the dissection excessively. Different techniques have been described to open the trachea. The simplest one, here described, has our preference. A limited transverse incision (a ¼ of the tracheal diameter long) is made between two tracheal rings. Through this incision, two stay sutures of large size (e.g. 4-metric, non-absorbable monofilament such as nylon or polypropylene) are placed around the tracheal rings adjacent to the incision. Using the stay sutures, the trachea is gently elevated and the incision can be extended under direct visual control. Care must be taken not to incise too extensively (<50% of the tracheal diameter). I prefer to progressively enlarge the initial incision until the chosen tracheal tube can be inserted without inappropriate strain on the tracheal incision edges. The tube diameter should not be more than 50% of that of the trachea. The stay sutures are left in place and marked with tape at their ends, so that they can be easily identified in case of emergency. The tube is secured with cutaneous sutures, umbilical tape around the neck, or both. If the cutaneous incision length exceeds by far what is necessary for the tube, the wound can be partially closed.
FIGURE 4: TRANSVERSE TEMPORARY TRACHEOSTOMY28
Tracheostomy care The placement of a tracheostomy tube is straightforward and of no significant difficulty. The most critical aspect of a tracheostomy is the amount of care it requires after placement.

9/36
The presence of the tube has several consequences. One of the roles of the upper airways is to warm and humidify the inspired air. In our countries, ambient air is 50% humidified and at temperatures around 20°C. Under normal circumstances, the air reaching the alveolae is 100% humidified and at core body temperature (38°C). When a tracheostomy tube is placed, the upper airways are by-passed and the air has to be humidified before administration to prevent desiccation of the airways. This can be done by means of humidifiers or nebulisers, 4 to 6 times daily for 15 to 20 minutes. Only sterile fluids, either water or preferably saline, should be used. Alternatively, if no such treatments are available, 2 to 5 millilitres of sterile saline can be instilled down the trachea through the tracheostomy tube every 1 to 2 hours.
The upper airways also act as filters for large particles. When a tracheostomy is performed, such particles are more likely to reach the lower airways and promote local inflammation and infection.
Tracheostomies predispose to retention of bronchoalveolar secretions by several mechanisms. First of all, within minutes of placement of a tracheostomy tube, the mucociliary escalator is depressed and the airways tend to dehydrate, which make the secretions thicker. Furthermore, the animal can cough, but the closed glottis is by-passed. Therefore, the cough is ineffective and removal of secretions by this means is impossible. The retained secretions predispose to infections, especially as the trachea is rapidly colonized with oropharyngeal flora after tracheostomy. Therefore, efforts have to be made to keep the airways as clean and unobstructed as possible. To this purpose, the trachea is regularly humidified and sucked. Usually, this is performed every 1 or 2 hours initially. After humidification, chest percussion (coupage) is also useful in mobilising the secretions, which are therefore more likely to be removed by suction. A purpose-designed suction catheter can be used, but if not available, soft urinary catheters or feeding tubes can be mounted on the suction machine. The diameter of the suction tube must not exceed 50% of the tracheostomy tube diameter to avoid inducing massive pulmonary actelectasis. Care must be taken not to traumatise the airways and to apply suction in short separate periods (10-15 sec) to minimise the discomfort and the respiratory impairment it induces. Moreover, suction of the airway induces vagal stimulation which can lead to cardiac bradyarrhythmias. Clinically or electrocardiographically monitoring the heart rate and rhythm is therefore appropriate.
The tracheostomy site is an open wound and must be treated as such. It should be cleaned and disinfected at least daily, or more frequently as needed.
In cats, the risk of tube occlusion as a result of secretion production is reported to particularly be a problem29. Cats are known to produce large amounts of thick secretions, which are prone to occlude the tube, especially as their small trachea only accommodates narrow tubes. In a retrospective study involving 23 cats, it appeared that the complication rate was high after temporary tracheostomy: 40% of cats had major complications (life-threatening) and 67% had minor complications (not life-threatening)30. The overall complication rate was 87%30. However, many of these cats had a temporary tracheostomy as part of the management of laryngeal masses, which have been reported to be associated with increased secretions. When cats affected with a neoplastic process were excluded, it appeared that the tracheostomy was associated with a good prognosis with 91% of animals discharged to home without subsequent complications30. Therefore, in cats, the tracheostomy care is even more demanding than in dogs, but if carried out properly, temporary tracheostomies themselves are associated with a good prognosis, unless the underlying disease is neoplastic, especially affecting the larynx.

10/36
Tracheostomy tube removal Because of the consequences of the presence of the tracheostomy tube, it should be removed as soon as the animal can breathe without it. It is therefore useful to regularly evaluate whether the animal can be weaned off the tube. To this purpose, the tube should never be left in place and obturated! The tube occupies a significant portion of the tracheal lumen and closing it results in severe obstruction. Furthermore, when closed, the tube is nothing but a narrowing of the tracheal lumen, which favours tracheal collapse and inflammation as a result of the Venturi and Bernoulli effects.
To test whether the animal can breathe without the tube, it must be removed. However, the surgeon must be ready to replace the tube, should significant dyspnoea result. Alternatively, the tube can be replaced by a smaller tube. If the animal breathes well with this smaller tube, it is left in place and another test is carried out later.
The stay sutures in the trachea are left in place until it is ascertained that the animal will not need the tube to be replaced (e.g., 12-24 h after tube removal). They can then be removed and the wound is left open to heal by second intention. It should not be bandaged. Wound and tracheal healing complications are uncommon.
When a tracheostomy is performed under sterile conditions and left a few hours only, as when it is a preliminary step in a surgical procedure, in can be closed primarily. A few slowly-absorbable or non-absorbable monofilament sutures (e.g. polydioxanone, polypropylene) are used to suture the tracheal incision and the rest of the wound is closed routinely.
Permanent tracheostomy
When the obstruction is thought to be permanent and not amenable to treatment, a permanent tracheostomy can be considered as a definitive treatment.
Different techniques have described29. Whichever technique is chosen, three main points have to be remembered. First, the tension on the stoma must be reduced as much as possible. To this purpose, the separated sternohyoid muscles can be sutures together dorsal to the trachea so that they push it ventrally and bring it closer to the cutaneous level. Second, it should be accounted that the stoma will contract during would healing, and the initial size sought must be approximately 50% larger than the desired final size. Third, to minimise stenosis and granuloma formation at the stoma edges, it is important to achieve precise muco-cutaneous anastomosis.
In the simplest technique, the approach is similar to that of a temporary tracheostomy. The trachea is dissected over approximately 4 to 6 rings on its entire periphery. The sternohyoid muscles, separated during the approach, are joined and sutured dorsally to the trachea as mentioned above. The trachea is thereby brought superficially in the surgical field. Over 3 to 5 tracheal rings, a rectangle incision outlining the ventral 1/3 of the trachea is made and care is taken not to include the tracheal mucosa. The choice of the tracheostomy length has to account for an average of 50% contraction in the long-term, but also depends on the tracheal wall. The longer the tracheostomy site, the more likely the trachea is to collapse at its level. Caution must therefore be exerted when performing tracheostomies on flaccid tracheas. The

11/36
tracheal rings and ligaments are dissected free of the tracheal mucosa. After excision of the ventral third of 3 to 5 rings, the extraluminal side of the mucosa should be visible and intact in the rectangle. A slightly larger rectangle or ellipse of skin, centred over the initial cutaneous incision is also excised. I usually then place a few sutures between the remaining part of the tracheal rings at the edges of the excised rectangle and the soft tissues around the planned stoma site, in an effort to limit tension of the future mucocutaneous anastomosis. The mucosa is then incised longitudinally in its midline, opened, and anastomosed to the skin.
In the first few days after surgery, the same type of care as after temporary tracheostomies can be applied. Progressively, the airway can be less and less often humidified. Eventually, no humidification is required, and the airway adapts to drier air by undergoing squamous metaplasia. The wound must however always be kept clean and free or hair, for the rest of the animal’s life. Petroleum ointment can be applied to prevent desiccation of the stoma and ease removal of tracheal debris which will accumulate around it. In my experience, such debris are abundant initially but their amount decreases over time.
Operated dogs should be prevented from running is high grass fields as they may inhale particles, or the stoma must be protected. Of course, going for a swim will no longer be an option!
Permanent tracheostomies can be straightforward and well tolerated. However, in a fair number of cases, difficulties arise from the neck conformation and its loose skin. Depending on the dog’s position, skin folds can occlude the tracheostomy site. In certain cases, combining judicious skin excision with the tracheostomy can minimise these complications. This is however better done after complete healing of the stoma, as it my otherwise result in more tension on the muco-cutaneous anastomosis. In the meantime, a tracheostomy tube can be used to prevent occlusion. In cats, permanent tracheostomies have been associated with high complication and mortality rates: in a study involving 21 cats, the median survival time was 20 days31. Fourteen cats were dyspnoeic postoperatively, most often because of mucous plug formation at the tracheal stoma or elsewhere in the respiratory tract. Eleven cats died (6 in hospital, 5 at home) and 7 were euthanased as a result of progression of the disease prompting tracheostomy.
Dehiscence is another potential complication although, if care is taken to minimise tension of the anastomosis, it is uncommon.
FIGURE 5: PERMANENT TRACHEOSTOMY28

