unravelling renal tubular acidosis (rta)
TRANSCRIPT
UnravellingUnravelling RRenal enal TTubular ubular AAcidosis (cidosis (RTARTA))
Robert Unwin(Centre for Nephrology – London Epithelial Group – University College London)
•A definition of RTA
•Clinical aspects of RTA
•Underlying (molecular) mechanisms of RTA
•An unanswered question in (distal) RTA – the puzzle of potassium
An outline of my talk
A definition of A definition of RTARTA
Impaired renal acid excretion (as suggested
by a raised urine pH) in the context of a:
Hyperchloraemic, Hyperchloraemic, normalnormal anion gap anion gap
metabolic metabolic acidosisacidosis and and normalnormal GFRGFR*
(*To distinguish it from ‘‘uraemic acidosisuraemic acidosis’’ -- CRFCRF)
• Type 1Type 1 - distaldistal RTA (most common) – ‘complete’ and
‘incomplete’ (Oliver Wrong) - hypohypokalaemickalaemic
• Type 2Type 2 - proximalproximal RTA (often part of a renal Fanconi
syndrome)
• (Type 3 (Type 3 -- a poorly a poorly characterisedcharacterised mixture of 1 and 2 in infants and mixture of 1 and 2 in infants and
which may reflect an which may reflect an ‘‘immatureimmature’’ renal tubule or, more generally renal tubule or, more generally
accepted, CA(II) deficiencyaccepted, CA(II) deficiency))
• Type 4Type 4 - hypohypoaldosteronismaldosteronism (real or apparent) - distal-
like – hyperhyperkalaemickalaemic (impaired NH(impaired NH44++ generation/excretion)generation/excretion)
The The enen(n)(n)ccumberedumbered ‘‘clinicalclinical’’ classification of classification of RTARTA
To maintain systemic acidTo maintain systemic acid--base balance base balance the kidneys:the kidneys:
•• ReclaimReclaim almost all the filtered HCO3- (by H+
secretion) - and also generate ‘new’ HCO3- (from
NH3/NH4+ synthesis)
•• ExcreteExcrete ca. 40-70 mmol H+ per day (~1 mmol/kg - by H+ secretion) - depending on diet -to produce an acid (relative to plasma) urine
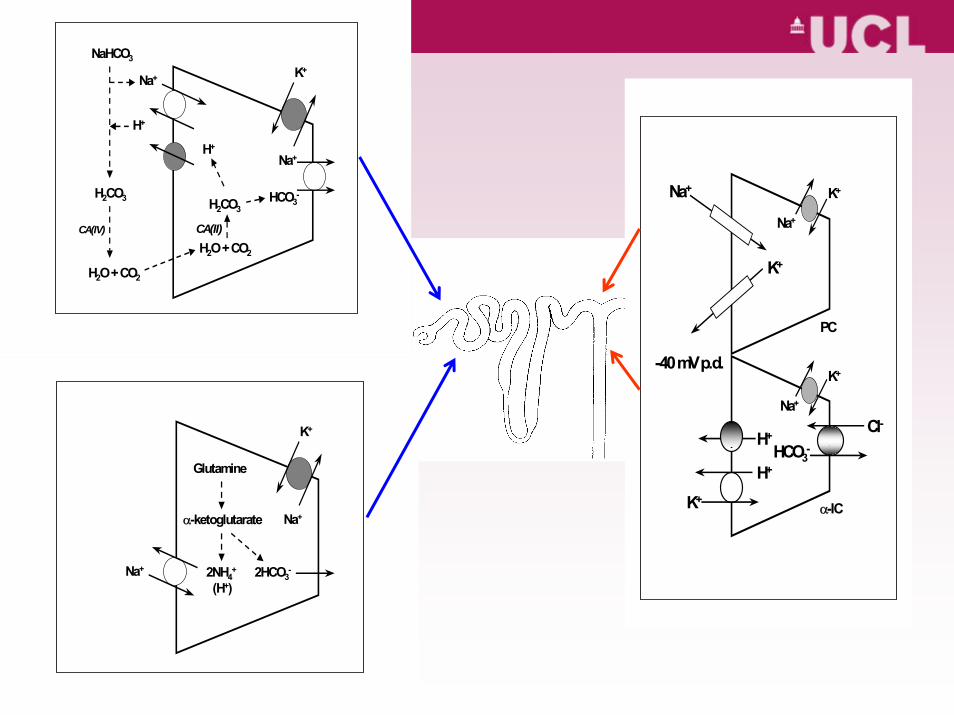
Main sites of HMain sites of H++ secretion:secretion:
•• HCOHCO33-- reabsorptionreabsorption - proximal nephron (PT
