update on congenital in california - fhop.ucsf.edu · na/an a/pi black latina white note: na/an =...
TRANSCRIPT
STD Control Branch
Update on Congenital Syphilis in California
Julie Stoltey, MD MPHPublic Health Medical Officer
California Department of Public HealthSTD Control Branch
MCAH Action May 18, 2017Folsom, CA
STD Control Branch
Overview
• Summarize epidemiologic trends in STDs in California, including syphilis in women and congenital syphilis
• Describe syphilis stages and natural history• Review CDC guidelines for screening for syphilis in pregnant women
• Describe characteristics of congenital syphilis cases in California and prevention opportunities

STD Control Branch
Chlamydia, Gonorrhea, and Early SyphilisCalifornia Incidence Rates, 1995–2016
0
100
200
300
400
500
1995 2000 2005 2010 2016
Rate per 100,000
pop
ulation
28.4(N=11,173)
Rev. 4/18/2017
Syphilis
165.0(N=64,929)
504.7(N=198,607)Chlamydia
Gonorrhea
Provisional data 4.2017
STD Control Branch
0
100
200
300
400
500
1990 1995 2000 2005 2010 2015
Rate per 100,000
pop
ulation
Year
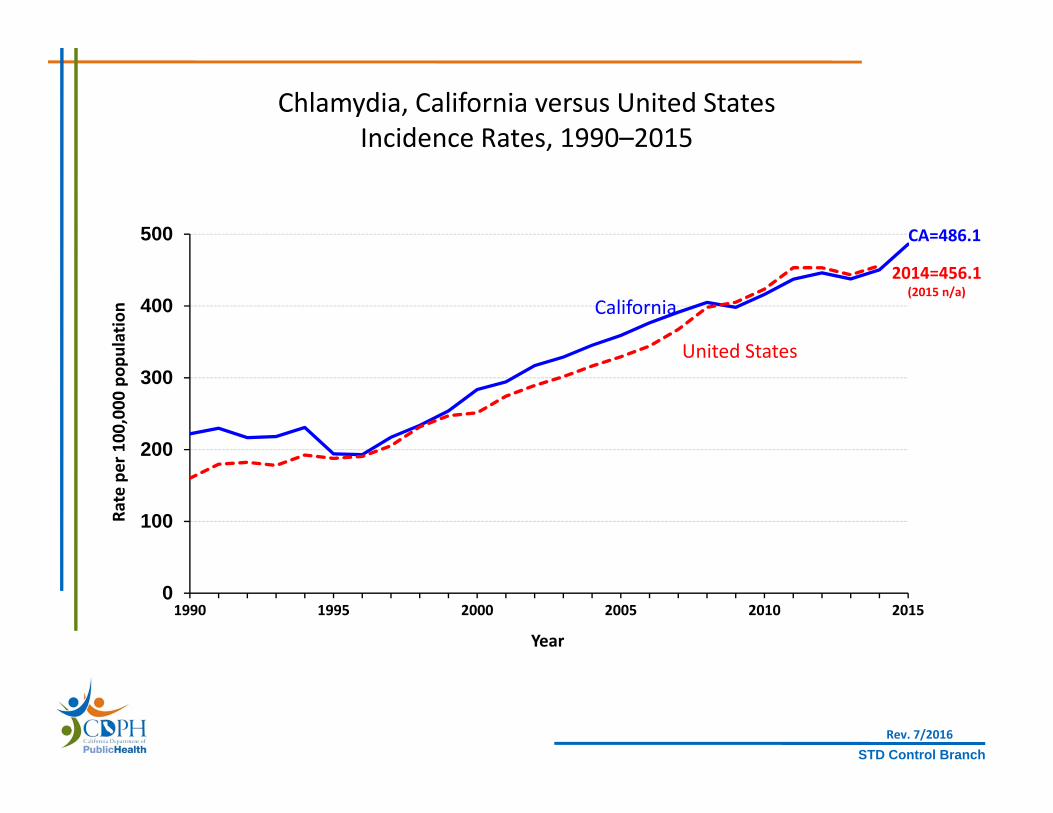
California
United States
CA=486.1
Chlamydia, California versus United StatesIncidence Rates, 1990–2015
Rev. 7/2016
2014=456.1(2015 n/a)

STD Control Branch
0
100
200
300
400
500
600
700
1990 1995 2000 2005 2010 2015
Rate per 100,000
pop
ulation
Year
Chlamydia, Incidence Rates by GenderCalifornia, 1990–2015
Total
Female
Male
Rev. 7/2016
STD Control Branch
01,0002,0003,0004,000 0 1,000 2,000 3,000 4,000
10‐14
15‐19
20‐24
25‐29
30‐34
35‐44
45+
Total
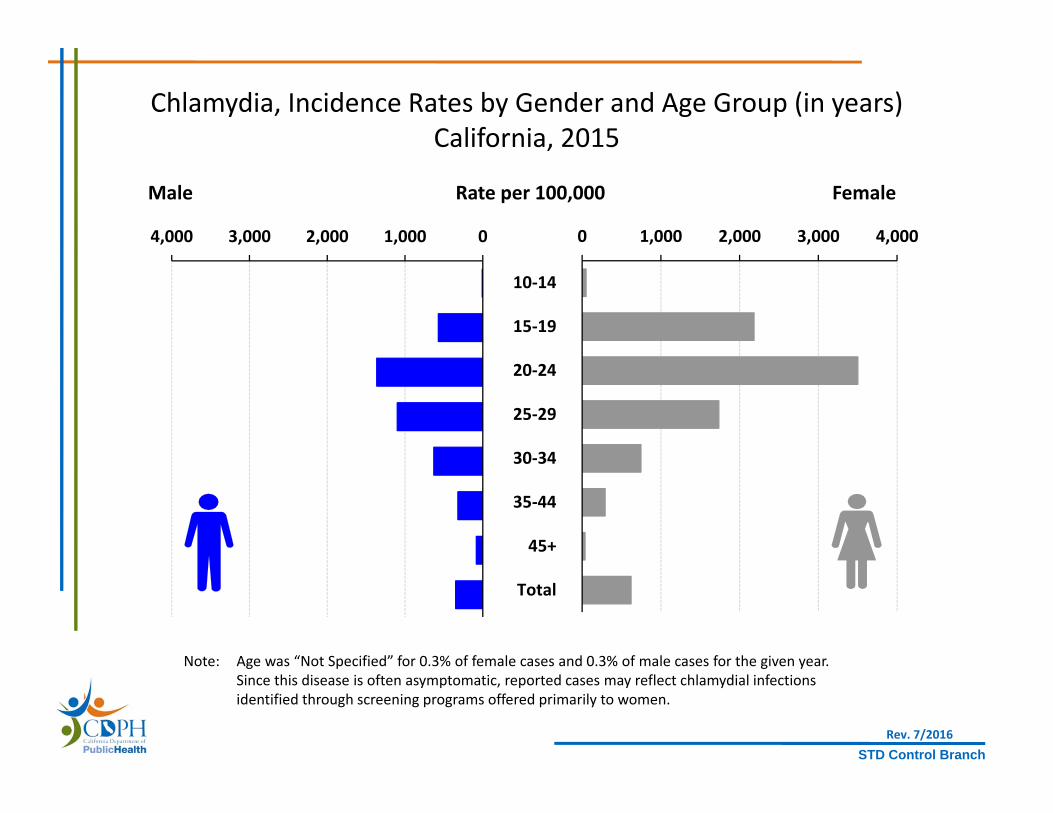
Chlamydia, Incidence Rates by Gender and Age Group (in years)California, 2015
Note: Age was “Not Specified” for 0.3% of female cases and 0.3% of male cases for the given year.Since this disease is often asymptomatic, reported cases may reflect chlamydial infectionsidentified through screening programs offered primarily to women.
Male Rate per 100,000 Female
Rev. 7/2016

STD Control Branch
0
300
600
900
1,200
1,500
2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
Rate per 100,000
pop
ulation
Year
NA/AN A/PI Black Latina White
Note: NA/AN = Native American/Alaskan Native, A/PI = Asian/Pacific Islander.Race/ethnicity “Not Specified” ranged from 33.1% to 40.3% of cases for females in any given year.
Chlamydia, Incidence Rates for Females by Race/Ethnicity California, 2006–2015
Rev. 7/2016
STD Control Branch
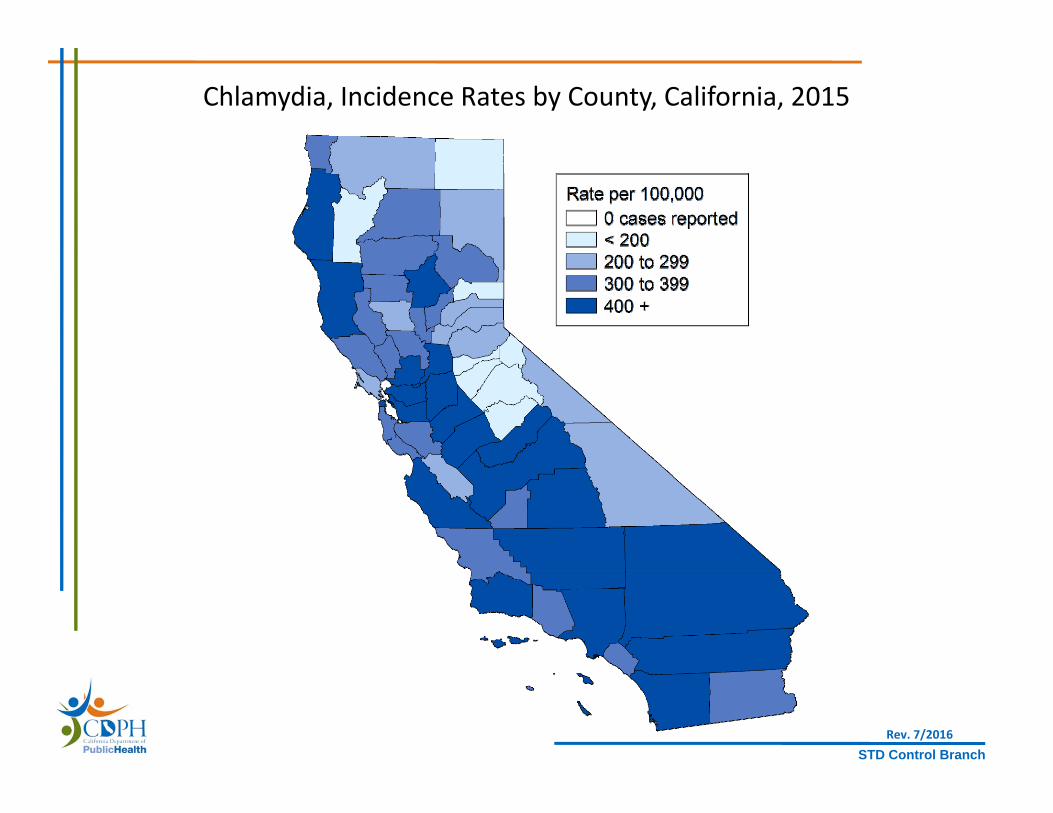
Chlamydia, Incidence Rates by County, California, 2015
Rev. 7/2016
STD Control Branch
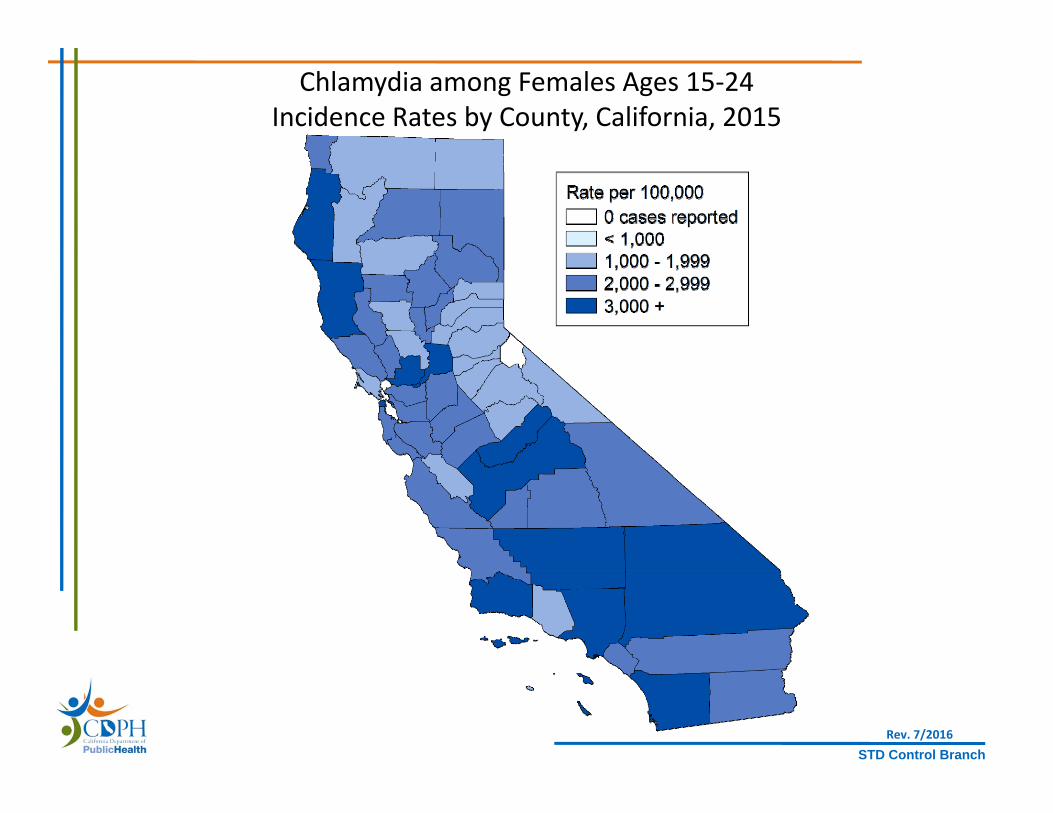
Chlamydia among Females Ages 15‐24Incidence Rates by County, California, 2015
Rev. 7/2016

