university of maryland upper chesapeake...
TRANSCRIPT

#606814v4 011888-0023
UNIVERSITY OF MARYLAND UPPER CHESAPEAKE MEDICAL CENTER Certificate of Need Application
Special Psychiatric Hospital Matter No. 17-12-2403
Responses to Additional Information Questions Dated October 4, 2017
PART I – PROJECT IDENTIFICATION AND GENERAL INFORMATION
1. Please provide the following additional information and clarifications of the comprehensive project description:
a) Project cost: it is listed as $56,265,809 (Table E, Project Budget), but stated as $52,421,120 in the Executive Summary (p.5). Clarify.
Applicant Response
The project budget of $56,265,809 as listed on Table E is accurate. The last sentence of the Project Description on page 5 of UM Upper Chesapeake Health’s Certificate of Need Application to develop a special psychiatric hospital (“UM UCH’s CON Application”) should be amended to state: “The total projected cost of the special psychiatric hospital is $56,265,809.”
b) Space: There are many contradictions at various places in the application materials. Table B shows the project to encompass 66,840 SF, while the project description says 67,632.
Applicant Response
Enclosed as a replacement for Exhibit 2 are revised project drawings for UC Behavioral Health and UC FMF. The amended project drawings are now consistent with Table B submitted with Exhibit 1 to UM UCH’s CON Application to develop a special psychiatric hospital and Table B and Exhibit 1 to UM Upper Chesapeake Medical Center’s and UM Harford Memorial Hospital’s joint Request for Exemption from Certificate of Need Review for the Conversion of University of Maryland Harford Memorial Hospital to a Freestanding Medical Facility. Table 21 below reflects the square footage of both UC Behavioral Health and UC FMF, with shared space allocated 52% to UC Behavioral Health and 48% to UC FMF. Table 21 corrects the Applicants’ square footage descriptions on pages 4 and 8 and footnote 1 of UM UCH’s CON Application.

#606814 2 011888-0023
Table 21 Department Gross Square Footage UC FMF and UC Behavioral Health
UC BehavioralHealth
UC FMF Total
Total Floor Plate Square Footage 78,763(ground floor)
50,800(first floor)
129,563
Dedicated Departmental SquareFootage
53,922 49,857 103,779
Shared Space Allocation 12,918 12,866 25,784Shared Space Allocation % 52% 48% 100%Total Gross Departmental SquareFeet consistent with Table B
66,840 62,723 129,563
c) Space: Footnote 1 on p.4 describes the ground floor of the structure to include 55,524 SF for psych and 23,285 shared/allocated SF part of the ground floor for a total of 78,809 SF; yet the drawings submitted with the application allocate 53,996 SF to the psych hospital and 24,767 SF as shared space (totaling 78,763, not 78,809) and 47,036 SF to the FMF. These SF allotments total 125,845; this is not consistent with the description of the physical plant and design on the bottom of p.8, which shows a total SF of 129,609. Please provide definitive SF totals for each function.
Applicant Response
See Applicant’s response to Question 1(b) above.
d) The application variously describes replacing HMH’s 29 (p. 5) and 26 (p.37) psychiatric beds. Which is it?
Applicant Response
In the fiscal year from July 1, 2017 to June 30, 2018, HMH is licensed for twenty-nine (29) acute adult psychiatric beds and fifty-seven (57) MSGA beds. See Exhibit 12.
2. Is the Regional Collaborative for Behavioral Health formalized into a corporation or business unit? If so, who are the owners?
Applicant Response
The activities of the Regional Collaborative for Behavioral Health (“Regional Collaborative”) described on pages 7-8 of UM UCH’s CON Application were undertaken through an informal arrangement between UM UCH and Union Hospital of Cecil County (“Union Hospital”) to coordinate and facilitate access to services for individuals in need of behavioral health services. The efforts and activities of the Regional Collaborative are governed by a memorandum of understanding. The Regional Collaborative board does meet quarterly and behavior health program clinical coordination takes place on an ongoing basis between UM
#606814 3 011888-0023
UCH, Union Hospital, and community partner, Upper Bay Counseling and Support Services, Inc. The Regional Collaborative has an active board which is anticipating expanding participation to additional community partners.
UM UCH and Union Hospital did form a legal joint venture named Behavioral Health Management Services, LLC on January 5, 2015. This entity was to be governed by a board of not more than six managers, with three (3) managers designated by Upper Chesapeake Health Ventures, Inc., and three (3) managers designated by Union Hospital of Cecil County Ventures, LLC. The purpose of the Behavioral Health Management Services, LLC was to facilitate and provide better integration of behavioral health services in Harford, Cecil, and Baltimore Counties and to engage in any other lawful business permitted by the Maryland Limited Liability Act. Behavioral Health Management Services, LLC’s corporate identity was forfeited on October 11, 2016. The activities of the Regional Collaborative for Behavioral Health as identified on pages 7-8 of the CON Application have been performed through the informal arrangement described above rather than through the joint venture LLC.
3. The application states that the “proposed project/program square footage per bed falls well within the expected and customary range for such facilities.” Back up this statement with data and comparisons with similar facilities.
Applicant Response
Consistent with the Applicant’s response to Question 1(a) above, Table 21, and Table B submitted with UM UCH’s CON Application, the statement on page 10 of UM UCH’s CON Application should be corrected to state: “With forty (40) inpatient beds, the proposed project is: (1) 1,671 gross square feet per inpatient bed, including the outpatient behavioral health therapy program and the facility support space; and (2) 1,298 gross square feet per inpatient bed, including the facility support space, but not including the outpatient behavioral health therapy program.”
In the most recently approved CON application to establish a special psychiatric hospital, In re Sheppard Pratt at Elkridge, Docket No. 15-152367, the Commission approved an 85-bed facility that was 155,707 gross square feet, equaling 1,832 gross square feet per inpatient bed. See Staff Report and Recommendation at 1, 17 (Sept. 20, 2016). UC Behavioral Health is well within the square foot per bed range approved by the Commission for the relocation of Sheppard Pratt at Elkridge.
4. The statement is made that the outpatient facilities incorporated into this project “will also afford greater and easier access to the appropriate level of care for behavioral health patients across the region” (p. 10). That is likely not the case for the patients who would otherwise be hospitalized at Union based on where they live. Please describe how they will be served.
Applicant Response
UC Behavioral Health is centrally located in its projected service area as reflected by the map on page 37 of the CON Application. Planned outpatient behavioral health services at both UC Behavioral Health and Union Hospital will provide greater options, flexibility, and a continuum of care for patients than is currently available in Harford and Cecil Counties.

#606814 4 011888-0023
UC Behavioral Health will offer a broader continuum-of-care that will include a Partial Hospitalization Program (“PHP”) and a larger Intensive Outpatient Program (“IOP”) than presently exists at either HMH or Union. These additional and expanded outpatient services at UC Behavioral Health will provide easier access to many Union County residents who currently live closer to UC Behavioral Health but currently travel to Union in Elkton for inpatient behavioral health services.
In addition, for those service area residents closer to Union, a full continuum of outpatient care is envisioned at Union’s campus, including Behavioral Health Crisis Services and a PHP program. These expanded behavioral health outpatient services at Union will offer an alternative to inpatient admission for certain patients experiencing behavioral health needs and allow patients to continue to receive outpatient behavioral health services close to home following an inpatient admission at UC Behavioral Health.
PART II – PROJECT BUDGET
5. We assume that cost of special hospital (including the allocation for shared space) is reported in Table E. Please revise the table to show: the cost of FMF in the “other structure” column; the combined cost of the psychiatric special hospital and FMF in the “total” column. Describe the method of allocating the cost of the shared space attributed to each of the special hospital and FMF.
Applicant Response
A new Table E submitted herewith as Exhibit 13 shows the cost of the FMF in the “other structure” column and the combined costs of the psychiatric special hospital and the FMF in the “total” column. As set forth in footnote 1 of UM UCH’s CON Application, shared space and associated costs of construction was allocated 52% to UC Behavioral Health and 48% to UC FMF. This represents a pro-rata allocation based on the overall size of each facility in relation to the total Dedicated Departmental Square Footage of each facility. See also Table 21 above.
6. Describe the services represented by the “other” lines in 2.c2 (CON assistance) and 2d2 (non-CON consulting fees) on the Project Budget (Table B).
Applicant Response
On Table E, Line 2.c2 totaling $143,000 includes fees for UM UCH’s consultants, KPMG, LLP and Andrew Solberg, in support of filing the Exemption Application with the Maryland Health Care Commission. Line 2.d2 totaling $492,000 includes support from several vendors with pre-application tasks such as design, planning, and assessing the financial impact of this project for UM UCH. Vendors include BRG and KPMG, LLP for strategic planning, Morris Richie for architecture and engineering support, and Gallagher, Evelius & Jones, LLP for pre-application assistance.
7. If the applicant issues bonds to finance the project, please explain why $276,967 is set aside for Loan Placement Fees?

#606814 5 011888-0023
Applicant Response
The “Loan Placement Fees” as reflected on Table E are synonymous with “Costs of Bond Issuance.” The projected cost of bond issuance approximates 0.5% of the bonds and represents fees either paid by the borrower and reimbursed through financing or paid at the closing of the bond financing. These costs typically include, without limitation, attorney/counsel fees (underwriter’s counsel, bond and tax counsel, borrower’s counsel), auditor fees associated with completing the agreed upon procedures letter, rating agency fees associated with rating the bonds, the bond issuer’s application fee, production costs of the official statement and fees of the financial advisors for the borrower and the bond issuer.
APPLICATION TABLE PACKAGE
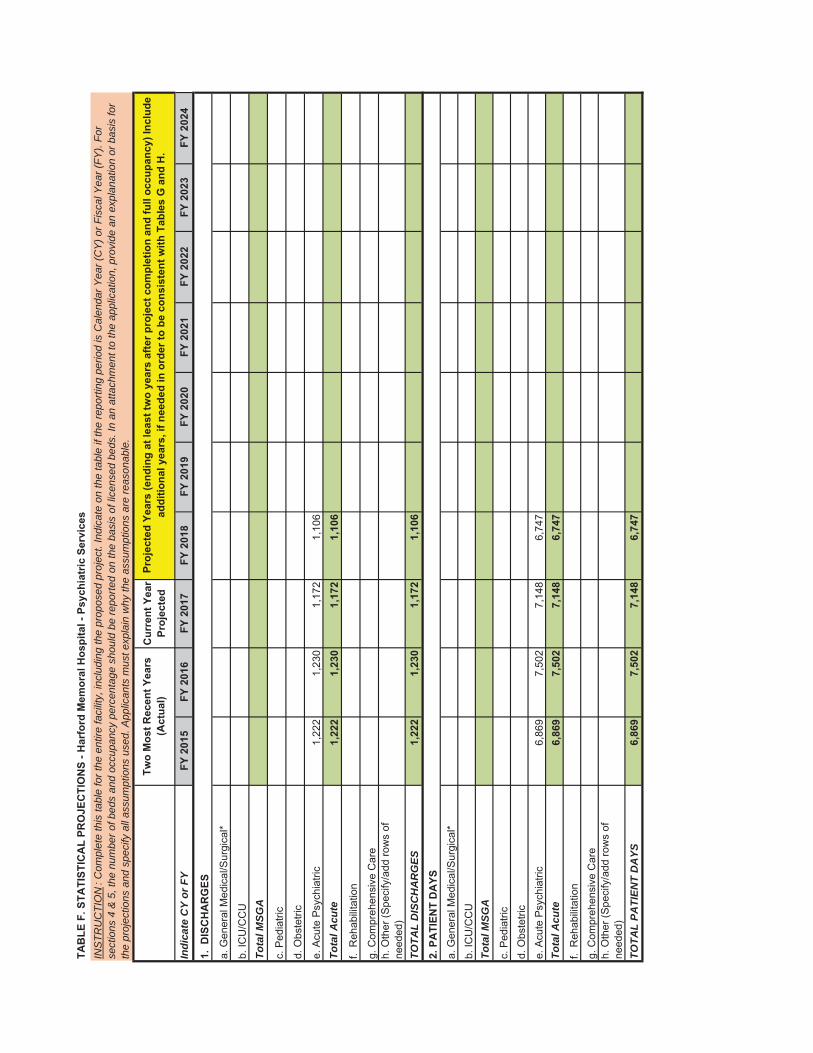
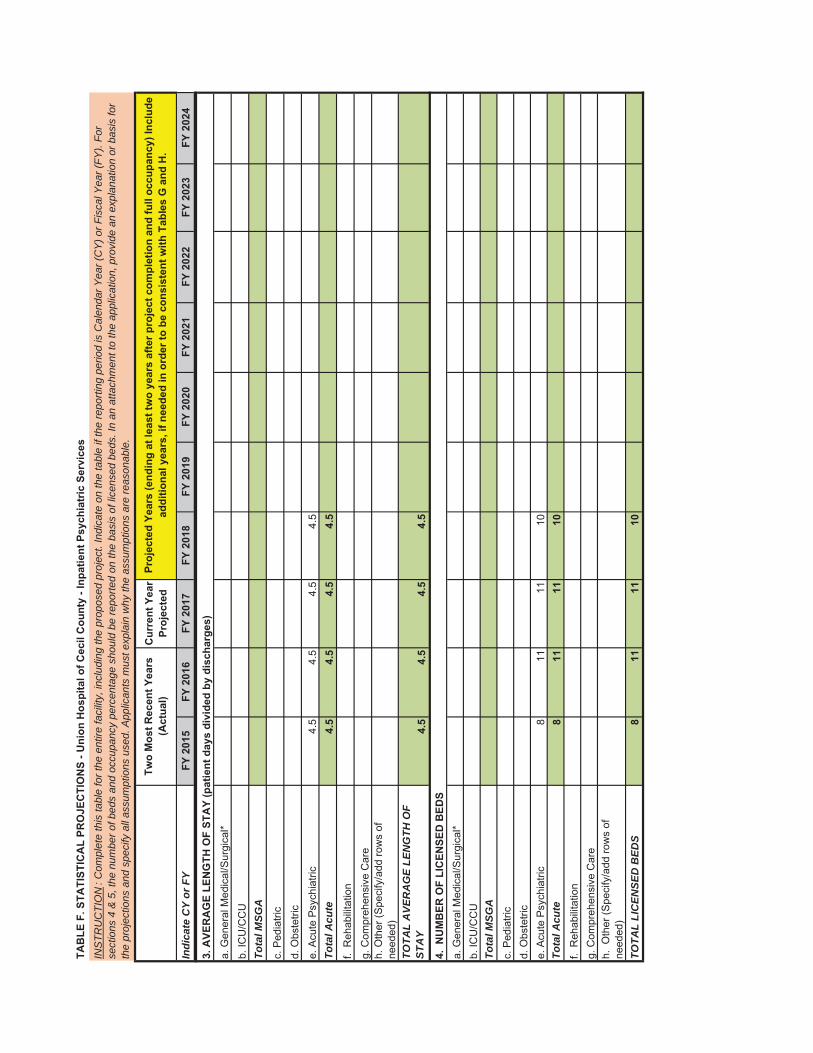
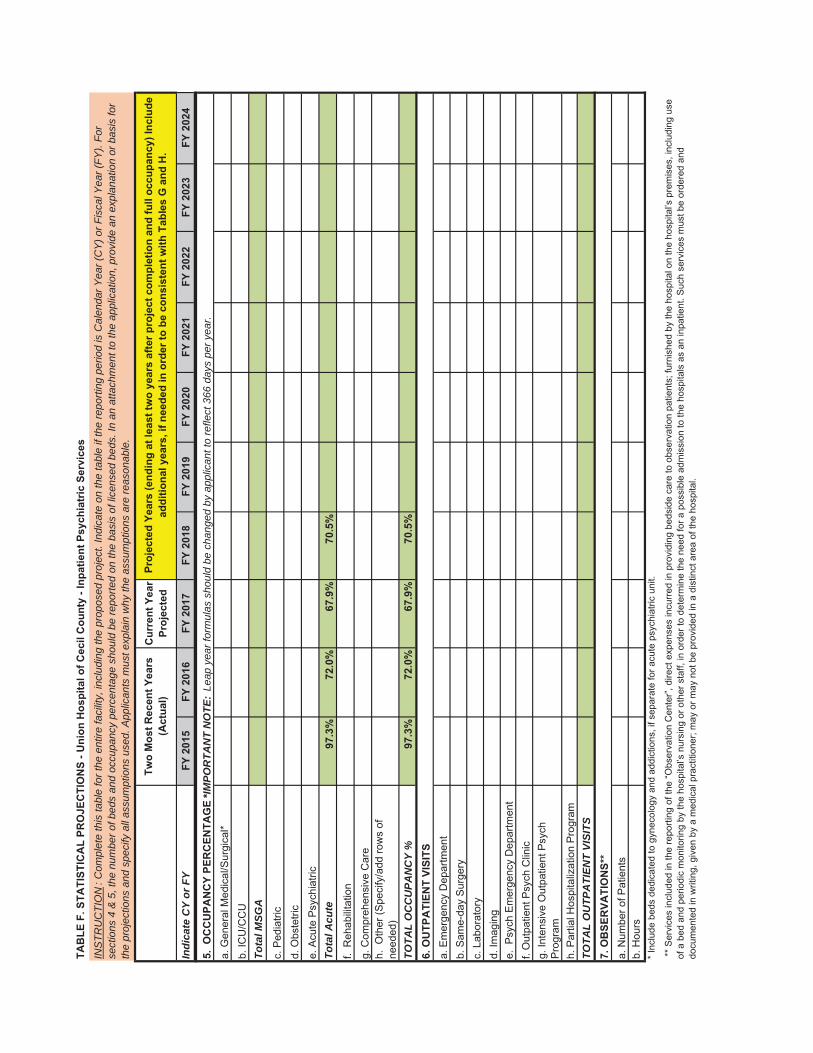
8. Please provide the historical (FY 15-17) and current (FY18 projected) sections of the utilization tables – separately and combined – for HMH and Union Memorial psychiatric services. This is essentially a Table F for each, and a Table F combined. This history is necessary to assess future projections.
Applicant Response
Submitted as Exhibit 14 are sections of utilization tables, separately and combined, for HMH and Union Hospital psychiatric services for fiscal years 2015 through 2017 and projections for fiscal year 2018.
9. Table L is not completed properly, perhaps because it asks for data from the “current entire facility,” which of course is not in existence. In order to customize the table to match its purpose, please:
complete the “current facility” portion for the 29 bed behavioral health unit at HMH;
complete the rest of the table to show the changes that will occur with the project.
Note that the “total cost” column should reflect the total cost of employing those in each category. It is not clear what value you placed in the CON filing (hourly rate?).
Applicant Response
Presented in Exhibit 15 is Table L with full time equivalents (“FTEs”) and related salary costs for the direct and allocated staff that support the provision of behavioral health services at HMH in fiscal year 2017. Because the projected FTEs and salary costs in fiscal year 2024 reflect direct and allocated staff that support both inpatient and outpatient behavioral health services at UC Behavioral, the fiscal year 2017 FTEs and salary costs reflect direct and allocated staff that support both inpatient and outpatient behavioral health services at HMH, not just the 29 bed behavioral health unit. The changes between fiscal years 2017 and 2018 reflect a reduction in Administration and Support FTEs, offset partially by an increase in Direct Care FTEs.

