updated treatment approach of the shoulder girdle complex
TRANSCRIPT

3/30/2016
1
Updated Treatment Approach of the Shoulder Girdle Complex as
it Relates to Regional Interdependence with the
Cervical Spine
Julie Whitbeck, PT DMT OCS FAAOMPT COMT
Julie Whitbeck, PT DMT OCS FAAOMPT COMT
Objectives
• Participants will understand regional interdependence concepts for the upper quarter.
• Participants will identify evaluation techniques to rule in/out cervical involvement or origin of symptoms as it relates to shoulder girdle symptoms.
• Participants will take the differential diagnosis knowledge and apply it to treatment strategies with incorporating overflow concepts.
• Participants will learn basic exercise dosage principles and qualities based on deficits identified.
3/30/2016
2
Regional Interdependence
• What is it?
• “Refers to the concept that seemingly unrelated impairments in a remote anatomical region may contribute to, or be associated with, the patient’s primary complaint”
• Wainner et al. 2007
• Biomechanical model of assessment and treatment
• Test-treat-retest approach
Types of Pain
• Referred pain: Pain that is perceived in a location other than the actual site of stimulus or the tissue symptom generator
• Radicular pain: Pain that originates from the spinal nerve and symptoms are experienced remotely along the nerve root distribution.
• Somatovisceral pain: May be a source of referred pain or mimic musculoskeletal pain
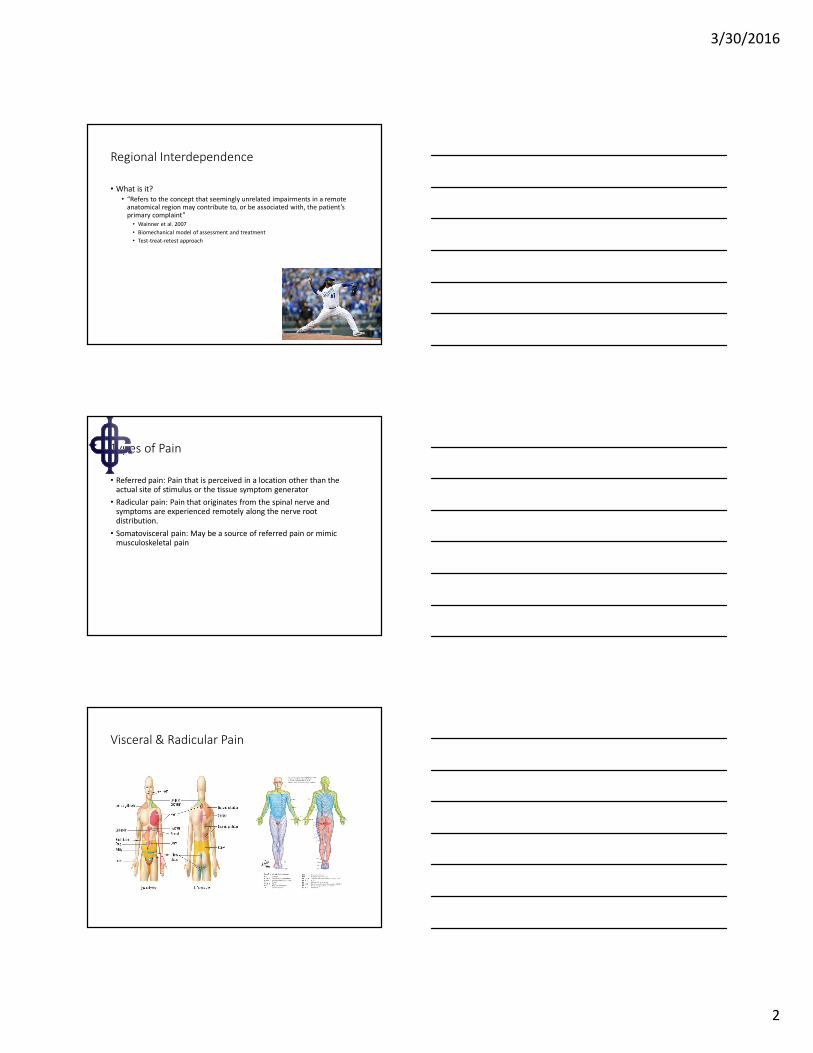
Visceral & Radicular Pain

