update on the management of immune thrombocytopenic
TRANSCRIPT
Update on the Management of
Immune Thrombocytopenic Purpura (ITP)
Dr Raymond Wong Department of Medicine & Therapeutics Prince of Wales Hospital

Immune Thrombocytopenia (ITP)
• Immune-mediated acquired disease of adults and children
• ITP is characterized by:
• A low platelet count (<100 x 109/L,
transient or persistent)1
• An increased risk of bleeding due to impaired
clotting mechanism2-4
HCV, hepatitis C virus; HIV, human immunodeficiency virus 1. Rodeghiero F, et al. Blood 2009; 113: 2386–93; 2. Stasi R, Provan D. Mayo Clin Proc 2004; 79: 504–22; 3. Chang M, et al. Blood 2003; 102: 887–95; 4. Cooper N, Bussel J. Br J Haematol 2006; 133: 364–74; 5. Terrell D, et al. Am J Hematol 2010; 85: 174–80; 6. Schoonen W, et al. Br J Haematol 2009; 145: 235–44
• The overall incidence of ITP among adults is
estimated at 3.3 per 100,000 person-years5
• Higher incidence in women versus men6
• Male:female ratio increases with age
• Higher incidence at older ages6

Clinical presentation of ITP varies
Dependent on the severity of thrombocytopenia,
the clinical presentation of ITP varies1,2
• Most patients are asymptomatic but may
complain of fatigue and easy bruising
• As platelet counts fall, symptoms become more
severe and may include:
- purpuric skin lesions
- cutaneous bleeding
- epistaxis
- gingival or gastrointestinal bleeding
- haematuria or menorrhagia
• Thromboembolic event risk increased3
Purpura (reddish purple spots)
Petechiae
1 cm 2 cm 3 cm
Actual scale:
1. Stasi R, Provan D. Mayo Clin Proc 2004; 79: 504–22; 2. Cines D, McMillan R. Annu Rev Med
2005; 56: 425–42; 3. Sarpatwari A, et al. Haematologica 2010; 95: 1167–75

4
Current Understanding of
Pathogenesis of ITP

Platelet count after infusion with patient plasma
Antiplatelet antibodies: 19511 Inhibition of megakaryocytes by
plasma from ITP patients: 20042
Immune pathogenesis of Immune Thrombocytopenia (ITP) Evidence that ITP is a B cell disease
1. Harrington WJ et al. J Lab Clin Med 1951;38:1–10; 2. McMillan R et al. Blood 2004;103:1364–1369
Pla
tele
ts (
×1
09/L
)
0
400
600
800
1000
200
1 2 3 1 2 3 4 5 6 7 8 9
Hours Days
Contr
ol m
egakary
ocyte
s (
%)
100
75
50
25
0

Thrombopoietin (TPO) Signaling Pathways
Stem cell
Bilineal progenitor cell
Committed megakaryocyte progenitor cell
Immature megakaryocyte
Mature megakaryocyte
Platelets
TPO
TPO
TPO
TPO
1. Kuter D, et al. Blood 2002; 100: 3456–69; 2. Kaushansky K. N Engl J Med 1998; 339: 746–54; 3. Wolber E, Jelkmann W. News Physiol Sci 2002; 17: 6–10. Figure adapted with permission from Kaushansky K. N Engl J Med 1998; 339: 746–54
TPO regulates the maturation of megakaryocytes,
via signal transduction pathways, into platelet-
producing cells

Thrombopoietin levels are lower than expected in ITP
1. Kosugi S et al. Br J Haematol 2003;93:704–706; 2. Aledort LM et al. Am J Hematol 2004;76:205–213
14
Th
rom
bopoie
tin
leve
l
Normal
12
10
8
6
4
2
0
ITP Aplastic
anemia
No correlation between platelet
count and TPO levels in patients
with ITP1
No significant difference in TPO
levels between patients with ITP
and controls2