and LOH) - >90% of filtered load
•• Net acid excretionNet acid excretion and residual HCO3-
reabsorption (ammonium plus titratable acid minus
bicarbonate) - distal nephron (DT & CD)
Na+
Na+
K+
H+
H2CO3
H2O + CO2
CA(IV)
H2O + CO2
H2CO3HCO3
-
H+
NaHCO3
CA(II)
Na+
Na+
K+
2HCO3-
(H+)
Glutamine
α-ketoglutarate
2NH4+
Na+
K+Na+
K+
-40 mV p.d.K+
Na+
H+
K+
H+ Cl-
HCO3-
PC
α-IC
What can determine urine pH?What can determine urine pH?
Urinary free [H+] depends on- tubular H+ secretion- tubular fluid buffer content (NH4
+ and Pi)
Urine pH can be because of- infection (urea-splitting)- left standing (CO2 loss)- high NH4
+ content*
(*A failure to lower urine pH following an acute acid load might indicate H+ secretion OR NH3 and
NH4+ excretion)
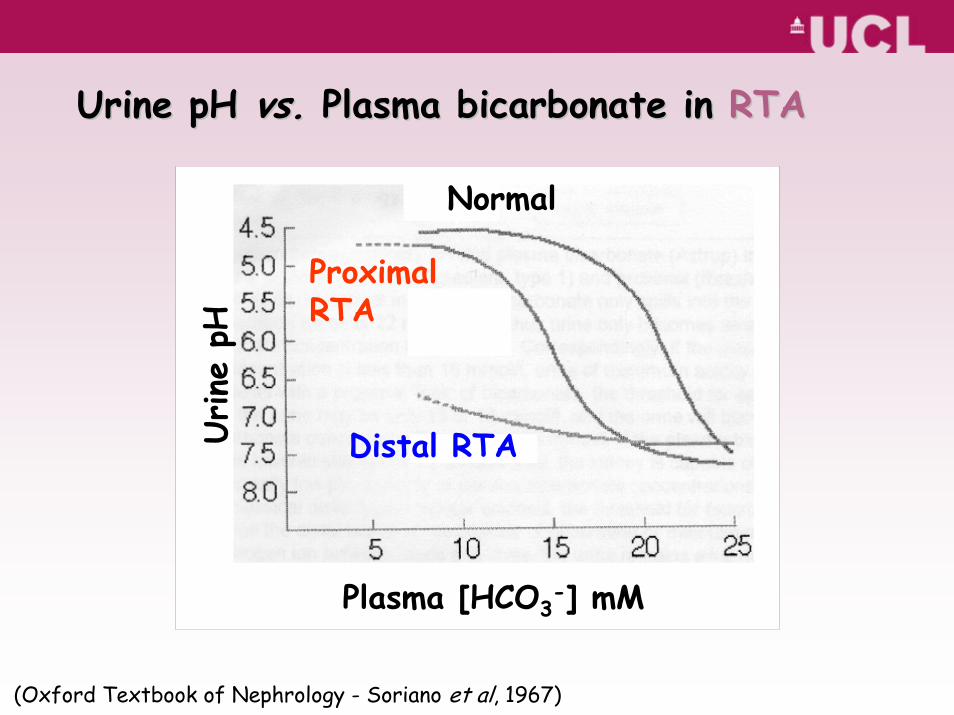
Urine
pH
Plasma [HCO3-] mM
Normal
ProximalRTA
Distal RTA
(Oxford Textbook of Nephrology - Soriano et al, 1967)
Urine pH Urine pH vs.vs. Plasma bicarbonate in Plasma bicarbonate in RTARTA
Diagnosis of Diagnosis of RTARTA
• In the presence of systemic acidosis (plasma [HCO3-]
<20 mM), urine >5.3
• Casual EMU (second void preferable) pH >5.5* (and lowcitrate/creatinine ratio in alkaline urine)
Tests of urinary acidification:- ‘short’ NH4Cl (Wrong & Davies) (dRTA)
- frusemide and fludrocortisone (modified Batlle) (dRTA)
- bicarbonate loading and fractional HCO3- excretion
(pRTA)- (urine - blood) pC02 (but is it valid in the presence of nephrocalcinosis?)- urine anion (net charge) and osmolar gaps as surrogates for NH4
+
excretion
• A failure of tubular cell ion transport (H+ or HCO3-)
- including driving force (voltage defect - aldosterone, amiloride)
• A failure of H+ generation (e.g. lack of carbonic anhydrase - CA(II))
• A failure to maintain an H+ gradient – ‘leaky’ apical (luminal) cell membrane (e.g. amphotericin)
• A failure of NH4+ generation (e.g. in hyperkalaemia)
or its ‘circulation’ within the kidney
Mechanisms of Mechanisms of RTARTA
•Fanconi syndrome - drug-induced, heavy metals, inherited metabolic disorders