STD Control Branch
Ranking of County Chlamydia Rates among Females Ages 15‐24California, 2015
(with 95% Confidence Intervals*)
Rev. 7/2016
0
1,000
2,000
3,000
4,000Sacram
ento
Fresno
Solano
Kern
Men
docino
San Francisco
San Diego
Madera
Los A
ngeles
Santa Ba
rbara
San Be
rnardino
Humbo
ldt
Alam
eda
Butte
Stanislaus
San Joaquin
Lake
Kings
Contra Costa
Tulare
Del N
orte
Mon
terey
Sono
ma
Impe
rial
Shasta
San Luis Obispo
Plum
asRiverside
Inyo
Merced
Lassen
Glenn
Santa Clara
Santa Cruz
Yuba
Orange
Sutter
San Mateo
Napa
Tehama
Placer
Ventura
El Dorado
Amador
Yolo
Marin
Colusa
San Be
nito
Tuolum
neNevada
Trinity
Calaveras
Mon
oSierra
Siskiyou
Mariposa
Mod
oc
Rate per 100,000
pop
ulation State Rate = 2,869.3
* Confidence intervals were calculated using Poisson exact method; excludes counties with no cases or statistically unstable rates.Note: Rates are per 100,000 population.
Source: California Department of Public Health, STD Control Branch
STD Control Branch
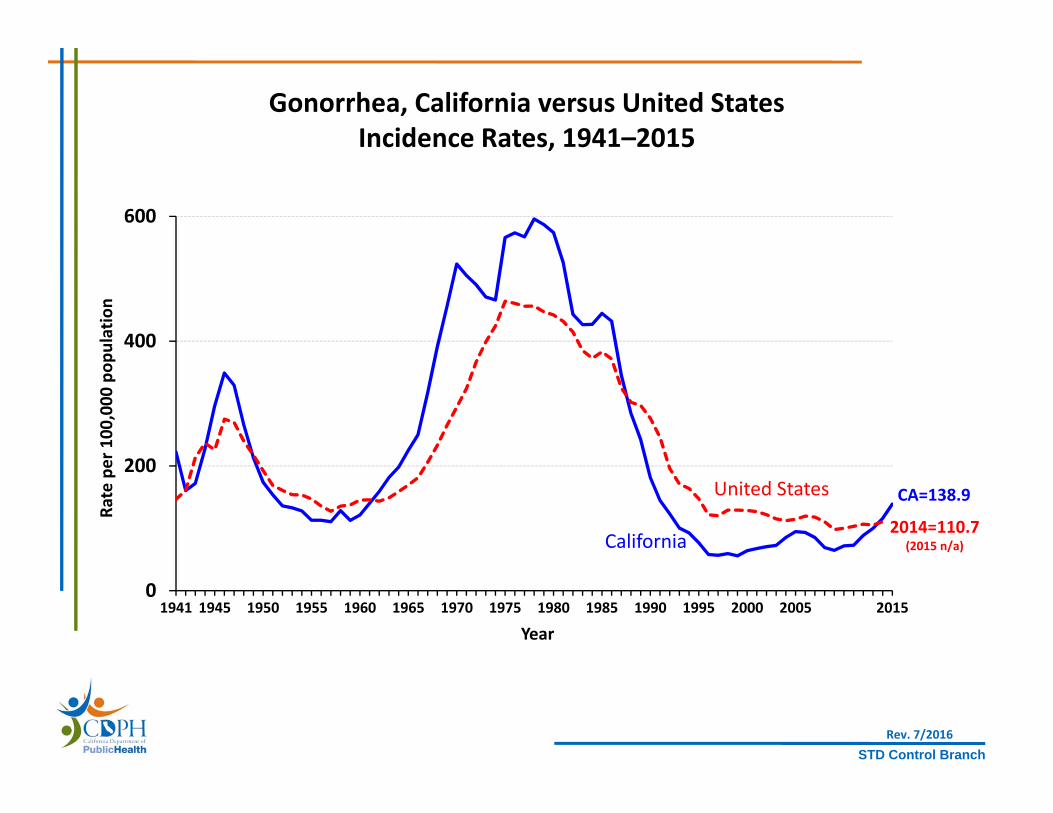
0
200
400
600
1941 1945 1950 1955 1960 1965 1970 1975 1980 1985 1990 1995 2000 2005 2015
Rate per 100,000
pop
ulation
Year
California
United States CA=138.9
Gonorrhea, California versus United StatesIncidence Rates, 1941–2015
Rev. 7/2016
2014=110.7(2015 n/a)

STD Control Branch
0
50
100
150
200
250
1995 2000 2005 2010 2016
Rate per 100,000
pop
ulation
Year
Gonorrhea, Incidence Rates by Gender, California, 1995–2016
Female
Male
In 2016, MSM made of 65% of male interviewed cases; 34% of MSM were HIV+(MSM = Gay, bisexual, and other men who have sex with men)
Rev. 4/18/2017

STD Control Branch
0200400600 0 200 400 600
10‐14
15‐19
20‐24
25‐29
30‐34
35‐44
45+
Total
Gonorrhea, Incidence Rates by Gender and Age Group (in years)California, 2015
Male Rate per 100,000 Female
Note: Age was “Not Specified” for 0.4% of female cases and 0.3% of male cases for the given year.
Rev. 7/2016

STD Control Branch
Gonorrhea, Female Incidence Rates by Race/Ethnicity and Age Group (in years), California, 2015
WhiteHispanic
Black
0
250
500
750
1,000
1,250
1,500
1,750
10 ‐ 14 15 ‐ 19 20 ‐ 24 25 ‐ 29 30 ‐ 34 35 ‐ 44 45+
Rate per 100,000
pop
ulation
Age Group
11 timeswhite rate
7 timeswhite rate
Rev. 7/2016

STD Control Branch
Gonorrhea, Incidence Rates by County, California, 2015
Rev. 7/2016
STD Control Branch
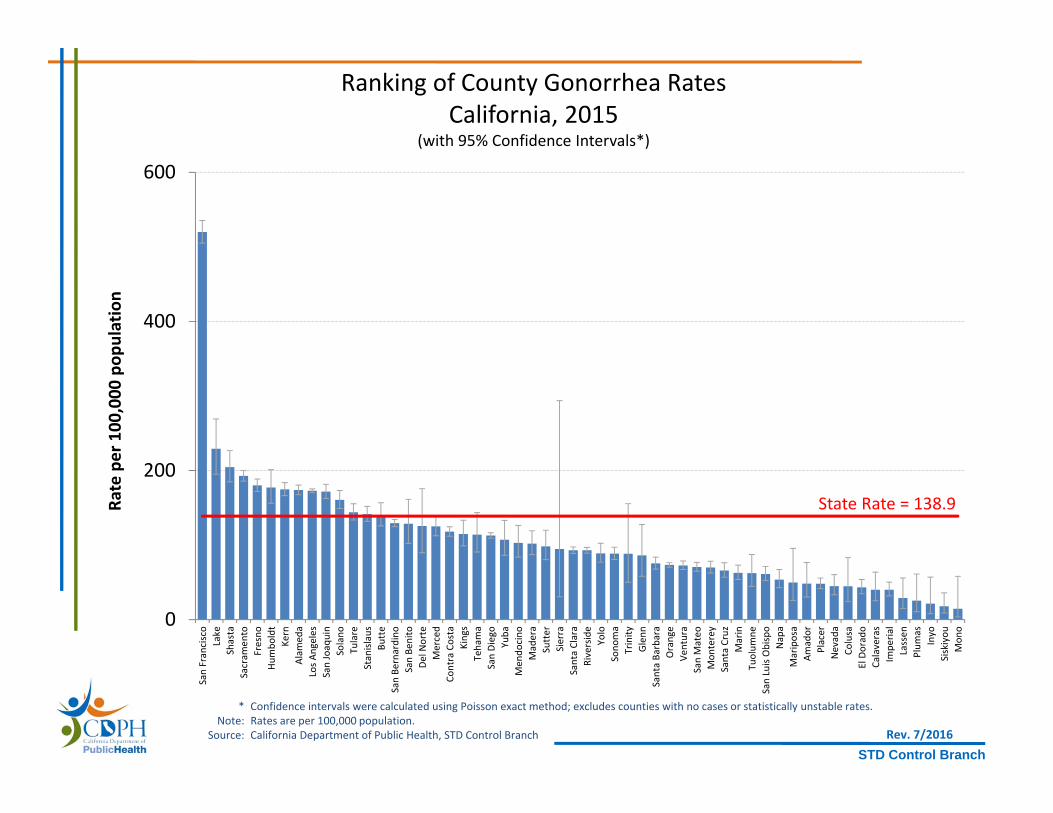
Ranking of County Gonorrhea RatesCalifornia, 2015
(with 95% Confidence Intervals*)
Rev. 7/2016
0
200
400
600San Francisco
Lake
Shasta
Sacram
ento
Fresno
Humbo
ldt
Kern
Alam
eda
Los A
ngeles
San Joaquin
Solano
Tulare
Stanislaus
Butte
San Be
rnardino
San Be
nito
Del N
orte
Merced
Contra Costa
Kings
Tehama
San Diego
Yuba
Men
docino
Madera
Sutter
Sierra
Santa Clara
Riverside
Yolo
Sono
ma
Trinity
Glenn
Santa Ba
rbara
Orange
Ventura
San Mateo
Mon
terey
Santa Cruz
Marin
Tuolum
neSan Luis Obispo
Napa
Mariposa
Amador
Placer
Nevada
Colusa
El Dorado
Calaveras
Impe
rial
Lassen
Plum
asInyo
Siskiyou
Mon
o
Rate per 100,000
pop
ulation
State Rate = 138.9
* Confidence intervals were calculated using Poisson exact method; excludes counties with no cases or statistically unstable rates.Note: Rates are per 100,000 population.
Source: California Department of Public Health, STD Control Branch
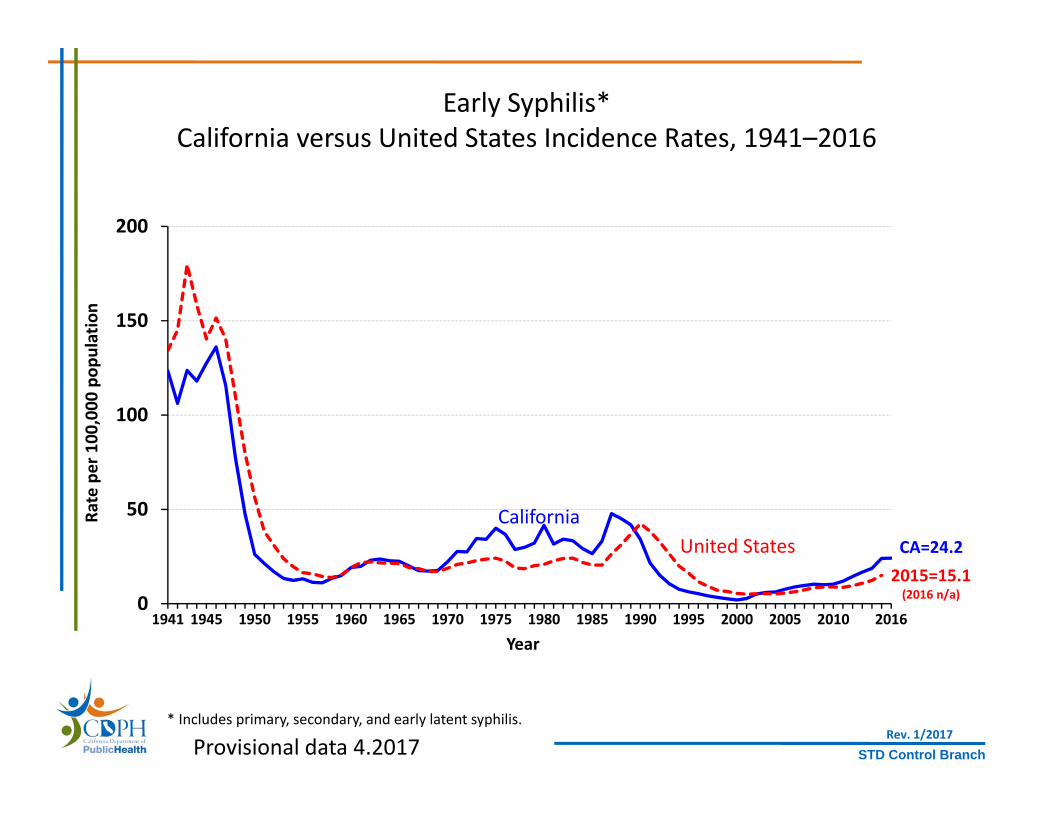
STD Control Branch
0
50
100
150
200
1941 1945 1950 1955 1960 1965 1970 1975 1980 1985 1990 1995 2000 2005 2010 2016
Rate per 100,000
pop
ulation
Year
CaliforniaUnited States CA=24.2
Early Syphilis*California versus United States Incidence Rates, 1941–2016
* Includes primary, secondary, and early latent syphilis.
2015=15.1(2016 n/a)
Rev. 1/2017Provisional data 4.2017