ITP is caused by lower production and higher destruction of
platelets
Nugent D et al. Br J Haematol 2009;146:585–596 Ab, antibody
Increased platelet destruction
(spleen)
Decreased platelet production
(bone marrow)
Antiplatelet
immunity
(Ab + T cell)
Anti-megakaryocyte
immunity
(Ab + T cell)
Healthy
(normal platelet counts)
ITP effector immunity is primarily comprised of antibodies and T cells

Complex ITP pathophysiology underlies platelet regulation
Adapted from Stasi R et al. Thromb Haemost 2008;99:4–13 IFN, interferon; MHC, major histocompatibility complex;
Tc, cytotoxic T cell; TCR, T cell receptor
Th cell
IL-2 IFN-γ
B cell
Impaired megakaryocyte
maturation
Reduced platelet production
Megakaryocyte
Tc cell
Tc-cell-mediated
platelet
destruction
Platelets
Epitope
spreading
Macrophage
Platelet
phagocytosis
CD80
CD80
CD28
CD28
CD40
CD40
MHC II TCR
CD154
CD154
Platelet autoantibody production

10
Diagnosis of Immune
Thrombocytopenia (ITP)

Guidelines for diagnosis of ITP
• ITP remains a diagnosis of exclusion of other conditions or factors that cause
thrombocytopenia1
• Assessment of the following is needed to diagnose ITP:1
– Patient and family history
– Physical examination
– Complete blood count
– Peripheral blood film
– Other laboratory investigations
• There is no robust clinical or laboratory test that can establish a diagnosis with
accuracy1
• A platelet count <100 x 109/L has been defined as the threshold for diagnosis2
1. Provan D, et al. Blood 2010; 115: 168–86; 2. Rodeghiero F, et al. Blood 2009; 113: 2386–93
Results do not suggest
other aetiologies for
thrombocytopenia1

Diagnostic Approach in Suspected ITP
Basic evaluation Tests of potential utility Tests of unproven benefit
• Patient/family history
• Physical examination
• CBC and reticulocyte count
• Peripheral blood film
• Quantitative
immunoglobulin level
measurement*
• Bone marrow
(in selected patients)
• Blood group (Rh)
• Direct antiglobulin test
• H. pylori**/***; HIV/HCV**
• Glycoprotein-specific
antibody
• Antiphospholipid antibodies
(including anticardiolipin and
lupus anticoagulant)
• Antithyroid antibodies and
thyroid function
• Pregnancy test in women of
childbearing potential
• Antinuclear antibodies***
• PCR for parvovirus and CMV
• TPO
• Reticulated platelets
• PaIgG
• Bleeding time
• Platelet survival study
• Serum complement
*Should be considered in children; recommended in children with persistent or chronic ITP
**Recommended for adult patients regardless of geographic location
***Not recommended in children according to the American Society of Hematology guidelines (2011)1
CBC, complete blood count; CMV, cytomegalovirus; HCV, hepatitis C virus; HIV, human immunodeficiency virus; PaIgG, platelet-associated immunoglobulin G; PCR, polymerase chain reaction; Rh, rhesus 1. Neunert C, et al. Blood 2011; 117: 4190207; Table reproduced with permission from Provan D, et al. Blood 2010; 115: 168–86

Diagnosis of ITP
• The diagnosis of ITP remains one of exclusion; known causes of
thrombocytopenia include:
• Lupus erythematosus, infection (HIV, HCV), thrombotic thrombocytopenic purpura
• Hereditary thrombocytopenia: absent radius syndrome,
radio-ulnar synostosis, congenital amegakaryocytic thrombocytopenia, Wiskott-Aldrich
Syndrome, MYH9-associated thrombocytopenia, Bernard-Soulier Syndrome
• Vaccinations and transfusions
• Medication/drugs/diet (e.g. platelet-lowering treatments, alcohol, vitamin deficiency,
quinine from tonic water)
• Liver disease
• Other bone marrow disease/leukemia
HCV, hepatitis C virus; HIV, human immunodeficiency virus Provan D, et al. Blood 2010; 115: 168–86