3/30/2016
3
Example of Cervical Pain Patterns
Biomechanical Model
• Hypomobility vs. hypermobility
• Alignment/Posture
• Tissue trauma
• Meniscoid entrapment
• Steindler (1955) proposed ‘Kinetic Chain’ and described how movement at one joint can affect joints above or below-i.e. Decreased DF at the talocrural joint may produce biomechanical compensation in the knee and hip
• Pitfalls to this approach: only transient biomechanical effects are supported in the literature with studies that quantify motion, not lasting positional changes; biomechanical assessment is not reliable; joint biased techniques are dissipated over large area; forces between clinicians are not reproducible, etc
Controversy
• Bialosky et al. (2009) questioned the underlying mechanisms of RI in a commentary to Wainner et al. article (2007)
• Suggested the biomechanical model did not explain the mechanisms behind the relationships within the musculoskeletal system
• Original RI defined musculoskeletal system as primary source and manifestations of impairments
• RI concepts may have underlying neurophysiological basis and or the combination of the two (biomechanical and neurophysiological)
• Importance of combining theories may yield dose dependent neurophysiological responses

3/30/2016
4
Neurophysiological Model
• Facilitated segment
• Central sensitization
• Nerve root entrapment or compression
• CRPS
• Pitfalls: nerve biased techniques are not specific to a single nerve
• Responses are based on those originating from peripheral mechanisms, spinal cord mechanisms, and/or supraspinalmechanisms
• Fernandez-de-las-Penas et al (2007) conducted a study with results supporting activation of central structures since unilateral manipulation at C5-C6 produced bilateral response at the elbows for increase in PPT in healthy subjects
RI redefined
RI Redefined
• “The concept that a patient’s primary musculoskeletal system(s) may be directly or indirectly related or influenced by impairments from various body regions and systems regardless of proximity to the primary symptom(s)”
• Functional movement patterns originate from more than one joint/region, so why not target asymptomatic regions for relief at the primary site of pain?
Sueki et al 2013

3/30/2016
5
Case Study
• Prolonged sitting or physical inactivity is an epidemic and are identified as risk factors for work related symptoms
• Example: Stephen-35 y/o who presents with script of left shoulder impingement; insidious onset of pain x 3 months
• Symptoms: 8/10 pain, radicular N/T/pain along ulnar nerve distribution, patient frequently observed to stretch his neck
• AROM: Shdr flexion:160, abduction: 180, ER: 88. Cervical flexion:17, extension: 30, R SB: 17, L SB: 25, R rot: 42, L rot: 50. PROM: Cspflexion: reproduces radiculopathy, ext & R SB caused sharp pain in lateral shoulder, R rot: tingling L thumb.
• MMT: Shoulder: WNL all planes. Weak Csp SB and rotation in sidelying; ext & L SB aggravate L shoulder symptoms
Link Between Cervical Spine & Shoulder
• Sobel et al (1996): more than 40% of patients with shoulder complaints have impairments of the cervicothoracic spine and adjacent ribs