STD Control Branch
Early Syphilis, Number of Cases by Gender & Gender of Sex Partners, California, 1995–2016
0
2,500
5,000
7,500
10,000
1995 2000 2005 2010 2016
Num
ber o
f Cases
Year
ALL MALE
FEMALE
MSM
In 2016, MSM made of 72% of male cases; 55% of MSM were HIV+
Rev. 4/18/2017Provisional data 4.2017

STD Control Branch
0255075100125 0 25 50 75 100 125
10‐14
15‐19
20‐24
25‐29
30‐34
35‐44
45+
Total
Early Syphilis*Incidence Rates by Gender and Age Group (in years)
California, 2016
Male Rate per 100,000 Female
* Includes primary, secondary, and early latent syphilis.Rev. 1/2017
Provisional data 4.2017
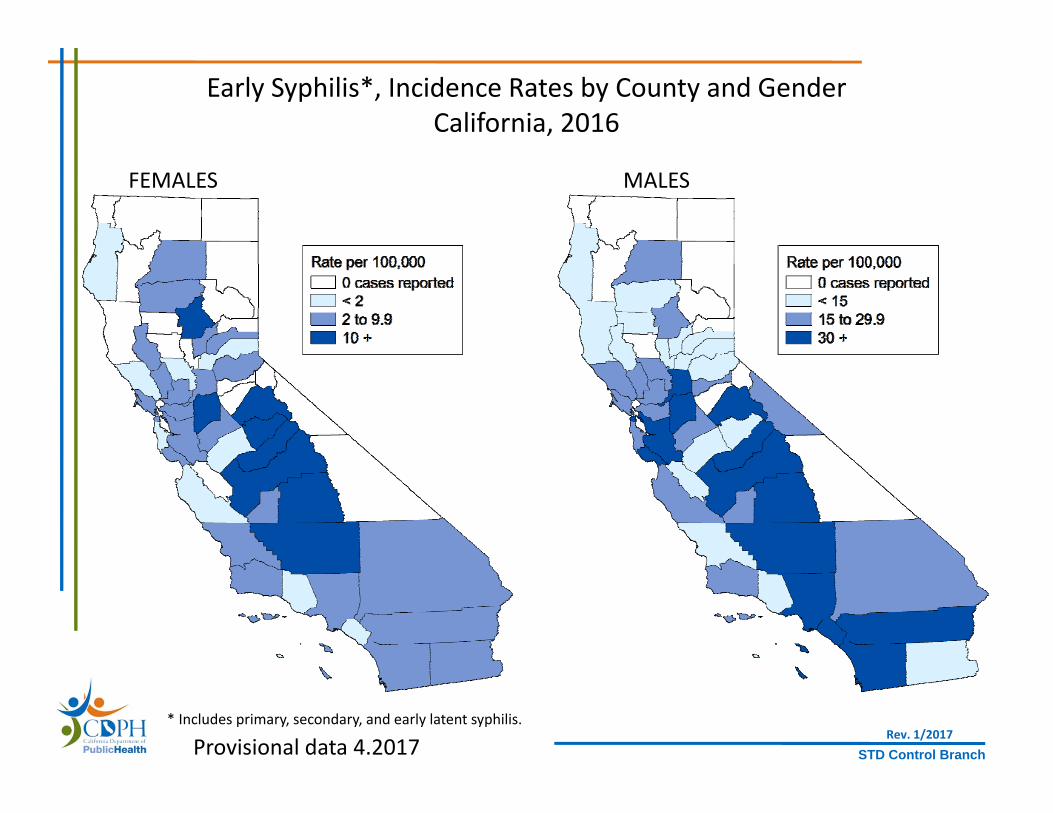
STD Control Branch
Early Syphilis*, Incidence Rates by County and GenderCalifornia, 2016
* Includes primary, secondary, and early latent syphilis.
FEMALES MALES
Rev. 1/2017Provisional data 4.2017

STD Control Branch
Ranking of County Early Syphilis* Rates among Females Ages 15‐44California, 2016
(with 95% Confidence Intervals*)
Rev. 1/2017
0
25
50
75
100
125
Rate per 100,000
pop
ulation
* Includes primary, secondary, and early latent syphilis.† Confidence intervals were calculated using Poisson exact method; excludes counties with no cases or statistically unstable rates.
Note: Rates are per 100,000 population.Source: California Department of Public Health, STD Control Branch
State Rate = 12.5
Provisional data 4.2017

STD Control Branch
0
3
6
9
12
15
2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
Rate per 100,000
pop
ulation
Year
NA/AN A/PI Black Latina White
Note: NA/AN = Native American/Alaskan Native, A/PI = Asian/Pacific Islander.Race/ethnicity “Not Specified” ranged from 0% to 7.2% of cases for females in any given year.
Early Syphilis*Incidence Rates for Females by Race/Ethnicity
California, 2006–2015
* Includes primary, secondary, and early latent syphilis. Rev. 7/2016

STD Control Branch
Methamphetamine Use among Early Syphilis Cases by Sexual Orientation, California, 2007–2016
0
10
20
30
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
Percen
t of Interview
ed Cases
Year
MSM only
MSW
Female
* Includes primary, secondary, and early latent syphilis.MSM=Men who have sex w/men, MSW=Men who have sex w/women, MSU=Men of unknown sexual orientation
Rev. 4/18/2017
Provisional data 4.2017

STD Control Branch
0
25
50
75
100
125
1965 1970 1975 1980 1985 1990 1995 2000 2010 2016
Rate per 100,000
live births
Year
California
CA=35.6
Congenital SyphilisCalifornia versus United States Incidence Rates, 1963–2016
2020 Objective(9.6)
Note: The Modified Kaufman Criteria were used through 1989. The CDC Case Definition (MMWR 1989; 48: 828) was used effective January 1, 1990.California data prior to 1985 include all cases of congenital syphilis, regardless of age.
United States
2015=12.4(2016 n/a)
Rev. 1/2017Provisional data 4.2017
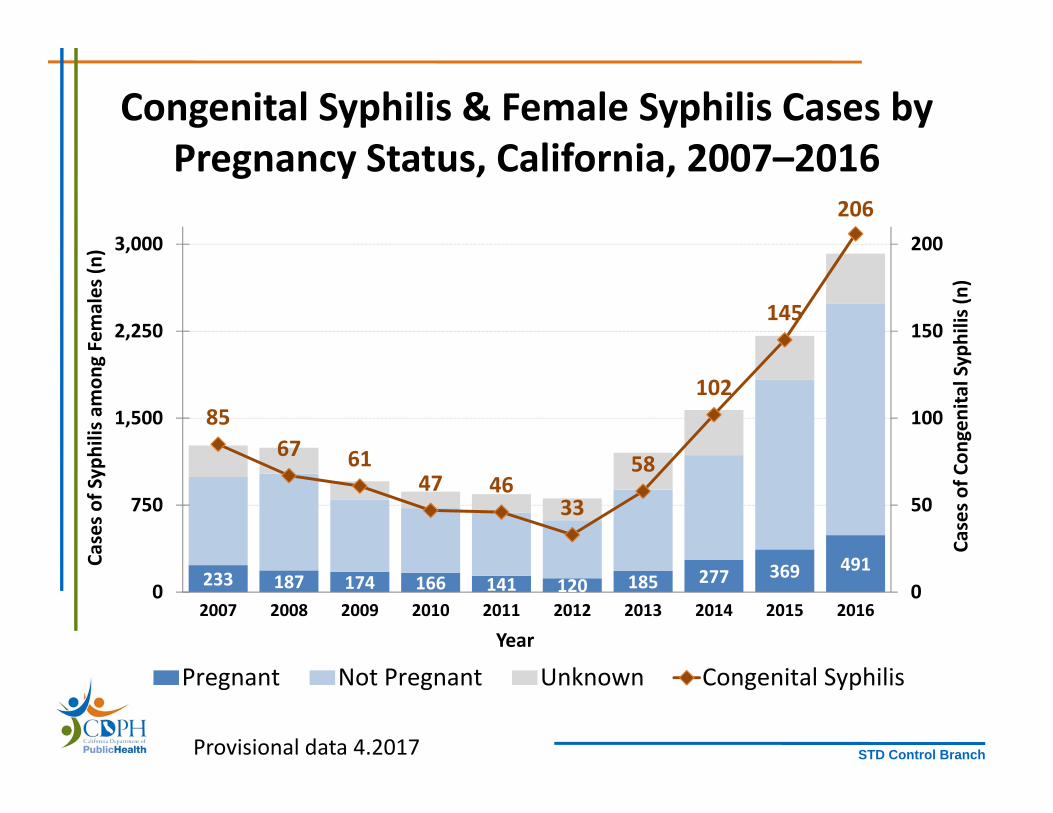
STD Control Branch
233 187 174 166 141 120 185 277 369 491
8567 61
47 4633
58
102
145
206
0
50
100
150
200
0
750
1,500
2,250
3,000
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016
Cases o
f Con
genital Syphilis (n
)
Cases o
f Syphilis amon
g Females (n
)
Year
Pregnant Not Pregnant Unknown Congenital Syphilis
Congenital Syphilis & Female Syphilis Cases by Pregnancy Status, California, 2007–2016
Provisional data 4.2017