#606814 6 011888-0023
PART IV - CONSISTENCY WITH GENERAL REVIEW CRITERIA
The State Health Plan -Psychiatric Services Standards
10. Concerning Standard AP 4b: please describe the clinical/programmatic distinctions that will exist between the adult and geriatric units.
Applicant Response
On the geriatric unit, individual and group interventions will be tailored to focus on the phase of life issues which arise in the generally older population and adjusted to accommodate the cognitive impairment common in this group. There will be a larger general medical consultation, physical therapy, and occupational therapy presence. Though family involvement will be a focus on all units, the geriatric population will require a more consistent, structured approach.
11. With regard to Standard AP 11:
a) What is the source of case and charge data in Table 3?
Applicant Response
The source of case and charge data in Table 3 of UM UCH’s CON Application is 2016 HSCRC abstract data (final).
b) How was the age adjustment done?
Applicant Response
Age adjustment was done by calculating the health planning region’s charge per case at a case mix index (“CMI”) of 1.0 within the pre-determined age groups (see Table 3) and then multiplying these numbers by UC Behavioral Health’s projected case volume. By doing so, UC Behavioral Health reached a total revenue number that could be compared to UC Behavioral Health.
c) Describe and show how the calculations of charge/case for the planning region and for UCBH are arrived at.
Applicant Response
The charge/case for the planning region was calculated by dividing the $18,617,697 reflected in the far right column of Table 3 by UC Behavioral Health’s 1,568 projected cases. See Table 22 below for calculation of UC Behavioral Health charge/case.

#606814 7 011888-0023
Table 22 UC Behavioral Health Projected Charge Per Case Price Leveled to FY 2016 Prices
12. Standard AP 13: as the standard requires, provide a copy of the written policies governing discharge planning and referrals between the program and a full range of other services.
Applicant Response
A copy of UM Upper Chesapeake Health’s polices relating to Interdisciplinary Discharge Planning for Behavioral Health and Patient Transfers are submitted herewith as Exhibits 16 and 17, respectively.
13. Standard AP 13: as required by the standard, please provide a letter of acknowledgement from the Maryland Department of Health and Mental Hygiene.
Applicant Response
UM UCH has requested a letter of acknowledgement from the Maryland Department of Health and understands that the Acting Secretary will provide a letter of acknowledgment directly to the staff of the Maryland Health Care Commission.
Need
14. Table 4 on p. 35 appears to be a duplicate of Table 3 on p.32, yet it is referenced on p. 39 related to population projections; please explain or correct the reference.
Applicant Response
The reference to “Table 4” on page 39 of the CON Application is incorrect. The sentence should state: “Using the compound annual growth rate from 2016 to 2021, as set forth in Table 6, population projections were extrapolated through 2024 and applied to UM Behavioral Health’s fiscal years.”
Total Estimated Service Area Psych Discharges at UCBH in FY 2016 1,671 Total Estimated Service Area Psych Discharges at UCBH in FY 2022 1,346
% Decline in Discharges -19.4%
Projected FY 2022 Inpatient Revenue at UCBH $25,955,056Deflation Factor -14.2%
Projected FY 2016 Inpatient Revenue at UCBH $22,278,277
% Decline in Discharges Projected for -19.4%
Projected FY 2016 Inpatient Revenue at UCBH with Volume Decline $17,945,278
Projected Cases 1,568
Projected FY 2016 Charge per Case $11,445

#606814 8 011888-0023
15. Please explain the methodology and assumptions of the extrapolation of the population estimates described on p. 39.
Applicant Response
Historical and projected population estimates were obtained from Nielsen Claritas for years 2010, 2016, and 2021. These historical and projected population estimates were grouped into two age groups, ages 18-64 and ages 65 and over. The compounded annual growth rates between 2016 and 2021 for each of these age groups was calculated and used to project population growth in years 2022, 2023 and 2024.
16. What is the source of the use rate data in Tables 9 and 10? Of the discharges shown in Table 11?
Applicant Response
The historical use rates presented in Tables 9 and 10 are based on the calculation of psychiatric discharges for residents in UC Behavioral Health’s projected service area from acute and specialty hospitals in Maryland and Delaware divided by the estimated population in the service area. The population estimate for 2016 was obtained from Nielsen Claritas. The population estimate for 2015 was interpolated between the estimates of population obtained from Nielsen Claritas for 2010 and 2016 using the compounded annual growth rate between these years. The psychiatric discharges used in the calculation of use rates in Tables 9 and 10 and presented in Table 11 were obtained from The St. Paul Group’s non-confidential abstract patient level database for acute hospitals in Maryland, The St. Paul Group’s summarized database of discharges for specialty hospitals in Maryland, and the Delaware Health Information Network summarized database of discharges for hospitals in Delaware.
The projected use rates presented in Tables 9 and 10 are based on the application of assumptions regarding future changes in use rates to the historical calculated use rates. The assumptions regarding future changes in use rates are presented on pages 40 and 41 of UM UCH’s CON application. The projected service area discharges presented in Table 11 are based on the multiplication of projected population times the projected use rates in each year.
17. Reference is made to non-geriatric patients aged 65+; please explain how the geriatric/non-geriatric classification is made.
Applicant Response
An adult patient will likely be admitted to the geriatric unit if the patient suffers from any of the diagnoses presented on Table 8 on page 40 of UM UCH’s CON Application. While age is often the most common marker to denote someone who is “geriatric,” that line may be blurred by the cognitive and activity level of the individual. Dementia, Alzheimer’s and other diseases commonly associated with aging as reflected on Table 8, will be the primary determinants of admission to a geriatric unit more so than age.
18. Provide sourcing for Tables 12, 13, 14, and 15.

#606814 9 011888-0023
Applicant Response
UC Behavioral Health’s historical market share, as presented in Tables 12 and 13, are based on the division of historical psychiatric discharges from HMH and Union Hospital for residents of UC Behavioral Health’s projected service area by the total number of psychiatric discharges from acute and specialty hospitals in Maryland and Delaware for UC Behavioral Health’s service area. The psychiatric discharges used in these calculations of market share were obtained from The St. Paul Group’s non-confidential abstract patient level database for acute hospitals in Maryland, The St. Paul Group’s summarized database of discharges for specialty hospitals in Maryland, and the Delaware Health Information Network summarized database of discharges for hospitals in Delaware.
The projected market shares presented in Tables 12 and 13 are based on the application of assumptions regarding future changes in market share to the historical calculated market shares. The assumptions regarding future changes in market share are presented in the on pages 42 and 43 of the CON application.
UC Behavioral Health’s historical out-of-service area discharges expressed as a percentage of UC Behavioral Health’s service area discharges, as presented in Tables 14 and 15, are based on the division of historical psychiatric discharges from HMH and Union Hospital related to zip codes outside of the UC Behavioral Health service area by HMH and Union Hospital’s historical psychiatric discharges from zip codes within the service area. The psychiatric discharges used in these calculations were obtained from The St. Paul Group’s non-confidential abstract patient level database for acute hospitals in Maryland. The projected out-of-service area discharges expressed as a percentage of UC Behavioral Health’s service area discharges, as presented in Tables 14 and 15, are expected to remain constant at the historical fiscal year 2016 levels.
19. Provide historical (3 years) and projected inpatient psychiatric market share data for each zip code in the projected primary and secondary service areas.
Applicant Response
Presented below is UC Behavioral Health’s combined primary and secondary service area market share data between fiscal years 2014 and 2016, by zip code, and separately provided for the Geriatric 18-64, Geriatric 65+, Non-Geriatric 18-64, and Non-Geriatric 65+ cohorts. While discharges from Maryland acute hospitals could be identified by zip code, the discharges from Maryland specialty hospitals and Delaware hospitals were provided in summary reports that did not identify zip codes.
The projection of UC Behavioral Health’s psychiatric market share as calculated for the four cohort levels, including both geriatric and non-geriatric patients at both ages 18-64 and ages 65 and over, is set forth in Tables 23 through 26 below. The assumptions regarding future changes in market share, by cohort, are presented on pages 42 and 43 of UM UCH’s CON application. These changes, at the cohort level, are inherently applied to each zip code with equal weight.

#606814 10 011888-0023
Table 23
UC Behavioral HealthService Area Market Share by Zip Code (Geriatric 18-64)
FY2014 - FY201618-64
Service Area Discharges UCBH Discharges UCBH Market ShareZip Codes FY2014 FY2015 FY2016 FY2014 FY2015 FY2016 FY2014 FY2015 FY2016
21001 4 2 3 3 2 3 75.0% 100.0% 100.0%21005 - - 1 - - 1 0.0% 0.0% 100.0%21009 2 2 3 1 1 3 50.0% 50.0% 100.0%21014 3 3 4 1 3 3 33.3% 100.0% 75.0%21015 - 5 3 - 4 3 0.0% 80.0% 100.0%21028 - - 1 - - 1 0.0% 0.0% 100.0%21040 1 - 3 1 - 2 100.0% 0.0% 66.7%21047 2 1 3 1 - 3 50.0% 0.0% 100.0%21050 2 1 2 2 1 1 100.0% 100.0% 50.0%21078 2 1 3 2 1 3 100.0% 100.0% 100.0%21084 - - 1 - - 1 0.0% 0.0% 100.0%21085 4 1 2 3 - 2 75.0% 0.0% 100.0%21160 1 - - 1 - - 100.0% 0.0% 0.0%21161 1 - - - - - 0.0% 0.0% 0.0%21220 4 2 4 - - - 0.0% 0.0% 0.0%21221 3 4 6 - - 1 0.0% 0.0% 16.7%21222 7 4 8 1 - - 14.3% 0.0% 0.0%21234 6 4 7 1 - - 16.7% 0.0% 0.0%21901 1 - - 1 - - 100.0% 0.0% 0.0%21903 3 - - 2 - - 66.7% 0.0% 0.0%21904 2 1 2 1 1 1 50.0% 100.0% 50.0%21911 - 1 - - - - 0.0% 0.0% 0.0%21914 - - 1 - - 1 0.0% 0.0% 100.0%21918 2 1 1 1 1 1 50.0% 100.0% 100.0%21919 - - - - - - 0.0% 0.0% 0.0%21921 1 2 9 - 1 9 0.0% 50.0% 100.0%MD Specialty Hospitals 8 6 9 - - - 0.0% 0.0% 0.0%Delaware Hospitals 3 2 4 - - - 0.0% 0.0% 0.0%
Total 62 43 80 22 15 39 35.7% 35.1% 48.9%
Sources: - St. Paul's non-confidential abstract patient level database for acute hospitals- St. Paul's summarized database of discharges for specialty hospitals- Delaware Health Information Network for Delaware hospital discharges