3/30/2016
6
Link Between Cervical Spine & Elbow
• Vicenzino et al. (1996) revealed increased pain-free grip strength, pressure pain threshold, and increased shoulder abduction during a neurodynamic test of the radial nerve, and pain scores after manipulative therapy to the C5-C6 level. (15 subjects)
• Vicenzino and Wright (1996): 90% of subjects with lateral elbow pain had segmental hypomobility in the lower cervical spine
Martinez-Segura et al (2012): Randomized Clinical Trial. Cervical and Thoracic Manipulation & Distal Effects
• Examined cervical and thoracic manipulation and effect on pain pressure threshold, reported neck pain, and cervical ROM in subjects w bilateral chronic mechanical neck pain. One treatment was assessed.
• PPT was assessed bilaterally at the C5-C6 zygapophyseal joint, lateral epicondyle, and tibialis anterior
• Results: Effects of cervical and thoracic manipulation were similar when looking at above symptoms
• Differed from Fernandez-Carnero et al study (2011) where they found cervical manipulation produced greater increases in PPT at the lateral epicondyle as compared with thoracic. Their study recruited subjects that had lateral epicondylalgia rather than neck pain, which may account for differences
Cervical vs. Thoracic Spine Manual Therapy
• Cleland et al (2005)-Tsp manip and neck pain: Study was a RCT with 36 symptomatic patients with mechanical neck pain. 2 groups: 1 placebo manip, other supine Tsp manip at restricted levels. Patients receiving Tsp manip had immediate improvements in pain as compared w placebo group. Results do not suggest avoiding Cspmanip, but offers good alternative w Tsp manip.
• Gonzalez-Iglesias et al (2009)-Tsp manip and neck pain
• Many therapists prefer thoracic manipulation over cervical due to small risks involved
• Benefit vs. risk analysis

3/30/2016
7
Norlander et al studies-Upper Quarter Relationship
• Correlation between mobility at CT junction and thoracic spine with neck-shoulder pain
• Utilized cross sectional study (142 male & 139 female workers) revealed hypomobility at C7-T1 and T1-T2 significantly predicted neck-shoulder pain and symptom weakness in the hands
• Positive predictive value of 84% (prospective 2 yr study)
Link Between Thoracic Spine & Shoulder
• Sueki and Chaconas (2011)-Tsp manip and shdr function
• Winters et al (1997)–shdr pain was attributable to dysfunctions in Csp, upper Tsp, or ribs
• McCormack (2012)-a single case report w patient that had adhesive capsulitis and benefited from added Tsp manip
• Crosbie et al (2008) completed a study of healthy individuals revealing thoracic spine motion with unilateral or bilateral shoulder elevation
• Case study-6 anchor repair-47 y/o male

3/30/2016
8
Haik et al (2014)
• Examined scapular kinematics and pain levels pre and post thoracic spinal manipulation with individuals with and without shoulder impingement symptoms
• Compares thoracic manipulation to sham manipulation
• Results: Pain immediately decreased during arm elevation and lowering following single session to mid thoracic spine in subjects with SIS (60% w thoracic vs 36% w sham manipulation)
• Immediate effects of upward rotation independent of shoulder symptoms following thoracic manipulation
Strunce et al study (2009)
• 21 participants with primary complaints of shoulder pain
• 1 of 4 techniques used based on assessment and identified restrictions: Seated distraction CT manipulation, supine unilateral rib manipulation, supine flexion manipulation, or prone extension manipulation
• Physical exam: 71% had CT restrictions, 100% had upper thoracic flexion restrictions, 7% had thoracic extension restrictions, 79% had unilateral rib restrictions
• Results: Statistically and clinical improvements in entire group regarding shoulder ROM and VAS scores: Flexion: 106.8 (145.2), abduction: 98 (135.7), rotation: 128.3 (157.8); VAS 63.1 (31.2)
• Why?: Biomechanical changes allowing for greater shoulder ROM with OH motions, restoration of normal neurophysiological motor control of the shoulder girdle, or hypoalgesic effect of manipulation may decrease overall pain and allow for greater ROM
Muth et al (2012) Study-Changes w Scapular Kinematics and Thoracic Manipulation
• 36 subjects with signs of RTC pathology
• Humeral elevation was loaded (weight determined by body weight) and assessed in relation to the thoracic sensors and is referred to as “humero-thoracic elevation”
• Subjects received mid thoracic and CT junction manipulation in seated position
• Significant decrease in scapular upward rotation noted following manipulation and increase in middle trap activity
• Significant improvement in pain with performance of provocative tests and RTC pathology and with loaded elevation following manipulation
• No other changes in scapular kinematics were noted; no change in humerothoracic elevation
• Improved shoulder function at follow-up 7-10 days after the manipulation