Role of Bone Marrow Examination in the diagnosis of ITP
may be informative in patients > 60 years of age, in those with systemic
symptoms or abnormal signs, or in some cases pre-splenectomy
is not necessary irrespective of age in patients presenting with typical ITP
International consensus report on the investigation and management
of primary immune thrombocytopenia
Provan D, Stasi R, Newland AC, Blanchette VS, Bolton-Maggs P, Bussel JB, Chong BH, Cines
DB, Gernsheimer TB, Godeau B, Grainger J, Greer I, Hunt BJ, Imbach PA, Lyons G, McMillan R,
Rodeghiero F, Sanz MA, Tarantino M, Watson S, Young J, Kuter DJ. Blood 2010;115:168–186
The American Society of Hematology 2011 evidence-based practice
guideline for immune thrombocytopenia
Neunert C, Lim W, Crowther M, Cohen A, Solberg L Jr, Crowther MA;
American Society of Hematology. Blood 2011;117:4190–4207
Provan D, et al. Blood 2010; 115: 168–86. Neunert C, et al. Blood 2011; 117: 4190 207;

15
Treatment strategies
for patients with ITP

Factors That Contribute to ITP Management Decisions
• In patients with platelet counts >50 x 109/L treatment is not usually indicated unless the patient has other risk factors (e.g. bleeding or surgery)1
• A platelet count of <30 x 109/L is commonly used as the threshold for treatment in asymptomatic patients
1. Rodeghiero F, et al. Blood 2009; 113: 2386–93; 2. Neunert C, et al. Blood 2011; 117: 4190–207; 3. Provan D, et al. Blood 2010; 115: 168–86
The goal of treatment in chronic ITP is not well defined and depends on balancing efficacy against the adverse effects of a given treatment1

Treatments for ITP: mechanisms of action
Newland A, et al. Immunotherapy (2018) 10(1), 9–25

International Consensus Report (2010):
Guidelines on First-line Treatment Options
IVIg, intravenous immunoglobulin Adapted with permission from Provan D, et al. Blood 2010; 115: 168–86
Clinical situation Therapy option
• Corticosteroids (standard initial treatment)
• Dexamethasone
• Methylprednisolone
• Prednis(ol)one
• Intravenous anti-D (Rho) immunoglobulin
• IVIg
Second-line therapy
Treatment for patients
failing first- and second-line
therapies
First-line therapy (initial treatment for newly diagnosed ITP)

ITP: Corticosteroid Treatment Strategy
Recommended
treatment strategy
Response
rate
Time to
response
Toxicities Duration of
sustained response
Dexamethasone
40 mg daily for
4 days every
2–4 weeks for
1–4 cycles
Up to 90% of
patients
respond
initially
Several days
to several
weeks
Can include: mood swings,
weight gain, anger, fluid
retention insomnia,
Cushingoid faces, dorsal fat,
diabetes, osteoporosis, skin
changes, alopecia,
hypertension, gastrointestinal
distress, ulcers, avascular
necrosis, immunosuppression,
psychosis, cataracts,
opportunistic infections,
adrenal insufficiency,
hypertension, anxiety.
Tolerability decreases with
repeated dosing
50–80%, the latter
with 3–6 cycles
Methylprednisolone
30 mg/kg/day for 7
days
As high as
95%
4.7 days (high
dose)
23% have sustained
platelet count (>50 x
109/L) at 39 months
Prednis(ol)one
0.5–2 mg/kg/day for
2–4 weeks
70–80% of
patients
respond
initially
Several days
to several
weeks
Remains uncertain;
estimated 10 year
disease-free survival
for 13–15%
Adapted with permission from Provan D, et al. Blood 2010; 115: 168–86