•CA inhibitors – acetazolamide
•CA(II) mutation(s) - autosomal recessive (Sly et al)
•Na+-HCO3- (NBC1 - SLC4A4) mutation(s) -
autosomal recessive (Igarashi et al)
ProximalProximal RTARTA
Hypokalaemia variable Nephrocalcinosis/renal stones less common
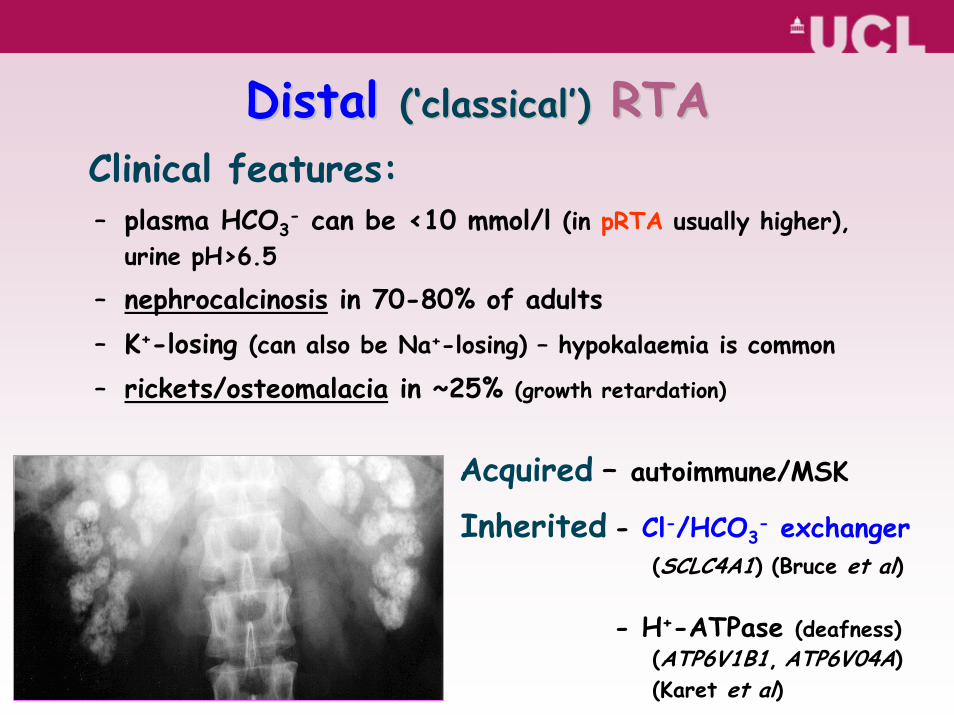
Clinical features:– plasma HCO3
- can be <10 mmol/l (in pRTA usually higher), urine pH>6.5
– nephrocalcinosis in 70-80% of adults– K+-losing (can also be Na+-losing) – hypokalaemia is common
– rickets/osteomalacia in ~25% (growth retardation)
Acquired – autoimmune/MSK
Inherited - Cl-/HCO3- exchanger
(SCLC4A1) (Bruce et al)
- H+-ATPase (deafness)(ATP6V1B1, ATP6V04A)(Karet et al)
DistalDistal ((‘‘classicalclassical’’)) RTARTA
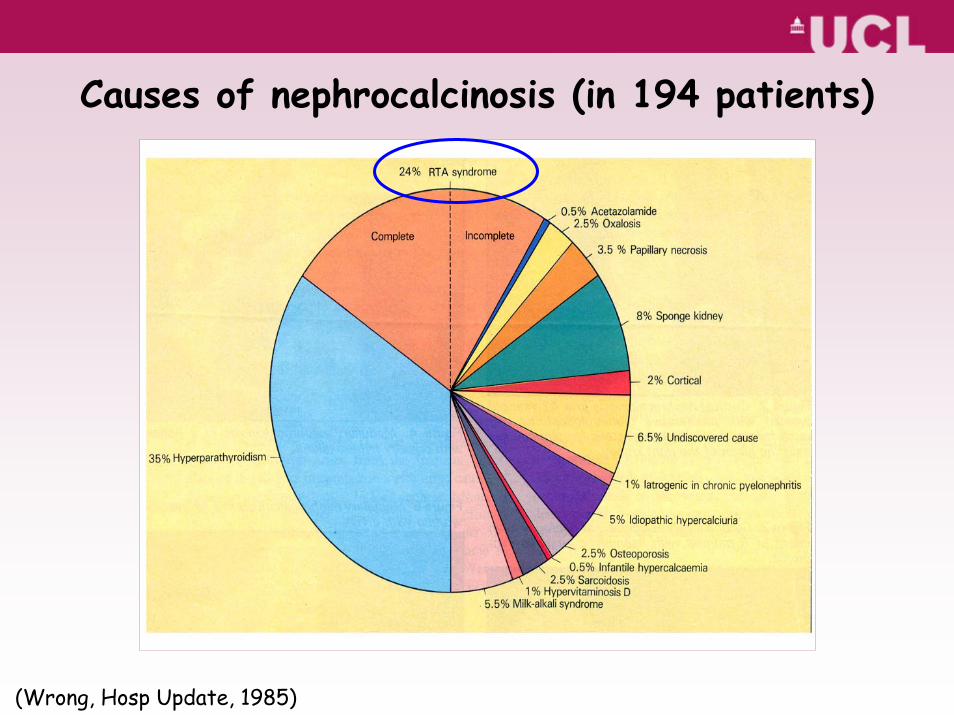
Causes of nephrocalcinosis (in 194 patients)
(Wrong, Hosp Update, 1985)
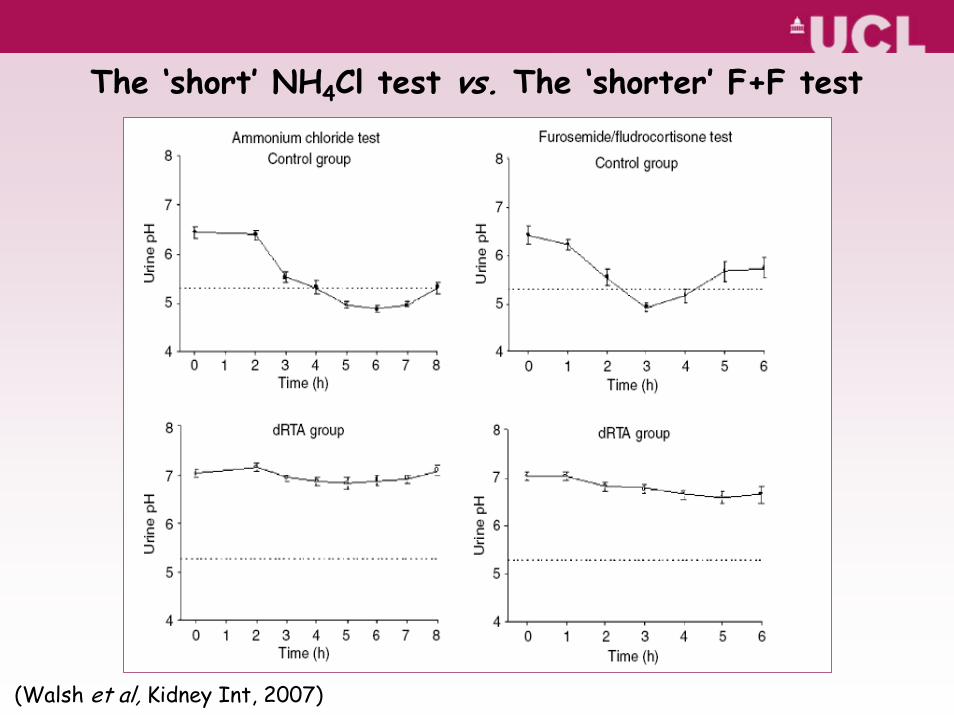
(Walsh et al, Kidney Int, 2007)
The ‘short’ NH4Cl test vs. The ‘shorter’ F+F test
Empirical TreatmentEmpirical Treatment
•• Alkali therapyAlkali therapy in small doses (already used in ancient India for ‘calculi’) - 1-2 mmol/kg; target plasma [HCO3
-] >20 mmol/l
– to heal bones
– prevention of stones/(limit progression of nephrocalcinosis?)
• K+ supplements may be necessary
• (Vitamin D may be necessary)
• (Thiazide diuretics may help in pRTA)
• Long-term follow-up for renal stone complications
CITRITRATETE
BBIICCAARRBBOONNAATTEE
FFRRUUIITTSVEGETVEGETABLESBLESAA
LLKKAALLII
++
In essence…
0
1 0 0
0.8
1.2
1.9
3.0
14
9
6
4
1.00.50.20.1
1.8
2.6
3.8
5.5
0.5
1.1
2.5
5.7
7.8
7.1
6.4
5.7
4.7 5.3 5.9 6.6
2.3
3.4
5.1
7.6
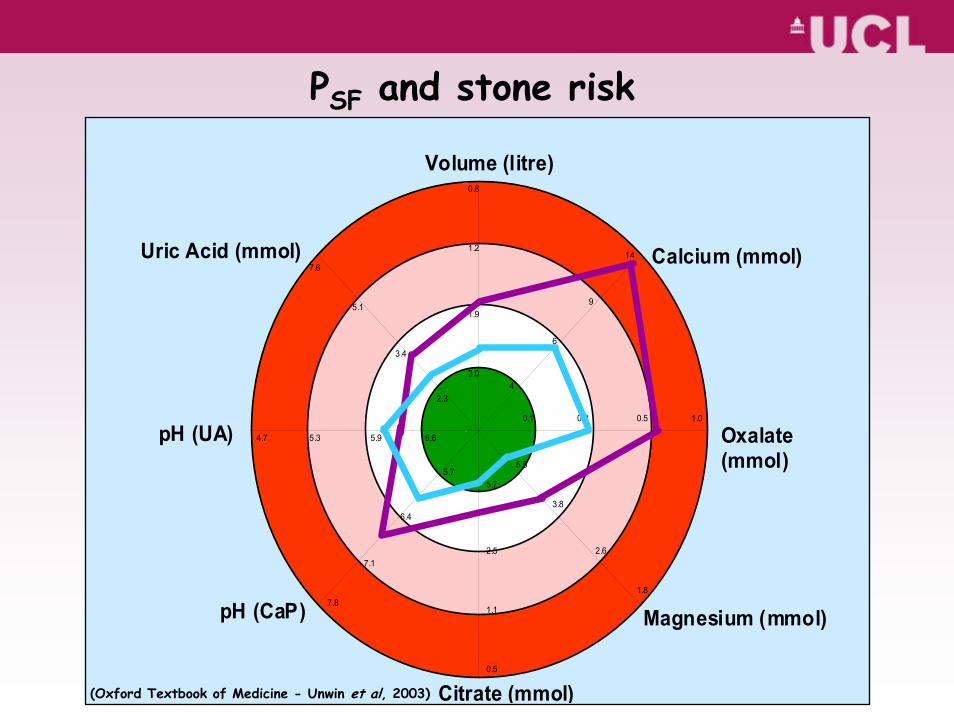
Volume (litre)
Calcium (mmol)
Oxalate(mmol)
Magnesium (mmol)pH (CaP)
pH (UA)
Uric Acid (mmol)
Citrate (mmol)
PSF and stone risk
(Oxford Textbook of Medicine - Unwin et al, 2003)
0.9999 -
0.999 -
0.99 -
0.9 -
0.5 -
0.1 -
0.01 -
0.001 -
0.0001 -
Relative
Pro
babi
lity
(PRe
lative
Pro
babi
lity
(PSFSF))
0
1
2
3
4
5
6
7
8
9
10
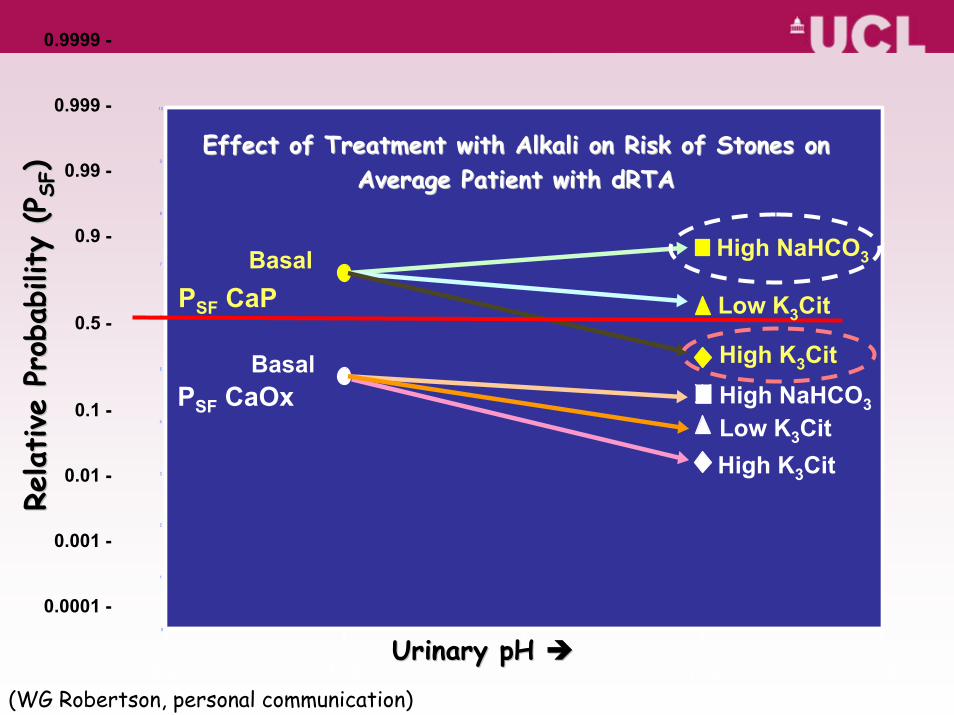
6.2 6.6 7 7.4 7.8Urinary pH Urinary pH
PSF CaP
High NaHCO3