3/30/2016
9
Boyles et al (2009) study: SIS Treated w Mid Thoracic & CT Manipulation
• 56 subjects with SIS, all received mid thoracic HVLA in addition to CT junction in seated position. Subjects with rib angle tenderness also received a rib manipulation in supine at the level of tenderness.
• No control group or randomization of subjects
• Results: Thoracic manipulation treatment is correlated with significant changes in pain and disability at the 48 hour follow-up
Bergman et al study (2004): Usual Medical Care & Manipulative Therapy
• Randomly assigned subjects with primary reports of shoulder pain into 2 groups
• 1 group received usual medical care from PCP
• 2nd group received usual medical care + manipulative therapy directed at CT spine and adjacent rib cage
• Results: no difference between groups at the 6 week mark, however, the 2nd group demonstrated significantly higher rates of full recovery and more improvement in the severity of primary complaints and disability at the 12, 26, and 52 week follow-up
• Is there a subgroup of patients that benefit to these interventions?
Mintken et al study (2010):Are there prognostic factors to identify patients with shoulder pain who would benefit from thrust and non-thrust manipulation?
• Treatment outcome was the reference criterion, so all subjects (80 in total) received the same treatment regardless of exam findings-1 non-thrust mobilization directed at lower cervical spine (C5-C7 in neutral and slight flexion) and 5 different thrust techniques at the thoracic spine (received thrust techniques twice)
• Results: 61% experienced a successful outcome by 3rd session
• 5 prognostic variables: pain-free shoulder flexion <127 degrees, shoulder IR <53 degrees, (-) Neer test, not taking medications of any kind for shoulder pain, and duration of symptoms <90 days
• If 3 of 5 variables present, likelihood of success was 89% and if 4 of 5 variables were present the likelihood of success was 100%

3/30/2016
10
Link Between Thoracic Spine & Elbow
• Berglund et al (2008):Purpose of the study was to determine the prevalence of cervical and/or thoracic pain in subjects with and without lateral elbow pain.
• 70% of subjects in the experimental group with lateral elbow pain had cervical and/or thoracic pain as compared with 16% in the control group
• Frequency of positive responses to provocative tests of cervical and thoracic spine were significantly higher
• Frequency of positive responses to neurodynamic tests of the radial nerve
• Cervical AROM into flexion and extension were significantly lower as compared with control group
Examination Techniques To Rule In/Out Cervical Spine
• Cluster of tests to implicate cervical radiculopathy: ULTT A (median nerve bias), Spurling test, Distraction test, cervical rotation <60 degrees to the ipsilateral side
• Examine segmental mobility of the cervical and thoracic spines
• Test recruitment patterns and endurance of deep cervical flexor muscles with supine cervical flexion test and supine break test, deep cervical flexor endurance test, resisted MMT in all planes for cervical spine in 3 positions
• Go thru full screen with evaluation
Examination
• Initial observation
• History and interview
• Structural inspection
• AROM
• PROM
• Resisted movements
• Palpation
• Neurology
• Special tests
• Mobility testing
• Review of diagnostics

