university of copenhagenhealthsciences.ku.dk/.../degree/doctoral_dissertation_bo_chawes.pdf ·...
TRANSCRIPT

U N I V E R S I T Y O F C O P E N H A G E N F A C U L T Y O F H E A L T H A N D M E D I C A L S C I E N C E S
LOW-GRADE DISEASE ACTIVITY IN EARLY LIFE PRECEDES
CHILDHOOD ASTHMA AND ALLERGY
DMSC THESIS BY
BO L. K. CHAWES, MD, PHD
Copenhagen Prospective Studies on Asthma in Childhood,
Herlev and Gentofte Hospital, University of Copenhagen;
Denmark

DMSc Thesis by Bo Chawes
1
The Faculty of Health and Medical Sciences at the University of
Copenhagen has accepted this dissertation for public defence for the
doctoral degree in medicine.
Copenhagen, 10 March 2016. Ulla Wewer, Head of Faculty
The public defence will take place 3 June 2016 at 13:00 in the large
auditorium at Gentofte Hospital,Kildegårdsvej 28, 2900 Hellerup.

DMSc Thesis by Bo Chawes
2
Papers included in the thesis The following published papers are referred to by their roman numerals
in the thesis:
I. Cord Blood 25(OH)-Vitamin D Deficiency and Childhood Asthma, Allergy and Eczema: The COPSAC2000 Birth Cohort Study. Chawes BL, Bønnelykke K, Jensen PF, Schoos AM, Heickendorff L, Bisgaard H. PLoS One. 2014 Jun 12;9(6):e99856
II. Cord blood Th2-related chemokine CCL22 levels associate with
elevated total-IgE during preschool age. Følsgaard NV, Chawes BL, Bønnelykke K, Jenmalm MC, Bisgaard H. Clin Exp Allergy. 2012 Nov;42(11):1596-603
III. Elevated eosinophil protein X in urine from healthy neonates
precedes development of atopy in the first 6 years of life. Chawes BL, Bønnelykke K, Bisgaard H. Am J Respir Crit Care Med. 2011 Sep 15;184(6):656-61
IV. Elevated exhaled nitric oxide in high-risk neonates precedes
transient early but not persistent wheeze. Chawes BL, Buchvald F, Bischoff AL, Loland L, Hermansen M, Halkjaer LB, Bønnelykke K, Bisgaard H. Am J Respir Crit Care Med. 2010 Jul 15;182(2):138-42
V. DENND1B gene variants associate with elevated exhaled nitric oxide
in healthy high-risk neonates. Chawes BL, Bischoff AL, Kreiner-Møller E, Buchvald F, Hakonarson H, Bisgaard H. Pediatr Pulmonol. 2015 Feb;50(2):109-17
VI. Neonatal bronchial hyperresponsiveness precedes acute severe viral
bronchiolitis in infants. Chawes BL, Poorisrisak P, Johnston SL, Bisgaard H. J Allergy Clin Immunol. 2012 Aug;130(2):354-61
VII. Neonates with Reduced Neonatal Lung Function Have Systemic Low-
grade Inflammation. Chawes BL, Stokholm J, Bønnelykke K, Brix S, Bisgaard H.
J Allergy Clin Immunol. 2015 Jun;135(6):1450-1456

DMSc Thesis by Bo Chawes
3
Table of Contents Abstract ............................................................... 4
Abbreviations .......................................................... 5
Introduction ........................................................... 6 The Disease Burden ................................................... 6 The Pathophysiology .................................................. 7 Exploring The Origins ................................................ 8
Objective .............................................................. 9 The COPSAC2000 Birth Cohort ........................................... 10 Neonatal Biomarkers ................................................. 12 Neonatal Lung Function .............................................. 13 Clinical Outcomes ................................................... 13
Cord Blood Biomarkes .................................................. 16 Specific and Unspecific IgE Antibodies .............................. 16 Immune Cell Subsets, Proliferation and Mediators .................... 17 Vitamin D ........................................................... 21 Other Cord Blood Biomarkers ......................................... 28
Urinary Biomarkers .................................................... 29 Inflammatory Biomarkers ............................................. 29 Metabolomic Profiling ............................................... 33
Biomarkers in Exhaled Breath .......................................... 35 FeNO ................................................................ 35 Exhaled Breath Condensate ........................................... 41 Volatile Organic Compounds (VOCs) ................................... 42
Neonatal Lung Function ................................................ 44 Bronchiolitis, Recurrent Wheeze and Asthma .......................... 44 Systemic Low-grade Inflammation ..................................... 48
Conclusions and Future Directions ..................................... 53
Summary ............................................................... 57
Danish Summary ........................................................ 60
Acknowledgements ...................................................... 64
References ............................................................ 65
Appendix A: Paper I-VII ............................................... 85

DMSc Thesis by Bo Chawes
4
Abstract Epidemiological data suggest that asthma and allergy originate in early
life, where many cases become clinically manifest and the diseases are
highly prevalent. An improved insight into the subtle anteceding
pathophysiological steps leading to penetrance of symptoms is warranted
to improve prevention and treatment.
The objective of this thesis is to investigate the presence of an early
life disease activity before symptoms emerge. The thesis is built on
seven studies from the Copenhagen Prospective Studies on Asthma in
Childhood (COPSAC2000) birth cohort examining markers of disease activity
in asymptomatic neonates prior to development of asthma and allergy-
related disorders.
First, it is explored how studies of biomarkers in cord blood, urine and
exhaled breath support the theory of a pre-symptomatic early life low-
grade disease activity. Second, it is explored how studies of neonatal
lung function and bronchial responsiveness further corroborate this
theory. Third, it is discussed how these findings could represent a
common systemic low-grade inflammation, which is part of the trajectory
to develop asthma and allergy, but possibly also several other non-
communicable welfare diseases of modernity. Last, it is discussed how
these findings could be enforced and refined by applying novel biomarker
omics technologies, which may provide a novel avenue for improved
prevention and treatment of the asthma and allergy pandemic.
DMSc Thesis by Bo Chawes
5
ABBREVIATIONS - CCL17 = C-C motif ligand 17 (previously TARC) - CCL22 = C-C motif ligand 22 (previously MDC) - COPSAC = Copenhagen Prospective Studies on Asthma in Childhood - CXCL10 = C-X-C motif ligand chemokine 10 (previously IP-10) - CXCL11 = C-X-C motif ligand chemokine 11 (previously I-TAC) - CV = Coefficient of Variation - Crs = Airway conductance - EBC = Exhaled Breath Condensate - FEF50 = Forced Expiratory Flow at 50% of - FeNO = Fractional exhaled Nitric Oxide - FEV0.5 = FVC Forced Expiratory Volume at 0.5s - FRC = Functional Residual Capacity - FVC = Forced Vital Capacity - IgE = Immunoglobulin E - IL = Interleukin - LCPUFA = Long chain polyunsaturated fatty acids - LRTI = Lower respiratory tract illness - NCD = Non-communicable diseases - NOS = Nitric oxide synthases - PCA = Principal component analysis - PD15 = The provocative dose causing a 15% drop in PtcO2 - PtcO2 = Transcutaneous oxygen saturation - ppb = Parts per billion - Rrs = Airway resistance - RSV = Respiratory syncytial virus - Th2 = T helper type 2 cell - Th17 = T helper 17 cell - Treg = T regulatory cell - TROLS = Troublesome lung symptoms - u-EPX = Urinary eosinophil protein X - u-LTC4/D4/E4 = Urinary leukotriene C4/D4/E4 - u-11β-PGF2α = Urinary 11β-prostaglandin F2α - VmaxFRC = Maximum flow at FRC - VOC = Volatile organic compounds - WHO = World Health Organization - 25(OH)-Vitamin D = 25-hydroxyvitamin D