12/36
Laryngeal paralysis
Laryngeal paralysis (LP) is a common cause of upper airway obstruction. It is more common in dogs, but occasionally affects cats32-34. It is most frequently an acquired disease, although a congenital form affecting young dogs is well-known and most commonly encountered in Bouviers des Flandres, Siberian Huskies, Dalmatians, English and Staffordshire bull terriers and Rottweilers. The acquired form affects older dogs, most commonly of large breeds. In many studies of acquired LP, Labrador retrievers were the most frequently affected breed35-49.
Anatomy50, 51
The larynx mainly consists of 4 cartilages: the epiglottic, arytenoid (paired), thyroid and cricoid cartilages (Figure 1). These cartilages are united by joints (fibrous or synovial) and muscles. The combined actions of intrinsic laryngeal muscles on these cartilages modify the size, shape and position of the glottis, rostral opening to the (infraglottic) laryngeal lumen and trachea. All intrinsic laryngeal muscles except the cricothyroid, which is innervated by the cranial laryngeal nerve, are innervated by the caudal laryngeal nerve, terminal segment of the recurrent laryngeal nerve (RLN). The RLN originates in the thorax from the vagus nerve and courses cranially up to the larynx, dorsolaterally to the trachea.
FIGURE 6: ANATOMY OF THE LARYNX, LATERAL AND CRANIAL VIEWS (1: CRICOARYTENOID JOINT; 2: CRICOTHYROID JOINT)
Physiopathology
The larynx keeps the entrance to the trachea. At rest, the passageway through the glottis, called rima
glottidis, is narrow. On inspiration, the rima glottidis is made larger mainly by the action of the cricoarytenoideus dorsalis muscle, which rotates the arytenoid so that its vocal process moves laterally (Figure 2). When swallowing, the rima glottidis is made narrower by the combined action of several intrinsic laryngeal muscles (cricoarytenoideus lateralis, thyroarytenoideus, ventricularis and arytenoideus transversus). In addition, when swallowing, the hyoid bone and pharynx are pulled rostrally, which brings the rima glottidis under the lifted epiglottis. The epiglottis then completely covers the narrowed rima glottidis, thereby preventing the passage of ingesta through the larynx into the trachea.

13/36
FIGURE 7: SCHEMATIC REPRESENTATION OF THE LARYNGEAL FUNCTION (A: REST; B: ABDUCTION)
Laryngeal paralysis results from disease of the recurrent laryngeal nerve(s). The origin of this disease is unknown in most cases of acquired LP, which is then called idiopathic. Neoplasia, trauma, infection or complications from cervical or thoracic surgery have however been reported as infrequent causes of LP. In idiopathic LP, the RLN disease is progressive, non-inflammatory and degenerative52. More and more evidence exists indicating that LP may be an early sign of a generalized neuromuscular disease rather than an isolated condition35, 36, 39, 53. A study of 11 dogs with acquired LP confirmed that these dogs were polyneuropathic through electrodiagnostic and histopathological examinations35. This underlying polyneuropathy is of great clinical relevance as, in the same study, neurological clinical signs progressed in 8 of the 9 dogs during the follow-up period (16 months or more)35. Another study revealed that dogs with idiopathic LP also suffered from oesophageal dysfunction, and that the more severe this dysfunction, the higher the risk for aspiration pneumonia36. In this study, 24 dogs could be followed over 12 months. Neurological clinical signs were observed in 25% of them at enrolment, whereas such signs were found in 58% and 100% of these dogs at 6 and 12-month follow-ups respectively36. At 12 months, the neurological signs observed were slight ataxia and weakness, with proprioceptive deficits in 17% of dogs, obvious ataxia, muscle atrophy and weakness in 38% of dogs, marked paraparesis in 42% and non-ambulatory paresis in 4% of dogs36. The cause for such generalised polyneuropathy remains unknown in most cases, although hypothyroidism, diabetes mellitus and myasthenia gravis have been found to infrequently cause LP. Several studies provide evidence that LP can result from a “dying-back” neuropathy, in which the most distal portion of axons degenerates first35, 39, 54. This could explain why LP would be an early sign of the generalised neuropathy, as the RLN, being a very long nerve, should be more susceptible to dying-back neuropathies than shorter nerves. However, this has not been demonstrated histopathologically35 and it has also been suggested that many different types of generalised neuropathy could cause idiopathic LP39.
Regardless of its cause, RLN dysfunction results in the paresis or paralysis of all intrinsic laryngeal muscles except for the cricothyroid muscle. On inspiration, the arytenoids are not actively rotated and the rima glottidis remains narrow, which cause upper airway obstruction. When swallowing, the rima glottidis is not narrowed, which increases the risk of aspiration pneumonia55. Vocalisation is also affected, as the muscles responsible for tensing and relaxing the vocal folds are weak or paralysed.

14/36
Diagnosis
Laryngeal paralysis is essentially a clinical diagnosis, later confirmed by other investigations. When using laryngoscopic observation as the gold standard for diagnosis of LP, clinical suspicion appeared very sensitive (91.6%) and specific (98.5%) for severe LP56. Early clinical signs are a change in phonation, inspiratory stridor and exercise intolerance. Gagging, coughing and retching, as well as vomiting/regurgitations and dysphagia may also be reported. Later in the course of the disease, dyspnoea, respiratory distress, cyanosis and syncopes may be observed. In addition, hyperthermia is frequently observed in dogs with LP, of which it can be a life-threatening consequence. It results from the increased work from the ventilatory muscles and decreased heat dissipation because of the impaired airflow secondary to the airway obstruction57.
Once a suspicion of LP has been raised, it can be confirmed in several ways. The most common is direct or videoscopic transoral observation of the larynx under light general anaesthesia. Most anaesthetic agents reduce laryngeal movements, which can mimic laryngeal paresis / paralysis. The influence of several anaesthetic protocols on laryngeal motion have been evaluated in normal dogs 58: associations of acepromazine + thiopental, acepromazine + propofol and ketamine + diazepam resulted in no laryngeal motion in 67%, 50% and 50% of dogs, respectively, and were not recommended. Greater arytenoid motion was observed with thiopental used as a single agent. When dogs were premedicated with acepromazine or opioids, mask induction with isoflurane was recommended to minimise laryngeal motion inhibition. Alternatively, intravenous administration of doxapram (2-5 mg/kg) can be used to increase respiratory motion41, 58, 59. However, in dogs with LP the use of doxapram can result in increased paradoxical motion of the arytenoids and respiratory distress, which can mandate prompt endotracheal intubation41. Paradoxical laryngeal movements can be observed in animals with LP. They consist of narrowing of the rima glottidis on inhalation, as a result of the negative pressure caused by the airflow through the narrow laryngeal ostium (Bernouilli effect), and “opening” of the rima glottidis on exhalation as a result of air pressure. It is therefore critical to determine how laryngeal and respiratory movements are coordinated to avoid misdiagnosis. Other diagnostic tests have been reported: electromyography, ultrasonography45 and transnasal laryngoscopy42. A recent study comparing ultrasound, transnasal laryngoscopy and laryngoscopy per os concluded that ultrasound was less effective in diagnosing LP than the other two methods because of the difficulty in differentiating normal from paradoxical laryngeal movements60. No significant difference was found between transnasal laryngoscopy and laryngoscopy per os. Being less risky to perform, laryngoscopy per os was the recommended method60.
Diagnostic tests aiming at screening for concurrent diseases are also carried out: haematology, blood biochemistry, thyroid function exploration and acetylcholine receptor antibody titres (myasthenia gravis). Thoracic x-rays are also recommended to rule out pre-existing aspiration pneumonia and other concurrent diseases which could affect the prognosis, such as megaoesophagus.
Treatment
For dogs presented as an emergency for respiratory distress, the initial treatment includes oxygen supplementation, steroidal anti-inflammatories (e.g. dexamethasone 0.1-0.3 mg/kg) and sedation (acepromazine 0.05-0.1 mg/kg). Sedation is contraindicated in dogs with decreased thoracic compliance

15/36
because of concomitant intrathoracic disease. When administered, sedation will improve breathing by reducing the respiratory efforts, thereby minimizing airflow velocity and associated Bernouilli effect. Sedation will also facilitate resolution of the potential hyperthermia shown by dogs with LP. Most dogs can be stabilised with such treatment. When insufficient, endotracheal intubation and surgical correction of the LP or temporary tracheostomy must be carried out promptly.
Several techniques of surgical correction of laryngeal paralysis have been described including ventriculocordectomy, partial arytenoidectomy, arytenoid lateralisation, (modified) castellated laryngofissure, combinations thereof and permanent tracheostomy37, 38, 49, 61-65. Currently, only two types of techniques are commonly used: arytenoid lateralisation techniques and partial laryngectomy techniques. Partial laryngectomy techniques are most commonly performed transorally and carry the risk of specific complications resulting from associated intralaryngeal trauma including blood aspiration, oedema, haematoma and laryngeal webbing. Such complications may however be much less frequent when the arytenoidectomy is performed using a diode laser37. To avoid intralaryngeal trauma, unilateral arytenoid lateralisation techniques are often preferred to partial laryngectomy techniques. In particular, unilateral arytenoid lateralisation (UAL) is considered by many surgeons as the treatment of choice38, 66-68, as it appeared associated with fewer complications than bilateral arytenoid lateralisation and partial laryngectomy46. It has our preference and will be the only treatment described here. Descriptions of other treatment modalities can be found elsewhere52, 57, 69.
When preparing the patient for a UAL, a smaller than usual endotracheal (ET) tube is used for maintenance of anaesthesia. Endotracheal intubation results in arytenoid abduction prior to surgical correction and too large a tube will favour excessive lateralisation at surgery. For a lateral approach, the animal is placed in lateral recumbency and a cushion can be placed under its neck to elevate the laryngeal area towards the surgeon. The skin is incised over the larynx, ventrally and parallel to the external jugular vein. The subcutaneous connective tissues and cutaneous muscles (sphincter colli superficialis, platysma and sphincter colli profundus) overlying the larynx are reflected by a combination of blunt and sharp dissection. The thyropharyngeus and cricopharyngeus muscles are then visible and the dorsal border of the thyroid cartilage lamina is palpable through them. Rather than transecting the thyropharyngeus muscle transversely, we prefer to separate its fibres by blunt dissection over the middle of the dorsal edge of the thyroid cartilage. The separated fibres are then retracted with blunt Gelpi retractors, which provides enough exposure of the thyroid cartilage lamina, covered by a fascial membrane. This laryngeal fascial membrane is incised and the laryngeal mucosa is detached from the medial aspect of the lamina of the thyroid cartilage. This is done by combination of scalpel incision over the dorsal edge of the thyroid cartilage and blunt dissection with a Freer periosteal elevator or cotton-buds. Dissection is performed delicately to avoid perforation of the laryngeal mucosa and penetration into the lumen of the larynx. In addition, dissection is limited cranially to avoid damage to the cranial laryngeal nerve, which carries fibres supplying the sensory information from laryngeal mucosa. Preserving these fibres may minimise the incidence of postoperative aspiration of food44, 70. The lamina of the thyroid cartilage is retracted laterally using one stay suture. Disarticulation of the cricothyroid joint is not necessary for sufficient exposure of the arytenoid cartilage. Furthermore, it may reduce the diameter of the rima glottidis after arytenoid lateralisation71 and disrupt the lateral support of the larynx, which makes the larynx more prone to collapse dorsoventrally72. Another study showed no effect of the disarticulation of the cricothyroid joint