ITP: Intravenous Immunoglobulin (IVIg) Therapy
Provan D, et al. Blood 2010; 115: 168–86
Profile
• Have an initial response rate comparable to corticosteroids with a shorter time to response
• Many recipients attain a platelet increase within 24 hours at a dose of 1 g/kg
• In some patients, corticosteroids may enhance the IVIg response
Safety and efficacy
• Associated with higher toxicity than corticosteroids, especially headaches
• There is a need for a prolonged infusion over several hours
• Rare but serious toxicities include renal failure and thrombosis
• Transient response

ITP: Intravenous Anti-D Immunoglobulin
IVIg, intravenous immunoglobulin 1. Provan D, et al. Blood 2010; 115: 168–86; 2. Neunert C, et al. Blood 2011; 117: 4190–207
Profile
• Appropriate for Rhesus D-positive, non-splenectomised ITP patients1,2
• May be an effective alternative to IVIg:1
• It can be infused in a shorter time
• It has a potentially longer response
• May reduce the need for splenectomy
Limitations
• Not recommended for use in patients with autoimmune haemolytic anaemia to avoid exacerbation of haemolysis1,2
• Mild anaemia is expected and may be dose-limiting1
• It has a small donor pool and therefore the potential for limited availability1
ITP: Second-line Therapy
Provan D, et al. Blood 2010; 115: 168–86
Treatment decisions to be individualised based on:
Comorbidities
Patient expectations Compliance
Bleeding history
When first-line therapy fails, it is appropriate to move to second-line therapy in an attempt to gain a sustained increase in platelet count

International Consensus Report (2010):
Guidelines on Second-line Treatment Options
Adapted with permission from Provan D, et al. Blood 2010; 115: 168–86
Clinical situation Therapy option
First-line therapy
• Azathioprine
• Cyclosporin A
• Cyclophosphamide
• Danazol
• Dapsone
• Mycophenolate mofetil
• Rituximab
• Splenectomy
• TPO-R agonists (eltrombopag, romiplostim)
• Vinca alkaloid regimens
Treatment for patients failing first-
and second-line therapies
Second-line therapy

Second-line Immunosuppressive Agents for Adult ITP Patients
Adapted from Provan D, et al. Blood 2010; 115: 168–86

ITP: Rituximab Treatment
Chimeric, monoclonal antibody against B-cell antigen CD201 that
causes a transient elimination of B-cells2
Rituximab is not currently approved for treatment of ITP
The ASH guidelines indicate rituximab as a consideration for patients at
risk of bleeding who have failed one line of therapy such as
corticosteroids, IVIg, or splenectomy3
Initial response was seen in 62.5% of cases with a complete response
in 46.3% of patients*4
The 5-year response rate is approximately 21% for adults5
IVIg, intravenous immunoglobulin
*a complete response was defined as platelet count >150 x 109/L and overall response as a platelet count >50 x 109/L
1. Godeau B, et al. Blood 2008; 112: 999–1004; 2. Stasi R, et al. Thromb Haemost 2008; 99: 4–13; 3. Neunert C, et al. Blood 2011; 117; 4190–207; 4. Arnold D, et al. Ann Intern Med 2007;
146: 25–33; 5. Patel V, et al. Blood 2010; 116: abstract 72