DMSc Thesis by Bo Chawes
6
INTRODUCTION THE DISEASE BURDEN Asthma and allergy are the most common chronic diseases found in
childhood1–3. The prevalence of these diseases has increased dramatically
with a more than doubling of the prevalence in developed societies
worldwide over the recent decades4. The World Health Organization (WHO)
estimates that there are a total of 300 million asthma and allergy
sufferers globally, for most of whom the disease originated in early
childhood5. WHO assumes that the disease prevalence will continue to
rise, in particular in developing countries6, involving further 100
million patients till the year 2025 (www.WHO.int).
In westernized cultures, where the highest disease burden is seen7,
approximately half of young children will experience wheezing in
relation to respiratory infections8 and one out of five preschool
children will develop recurrent asthma-like symptoms1. At school age,
approximately 8-10% will suffer from asthma4 and 10-15% will have
symptoms characteristic of allergic rhinitis9–11. Asthma and allergy are
now the main reasons for hospitalization during childhood, chronic
medication usage, and repeated contact with health care providers, with
an associated immense direct public healthcare expenditure3 and a large
indirect societal cost due to parents’ loss of work days.
Although asthma and allergies are usually not considered severe
diseases, they have a major impact on quality of life for the affected
children and their families. Asthma and allergy in childhood can result
in a range of psychosocial impairments12,13: Children with asthma are less
physically active14 and may be unable to play like their peers and
participate in sports15. Sleep disturbances are common, which result in
daytime fatigue and negatively affect the child’s social activities and
interactions16,17. School-aged children with asthma and allergies have
increased school absenteeism18; they may experience learning impairment19
and have reduced performance at school exams during the pollen season20.
In general, living with asthma and allergy causes stress and anxiety due
to physical discomfort and limitations and due to the unpredictable
occurrence of asthma attacks and allergic reactions21.

DMSc Thesis by Bo Chawes
7
Obviously, improved preventive strategies are warranted to alleviate the
large global burden of these common childhood disorders. However,
despite decades of intensive research this clinical need has not been
met, which is presumably due to a lack of knowledge into responsible
pathophysiological mechanisms.
THE PATHOPHYSIOLOGY Asthma is a heterogeneous disease with divergent temporal presentations
of either episodic or more persistent chronic symptoms such as cough,
wheezing and breathlessness, which are typically triggered by airway
infections, physical exercise, and exposure to aeroallergens or
unspecific irritants such as tobacco smoke22. Established underlying
pathophysiological mechanisms are reversible and variable airway
obstruction, bronchial hyperresponsiveness, and airway inflammation.
The asthmatic airway inflammation is traditionally described as a T
helper type 2 cell (Th2) mediated eosinophilic inflammation with
predominance of eosinophils and mast cells. More recently, a role of T
regulatory cells (Treg) has been described in Th2 associated airway
inflammation23 and emerging evidence also pinpoints a role of T helper 17
cells (Th17) characterizing steroid non-responsive neutrophilic airway
inflammation24.
Clinical allergy manifestations can involve multiple organs such as the
skin, the respiratory system, the cardiovascular system, and the
gastrointestinal tract, and range from mild to very severe life
threatening anaphylactic reactions. The allergy-associated disease
entities are allergic rhinoconjunctivitis, food, drug and venom
allergies, asthma, and eczema, which can be partially or solely ascribed
to exposure to allergens.
The biological mechanism behind allergic reactions is archetypically
thought to be a Th2 cell polarized immune response involving the release
of a complex cascade of mediators such as interleukin-4 (IL-4), IL-5 and
IL-13, which drive immunoglobulin E (IgE) production from B cells and
recruits eosinophil granulocytes25. When the child is sensitized to
allergen specific IgE, symptoms arise upon exposure to the specific

DMSc Thesis by Bo Chawes
8
allergen in a dual early- and late-phase reaction26. The early-phase
reaction is orchestrated by degranulation of mast cells after surface
binding of allergens with release of cysteinyl leukotrienes,
prostaglandins, histamine, and cytokines, and subsequently acute
symptoms of e.g. allergic rhinoconjunctivitis27,28. The late-phase
reaction is characterized by focal influx of inflammatory cells such as
mast cells, mononuclear cells, eosinophil, basophil, and neutrophil
granulocytes27,28. The eosinophils dominate the chronic late-phase
reaction, where the release of e.g. cysteinyl leukotrienes, cationic
proteins, major basic proteins and eosinophil peroxidase sustains the
inflammatory process25.
EXPLORING THE ORIGINS Evidence suggests that asthma and allergy are programmed already in the
pre- or neonatal life as a result of complex gene–environment
interactions occurring long before symptoms develop29. However, studies
examining the pathophysiology of asthma and allergy are primarily done
in subjects with manifest clinical disease in a case-control design.
Unfortunately, this approach only adds limited insight into the
mechanisms involved in the inception of these diseases. Thus,
investigations of the underlying pathophysiological mechanisms must be
performed in earliest life in longitudinal birth cohort studies in order
to gain thorough insight and ultimately improved preventive strategies,
precise30 and personalized medical care31.

DMSc Thesis by Bo Chawes
9
OBJECTIVE The objective of this thesis is to investigate the presence of early
life disease activity prior to clinical symptoms to understand the
etiology of childhood asthma and allergy. The thesis is built on seven
studies (I-VII) originating from the Copenhagen Prospective Studies on
Asthma in Childhood (COPSAC2000) birth cohort investigating markers of
disease activity in asymptomatic neonates in relation to subsequent
development of asthma, allergy, and their associated intermediate
phenotypes.
First, it is explored how studies of biomarkers in cord blood (I-II),
urine (III) and exhaled breath (IV-V) have established the theory of an
early life low-grade disease activity preceding symptom penetrance.
Thereafter, it is explored how studies of neonatal lung function and
bronchial responsiveness (VI-VII) further corroborate this theory and
suggest that systemic low-grade inflammation is part of the trajectory
to develop asthma, allergy, and possibly several other common non-
communicable diseases (NCDs). Last, it is discussed how these findings
could be enforced and refined utilizing novel biomarker omics
technologies, which might prepare the ground for improved prevention and
treatment strategies to combat the asthma and allergy pandemic.

DMSc Thesis by Bo Chawes
10
THE COPSAC APPROACH THE COPSAC2000 BIRTH COHORT The Danish COPSAC2000 birth cohort is an at-risk, single-center
prospective study comprising 411 children born to mothers with
physician-diagnosed asthma, recruitment of whom is previously described
in details32. The children were enrolled at age 4 weeks excluding
subjects with gestational age <36 weeks, severe congenital abnormality
or systemic illness, neonatal mechanical ventilation, and lower airway
symptoms at any time prior to inclusion. Baseline characteristics of the
participating children are outlined in Table 1.
The children attended the COPSAC clinical research unit at age 4 weeks
for assessment of neonatal lung function and collection of exhaled
breath and urine for biomarker analyses. Thereafter, the children were
seen at scheduled clinical investigations at 6-monthly intervals till
age 7 years as well as at acute visits arranged upon occurrence of any
respiratory- or allergy-related symptoms33,34. At every visit a full
physical examination was performed and medical history was obtained by
parental interviews using predefined questions with closed response
categories. The medical history was supported by day-to-day diary cards
fulfilled from birth, capturing burden of troublesome lung symptoms
(TROLS) between visits. TROLS were defined as clinically significant
cough or wheeze or dyspnea explained to the parents as wheeze or
whistling sounds, breathlessness, or recurrent troublesome cough
severely affecting the well-being of the child and recorded in the diary
chart as a dichotomized daily score (yes/no)35. The pediatricians
employed at the COPSAC research unit, not the general practitioners,
were the ones solely responsible for diagnosing and treating asthma and
allergy strictly adherent to predefined validated algorithms36.