#606814 11 011888-0023
Table 24
UC Behavioral HealthService Area Market Share by Zip Code (Geriatric 65+)
FY2014 - FY201665+
Service Area Discharges UCBH Discharges UCBH Market ShareZip Codes FY2014 FY2015 FY2016 FY2014 FY2015 FY2016 FY2014 FY2015 FY2016
21001 7 5 22 5 4 18 71.4% 80.0% 81.8%21009 8 12 20 6 11 10 75.0% 91.7% 50.0%21014 28 11 22 22 10 20 78.6% 90.9% 90.9%21015 15 14 7 15 12 6 100.0% 85.7% 85.7%21017 6 1 3 4 1 2 66.7% 100.0% 66.7%21028 2 2 2 2 2 2 100.0% 100.0% 100.0%21034 - 3 2 - 1 1 0.0% 33.3% 50.0%21040 3 6 2 1 6 1 33.3% 100.0% 50.0%21047 5 8 6 3 6 1 60.0% 75.0% 16.7%21050 18 7 8 17 5 6 94.4% 71.4% 75.0%21078 8 7 16 7 3 11 87.5% 42.9% 68.8%21084 3 2 5 3 2 1 100.0% 100.0% 20.0%21085 8 8 15 3 7 6 37.5% 87.5% 40.0%21132 1 - 1 1 - 1 100.0% 0.0% 100.0%21154 3 5 4 3 5 3 100.0% 100.0% 75.0%21160 1 2 3 1 1 2 100.0% 50.0% 66.7%21161 1 3 - 1 2 - 100.0% 66.7% 0.0%21220 17 17 23 - 1 - 0.0% 5.9% 0.0%21221 22 21 31 - - - 0.0% 0.0% 0.0%21222 31 28 38 - - - 0.0% 0.0% 0.0%21234 44 34 56 - - - 0.0% 0.0% 0.0%21635 1 - - 1 - - 100.0% 0.0% 0.0%21901 2 2 7 1 2 4 50.0% 100.0% 57.1%21903 3 1 2 3 1 1 100.0% 100.0% 50.0%21904 2 2 2 2 2 1 100.0% 100.0% 50.0%21911 1 4 4 1 3 4 100.0% 75.0% 100.0%21915 - - 1 - - 1 0.0% 0.0% 100.0%21917 2 - 1 2 - 1 100.0% 0.0% 100.0%21918 1 3 1 1 3 1 100.0% 100.0% 100.0%21919 1 - - 1 - - 100.0% 0.0% 0.0%21921 12 7 15 9 7 14 75.0% 100.0% 93.3%MD Specialty Hospitals 178 196 156 - - - 0.0% 0.0% 0.0%Delaware Hospitals 13 11 24 - - - 0.0% 0.0% 0.0%
Total 447 422 499 115 97 118 25.7% 23.0% 23.7%
Sources: - St. Paul's non-confidential abstract patient level database for acute hospitals- St. Paul's summarized database of discharges for specialty hospitals- Delaware Health Information Network for Delaware hospital discharges

#606814 12 011888-0023
Table 25
UC Behavioral HealthService Area Market Share by Zip Code (Non-Geriatric 18-64)
FY2014 - FY201618-64
Service Area Discharges UCBH Discharges UCBH Market ShareZip Codes FY2014 FY2015 FY2016 FY2014 FY2015 FY2016 FY2014 FY2015 FY2016
19702 6 2 6 5 2 6 83.3% 100.0% 100.0%21001 221 179 207 198 168 176 89.6% 93.9% 85.0%21005 8 2 7 7 2 7 87.5% 100.0% 100.0%21009 111 86 100 82 60 79 73.9% 69.8% 79.0%21014 156 145 132 115 118 114 73.7% 81.4% 86.4%21015 81 69 72 65 56 56 80.2% 81.2% 77.8%21017 47 40 47 45 36 39 95.7% 90.0% 83.0%21028 14 10 13 8 7 10 57.1% 70.0% 76.9%21034 10 14 6 7 13 5 70.0% 92.9% 83.3%21040 186 197 166 140 165 129 75.3% 83.8% 77.7%21047 19 19 29 13 13 17 68.4% 68.4% 58.6%21050 43 37 58 32 26 43 74.4% 70.3% 74.1%21078 127 137 118 110 123 106 86.6% 89.8% 89.8%21084 21 15 20 11 8 14 52.4% 53.3% 70.0%21085 67 71 71 43 38 39 64.2% 53.5% 54.9%21132 4 1 8 4 1 6 100.0% 100.0% 75.0%21154 19 29 17 17 22 14 89.5% 75.9% 82.4%21160 12 6 5 11 4 5 91.7% 66.7% 100.0%21161 8 5 10 8 1 4 100.0% 20.0% 40.0%21220 298 269 280 9 13 10 3.0% 4.8% 3.6%21221 339 310 290 8 6 3 2.4% 1.9% 1.0%21222 467 486 477 18 8 5 3.9% 1.6% 1.0%21234 343 275 280 19 11 3 5.5% 4.0% 1.1%21635 11 14 7 8 8 5 72.7% 57.1% 71.4%21901 100 81 80 92 79 79 92.0% 97.5% 98.8%21903 39 27 49 38 23 43 97.4% 85.2% 87.8%21904 48 30 44 43 28 41 89.6% 93.3% 93.2%21911 47 44 35 43 39 32 91.5% 88.6% 91.4%21914 6 9 9 5 6 9 83.3% 66.7% 100.0%21915 9 12 9 9 10 9 100.0% 83.3% 100.0%21917 12 4 4 11 4 4 91.7% 100.0% 100.0%21918 23 15 15 20 14 15 87.0% 93.3% 100.0%21919 7 16 7 6 16 7 85.7% 100.0% 100.0%21921 242 273 280 233 261 267 96.3% 95.6% 95.4%21922 6 13 6 6 13 6 100.0% 100.0% 100.0%MD Specialty Hospitals 8,275 8,016 8,090 - - - 0.0% 0.0% 0.0%Delaware Hospitals 572 548 553 - - - 0.0% 0.0% 0.0%
Total 12,004 11,506 11,607 1,489 1,402 1,407 12.4% 12.2% 12.1%
Sources: - St. Paul's non-confidential abstract patient level database for acute hospitals- St. Paul's summarized database of discharges for specialty hospitals- Delaware Health Information Network for Delaware hospital discharges

#606814 13 011888-0023
Table 26
UC Behavioral HealthService Area Market Share by Zip Code (Non-Geriatric 65+)
FY2014 - FY201665+
Service Area Discharges UCBH Discharges UCBH Market ShareZip Codes FY2014 FY2015 FY2016 FY2014 FY2015 FY2016 FY2014 FY2015 FY2016
21001 16 16 11 8 15 9 50.0% 93.8% 81.8%21005 - - 1 - - 1 0.0% 0.0% 100.0%21009 1 5 17 - 4 11 0.0% 80.0% 64.7%21014 16 9 11 10 7 9 62.5% 77.8% 81.8%21015 5 6 7 2 5 7 40.0% 83.3% 100.0%21017 1 2 1 1 2 - 100.0% 100.0% 0.0%21034 1 - - 1 - - 100.0% 0.0% 0.0%21040 2 5 2 1 2 2 50.0% 40.0% 100.0%21047 6 3 3 4 2 2 66.7% 66.7% 66.7%21050 1 3 5 1 3 1 100.0% 100.0% 20.0%21078 11 3 8 9 3 7 81.8% 100.0% 87.5%21084 1 3 1 - 2 1 0.0% 66.7% 100.0%21085 9 4 9 2 2 5 22.2% 50.0% 55.6%21132 2 1 - 1 - - 50.0% 0.0% 0.0%21154 3 5 - 1 1 - 33.3% 20.0% 0.0%21161 1 - 1 - - - 0.0% 0.0% 0.0%21220 18 24 15 1 - - 5.6% 0.0% 0.0%21221 18 26 14 1 - - 5.6% 0.0% 0.0%21222 35 35 29 - 1 - 0.0% 2.9% 0.0%21234 24 26 24 - - - 0.0% 0.0% 0.0%21901 3 3 5 3 3 4 100.0% 100.0% 80.0%21903 1 5 4 1 5 4 100.0% 100.0% 100.0%21904 1 3 5 1 3 5 100.0% 100.0% 100.0%21911 3 4 7 3 3 5 100.0% 75.0% 71.4%21914 1 3 1 - - - 0.0% 0.0% 0.0%21915 1 1 - 1 1 - 100.0% 100.0% 0.0%21917 - 1 3 - 1 3 0.0% 100.0% 100.0%21918 3 1 5 1 - 4 33.3% 0.0% 80.0%21921 14 21 30 13 18 27 92.9% 85.7% 90.0%MD Specialty Hospitals 596 558 572 - - - 0.0% 0.0% 0.0%Delaware Hospitals 40 39 40 - - - 0.0% 0.0% 0.0%
Total 834 815 831 66 83 107 7.9% 10.2% 12.9%
Sources: - St. Paul's non-confidential abstract patient level database for acute hospitals- St. Paul's summarized database of discharges for specialty hospitals- Delaware Health Information Network for Delaware hospital discharges

#606814 14 011888-0023
20. What is the assumption regarding inpatient market share from the portion of the market that currently primarily uses Union Memorial? If it is assumed that UCBH will replicate Union’s historical share, comment on the likelihood of that given the increased distance that patients from most parts of Union’s service area would have to travel. What are their alternatives?
Applicant Response
It is anticipated, that UC Behavioral Health will capture the same market share that had been captured within the inpatient psychiatric service area by Union Hospital due to market forces. For those in need of inpatient services for treatment of acute behavioral health disorders, there is very little choice in the Elkton marketplace and eastern Cecil County. Financial barriers created by Delaware hospitals not accepting Maryland Medicaid effectively precludes all Maryland Medicaid individuals from crossing the state line to access care at Delaware hospitals (e.g., Christiana Care Health System). UC Behavioral Health’s convenient location off of Interstate 95 will improve access to residents of Cecil County. Finally, for some inpatients whose needs can be appropriately treated in a less restrictive level of care, they will be better served by the continuum of outpatient services that are planned by Union Hospital.
21. Re: UC Behavioral Health Non-Geriatric Program Market Share (p.43):
a) You state that it “declined in fiscal year 2015, but then increased in fiscal year 2016.” What was that share in 2013 and 2014?
Applicant Response
UC Behavioral Health’s geriatric market share in the 18-64 age cohort increased from 31.7% in fiscal year 2013 to 48.9% in fiscal year 2016 while market share in the 65+ age cohort remained relatively constant. UC Behavioral Health’s non-geriatric market share in the 18-64 age cohort declined from 13.7% in fiscal year 2013 to 12.1% in fiscal year 2016 while market share in the 65+ age cohort increased from 8.5% in fiscal year 2013 to 12.9% in fiscal year 2016. See Table 27 below.

#606814 15 011888-0023
Table 27
b) Provide the historical market shares (3 years) of other providers UCBH is competing with in this market area.
Applicant Response
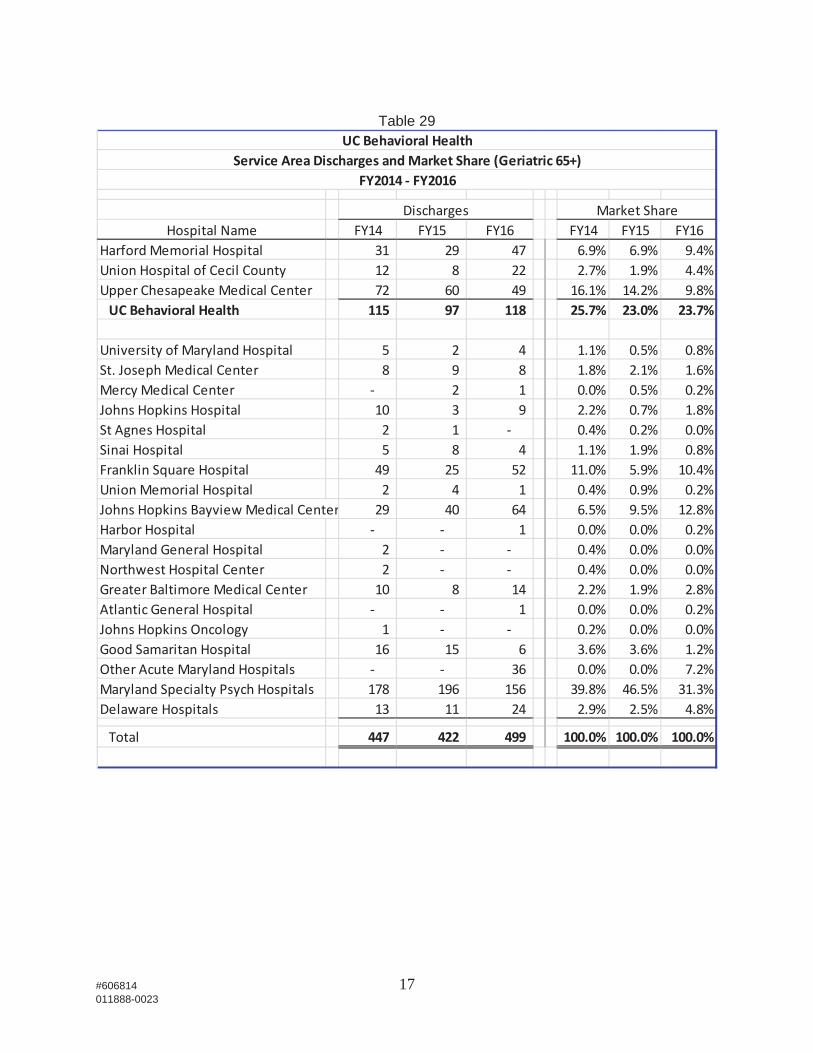
As presented in the Tables 28-31 reflecting historical market share, by cohort, the other acute hospitals that provide the majority of inpatient psychiatric services to the residents of UC Behavioral Health’s service area include Franklin Square Hospital, St. Joseph Medical Center, Johns Hopkins Bayview Medical Center, and Union Memorial Hospital.
UC Behavioral HealthHistorical Market Share
HistoricalFY2013 FY2014 FY2015 FY2016
Market Share
Geriatric
18-64 31.7% 35.7% 35.1% 48.9%%Change 12.7% -1.8% 39.3%
65+ 23.8% 25.7% 23.0% 23.7%%Change 8.2% -10.6% 2.9%
Non-Geriatric18-64 13.7% 12.4% 12.2% 12.1%%Change -9.5% -1.8% -0.5%
65+ 8.5% 7.9% 10.2% 12.9%%Change -7.1% 28.7% 26.5%