PSF CaOx High NaHCO3
High K3CitLow K3Cit
High K3Cit
Low K3Cit
Effect of Treatment with Alkali on Risk of Stones on Effect of Treatment with Alkali on Risk of Stones on Average Patient with dRTAAverage Patient with dRTA
Basal
Basal
(WG Robertson, personal communication)
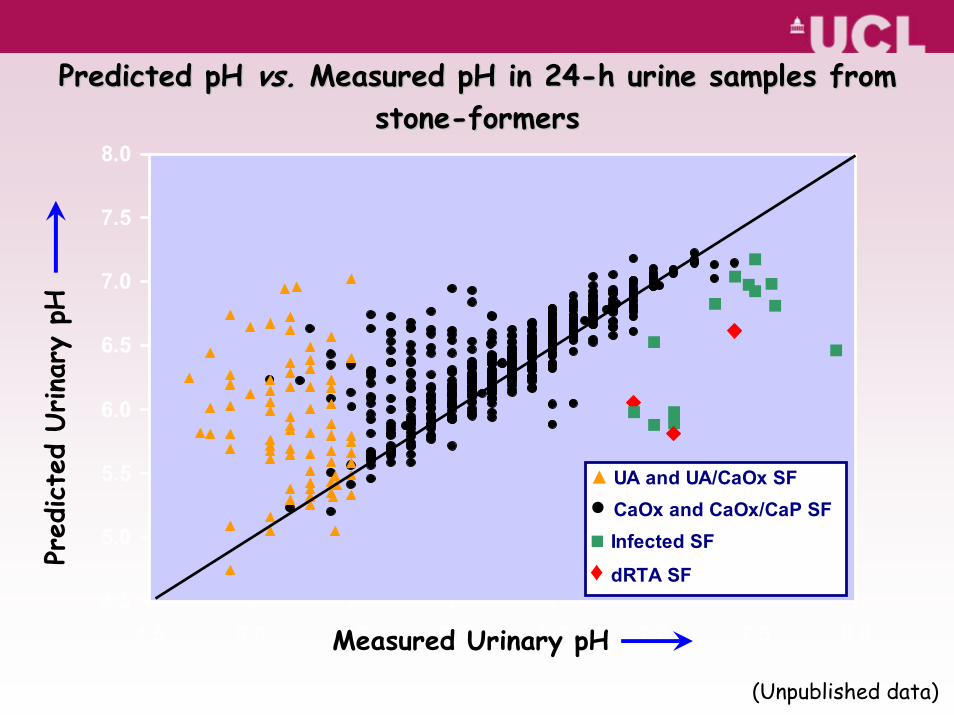
4.5
5.0
5.5
6.0
6.5
7.0
7.5
8.0
4.5 5.0 5.5 6.0 6.5 7.0 7.5 8.0
▲ UA and UA/CaOx SF● CaOx and CaOx/CaP SF■ Infected SF♦ dRTA SF
Predicted pH Predicted pH vs.vs. Measured pH in 24Measured pH in 24--h urine samples from h urine samples from stonestone--formersformers
Pred
icte
d Urina
ry p
H
Measured Urinary pH
(Unpublished data)
Acidosis and Potassium ExcretionAcidosis and Potassium Excretion
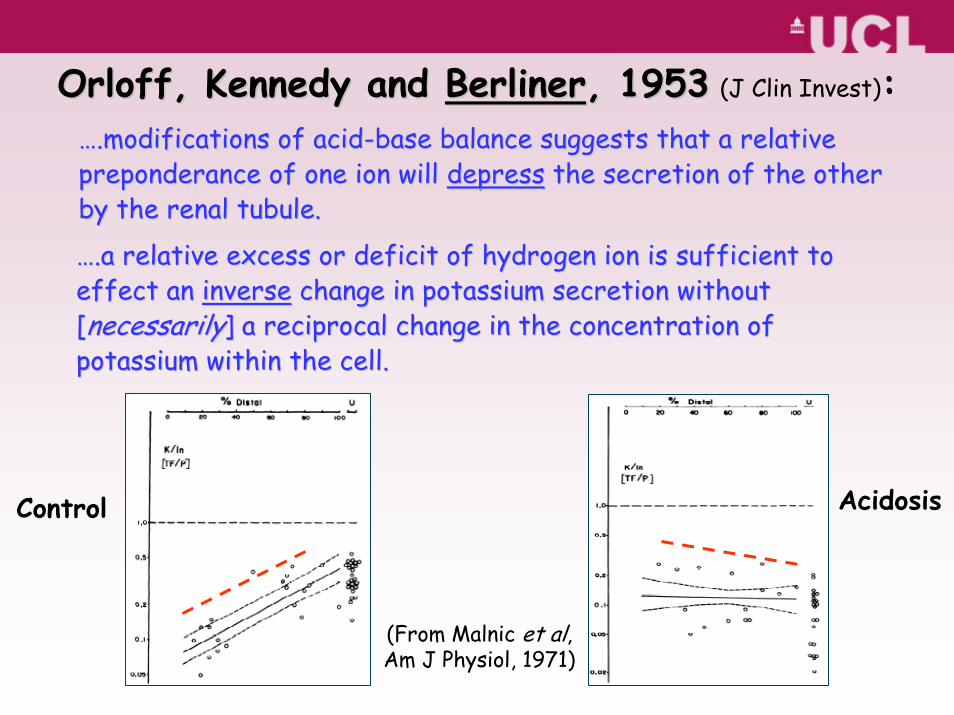
OrloffOrloff, Kennedy and , Kennedy and BerlinerBerliner, 1953, 1953 (J Clin Invest):…….modifications of acid.modifications of acid--base balance suggests that a relative base balance suggests that a relative preponderance of one ion will preponderance of one ion will depressdepress the secretion of the other the secretion of the other by the renal tubule.by the renal tubule.
…….a relative excess or deficit of hydrogen ion is sufficient to .a relative excess or deficit of hydrogen ion is sufficient to effect an effect an inverseinverse change in potassium secretion without change in potassium secretion without [[necessarilynecessarily] a reciprocal change in the concentration of ] a reciprocal change in the concentration of potassium within the cell.potassium within the cell.
Control Acidosis
(From Malnic et al,Am J Physiol, 1971)
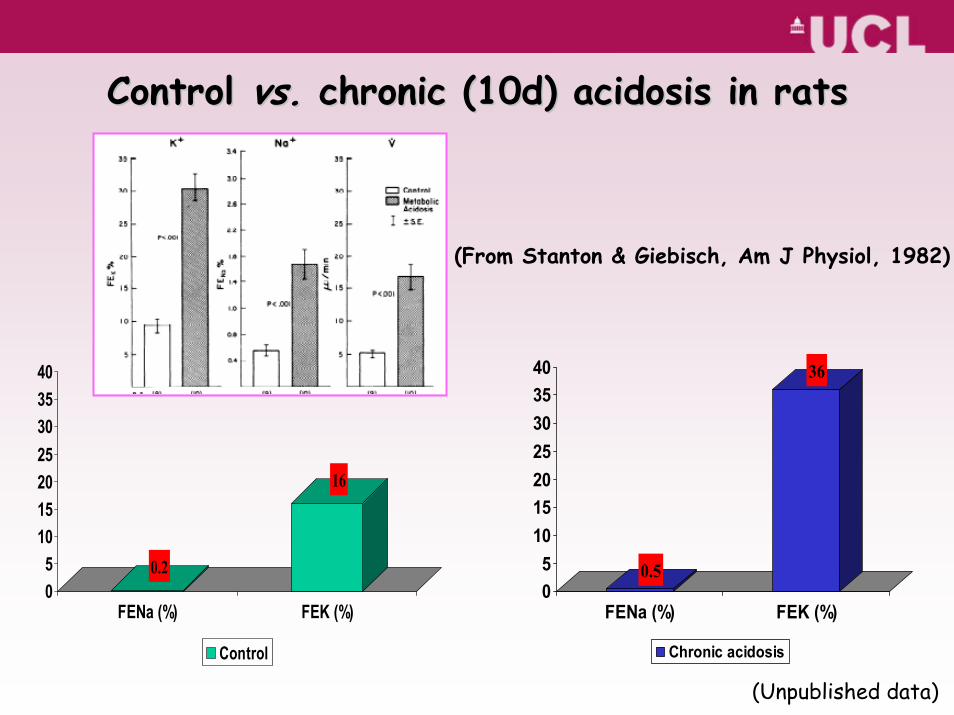
Control Control vs.vs. chronic (10d) acidosis in ratschronic (10d) acidosis in rats
(Unpublished data)
0.2
16
05
10152025303540
FENa (%) FEK (%)
Control
0.5
36
05
10152025303540
FENa (%) FEK (%)
Chronic acidosis
(From Stanton & Giebisch, Am J Physiol, 1982)
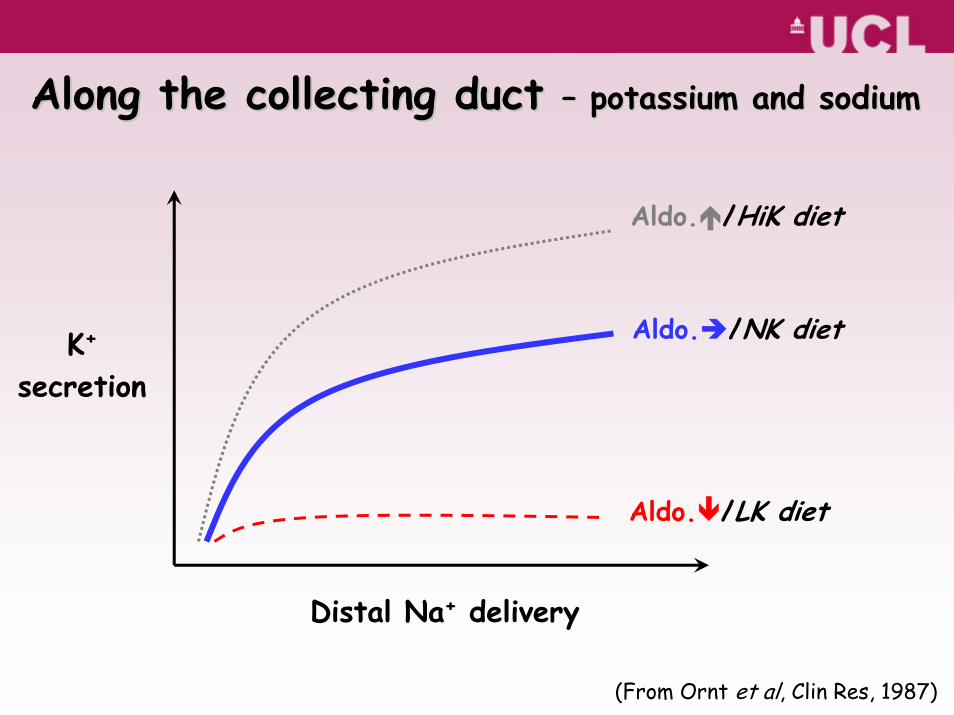
Aldo. /HiK diet
Aldo. /NK diet
Aldo. /LK diet
Distal Na+ delivery
K+
secretion