16/36
or section of the interarytenoid sesamoid on the area of the rima glottidis73. These techniques did not have a significant effect on laryngeal airflow either73 and are therefore left to the surgeon’s discretion. The muscular process of the arytenoid is palpated and the cricoarytenoideus dorsalis is transected just caudally to it. The caudal part of the cricoarytenoid joint capsule is incised, but its rostral part is left intact to limit the later abduction of the arytenoid68. I do not section the interarytenoid structures (interarytenoid “band”) in order to minimise the laryngeal disruption and decrease the risk of mucosal perforation. One or two “simple interrupted” sutures are placed between the dorsolateral aspect of the cricoid cartilage and the muscular process of the arytenoid cartilage (Figure 3). Placement of the suture through the cricoid cartilage is done in a caudo-rostral direction. The caudal border of the cricoid cartilage is only palpated: dissection aiming at visualising it is unnecessary. Alternatively, a thyroarytenoid suture may be used by placing the suture through the caudo-dorsal portion of the lamina of the thyroid cartilage. The use of thyroarytenoid sutures instead of cricoarytenoid sutures results in a lesser increase of the rima glottidis area, but is shorter to perform and is associated with a similarly satisfactory outcome47. It has however been shown to be less effective in improving the laryngeal airflow in isolated canine larynges73. Subjectively, it is less technically and may be preferred by surgeons with little experience. In the arytenoid cartilage, the suture is passed medio-laterally. Along the rostro-caudal axis, both sutures are placed in the middle of the arytenoid articular surface. Along the ventro-dorsal axis, the two sutures are evenly spaced, at the ventral and dorsal third of the arytenoid articular surface74. The sutures are tied but not excessively tightened, as low-tension sutures have proved equally efficient in decreasing airway resistance68 and decrease the portion of the rima glottidis remaining uncovered when the epiglottis is closed75. In doubt, an assistant may extubate the animal and control transorally that the arytenoid abduction is satisfactory. The lamina of the thyroid cartilage is released, the thyropharyngeus muscle fibres are apposed in a cruciate pattern and the wound is closed routinely. If it has not been assessed intra-operatively, the arytenoid abduction is controlled postoperatively by transoral visualisation.
FIGURE 8: SCHEMATIC REPRESENTATION OF THE PLACEMENT OF A CRICOARYTENOID SUTURE WITHOUT DISRUPTION OF THE CRICOTHYROID JOINT
Prognosis
In dogs without clinical signs of concurrent disease, the prognosis after UAL is good: in one study in which dogs with swallowing or neurologic abnormalities were excluded, 91% of dogs were considered to have had a very satisfactory outcome 1 year after surgery and complications were only observed in 10% of

17/36
cases49. In another study, postoperative complications were observed in 31 of 109 dogs (28%) which underwent UAL, 21 (19%) of which were aspiration pneumonia46.
However, as described above, most affected animal suffer from generalised neuromuscular disease, which is the main determinant of their long-term prognosis. In one study, 6 of 11 dogs with acquired LP died or were euthanized within 15 months of diagnosis as a result of progression of clinical signs associated with their polyneuropathy35. Although neurological signs are likely to worsen over time, the polyneuropathy may progress slowly and long remain compatible with a reasonable quality of life. Therefore, in spite of this permanent risk of neurological deterioration, seeking surgical treatment for LP is appropriate to address the respiratory obstruction, which can be life-threatening in the short-term.
Aspiration pneumonia is the most commonly described complication after surgical treatment for LP. After unilateral arytenoid lateralisation, it has been reported to occur in 8 to 19% of cases36, 40, 43, 44, 46, 47. Aspiration pneumonia can occur months to years after surgery and operated dogs remain are at risk for the remainder of their lives36, 40, 43, 46, but it seems that the risk decreases over time40, 43, 66. Perioperative administration of metoclopramide may lower the risk of aspiration pneumonia76. In addition, if owners are given clear instructions of monitoring, aspiration pneumonia can often be detected early and respond favourably to treatment36. Other commonly reported complications after UAL include persistent coughing and gagging (16-28%)40, 43, surgical repair failure and recurrence of clinical signs (0-8%)43, 44, 46, 49, persistent exercise intolerance (23%)40 and seroma requiring drainage (3-10%)40, 49.
Laryngeal paralysis in cats
Laryngeal paralysis is much less common in cats than in dogs. Like in dogs, laryngeal paralysis appear to be either congenital or acquired in cats33, 52. Clinical signs are rather similar in the two species, although cats seem to be only rarely be hyperthermic on presentation34. In case of unilateral LP, cats seem more prone to show clinical signs than dogs with unilateral LP33. Similarly to dogs, acquired laryngeal paralysis may be associated with more generalised neuromuscular diseases: in one study of 16 cats with LP, 2 were found to have concurrent megaoesophagus34 and in a study of 4 cats with LP, signs of a generalised neuromuscular disease were observed in 277. Several techniques have been used for surgical treatment of LP in cats, including ventriculocordectomy, partial arytenoidectomy, arytenoid lateralisation and castellated laryngofissure52. Like in dogs, we prefer low-tension unilateral arytenoid lateralisation, performed following the technique described above for dogs. Whereas it seems associated with few complications in dogs (but is, in our experience, unnecessary), disarticulation of the cricothyroid joint and interarytenoid band is not recommended in cats. Respiratory tract cartilages are much more fragile and friable in cats compared with dogs and the procedure is therefore more demanding in this species: great care must be taken no to fracture the laryngeal cartilages while grasping them or passing needles through them. Cutting needles should therefore be avoided. If such fractures happen intra or postoperatively, a contralateral intervention may be necessary. The incidence of postoperative aspiration pneumonia seems to be much lower in cats compared with dogs34, except when arytenoid lateralisation is performed bilaterally33. Bilateral arytenoid lateralisation is therefore not recommended in cats.

18/36
References
1. Poncet CM, Dupre GP, Freiche VG, Estrada MM, Poubanne YA, Bouvy BM. Prevalence of gastrointestinal tract lesions in 73 brachycephalic dogs with upper respiratory syndrome. Journal of Small
Animal Practice. 2005;46: 273-279. 2. White RN. Surgical management of laryngeal collapse associated with brachycephalic airway obstruction syndrome in dogs. Journal of Small Animal Practice. 2012;53: 44-50. 3. Poncet CM, Dupre GP, Freiche VG, Bouvy BM. Long-term results of upper respiratory syndrome surgery and gastrointestinal tract medical treatment in 51 brachycephalic dogs. Journal of Small Animal
Practice. 2006;47: 137-142. 4. Wykes PM. Brachycephalic airway obstructive syndrome. Problems in Veterinary Medicine. 1991;3: 188-197. 5. Findji L, Dupré G. Folded flap palatoplasty for treatment of elongated soft palates in 55 dogs. Wiener Tierärztliche Monatsschrift. 2008;95: 56-63. 6. Grandage J. Functional Anatomy of the Respiratory System. In: Slatter D (ed): Textbook of Small
Animal Surgery. Philadelphia: Saunders, 2003;763-780. 7. Hendricks JC, Kline LR, Kovalski RJ, O'Brien JA, Morrison AR, Pack AI. The English bulldog: a natural model of sleep-disordered breathing. J Appl Physiol. 1987;63: 1344-1350. 8. Amis TC, Kurpershoek C. Pattern of breathing in brachycephalic dogs. American Journal of
Veterinary Research. 1986;47: 2200-2204. 9. Findji L, Dupré G. Folded flap palatoplasty for treatment of elongated soft palates in 55 dogs. European Journal of Companion Animal Practice. 2009;19: 125-132. 10. Dupré G, Findji L, Poncet C. The Folded Flap Palatoplasty: a new technique for treatment of elongated soft palate in dogs. In: Schramme M, Tremaine H, Walmsley J, Bellenger CR, Houlton J (eds): ECVS Annual Scientific Meeting. Lyon, France, 2005;265-267. 11. Dupré G, Findji L. La palatoplastie modifiée chez le chien. Le Nouveau Praticien Vétérinaire. 2004: 553-556. 12. Pichetto M, Arrighi S, Roccabianca P, Romussi S. The anatomy of the dog soft palate. II. Histological evaluation of the caudal soft palate in brachycephalic breeds with grade I brachycephalic airway obstructive syndrome. Anatomical Record : Advances in Integrative Anatomy and Evolutionary
Biology. 2011;294: 1267-1272. 13. Grand JGR, Bureau S. Structural characteristics of the soft palate and meatus nasopharyngeus in brachycephalic and non-brachycephalic dogs analysed by CT. Journal of Small Animal Practice. 2011;52: 232-239. 14. Crosse KR, Bray JP, Orbell GMB, Preston CA. Histological evaluation of the soft palate in dogs affected by brachycephalic obstructive airway syndrome. New Zealand Veterinary Journal. 2015;63: 319-325. 15. Dunié-Mérigot A, Bouvy B, Poncet C. Comparative use of CO2 laser, diode laser and monopolar electrocautery for resection of the soft palate in dogs with brachycephalic airway obstructive syndrome. Veterinary Record. 2010;167: 700-704. 16. Brdecka DJ, Rawlings CA, Perry AC, Anderson JR. Use of an electrothermal, feedback-controlled, bipolar sealing device for resection of the elongated portion of the soft palate in dogs with obstructive upper airway disease. Journal of the American Veterinary Medical Association. 2008;233: 1265-1269.