STD Control Branch
Congenital Syphilis Cases by County, California, 2016
Rev. 4/18/2017
San Bernardino
Provisional data 4.2017
Los Angeles
Kern
Fresno
San JoaquinSacramento
San Diego
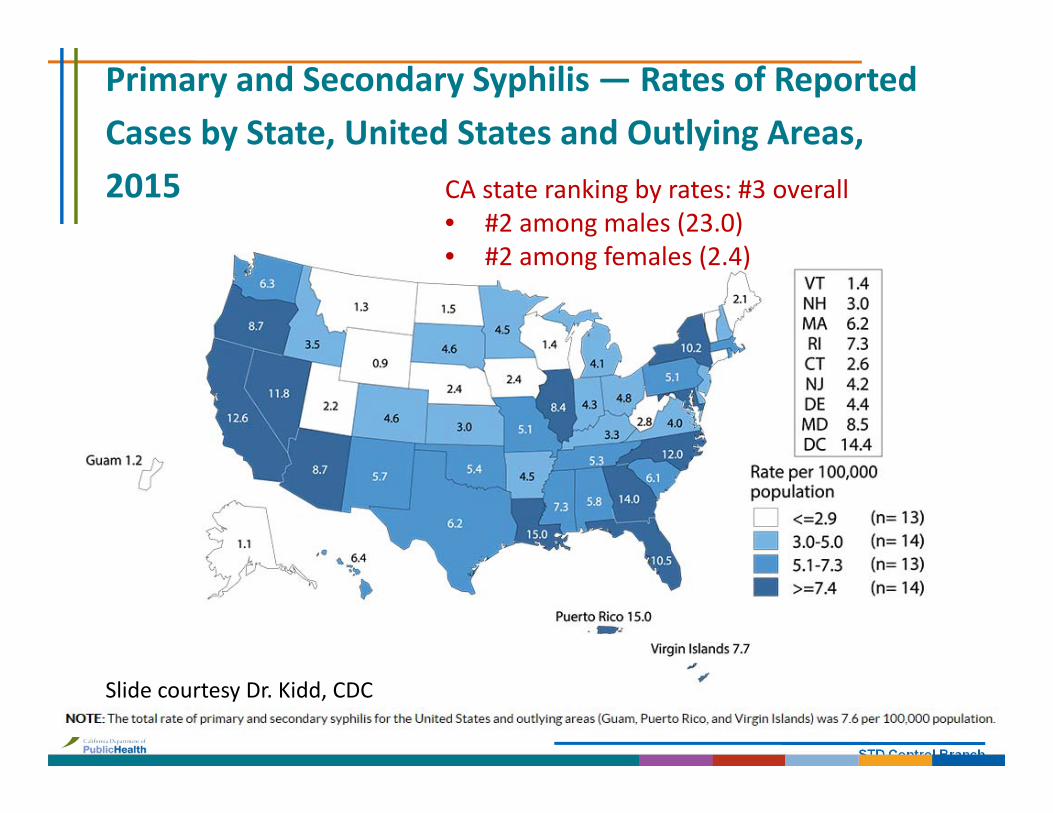
STD Control Branch
Primary and Secondary Syphilis — Rates of Reported Cases by State, United States and Outlying Areas, 2015 CA state ranking by rates: #3 overall
• #2 among males (23.0)• #2 among females (2.4)
Slide courtesy Dr. Kidd, CDC
STD Control Branch
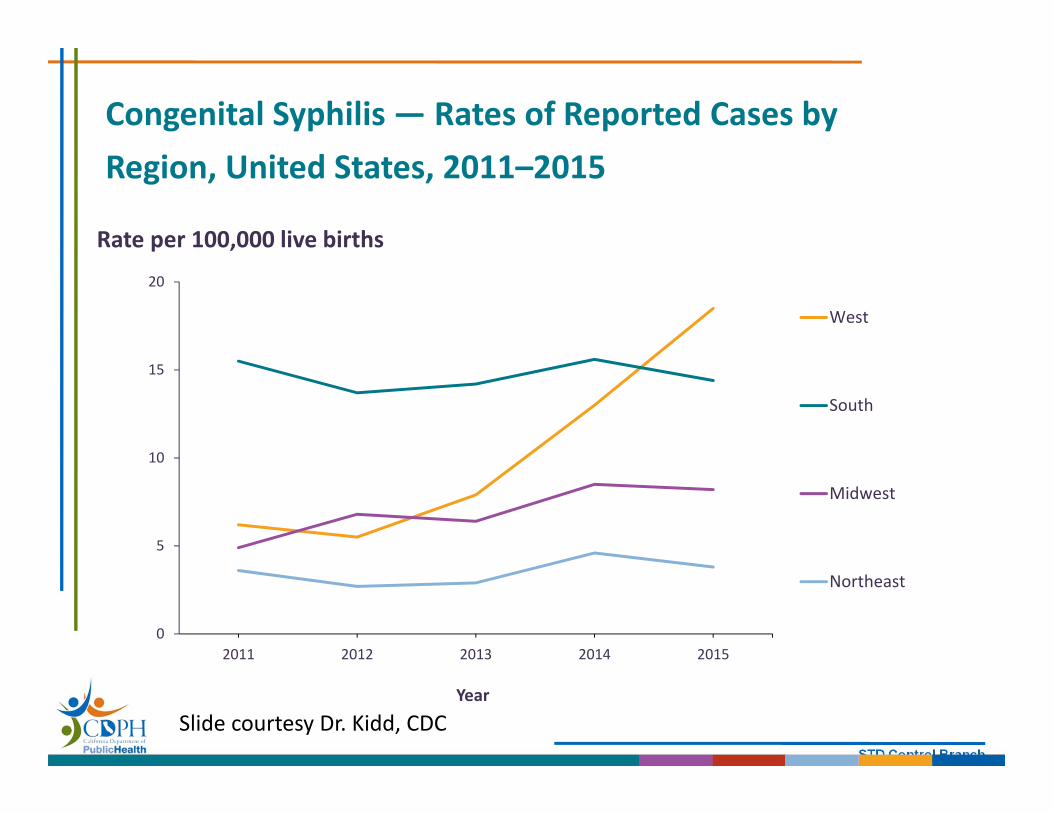
Congenital Syphilis — Rates of Reported Cases by Region, United States, 2011–2015
0
5
10
15
20
2011 2012 2013 2014 2015
Year
West
South
Midwest
Northeast
Rate per 100,000 live births
Slide courtesy Dr. Kidd, CDC
STD Control Branch
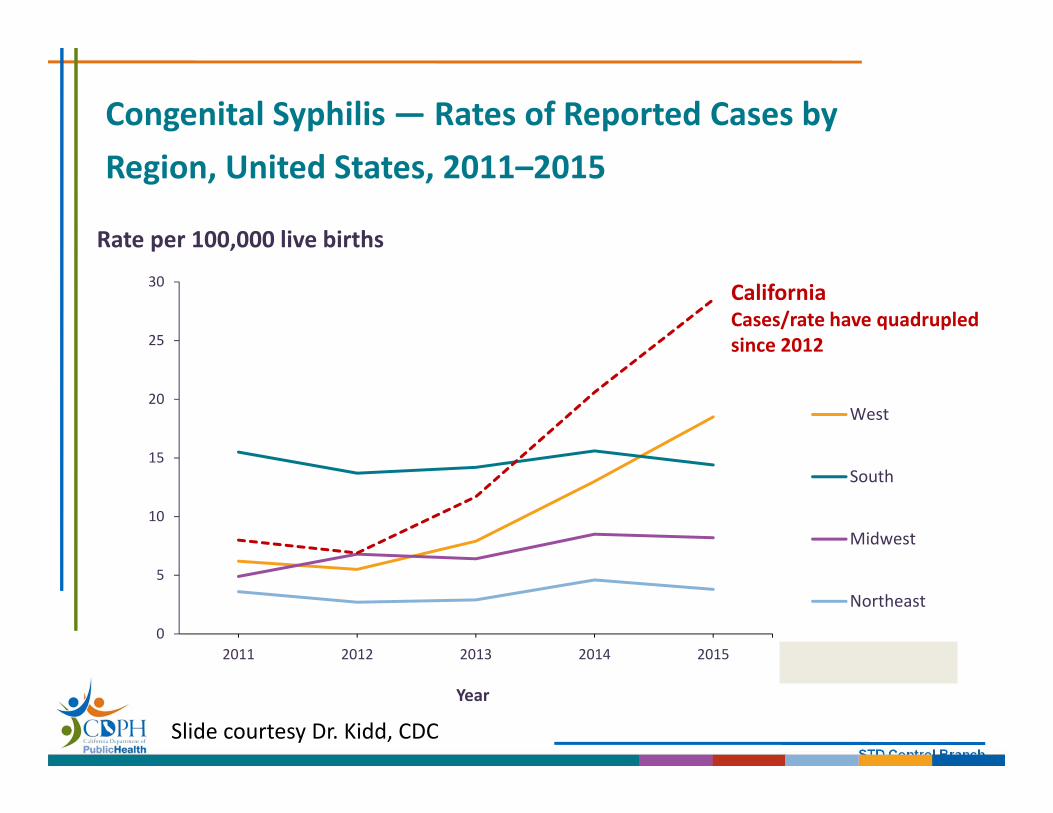
Congenital Syphilis — Rates of Reported Cases by Region, United States, 2011–2015
0
5
10
15
20
25
30
2011 2012 2013 2014 2015
Year
West
South
Midwest
Northeast
Column1
Rate per 100,000 live births
CaliforniaCases/rate have quadrupled since 2012
Slide courtesy Dr. Kidd, CDC
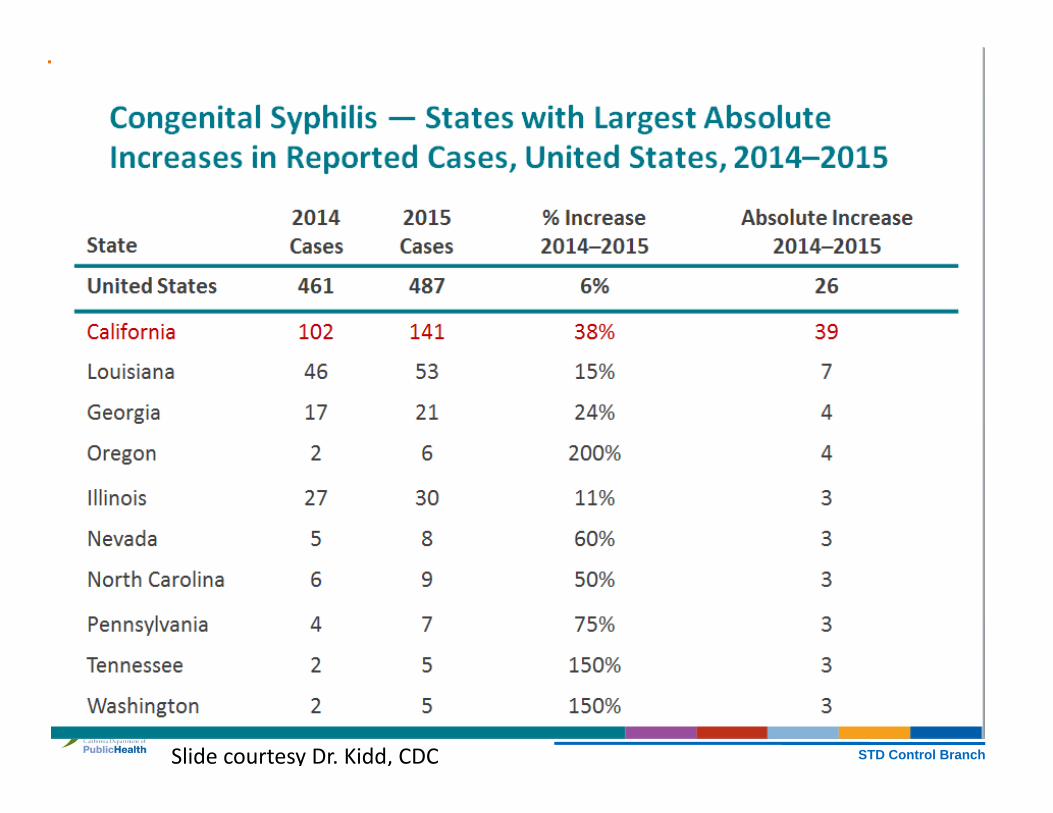
STD Control BranchSlide courtesy Dr. Kidd, CDC
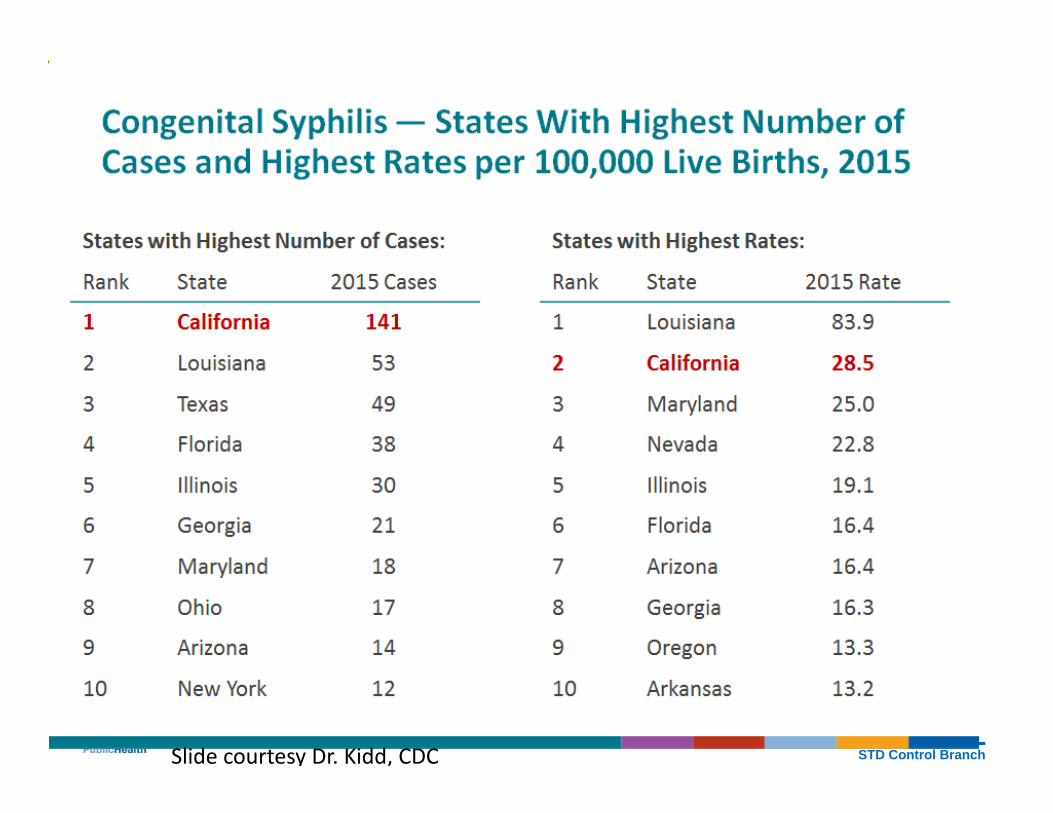
STD Control BranchSlide courtesy Dr. Kidd, CDC