Along the collecting duct Along the collecting duct –– potassium and sodiumpotassium and sodium
(From Ornt et al, Clin Res, 1987)
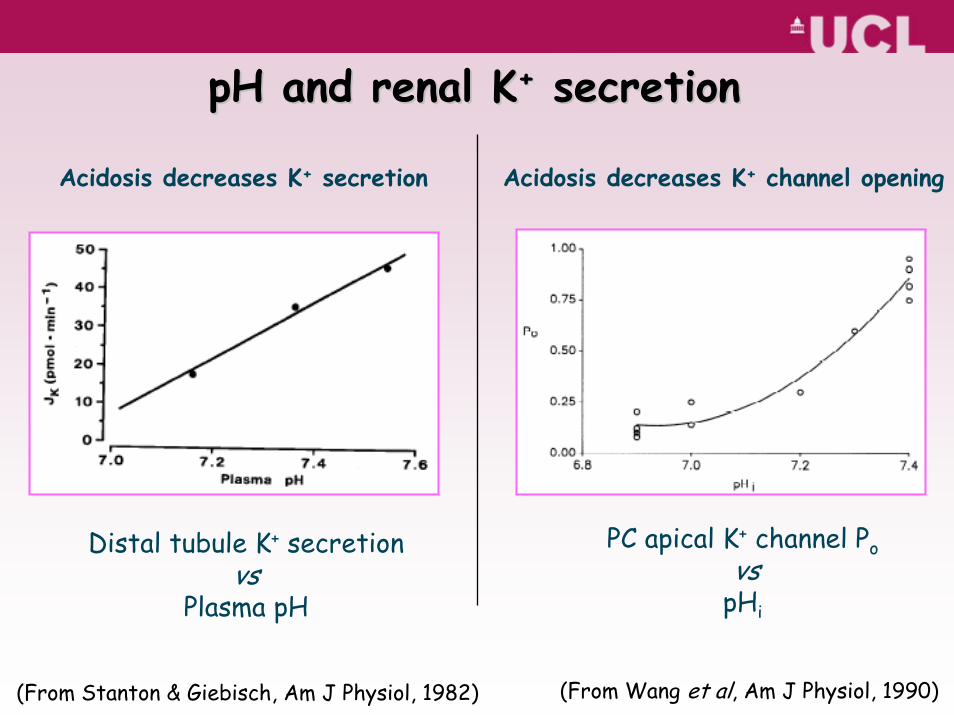
Distal tubule K+ secretionvs
Plasma pH
pH and renal KpH and renal K++ secretionsecretion
(From Stanton & Giebisch, Am J Physiol, 1982)
Acidosis decreases K+ secretion
PC apical K+ channel Povs
pHi
(From Wang et al, Am J Physiol, 1990)
Acidosis decreases K+ channel opening
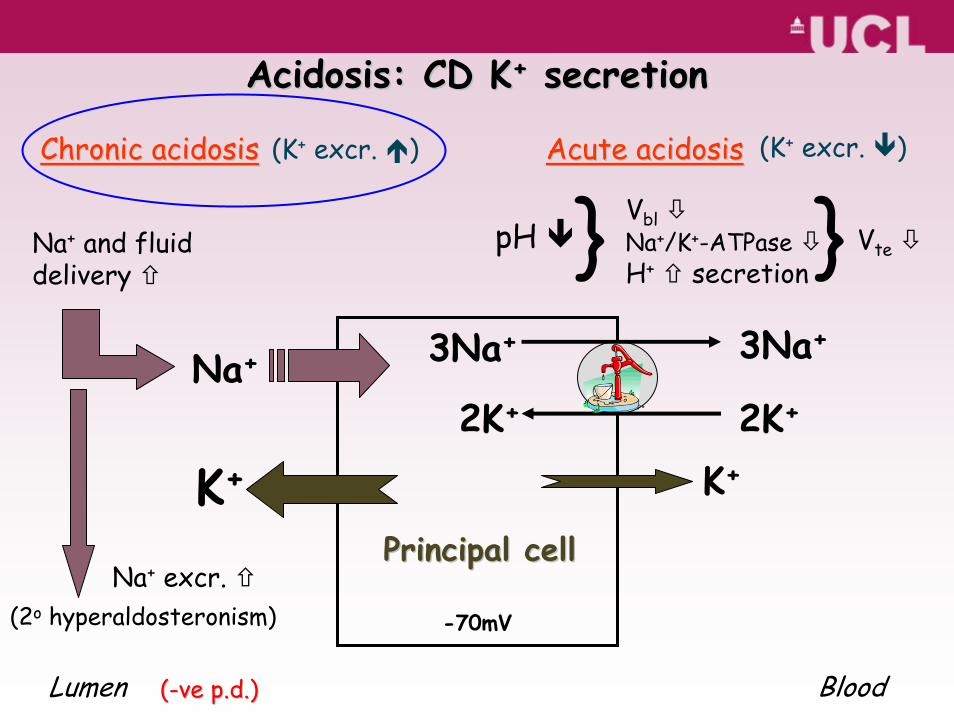
2K+
3Na+
K+
Na+
Principal cellPrincipal cell
Acidosis: CD KAcidosis: CD K++ secretionsecretion
-70mV
K+
3Na+
2K+
Lumen Blood((--veve p.d.)p.d.)
pH Vbl
VteNa+/K+-ATPaseH+ secretion} }
Acute acidosisAcute acidosis
Na+ and fluid delivery
Na+ excr. (2o hyperaldosteronism)
Chronic acidosisChronic acidosis (K+ excr. )(K+ excr. )
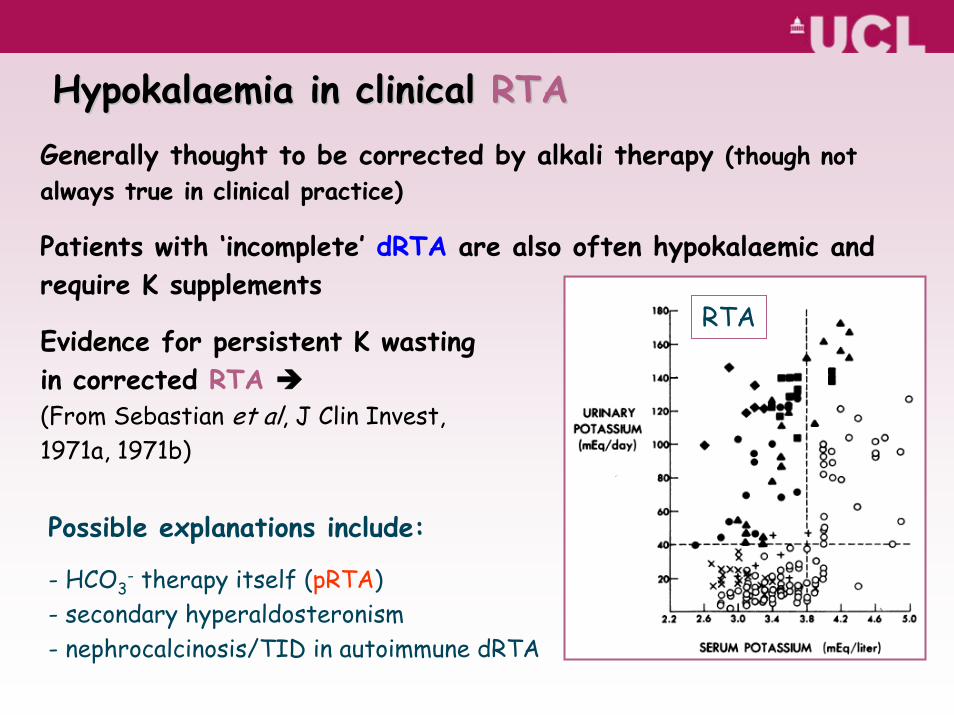
Hypokalaemia in clinical Hypokalaemia in clinical RTARTAGenerally thought to be corrected by alkali therapy (though not always true in clinical practice)
Patients with ‘incomplete’ dRTA are also often hypokalaemic and require K supplements
Evidence for persistent K wasting in corrected RTA(From Sebastian et al, J Clin Invest, 1971a, 1971b)
Possible explanations include:
- HCO3- therapy itself (pRTA)
- secondary hyperaldosteronism- nephrocalcinosis/TID in autoimmune dRTA
RTA
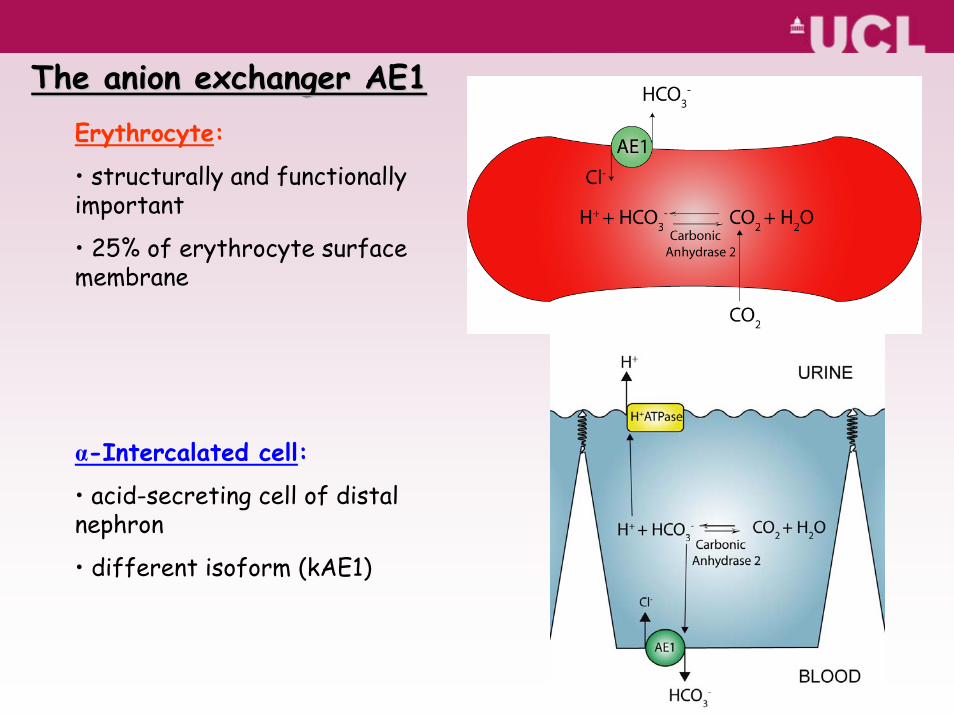
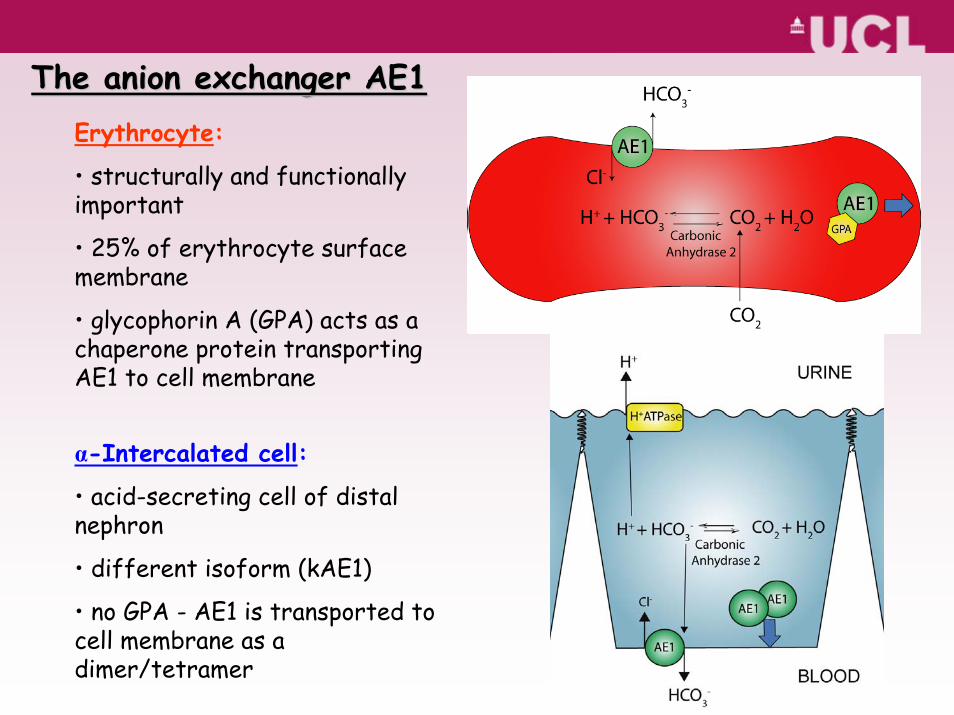
The anion exchanger AE1The anion exchanger AE1Erythrocyte:
• structurally and functionally important
• 25% of erythrocyte surface membrane
α-Intercalated cell:
• acid-secreting cell of distal nephron
• different isoform (kAE1)
Erythrocyte:
• structurally and functionally important
• 25% of erythrocyte surface membrane
• glycophorin A (GPA) acts as a chaperone protein transporting AE1 to cell membrane
α-Intercalated cell:
• acid-secreting cell of distal nephron
• different isoform (kAE1)
• no GPA - AE1 is transported to cell membrane as a dimer/tetramer
The anion exchanger AE1The anion exchanger AE1
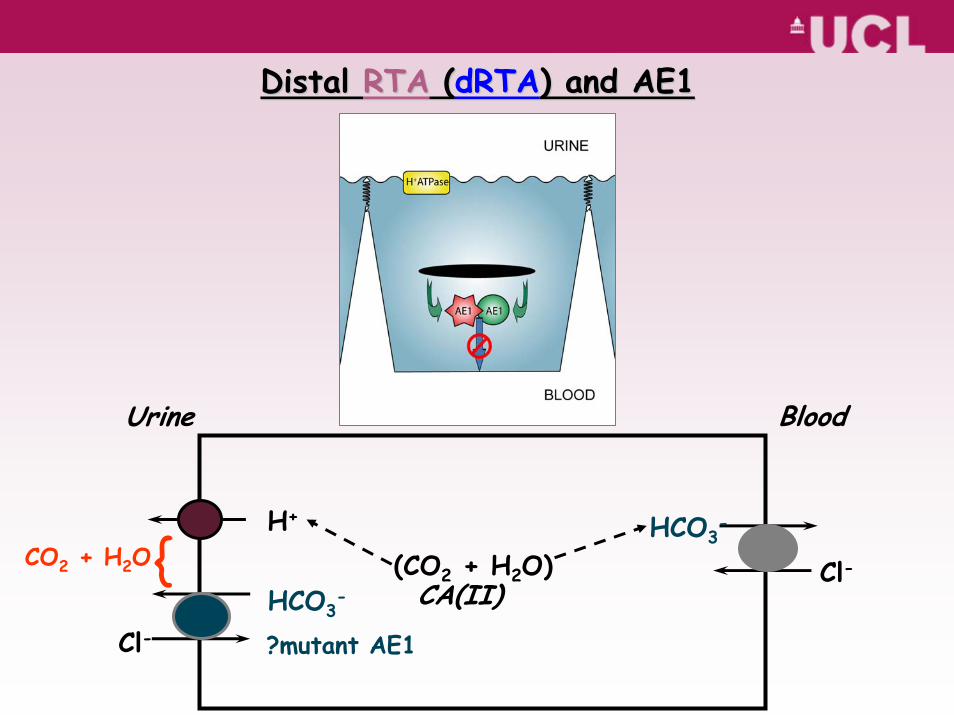