3/30/2016
11
Treatment Strategies & Overflow Concepts
• Research has yet to define optimal dosing, treatment techniques or patient populations to apply the RI approach to
• Treatment must consider passive restraints as well as neuromuscular control-i.e. hypermobility vs. instability vs. hypomobility
• Combination of biomechanical and neurophysiological
• Resolve adjacent hypomobilities in the presence of hypermobilitiesto allow for proper afferent feedback and motor facilitation to resolve impaired motor patterns-manual therapy followed by exercise
General vs. Specific Training
• Multi-resistance training: Patient position, gravitational forces, type of resistance (pulleys, bands, hand weights), isometric vs dynamic movements, direction of force
Manual Therapy Lesion
• 1. Collagen Trauma
• 2. Receptor Damage
• 3. Reduced Muscle Fiber Recruitment
• 4. Tonic Fiber Atrophy
• 5. Reduced Anti-Gravity Stability
• 6. Motion Around Non-Physiological Axis
• 7. Trauma/Acute Locking/Degeneration
• 8. Pain/Guarding

3/30/2016
12
Exercise Dosing Principles
• Bialosky et al (2009) refers to neurophysiological responses being dose dependent
• Goals of treatment: Provide optimal stimulus for tissue repair, eliminate impairments, restore function
• Address postural alignment, restore ROM around a physiological axis, restore coordination/motor control, improved endurance and strength
• Target correct plane of motion, key muscles, dosage for desired outcome, and address angle of motion for optimal recruitment
Shoulder Flexion Is Not Treated Equally
Exercise Dosing
• Mobilization: assisted to <50% 1 RM, 1-5 sets, 10-60 reps
• Vascularity: 55-65% 1 RM, 1-3 sets, 25-30 reps
• Coordination: <50% 1 RM, 2-5 sets, 30-50 reps, daily
• Endurance: 60% 1 RM, 1-3 sets, 24-30 reps
• Strength: 60-80% 1 RM, 1-3 sets, 6-12 reps
• Volume (hypertrophy): 70% 1 RM, 12-15 reps
• Power: >80%, 1-3 sets, 3-6 reps, 1x/week

3/30/2016
13
Take Home Message
• Consider joints adjacent to reported symptoms as well as other systems to be source generator during assessment
• Seek to identify the pathoanatomical tissues that may be the source generator
• RI model should be viewed as holistic approach to assessment and treatment, combining models of pathology for improved outcomes
• Regional exam and treatment approach in addition to local treatment may lead to more efficient and effective treatment and outcomes.
• Why does any of this matter? Cost of healthcare, less visits approved, better outcomes
Thank You