19/36
17. Brdecka D, Rawlings C, Howerth E, Cornell K, Stiffler K. A histopathological comparison of two techniques for soft palate resection in normal dogs. Journal of the American Animal Hospital Association. 2007;43: 39-44. 18. Monnet E. Brachycephalic Airway Syndrome. In: Slatter D (ed): Textbook of Small Animal Surgery. Philadelphia: Saunders, 2003;808-813. 19. Koch DA, Arnold S, Hubler M, Montavon PM. Brachycephalic syndrome in dogs. Compendium on
Continuing Education for the Practicing Veterinarian. 2003;25: 48, 50-54. 20. Hobson HP. Brachycephalic syndrome. Seminars in Veterinary Medicine and Surgery (Small
Animal). 1995;10: 109-114. 21. Aron DN, Crowe DT. Upper airway obstruction. General principles and selected conditions in the dog and cat. Vet Clin North Am Small Anim Pract. 1985;15: 891-917. 22. Bright RM, Wheaton LG. A modified surgical technique for elongated soft palate in dogs. J Am
Anim Hosp Assoc. 1983;19: 288. 23. Harvey CE. Upper airway obstruction surgery. 2. Soft palate resection in brachycephalic dogs. Journal of the American Animal Hospital Association. 1982;18: 538-544. 24. Harvey CE, Venker-von Haagan A. Surgical management of pharyngeal and laryngeal airway obstruction in the dog. Vet Clin North Am. 1975;5: 515-535. 25. Singleton WB. Partial velum palatiectomy for relief of dyspnea in brachycephalic breeds. J Small
Anim Pract. 1962: 215-216. 26. Farquharson J, Smith DW. Resection of the soft palate in the dog. J Am Vet Med Assoc. 1942: 427-430. 27. Davidson EB, Davis MS, Campbell GA, Williamson KK, Payton ME, Healey TS, et al. Evaluation of carbon dioxide laser and conventional incisional techniques for resection of soft palates in brachycephalic dogs. Journal of the American Veterinary Medical Association. 2001;219: 776-781. 28. Sura PAD, A.M. Trachea and Bronchi. In: Tobias KM, Johnston SA (eds): Veterinary surgery : small
animal. St. Louis, Mo.: Elsevier, 2012;1734-1751. 29. Colley P, Huber M, Henderson R. Tracheostomy techniques and management. Compendium on
Continuing Education for the Practicing Veterinarian. 1999;21: 44-47, 50-53. 30. Guenther-Yenke CL, Rozanski EA. Tracheostomy in cats: 23 cases (1998-2006). Journal of Feline
Medicine and Surgery. 2007;9: 451-457. 31. Stepnik MW, Mehl ML, Hardie EM, Kass PH, Reimer SB, Campbell BG, et al. Outcome of permanent tracheostomy for treatment of upper airway obstruction in cats: 21 cases (1990-2007). Journal
of the American Veterinary Medical Association. 2009;234: 638-643. 32. Taylor SS, Harvey AM, Barr FJ, Moore AH, Day MJ. Laryngeal disease in cats: a retrospective study of 35 cases. Journal of Feline Medicine and Surgery. 2009;11: 954-962. 33. Hardie RJ, Gunby J, Bjorling DE. Arytenoid lateralization for treatment of laryngeal paralysis in 10 cats. Veterinary Surgery. 2009;38: 445-451. 34. Schachter S, Norris CR. Laryngeal paralysis in cats: 16 cases (1990-1999). Journal of the American
Veterinary Medical Association. 2000;216: 1100-1103. 35. Thieman KM, Krahwinkel DJ, Sims MH, Shelton GD. Histopathological confirmation of polyneuropathy in 11 dogs with laryngeal paralysis. Journal of the American Animal Hospital Association. 2010;46: 161-167.

20/36
36. Stanley BJ, Hauptman JG, Fritz MC, Rosenstein DS, Kinns J. Esophageal dysfunction in dogs with idiopathic laryngeal paralysis: a controlled cohort study. Veterinary Surgery. 2010;39: 139-149. 37. Olivieri M, Voghera SG, Fossum TW. Video-assisted left partial arytenoidectomy by diode laser photoablation for treatment of canine laryngeal paralysis. Veterinary Surgery. 2009;38: 439-444. 38. Schofield DM, Norris J, Sadanaga KK. Bilateral thyroarytenoid cartilage lateralization and vocal fold excision with mucosoplasty for treatment of idiopathic laryngeal paralysis: 67 dogs (1998-2005). Veterinary Surgery. 2007;36: 519-525. 39. Jeffery ND, Talbot CE, Smith PM, Bacon NJ. Acquired idiopathic laryngeal paralysis as a prominent feature of generalized neuromuscular disease in 39 dogs. Veterinary Record. 2006;158: 17-21. 40. Hammel SP, Hottinger HA, Novo RE. Postoperative results of unilateral arytenoid lateralization for treatment of idiopathic laryngeal paralysis in dogs: 39 cases (1996-2002). Journal of the American
Veterinary Medical Association. 2006;228: 1215-1220. 41. Tobias KM, Jackson AM, Harvey RC. Effects of doxapram HCl on laryngeal function of normal dogs and dogs with naturally occurring laryngeal paralysis. Veterinary Anaesthesia and Analgesia. 2004;31: 258-263. 42. Radlinsky MAG, Mason DE, Hodgson D. Transnasal laryngoscopy for the diagnosis of laryngeal paralysis in dogs. Journal of the American Animal Hospital Association. 2004;40: 211-215. 43. Snelling SR, Edwards GA. A retrospective study of unilateral arytenoid lateralisation in the treatment of laryngeal paralysis in 100 dogs (1992-2000). Australian Veterinary Journal. 2003;81: 464-468. 44. Demetriou JL, Kirby BM. The effect of two modifications of unilateral arytenoid lateralization on rima glottidis area in dogs. Veterinary Surgery. 2003;32: 62-68. 45. Rudorf H, Barr FJ, Lane JG. The role of ultrasound in the assessment of laryngeal paralysis in the dog. Veterinary Radiology & Ultrasound. 2001;42: 338-343. 46. MacPhail CM, Monnet E. Outcome of and postoperative complications in dogs undergoing surgical treatment of laryngeal paralysis: 140 cases (1985-1998). Journal of the American Veterinary
Medical Association. 2001;218: 1949-1956. 47. Griffiths LG, Sullivan M, Reid SWJ. A comparison of the effects of unilateral thyroarytenoid lateralization versus cricoarytenoid laryngoplasty on the area of the rima glottidis and clinical outcome in dogs with laryngeal paralysis. Veterinary Surgery. 2001;30: 359-365. 48. Ross JT, Matthiesen DT, Noone KE, Scavelli TA. Complications and long-term results after partial laryngectomy for the treatment of idiopathic laryngeal paralysis in 45 dogs. Vet Surg. 1991;20: 169-173. 49. White RAS. Unilateral arytenoid lateralisation: an assessment of technique and long term results in 61 dogs with laryngeal paralysis. Journal of Small Animal Practice. 1989;30: 543-549. 50. Hermanson JW, Evans HE. The muscular system. In: Evans HE (ed): Miller's anatomy of the dog. Philadelphia ; London: W.B. Saunders, 1993;258-384. 51. Evans HE. The respiratory system. In: Evans HE (ed): Miller's anatomy of the dog. Philadelphia ; London: W.B. Saunders, 1993;463-493. 52. Griffin JF, Krahwinkel DJ. Laryngeal paralysis: pathophysiology, diagnosis, and surgical repair. Compendium on Continuing Education for the Practicing Veterinarian. 2005;27: 857-869. 53. Shelton GD. Acquired laryngeal paralysis in dogs: evidence accumulating for a generalized neuromuscular disease. Vet Surg. 2010;39: 137-138.