#606814 16 011888-0023
Table 28
UC Behavioral HealthService Area Discharges andMarket Share (Geriatric 18 64)
FY2014 FY20165 6 7
Discharges Market ShareHospital Name FY14 FY15 FY16 FY14 FY15 FY16
Harford Memorial Hospital 7 10 13 11.4% 23.4% 16.3%Union Hospital of Cecil County 1 11 0.0% 2.3% 13.8%Upper Chesapeake Medical Center 15 4 15 24.4% 9.4% 18.8%UC Behavioral Health 22 15 39 35.7% 35.1% 48.9%
University of Maryland Hospital 3 1 2 4.9% 2.3% 2.5%Holy Cross Hospital 1 0.0% 0.0% 1.3%St. Joseph Medical Center 1 2 0.0% 2.3% 2.5%Mercy Medical Center 1 0.0% 0.0% 1.3%Johns Hopkins Hospital 4 2 3 6.5% 4.7% 3.8%Sinai Hospital 2 0.0% 4.7% 0.0%Franklin Square Hospital 7 5 5 11.4% 11.7% 6.3%Union Memorial Hospital 1 0.0% 0.0% 1.3%Johns Hopkins Bayview Medical Center 6 6 5 9.7% 14.0% 6.3%Harbor Hospital 1 0.0% 0.0% 1.3%Memorial Hospital at Easton 1 1.6% 0.0% 0.0%Northwest Hospital Center 1 1 1.6% 2.3% 0.0%Greater Baltimore Medical Center 3 1 1 4.9% 2.3% 1.3%Johns Hopkins Oncology 1 0.0% 0.0% 1.3%Good Samaritan Hospital 1 1 1 1.6% 2.3% 1.3%Shock Trauma Center 3 1 4.9% 0.0% 1.3%Other Acute Maryland Hospitals 3 0.0% 0.0% 3.8%Maryland Specialty Psych Hospitals 8 6 9 13.0% 14.0% 11.3%Delaware Hospitals 3 2 4 4.1% 4.1% 4.8%
Total 62 43 80 100.0% 100.0% 100.0%
#606814 17 011888-0023
Table 29
UC Behavioral HealthService Area Discharges andMarket Share (Geriatric 65+)
FY2014 FY20165 6 7
Discharges Market ShareHospital Name FY14 FY15 FY16 FY14 FY15 FY16
Harford Memorial Hospital 31 29 47 6.9% 6.9% 9.4%Union Hospital of Cecil County 12 8 22 2.7% 1.9% 4.4%Upper Chesapeake Medical Center 72 60 49 16.1% 14.2% 9.8%UC Behavioral Health 115 97 118 25.7% 23.0% 23.7%
University of Maryland Hospital 5 2 4 1.1% 0.5% 0.8%St. Joseph Medical Center 8 9 8 1.8% 2.1% 1.6%Mercy Medical Center 2 1 0.0% 0.5% 0.2%Johns Hopkins Hospital 10 3 9 2.2% 0.7% 1.8%St Agnes Hospital 2 1 0.4% 0.2% 0.0%Sinai Hospital 5 8 4 1.1% 1.9% 0.8%Franklin Square Hospital 49 25 52 11.0% 5.9% 10.4%Union Memorial Hospital 2 4 1 0.4% 0.9% 0.2%Johns Hopkins Bayview Medical Center 29 40 64 6.5% 9.5% 12.8%Harbor Hospital 1 0.0% 0.0% 0.2%Maryland General Hospital 2 0.4% 0.0% 0.0%Northwest Hospital Center 2 0.4% 0.0% 0.0%Greater Baltimore Medical Center 10 8 14 2.2% 1.9% 2.8%Atlantic General Hospital 1 0.0% 0.0% 0.2%Johns Hopkins Oncology 1 0.2% 0.0% 0.0%Good Samaritan Hospital 16 15 6 3.6% 3.6% 1.2%Other Acute Maryland Hospitals 36 0.0% 0.0% 7.2%Maryland Specialty Psych Hospitals 178 196 156 39.8% 46.5% 31.3%Delaware Hospitals 13 11 24 2.9% 2.5% 4.8%
Total 447 422 499 100.0% 100.0% 100.0%

#606814 18 011888-0023
Table 30
UC Behavioral HealthService Area Discharges andMarket Share (Non Geriatric 18 64) FY 2014 FY2016
Discharges Market ShareHospital Name FY14 FY15 FY16 FY14 FY15 FY16
Harford Memorial Hospital 1,045 957 966 8.7% 8.3% 8.3%Union Hospital of Cecil County 444 445 441 3.7% 3.9% 3.8%UC Behavioral Health 1,489 1,402 1,407 12.4% 12.2% 12.1%
Meritus Medical Center 1 1 0.0% 0.0% 0.0%University of Maryland Hospital 115 74 51 1.0% 0.6% 0.4%Prince George's Hospital Center 1 0.0% 0.0% 0.0%Holy Cross Hospital 1 1 0.0% 0.0% 0.0%Frederick Memorial Hospital 2 2 0.0% 0.0% 0.0%St. Joseph Medical Center 155 147 150 1.3% 1.3% 1.3%Mercy Medical Center 3 2 1 0.0% 0.0% 0.0%Johns Hopkins Hospital 165 133 93 1.4% 1.2% 0.8%Dorchester General Hospital 8 9 7 0.1% 0.1% 0.1%Sinai Hospital 26 29 31 0.2% 0.3% 0.3%Bon Secours Hospital 80 67 69 0.7% 0.6% 0.6%Franklin Square Hospital 631 595 671 5.3% 5.2% 5.8%Washington Adventist Hospital 5 7 3 0.0% 0.1% 0.0%Montgomery General Hospital 1 5 6 0.0% 0.0% 0.1%Peninsula Regional Medical Center 1 7 1 0.0% 0.1% 0.0%Suburban Hospital 2 0.0% 0.0% 0.0%Union Memorial Hospital 122 102 116 1.0% 0.9% 1.0%Western Maryland Regional Medical Ce 2 0.0% 0.0% 0.0%St Mary's Hospital 2 1 0.0% 0.0% 0.0%Johns Hopkins Bayview Medical Center 231 243 217 1.9% 2.1% 1.9%Carroll Hospital Center 13 9 1 0.1% 0.1% 0.0%Maryland General Hospital 49 57 47 0.4% 0.5% 0.4%Calvert Memorial Hospital 1 2 0.0% 0.0% 0.0%Northwest Hospital Center 25 22 32 0.2% 0.2% 0.3%Baltimore Washington Medical Center 10 10 10 0.1% 0.1% 0.1%Greater Baltimore Medical Center 1 2 3 0.0% 0.0% 0.0%Howard County General Hospital 15 10 14 0.1% 0.1% 0.1%Southern Maryland Hosptial Center 3 7 0.0% 0.0% 0.1%Laurel Regional Hospital 5 2 5 0.0% 0.0% 0.0%Good Samaritan Hospital 3 5 0.0% 0.0% 0.0%Shock Trauma Center 1 0.0% 0.0% 0.0%Other Acute Maryland Hospitals 5 0.0% 0.0% 0.0%Maryland Specialty Psych Hospitals 8,275 8,016 8,090 68.9% 69.7% 69.7%Delaware Hospitals 572 548 552 4.8% 4.8% 4.8%
Total 12,004 11,506 11,606 100.0% 100.0% 100.0%

#606814 19 011888-0023
Table 31
22. Table 15 has a title that is, let’s say, somewhat confusing. Please restate it. Also, what is it attempting to communicate?
Applicant Response
The title for Table 15 should read “UC Behavioral Health’s Out-of-Service Area Discharges Expressed as a Percentage of UC Behavioral Health’s Service Area Discharges
UC Behavioral HealthService Area Discharges andMarket Share (Non Geriatric 65+)
FY2014 FY2016
Discharges Market ShareHospital Name FY14 FY15 FY16 FY14 FY15 FY16
Harford Memorial Hospital 44 59 74 5.3% 7.2% 8.9%Union Hospital of Cecil County 22 24 33 2.6% 2.9% 4.0%UC Behavioral Health 66 83 107 7.9% 10.2% 12.9%
University of Maryland Hospital 10 16 9 1.2% 2.0% 1.1%Holy Cross Hospital 1 0.1% 0.0% 0.0%St. Joseph Medical Center 18 14 12 2.2% 1.7% 1.4%Mercy Medical Center 1 0.0% 0.0% 0.1%Johns Hopkins Hospital 15 16 14 1.8% 2.0% 1.7%Sinai Hospital 1 3 2 0.1% 0.4% 0.2%Franklin Square Hospital 38 40 26 4.6% 4.9% 3.1%Washington Adventist Hospital 1 0.0% 0.0% 0.1%Montgomery General Hospital 1 0.0% 0.1% 0.0%Union Memorial Hospital 2 6 3 0.2% 0.7% 0.4%Johns Hopkins Bayview Medical Center 22 25 20 2.6% 3.1% 2.4%Maryland General Hospital 12 6 2 1.4% 0.7% 0.2%Northwest Hospital Center 4 2 0.5% 0.2% 0.0%Baltimore Washington Medical Center 1 1 0.1% 0.0% 0.1%Greater Baltimore Medical Center 4 1 0.0% 0.5% 0.1%Southern Maryland Hosptial Center 1 0.0% 0.0% 0.1%Good Samaritan Hospital 8 2 1.0% 0.2% 0.0%Other Acute Maryland Hospitals 19 0.0% 0.0% 2.3%Maryland Specialty Psych Hospitals 596 558 572 71.5% 68.5% 68.9%Delaware Hospitals 40 39 40 4.8% 4.8% 4.8%
Total 834 815 831 100.0% 100.0% 100.0%

#606814 20 011888-0023
Non-Geriatric Psychiatric FY2015- FY2024.” Similarly, the title for Table 14 should read “UC Behavioral Health’s Out-of-Service Area Discharges Expressed as a Percentage of UC Behavioral Health’s Service Area Discharges Geriatric Psychiatric FY2015- FY2024.” Both Tables 14 and 15 are designed to reflect the out-of-service area discharges at UC Behavioral Health as a percentage of service area discharges.
Revised Table 14 UC Behavioral Health’s Out-of-Service Area Discharges
Expressed as a Percentage of UC Behavioral Health’s Service Area Discharges Geriatric Psychiatric
FY2015 - FY2024
Revised Table 15 UC Behavioral Health’s Out-of-Service Area Discharges
Expressed as a Percentage of UC Behavioral Health’s Service Area Discharges Non-Geriatric Psychiatric
FY2015 - FY2024
23. On p. 46 the statement is made: “inpatient bed occupancy was conservatively projected at 85%.” Did you mean to say that the needed number of beds was projected based on a target occupancy of 85%? Or, as it says, occupancy was projected to be 85%? These are not synonymous.
Applicant Response
UM UCH calculated the projected average daily census based on the population, use rate, and market share factors explained on pages 36 through 45 of the CON application. Only after the projected average daily census was determined, did UM UCH apply the 85% occupancy percentage to calculate the number of beds needed in 2024, dividing the projected average daily census by 0.85. This was the meaning of “inpatient bed occupancy was conservatively projected at 85%.”
Historical Projected % ChangeFY2015 FY2016 FY2017 FY2018 FY2019 FY2020 FY2021 FY2022 FY2023 FY2024 FY16-FY24
Out-of-Service Area Discharges % of Service Area Discharges
Geriatric18-64 6.7% 5.1% 5.1% 5.1% 5.1% 5.1% 5.1% 5.1% 5.1% 5.1%%Change -7.0% -1.5% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0%
65+ 11.3% 8.5% 8.5% 8.5% 8.5% 8.5% 8.5% 8.5% 8.5% 8.5%%Change -7.0% -1.5% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0%
Historical Projected % ChangeFY2015 FY2016 FY2017 FY2018 FY2019 FY2020 FY2021 FY2022 FY2023 FY2024 FY16-FY24
Out-of-Service Area Discharges % of Service Area DischargesNon-Geriatric
18-64 22.1% 18.6% 18.6% 18.6% 18.6% 18.6% 18.6% 18.6% 18.6% 18.6%%Change -6.2% -3.5% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0%
65+ 12.0% 6.5% 6.5% 6.5% 6.5% 6.5% 6.5% 6.5% 6.5% 6.5%%Change 4.6% 5.5% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0%
#606814 21 011888-0023
UM UCH had looked at the State Health Plan section on “State Health Plan for Facilities and Services: Overview, Psychiatric Services, and Emergency Medical Services” (COMAR 10.21.07) (which dates back to 1984) and found that there is only one reference to facility specific occupancy rates. This can be found on page AP-11, under standard AP 10, which states:
AP 10. Expansion of existing adult acute psychiatric bed capacity will not be approved in any hospital that has a psychiatric unit that does not meet the following occupancy standards for two consecutive years prior to formal submission of the application.
Psychiatric Bed 'Range (PBR) Occupancy Standards PBR<20 80%
20 PBR<40 85% PBR 40 90%
While (as stated on page 32 of the application) UM UCH believes that this standard is inapplicable because the proposed project does not involve expansion of existing adult care psychiatric beds, UM UCH decided to use this standard as a guide in regard to which occupancy percentage it should use. UM UCH considered whether it should apply the 85% occupancy percentage to the 28 beds for Acute Psychiatric care and the 80% occupancy percentage for the separate 12 bed Geropsychiatric unit. UM UCH chose to apply the 85% occupancy to both units. Hence, UCH determined that it was being conservative.
Availability of more cost-effective alternatives
24. The statement is made (p. 53) that “UM UCH and Union Hospital have established a two-county behavioral health joint venture that will oversee the distribution of all behavioral health services in Harford and Cecil Counties.” Similar to question 2 above, is this “joint venture” a formal business agreement or a loose collaboration/partnership? Describe it more definitively, in corporate and legal terms.
Applicant Response
See the Applicant’s response to Question 2 above.
25. Explain:
a) The statement on p. 53 that “A new special psychiatric hospital would provide Maryland system saving of $3.1 million annually due to the special psychiatric hospital’s reimbursement being based on the Medicare prospective payment system and a reduction in rates for Medicaid utilization.” What conditions or assumptions are behind that statement?