STD Control Branch
Syphilis Overview
• Causative organism: Treponema pallidum, a spirochete bacterium, that replicates in 30 hours
• Transmitted by intimate skin‐to‐skin contact• Causes systemic infection• Incubation period: 10‐90 days• Characterized by episodes of active disease
interrupted by periods of latent infection• Without treatment, remains chronic or resolves

STD Control Branch
Syphilis Natural History
30‐50%Exposure Primary 30% TertiaryLatentSecondary
25%
Neurosyphilis can occur at any stage
IncubationPeriod
3‐4 weeks
2‐6 weeks
After 3‐8 weeks lesions disappear spontaneously
2‐20 yearsPossible relapse
STD Control Branch
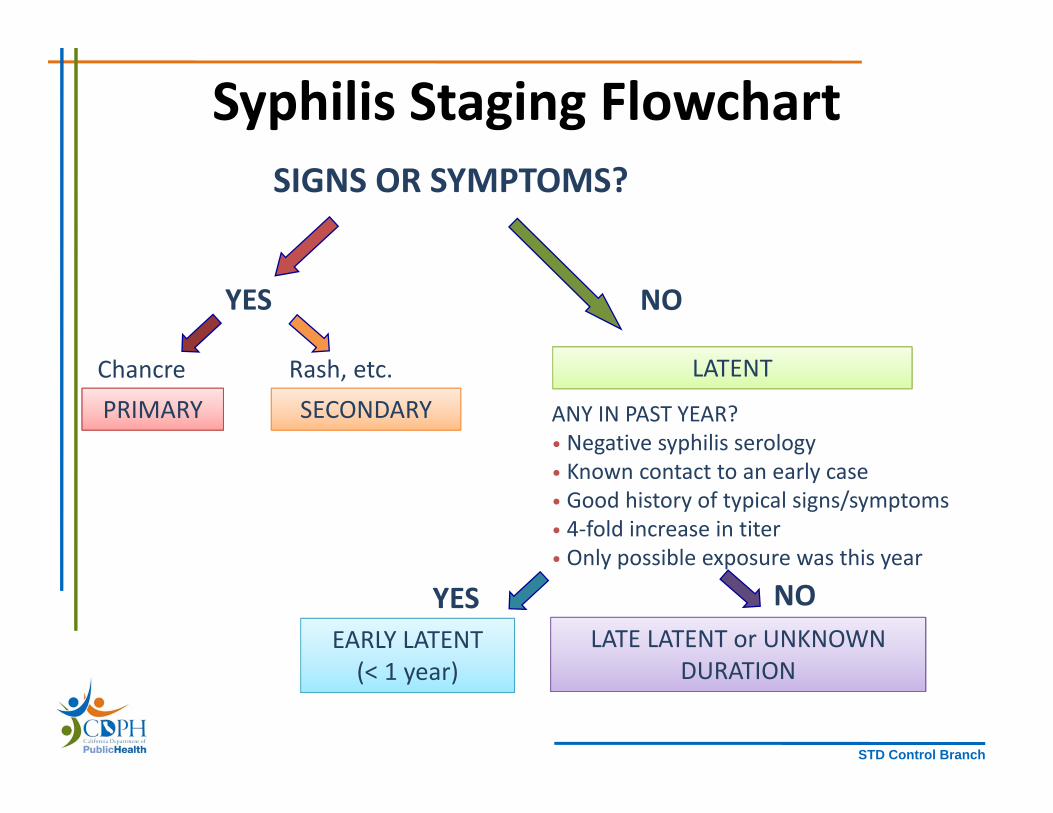
Syphilis Staging Flowchart
YES
Chancre Rash, etc.
NO
PRIMARY SECONDARYLATENT
ANY IN PAST YEAR?• Negative syphilis serology• Known contact to an early case• Good history of typical signs/symptoms • 4‐fold increase in titer• Only possible exposure was this year
NOYESEARLY LATENT(< 1 year)
LATE LATENT or UNKNOWN DURATION
SIGNS OR SYMPTOMS?

STD Control Branch
Treatment is Based on Duration of Infection
PRIMARY, SECONDARY, and EARLY LATENT (< 1 year)
LATE LATENT or UNKNOWN DURATION
Benzathine penicillin G 2.4 million units IM in a single dose
Benzathine Penicillin G 2.4 million units once per week for 3 weeks**
CDC 2015 STD Treatment Guidelines www.cdc.gov/std/treatment
**In pregnancy, must adhere to strict 7 days between doses

STD Control Branch
Brief Clinical Overview of Congenital Syphilis
Public Health Image Library, CDC

STD Control Branch
Early Congenital Syphilis (<age 2)Common Presentations
• Asymptomatic presentations are common– ~2/3 infants born with CS are asymptomatic at birth – if
untreated will develop symptoms• Bone abnormalities• Enlargement of liver +/‐ jaundice
– Hepatomegaly present in almost all infants with CS• Skin rash • Nasal discharge (“snuffles”)• Blood abnormalities• Neurologic abnormalities• Others
STD Control Branch
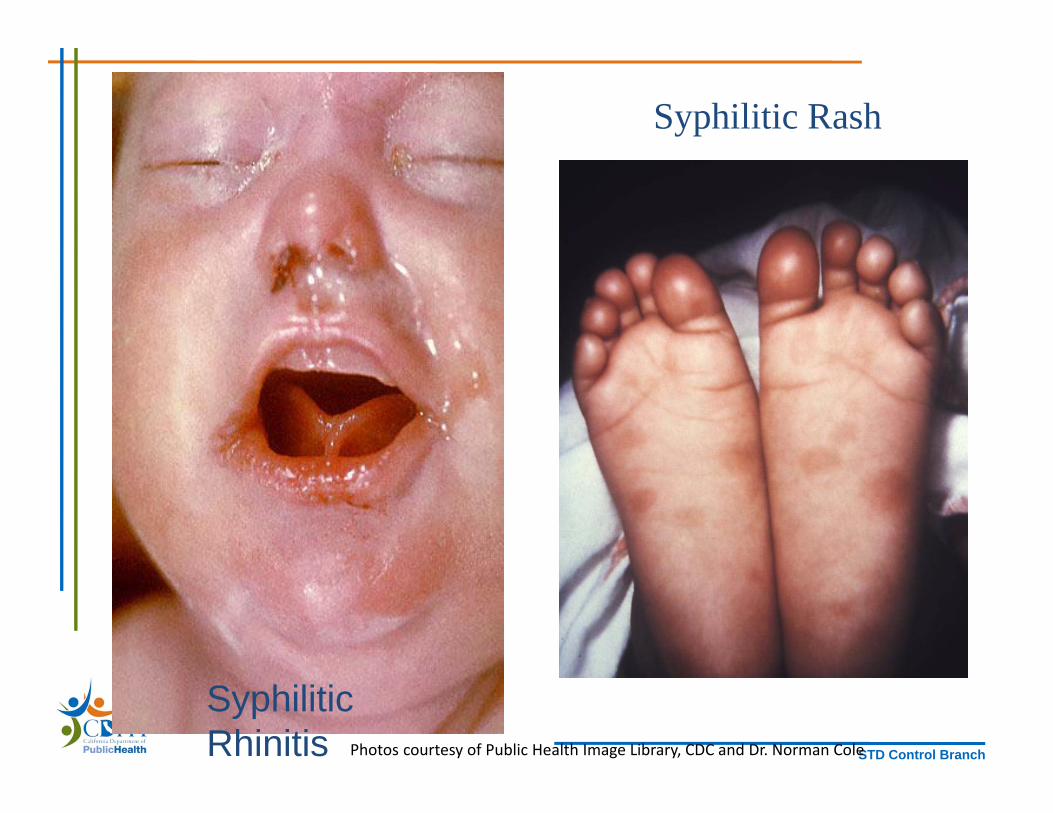
Syphilitic Rhinitis
Syphilitic Rash
Photos courtesy of Public Health Image Library, CDC and Dr. Norman Cole
STD Control Branch
Late Congenital Syphilis (>age 2)Common Presentations
• Hearing loss (puberty – adulthood).– Can develop suddenly
• Interstitial keratitis (5 years old – adulthood) – Inflammation of tissue of cornea, can lead to vision loss
• Bone or tooth abnormalities• Neurologic abnormalities• Gummas (granulomatous inflammatory response to spirochetes) in the skin or mucous membranes
• Others

STD Control Branch
Interstitial Keratitis
Photos courtesy of Public Health Image Library, CDC/Susan Lindsley