ITP: Splenectomy
Splenectomy:
Is considered the traditional second-line therapy in adults with chronic ITP resistant to first-line treatments1
80% of patients respond to splenectomy with ~66% achieving a lasting response2
Splenectomy complication and mortality rates have been seen to be higher with laparotomy than in laparoscopy2
Criteria for splenectomy:1
Severe thrombocytopenia (platelet count <10 x 109/L)
A high risk of bleeding for platelet counts <30 x 109/L
The requirement of continuous corticosteroid therapy to maintain safe platelet counts
Splenectomy is deferred in most patients for ≥6 months2 but often for >12 months3 after diagnosis
1. Stasi R, et al. Thromb Haemost 2008; 99: 4–13; 2. Provan D, et al. Blood 2010; 115: 168–86; 3. Neunert C, et al. Blood 2011; 117: 4190–207
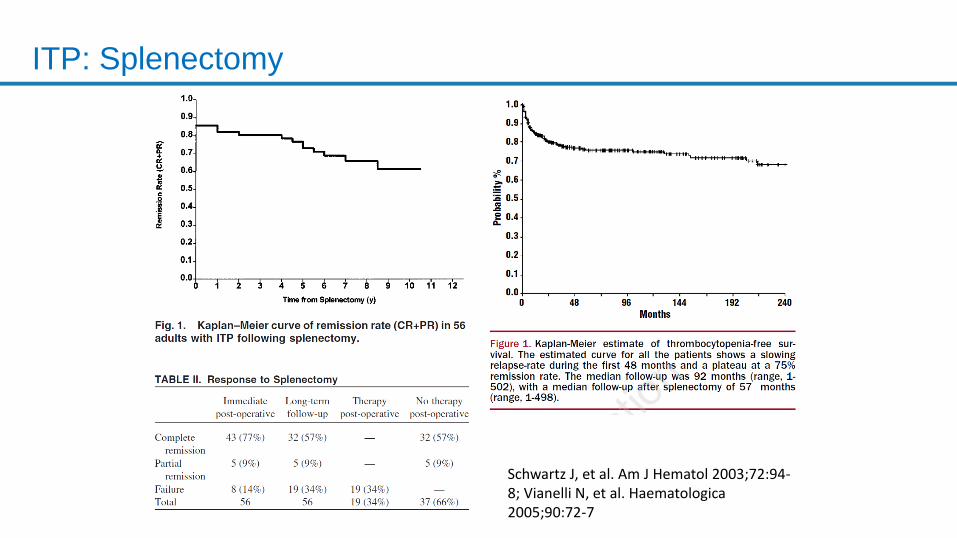
ITP: Splenectomy
Schwartz J, et al. Am J Hematol 2003;72:94-8; Vianelli N, et al. Haematologica 2005;90:72-7

ITP: Splenectomy
Standard second-line therapy for ITP1,2
Timing of
treatment
• Generally considered from 6 months after failure of primary treatment1,2
Efficacy • Initial haemostatic response in 70–80% of patients1,2
• 15–25% of patients relapse within 10 years1
• Success rate of ~66% with a sustained complete response1,3
Safety/
tolerability
• Splenectomy is associated with significant morbidity and a risk of overwhelming
and fatal Streptococcus pneumoniae infection2
• Complications of splenectomy can include infections, long-term relapse, prolonged
hospitalisation and risk of death1,2
• Risk of serious post-splenectomy infection is greater in patients >65 years of age1
• There may be a lower mortality rate with laparoscopic splenectomy1,3
• Occasionally, patients may fail to respond to splenectomy because of the failure to
remove an accessory spleen3
1. Provan D, et al. Blood 2010; 115: 168–86; 2. Neunert C, et al. Blood 2011; 117: 4190–207; 3. Stasi R, et al. Thromb Haemost 2008; 99: 4–13

TPO-R Agonists
• A novel therapeutic class of agents for chronic adult ITP which stimulate platelet
production:
• Bind and activate the TPO-R, helping to balance platelet production against
destruction1
• Agents include TPO peptide agonists (e.g. [romiplostim]) and TPO non-peptide
agonists (e.g. [eltrombopag])
Figure not to scale
Kuter D. Blood 2007; 109: 4607–16