#606814 22 011888-0023
Applicant Response
The $3.1 million Maryland system savings was calculated using assuming the rates that Medicare will pay UC Behavioral health will be approximately 35% below what Medicare currently pays in the current regulated settings at HMH and Union Hospital. Potential reduction in Medicaid payments was not considered in this calculation.
b) What the terms of an agreement with HSCRC would need to be to obviate the need for a rate increase (relevant to the statement: “Pending an agreement with the HSCRC regarding distribution of HMH’s global budget revenue, an increase in rates from the HSCRC will not be required under Alternative 4…”, p. 54).
Applicant Response
UM Upper Chesapeake Health is negotiating with the HSCRC to reallocate revenue from HMH’s global budget revenue cap to cover capital expenses and volume redistribution at UC Behavioral Health, UCMC, and UC FMF. Assuming that a sufficient amount of HMH’s global budget revenue cap is reallocated within UM UCH, UM UCH anticipates that an increase in rates will not be required under Alternative 4.
26. On p. 53 the application states: “The new FMF will cost $51,962,824. The FMF would cost approximately $6,972,020 less if built as a stand-along (sic) facility because project site work and other costs can be shared with another facility. Don’t you mean would cost more if built by itself?
Applicant Response
Construction of UC FMF and UC Behavioral Health at the same time and with shared systems and architecture will achieve $6,972,020 in cost savings as opposed to being constructed at different times in different locations. Accordingly, UC FMF would cost approximately $6,972,020 more if built as a stand-alone facility.
Viability
27. Please discuss how the proposed 40-bed behavioral health pavilion will address the Medicaid Institutions for Mental Diseases (“IMD”) exclusion that prohibits the use of federal Medicaid financing for mental health facilities larger than 16 beds that are not part of general hospitals.
a) What is the applicant’s assumption regarding the impact of the IMD exclusion on reimbursement?
Applicant Response
The Applicant assumes that Maryland Medicaid will reimburse UC Behavioral Health at 94% of HSCRC rates for inpatient admissions of Medicaid beneficiaries aged 21-64 as it presently does with existing IMDs following the end of Maryland’s participation in the Medicaid Emergency Psychiatric Demonstration. Because the so-called Medicaid IMD exclusion or

#606814 23 011888-0023
prohibition of federal financial participation for Medicaid payments to institutions for mental disease (“IMDs”) applies only to “residents” between the ages 21 and 64, the Applicant does not project that the IMD exclusion will have any impact on federal Medicaid funding for outpatient services, or inpatient services to adult Medicaid beneficiaries under 21 years of age and those older than 64.
b) Please discuss the potential impact on the proposed facility if – because of the IMD exclusion -- adequate funding through the Medicaid program to cover the costs associated with indigent patients who require psychiatric care is not provided by the State.
Applicant Response
As noted above, given UC Behavioral Health’s benefits to the health delivery system, the Applicant does not anticipate reduced rates for Medicaid inpatients subject to the IMD exclusion. Recognizing the benefits that IMDs serve to the health care delivery system, Maryland has continued to budget for and fund Medicaid payments to IMDs following the end of the Medicaid Emergency Psychiatric Demonstration. A worst-case scenario assumes that UC Behavioral Health would continue to provide the same level of inpatient care to Medicaid beneficiaries but Medicaid payments to Maryland IMDs would be reduced to the state’s share of Medicaid expenditures calculated according to Maryland’s historic 0.50 federal matching assistance percentage (“FMAP”). Under this “worst-case” scenario UC Behavioral Health could lose approximately $5 million annually in Medicaid reimbursement as calculated in Table 33. Notably, this “worst-case” calculation assumes a 50% reduction in all Medicaid payments for inpatient admissions, and, therefore, overstates the potential reduction in Medicaid reimbursement. As noted above, Medicaid would still reimburse UC Behavioral Health at 94% for Medicaid inpatients not subject to the IMD exclusion, including adult Medicaid patients under 21 years of age and those older than 64.
Table 32 Assumed 50% Reduction in Medicaid Inpatient Reimbursement
Projected FY 2022 IP Charges (Table H, Line 1.a) $25,955,056Estimated IP Psych Medicaid Payer Mix (Table H, Line 4.a.2) 41.30%IP Medicaid Psych Revenue at 100% of Charges $10,719,438
6% Contractual Allowance $643,166.00IP Medicaid Psych Revenue at 94% of Charges $10,076,272New Medicaid Payment Factor 50%IP Medicaid Revenue Under Worst Case Scenario $5,038,136
This projected “worst-case” scenario loss of inpatient Medicaid revenue would also be offset by Medicaid disproportionate share payments to UC Behavioral Health for which matching federal funding is available regardless of a facility’s IMD status.
The Applicant should also note that this “worst-case” scenario is unlikely even if Maryland determines that it can no longer continue to fund state-share only Medicaid payments to IMDs. On May 6, 2016, the Centers for Medicaid and Medicare Services (“CMS”) issued a final rule clarifying certain Medicaid managed care regulations to allow federal financial

#606814 24 011888-0023
participation associated with capitation payments to Medicaid managed care organizations for plan enrollees who are inpatients in an IMD for 15 days or less in one month and up to 30 days if such inpatient admissions span two months. See Department of Health and Human Services, Centers for Medicare and Medicaid Services, Medicaid and Children’s Health Insurance Programs; Medicaid Managed Care, CHIP Delivered in Managed Care, Medicaid and CHIP Comprehensive Quality Strategies, and Revisions to Third Party Liability, 81 Fed. Reg. 27,498, 27,555-27,564 (May 6, 2016). More specifically, CMS’s final rule clarified that states may receive federal financial participation and make capitation payments to managed care organizations, prepaid inpatient health plans, and prepaid ambulatory health plans for short term stays in an IMD “in lieu of” covered Medicaid services, such as an inpatient admission for psychiatric treatment in an acute general hospital, subject to regulatory requirements of 42 C.F.R. § 438.6(e)(2).
This clarification does not currently affect Maryland Medicaid because the state has carved behavioral health services in an IMD out of its HealthChoice managed care program. In the event adequate state funding were not available to reimburse IMDs for inpatient services to Medicaid beneficiaries aged 21-64, however, the Applicant anticipates regulatory changes would be made to Maryland’s Medicaid program to take advantage of additional federal Medicaid funding under the clarified managed care regulations. See also Maryland Department of Health and Mental Hygiene, Report on Substance Use Disorder Carve-Out at 6-8, 68 (December 2016) (discussing CMS’s clarification of managed care regulations and explaining that flexible managed care options regarding coverage of IMD services may warrant further consideration).
Impact
28. The application states: “Pending final approval from the HSCRC regarding distribution of HMH’s global budget revenue, the proposed project would also provide Maryland system saving of $3.1 million annually due to the hospital’s reimbursement being based on the Medicare prospective payment system and a reduction in rates for Medicaid utilization.” Describe:
a) The proposal made to HSCRC, and when a response is expected.
Applicant Response
UM Upper Chesapeake Health is negotiating with the HSCRC to reallocate revenue from HMH’s global budget revenue cap to cover capital expenses and volume redistribution at UC Behavioral Health, UCMC, and UC FMF. The proposal to the HSCRC involves the construction of a Freestanding Medical Facility (“FMF”) in place of Harford Memorial Hospital (“HMH”) along with the construction of UC Behavioral Health. HMH inpatient volume will shift to the market, including UCMC and UC Behavioral Health, while HMH outpatient volume will either shift to UCMC, the unregulated setting, or will remain at either UC FMF or UC Behavioral Health. The proposal involves retaining revenue at UM Upper Chesapeake Health that is currently at HMH in order to pay for capital and volume. An agreement with the HSCRC on the distribution of HMH’s global budget revenue cap is anticipated before the Maryland Health Care Commission’s (“MHCC”) final approval of any of the three capital projects for which UM Upper Chesapeake Health and its constituent hospitals have sought the MHCC’s approval and is expected to predate any viability approval issued by the HSCRC.

#606814 25 011888-0023
b) How this $3.1 million saving would be realized.
Applicant Response
See the Applicant’s response to Question 25(a) above.

#606814 26 011888-0023
Table of Exhibits
Exhibit Description
2 Revised Exhibit 2 Project Drawings
12 HMH Fiscal Year 2018 Licensed Bed Designation
13 Table E – Including UC FMF and UC Behavioral Health (Question 5)
14 Tables F – HMH, Union Hospital, and Combined Utilization Tables (Question 8)
15 Table L – Current Entire Facility Including HMH (Question 9)
16 UM Upper Chesapeake Health’s policy relating to Interdisciplinary Discharge Planning for Behavioral Health
17 UM Upper Chesapeake Health’s polices relating to Patient Transfers
Table of Tables
Table Description
14
Revised UC Behavioral Health’s Out-of-Service Area Discharges Expressed as a Percentage of UC Behavioral Health’s Service Area Discharges Geriatric Psychiatric FY2015- FY2024
15
Revised UC Behavioral Health’s Out-of-Service Area Discharges Expressed as a Percentage of UC Behavioral Health’s Service Area Discharges Non-Geriatric Psychiatric FY2015- FY2024
21 Department Gross Square Footage UC FMF and UC Behavioral Health
22 UC Behavioral Health Projected Charge Per Case Price Leveled to FY 2016 Prices
23 UC Behavioral Health Service Area Market Share by Zip Code (Geriatric 18-64) FY 2014-FY2016
24 UC Behavioral Health Service Area Market Share by Zip Code (Geriatric 65+) FY 2014-FY2016
25 UC Behavioral Health Service Area Market Share by Zip Code (Non-Geriatric 18-64) FY 2014-FY2016
26 UC Behavioral Health Service Area Market Share by Zip Code (Non-Geriatric 65+) FY 2014-FY2016
#606814 27 011888-0023
27 UC Behavioral Health Historic Market Share
28 UC Behavioral Health Service Area Discharges and Market Share (Geriatric 18-64) FY 2014-FY2016
29 UC Behavioral Health Service Area Discharges and Market Share (Geriatric 65+) FY 2014-FY2016
30 UC Behavioral Health Service Area Discharges and Market Share (Non-Geriatric 18-64) FY 2014-FY2016
31 UC Behavioral Health Service Area Discharges and Market Share (Non-Geriatric 65+) FY 2014-FY2016
32 Assumed 50% Reduction in Medicaid Inpatient Reimbursement



#607962 011888-0023
I hereby declare and affirm under the penalties of perjury that the facts stated in
this application and its attachments are true and correct to the best of my knowledge,
information, and belief.
October 18, 2017 Date Andrew L. Solberg
A.L.S. Healthcare Consultant Services


EXHIBIT 2
REVISED






EXHIBIT 12




EXHIBIT 13

UC Behavioral Health UC FMF Total
SUBTOTAL
SUBTOTAL
SUBTOTAL $21,877,602 $20,592,109
TOTAL CURRENT CAPITAL COSTS
Land Purchase
TOTAL CAPITAL COSTS
c1. Legal Fees c2. Other (Specify/add rows if needed)
d1. Legal Feesd2. Other (Specify/add rows if needed)
SUBTOTAL $4,739,937 $4,429,067
TOTAL USES OF FUNDS $56,265,809 $51,962,824 $108,228,633
INSTRUCTION: Estimates for Capital Costs (1.a-e), Financing Costs and Other Cash Requirements (2.a-g), and Working Capital Startup Costs (3) must reflect current costs as of the date of application and include all costs for construction and renovation. Explain the basis for construction cost estimates, renovation cost estimates, contingencies, interest during construction period, and inflation in an attachment to the application.
NOTE: Inflation should only be included in the Inflation allowance line A.1.e. The value of donated land for the project should be included on Line A.1.d as a use of funds and on line B.8 as a source of funds

UC Behavioral Health UC FMF Total
INSTRUCTION: Estimates for Capital Costs (1.a-e), Financing Costs and Other Cash Requirements (2.a-g), and Working Capital Startup Costs (3) must reflect current costs as of the date of application and include all costs for construction and renovation. Explain the basis for construction cost estimates, renovation cost estimates, contingencies, interest during construction period, and inflation in an attachment to the application.
NOTE: Inflation should only be included in the Inflation allowance line A.1.e. The value of donated land for the project should be included on Line A.1.d as a use of funds and on line B.8 as a source of funds
TOTAL SOURCES OF FUNDS $56,265,809 $51,962,824
UC Behavioral Health UC FMF Total

EXHIBIT 14
Indi
cate
CY
or F
Y
Tota
l MSG
A
Tota
l Acu
te
TOTA
L D
ISC
HA
RG
ES
Tota
l MSG
A
Tota
l Acu
te
TOTA
L PA
TIEN
T D
AYS
INS
TRU
CTI
ON
: Com
plet
e th
is ta
ble
for t
he e
ntire
faci
lity,
incl
udin
g th
e pr
opos
ed p
roje
ct. I
ndic
ate
on th
e ta
ble
if th
e re
porti
ng p
erio
d is
Cal
enda
r Yea
r (C
Y) o
r Fis
cal Y
ear (
FY).
For
sect
ions
4 &
5, t
he n
umbe
r of b
eds
and
occu
panc
y pe
rcen
tage
sho
uld
be re
porte
d on
the
basi
s of
lice
nsed
bed
s. In
an
atta
chm
ent t
o th
e ap
plic
atio
n, p
rovi
de a
n ex
plan
atio
n or
bas
is fo
r th
e pr
ojec
tions
and
spe
cify
all
assu
mpt
ions
use
d. A
pplic
ants
mus
t exp
lain
why
the
assu
mpt
ions
are
reas
onab
le.

Indi
cate
CY
or F
Y
INS
TRU
CTI
ON
: Com
plet
e th
is ta
ble
for t
he e
ntire
faci
lity,
incl
udin
g th
e pr
opos
ed p
roje
ct. I
ndic
ate
on th
e ta
ble
if th
e re
porti
ng p
erio
d is
Cal
enda
r Yea
r (C
Y) o
r Fis
cal Y
ear (
FY).
For
sect
ions
4 &
5, t
he n
umbe
r of b
eds
and
occu
panc
y pe
rcen
tage
sho
uld
be re
porte
d on
the
basi
s of
lice
nsed
bed
s. In
an
atta
chm
ent t
o th
e ap
plic
atio
n, p
rovi
de a
n ex
plan
atio
n or
bas
is fo
r th
e pr
ojec
tions
and
spe
cify
all
assu
mpt
ions
use
d. A
pplic
ants
mus
t exp
lain
why
the
assu
mpt
ions
are
reas
onab
le.
Tota
l MSG
A
Tota
l Acu
te
TOTA
L A
VER
AG
E LE
NG
TH O
F ST
AY
Tota
l MSG
A
Tota
l Acu
te
TOTA
L LI
CEN
SED
BED
S

Indi
cate
CY
or F
Y
INS
TRU
CTI
ON
: Com
plet
e th
is ta
ble
for t
he e
ntire
faci
lity,
incl
udin
g th
e pr
opos
ed p
roje
ct. I
ndic
ate
on th
e ta
ble
if th
e re
porti
ng p
erio
d is
Cal
enda
r Yea
r (C
Y) o
r Fis
cal Y
ear (
FY).
For
sect
ions
4 &
5, t
he n
umbe
r of b
eds
and
occu
panc
y pe
rcen
tage
sho
uld
be re
porte
d on
the
basi
s of
lice
nsed
bed
s. In
an
atta
chm
ent t
o th
e ap
plic
atio
n, p
rovi
de a
n ex
plan
atio
n or
bas
is fo
r th
e pr
ojec
tions
and
spe
cify
all
assu
mpt
ions
use
d. A
pplic
ants
mus
t exp
lain
why
the
assu
mpt
ions
are
reas
onab
le.
Tota
l MSG
A
Tota
l Acu
te
TOTA
L O
CC
UPA
NC
Y %
TOTA
L O
UTP
ATI
ENT
VISI
TS
*IMPO
RTA
NT
NO
TE:
Leap
yea
r for
mul
as s
houl
d be
cha
nged
by
appl
ican
t to
refle
ct 3
66 d
ays
per y
ear.