STD Control Branch
Hutchinson’s Teeth
Photos courtesy of Public Health Image Library, CDC/Susan Lindsley (left) and Robert Sumpter (rt)
Permanent incisor teeth are narrow and notched.
STD Control Branch
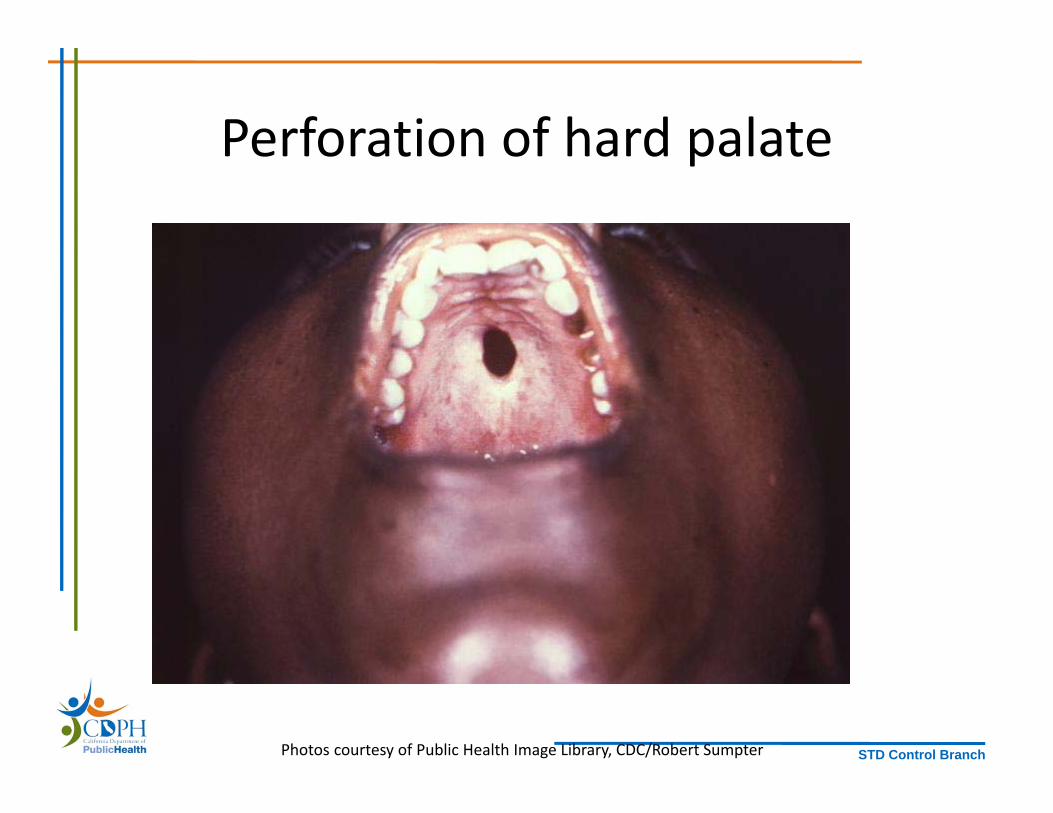
Perforation of hard palate
Photos courtesy of Public Health Image Library, CDC/Robert Sumpter

STD Control Branch
Saber ShinsClutton’s Joints
Photos courtesy of Public Health Image Library, CDC/J. Pledger
STD Control Branch
Syphilis in Pregnancy and Congenital Syphilis

STD Control Branch
Screening Recommendations – CDC
• All pregnant women should be screened for syphilis at the first prenatal visit
• Women who are at high risk for syphilis, live in areas of high syphilis morbidity, or are previously untested should be screened again both:– Early in the third trimester (approx 28 weeks GA)– At delivery
Penicillin treatment of pregnant women with syphilis is highly effective at preventing CS

STD Control Branch
Early Syphilis* among Females of Childbearing Age (15‐44)
Incidence Rates by County, California, 2016
California Counties with Third Trimester +/‐ Delivery Syphilis
Screening Recommendations for All Pregnant Women, 5/2017
* Includes primary, secondary, and early latent syphilis. Rev. 4/18/2017All 2016 data are provisional

STD Control Branch
CDC Screening Recommendations
• No infant should leave the hospital without the maternal serologic status having been determined at least once during pregnancy, and again at delivery if at risk.– If mother presents at delivery with no prenatal care, STAT RPR should be performed
– If baby has congenital syphilis and is asymptomatic, there is still an opportunity to treat the infant to prevent further morbidity
• Any woman who delivers a stillborn infant should be tested for syphilis

STD Control Branch
Treatment of Syphilis in Pregnancy
• The only treatment of syphilis in pregnancy is penicillin. There are no alternatives.
• Pregnant women should be treated with the penicillin regimen appropriate for their stage of infection.– Some experts recommend a 2nd dose of benzathinepenicillin G be given a week after the initial dose in early syphilis
• Pregnant women with penicillin allergy should be desensitized and treated with penicillin.
All patients with syphilis should be tested for HIV.
STD Control Branch
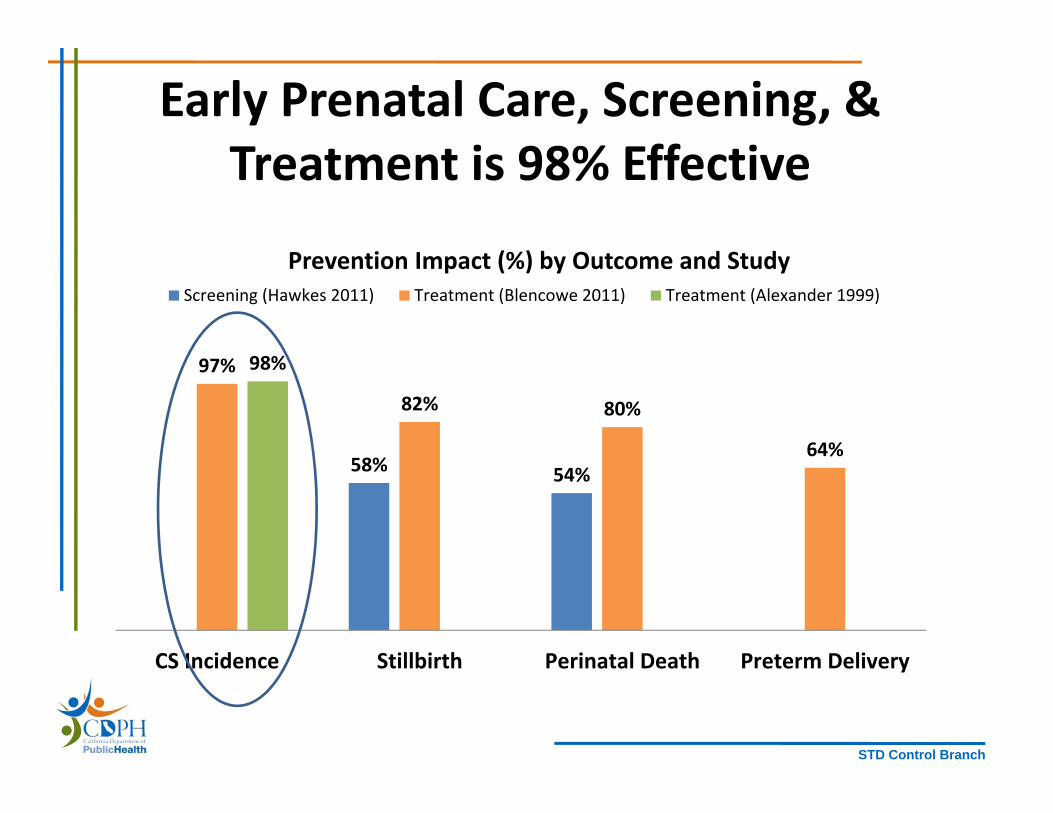
Early Prenatal Care, Screening, & Treatment is 98% Effective
58% 54%
97%
82% 80%
64%
98%
CS Incidence Stillbirth Perinatal Death Preterm Delivery
Screening (Hawkes 2011) Treatment (Blencowe 2011) Treatment (Alexander 1999)
Prevention Impact (%) by Outcome and Study
STD Control Branch
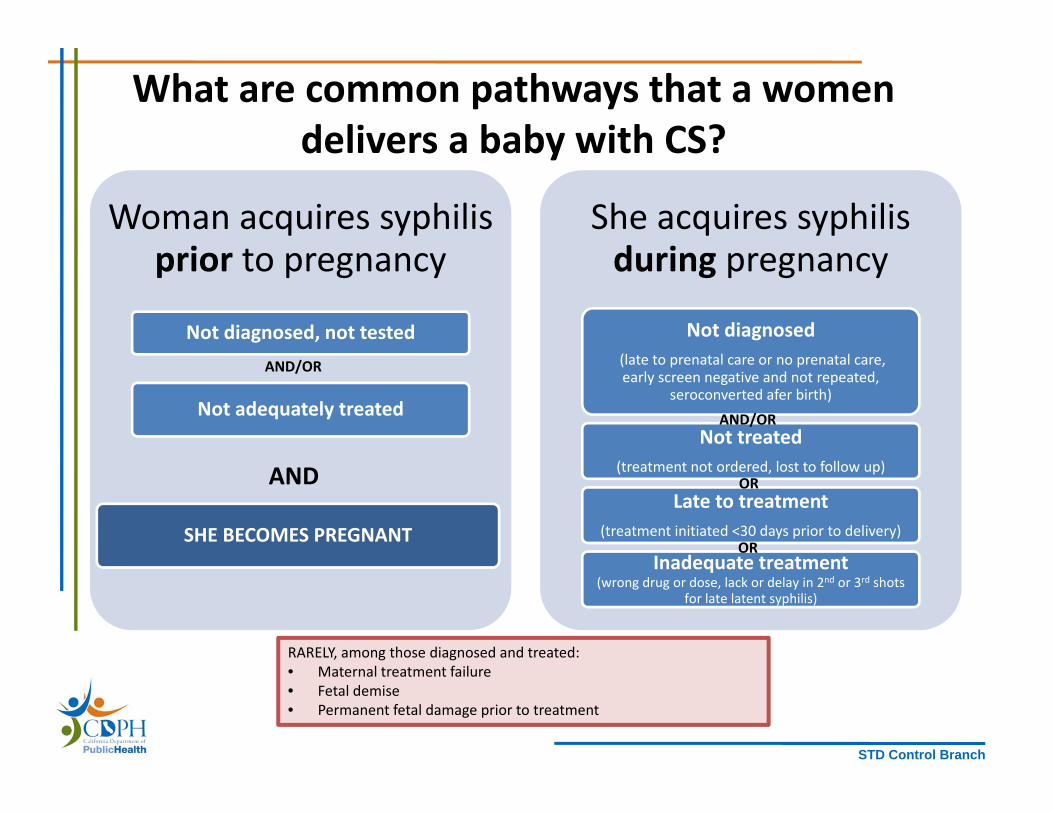
What are common pathways that a women delivers a baby with CS?
Woman acquires syphilis prior to pregnancy
Not diagnosed, not tested
Not adequately treated
SHE BECOMES PREGNANT
She acquires syphilis during pregnancy
Not diagnosed(late to prenatal care or no prenatal care, early screen negative and not repeated,
seroconverted afer birth)
Not treated (treatment not ordered, lost to follow up)
Late to treatment (treatment initiated <30 days prior to delivery)
Inadequate treatment (wrong drug or dose, lack or delay in 2nd or 3rd shots
for late latent syphilis)
AND/OR
AND/OR
OR
OR
AND
RARELY, among those diagnosed and treated: • Maternal treatment failure• Fetal demise • Permanent fetal damage prior to treatment

STD Control Branch
What do we know about the cases?California Project Area CS Cases 2007‐2015:
Infant Characteristics (n=391)
30%
32%
9%
10%
11%
7%
0 5 10 15 20 25 30 35
Preterm birth
Abnormal CSF
Reactive CSF VDRL
Long bone abnormalities
Signs of CS on exam
Stillbirth
Credits: Stoltey, Ng