3/30/2016
14
Berglund KM, Persson BH, Denison E. Prevalence of pain and dysfunction in the cervical and thoracic spine in persons with and
without lateral elbow pain. Manual Therapy. 2008;13(4):295-299.
Bergman GJD, Winters JC, Groenier KH, et al. Manipulative therapy in addition to usual medical care for patients with shoulder
dysfunction and pain: a randomized controlled trial. Ann Intern Med. 2004;141:432-439.
Bialosky JE, Bishop MD, Price DD, Robinson ME, George SZ. The mechanisms of manual therapy in the treatment of musculoskeletal
pain: a comprehensive model. Manual Therapy. 2009;14(5):531-538.
Boyles RE, Ritland BM, Miracle BM, Barclay DM, Faul MS, Moore JH, et al. The short-term effects of thoracic spine thrust
manipulation on patients with shoulder impingement syndrome. Manual Therapy. 2009;14(4):375-380.
Cleland JA, Childs JD, McRae M, Palmer JA, Stowell T. Immediate effects of thoracic manipulation in patients with neck pain: a
randomized clinical trial. Manual Therapy. 2005;10(2):127-135.
Crosbie J, Kilbreath SL, Hollmann L, York S. Scapulohumeral rhythm and associated spinal motion. Clin Biomech. 2008;23:184-192.
Deschenes MR, Kraemer WJ. Performance and physiologic adaptations to resistance training. Am J Phys Med Rehabil. 2002;81(11
suppl):S3-16.
Dishman JD, Burke J. Spinal reflex excitability changes after cervical and lumbar spinal manipulation: a comparative study. Spine.
2003;3:204-212.
Domenech MA, Sizer PS, Dedrick GS, McGalliard MK, Brismee JM. The deep neck flexor endurance test: normative data scores in
healthy adults. PM R. 2011;3(2):105-110.
Falla D, Jull GA, Edwards S, Koh K, Rainoldi A. Neuromuscular efficiency of the sternocleidomastoid and anterior scalene muscles in
patients with chronic neck pain. Disabil Rehabil. 2004;26(12):712–717.
References
Falla D, Jull GA, Hodges PW. Patients with neck pain demonstrate reduced electromyographic activity of the deep cervical flexor muscles
during performance of the craniocervical flexion test. Spine. 2004;29(19):2108–2114.
Falla D, O'Leary S, Farina D, Jull G. Association between intensity of pain and impairment in onset and activation of the deep cervical
flexors in patients with persistent neck pain. Clin J Pain. 2011;27(4): 309-314.
Fernandez-Carnero J, Cleland JA, La Touche Arbizu R. Examination of motor and hypoalgesic effects of cervical vs thoracic spine
manipulation in patients with lateral epicondylalgia: a clinical trial. J Manipulative Physiol Ther. 2011;34:432-440.
Fernandez-de-las-Penas C, Perez-De-Heredia M, Brea-Rivero M, Miangolarra-Page JC. Immediate effects of pressure pain threshold
following a single cervical spine manipulation in healthy subjects. J Orthop Sports Phys Ther. 2007;37(6):325-329.
Gonzalez-Iglesias J, Fernandez-de-las-Penas C, Cleland JA, Gutierrez-Vega Mdel R. Thoracic spine manipulation for the management of
patients with neck pain: a randomized clinical trial. J Ortho Sports Phys Ther. 2009;39(1):20-27.
Grimsby O, Rivard J. Science, Theory and Clinical Application in Orthopaedic Manual Physical Therapy: Volume 1. 2008.
Haik MN, Alburquerque-Sendin F, Silva CZ, Siqueira-Junior AL, Ribeiro IL, Camargo PR. Scapular kinematics pre- and post-thoracic thrust
manipulation in individuals with and without shoulder impingement symptoms: A randomized controlled study. J Orthop Sports Phys Ther.
2014;44(7): 475-487.
Harris KD, Heer DM, Roy TC, Santos DM, Whitman JM, Wainner RS. Reliability of a measurement of neck flexor muscle endurance.
Physical Therapy. 2005;85(12):1349-1355.
Herzog W, Scheele D, Conway PJ. Electromyographic responses of back and limb muscles associated with spinal manipulative therapy.
Spine. 1999;24:146-152.
Johansson H, Sojka P. Pathophysiological mechanisms involved in genesis and spread of muscular tension in occupational muscle pain and
in chronic musculoskeletal pain syndromes: a hypothesis. Med Hypotheses. 1991;35(3):196-203.
Korr IM. The neural basis of the osteopathic lesion. J Am Osteopath Assoc. 1947;47:191-198.
Kraemer WJ, Adams K, Cafarelli E, et al. American College of Sports Medicine position stand. Progression models in resistance training for
healthy adults. Med Sci Sports Exerc. 2002;34(2):364-380.
Kraemer WJ, Newton RU. Training for muscular power. Phys Med Rehabil Clin N Am. 2000;11(2):341-368.
Martinez-Segura R, De-La-Llave-Rincon AI, Ortega-Santiago R, Cleland JA, Fernandez-de-las-Penas C. Immediate changes in widespread
pressure pain sensitivity, neck pain, and cervical range of motion after cervical or thoracic thrust manipulation in patients with bilateral
chronic mechanical neck pain: A randomized clinical trial. J Orthop Sports Phys Ther. 2012;42(9):806-814.
McCormack JR. Use of thoracic spine manipulation in the treatment of adhesive capsulitis: a case report. J Man Manipulative Therapy.
2012;20(1): 28-34.
Mintken PE, Cleland JA, Carpenter KJ, Bieniek ML, Keirns M, Whitman JM. Some factors predict successful short-term outcomes in
individuals with shoulder pain receiving cervicothoracic manipulation: a single-arm trial. Physical Therapy. 2010;90(1):26-42.
Muth S, Barbe MF, Lauer R, McClure P. The effects of thoracic spine manipulation in subjects with signs of rotator cuff tendinopathy. J
Orthop Sports Phys Ther. 2012;42(12): 1005-1016.
Norlander S, Aste-Norlander U, Nordgram B, Sahlstedt B. Mobility in the cervico-thoracic motion segment: an indicative factor of
musculoskeletal neck-shoulder pain. Scandinavian Journal of Rehabilitation Medicine. 1996;28(4):183-192.
Norlander S, Gustavsson BG, Lindell J, Nordgren B. Reduced mobility in the cervico-thoracic motion segment-a risk factor for
musculoskeletal neck-shoulder pain: a two-year prospective follow-up study. Scandinavian Journal of Rehabilitation Medicine.
1997;29(3):167-174.
Norlander S, Nordgren B. Clinical symptoms related to musculoskeletal neck-shoulder pain and mobility in the cervico-thoracic spine.
Scandinavian Journal of Rehabilitation Medicine. 1998;30(4):243-251.
O'Leary S, Falla D, Jull G, Vicenzino B. Muscle specificity in tests of cervical flexor muscle performance. J Electromyogr Kinesiology.
2007;17(1):35-40.
Pickar JG, Wheeler JD. Response of muscle proprioceptors to spinal manipulative-like loads in the anesthetized cat. J Manipulative
Physiol Ther. 2001;24:2-11.
Sobel JS, Kremer I, Winters JC, et al. The influence of the mobility in the cervicothoracic spine and the upper ribs (shoulder girdle) on the
mobility of the scapulohumeral joint. J Manipulative Physiol Ther. 1996;19:469-474.
Steindler A. Kinesiology of the human body: under normal and pathological conditions. Springfield (IL): Charles C Thomas; 1955.