DMSc Thesis by Bo Chawes
11
Table 1. Baseline characteristics of the COPSAC2000 birth cohort.
Characteristics of the COPSAC2000 birth cohort Mothers enrolled, N 452 Number of newborns, N 411
Birthdate, range 02.08.1998 – 29.02.2001
Boys 49.4% Twins pairs 2% Sibling pairs 2% Caucasian 97% Mother's age at birth, mean (SD), years 30.0 (4.5) Father's age at birth, mean (SD), years 32.0 (5.2) Season of birth Winter 23% Spring 21% Summer 27% Fall 29% Pregnancy and birth Gestational age, mean (SD), weeks 39.9 (1.6) Birth weight, mean (SD), kg 3.52 (0.52) Birth length, mean (SD), cm 52.3 (2.3) Head circumference at 1 week, mean (SD), cm 35.2 (1.6) Apgar score at 5 min., mean (SD) 9.8 (0.6) Mode of delivery, Caesarean section 21% Exposures Older children in household 0 64% 1 24% 2 9% >2 3% Mother smoking during pregnancy, any 24% Mother’s alcohol use during pregnancy, any 26% Mother’s antibiotics use during pregnancy, any 30% Furred pets at home, any 30% Duration of solely breastfeeding, mean (SD), days 113 (62) Age at start in daycare, mean (SD), days 349 (147) Hair nicotine level at age 1 yr, mean (SD), ng/mg 3.28 (7.98) Socioeconomics Household annual income <53.000 Euro 29% 53.000 – 80.000 Euro 47% >80.000 Euro 24% Mother with university education (>3yrs) 13% Father with university education (>3yrs) 17% Mother without occupation (unemployed or student) 19% Father without occupation (unemployed or student) 7% Atopic disposition (diagnosed by doctor) Mother with asthma 100% Mother with allergic rhinitis 73% Mother with eczema 46% Father with asthma 15% Father with allergic rhinitis 30% Father with eczema 11% Genetics ORMDLR3, TT genotype (rs7216389) 29% DENND1B (rs2786098) AA 4% AC 27% CC 69% Filaggrin mutation (R501X or 2282del4 null mutation) 11%

DMSc Thesis by Bo Chawes
12
NEONATAL BIOMARKERS Cord blood: The midwives of the participating COPSAC mothers were given
written instructions to collect 14 ml cord blood by needle puncture from
the umbilical cord vein. The samples were sent by mail to the COPSAC
research unit, centrifuged for 10 min at 4300 rpm to separate serum and
plasma, and subsequently frozen at -80oC (I-II).
The chemokines C-X-C motif ligand chemokine 10 (CXCL10), CXCL11, C-C
motif ligand 17 (CCL17), and CCL22 were analysed in duplicates utilizing
an in-house multiplexed Luminex assay (II) and re-analysing samples if
the coefficient of variation (CV) was >15%37.
Serum 25-hydroxyvitamin D (25(OH)-Vitamin D) levels were measured in
duplicates by isotope dilution liquid chromatography-tandem mass
spectrometry using calibrators traceable to NIST SRM 972 (Chromsystems
Instruments and Chemicals©, Munich, Germany) (I). If both 25(OH)-Vitamin
D2 and D3 were below the detection limit, the combined value was set to
10 nmol/L38,39.
Urine was collected at the COPSAC clinic at age 4 weeks into a sterile
plastic bag adherent to the skin and stored without addition of
preservatives at -80°C. Urinary eosinophil protein X (u-EPX) level was
measured utilizing a double-antibody immunoassay (RIA - Pharmacia
Upjohn©, AB, Uppsala, Sweden) and urinary leukotriene C4/D4/E4 (u-
LTC4/D4/E4) and 11β-prostaglandin F2α (u-11β-PGF2α) by ELISA test kits (Neogen Corporation©, Lexington, USA) (III) adjusting for creatinine
excretion40.
Exhaled breath was collected at age 4 weeks into an impermeable bag (750
ml, Quintron Instrument©, Milwaukee, USA) at stable tidal breathing
after completion of neonatal lung function testing during sedation41,42.
Concentration of fractional exhaled nitric oxide (FeNO) was measured in
duplicates using an off-line technique43 with a chemiluminescence
analyzer (EcoPhysics CLD 77 AM, Duernten, Switzerland) cancelling
measurement if ambient NO exceeded 10 parts per billion (ppb) (IV-V).

DMSc Thesis by Bo Chawes
13
NEONATAL LUNG FUNCTION Forced volumes and flows were measured by spirometry at age 4 weeks from
three to five acceptable curves obtained by the raised volume rapid
thoraco-abdominal compression technique44. In brief, repeated
ventilations to a predefined mouth-pressure were applied to assure
expansion of the lung volume before an instant inflation of the “sqeeze”
jacket caused a forced exhalation where the flow was measured by a
pneumotachograph with an aircushion facemask41,42. The software identified
the Forced Vital Capacity (FVC), the Forced Expiratory Volume at 0.5 s
(FEV0.5), and the Forced Expiratory Flow at 50% of FVC (FEF50) from the
obtained volume-time curve (VI-VII).
Bronchial responsiveness to methacholine was assessed after an initial
saline inhalation by administering methacholine in quadrupling dose-
steps via a dosimeter attached to a nebulizer (SPIRA 08 TSM 133;
Respiratory Care Center; Hämeenlinna, Finland)42. The responsiveness was
determined by continuous assessment of transcutaneous oxygen saturation
(PtcO2) (TCM3; Radiometer; Copenhagen, Denmark) calculating the
provocative dose causing a 15% drop in PtcO2 (PD15) from baseline (VI-
VII).
CLINICAL OUTCOMES Recurrent wheeze at age 0-7 years was diagnosed according to a
quantitative algorithm from the lung symptom diaries reviewed by the
COPSAC pediatricians in conjunction with the parents at the scheduled or
acute visits to the research clinic. Recurrent wheeze was defined as
five diary-verified episodes of TROLS lasting at least three consecutive
days within six months or daily TROLS for four consecutive weeks33,34,45.
Children with such a symptom burden were prescribed a 3-month trial of
inhaled budesonide 200 mcg twice daily.
Asthma at age 7 years was diagnosed according to recognized
international guidelines22,46 and was based on (1) recurrent wheeze as
defined above, (2) typical asthma symptomatology such as exercise-
related symptoms, prolonged nocturnal cough, recurrent cough outside
common cold, symptoms causing wakening at night, (3) intermittent need

DMSc Thesis by Bo Chawes
14
of rescue inhaled β2-agonist, and (4) responding to a 3-month trial of inhaled corticosteroids and relapsing upon cessation33,34,45.
Acute bronchiolitis was defined irrespective of viral trigger as an
acute respiratory illness with coryza progressing over a few days to
cough, tachypnea, chest retractions and auscultative wide spread
crepitation and/or rhonchi in a child below 2 years47,48 either diagnosed
at the COPSAC clinic or from retrieved hospital records.
Allergic sensitization: Levels of specific IgE antibodies were measured
at ages ½, 1½, 4, and 6 years against a range of common inhalant
allergens (cat, dog, horse, birch, timothy grass, mugwort, house dust
mites, or molds) and food allergens (hen’s egg, cow’s milk, fish, wheat,
peanut, soybean, or shrimp) by ImmunoCAP assay (Pharmacia Diagnostics
AB, Uppsala, Sweden)49. Allergic sensitization was defined as specific
IgE levels ≥0.35kU/L50,51.
Skin prick tests were performed at the same age-points against the same
allergen panel as specific IgE assessments. A positive test was defined
as a wheal diameter ≥2 mm larger than the negative control at age ½ and 1½ year and ≥3 mm at age 4 and 6 years49.
Allergic rhinitis was diagnosed at age 7 years by the COPSAC
pediatricians based on clinical interviews (not questionnaires) of the
parents on history of symptoms in the child’s 7th year of life11,36,52.
Rhinitis was defined as bothersome sneezing or blocked or runny nose in
the past 12 months outside periods with common cold or flu53.
Figure 1 summarizes the COPSAC2000 investigator-diagnosed clinical
endpoints, intermediate phenotypes, and neonatal biomarkers and lung
function incentives utilized in the studies presented in this thesis.