Distal Distal RTARTA ((dRTAdRTA) and AE1) and AE1
H+
Cl-
HCO3-
Cl-CA(II)
Urine Blood
(CO2 + H2O)HCO3
-
?mutant AE1
CO2 + H2O{
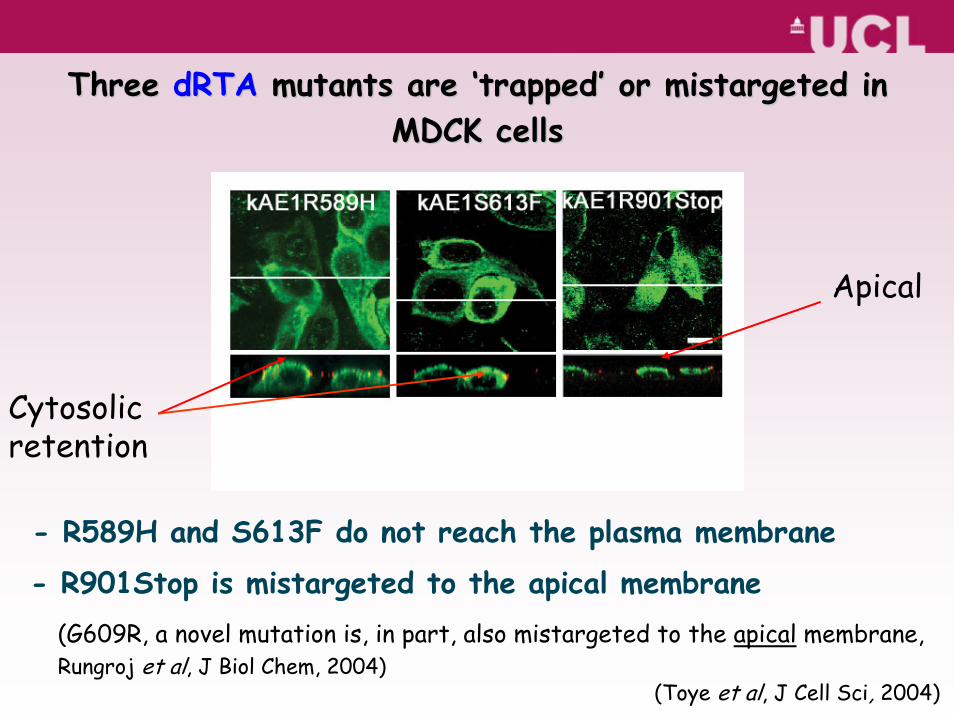
- R589H and S613F do not reach the plasma membrane
- R901Stop is mistargeted to the apical membrane
Three Three dRTAdRTA mutants are mutants are ‘‘trappedtrapped’’ or mistargeted in or mistargeted in MDCK cellsMDCK cells
(Toye et al, J Cell Sci, 2004)
Apical
(G609R, a novel mutation is, in part, also mistargeted to the apical membrane,Rungroj et al, J Biol Chem, 2004)
Cytosolicretention
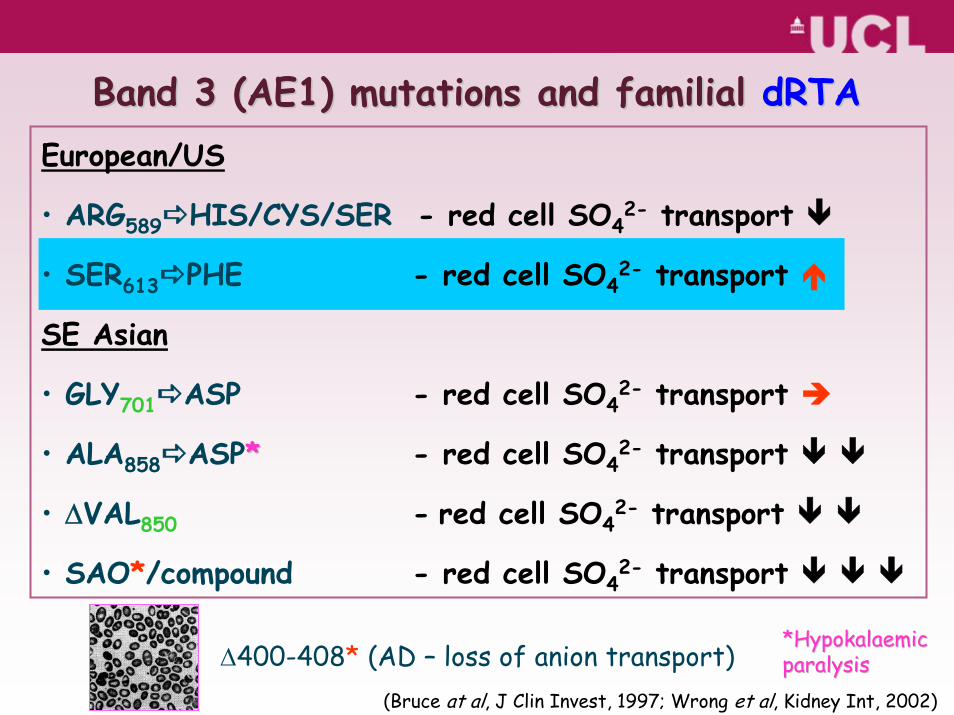
European/US
• ARG589 HIS/CYS/SER - red cell SO42- transport
• SER613 PHE - red cell SO42- transport
SE Asian
• GLY701 ASP - red cell SO42- transport
• ALA858 ASP** - red cell SO42- transport
• ΔVAL850 - red cell SO42- transport
• SAO*/compound - red cell SO42- transport
Band 3 (AE1) mutations and familial Band 3 (AE1) mutations and familial dRTAdRTA
Δ400-408* (AD – loss of anion transport) *Hypokalaemic *Hypokalaemic paralysisparalysis
(Bruce at al, J Clin Invest, 1997; Wrong et al, Kidney Int, 2002)
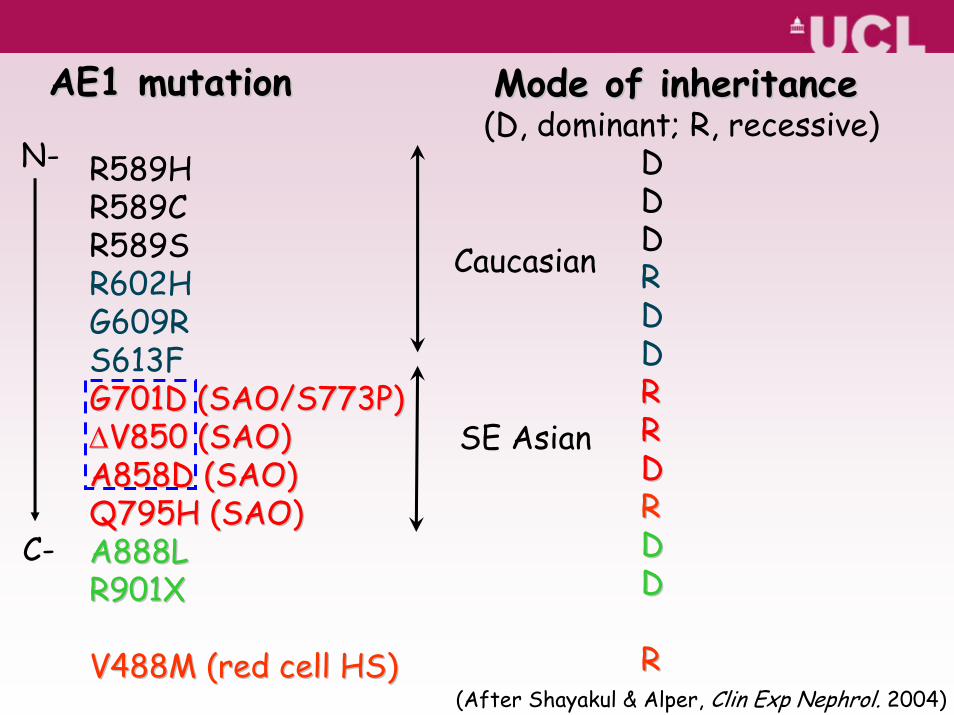
R589HR589CR589SR602HG609RS613FG701D (SAO/S773P)G701D (SAO/S773P)ΔΔV850 (SAO)V850 (SAO)A858D (SAO)A858D (SAO)Q795H (SAO)Q795H (SAO)A888LA888LR901XR901X
V488M (red cell HS)V488M (red cell HS)
DDDRDDRRRRDDRRDDDD
RR
AE1 mutationAE1 mutation Mode of inheritanceMode of inheritance
(After Shayakul & Alper, Clin Exp Nephrol. 2004)
N-
C-
(D, dominant; R, recessive)
Caucasian
SE Asian
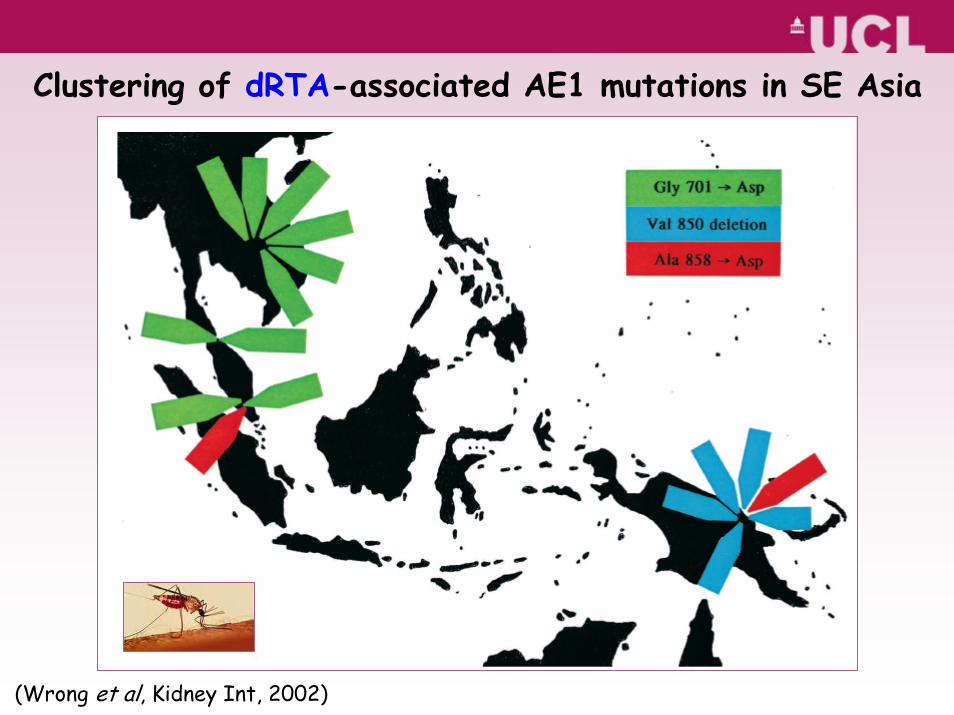
Clustering of dRTA-associated AE1 mutations in SE Asia
(Wrong et al, Kidney Int, 2002)
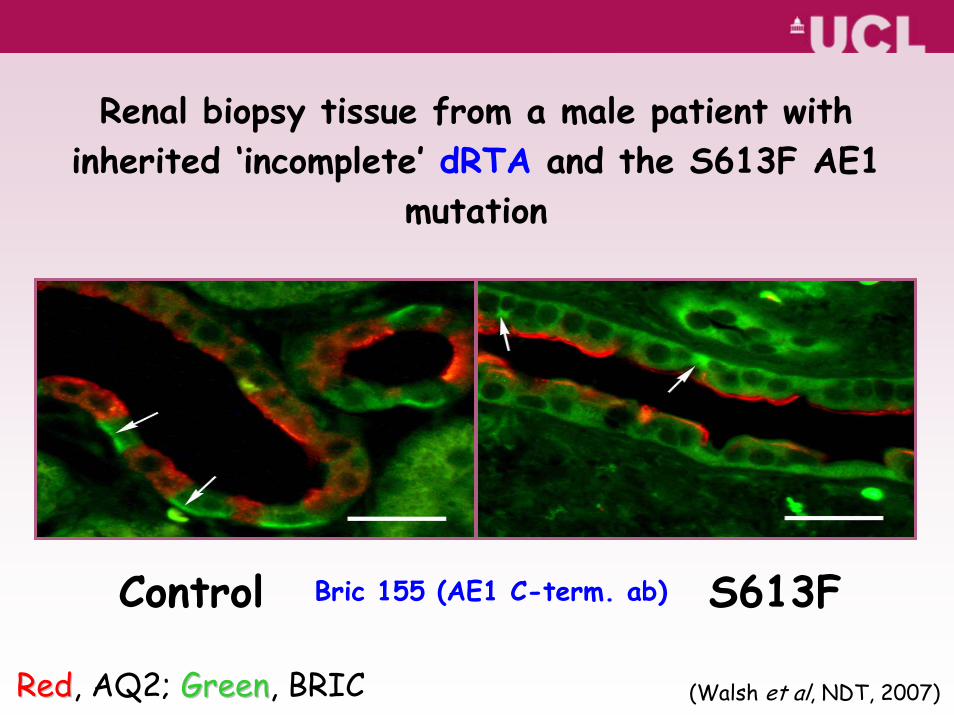
Bric 155 (AE1 C-term. ab)Control S613F
Renal biopsy tissue from a male patient with inherited ‘incomplete’ dRTA and the S613F AE1
mutation
RedRed, AQ2; GreenGreen, BRIC (Walsh et al, NDT, 2007)
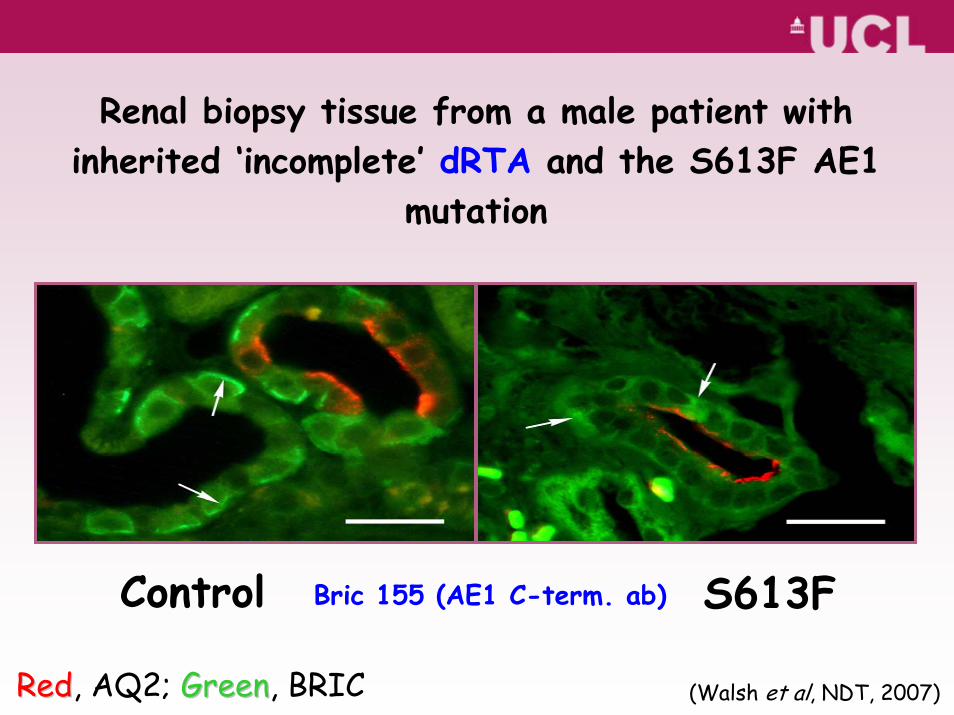
RedRed, AQ2; GreenGreen, BRIC
Control S613FBric 155 (AE1 C-term. ab)
Renal biopsy tissue from a male patient with inherited ‘incomplete’ dRTA and the S613F AE1