Licensed TPO-RAs
Bussel JB et al. N Engl J Med 2006;355:1672–1681; Bussel JB et al. N Engl J Med 2007;357:2237–2247; Kuter DJ. Semin Hematol 2010;47:243–248
Small molecule, non-peptide
Does not compete with TPO for binding to TPO-R
Orally bioavailable, once-daily dosing
Low immunogenic potential
Advised not to take 2 hours before or 4 hours after a high-calcium meal or products containing polyvalent cations
Eltrombopag
TPO
Eltrombopag
Thrombopoiesis-stimulating peptibody
Structurally unrelated to TPO
Two dipeptides linked to the Fc fragment of an IgG1, administered subcutaneously once a week
Recycled via FcRn
Romiplostim
Fc Carrier Domain
TPO-RA
Peptides
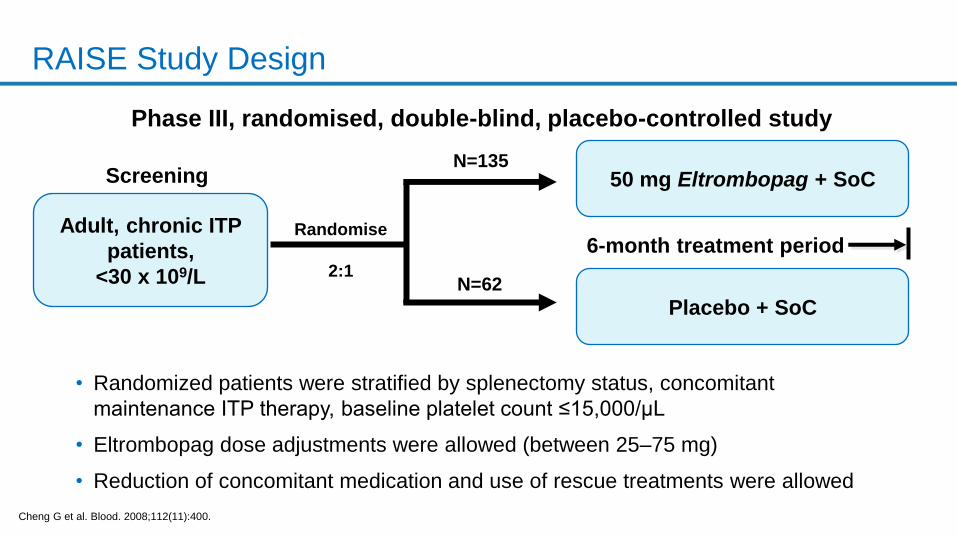
RAISE Study Design
Cheng G et al. Blood. 2008;112(11):400.
Randomise
2:1
Phase III, randomised, double-blind, placebo-controlled study
N=135
N=62
Screening
6-month treatment period Adult, chronic ITP
patients,
<30 x 109/L
50 mg Eltrombopag + SoC
Placebo + SoC
• Randomized patients were stratified by splenectomy status, concomitant
maintenance ITP therapy, baseline platelet count ≤15,000/µL
• Eltrombopag dose adjustments were allowed (between 25–75 mg)
• Reduction of concomitant medication and use of rescue treatments were allowed

RAISE: Sustained Increase in Median Platelet Count versus Placebo
During Treatment with Eltrombopag
Median platelet counts rose from 16 x 109/L to ~36 x 109/L after 1 week in the eltrombopag group
Cheng G, et al. Lancet 2011; 377: 393-402. Erratum: Lancet 2011; 377: 382
59
131
60
134
58
128
58
129
120
On treatment
20
140
60
0
61
135
Eltrombopag
Placebo
40
100
59
128
59
123
43
96
46
101
44
95
43
91
53
110
54
110
55
118
58
119
Placebo
Eltrombopag Number of
patients
80
Post-
treatment
0 1 5 6 2 4 10 14 18 22 26 1 2 4 3 Study week

RAISE: Eltrombopag Reduces Clinically Significant Bleeding versus
Placebo
Over 6 months’ treatment, the odds of bleeding and clinically significant bleeding with eltrombopag were respectively 76% and 65% less compared with placebo (OR 0.24, 95% CI 0.16, 0.38; p<0.0001 and OR 0.35, 95% CI 0.19, 0.64; p=0.0008)
World Health Organization Bleeding Scale: Grade 2, mild blood loss; Grade 3, gross blood loss; Grade 4, debilitating blood loss CI, confidence interval; OR, odds ratio Cheng G, et al. Lancet 2011; 377: 393-402. Erratum: Lancet 2011; 377: 382
Eltrombopag
Placebo