DMSc Thesis by Bo Chawes
15
Figure 1. Overview and temporal collection of biomarkers and endpoints from the COPSAC2000 birth cohort presented in the thesis.
Birth
Acute symp.
0 1 6 1 2 3 4 5 6 7
Neonatal Biomarkers
Cord blood
Chemokines (CXCL10, CXCL11, CCL17, CCL22) ▼
25(OH)-Vitamin D3 ▼
Urine
u-EPX, u-LTC4/D4/E4, u-11β-PGF2α ▼
Exhaled breath
FeNO ▼
Neonatal Lung Function
Spirometry ▼
Airway reactivity, metacholine ▼
Clinical Endpoints
Respiratory symptoms, infections and eczema
Daily diary on symptoms and medication ▼
Prospective diagnosis by reserach staff ▼
Physical Examination ▼ ▼ ▼ ▼ ▼ ▼ ▼ ▼ ▼ ▼ ▼ ▼ ▼ ▼ ▼ ▼
Allergy
Skin Prick Test ▼ ▼ ▼ ▼ ▼
Specific IgE ▼ ▼ ▼ ▼ ▼
Nasal eosinophilia ▼
Allergic Rhinitis ▼ ▼
Intermediary Phenotypes
Blood
hs-CRP, IL-1β, IL-6, TNF-α, CXCL8 ▼
Total IgE ▼ ▼ ▼ ▼ ▼
Eosinophil count ▼ ▼ ▼ ▼ ▼
Lung Function
Spirometry ▼ ▼ ▼ ▼ ▼ ▼
Airway reversibility ▼ ▼ ▼ ▼ ▼ ▼
Airway reactivity, metacholine ▼
Years
<"""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""">
<"""""""""""""""""""""""""""""""""""""""""""""""""""""""""""""">
Months
COPSAC2000 Neonatal Biomarkers and Clinical Endpoints

DMSc Thesis by Bo Chawes
16
CORD BLOOD BIOMARKES SPECIFIC AND UNSPECIFIC IGE ANTIBODIES Cord blood is an easily accessible biomaterial to sample and investigate
for the presence of low-grade disease activity already at birth, which
would support the hypothesis of fetal programming of childhood asthma
and allergy54.
Priming of the developing immune system starts in utero55 and it has been
shown that the fetus is capable of producing IgE already during
gestational week 1156,57. Furthermore, it is a general belief that IgE
antibodies do not cross the placenta barrier58 and, therefore, cord blood
IgE is assumed to be of fetal origin. Based on this, a large amount of
studies have investigated the role of cord blood IgE for determining the
child’s propensity to develop asthma and allergy later in childhood.
The relevance of cord blood IgE as a marker of predisposition to
allergic disease has been suggested by studies showing association
between supposed prenatal risk factors such as allergen exposure during
pregnancy 59,60, maternal allergy status61, maternal age62, birth order63,
the child’s gender62,64 and elevated cord blood total IgE. In addition,
some studies have shown that both high total IgE61,65–67 and specific IgE68
levels in cord blood predict subsequent development of allergic
sensitization, wheezing, and asthma. These findings suggest that
elevated cord blood IgE might be a surrogate marker of allergic disease
propensity and that reduced exposure to e.g. allergenic foods such as
peanut during pregnancy could alter the child’s risk of allergy69.
However, clinical trials of avoiding either aeroallergens70 or food
allergens71,72 during pregnancy have not shown a beneficial effect on
sensitization in childhood. The reason for these disappointing results
is presumably that a large proportion of detected IgE in cord blood is
not a result of fetal de novo synthesis, but merely a reflection of
maternofetal transfer and thus maternal IgE levels.
Although some studies have proposed mechanisms for intrauterine
sensitization of the fetus73, there are several reasons to believe that
allergen specific IgE in cord blood is predominantly acquired from the

DMSc Thesis by Bo Chawes
17
mother. First, a range of recent studies have consistently shown a
linear association between maternal and fetal levels of specific IgE62,74–
76. Second, data from the COPSAC2000 cohort showed that cord blood specific
IgE was only detected when the mother had the same specific IgE, there
was a strong fingerprinting between the types of specific IgE detected
in cord blood and maternal blood, and there was no association with
paternal IgE or specific IgE level in the cord blood and at 6 months of
age77. Third, cellular studies of cord blood immune cells pinpoint that
putative T cell memory is not caused by allergen specific priming78 and
that such specific Th2 polarization is first acquired after birth79.
Cord blood unspecific IgE may also largely be a result of maternofetal
transfer through e.g. placental bleedings during pregnancy or labor, or
by contamination with maternal blood during cord venopuncture as
illustrated by increased cord blood IgA80. Another plausible mechanism is
transplacental transfer suggested by normal cord blood IgA level, but
detectable specific IgE mirroring maternal specific IgE81. However, in
some samples with elevated total IgE (>0.5IU/mL) there are no indicia of
maternal contamination, which suggests fetal IgE production and is
further supported by association with IgE levels later in childhood81.
Thus, despite the discussed restrictions and precautions, high level of
cord blood total IgE, but not specific IgE, is in some cases compatible
with a low-grade disease activity in early life before symptoms develop.
IMMUNE CELL SUBSETS, PROLIFERATION AND MEDIATORS At birth, the fetal immature immune system is thought to be dominated by
a default low-level Th2 skewed T cell response82. During early childhood,
normal T cell maturation leads to the adult-like Th1 oriented immune
constitution whereas continuation of the fetal Th2 pattern is seen in
children developing asthma and allergy83.
In line with this, a stimulation study of cord blood and peripheral
blood mononuclear cells from 31 children with house dust mite, cat
allergen, and tetanus toxoid showed a suppression of the inborn Th2
response in healthy children contrasting a persistent Th2 response in
terms of T cell proliferation and cytokine release in children
developing atopy-related disorders at age 2 years84. Another similar

DMSc Thesis by Bo Chawes
18
study showed a significantly increased proliferative response upon
stimulation of cord blood mononuclear cell with inhaled (house dust
mite) and food (betalactoglobulin and ovalbumin) allergens in children,
who developed allergic disease by one year of age compared to healthy
children85.
Treg cell responses are assumed to play a key role in such early life
skewing of the immature plastic immune system as they are capable of
inhibiting allergen-specific T cell proliferation and secretion of Th2-
type cytokines with the ability to suppress IgE production and activity
of effector cells in the allergic inflammatory cascade86. This has been
demonstrated in a study examining T cell responses to innate (lipid
A/peptidoglycan) and adaptive (Dermatophagoides pteronyssinus) immune
stimulation of cord blood from the offspring of 161 atopic and non-
atopic mothers87. In addition to a decreased secretion of the classical
Th1-type cytokine, interferon-gamma, cord blood from children of atopic
mothers showed a reduced Treg cell number, expression and function,
which may be an important step in the inception of asthma and allergies.
Furthermore, the same group showed an increased Treg cell count and an
associated decreased level of IL-5 after peptidoglycan stimulation of
cord blood cells from mothers with farming exposure during pregnancy88,
which is believed to protect against development of allergic disorders89.
Apparently, several studies of cord blood immune cell subsets and their
associated mediator release suggest a distinct response to innate and
adaptive stimuli in children with a predisposition to asthma and
allergy. However, even though these studies are intriguing and
hypothesis generating, they should be interpreted with caution as such
stimulation induces an unphysiological, exaggerated response. Thus, a
clinical follow-up on one of those studies was not able to demonstrate
an association between the perinatal immune response and allergic
diseases at 6 years of age90, and another study found no association
between cord blood reactivity to house dust mites and later development
of dust mite specific IgE79.
An approach to overcome the limitations of challenge models could be to
measure unstimulated, circulating levels of cord blood cytokines