21/36
54. Braund KG, Steinberg HS, Shores A, Steiss JE, Mehta JR, Toivio-Kinnucan M, et al. Laryngeal paralysis in immature and mature dogs as one sign of a more diffuse polyneuropathy. Journal of the
American Veterinary Medical Association. 1989;194: 1735-1740. 55. Millard RP, Tobias KM. Laryngeal paralysis in dogs. Compendium Continuing Education for
Veterinarians. 2009;31: 212-212...219. 56. Broome C, Burbidge HM, Pfeiffer DU. Prevalence of laryngeal paresis in dogs undergoing general anaesthesia. Australian Veterinary Journal. 2000;78: 769-772. 57. Holt DE, Brockman D. Laryngeal paralysis. In: King LG (ed): Textbook of respiratory diseases in
dogs and cats. Philadelphia, Pa. ; [Great Britain]: Saunders, 2004;319-328. 58. Jackson AM, Tobias K, Long C, Bartges J, Harvey R. Effects of various anaesthetic agents on laryngeal motion during laryngoscopy in normal dogs. Veterinary Surgery. 2004;33: 102-106. 59. Miller CJ, McKiernan BC, Pace J, Fettman MJ. The effects of doxapram hydrochloride (Dopram-V) on laryngeal function in healthy dogs. Journal of Veterinary Internal Medicine. 2002;16: 524-528. 60. Radlinsky MG, Williams J, Frank PM, Cooper TC. Comparison of three clinical techniques for the diagnosis of laryngeal paralysis in dogs. Veterinary Surgery. 2009;38: 434-438. 61. Smith MM, Gourley IM, Kurpershoek CJ, Amis TC. Evaluation of a modified castellated laryngofissure for alleviation of upper airway obstruction in dogs with laryngeal paralysis. Journal of the
American Veterinary Medical Association. 1986;188: 1279-1283. 62. Rosin E, Greenwood K. Bilateral arytenoid cartilage lateralization for laryngeal paralysis in the dog. Journal of the American Veterinary Medical Association. 1982;180: 515-518. 63. Holt D, Harvey C. Idiopathic laryngeal paralysis: results of treatment by bilateral vocal fold resection in 40 dogs. Journal of the American Animal Hospital Association. 1994;30: 389-395. 64. Trout NJ, Harpster NK, Berg J, Carpenter J. Long term results of unilateral ventriculocordectomy and partial arytenoidectomy for the treatment of laryngeal paralysis in 60 dogs. Journal of the American
Animal Hospital Association. 1994;30: 401-407. 65. Zikes C, McCarthy T. Bilateral ventriculocordectomy via ventral laryngotomy for idiopathic laryngeal paralysis in 88 dogs. Journal of the American Animal Hospital Association. 2012;48: 234-244. 66. White RA. Canine laryngeal surgery: time to rethink? Vet Surg. 2009;38: 432-433. 67. Pascoe JR. At the crossroads: conundrums and challenges in laryngeal surgery. Vet Surg. 2007;36: 513-514. 68. Greenberg MJ, Bureau S, Monnet E. Effects of suture tension during unilateral cricoarytenoid lateralization on canine laryngeal resistance in vitro. Vet Surg. 2007;36: 526-532. 69. Monnet E. Laryngeal paralysis and devocalisation. In: Slatter DH (ed): Textbook of small animal
surgery. Philadelphia, Pa. ; London: W. B. Saunders, 2003;837-845. 70. Burbidge HM, Goulden BE, Jones BR. Laryngeal paralysis in dogs: an evaluation of the bilateral arytenoid lateralisation procedure. Journal of Small Animal Practice. 1993;34: 515-519. 71. Monnet E. Laryngeal paralysis. The North American Veterinary Conference. Gainesville, 2009;1527-1529. 72. Lozier S, Pope E. Effects of arytenoid abduction and modified castellated laryngofissure on the rima glottidis in canine cadavers. Veterinary Surgery. 1992;21: 195-200. 73. Wignall JR, Baines SJ. Effects of unilateral arytenoid lateralization technique and suture tension on airway pressure in the larynx of canine cadavers. American Journal of Veterinary Research. 2012;73: 917-924.

22/36
74. Mathews KG, Roe S, Stebbins M, Barnes R, Mente PL. Biomechanical evaluation of suture pullout from canine arytenoid cartilages: effects of hole diameter, suture configuration, suture size, and distraction rate. Veterinary Surgery. 2004;33: 191-199. 75. Bureau S, Monnet E. Effects of suture tension and surgical approach during unilateral arytenoid lateralization on the rima glottidis in the canine larynx. Veterinary Surgery. 2002;31: 589-595. 76. Greenberg MJ, Reems MR, Monnet E. Use of perioperative metoclopramide in dogs undergoing surgical treatment of laryngeal paralysis: 43 cases (1999-2006). Vet Surg. 2007;36: E11. 77. White RAS, Littlewood JD, Herrtage ME, Clarke DD. Outcome of surgery for laryngeal paralysis in four cats. Veterinary Record. 1986;118: 103-104.
23/36
DAY 2
Thoracic surgery

24/36
Thoracic surgery
Laurent Findji DMV, MS, MRCVS, Diplomate ECVS Fitzpatrick Referrals, Surrey, UK
Thoracic trauma
Thoracic traumatic injury can result from blunt force (e.g., road traffic accident), biting or penetrating. The inherent resilience of the chest makes it resistant to compressive forces. It is therefore frequent that no significant lesion of the thoracic wall results from blunt trauma, when internal thoracic lesions (internal bleeding, pulmonary contusions) are sometimes severe. However, except for the management of haemothorax, such cases are not dealt with surgically.
Rib fractures are usually addressed conservatively. Likewise, when several ribs are fractured in multiple sites, a mobile portion of the chest wall can be created, that moves paradoxically: it moves inward during inspiration and outward during expiration. Such a condition is called a flail chest. Whereas treatment of flail chest is commonly described as involving external or internal fixation of the fractured ribs, it is my experience that most flail chests can be treated conservatively. Pain relief is in any case important and local nerve blocks of intercostal nerves associated with all fractured ribs and the two ribs cranial and caudal to them are quite effective. Another area of controversy is the positioning of recumbent animals with flail chest. Many authors recommend placing the animal with the affected side down (i.e. right recumbency for a right flail chest, and vice versa), so that the flail chest is slightly stabilised and the lung less affected is up, thereby minimizing the perfusion/ventilation (V/Q) mismatch. However, this may result in more pain, as the animal’s weight is pressing on the broken ribs and some authors tend to prefer placing the affected side up. It seems judicious to evaluate this on an individual basis. Most animals do not show significant V/Q mismatch and can be placed with the affected side upwards. On the other hand, if the movement of the free portion of the rib cage is judged hazardous for internal thoracic structures, provided proper analgesia is administered, the animal can be lying on the affected side with minimal discomfort.
In the rare cases where conservative treatment is judged inappropriate, flail chests can be stabilised either externally, using splints and casts, or internally. The former can be performed in an emergency basis. Care should be taken, however, not to overly restrict the rib cage’s mobility, which would result in respiratory impairment. Ribs are tied to the external coaptation device using non-absorbable monofilament sutures. Internal repair is a delayed procedure following the general rules of fracture repair, which is not to be performed on an emergency basis.
The more severe lesions to the thoracic wall probably result from bite wounds. Lesions of internal thoracic organs (lungs, diaphragm, etc.) can also be present. Classically, bite wounds result in limited visible trauma (a few small cutaneous wounds and variably extensive bruising) whereas internal lesions are often quite severe. Furthermore, such wounds are to be considered at least contaminated with oral

25/36
flora, including anaerobes. For these reasons, it is appropriate to surgically explore all thoracic bite wounds as soon as the animal is judged fit for general anaesthesia. The general rules of wound management apply to thoracic wounds. Debridement must be thorough and any unviable tissues, including ribs, of should be excised. The thoracic wall should then be reconstructed with local healthy tissues. If such tissues are lacking, the omentum can be brought to the thoracic wall to provide supplemental vascular supply and host defences against infection. The thorax is drained by placing a chest tube before closure under direct visual control, and the thoracic wall wound is separately drained with an active (Redon) or passive (Penrose) drain, as appropriate.
Finally, penetrating foreign bodies are uncommon but require timely management. One golden rule is to never remove the foreign body at any time before surgery. If a large part of the foreign body remains outside the thorax, is can be cut shorter to ease manipulations. Care must however be taken not to move its internal part while doing so. The patient is optimised, with the penetrating foreign body untouched, in view of surgical exploration. Usually, a lateral approach is appropriate, unless the foreign body’s localisation indicates that it may have damaged thoracic structures on both sides of the thorax. X-rays or CT-scan can help determine that latter point. The surgical area is prepared as aseptically as possible and the thorax is approached. Only when a direct visual control of the internal portion of the foreign body is gained should the foreign body be removed. The surgeon must then be ready to act promptly to repair any life-threatening lesion ensuing, especially lesions of great vessels.
Diaphragmatic hernia
Diaphragmatic hernias are common consequences from blunt trauma applied to the abdomen while the glottis is open. The diaphragm can be torn is different shapes, and variable combinations of abdominal organs herniate into the thorax. It is a surgical condition and the treatment involves replacing the abdominal organs in place and repairing the diaphragm. The details of the surgical treatment will not be discussed here as it is the topic of a subsequent presentation of this course.
Technically, repair of diaphragmatic hernias is seldom demanding. The difficulty in managing such cases lies in the pre and postoperative management. The key to success should be sought in these phases more than in the surgical procedure itself.
Preoperatively, management of animals with diaphragmatic hernia relies on gentle manipulation avoiding any supplemental stress, providing oxygen supplementation and optimising the patient with regards to any concurrent hypovolaemia, blood loss and acidosis. Hypotensive optimisation is indicated rather than aggressive fluid therapy, as these animals will be prone to pulmonary oedema in the postoperative period.
Early studies report increased mortality in animals operated on an emergency basis, i.e. within 24 hours. This has led to the widespread idea that these animals should not be operated early after presentation, unless the stomach is herniated. When reviewing the evidence supporting this idea, it seems that other factors may have been responsible for this apparent increase in mortality. More recently, this dogma has therefore been challenged and it should no longer be strictly obeyed. Instead, animals with diaphragmatic hernia should be optimised and surgically addressed as soon as shock is treated and the animal is stable from a cardiovascular viewpoint. Presence of the stomach in the thorax changes little to this plan. When