STD Control Branch
Number of congenital syphilis cases, by maternal stage:
Majority of mothers had late syphilis
0102030405060708090100110120130
2007(n=36)
2008(n=26)
2009(n=28)
2010(n=20)
2011(n=18)
2012(n=23)
2013(n=50)
2014(n=70)
2015(n=120)
# of con
genital syphilis cases
Late syphilis Early syphilis Unknown stage
62%61%56% 63%50%61%42%61% 65%
Credits: Stoltey, Ng
STD Control Branch
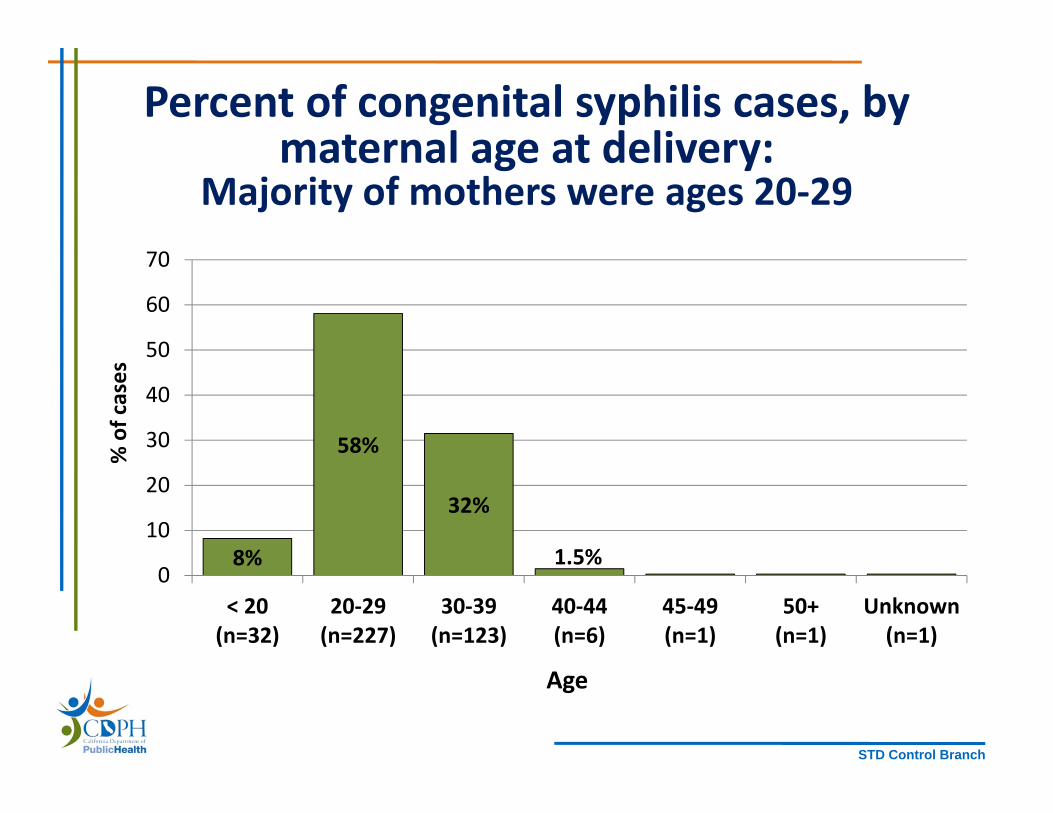
Percent of congenital syphilis cases, by maternal age at delivery:
Majority of mothers were ages 20‐29
8%
58%
32%
1.5%0
10
20
30
40
50
60
70
< 20(n=32)
20‐29(n=227)
30‐39(n=123)
40‐44(n=6)
45‐49(n=1)
50+(n=1)
Unknown(n=1)
% of cases
Age
64%
61%56%
59%

STD Control Branch
Congenital SyphilisIncidence Rates per 100,000 (L) and Number of Cases (R) by Race/Ethnicity of
Mother, California, 2016
0
25
50
75
100
125
NA/AN API Black Latina White
Rev. 1/2017
0
25
50
75
100
NA/AN API Black Latina White
Incidence Rates Number of Cases
STD Control Branch
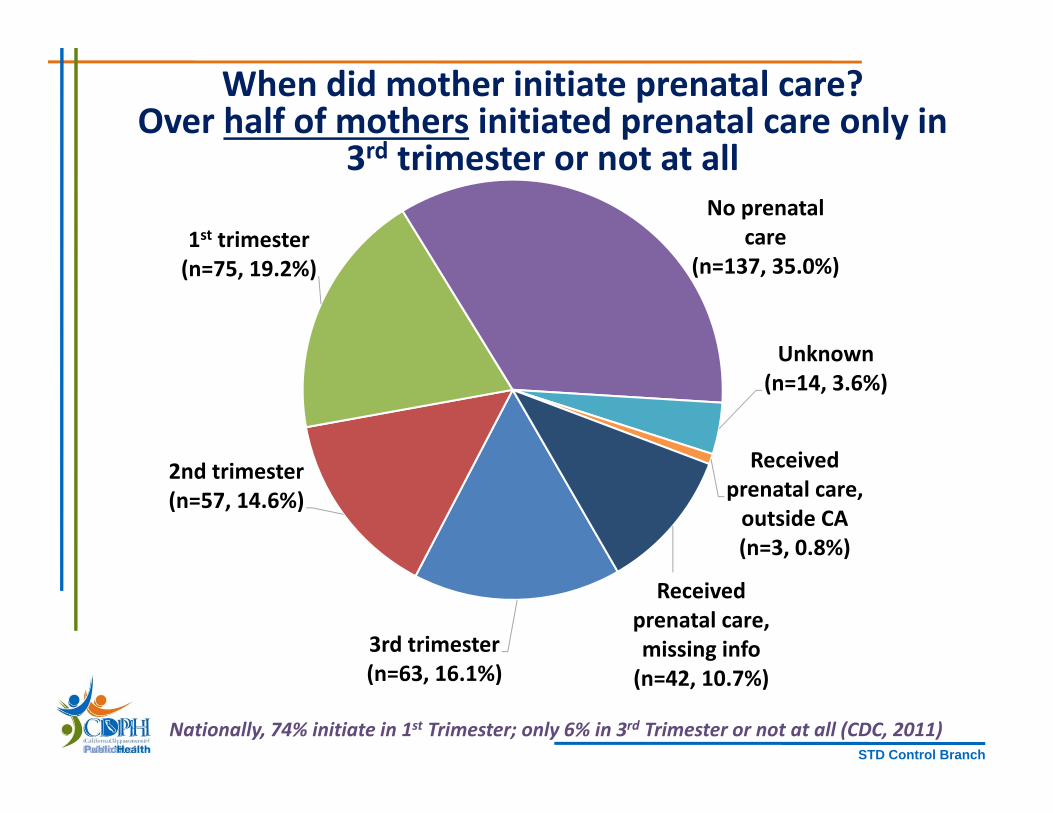
3rd trimester(n=63, 16.1%)
2nd trimester(n=57, 14.6%)
1st trimester(n=75, 19.2%)
No prenatal care
(n=137, 35.0%)
Unknown(n=14, 3.6%)
Received prenatal care, outside CA(n=3, 0.8%)
Received prenatal care, missing info(n=42, 10.7%)
When did mother initiate prenatal care?Over half of mothers initiated prenatal care only in
3rd trimester or not at all
Nationally, 74% initiate in 1st Trimester; only 6% in 3rd Trimester or not at all (CDC, 2011)
STD Control Branch
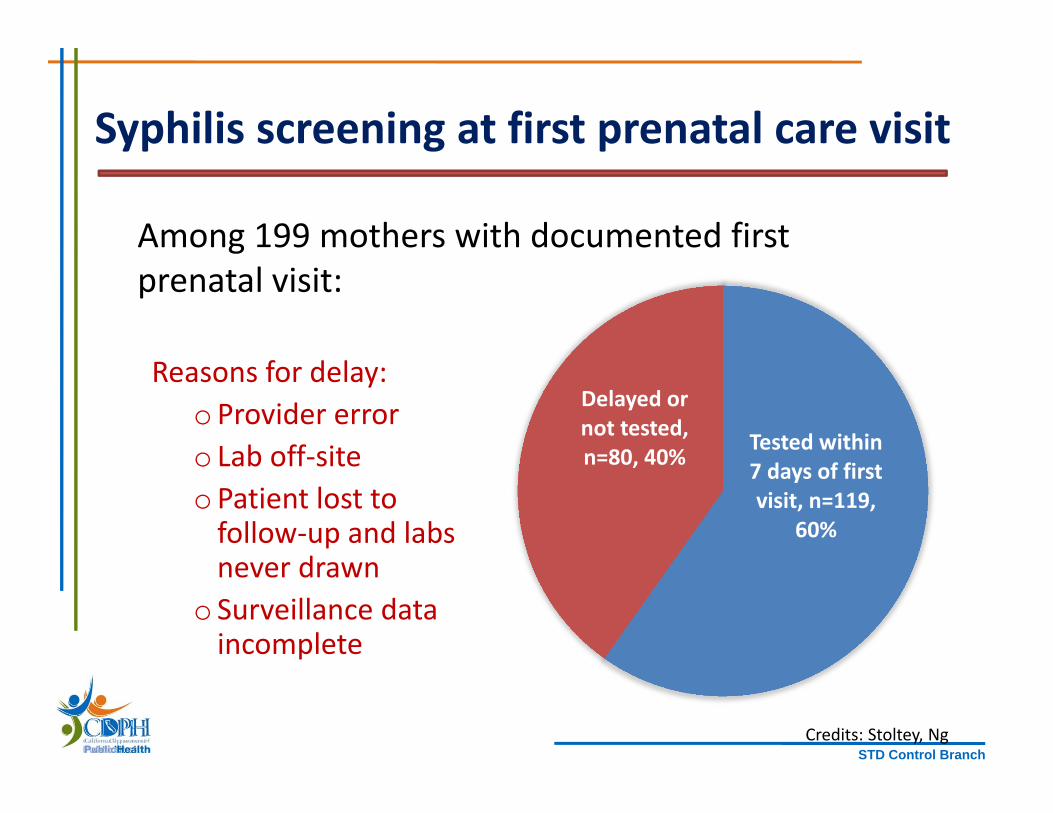
Syphilis screening at first prenatal care visit
Reasons for delay:oProvider erroro Lab off‐siteoPatient lost to follow‐up and labs never drawn
o Surveillance data incomplete
Tested within 7 days of first visit, n=119,
60%
Delayed or not tested, n=80, 40%
Among 199 mothers with documented first prenatal visit:
Credits: Stoltey, Ng

STD Control Branch
Treatment of mothers accessing prenatal care in 1st/2nd trimester with reactive test ≥ 30 days
prior to delivery (n=67)
31%
27%
16%
15%
10%
Treated Inappropriately
n=21
Adequately Treatedn=18
Not Treatedn=11
Started Treatment < 30 Days Before Deliveryn=10
Unknown Treatment
n=7

STD Control Branch
Maternal risk characteristics forinterviewed early syphilis cases (n=92)
70% (92 of 132) interviewed
22%
6.5%13%
44%
13% 13%
05101520253035404550
Methamphetamine use Exchange of sex for money,drugs
Jail, juvenile hall, prison
%
Risk in 12 months prior to diagnosis
2007‐12 (n=46) 2013‐15 (n=46)n=20
n=10
n=3
n=6 n=6 n=6