DMSc Thesis by Bo Chawes
19
representative of T cell polarizations characteristic of manifest asthma
and allergy. However, cord blood cytokines are difficult to quantify as
the circulating levels are very low and close to the detection limit of
available assays, whereas chemokines, representing another family of
immune signaling proteins primarily with chemoatractant effects, are
more feasible to measure91. Inflammatory chemokines manage the migration
of immune cells in inflammatory processes92,93 in a distinct Th1/Th2
oriented manner as the receptors of e.g. CCL17 and CCL22 are expressed
on eosinophils and Th2 lymphocytes, whereas the receptors of e.g. CXCL10
and CXCL11 are expressed on the surface of Th1 lymphocytes and natural
killer cells74. Inflammatory chemokines are as relevant as cytokines to
examine in this context as they have been shown to express specific
Th1/Th2 immunity patterns in children with ongoing asthma, allergy and
eczema94–96. However, there is limited knowledge of cord blood chemokine
patterns preceding asthma, allergy, and related conditions94,97.
We aimed to address this gap in knowledge in our current report
investigating unstimulated levels of selected inflammatory cord blood
Th1-associated chemokines (CXCL10 and CXCL11), Th2-associated chemokines
(CCL17 and CCL22) and their ratios in 223 samples in relation to the
longitudinal development of allergic sensitization, asthma, allergic
rhinitis, and associated intermediary phenotypes during preschool age
(II). The study showed a strong positive correlation between levels of
the Th2-associated chemokine CCL22, the Th2/Th1 ratio of CCL22/CXCL10
and total IgE levels. CCL22 also showed a trend of association with
increased risk of allergic sensitization, but this was not significant
after Bonferroni correction for multiple testing (Table 2). Amongst the
very few other published reports, comparable results have been shown in
smaller cohorts with significant correlations between cord blood CCL22
and development of elevated total IgE97 and specific IgE levels94,98 in the
offspring of mixed allergic and non-allergic mothers. These and our
findings are compatible with the presence of unchallenged traces of Th2
deviation in the immature immune system of newborns developing elevated
IgE antibodies during early childhood, which is a well-established
intermediary phenotype in asthma and allergy99,100.

DMSc Thesis by Bo Chawes
20
Table 2. Associations between cord blood chemokines and development of clinical endpoints during preschool age (modified from II). Results are odds ratios with 95% CI in brackets.
Association between cord blood chemokines and clinical endpoints Total IgE Specific IgE Allergic
Rhinitis Asthma
CCL22 1.54*** [1.25-1.89]
1.35 [0.94-1.95]
0.55 [0.2-1.5]
0.75 [0.4-1.5]
CCL17 1.02 [0.90-1.15]
0.97 [0.76-1.24]
1.07 [0.61-1.9]
0.97 [0.7-1.5]
CXCL10 1,05 [0.83-1.32]
1.15 [0.76-1.72]
1.01 [0.4-2.5]
0.73 [0.4-1.3]
CXCL11 0.93 [0.80-1.10]
0.94 [0.66-1.33]
0.95 [0.4-2.1]
0.87 [0.52-1.5]
CCL22/CXCL10 1.22* [1.03-1.43]
1.08 [0.80-1.45]
0.7 [0.35-1.5]
1.1 [0.7-1.7]
CCL22/CXCL11
1.31*** [1.13-1.51]
1.23 [0.90-1.68]
0.7 [0.38-1.55]
0.97 [0.6-1.5]
*p<0.05; **p<0.01; ***p<0.001
It is unknown whether CCL22 is directly involved in the pathogenesis of
asthma and allergies or is just secondary to a general immune imbalance,
but recent findings suggest that CCL22 has a crucial role for the
recruitment of Th2 lymphocytes into the airways during allergic
inflammation101. However, we were not able to detect any association with
asthma or allergic rhinitis. The lack of association with asthma at age
6 years is not unexpected as preschool asthmatic symptoms are more
closely related to viral than allergen triggers, whereas the classical
Th2-type allergic airway inflammation is a more common feature of asthma
during school age and later in life102. In line with this, an in vivo
study of CCL22 and CCL17 levels in 56 cord blood samples showed elevated
levels in children with asthma by age 6 years, which were most
pronounced among and primarily driven by children who had comorbid
allergic sensitization97. In contrast, another study measuring the same
chemokines in 61 samples found no differences for CCL22 levels, but
increased CCL17 in children developing recurrent wheeze during the first
two years of life. However, the study was on infants enrolled in a
placebo-controlled trial of Lactobacillus reuteri during the last month
of gestation and the first year of life, which may have impacted the
findings37.

DMSc Thesis by Bo Chawes
21
The lack of association with allergic rhinitis, despite a trend of
association with sensitization, may be attributable to the relative low
number of cases in our cohort or the fact that the complex nature of the
involved immune imbalance is not sufficiently described by the selected
panel of chemokines; e.g. not encompassing markers of Treg or Th17
responses. Thus, apart from applying assays with improved sensitivity,
future cord blood mediator studies should aim to assess a broader panel
of mediators representing both Th1, Th2, Treg, and Th17 lymphocyte
subsets. Furthermore, additional information of underlying immune
patterns could be accomplished by applying pattern recognition analyses
(e.g. principal component analyses (PCA)) unbiased from preconceived
assumptions of pathophysiological pathways and grouping of mediators.
Another important issue to consider is whether maternofetal transfer of
inflammatory chemokines is apparent and thus a potential source of bias
as demonstrated for cord blood IgE studies77,81. However, inflammatory
chemokine levels are typically higher in cord blood than in maternal
blood, and maternofetal transfer may, therefore, be less important
compared to specific IgE levels, which are often 1000 times higher in
maternal blood than in cord blood81. Despite this, future studies should
investigate and subsequently adjust for maternofetal transfer as it has
been shown that inflammatory chemokines such as CCL17 are capable of
passing the blood placenta barrier103.
Still, our finding of an imbalance in unstimulated circulating levels of
cord blood Th1- and Th2-associated chemokines in children developing
elevated total IgE, underpins the presence of a low-grade disease
activity in early life. We recently demonstrated an aberrant immune
signature in the airways of neonates born to atopic vs. non-atopic
mothers suggesting that such early life immune deviation is a hereditary
trait104. However, non-heritable factors such as microflora, diet
composition, and other lifestyle associated influences are thought to
explain a large proportion of the variation in the human immune system105.
VITAMIN D Vitamin D status is highly dependent on lifestyle as production of the
biologically active form of vitamin D, 1,25(OH)2-vitamin D, depends on

DMSc Thesis by Bo Chawes
22
dietary intake and exposure to sunlight106. Only 10-20% of vitamin D is
obtained from foods such as oily fish, fortified products and dietary
supplements107, whereas the main contributor in humans is synthesis from
UVB light, which facilitates the conversion of cutaneous 7-
dehydrocholesterol to vitamin D3 that subsequently enters the
circulation. Vitamin D3 from this source, together with ingested vitamin
D, is thereafter hydroxylated in the liver to 25(OH)-vitamin D, the
storage form of vitamin D, which is converted to 1,25(OH)2-vitamin D
predominantly in the kidneys, but also in the respiratory epithelium and
in certain immune cells108.
Vitamin D serves an important function for calcium absorption and bone
homeostasis and hypovitaminosis D can lead to disorders such as rickets.
However, more recently it has been shown that vitamin D also possesses a
range of immune regulatory properties which, if distorted, may
constitute a fetal programming effect towards asthma and allergy
development109,110. This hypothesis is supported by the recent decades’
global surge of vitamin D deficiency induced by a westernized more
sedentary indoor lifestyle and decreased dietary vitamin D intake111
occurring in parallel with the arising asthma and allergy pandemic4. Of
note, vitamin D deficiency is especially prevalent among pregnant and
lactating mothers, whose vitamin D levels are highly correlated with
levels in their offspring112. In addition, some studies have shown
significant associations between polymorphisms in the vitamin D receptor
gene113 and in genes involved in vitamin D metabolism and signaling
pathways114 and increased susceptibility to childhood asthma and allergy.
Murine models of allergic asthma have revealed a general downregulating
effect of vitamin D on the inflammatory response with decreased IL-4
level in bronchoalveolar lavage fluid115. Further experimental data from
murine models have demonstrated that vitamin D through binding to the
vitamin D receptor on the surface of immune cells such as T lymphocytes
has the ability to shift the balance of Th1 and Th2-type cytokines
towards the allergic prototypic Th2 predominance116,117. This is supported
by a human cord blood study showing that vitamin D enhances interferon-
gamma production and reduces secretion of IL-4 and IL-13118 and by an