Indi
cate
CY
or F
Y
Tota
l MSG
A
Tota
l Acu
te
TOTA
L D
ISC
HA
RG
ES
Tota
l MSG
A
Tota
l Acu
te
TOTA
L PA
TIEN
T D
AYS
INS
TRU
CTI
ON
: Com
plet
e th
is ta
ble
for t
he e
ntire
faci
lity,
incl
udin
g th
e pr
opos
ed p
roje
ct. I
ndic
ate
on th
e ta
ble
if th
e re
porti
ng p
erio
d is
Cal
enda
r Yea
r (C
Y) o
r Fis
cal Y
ear (
FY).
For
sect
ions
4 &
5, t
he n
umbe
r of b
eds
and
occu
panc
y pe
rcen
tage
sho
uld
be re
porte
d on
the
basi
s of
lice
nsed
bed
s. In
an
atta
chm
ent t
o th
e ap
plic
atio
n, p
rovi
de a
n ex
plan
atio
n or
bas
is fo
r th
e pr
ojec
tions
and
spe
cify
all
assu
mpt
ions
use
d. A
pplic
ants
mus
t exp
lain
why
the
assu
mpt
ions
are
reas
onab
le.
Indi
cate
CY
or F
Y
INS
TRU
CTI
ON
: Com
plet
e th
is ta
ble
for t
he e
ntire
faci
lity,
incl
udin
g th
e pr
opos
ed p
roje
ct. I
ndic
ate
on th
e ta
ble
if th
e re
porti
ng p
erio
d is
Cal
enda
r Yea
r (C
Y) o
r Fis
cal Y
ear (
FY).
For
sect
ions
4 &
5, t
he n
umbe
r of b
eds
and
occu
panc
y pe
rcen
tage
sho
uld
be re
porte
d on
the
basi
s of
lice
nsed
bed
s. In
an
atta
chm
ent t
o th
e ap
plic
atio
n, p
rovi
de a
n ex
plan
atio
n or
bas
is fo
r th
e pr
ojec
tions
and
spe
cify
all
assu
mpt
ions
use
d. A
pplic
ants
mus
t exp
lain
why
the
assu
mpt
ions
are
reas
onab
le.
Tota
l MSG
A
Tota
l Acu
te
TOTA
L A
VER
AG
E LE
NG
TH O
F ST
AY
Tota
l MSG
A
Tota
l Acu
te
TOTA
L LI
CEN
SED
BED
S
Indi
cate
CY
or F
Y
INS
TRU
CTI
ON
: Com
plet
e th
is ta
ble
for t
he e
ntire
faci
lity,
incl
udin
g th
e pr
opos
ed p
roje
ct. I
ndic
ate
on th
e ta
ble
if th
e re
porti
ng p
erio
d is
Cal
enda
r Yea
r (C
Y) o
r Fis
cal Y
ear (
FY).
For
sect
ions
4 &
5, t
he n
umbe
r of b
eds
and
occu
panc
y pe
rcen
tage
sho
uld
be re
porte
d on
the
basi
s of
lice
nsed
bed
s. In
an
atta
chm
ent t
o th
e ap
plic
atio
n, p
rovi
de a
n ex
plan
atio
n or
bas
is fo
r th
e pr
ojec
tions
and
spe
cify
all
assu
mpt
ions
use
d. A
pplic
ants
mus
t exp
lain
why
the
assu
mpt
ions
are
reas
onab
le.
Tota
l MSG
A
Tota
l Acu
te
TOTA
L O
CC
UPA
NC
Y %
TOTA
L O
UTP
ATI
ENT
VISI
TS
*IMPO
RTA
NT
NO
TE:
Leap
yea
r for
mul
as s
houl
d be
cha
nged
by
appl
ican
t to
refle
ct 3
66 d
ays
per y
ear.

Indi
cate
CY
or F
Y
Tota
l MSG
A
Tota
l Acu
te
TOTA
L D
ISC
HA
RG
ES
Tota
l MSG
A
Tota
l Acu
te
TOTA
L PA
TIEN
T D
AYS
INS
TRU
CTI
ON
: Com
plet
e th
is ta
ble
for t
he e
ntire
faci
lity,
incl
udin
g th
e pr
opos
ed p
roje
ct. I
ndic
ate
on th
e ta
ble
if th
e re
porti
ng p
erio
d is
Cal
enda
r Yea
r (C
Y) o
r Fis
cal Y
ear (
FY).
For
sect
ions
4 &
5, t
he n
umbe
r of b
eds
and
occu
panc
y pe
rcen
tage
sho
uld
be re
porte
d on
the
basi
s of
lice
nsed
bed
s. In
an
atta
chm
ent t
o th
e ap
plic
atio
n, p
rovi
de a
n ex
plan
atio
n or
bas
is fo
r th
e pr
ojec
tions
and
spe
cify
all
assu
mpt
ions
use
d. A
pplic
ants
mus
t exp
lain
why
the
assu
mpt
ions
are
reas
onab
le.

Indi
cate
CY
or F
Y
INS
TRU
CTI
ON
: Com
plet
e th
is ta
ble
for t
he e
ntire
faci
lity,
incl
udin
g th
e pr
opos
ed p
roje
ct. I
ndic
ate
on th
e ta
ble
if th
e re
porti
ng p
erio
d is
Cal
enda
r Yea
r (C
Y) o
r Fis
cal Y
ear (
FY).
For
sect
ions
4 &
5, t
he n
umbe
r of b
eds
and
occu
panc
y pe
rcen
tage
sho
uld
be re
porte
d on
the
basi
s of
lice
nsed
bed
s. In
an
atta
chm
ent t
o th
e ap
plic
atio
n, p
rovi
de a
n ex
plan
atio
n or
bas
is fo
r th
e pr
ojec
tions
and
spe
cify
all
assu
mpt
ions
use
d. A
pplic
ants
mus
t exp
lain
why
the
assu
mpt
ions
are
reas
onab
le.
Tota
l MSG
A
Tota
l Acu
te
TOTA
L A
VER
AG
E LE
NG
TH O
F ST
AY
Tota
l MSG
A
Tota
l Acu
te
TOTA
L LI
CEN
SED
BED
S

Indi
cate
CY
or F
Y
INS
TRU
CTI
ON
: Com
plet
e th
is ta
ble
for t
he e
ntire
faci
lity,
incl
udin
g th
e pr
opos
ed p
roje
ct. I
ndic
ate
on th
e ta
ble
if th
e re
porti
ng p
erio
d is
Cal
enda
r Yea
r (C
Y) o
r Fis
cal Y
ear (
FY).
For
sect
ions
4 &
5, t
he n
umbe
r of b
eds
and
occu
panc
y pe
rcen
tage
sho
uld
be re
porte
d on
the
basi
s of
lice
nsed
bed
s. In
an
atta
chm
ent t
o th
e ap
plic
atio
n, p
rovi
de a
n ex
plan
atio
n or
bas
is fo
r th
e pr
ojec
tions
and
spe
cify
all
assu
mpt
ions
use
d. A
pplic
ants
mus
t exp
lain
why
the
assu
mpt
ions
are
reas
onab
le.
Tota
l MSG
A
Tota
l Acu
te
TOTA
L O
CC
UPA
NC
Y %
TOTA
L O
UTP
ATI
ENT
VISI
TS
*IMPO
RTA
NT
NO
TE:
Leap
yea
r for
mul
as s
houl
d be
cha
nged
by
appl
ican
t to
refle
ct 3
66 d
ays
per y
ear.
EXHIBIT 15

(sho
uld
be
cons
iste
nt w
ith
proj
ectio
ns in
Ta
ble
G)
(Lis
t gen
eral
ca
tego
ries,
add
row
s if
need
ed)
INS
TRU
CTI
ON
: Lis
t the
faci
lity'
s ex
istin
g st
affin
g an
d ch
ange
s re
quire
d by
this
pro
ject
. Inc
lude
all
maj
or jo
b ca
tego
ries
unde
r eac
h he
adin
g pr
ovid
ed in
the
tabl
e. T
he n
umbe
r of F
ull T
ime
Equ
ival
ents
(FTE
s)
shou
ld b
e ca
lcul
ated
on
the
basi
s of
2,0
80 p
aid
hour
s pe
r yea
r equ
als
one
FTE
. In
an a
ttach
men
t to
the
appl
icat
ion,
exp
lain
any
fact
or u
sed
in c
onve
rting
pai
d ho
urs
to w
orke
d ho
urs.
Ple
ase
ensu
re th
at th
e pr
ojec
tions
in th
is ta
ble
are
cons
iste
nt w
ith e
xpen
ses
prov
ided
in u
ninf
late
d pr
ojec
tions
in T
able
s F
and
G.
CU
RR
ENT
ENTI
RE
FAC
ILIT
Y
PRO
JEC
TED
CH
AN
GES
AS
A R
ESU
LT O
F TH
E PR
OPO
SED
PR
OJE
CT
THR
OU
GH
TH
E LA
ST Y
EAR
OF
PRO
JEC
TIO
N (C
UR
REN
T D
OLL
AR
S)
OTH
ER E
XPEC
TED
CH
AN
GES
IN
OPE
RA
TIO
NS
THR
OU
GH
TH
E LA
ST
YEA
R O
F PR
OJE
CTI
ON
(CU
RR
ENT
DO
LLA
RS)
PRO
JEC
TED
EN
TIR
E FA
CIL
ITY
THR
OU
GH
TH
E LA
ST Y
EAR
OF
PRO
JEC
TIO
N
(CU
RR
ENT
DO
LLA
RS)
*

(sho
uld
be
cons
iste
nt w
ith
proj
ectio
ns in
Ta
ble
G)
INS
TRU
CTI
ON
: Lis
t the
faci
lity'
s ex
istin
g st
affin
g an
d ch
ange
s re
quire
d by
this
pro
ject
. Inc
lude
all
maj
or jo
b ca
tego
ries
unde
r eac
h he
adin
g pr
ovid
ed in
the
tabl
e. T
he n
umbe
r of F
ull T
ime
Equ
ival
ents
(FTE
s)
shou
ld b
e ca
lcul
ated
on
the
basi
s of
2,0
80 p
aid
hour
s pe
r yea
r equ
als
one
FTE
. In
an a
ttach
men
t to
the
appl
icat
ion,
exp
lain
any
fact
or u
sed
in c
onve
rting
pai
d ho
urs
to w
orke
d ho
urs.
Ple
ase
ensu
re th
at th
e pr
ojec
tions
in th
is ta
ble
are
cons
iste
nt w
ith e
xpen
ses
prov
ided
in u
ninf
late
d pr
ojec
tions
in T
able
s F
and
G.
CU
RR
ENT
ENTI
RE
FAC
ILIT
Y
PRO
JEC
TED
CH
AN
GES
AS
A R
ESU
LT O
F TH
E PR
OPO
SED
PR
OJE
CT
THR
OU
GH
TH
E LA
ST Y
EAR
OF
PRO
JEC
TIO
N (C
UR
REN
T D
OLL
AR
S)
OTH
ER E
XPEC
TED
CH
AN
GES
IN
OPE
RA
TIO
NS
THR
OU
GH
TH
E LA
ST
YEA
R O
F PR
OJE
CTI
ON
(CU
RR
ENT
DO
LLA
RS)
PRO
JEC
TED
EN
TIR
E FA
CIL
ITY
THR
OU
GH
TH
E LA
ST Y
EAR
OF
PRO
JEC
TIO
N
(CU
RR
ENT
DO
LLA
RS)
*
(Lis
t gen
eral
ca
tego
ries,
add
row
s if
need
ed)

(sho
uld
be
cons
iste
nt w
ith
proj
ectio
ns in
Ta
ble
G)
INS
TRU
CTI
ON
: Lis
t the
faci
lity'
s ex
istin
g st
affin
g an
d ch
ange
s re
quire
d by
this
pro
ject
. Inc
lude
all
maj
or jo
b ca
tego
ries
unde
r eac
h he
adin
g pr
ovid
ed in
the
tabl
e. T
he n
umbe
r of F
ull T
ime
Equ
ival
ents
(FTE
s)
shou
ld b
e ca
lcul
ated
on
the
basi
s of
2,0
80 p
aid
hour
s pe
r yea
r equ
als
one
FTE
. In
an a
ttach
men
t to
the
appl
icat
ion,
exp
lain
any
fact
or u
sed
in c
onve
rting
pai
d ho
urs
to w
orke
d ho
urs.
Ple
ase
ensu
re th
at th
e pr
ojec
tions
in th
is ta
ble
are
cons
iste
nt w
ith e
xpen
ses
prov
ided
in u
ninf
late
d pr
ojec
tions
in T
able
s F
and
G.
CU
RR
ENT
ENTI
RE
FAC
ILIT
Y
PRO
JEC
TED
CH
AN
GES
AS
A R
ESU
LT O
F TH
E PR
OPO
SED
PR
OJE
CT
THR
OU
GH
TH
E LA
ST Y
EAR
OF
PRO
JEC
TIO
N (C
UR
REN
T D
OLL
AR
S)
OTH
ER E
XPEC
TED
CH
AN
GES
IN
OPE
RA
TIO
NS
THR
OU
GH
TH
E LA
ST
YEA
R O
F PR
OJE
CTI
ON
(CU
RR
ENT
DO
LLA
RS)
PRO
JEC
TED
EN
TIR
E FA
CIL
ITY
THR
OU
GH
TH
E LA
ST Y
EAR
OF
PRO
JEC
TIO
N
(CU
RR
ENT
DO
LLA
RS)
*
(Lis
t gen
eral
ca
tego
ries,
add
row
s if
need
ed)
REG
ULA
R E
MPL
OYE
ES T
OTA
L16
7.3
(3.2
)
0.
0
(Lis
t gen
eral
ca
tego
ries,
add
row
s if
need
ed)
(Lis
t gen
eral
ca
tego
ries,
add
row
s if
need
ed)
(Lis
t gen
eral
ca
tego
ries,
add
row
s if
need
ed)
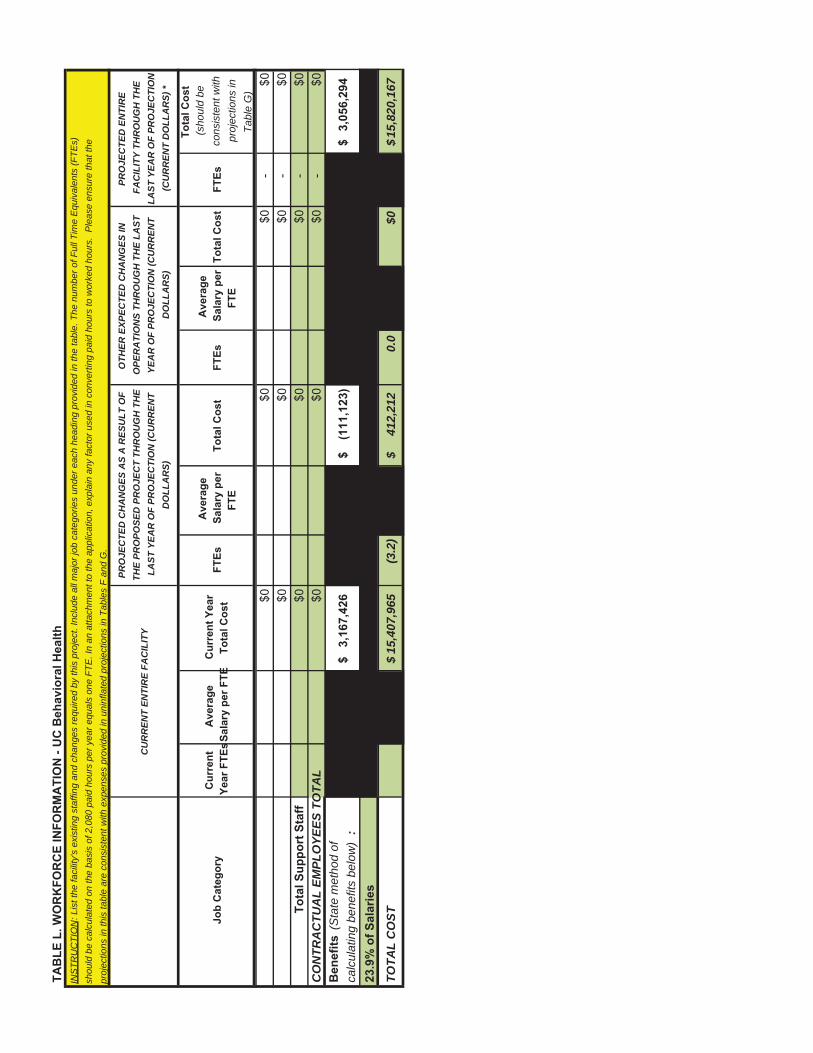
(sho
uld
be
cons
iste
nt w
ith
proj
ectio
ns in
Ta
ble
G)
INS
TRU
CTI
ON
: Lis
t the
faci
lity'
s ex
istin
g st
affin
g an
d ch
ange
s re
quire
d by
this
pro
ject
. Inc
lude
all
maj
or jo
b ca
tego
ries
unde
r eac
h he
adin
g pr
ovid
ed in
the
tabl
e. T
he n
umbe
r of F
ull T
ime
Equ
ival
ents
(FTE
s)
shou
ld b
e ca
lcul
ated
on
the
basi
s of
2,0
80 p
aid
hour
s pe
r yea
r equ
als
one
FTE
. In
an a
ttach
men
t to
the
appl
icat
ion,
exp
lain
any
fact
or u
sed
in c
onve
rting
pai
d ho
urs
to w
orke
d ho
urs.
Ple
ase
ensu
re th
at th
e pr
ojec
tions
in th
is ta
ble
are
cons
iste
nt w
ith e
xpen
ses
prov
ided
in u
ninf
late
d pr
ojec
tions
in T
able
s F
and
G.
CU
RR
ENT
ENTI
RE
FAC
ILIT
Y
PRO
JEC
TED
CH
AN
GES
AS
A R
ESU
LT O
F TH
E PR
OPO
SED
PR
OJE
CT
THR
OU
GH
TH
E LA
ST Y
EAR
OF
PRO
JEC
TIO
N (C
UR
REN
T D
OLL
AR
S)
OTH
ER E
XPEC
TED
CH
AN
GES
IN
OPE
RA
TIO
NS
THR
OU
GH
TH
E LA
ST
YEA
R O
F PR
OJE
CTI
ON
(CU
RR
ENT
DO
LLA
RS)
PRO
JEC
TED
EN
TIR
E FA
CIL
ITY
THR
OU
GH
TH
E LA
ST Y
EAR
OF
PRO
JEC
TIO
N
(CU
RR
ENT
DO
LLA
RS)
*
CO
NTR
AC
TUA
L EM
PLO
YEES
TO
TAL
(Sta
te m
etho
d of
ca
lcul
atin
g be
nefit
s be
low
):
TOTA
L C
OST
15,4
07,9
65$
(3.2
)
41
2,21
2$
0.0
$015
,820
,167
$