26/36
necessary, the stomach may be deflated by thoracocentesis or by placing a nasogastric tube to allow more time for preoperative stabilisation. One situation in which emergency surgery may be required is intractable bleeding from the herniated organs, such as the liver. This is however rare.
The second critical period is postoperative recovery. The main idea is that most cats not surviving surgical treatment die from pulmonary oedema and other complications associated with ischaemia-reperfusion injury. The surgeon and the anaesthetist must keep in mind at all times that overzealous attempts to re-inflate atelectatic lungs and restore normal pleural space volume leads to barotrauma and massive ischaemia-reperfusion injury. Previous recommendations that the lung should be re-inflated as much as possible during the surgical procedure and the thorax be thoroughly drained at the end of the intervention should therefore be abandoned! Instead, a small diameter thoracostomy tube can be placed during the procedure to allow progressive drainage over 12 to 24 hours. During the procedure, the anaesthetist should maintain moderate ventilation pressures (15-20 mmHg). At the end of the procedure, portions of the lungs still remaining atelectatic should be left unaddressed and the pleural space should be drained just enough for the breathing to be effective in maintaining normal oxygen saturation. A residual pneumothorax is therefore considered normal, even preferable. The patient is then closely monitored for pulmonary oedema. Oxygen supplementation and cautious fluid therapy are maintained as deemed appropriate according to perfusion and oxygen assessment parameters. The thorax is progressively drained through the thoracostomy tube, which is removed as soon as it is unproductive (usually within 24 hours).
Anaesthetic considerations
Depending on the underlying condition requiring thoracic surgery, the patients may suffer from respiratory compromise before surgery and require preoperative optimisation. Preoperative oxygenation (e.g. oxygen mask application for 5 minutes prior to induction) may be required to limit the risk of hypoxia at the time of induction of anaesthesia, before endotracheal intubation. As a rule, the induction of anaesthesia must be rapid to allow immediate control of the airways, classically by endotracheal intubation, but this is particularly important in patients with respiratory compromise.
Numerous protocols can be used to premedicate the patients and induce and maintain anaesthesia. Typically, animals are premedicated with a combination of a tranquiliser (e.g. acepromazine 0.02-0.05 mg/kg) and opioids (e.g. methadone 0.1-0.2 mg/kg). Anaesthesia is then induced with barbiturates or propofol and maintain with an inhalant anaesthetic (e.g. isoflurane). Ventilation parameters are especially important to monitor in patients undergoing thoracotomy. Preferably, constant monitoring for such patients should include capnography and pulse oxymetry.
In addition to systemic analgesics, local anaesthetics are used during thoracotomy procedures. Most often, intercostal injections of local anaesthetics are performed before closure of the thoracic cavity (e.g. total dose of 2 mg/kg of bupivacaine in dogs). In addition, in the postoperative period, similar doses of bupivacaine can be instilled in the chest drain every 3 to 6 hours. The bupivacaine instilled intrapleurally is best diluted with 0.9% sodium chloride and administered slowly, as it can be quite painful in itself if administered rapidly and in a concentrated form.

27/36
Patients undergoing thoracic surgery require mechanical ventilation from the moment the thorax is entered until it is closed and negative pressure is re-established in the pleural cavity. However, it is important to monitor the ventilation pressure and to keep it moderate (i.e., around 15 to 20 cmH2O) to prevent any barotrauma to the lungs. In addition, it is important to avoid restoring a void in the pleural cavity or re-expanding the lungs too aggressively, especially in patients whose lungs have been compressed for a prolonged period of time (e.g. large chest masses, chronic diaphragmatic hernias). Too rapid lung re-expansion exposes the patient to postoperative pulmonary oedema, which can be fatal. It is better to restore a moderate negative pressure in the pleural cavity at the end of surgery, allowing effective spontaneous ventilation of the patient in the immediate postoperative period, and progressively recreate the pleural void over 12 to 48 hours using the thoracic drain in place.
Thoracic drains
The choice of the side(s) of thoracostomy (chest) tube placement is made from radiographic views of the chest. Ultrasonography can also be useful to determine the optimal position of a chest drain, and it is widely used to assess loculation of the effusion and guide placement of small-bore catheters in human medicine1-4. Most commonly, chest tubes are placed under general anaesthesia. If the pleural effusion prompting placement of the tube(s) is causing respiratory impairment significantly increasing the anaesthetic risk, thoracocenteses are performed as necessary and the animal is optimised prior to chest tube placement.
Different types of tubes can be used as chest tubes. Commercially-available tubes are usually made of polyvinyl or silicone and contain a metal trocar-tipped stylet to facilitate placement. Many other types of tubes (e.g. feeding tubes) can be used as thoracostomy tubes and be placed with Carmalt-type forceps. When using non-specific tubes, additional holes need to be made, depending on the number of holes already present at the extremity of the tube. In this case, the length of the portion of the tube which will be inside the thoracic cavity must be anticipated so that no holes are located outside the thoracic cavity. Dedicated chest tubes usually are stiffer than other tubes, which eases their correct placement and make them more resistant to kinking and collapse. These stiffer tubes may however cause more discomfort than more supple ones. The widespread recommendations are to approximate the tube size to that of one of the mainstem bronchi, as seen on a lateral thoracic x-ray. This leads to using tubes ranging from 14 to 36 French, depending on the size of the patient. However, this rule should not be applied too rigidly and the tube size should also be adapted to the viscosity of the thoracic contents to be drained: smaller for air, intermediate for transudate or blood, larger for chyle or pus. Using tube which is larger than necessary will indeed induce more inflammation, which will itself be responsible for the production of thoracic effusion and discomfort. Recently, the use of small-bore chest tubes has gained interest in human medicine1, 2, 5 and has been found to be associated with lower complication rates than large-bore tubes placed under pressure. It has been studied in small animals and appeared to be efficacious and associated with minimal complications, even when used to drain viscous fluids such as pus6, 7. Such an approach is therefore worthy of consideration or, in the least, should engage to use smaller chest tubes than classically recommended.