DMSc Thesis by Bo Chawes
23
additional longitudinal study showing inhibited IL-5 and IL-13
production upon house dust mite stimulation at age 6 months in infants
with sufficient cord blood vitamin D levels119. However, timing, duration
and amount of vitamin D exposure seem crucial for the direction of the
resulting immune deviation117.
Vitamin D is also believed to promote induction of Treg cells120, which
may inhibit allergen-specific T cell activation and subsequently reduce
production of specific IgE in B lymphocytes. In line with this, a recent
human cord blood study of 568 newborns showed an association between
25(OH)-vitamin D level and number of Treg cells121, and downregulated
expression of the Treg cell transcription factor FOXP3 has been
demonstrated in placental tissue of vitamin D deficient pregnant women122.
In vitro studies have suggested that vitamin D is also involved in a
range of other immunologic pathways including increased macrophage
production of the antimicrobial polypeptides cathelicidin and β-defensin123, inhibited monocyte Toll-like receptor production, and the
promotion of tolerogenic dendritic cells124. The first has important
innate immunity functions in the defense towards bacteria and may impact
the constitution of the early life airway microbiome, which has been
related to an increased propensity to asthma in childhood34. The latter,
which was demonstrated by association between increased cord blood mRNA
transcripts from antigen-presenting tolerogenic dendritic cells and
vitamin D supplementation during pregnancy among 927 European children125,
may impact the trajectory towards allergy-related illnesses.
Apart from an immune modulating effect, studies in rodents have shown
that vitamin D has important functions for differentiation of fetal type
II alveolar cells, which are important for lung maturation, structure
and surfactant production126. Cellular studies of human fetal lung tissue
have shown presence of the vitamin D receptor and confirmed that in
utero vitamin D deficiency may interfere with fetal lung cell maturation
and subsequent lung function development originating as early as 2nd
trimester of pregnancy127. Thus, there is a growing amount of indirect
evidence linking vitamin D to mechanisms with a potential role in the
inception of asthma and allergies.

DMSc Thesis by Bo Chawes
24
Further hints for a protective role of a sufficient vitamin D exposure
in utero for development of asthma and allergies in childhood have been
provided from epidemiological studies. In 2007, two articles based on
independent mother-child cohorts for the first time demonstrated an
inverse association between maternal dietary vitamin D intake during
pregnancy and risk of wheezing in the offspring128,129. The studies were
based on 1,194 mother-child pairs from Boston, MA128, and 1,212 mother-
child pairs from Aberdeen, Scotland129, and both showed a more than 60%
reduced risk of recurrent wheeze among children born to mothers with the
highest vitamin D intake. These findings were replicated in a Finnish
cohort of 1,669 mother-child pairs130, whereas a similarly sized Spanish
study observed a protective effect on respiratory infections, but no
effect on wheezing or asthma development131. Additionally, a reduced risk
of allergic rhinitis at age 5 years has been reported130, whilst a large
register based Danish study of 32,456 pregnant mothers found no
relationship between predicted maternal vitamin D status and allergic
diseases in the offspring132. However, a major limitation of these
epidemiological studies is that maternal vitamin D status is
approximated from questionnaires on food sources, which only contribute
with 10-20% of vitamin D status and are thus not a direct measure of
circulating levels available for the developing fetus.
Recent studies133–143 including our own (I) circumvent estimating fetal
exposure from maternal dietary intake by measuring 25(OH)-Vitamin D
level in cord blood. This is much more direct, but still an
approximation as cord blood levels predominantly reflect exposure during
late pregnancy. The findings from these 12 cord blood studies are
summarized in Figure 2.
DMSc Thesis by Bo Chawes
25
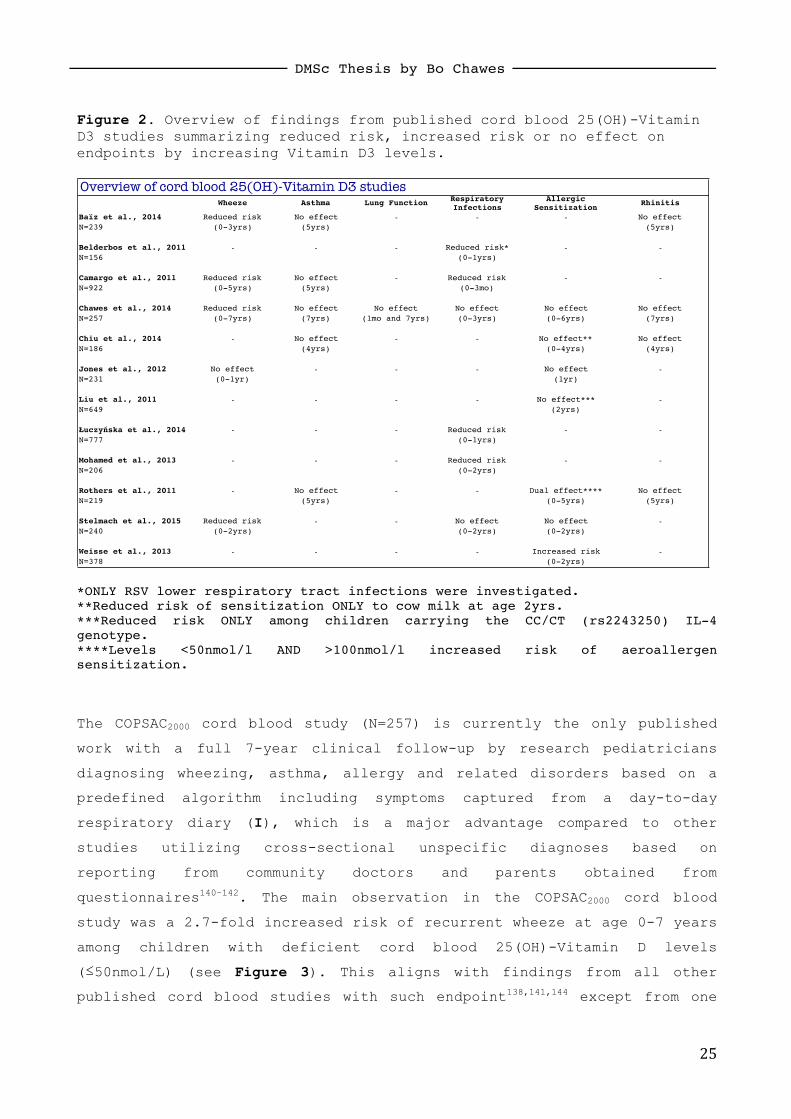
Figure 2. Overview of findings from published cord blood 25(OH)-Vitamin D3 studies summarizing reduced risk, increased risk or no effect on endpoints by increasing Vitamin D3 levels.
*ONLY RSV lower respiratory tract infections were investigated. **Reduced risk of sensitization ONLY to cow milk at age 2yrs. ***Reduced risk ONLY among children carrying the CC/CT (rs2243250) IL-4 genotype. ****Levels <50nmol/l AND >100nmol/l increased risk of aeroallergen sensitization.
The COPSAC2000 cord blood study (N=257) is currently the only published
work with a full 7-year clinical follow-up by research pediatricians
diagnosing wheezing, asthma, allergy and related disorders based on a
predefined algorithm including symptoms captured from a day-to-day
respiratory diary (I), which is a major advantage compared to other
studies utilizing cross-sectional unspecific diagnoses based on
reporting from community doctors and parents obtained from
questionnaires140–142. The main observation in the COPSAC2000 cord blood
study was a 2.7-fold increased risk of recurrent wheeze at age 0-7 years
among children with deficient cord blood 25(OH)-Vitamin D levels
(≤50nmol/L) (see Figure 3). This aligns with findings from all other
published cord blood studies with such endpoint138,141,144 except from one
Wheeze Asthma Lung Function Respiratory Infections
Allergic Sensitization
Rhinitis
Baïz et al., 2014 Reduced risk No effect ! ! ! No effect
N=239 (0-3yrs) (5yrs) (5yrs)
Belderbos et al., 2011 ! ! ! Reduced risk* ! !N=156 (0-1yrs)
Camargo et al., 2011 Reduced risk No effect ! Reduced risk ! !N=922 (0-5yrs) (5yrs) (0-3mo)
Chawes et al., 2014 Reduced risk No effect No effect No effect No effect No effect
N=257 (0-7yrs) (7yrs) (1mo and 7yrs) (0-3yrs) (0-6yrs) (7yrs)
Chiu et al., 2014 ! No effect ! ! No effect** No effect
N=186 (4yrs) (0-4yrs) (4yrs)
Jones et al., 2012 No effect ! ! ! No effect !N=231 (0-1yr) (1yr)
Liu et al., 2011 ! ! ! ! No effect*** !N=649 (2yrs)
Łuczyńska et al., 2014 ! ! ! Reduced risk ! !N=777 (0-1yrs)
Mohamed et al., 2013 ! ! ! Reduced risk ! !N=206 (0-2yrs)
Rothers et al., 2011 ! No effect ! ! Dual effect**** No effect
N=219 (5yrs) (0-5yrs) (5yrs)
Stelmach et al., 2015 Reduced risk ! ! No effect No effect !N=240 (0-2yrs) (0-2yrs) (0-2yrs)
Weisse et al., 2013 ! ! ! ! Increased risk !N=378 (0-2yrs)
Overview of cord blood 25(OH)-Vitamin D3 studies