EXHIBIT 16

UNIVERSITY OF MARYLAND UPPER CHESAPEAKE HEALTH HOSPITAL
TITLE: INTERDISCIPLINARY DISCHARGE PLANNING: BEHAVIORAL HEALTH Page 1
APPROVED BY: Medical Director Behavioral Health Services _____________________________________
Original Date: 10/11/17
PURPOSE:To provide a collaborative, interdisciplinary approach to meet a patient’s individualized needs at the time of discharge from Behavioral Health Services that addresses continuity of care, ongoing treatment, and/or referral to other, more appropriate services.
POLICY: I. UM Upper Chesapeake Health utilizes an interdisciplinary approach to identify, discuss
and coordinate the provision of an effective discharge plan that may occur across a continuum of care, treatment or services, in accordance with the individual’s needs, strengths, preferences, and goals. All clinical disciplines are responsible for the coordination of patient care.
II. The interdisciplinary and collaborative approach uses the following key elements to planning patient care and the discharge plan. A. Integrate assessment findings in the discharge planning process. B. Develop a plan of care that includes measurable patient care goals/outcomes. C. A patient’s physical and psychosocial needs will be assessed for continuing
care.D. Planning for transfer or discharge involves the individual served, his or her
family, if applicable, and staff. E. Provide patient and family education which includes:
1. The reason he/she is being discharged 2. The anticipated need for continued care, treatment and/or referral to
more appropriate services after discharge. 3. Education on how to obtain further care, treatment or services to
meet their identified needs 4. Works with the individual and/or their support (s) to ensure
discharge instructions and appropriate next steps are clear and understood.
III. UM Upper Chesapeake Health utilizes a proactive interdisciplinary approach to coordinate the provision of a safe and appropriate discharge plan. The healthcare team strives to achieve early identification of discharge planning needs so that the
Page 2

Complexities of arranging and following through with a comprehensive plan are anticipated and managed.
IV. To optimize compliance with a patient’s post-hospital plan of care, an assessment of the patient’s actual and potential discharge planning needs shall be initiated upon admission. A plan to meet these needs shall be developed, and interventions to meet specific discharge planning goals shall be designed. The plan shall be monitored and revised as necessary throughout the patient’s hospital stay.
V. UM UCH will not recommend or show preference for one service over another and shall leave the choice of the service provider to the patient and/or his or her family.
PROCEDURE:
I. Interdisciplinary Discharge Planning Procedure A. Plan for care, treatment and service is based on:
1. Data collected from appropriate disciplines’ specific assessments. 2. Input obtained from the patient and family as indicated and acceptable
to the patient.
B. Individualized and measurable goals/outcomes 1. Disciplines, as appropriate, develop plans of care and identify
individualized goals/outcomes in collaboration with the patient, family and/or other supports.
C. Monitoring of the effectiveness of plans of care and readiness for discharge: 1. The Treatment team reviews/updates plans of care with the patient,
based on the needs and desires of the patient.2. Address additional discharge planning needs with the patient based on
change of condition/status or situation. 3. The Treatment team will review, with the patient/family, readiness for
discharge, including patient/family perspectives, aftercare services needed, and connection to additional resources and entitlements.
II. Collaborative process to coordinate care, treatment and services. A. The registered nurse assigned to care for the patient on a daily basis:
1. Reviews:a) Target date of discharge b) Planned discharge disposition c) Interdisciplinary goals and outcomes
2. Coordinates appropriate resources to meet the on-going needs of the patient
a) Makes referrals/recommendations for other discipline involvement in care
b) Participates in multidisciplinary rounding Page 3

3. Reviews Plan of Care/Discharge Plan with patient and family
B. The, RN, Social Worker, Case Manager, physician, and other disciplines collaborate on the case of the patient.
1. Topics of discussion include: a) acute case criteria b) discharge plans c) patient/family educational needs d) available resources e) peer recovery services
2. The patient and/or family, whenever possible, are included in the discussion.
III. Discharge Process
A. Discharge1. Social Work
a) Identifies payor to determine resource options for patient care needs.
b) Finalizes plans with patient/family or post-acute facility/agency. A)Assesses patient/family readiness for discharge. B) Coordinates aftercare appointments for continuing care
providers including, but not limited to, outpatient, IOP, PHP, PRP, RRP, ALF, SU Services, Peer Recovery Support, etc.When possible, in-person hand-offs will be completed with continuing care services.
C) Provides education regarding continuing care, treatment and service that the patient will need.
D)Confirms transportation, medications, etc. E) Confirms understanding of discharge plan with
patient/family. F) Verifies that required documentation is prepared and
communicated. At the time of discharge or transfer, the hospital informs other service providers who will provide care, treatment, or services to the patient the following: 1. The reason for the patient’s discharge or transfer 2. The patient’s physical and psychosocial status 3. A summary of care, treatment, medications and
services it provided to the patient 4. The patient’s progress toward goals. 5. A list of community resources or referrals made or
provided to the patient. c) Coordinates transport to home or referred resource
Page 4
Provides appropriate information regarding the care and services provided during the inpatient stay to the post-acute facility or agency.
2. Nursinga) Verifies that required test results and consults are completed.
b) Reviews the discharge instructions and medication reconciliation with the patient/caregiver and provides them with a written copy.
c) Coordinates the discharge of patient to family/caregiver, ambulance personnel and/or post-acute facility.
d) Discharge to Another Acute Facility A)Transfer arrangements B) Ambulance transport C) Notifies caregiver
3. Physiciana) Discharge Order and Summary
A)Provides necessary orders to allow for post-acute services to be coordinated
B) Assesses patient and determines if discharge is safe. C) Dictates discharge summary in a timely manner to facilitate
discharge. The discharge summary includes the reason for hospitalization, procedures performed, care, treatment, and services provided, condition and disposition at discharge, information provided to patient/family, and provisions for follow-up care.
D)Completes medication reconciliation.
b) Discharge Instructions – Discharge Routine A) Complete the EMR Discharge Routine process and sign the
home medication list. Documents included are as follows: - Discharge instructions including home diet, activity,
follow-up care, prescriptions, equipment needs, return to work/school, etc.
- Disease/condition and medication education/instructions - Home medications list
c) The physician discusses discharge plan with the patient/caregiver prior to or at the time of discharge and ensures the plan is understood.
4. High Risk Case Manager a) High Risk Case Manager may be involved with discharge
planning for patients at high risk for readmission, history of multiple Emergency Room Visits, history of noncompliance with
Page 5

discharge plan or to assist with coordination of services at discharge.
b) Patient and Family are included in the discharge plan.
IV. Transfer
A. Medical Staff and clinical team members should use available information to assess the risk of transport.
B. See “Patient Transfer” policy in Hospital/Administrative Policy Manual. C. Associated policies: DHMH COMAR 10.21.05, The Joint Commission policy CTS
06.02.01-CTS 06.02.05

EXHIBIT 17

UNIVERSITY OF MARYLAND UPPER CHESAPEAKE HEALTH HOSPITALS HOSPITAL/ADMINISTRATIVE POLICY MANUAL
TITLE: PATIENT TRANSFER Page 1 of 10
APPROVED BY: President/CEO: ________________________________________
APPROVED BY Medical Executive Committee on: 4/06, 3/11, 8/14
Original Date: 7/96 Reviewed Date: 6/98, 11/12 Revised Date: 2/00, 2/02, 3/06; 3/07, 3/09, 2/11, 12/12, 9/13, 8/14
PURPOSE: To describe methods and procedures required for transfers of patients to a higher level of care within UCH hospitals, or between UCH hospitals, from UCH hospitals to other acute care facilities, and for local diagnostic and/or treatment related services (on or off campus) unavailable to inpatients at UCH hospitals.
Other Associated Policies/Documents: Transporting Patients within the Hospital Campus. Includes on campus transfers to the UCH Physician’s Pavilions and the Ambulatory Care Center, and transporting methods and requirements for in-house transporting of patients. Acute Patient Transfer Form (This form provides structure and ensures compliance with EMTALA transfer guidelines.) EMTALA Plan
POLICY: All patient transfers will be conducted in a safe manner, and when appropriate in strict compliance with the federal Emergency Medical Treatment and Active Labor Act (EMTALA).
For all transfers the following elements are required. These tools will assist in making the appropriate arrangements for transfer, provide necessary hand off communication to and from receiving locations, and documenting the necessity of the transfer.
Acute Patient Transfer Form Ticket-to-Ride Hand-off Communication A Physician Order for the transfer
PROCEDURES:
A. Transfers Between UCH Hospitals 1. Emergencies (Medical/Surgical):
a. UCMC will accept all patients from HMH needing emergency surgery where life or limb is at risk, regardless of bed availability, as long as a surgeon accepting the case has been identified and the procedure is one UCMC is prepared to perform.
b. The patient will be transported directly to the OR or ICU (bypassing the ED). c. Admitting will be responsible for registering the patient at UCMC.

Page 2 of 10 d. Coordinating the Transfer:
1. The AC/Nursing Support Coordinator, along with the Charge Nurse, from HMH and UCMC will coordinate to arrange the transfer. The Transferring Physician is responsible for obtaining an accepting Intensivist and/or Surgeon; initiating the chain of command, as needed, to secure transfer.
e. The Acute Patient Transfer Form must be completed before transfer. f. The Receiving Intensivist at UCMC is responsible for the following:
1. the need to clear a bed in ICU to receive the surgical emergency or manage the patient in PACU
2. identifying the patient most ready to be transferred to a lower level of care to make a bed available the surgical emergency;
3. care of the surgical emergency patient until the patient’s care is assumed by surgeon. g. The UCMC Support Coordinator will assist in locating available bed space and coordinating
staff support.h. The Receiving ICU Clinical Nurse Manager (or designee) / AC is responsible for facilitating the
relocation of existing ICU patient(s) to a lower level of care as directed by the Intensivist. i. The Sending AC (or designee) will ensure that the most timely and safe transport occurs. This
includes responsibility for arranging the most appropriate mode of transport, and ensuring full communication with accepting unit.
1. The Unit will gather pertinent medical records to include any records not available in the Meditech system. This should include copies of progress notes, if the patient has had an extended length of stay, progress notes of the most recent 7 days would be sufficient.
2. The sending unit will follow the below algorithms to arrange transport:
Note: All Harford County Medical Assistance patients must have Transcare contacted as first option of transport. All ETA expectations below are in place for Transcare. If unable to meet these expectations, continue with below algorithms.
STEMI Transport Leaving HMH: a. Call Hart to Heart directly. If they cannot provide 30 minute ETA, call Express Care
Communication Center (X1234) for Express Care unit from UCMC. If they cannot provide 30 minute ETA, call 911 and request ALS transport.
b. If an EMS crew is already located in the ED, they may be requested to provide the STEMI transport prior to contacting commercial companies, however they have the right to refuse the transport until all commercial transport companies have been contacted and demonstrated inability to respond within 30 minute expectation.
c. If a nurse is required and transport company cannot provide one in a timely manner so as not to delay the transport, HMH will send a nurse to manage the medications. This nurse must have 2 years critical care experience, current ACLS, and base station training.