28/36
To place a large-bore chest tube, the animal is positioned in lateral recumbency on the opposite side. The lateral aspect of the thorax is entirely clipped, extending over the cranial portion of the flank. It is then prepared for an aseptic procedure. Sterile surgical gloves are worn and sterile drapes are ideally used to cover the non-prepared areas of the body. The entire procedure is carried out in an aseptic manner.
The cutaneous and intercostal incisions must be staggered to reduce the risk of occurrence of a iatrogenic pneumothorax as the tube is inserted, left in place and after its removal. The skin incision is therefore always located a few centimetres caudodorsally to the site of penetration of the tube through the intercostal muscles, and the tube is tunnelled cranioventrally. It can be tunnelled directly under the skin or deeper, under the latissimus dorsi muscle8. In a cadaveric study, the use of trocar-implemented tubes tunnelled under the latissimus dorsi appeared the least prone to create a iatrogenic pneumothorax compared to trocar-implemented tubes tunnelled subcutaneously and Carmalt-forceps-implemented tubes tunnelled under the latissimus dorsi muscle or subcutaneously9. When a subcutaneous tunnel is chosen, 2 techniques exist to create it. The first technique is to make the cutaneous incision over the 2nd or 3rd intercostal space caudal to the intercostal space through which the tube should enter the thoracic cavity. The tunnel is then made by blunt dissection towards this targeted point of penetration. The second technique consists of having an assistant grab the skin over the craniolateral aspect of the thorax and pull it cranioventrally. The cutaneous incision is then made over the desired point of penetration of the thorax and the tube is then pushed into the thoracic cavity directly underneath this incision. When the skin is released, its movement in a caudodorsal direction will create the tunnel. Penetration of the tube inside the thorax is made by thrusting the trocar or Carmalt forceps through the thoracic wall, in the caudal portion of an intercostal space (i.e. immediately cranial to the caudal rib) to reduce the risk of injury to the intercostal artery, vein and nerve. This is usually done by hitting on the top of the trocar or Carmalt forceps to apply a brisk thrust. The penetration movement is perpendicular to the thoracic wall and must be controlled to minimise the risk of injury to the intrathoracic structures, especially the lungs. Less force is necessary to push trocar-implemented tubes through the thoracic wall which gives a better control of the movement, but the sharp tip of the trocar can damage intrathoracic structures more easily than Carmalt forceps. On the other hand, penetrating the thorax with Carmalt forceps requires considerable force, which makes precise control of the movement more difficult. In both cases, to avoid penetrating the thorax too deeply, the tube is grasped with the non-dominant hand 2 to 3 centimetres (corresponding to the desired depth of penetration) above the surface of the thoracic wall. This way, even on abrupt penetration of the chest, the length of instrument allowed to enter the chest will be limited. Once inside the thorax, the tube is advanced cranioventrally until its tip is expected to be immediately dorsal to the first sternebrae. With trocar-implemented tubes, this is done by withdrawing the trocar inside the tube, so that its sharp end is covered, and using the rigid trocar to orientate the tube in the right direction. The tube is then advanced along the trocar. With Carmalt-forceps implemented tubes, correctly positioning the tube can be more difficult, especially when the tube is very supple. The length of tube to insert is determined by measuring the distance between the cutaneous incision and the first sternebrae and marking the reported distance on the tube with a sterile marker. The tube will then be advanced until this mark comes flush with the skin incision. Alternatively, a second similar sterile tube can be used as a reference to ascertain that the appropriate length of tube is inside the thorax. The cutaneous incision is narrowed to march the size of the tube by placement of a purse-string or simple
29/36
suture. A wide simple suture can be placed around the tube midway between the skin incision and the point of intercostal penetration, to “close” the dissected tunnel around the tube. The chest tube is then secured by placement of a Chinese finger-trap suture. If a contralateral tube is needed, the tube is protected with a sterile padded dressing and the animal is positioned in lateral recumbency on the other side. The same procedure is repeated.
Correct placement of the tube(s) is controlled radiographically. Each tube exit point is disinfected, potentially protected with an antiseptic ointment (e.g. povidone ointment) and covered with dressings.
In tumour-related pleural disease, chest drains can be required to allow initial optimisation of the emergency patient. However, a thoracotomy is often required for definitive treatment and chest drains are then kept or placed during surgery for postoperative use, for drainage of the pleural cavity as well as intracavitary infusion of local anaesthetics or chemotherapeutic agents.
The chest tubes are then used for intermittent or continuous suction, depending on the type and amounts of air or fluids produced. When a tube is no longer needed, it is removed by simple traction after section of the finger-trap pattern suture. Its stoma is left to heal by second intention and need to be covered with a dressing for 24 to 48 hours. By then, it is usually sealed and airtight, and can be left uncovered. It is widely stated that the drain itself induces the production of 0.5 to 2 ml/kg/day of pleural fluid and that chest tubes should not be removed until less that 2 to 3 ml/kg/day of pleural effusion is drained. However, it has been showed that drains could be removed while the pleural effusion production was much greater than 3 ml/kg/day without incidence on the outcome, if data from clinical examination and clinical pathology supported their removal10. This shows that the amount of effusion produced is only one of many criteria to take into consideration in making the decision to remove chest drains.
Surgical approach
Lateral (intercostal) thoracotomy
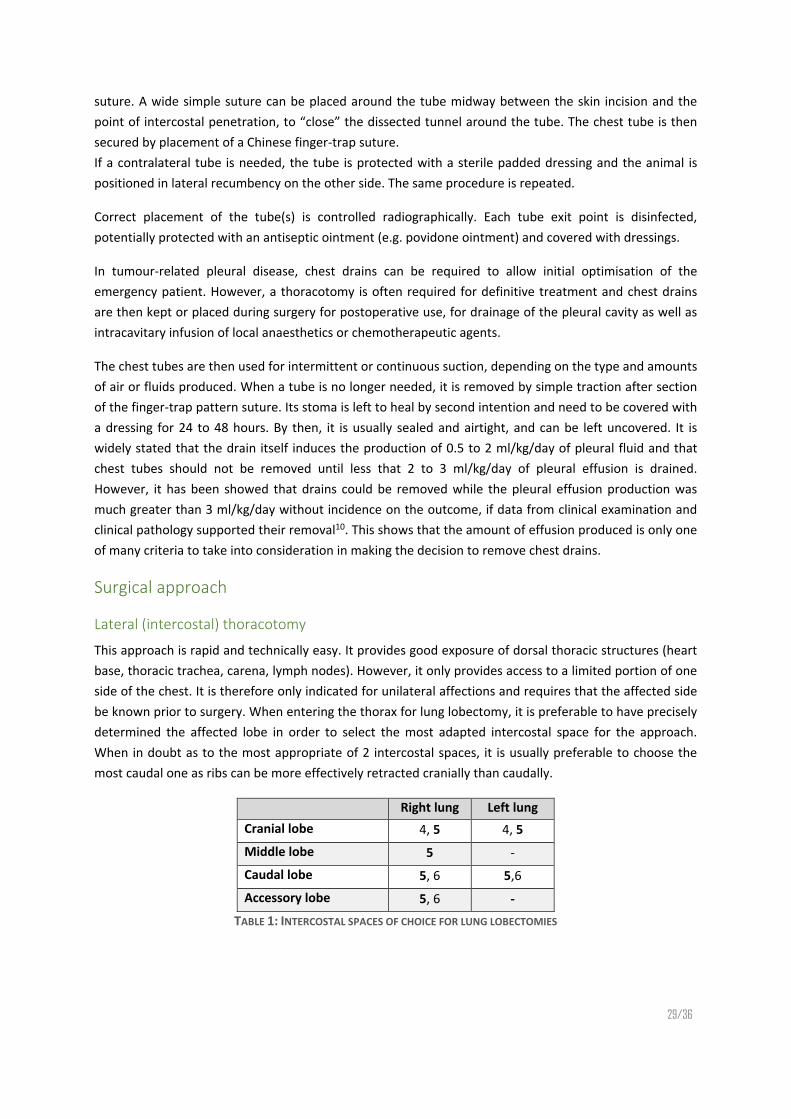
This approach is rapid and technically easy. It provides good exposure of dorsal thoracic structures (heart base, thoracic trachea, carena, lymph nodes). However, it only provides access to a limited portion of one side of the chest. It is therefore only indicated for unilateral affections and requires that the affected side be known prior to surgery. When entering the thorax for lung lobectomy, it is preferable to have precisely determined the affected lobe in order to select the most adapted intercostal space for the approach. When in doubt as to the most appropriate of 2 intercostal spaces, it is usually preferable to choose the most caudal one as ribs can be more effectively retracted cranially than caudally.
Right lung Left lung Cranial lobe 4, 5 4, 5 Middle lobe 5 - Caudal lobe 5, 6 5,6 Accessory lobe 5, 6 -
TABLE 1: INTERCOSTAL SPACES OF CHOICE FOR LUNG LOBECTOMIES

30/36
Right Left Heart, pericardium 4, 5 4, 5 PDA, PRAA 4, 5 Oesophagus (cranial) 3, 4 Oesophagus (caudal) 7 – 9 7 - 9 Thoracic duct (dog) 8-10 Thoracic duct (cat) 8-10
TABLE 2: INTERCOSTAL SPACES OF CHOICE TO REACH INTRATHORACIC STRUCTURES
For a lateral intercostal thoracotomy, the animal is placed in lateral recumbency opposite to the side to be operated (Figure 1). The affected hemithorax is entirely clipped and prepared for aseptic surgery. The ipsilateral thoracic limb is maintained mildly protracted to expose the cranial portion of the thoracic wall. The chosen intercostal space is identified by palpation. The skin and cutaneous trunci muscle are incised along this intercostal space. The latissimus dorsi muscle is then visible. It can either be retracted dorsally, which has my preference, or incised in its ventral portion, parallel to the underlying intercostal space. The bellies of the serratus ventralis muscle surrounding the chosen intercostal space are separated and ventrally, depending on the location, the scalenus or external oblique muscle is incised. The thoracic cavity is entered by blunt dissection through the intercostal muscles and the parietal pleura. This creates a pneumothorax, allowing the ipsilateral lung to fall away from the thoracic wall and thereby decreasing the risk of iatrogenic injury during the rest of the approach. The intercostal muscles of the selected intercostal space are then sectioned along a line parallel to this space, in its caudal half (closer from the cranial border of the caudal rib than from the caudal border of the cranial rib), to avoid iatrogenic injury to the intercostal nerve, artery and vein. Ventrally, attention is paid not to damage the internal thoracic artery and vein, which course inside the thoracic cavity. The borders of the rib next to the open intercostal space are protected with moist swabs and an autostatic retractor (e.g. Finochietto) is used to spread this space open.
When the intrathoracic step of the procedure is completed, a chest tube is placed under direct visual control (Figure 2). The retractor is removed and the thoracic cavity is closed by placing sutures around the ribs defining the open intercostal space. Monofilament absorbable sutures can be used to this purpose. Attention is paid not to damage the intercostal nerve, artery and vein caudal to the caudal rib when passing the suture caudal to it. In addition, care is taken not to overtighten the sutures to avoid maintaining the ribs around the open intercostal space too close, which is likely to cause unnecessary pain in the postoperative period. The latissimus dorsi muscle is either release or sutured, and the more superficial layers are closed routinely.

31/36
FIGURE 9: LATERAL THORACOTOMY11
FIGURE 10: LATERAL THORACOTOMY CLOSURE11
Median sternotomy
For a median sternotomy, the animal is placed in dorsal recumbency (Figure 3). The ventral ⅔ to ¾ of the thorax, caudal portion of the neck and cranial portion of the abdomen are clipped and prepared for aseptic surgery. The skin is incised on the ventral midline above the sternum. The sternum is exposed on the midline by minimal elevation of the insertions of the pectoral muscles on it. The sternum is then divided longitudinally using an oscillating saw, under constant irrigation to prevent thermic osteonecrosis.

32/36
As rapidly as possible, a small retractor (e.g. Gelpi) is placed in the wound and the interior of the thoracic cavity is palpated to ascertain the absence of adhesions and minimise the risks of iatrogenic injury to intrathoracic organs during the rest of the approach. Whenever possible, efforts are made to avoid dividing the entire length of the sternum. Leaving the cranial-most or caudal-most portion of the sternum intact, and possibly both, will markedly increase the stability of the sternal closure in the postoperative period and reduce the risks of wound healing complications. When the sternum is divided, the borders of the wound are protected with moist swabs and an autostatic retractor is placed to maintain the wound open.
FIGURE 11: MEDIAN STERNOTOMY11
When the intrathoracic step of the surgery is completed, a chest drain is placed under direct visual control and the sternum is repaired by placement of sutures or wire in a figure of eight around the sternebrae (Figure 4). Closing the sternum with metallic wires is preferred by some authors on the account that it provides a more rigid and stable repair, especially in large dogs12. I tend to use large non-absorbable monofilament sutures (e.g. polypropylene), irrespective of the dog’s size, provided at least one of the sternum extremities (manubrium or xiphoid sternum) could be left intact. The more superficial layers are closed in a routine fashion.