3/30/2016
15
Strunce JB, Walker MJ, Boyles RE, Young BA. The immediate effects of thoracic spine and rib manipulation on subjects with primary
complaints of shoulder pain. J Man Manip Ther. 2009;17(4):230-236.
Sueki DG, Chaconcas EJ. The effect of thoracic manipulation on shoulder pain: a regional interdependence model. Physical Therapy.
2011:16(5):399-408.
Sueki DG, Cleland JA, Wainner RS. A regional interdependence model of musculoskeletal dysfunction: research, mechanisms, and clinical
implications. J Man Manip Ther. 2013;21(2):90-102.
Vicenzino B, Collins D, Benson H, Wright A. An investigation of the interrelationship between manipulative therapy-induced hypoalgesia
and sympathoexcitation. J of Manipulative Physiol Ther. 1998;21(7):448-453.
Vicenzino B, Collins D, Wright A. The initial effects of a cervical spine manipulative physiotherapy treatment on the pain and dysfunction
of lateral epicondylalgia. Pain. 1996;68(1):69-74.
Wainner RS, Fritz JM, Irrgang JJ, Boninger ML, Delitto A, Allison S. Reliability and diagnostic accuracy of the clinical examination and
patient self-report measures for cervical radiculopathy. Spine. 2003;28:52-62.
Wainner RS, Whitman JM, Cleland JA, Flynn TW. Regional interdependence: A musculoskeletal examination model whose time has come.
J Orthop Sports Phys Ther. 2007;37:658-660.
Winters JC, Sobel JS, Groenier KH, Arendzen HJ, Meyboom-de Jong B. Comparison of physiotherapy, manipulation and corticosteroid
injection for treating shoulder complaints in general practice: Randomized, single blind study. BMJ. 1997;314:1320-1325.