EXTEND Study Design
Eltrombopag eXTENded Dosing (EXTEND) is an open-label safety and efficacy study of long-term treatment of adult patients with chronic ITP who had previously completed a eltrombopag olamine study1,2
eltrombopag olamine dosing period
Stage 1: eltrombopag olamine dosing initiation (≥100 x 109/L*)
Stage 2†: Minimizing ITP medications (≥50 x 109/L)
Stage 3: Optimizing eltrombopag olamine dosing (≥50 x 109/L)
Stage 4: Maintenance dosing
Dose modulated to platelet count
Start 50 mg
Screening
Patients
enrolled
N=301
The bars for each stage in the figure represent the period during which a cohort of patients were recruited to that phase of the study, and not the time over which a patient might take eltrombopag olamine *≥50 x 109/L in patients not receiving concomitant ITP medications at baseline †Only required for patients receiving concomitant ITP medications at baseline 1. Saleh et al. Blood 2011; 118: Abstract 3296; 2. Saleh et al. Poster presented at the 53rd Annual Meeting of the American Society of Hematology, Dec, 2011

EXTEND: Exposure
• Mean average daily dose
• 50.2 (range, 1–75) mg/day
• Overall median duration of exposure
• 2.4 years (range, 2 days to 8.8 years)
• 103 patients received rescue therapy
• 62% of patients were receiving
eltrombopag 50 or 75 mg at the end of the
study
Last recorded dose of eltrombopag, n (%)
N=302
Dose, mg
0 39 (12.9)
>0 to <25 26 (8.6)
25 43 (14.2)
>25 to <50 6 (2.0)
50 70 (23.2)
75 118 (39.1)
Wong R, et al. Blood 2017

EXTEND Study: Long-term Eltrombopag in patients with ITP
276/302 (91.4%) achieved platelet counts ≥30×109/L without rescue treatment
259/302 (85.8%) achieved platelet counts ≥50×109/L without rescue treatment
IQR, interquartile range aPlatelet count data were collected throughout the study as part of the complete blood count, weekly during the first 4 weeks, and at any dose change (eltrombopag or concomitant ITP medication). If a patient continued on a stable dose during any stage of the study for >4 weeks, platelets were assessed every ≥4 weeks; bFewer than 15 patients had platelet counts at each assessment after Week 250.
Wong R, et al. Blood 2017

Number taking concomitant medication at baseline
101/302 (33%)
Permanently stopped one or more concomitant ITP medications
34/101 (34%)
Reduced or permanently stopped ≥1 concomitant ITP medications without requiring rescue therapy
39/101 (39%)
Sustained reduction of at least 24 weeks
37/39 (95%)
EXTEND: Proportion of Patients Able to Permanently Stop or
Reduce Concomitant ITP Medications Taken at Baseline
Wong R, et al. Blood 2017

EXTEND: Incidence of Bleeding (WHO Bleeding Scale)
Wong R, et al. Blood 2017

Spleen tyrosine kinase (Syk) inhibition
Fosamatinib
An oral SYK
inhibitor, was
developed for the
treatment of
patients with ITP
and other additional
autoimmune
disorders
Newland A, et al. Immunotherapy (2018) 10(1), 9–25

Fosamatinib in the treatment of ITP
2 randomized study of fosamatinib versus placebo in ITP
Bussell J, et al. Am J Hematology 2018 [Epub ahead of print]

Advances in the Management of ITP
Concepts about the mechanisms of ITP have shifted from the traditional
view of platelet destruction mediated by antibodies, to a much more
complex situation where impaired platelet production has emerged as
playing a significant role.
Immunosuppressive therapy continue to be the mainstay of initial
therapy.
Patients who do not go into early remission (persistent ITP) should use
steroid-sparing agents.
Thrombopoietin receptor agonists (TPO-RAs) have been demonstrated
to be very effective in a high percentage of even refractory patients with
ITP. They are generally well-tolerated with good safety profile.

Thank you