33/36
FIGURE 12: MEDIAN STERNOTOMY CLOSURE11
Thoracoscopy
Thoracoscopy is used in small animal surgery for an increasing range of diagnostic and therapeutic purposes13-16. Diagnostic procedures include visual inspection of the thoracic cavity and thoracoscopic biopsies (e.g. masses, pleura, lymph nodes, lungs). An increasing number of therapeutic procedures have also been reported, including partial and total lung lobectomies, pericardectomy, thoracic duct ligation, tumour resections (e.g. thymoma, atrial tumour) and correction of vascular abnormalities (patent ductus arteriosus, persistent right aortic arch). The description of these techniques is beyond the scope of this text and the reader is referred elsewhere for further information13-18.
Lung lobectomies
Partial lung lobectomy
Partial lung lobectomies are performed to preserve a portion of a lung lobe whilst excising its apical portion to resect a focal lesion or obtain a large biopsy. Such biopsies can be performed by placement of overlapping sutures, both haemostatic and pneumostatic (Figure 1a). Alternatively, several rows of staggered matress sutures can be used for the same effect (Figure 1b). Partial lobectomies can also be performed using automatic sutures, which is quicker and technically easier. Thoracoabdominal (TA) and gastrointestinal (GIA) staplers are most appropriate for this purpose. After resection of a portion of a lung lobe, the airtightness of the sutures are tested by pouring a warm sterile isotonic solution in the thoracic cavity until the pulmonary section line in immerged. Whilst the section is immerged, the patient is mechanically ventilated and the fluid in the chest is inspected for signs of air bubbles. IF such bubbles are detected, the section is inspected to localise the source of the air leakage and additional mattress sutures are placed to seal the wound. Before closure of the thoracic cavity, the accessible lymph nodes are inspected and preferably biopsied.
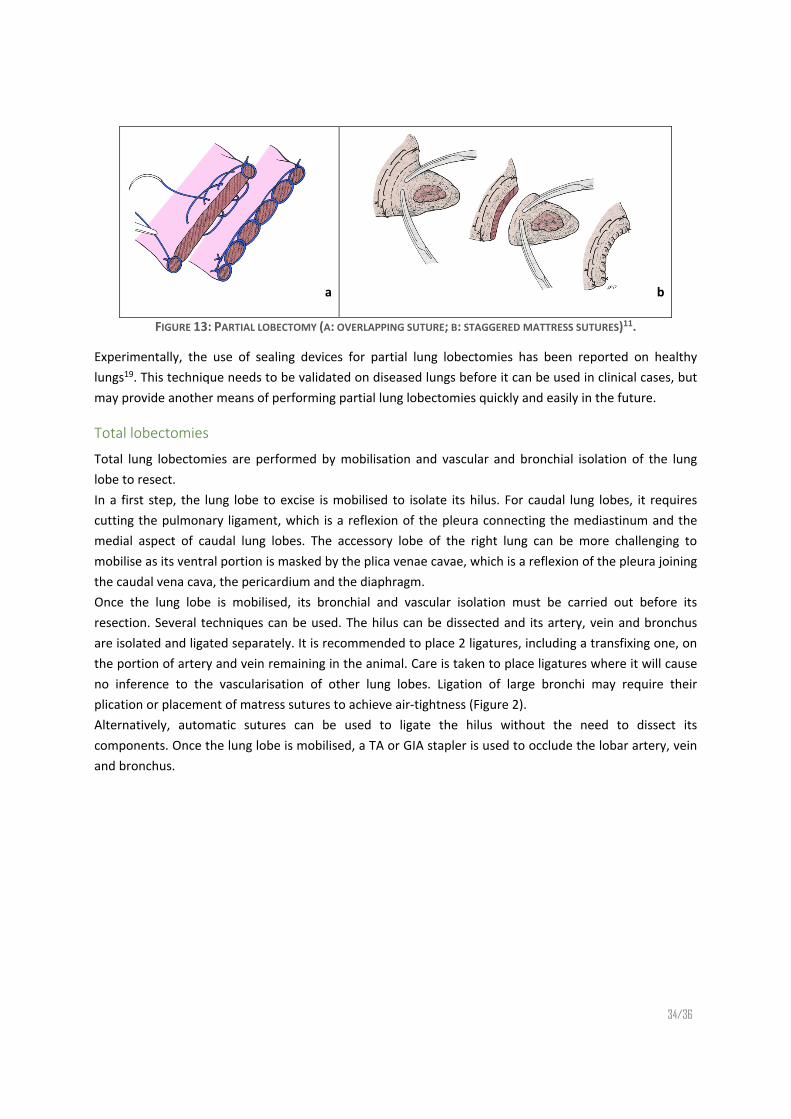
34/36
a b
FIGURE 13: PARTIAL LOBECTOMY (A: OVERLAPPING SUTURE; B: STAGGERED MATTRESS SUTURES)11.
Experimentally, the use of sealing devices for partial lung lobectomies has been reported on healthy lungs19. This technique needs to be validated on diseased lungs before it can be used in clinical cases, but may provide another means of performing partial lung lobectomies quickly and easily in the future.
Total lobectomies
Total lung lobectomies are performed by mobilisation and vascular and bronchial isolation of the lung lobe to resect. In a first step, the lung lobe to excise is mobilised to isolate its hilus. For caudal lung lobes, it requires cutting the pulmonary ligament, which is a reflexion of the pleura connecting the mediastinum and the medial aspect of caudal lung lobes. The accessory lobe of the right lung can be more challenging to mobilise as its ventral portion is masked by the plica venae cavae, which is a reflexion of the pleura joining the caudal vena cava, the pericardium and the diaphragm. Once the lung lobe is mobilised, its bronchial and vascular isolation must be carried out before its resection. Several techniques can be used. The hilus can be dissected and its artery, vein and bronchus are isolated and ligated separately. It is recommended to place 2 ligatures, including a transfixing one, on the portion of artery and vein remaining in the animal. Care is taken to place ligatures where it will cause no inference to the vascularisation of other lung lobes. Ligation of large bronchi may require their plication or placement of matress sutures to achieve air-tightness (Figure 2). Alternatively, automatic sutures can be used to ligate the hilus without the need to dissect its components. Once the lung lobe is mobilised, a TA or GIA stapler is used to occlude the lobar artery, vein and bronchus.

35/36
FIGURE 14: TOTAL LUNG LOBECTOMY11
Similarly to what is done after partial lobectomy, the airtightness of the sutures is tested by their immersion in warm isotonic solution poured in the thoracic cavity. Again, the accessible lymph nodes are inspected and biopsied as required.

36/36
References
1. Light R. Pleural Controversy: Optimal Chest Tube Size for Drainage. Respirology. 2010. 2. Horsley A, Jones L, White J, Henry M. Efficacy and complications of small-bore, wire-guided chest drains. Chest. 2006;130: 1857-1863. 3. Sahin U, Unlu M, Akkaya A, Ornek Z. The value of small-bore catheter thoracostomy in the treatment of malignant pleural effusions. Respiration. 2001;68: 501-505. 4. Parulekar W, Di Primio G, Matzinger F, Dennie C, Bociek G. Use of small-bore vs large-bore chest tubes for treatment of malignant pleural effusions. Chest. 2001;120: 19-25. 5. Taylor PM. Catheters smaller than 24 French gauge can be used for chest drains. BMJ. 1997;315: 186. 6. Frendin J, Obel N. Catheter drainage of pleural fluid collections and pneumothorax. Journal of
Small Animal Practice. 1997;38: 237-242. 7. Valtolina C, Adamantos S. Evaluation of small-bore wire-guided chest drains for management of pleural space disease. Journal of Small Animal Practice. 2009;50: 290-297. 8. Monnet E. Pleura and pleural space. In: Slatter DH (ed): Textbook of small animal surgery. Philadelphia, Pa. ; London: W. B. Saunders, 2003;387-405. 9. Yoon HY, Mann FA, Lee SH, Branson KR. Comparison of the amounts of air leakage into the thoracic cavity associated with four thoracostomy tube placement techniques in canine cadavers. American Journal of Veterinary Research. 2009;70: 1161-1167. 10. Marques AIDC, Tattersall J, Shaw DJ, Welsh E. Retrospective analysis of the relationship between time of thoracostomy drain removal and discharge time. Journal of Small Animal Practice. 2009;50: 162-166. 11. Monnet E. Lungs. In: Tobias KM, Johnston SA (eds): Veterinary surgery : small animal. St. Louis, Mo.: Elsevier, 2012;1752-1768. 12. Pelsue DH, Monnet E, Gaynor JS, Powers BE, Halling K, Parker D, et al. Closure of median sternotomy in dogs: suture versus wire. J Am Anim Hosp Assoc. 2002;38: 569-576. 13. Tams TR, Rawlings CA. Small animal endoscopy. St. Louis, Mo. ; London: Mosby, 2011. 14. McCarthy TC. Veterinary endoscopy for the small animal practitioner. Philadelphia, Pa. ; London: Elsevier Saunders, 2005. 15. Schmiedt C. Small Animal Exploratory Thoracoscopy. Veterinary Clinics of North America: Small
Animal Practice. 2009;39: 953-964. 16. Monnet E. Interventional Thoracoscopy in Small Animals. Veterinary Clinics of North America:
Small Animal Practice. 2009;39: 965-975. 17. Mayhew P. Surgical views: thoracoscopy: common techniques in small animals. Compendium
Continuing Education for Veterinarians. 2013;35: unpaginated. 18. Mayhew P. Surgical views: thoracoscopy: basic principles, anesthetic concerns, instrumentation, and thoracic access. Compendium Continuing Education for Veterinarians. 2013;35: unpaginated. 19. Mayhew PD, Culp WTN, Pascoe PJ, Arzi NV. Use of the ligasure vessel-sealing device for thoracoscopic peripheral lung biopsy in healthy dogs. Veterinary Surgery. 2012;41: 523-528.