mutation
(Walsh et al, NDT, 2007)
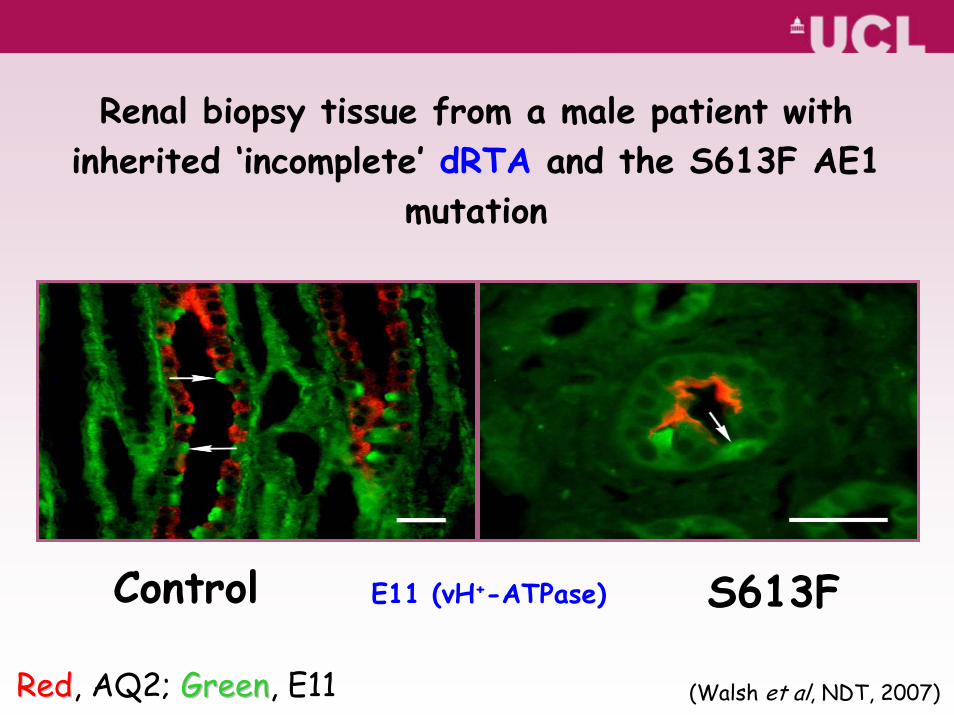
E11 (vH+-ATPase)
RedRed, AQ2; GreenGreen, E11
Control S613F
Renal biopsy tissue from a male patient with inherited ‘incomplete’ dRTA and the S613F AE1
mutation
(Walsh et al, NDT, 2007)
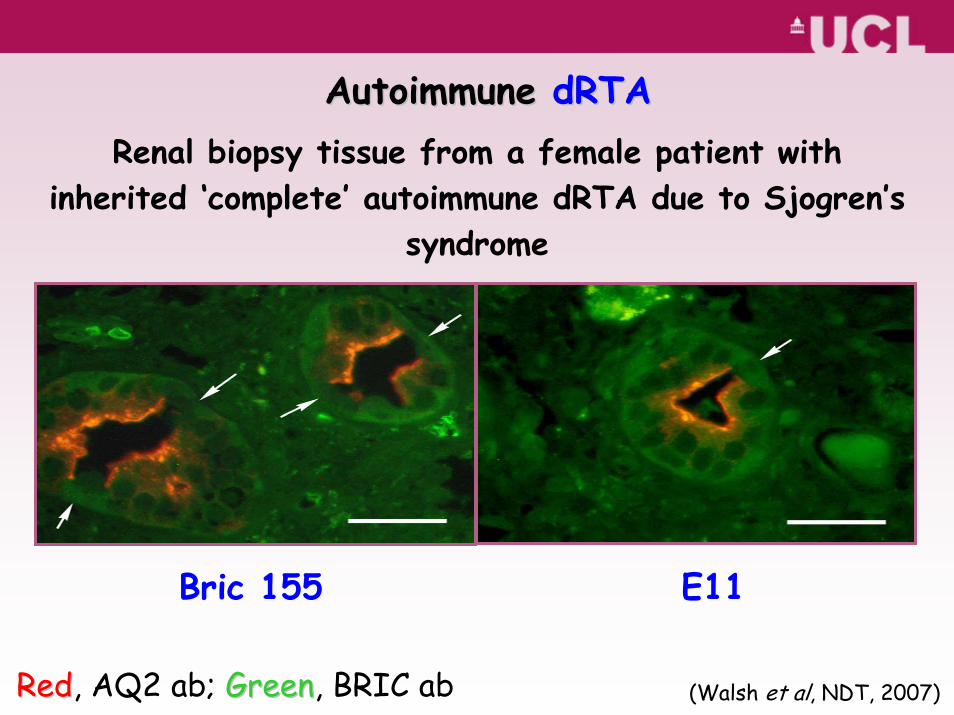
Bric 155
Autoimmune Autoimmune dRTAdRTARenal biopsy tissue from a female patient with
inherited ‘complete’ autoimmune dRTA due to Sjogren’s syndrome
RedRed, AQ2 ab; GreenGreen, BRIC ab
E11
(Walsh et al, NDT, 2007)
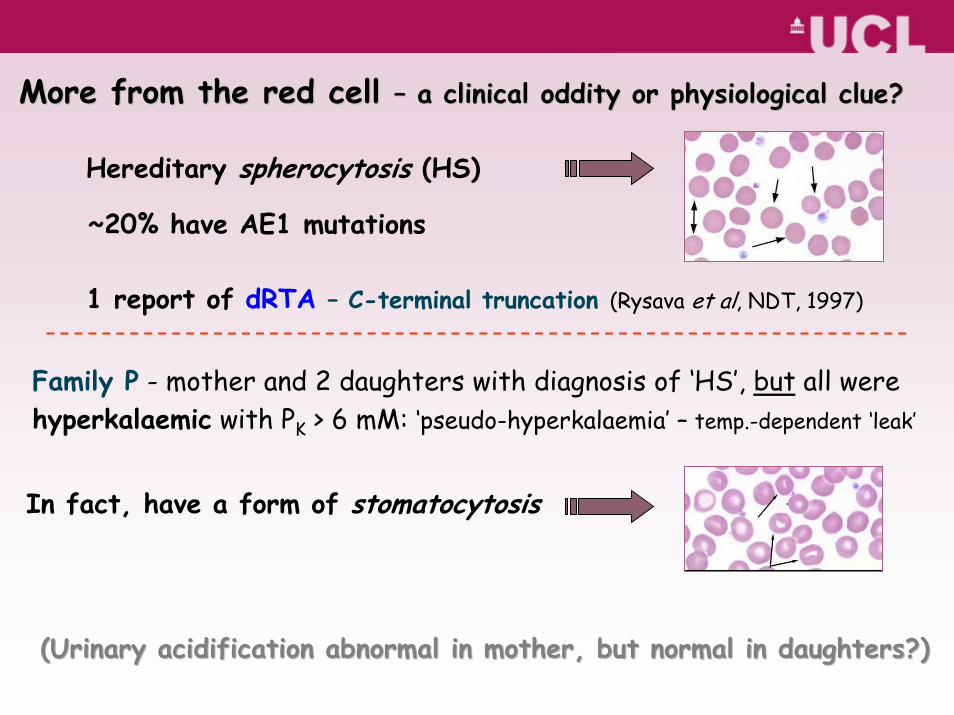
More from the red cell More from the red cell –– a clinical oddity or physiological clue?a clinical oddity or physiological clue?
Hereditary spherocytosis (HS)
~20% have AE1 mutations
1 report of dRTA – C-terminal truncation (Rysava et al, NDT, 1997)
(Urinary acidification abnormal in mother, but normal in daughte(Urinary acidification abnormal in mother, but normal in daughters?)rs?)
Family P - mother and 2 daughters with diagnosis of ‘HS’, but all were hyperkalaemic with PK > 6 mM: ‘pseudo-hyperkalaemia’ – temp.-dependent ‘leak’
In fact, have a form of stomatocytosis
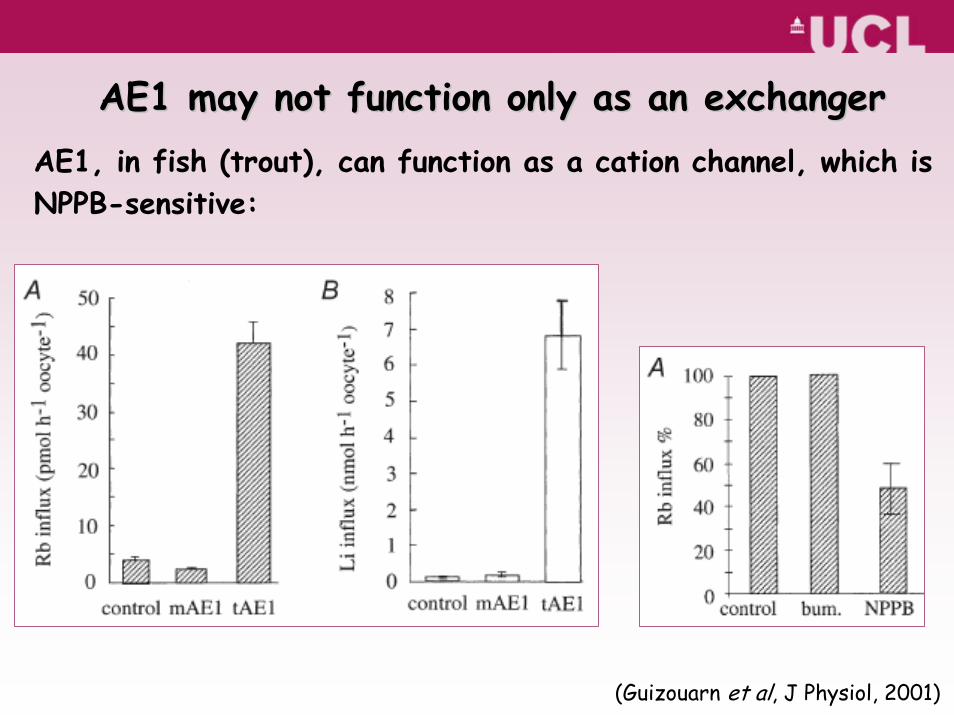
AE1 may not function only as an exchangerAE1 may not function only as an exchangerAE1, in fish (trout), can function as a cation channel, which isNPPB-sensitive:
(Guizouarn et al, J Physiol, 2001)
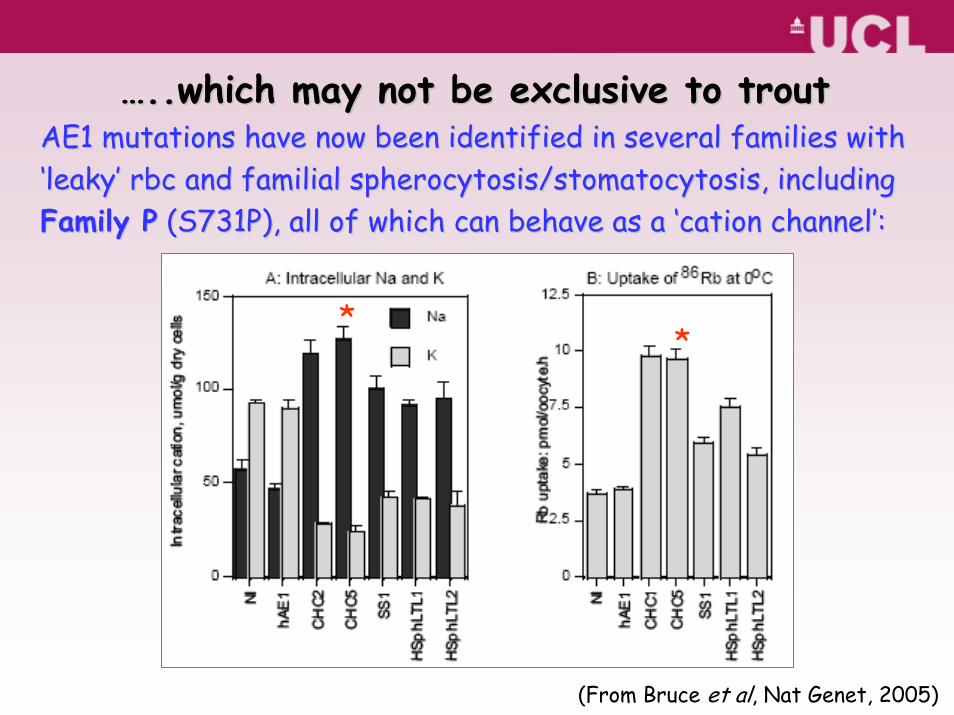
AE1 mutations have now been identified in several families with AE1 mutations have now been identified in several families with ‘‘leakyleaky’’ rbcrbc and familial and familial spherocytosis/stomatocytosisspherocytosis/stomatocytosis, including , including Family PFamily P (S731P), all of which can behave as a (S731P), all of which can behave as a ‘‘cationcation channelchannel’’::
(From Bruce et al, Nat Genet, 2005)
**
……..which may not be exclusive to trout..which may not be exclusive to trout
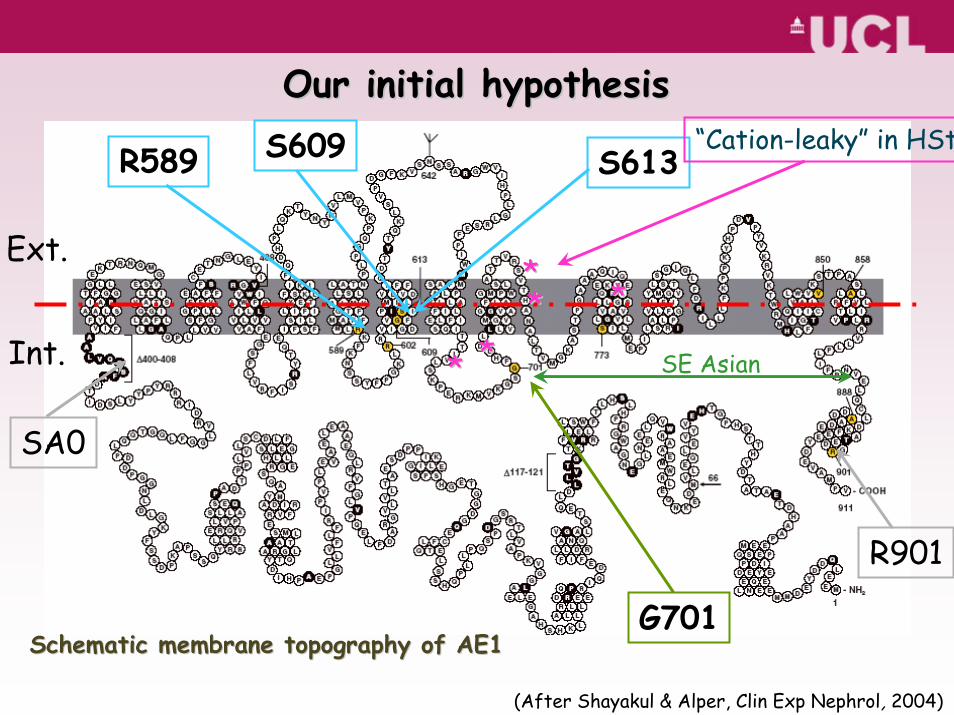
Schematic membrane topography of AE1Schematic membrane topography of AE1
Ext.