STD Control Branch
What will it take to eliminate CS?
• How can we use the epi data to drive program? • What additional data would be helpful?• How do we prioritize congenital syphilis prevention?• What partnerships should be leveraged?• How can we measure our effectiveness?• Are there policy solutions?
Previous Outbreaks in the U.S.
Crack cocaine, exchange for sex, NYC 1986‐88
Rural South, South Carolina 1991‐1993
Indian reservation, Arizona 2007‐2009
Chinese birth tourism, Los Angeles 2014
• Response requires customized strategies
STD Control Branch
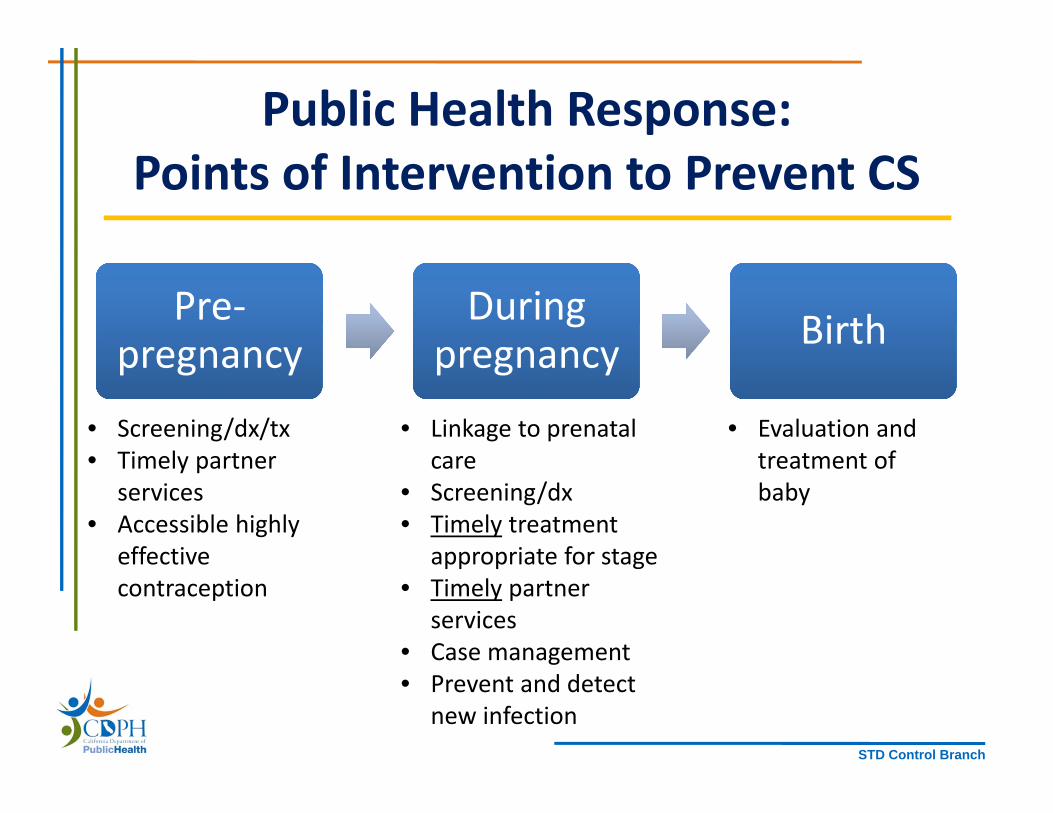
Public Health Response: Points of Intervention to Prevent CS
Pre‐pregnancy
Pre‐pregnancy
During pregnancyDuring
pregnancy BirthBirth
• Screening/dx/tx• Timely partner
services• Accessible highly
effective contraception
• Linkage to prenatal care
• Screening/dx• Timely treatment
appropriate for stage• Timely partner
services• Case management• Prevent and detect
new infection
• Evaluation and treatment of baby
STD Control Branch
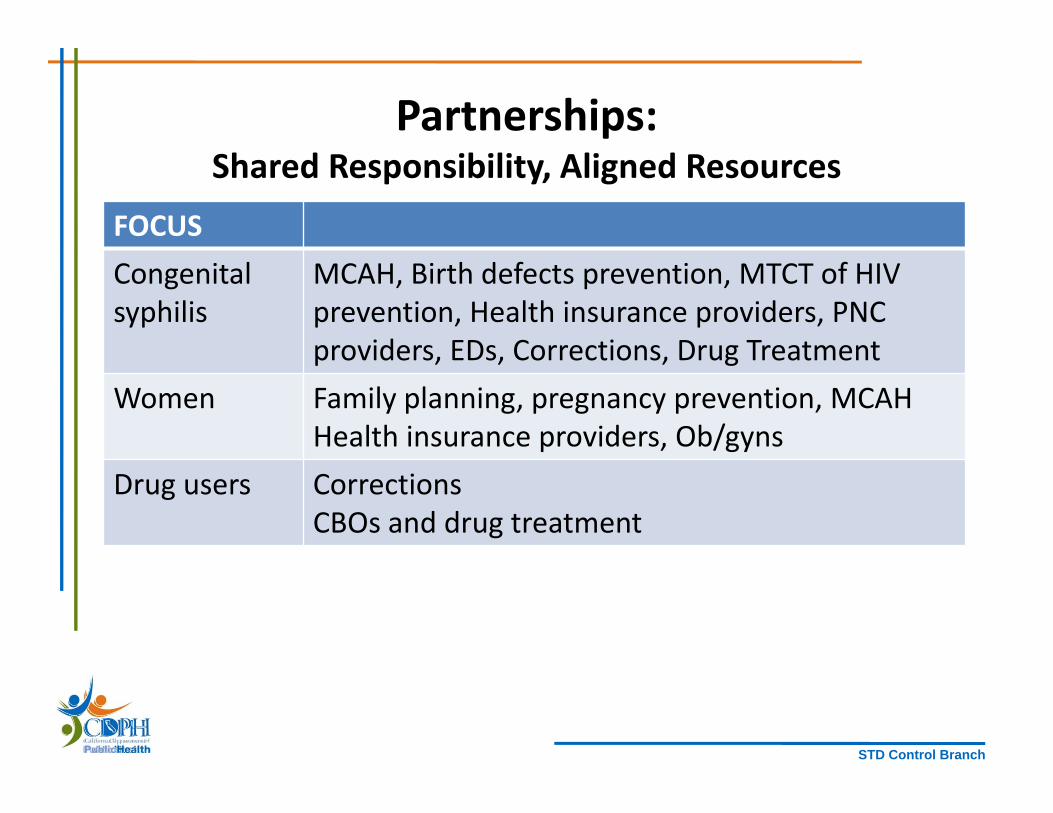
Partnerships: Shared Responsibility, Aligned Resources
FOCUSCongenital syphilis
MCAH, Birth defects prevention, MTCT of HIV prevention, Health insurance providers, PNC providers, EDs, Corrections, Drug Treatment
Women Family planning, pregnancy prevention, MCAHHealth insurance providers, Ob/gyns
Drug users CorrectionsCBOs and drug treatment

STD Control Branch
Congenital Syphilis Prevention Cascade, California Project Area 2007‐2014
10077 73 63
37
0
10
20
30
40
50
60
70
80
90
100
Infected with syphilis Received Prenatal Carein 1st or 2nd Trimester
Received SyphilisTesting >= 30 daysbefore delivery
Received timelyappropriate treatment
% Pregnant Women with Syphilis
Opportunity for Prevention of Disease and Complications
CS Cases PREVENTED
~4x More NON‐Pregnant Women with Syphilis
STD Control Branch
Congenital Syphilis
Prevention
Clinical
Policy
Surveillance/ Epidemiology
Disease Investigation
Health Promotion
STD Control Branch
Patient Education Materials
If you would like to customize and distributewithin your LHJ, contact Ashley Dockter at [email protected]

STD Control Branch
STD Control Branch
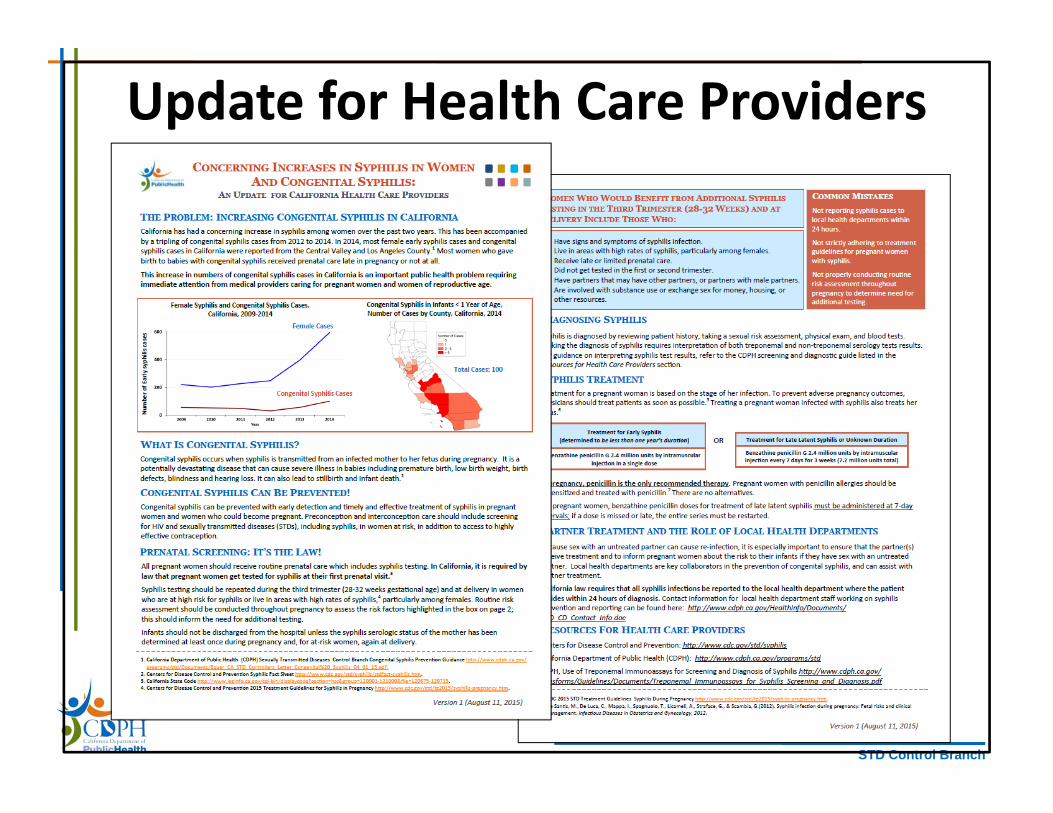
Update for Health Care Providers
STD Control Branch
STD Control Branch
STD Control Branch

STD Control Branch
STD Control Public Health ResponseConfirm pregnancy status on lab reports (females)
Prioritization by age, gender, pregnancy status
Ensure timely treatment of pregnant women
Contact tracing, partner testing and treatment
Field testing sexual/social contacts
Ensure adequate work up and treatment of neonates
STD Control Branch
Pre‐Pregnancy Prevention & Screening Strategies
Pregnancy prevention (LARC)
Pregnancy testing
Drug and mental health treatment
Venue‐based Screening
(Corrections*)
Syphilis screening & treatment in non‐pregnant
women
Syphilis screening & treatment of
MSW
STD Control Branch
Screening Adult Females in Correctional Settings: A Promising Approach
INTERVENTION: Qualitative (or STAT) RPR testing Search syphilis case registry database Treatment at the time of medical evaluation
OUTCOMES:• Treatment indicated for 190/760 (26%)• Increased syphilis treatment from 7% to 84% • Prevented 7 out of 8 potential congenital syphilis cases because
mother was treated before discharge from correctional facility• Cost: $8,200 to hook up STAT RPR equipment and registry and
$0.25 per STAT RPR screening test
Blank, S., et al. (1997). "New approaches to syphilis control. Finding opportunities for syphilis treatment and congenital syphilis prevention in a women's correctional setting." Sex Transm Dis 24(4): 218‐226.

STD Control Branch
Media
STD Control Branch
Areas for potential synergistic efforts in prevention of congenital syphilis?
• Case management of pregnant women at high risk?• Outreach to pregnant women who are not accessing
prenatal care ?• Alignment with Fetal and Infant Mortality Review in select
counties?• Outreach to delivery hospitals in high‐morbidity regions?• Strengthen health care provider/public health partnership
in prevention of congenital syphilis?• Include information about congenital syphilis in provider
education activities?

STD Control Branch
Take‐Home Points:Congenital Syphilis in California
• Female syphilis and congenital syphilis cases are increasing in California.
• Most congenital syphilis cases canand should be prevented.
• What activities, opportunities, and partnerships are available in your local health jurisdiction to assist with congenital syphilis prevention?
• What information can the CDPH STD Control Branch provide that would enhance prevention efforts in your counties?
Clinical Guidelines and Consultation
www.cdc.gov/std/treatment/www.std.ca.gov
Clinician Warmline
510‐620‐3400
CDC STD Treatment Guidelines AppAvailable now, free
Thanks! [email protected]‐620‐3408