DMSc Thesis by Bo Chawes
26
null study, which only assessed the children at 1 year of age where a
diagnosis of recurrent wheeze is quite infrequent in unselected
populations140.
Figure 3. Kaplan Meier curve showing the association between cord blood 25(OH)-Vitamin D levels and risk of recurrent wheeze (modified from I).
The increased propensity to develop recurrent wheeze in early childhood
could be ascribed to an inborn lung function deficit or
hyperresponsiveness among children with too low in utero vitamin D
exposure. This has hitherto only been investigated in our study (I),
where we were unable to demonstrate a relationship between cord blood
levels and neonatal lung function indices or lung function trajectories
in childhood, which argues against such hypothesis. It has also been
suggested that intrauterine vitamin D deficiency through immune
modulation predominantly increases frequency of respiratory
infections137,141 including RSV bronchiolitis143 and thus leads to viral-
Risk of recurrent wheeze stratified by cord blood 25(OH)-Vitamin D level.
0 1 2 3 4 5 6 70.0
0.2
0.4
0.6
0.8
1.0
Cumulated risk of recurrent wheeze
Age (years)
< 50 nmol/L
50-75 nmol/L
> 75 nmol/L
136
82
39
105
66
33
122
77
38
94
65
32
90
62
30
81
56
28
80
54
28
77
53
28
No. at risk

DMSc Thesis by Bo Chawes
27
induced transient early wheezing. However, we observed no effect on the
frequency of either upper or lower respiratory tract infections (I),
which aligns with a Polish study of 190 children followed till 2 years
of age138, but is in contrast to a large study of 777 mother-infant pairs
from Ulm, Germany136. Interestingly, the increased risk observed in the
latter study was most profound in the strata of children born to mothers
without allergy suggesting genetic effect modification136, which may
explain the contradicting results. We found no effect on current asthma
at age 7 years (I) fully comparable to the univocal null findings from
all other published cord blood studies analyzing asthma as a cross-
sectional endpoint at age 4-5 yrs133,134,141,142.
The results derived from cord blood studies on allergic sensitization
and clinical allergy manifestations are much more diverging compared to
wheezing and asthma. A recent study from Taiwan investigated inhalant
and food allergen specific IgE levels from 186 children at ages 0.5, 1,
1.5, 2, 3, and 4 years and found that low cord blood levels generally
increased the risk of food sensitization, but only significantly for
milk at age 2 yrs133. Conversely, a German study of 378 mother-child pairs
showed that higher maternal levels during pregnancy and in cord blood
conferred a higher risk for food allergy at age 2 yrs139. These disparate
findings could be explained by a non- linear relationship, which is
suggested by a study founded in the desert climate of Tucson showing a
U-shaped relationship with increased risk of aeroallergen sensitization
from both low and high cord blood 25(OH)-Vitamin D levels134. In the
COPSAC2000 cohort we did not detect an association with either inhalant or
food sensitization (I), which is in line with null reports from three
other cohorts135,138,140. However, in one of those studies vitamin D
deficiency did increase the risk of food sensitization, but only among
individuals with a certain IL-4 genotype suggesting presence of gene-
vitamin D interaction135.
The lesson learned from cord blood studies seems to be that vitamin D
deficiency is associated with increased risk of wheezing, whereas there
is no effect on asthma and no clear conclusions derived concerning
allergic sensitization. However, a major limitation of all these

DMSc Thesis by Bo Chawes
28
observational studies is that vitamin D levels are influenced by a
multitude of factors such as altitude, latitude, age at delivery, season
of birth, skin color, exposure to sun, skin coverage, time spent
outdoors, physical activity, tobacco smoke exposure, diet, supplement
use, etc.106. Although most researchers try to account for lifestyle in
vitamin D studies there is still a risk of residual confounding and the
question of causality can only be answered by randomized controlled
high-dose vitamin D supplementation trials during pregnancy (currently:
NCT00856947 and NCT00920621). Regardless of the outcomes of such studies
and the pathophysiological role(s) of vitamin D, deficient cord blood
level is an early life biomarker of disease activity prior to symptom
debut.
OTHER CORD BLOOD BIOMARKERS The dietary exposures in prenatal life are crucial for organogenesis and
fetal growth and may have a programming effect for asthma and allergy.
Apart from vitamin D, there are studies pinpointing a possible role of
other nutrients in mother’s diet such as glutathione, zinc, cobber145,
selenium146, iron147, vitamin A and E148, which may serve antioxidant and
immune modulating activities. Particularly, a pregnancy diet deprived of
n-3 polyunsaturated fatty acids (LCPUFA), which are known to influence
immune regulation, has been associated with increased risk of asthma and
allergies in the offspring149–151. However, randomized controlled trials of
n-3 LCPUFA supplementation during pregnancy have shown ambiguous
results152–154.