Page 3 of 10 NON-STEMI Priority One Transport Leaving HMH: a. Call Express Care Communication Center (X1234) to arrange transportation with a
30-45 minute ETA expectation. Order of requests should be Hart to Heart, Express Care ambulance, Harford County 911.
b. If a nurse is required and transport company cannot provide one in a timely manner so as not to delay the transport, HMH will send a nurse to manage the medications. This nurse must have 2 years critical care experience, current ACLS, and base station training.
Priority Two Transporta. Call Express Care Communication Center (X1234) to arrange transportation with a
45 to 60 minute ETA expectation.
Routine Dischargesa. Call Express Care Communication Center (X1234) to arrange routine discharge
transport with 60 to 180 minute ETA expectation.
Wheelchair Transport Services a. Call Express Care Communication Center (X1234) to pre-schedule with a minimum
24 hour notice.
3. When the transport service arrives the primary care nurse for the patient contacts the nurse on the accepting Unit to give report.
k. Delays in excess of 30 minutes from decision to transfer to acceptance by a surgeon shall trigger the Staff to initiate the Chain of Command to secure medical or administrative personnel to facilitate the transfer.
l. Delays in excess of 2 hours from decision to transfer to actual transport shall trigger the Staff to initiate the Chain of Command to secure medical or administrative personnel to facilitate the transfer.
2. Specialty Related Transfers / Non-Emergent (to include Behavioral Health (BHU), Family Birthplace, Pediatrics, or Surgical Evaluations)
a. The transferring physician is responsible for contacting the accepting unit and securing an accepting physician.
b. The accepting physician will determine the transfer location i.e. directly to the unit or the Emergency Department.
c. The Acute Patient Transfer Form must be completed before transfer.
Page 4 of 10 d. The Charge Nurse ensures all pertinent medical records are copied, to include lab and x-ray
reports and obtains MRI and CT films to be sent with the patient at the time of transfer. 1. The transferring and accepting physicians determine if ALS or BLS transport is required
and the Charge Nurse or designee contacts the transport service. If ambulance company determines a different level of transport service is required, based upon Maryland State EMS Protocols, this information is reported to the physician for documentation in the medical record. If the transporting service cannot provide timely and adequately trained personnel, UCH Nursing and or Medical Staff Administration will evaluate the efficacy of sending UCH personnel with appropriate transport training as the patient requires, and as required by Maryland Law. This nurse will have 2 years critical care experience, current ACLS, and Base Station training. They will provide care within the scope of practice of the hospital RN.
e. When the transport service arrives the primary care nurse for the patient contacts the nurse on the accepting unit to give report.
f. Psychiatric Patients - Transfers of any patient being transferred to or from a psychiatric unit will be accompanied by either:
1. an ambulance attendant or other individual of the same sex, whenever possible 2. the parent, spouse, adult sibling or adult offspring of the patient
B. Off Campus Specialty ServicesTemporary Off Campus transfers apply to inpatients transferred for diagnostic testing or medical/surgical services not offered on the campuses of Upper Chesapeake Hospitals, such as Open-MRI, TEE, ERCP, Oral Surgery, etc. 1. The Attending/Transferring Physician is responsible for writing an Order for the offsite service. A
planned daily/weekly trip during the same admission requires only one order and one form. 2. The Attending/Transferring Physician is responsible for documenting by way of the Acute Patient
Transfer Form, the necessity of the transfer, risks & benefits, and the patient’s condition. The Formmust be completed by the physician before transferring the patient.
3. Nursing staff or Unit Secretary will make scheduling arrangements for the procedure/test and direction sought as to special preparations needed such as diet restrictions or contrast prior to transfer, as well as addressing ‘current treatments in progress’ as indicated on the Acute Patient Transfer Form.
4. The transferring and accepting physicians determine if ALS or BLS transport is required and the charge nurse or designee contacts the transport service. If ambulance company determines a different level of transport service is required, based upon Maryland State EMS Protocols, this information is reported to the physician for documentation in the medical record.
5. Nursing team members prepare the patient for transport and complete a Ticket to Ride as the hand off communication to the receiving location.
a. The nurse will prepare the patient for transfer and have the medical record (including a copy of the medication reconciliation administration record) ready to accompany the patient.

Page 5 of 10
b. Team members caring for the patient will address toileting needs, medication needs and nutrition/fluid needs prior to the arrival of the transporter(s) to the unit.
c. The department housing the patient is responsible to assure that the patient is ready for transport in a timely manner.
6. When the transport service arrives the primary care nurse for the patient contacts the accepting facility to give report.
7. The receiving facility will be responsible for the patient upon arrival and is expected to utilize EMS services should the patient’s condition deteriorate and need to be emergently returned to the hospital.
C. On Campus Specialty Services (UCMC) Temporary On Campus Transfers apply to inpatients transferred to UCMC Physician Pavilions and Ambulatory Care Center1. The Attending Physician writes an Order for a medical or surgical ‘consult and treat’ for the patient.
a. If the provider/consultant requests the patient be seen in his/her private office during an inpatient admission, there will be direct physician to physician communication between the consulting and attending physicians regarding the appropriateness/medical necessity for the patient to leave the unit.
b. The Attending Physician will write the Order for the off campus transport for the intended care/treatment/service.
2. The Attending/Transferring Physician is responsible for documenting by way of the Acute Patient Transfer Form, the necessity of the transfer, risks & benefits, and the patient’s condition. The Formmust be completed by the physician before transferring the patient.
3. Nursing staff or Unit Secretary will make scheduling arrangements for the procedure/test and direction sought as to special preparations needed such as diet restrictions or contrast prior to transfer, as well as addressing ‘current treatments in progress’ as indicated on the Acute Patient Transfer Form.
4. Nursing team members prepare the patient for transport and complete a Ticket to Ride as the hand off communication to the receiving location.
a. The nurse will prepare the patient for transfer and have the medical record (including a copy of the medication reconciliation administration record) ready to accompany the patient.
b. Team members caring for the patient will address toileting needs, medication needs and nutrition/fluid needs prior to leaving the unit.
c. The department housing the patient is responsible to assure that the patient is transported in a timely manner.
5. The registered nurse or PCT will accompany the patient to the physician’s office / location with necessary equipment or Oxygen, the patient record,
a. Patients on O2 during transport must have their O2 placement and setting verified by the nurse prior to release of the patient and transport.
6. Upon return, the physician’s office will provide hand-off report occurs to the patient’s nurse and the complete Ticket to Ride.

Page 6 of 10
7. The Consulting/Treating Physician will provide a brief procedural note for any interventions that were performed or any medication administered in the office setting, for the inpatient record.
D. Transfers to External Acute Care Facility 1. The transferring physician is responsible for contacting the accepting unit and securing an accepting
physician at the receiving facility. 2. The accepting physician will determine the transfer location i.e. directly to the unit or the Emergency
Department. 3. The Acute Patient Transfer Form must be completed before transfer documenting the reason for
transfer, patient’s condition, consent, risks and benefits and other salient information contained in the form.
4. The Charge Nurse ensures all pertinent medical records are copied, to include lab and x-ray reports and obtains MRI and CT films to be sent with the patient at the time of transfer.
5. The transferring and accepting physicians determine if ALS or BLS transport is required and the charge nurse or designee contacts the transport service. If ambulance company determines a different level of transport service is required, based upon Maryland State EMS Protocols, this information is reported to the physician for documentation in the medical record.
1. If the transporting service cannot provide timely and adequately trained personnel, UCH Nursing and or Medical staff Administration will evaluate the efficacy of sending UCH personnel with appropriate training and experience as the patient requires, including 2 years critical care nursing experience, current ACLS, and Base Station training. They will provide care within the scope of the hospital RN.
6. When the transport service arrives the primary care nurse for the patient contacts the nurse / unit at the accepting facility to give report.
7. Psychiatric Patients - Transfers of any patient being transferred to or from a psychiatric unit will be accompanied by either:
a. an ambulance attendant or other individual of the same sex, whenever possible b. the parent, spouse, adult sibling or adult offspring of the patient
E. Transfer Documentation 1. An Acute Patient Transfer Form
a. The Form must be completed for all patients transferred from a UCH hospital inpatient setting to an off-site location, including on-campus services, before the patient leaves the Unit.
b. Completing this documentation is the responsibility of the physician transferring the patient, the nurse assigned to the patient's care at the time of the transfer, and a charge nurse or Administrative Coordinator.
c. An Acute Patient Transfer Form is not necessary for lateral transfers within the same hospital. This includes patient transfers to Radiation Oncology for treatment.
i. UCH Ticket to Ride will accompany patients transferred between UCH hospitals and for temporary transfers to outpatient services as defined above.
d. If the transferring physician is not physically present in the hospital, the physician portions of the Form may be completed by a PA provided that:
i. The PA documents consultation with the transferring physician on the Transfer Form.

Page 7 of 10 e. The Director/Clinical Nurse Manager/Charge Nurse of the unit caring for the patient, or the
Administrative Coordinator, must check the completeness of the Acute Patient Transfer Form,bring issues to the attention of the responsible physician or nurse for correction prior to the transfer.
f. Distribution of the Form is outlined on the Form itself. (One copy will be retained in the medical record, a second copy will be sent to the receiving facility and, for review purposes, the third copy will be forwarded as indicated and considered the transfer log.)
2. UCH Ticket to Ride will accompany patients transferred between UCH hospitals and for temporary transfers outpatient services as defined above.
3. Additional documentation regarding care provided by UCH personnel during the transfer, if any, shall be completed on the Acute Patient Transfer Form, if able or on a progress note.
F. Reasons for Transfer 1. The only reasons for which a patient may be transferred from a UCH hospital to another acute care
facility are: a. the patient's request for transfer despite being assured of the availability of care at UCH; b. the patient's need for a specialized capability not available at the transferring UCH hospital.
2. Temporary transfers to outpatient setting for diagnostic and or treatment services not readily available are permitted and procedurally defined above.
3. UCH nursing personnel shall report any proposed transfer not supported by these to their Department Director, the Administrative Coordinator or the Administrator On Call on an urgent basis, and Risk Management/Corporate Compliance.
G. Certification of Condition 1. Before any patient may be transferred from a UCH Hospital to another acute care facility the
transferring physician must make one of the following certifications in writing regarding the patient's condition:
a. the patient has been stabilized such that within a reasonable degree of medical probability, no material deterioration of the individual's condition (or the condition of a mother and her unborn child) is likely to result from the transfer;
b. the patient's condition has not stabilized, however, the patient will benefit from a higher level of care that outweighs the risks associated with transfer; or
c. the patient is in labor, however the benefits of transfer outweigh the potential risks to the mother and her unborn child(ren).
2. The physician will document this Certification in writing on the Acute Patient Transfer Form and include:
a. Risks of Transfer and b. Benefits of Care at the other facility considered in reaching this certification.
H. Patient Consent and Refusal 1. No patient will be transferred between or from a UCH hospital without the patient's or the patient's
surrogate decision maker's informed consent to the transfer, except in the case of transfer for inpatient hospitalization following involuntary commitment.

Page 8 of 10
2. Obtaining informed consent to the transfer is the responsibility of the physician recommending the transfer. Documenting the consent or the patient's involuntary commitment on the Acute Patient Transfer Form is a nursing responsibility.
3. Patient refusals to accept transfers that are recommended by a physician shall be documented in the patient record or on an Against Medical Advice Form.
4. Prior to any transfer to due to the change in a patient’s condition or need for a change in level of care within the hospitals, communication should occur between a member of the care team and the patient’s family and/or surrogate decision maker, and consent obtained as appropriate. This does not apply to transfers for operational needs, such as bed placement or availability.
I. Other Requirements 1. Continuing care - Prior to transferring a patient to another acute care facility, all necessary medical
treatment within the capabilities available at the UCH hospital will be provided in order to minimize risks of the transfer to the patient's health and, in the case of a woman in labor, the health of her unborn child.
2. Records - UCH will send receiving hospitals copies of all necessary medical records related to the individual's condition which is available at the time of transfer. Copies of additional records, such as laboratory results, which become available after the patient has left the UCH facility, will also be sent to the receiving hospital as soon as possible. These records may be sent by fax.
3. Care during transfer - UCH will assure care of the patient during the transfer by appropriate levels of life support, personnel and equipment. Determining the required level of support, personnel and equipment is the responsibility of the transferring physician. If the transporting service cannot provide timely and adequately trained personnel, UCH Nursing and or Medical staff Administration will evaluate the efficacy of sending UCH personnel with appropriate training and experience as the patient requires. This nurse will have 2 years critical care experience, current ACLS, and Base Station training. They will provide care within the scope of practice of the hospital RN.
4. Transfer orders and discharge summaries - For patients transferred from an inpatient unit to another acute care facility, the transferring physician must provide transfer orders and a discharge summary of the patient's hospitalization at UCH. Discharge summaries for transferred patients are queued to a priority status for transcription.
5. Transfers due to the failure or refusal of an on-call physician to appear - If a patient must be transferred to another hospital due to the refusal or failure of an on-call physician to appear:
a. the physician's name and address must be documented on the Acute Patient Transfer Form and,b. before the transfer takes place, the physician's department chairperson and the Administrator on
Call must be notified of the physician's refusal/failure to appear so that alternative coverage, if possible, may be obtained.
6. Improper Transfers from Other facilities - If any patient is received from another facility in a manner that suggests that the other facility may have violated the federal Emergency Medical Treatment and Active Labor Act (EMTALA), the receiving nurse must notify the Administrative Coordinator and/or the Administrator on Call on an urgent basis so that the facility can determine if it has an obligation to report the transfer to the appropriate agency.
7. Psychiatric Patients - Transfers of any patient being transferred to or from a psychiatric unit will be accompanied by either:
i. an ambulance attendant or other individual of the same sex, whenever possible ii. the parent, spouse, adult sibling or adult offspring of the patient

Page 9 of 10
J. Patient Transfer by Helicopter 1. All measures will be taken to ensure the safety of all persons/property during the arrival and departure of
helicopters at either hospital. 2. Upper Chesapeake Medical Center (UCMC):
a. Upon notification that UCMC will be receiving a helicopter, the following procedure will be followed:
i. The Emergency Department will notify the following : 1. Administrative Coordinator/Charge Nurse 2. Security (2444)
ii. The following information will be provided to the above: 1. The reason the helicopter is coming 2. The Estimated Time of Arrival (ETA)
b. A member of the nursing team may assist in the transportation of the patient to or from the helicopter, however, the placement of the patient in the helicopter will be under the direction of the Flight Paramedic.
c. The Landing Zone (LZ) is located off the Emergency Department. d. Upon notification of an inbound helicopter, a Security Officer will respond to the LZ.
i. The Security Officer will ensure the area is cleared of people and any debris that could be blown around as a result of rotor wash from the main and/or tail rotors of the aircraft.
ii. During the arrival and departure of the aircraft, Upper Chesapeake Drive will be closed to pedestrian/vehicular traffic in the area potentially affected by debris.
iii. If necessary, the Facilities Services Team may be utilized to assist.iv. The Security Officer will remain at the LZ until the helicopter has departed to ensure no
unauthorized pedestrians approach the aircraft. v. During this period, all hospital team members will turn their heads away from the helicopter
to avoid blowing debris. e. The Team Member entrance and doors adjacent to the Emergency Department will be closed
during the arrival and departure of the aircraft. f. The Security Officer will submit a Security Report outlining the circumstances any time a helicopter
arrives. If any unusual event occurs (i.e., debris is blown into a vehicle causing damage), that too will be documented in the report.
3. Harford Memorial Hospital (HMH): a. Due to its proximity to homes, there is no helipad at Harford Memorial Hospital. b. Helicopter transfers to and from Harford Memorial Hospital will be made at the helipad located at
the Maryland Army National Guard Complex, located on Old Bay Lane. c. To arrange helicopter transfer, HMH ED Charge Nurse, AC, or designee will contact Express Care
Communication Center (X1234). Express Care Communication Center will contact Hart to Heart to determine their availability to provide ground transport from helipad to hospital and return trip. If Hart to Heart is not available, Express Care Communication Center will contact Harford County 911 to arrange for transport.

Page 10 of 10
d. Upon arrival at the helipad, the Flight Paramedic will be transported to Harford Memorial by commercial ambulance, or when not available, Harford County Ambulance/Fire Personnel. Patients will be transported to and/or from the helipad by ambulance, utilizing the ambulance stretcher. The patient will be transferred to the aviation stretcher at the helipad.
e. The transfer of all patients will be done at the direction of the Flight Paramedic. f. All Harford Memorial Hospital Team Members will make every effort to assist the Fire/Ambulance
Company and flight crew.
REFERENCES: 42 U.S.C. 1395 dd 42 C.F.R. 489.24 Md. Code Ann. Health-Gen. 10-625, 10-807 and 19.308.2 COMAR 10.07.01.23