Int.
(After Shayakul & Alper, Clin Exp Nephrol, 2004)
S613
SA0
R589
R901
** ****
****
“Cation-leaky” in HSt
SE Asian
Our initial hypothesisOur initial hypothesis
G701
S609
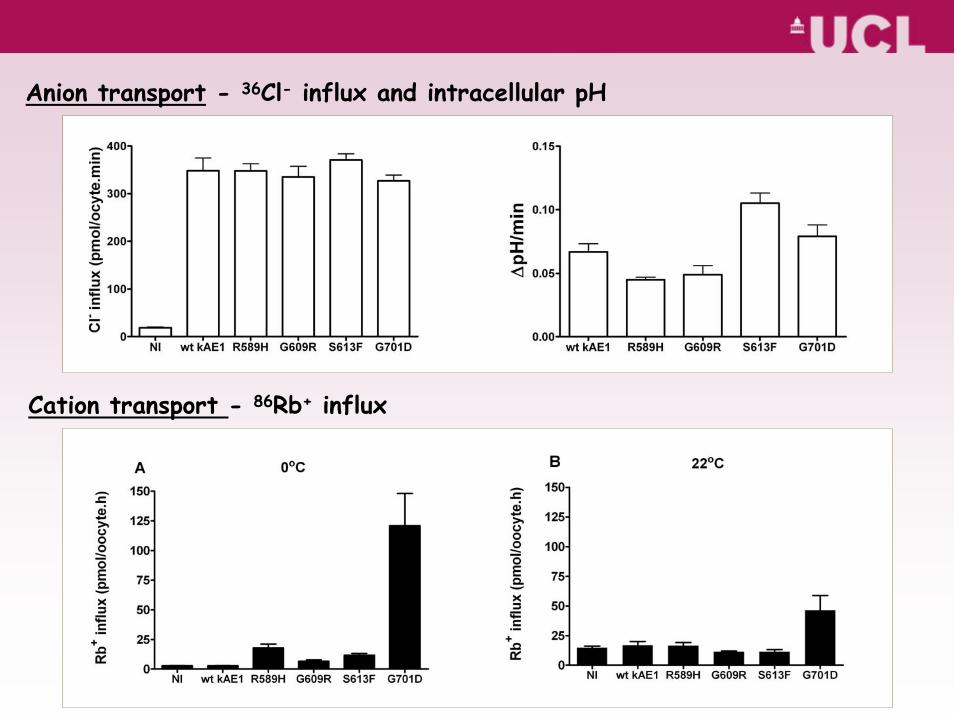
Anion transport - 36Cl- influx and intracellular pH
Cation transport - 86Rb+ influx
(Unpublished observations)
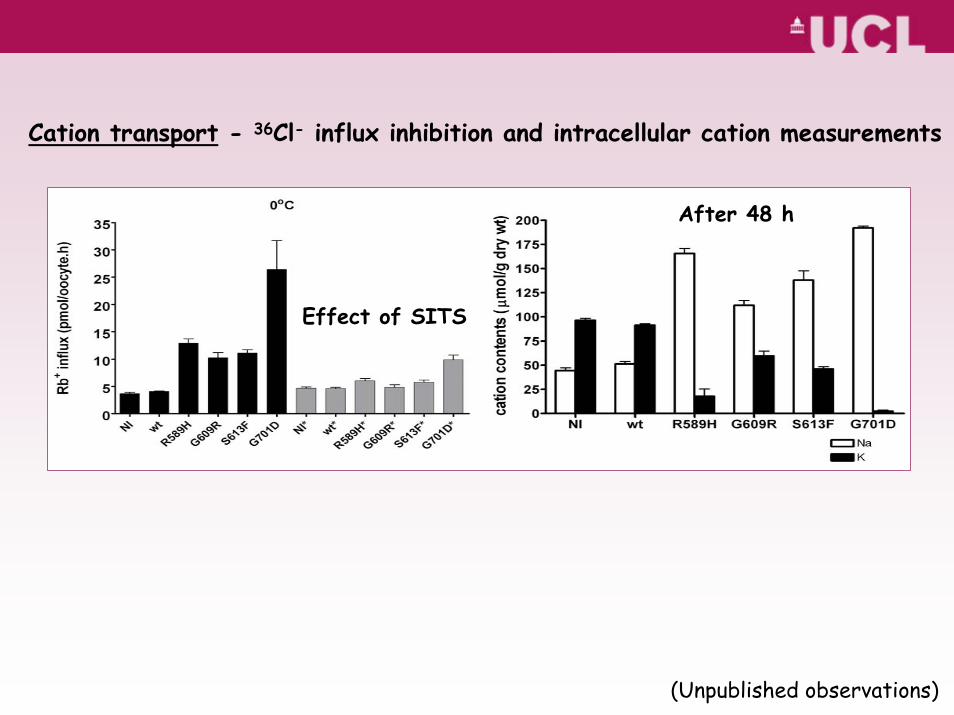
Cation transport - 36Cl- influx inhibition and intracellular cation measurements
After 48 h
Effect of SITS
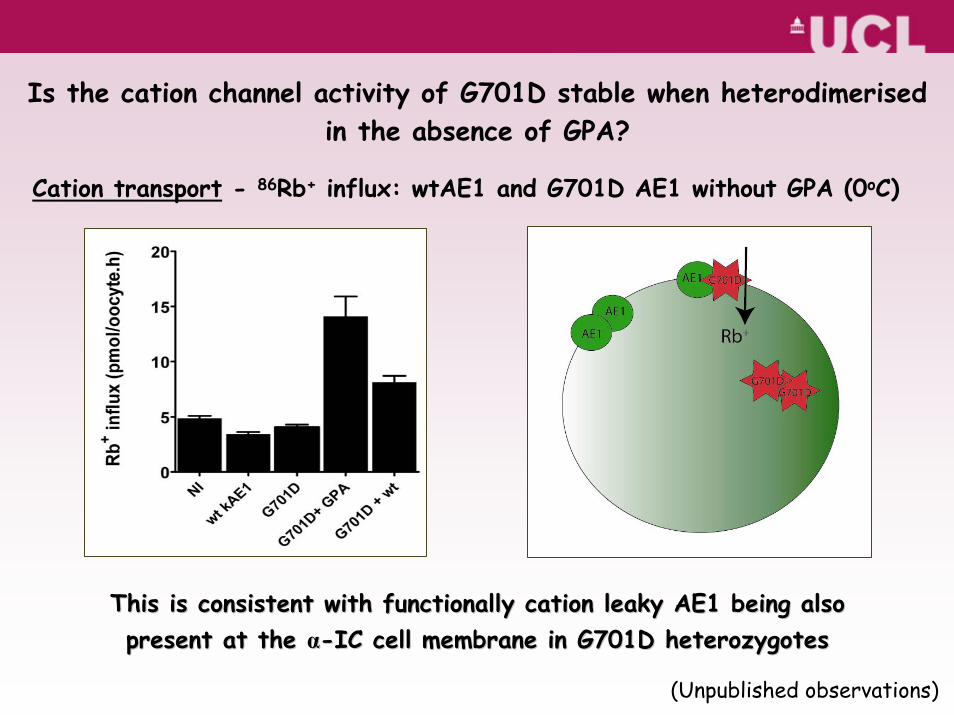
Is the cation channel activity of G701D stable when heterodimerisedin the absence of GPA?
Cation transport - 86Rb+ influx: wtAE1 and G701D AE1 without GPA (0oC)
This is consistent with functionally cation leaky AE1 being alsoThis is consistent with functionally cation leaky AE1 being alsopresent at the present at the αα--IC cell membrane in G701D IC cell membrane in G701D heterozygotesheterozygotes
(Unpublished observations)
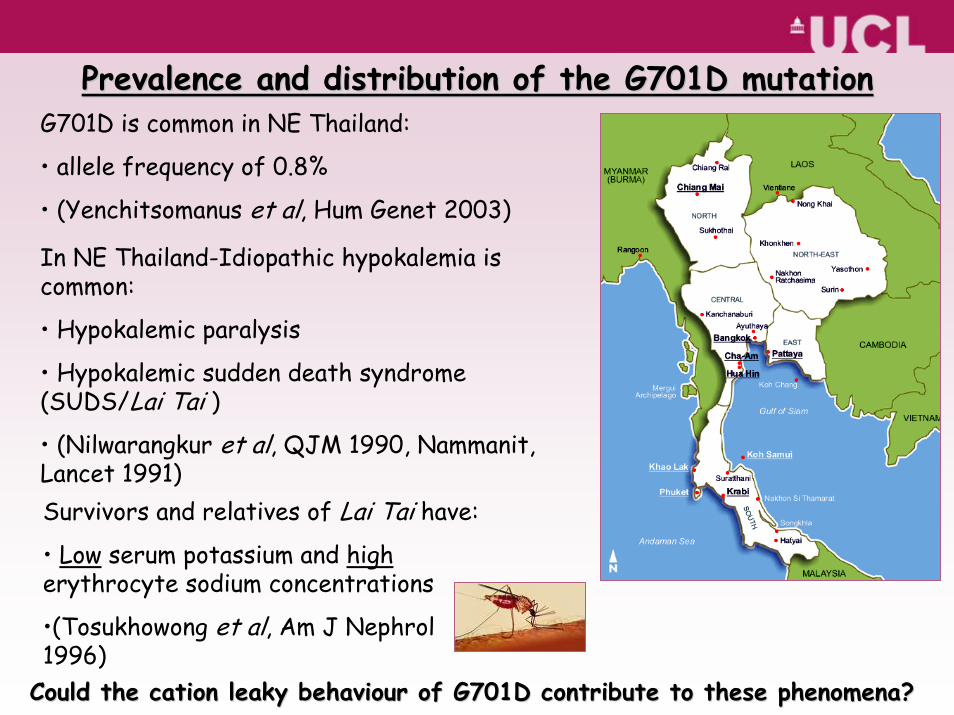
Prevalence and distribution of the G701D mutationPrevalence and distribution of the G701D mutationG701D is common in NE Thailand:
• allele frequency of 0.8%
• (Yenchitsomanus et al, Hum Genet 2003)
In NE Thailand-Idiopathic hypokalemia is common:
• Hypokalemic paralysis
• Hypokalemic sudden death syndrome (SUDS/Lai Tai )
• (Nilwarangkur et al, QJM 1990, Nammanit, Lancet 1991)Survivors and relatives of Lai Tai have:
• Low serum potassium and higherythrocyte sodium concentrations
•(Tosukhowong et al, Am J Nephrol1996)
Could the cation leaky behaviour of G701D contribute to these phCould the cation leaky behaviour of G701D contribute to these phenomena?enomena?
“A merry Christmas to everybody! A happy New Year to all the world!”
“An idea, like a ghost, must be spoken to a little before it will explain itself.”
(Charles Dickens, 1812-1870)