DMSc Thesis by Bo Chawes
29
URINARY BIOMARKERS Urine is an easy biofluid to sample from children of all ages without
the need for stressful or invasive sampling procedures. Despite this
there has been a limited search for urinary biomarkers of asthma and
allergy in children and there is a striking paucity of studies
investigating young children before symptoms emerge.
INFLAMMATORY BIOMARKERS The most commonly studied urinary biomarkers in relation to asthma and
allergy are the cationic granules proteins of eosinophil granulocytes
such as eosinophil protein X (u-EPX), leukotrienes including C4, D4, E4
(u-LTC4/D4/E4), and major metabolites of prostaglandin D2 such as 11β-prostaglandin F2α (u-11β-PGF2α).
Eosinophil cationic protein (ECP) and eosinophil protein X/ eosinophil-
derived neurotoxin155 are both members of the ribonuclease A superfamily
and contain a range of properties including neurotoxicity. They are
solely released after degranulation of activated eosinophils in the
chronic late-phase allergic reaction inducing and sustaining
inflammation and symptoms from the nose and lungs such as nasal
congestion, bronchial irritability and coughing. EPX is the only of the
4 basic eosinophil granules proteins that can be reliably detected in
urine156, it is correlated to eosinophil count in blood and
bronchoalveolar lavage fluid157 as well as serum ECP levels158 proposing a
usage as a marker of eosinophilic activation.
Leukotrienes and prostaglandins are released after degranulation of mast
cells and basophils during the immediate early-phase allergic reaction
caused by allergen induced cross-linking of surface anchored IgE-Fc
receptor (FcεRI) complexes, but they are also released from mononuclear cells, mast cells and basophil during the first hours of the late-phase
reaction27. The cysteinyl leukotrienes (C4/D4/E4) and prostaglandin D2
recruit inflammatory cell types, are potent triggers of smooth muscle
contraction in the bronchioles, increase mucus secretion, and induce
vasodilation and increased vascular permeability, which leads to the
classical acute symptoms of asthma and rhinitis such as
bronchoconstriction and rhinorrhea. u-LTC4/D4/E4 represents an established
DMSc Thesis by Bo Chawes
30
measure of total body cysteinyl leukotriene production, whereas the u-
11β-PGF2α level is a stable measure of prostaglandin D2 production by
activated mast cells159.
Clinical studies of urinary inflammatory biomarkers have predominantly
investigated: (1) differences between children with manifest asthma,
wheezing or allergy vs. healthy controls, (2) the predictive value for
persistence of disease among symptomatic children, and (3) whether
biomarker levels can predict treatment response. Quite consistently,
elevated u-EPX has been reported in children of different ages with
current allergic sensitization compared to non-sensitized controls160,161.
The longitudinal English Manchester Asthma and Allergy Study (MAAS) of
903 children found elevated u-EPX at age 3 years in children with
aeroallergen and cow’s milk sensitization, which was most pronounced for
subjects sensitized both at age 1 and 3 years160. In the COPSAC2000 study
of 369 children we also observed elevated u-EPX levels at age 6 months
among sensitized children (III). Similarly, increased u-EPX levels were
seen among Austrian schoolchildren (N=877) sensitized to common inhaled
allergens in particular for perennial allergens161. Eosinophil activity
and u-EPX is also influenced by presence of eczema (III) and depends on
eczema severity scores158, but the effect of concurrent sensitization is
stronger than the observed eczema effects and yields higher u-EPX
levels162.
The findings for wheezing and asthma are less univocal compared to
sensitization. Some studies found elevated u-EPX among wheezy
preschoolers160, whereas we did not detect differences between 6-month-old
children with current wheezing and healthy peers (III), which is in line
with another study of 1-year-old children with ongoing respiratory
symptoms163. In addition, u-EPX level measured in 105 children
hospitalized with severe wheezing during their 1st year of life was
unable to predict recurrent wheeze two years later, but high levels were
associated with skin prick test reactivity towards food and inhalant
allergens164. In populations of children >5 years of age with asthma plus
sensitization u-EPX is raised compared to healthy children156,165,166; it is
associated with declining lung function (FEV1) over time167, and levels

DMSc Thesis by Bo Chawes
31
decrease at commencement of inhaled corticosteroids156,168. Despite these
promising findings, the usage of u-EPX in clinical practice for
diagnosing and monitoring childhood asthma is significantly hampered by
low sensitivity and specificity169. Another marker of eosinophil activity,
urinary bromotyrosine, which is a marker of eosinophil-catalyzed protein
oxidation, has been suggested to reflect asthma control in children170,
but this finding still awaits replication.
Urinary leukotriene E4 (u-LTE4) was explored in 108 German 10-year-old
children showing higher levels in children diagnosed with moderate-
severe atopic asthma compared to controls171. Although excretion of u-LTE4
was correlated with lung function, there were non-significant
differences between mild steroid-naïve asthmatics vs. moderate-severe
cases and a great overlap in levels between controls and mild cases171. A
study of children <3 years found that u-LTE4 could separate non-atopic
children with RSV bronchiolitis (N=32) from controls (N=23) and reported
even higher levels among recurrent wheezers with coexisting allergic
sensitization (N=35)172. In line with this, two similarly sized studies of
preschool children observed increased u-LTE4 levels during acute viral
wheeze, which was exaggerated among children with high total-IgE levels173
and sensitization174. In contrast, a study of 1-year-old children with
atopic predisposition saw no differences in u-LTE4 in children with a
history of wheezy breathing or any other respiratory symptoms163.
Pediatric studies of u-11β-PGF2α in relation to asthma and allergy are scarce and solely related to challenges or exacerbations. A brief
communication showed that u-11β-PGF2α rose significantly in 31 children with food sensitization after a positive oral allergen challenge,
whereas there were no differences at baseline compared to non-sensitized
children (N=16)175. Another small study of 30 children demonstrated
elevated levels upon admission to hospital with an acute asthma attack,
which declined during convalescence176. Additionally, elevated u-11β-PGF2α after exercise challenge testing compared to baseline has been
demonstrated in two childhood studies with 86177 and 14 children176,
respectively, whereas rising levels after inhaled allergen challenge and
aspirin challenge are documented solely in adult settings178,179.

DMSc Thesis by Bo Chawes
32
The COPSAC2000 high-risk birth cohort study is the first and hitherto only
study investigating levels of inflammatory biomarkers in the urine of
healthy asymptomatic neonates before development of any symptoms (III).
We demonstrated that elevated u-EPX at age 4 weeks significantly
increased the risk of allergic sensitization during preschool age,
presence of nasal eosinophilia at age 6 years, and eczema development in
early childhood (Figure 4). We did not detect an association with
development of any wheezy phenotype (recurrent, episodic viral, early
transient, late onset, persistent) nor asthma at age school age, but we
did not investigate the combined endpoint of wheezing/asthma plus
sensitization. The risk of such combined endpoint might have been
increased, but as allergy is seldom the trigger of respiratory symptoms
in this age group, a possible effect of u-EPX would, therefore,
presumably be driven by the tendency to produce specific IgE antibodies
and not the wheeze propensity. Neonatal levels of u-LTC4/D4/E4 and u-11β-PGF2α were not associated with subsequent development of any of the
studied endpoints (III).
The study design investigating asymptomatic neonates is of utmost
importance to unravel whether elevated biomarkers herald onset of asthma
and allergy as levels are confounded by concurrent eczema158, respiratory
symptoms and infections, and use of anti-asthmatic drugs156. Furthermore,
the narrow age range at urine sampling, the equal gender distribution,
and collection of samples consecutively during a 3-year period accounted
for variation caused by those factors161, whereas the effect of the
circadian rhythm represents a possible residual confounder180.
Interestingly, u-EPX was a better predictor of allergy development
during preschool age than the blood eosinophil count at age 6 months
suggesting that the low-grade disease activity in neonates characterized
by elevated u-EPX is an increased degranulation liability of eosinophils
rather than increased amounts of cells. This may be caused by a
dysfunctional eosinophil granulocyte phenotype and/or genetically
determined variation in the activation of eosinophils such as deviations
in immune regulation by e.g. IL-5, IL-10, IL-13, and IFN-gamma181,182. In
support of the latter, a recent Danish twin study showed that genetic
factor accounted for 57% of the variation in serum eosinophil cationic

DMSc Thesis by Bo Chawes
33
protein levels183. Thus, in order to further explore how increased u-EPX
contributes to a trajectory to develop childhood allergies, future
studies should assess functional and regulatory aspects of eosinophils.
Figure 4. Odds ratio plot illustrating the associations between neonatal u-EPX and development of atopic endpoints (modified from III).
METABOLOMIC PROFILING Metabolomics is an omics approach to study the human systemic metabolism
applied to disentangle complex molecular foundations of diseases or
metabolic consequences of environmental effects184. The approach includes
assessment of the dynamic metabolome, which is the complete set of
small-molecule metabolites (e.g. cholesterols, triglycerides, fatty
acids, metabolic substrates, amino acids, and other signaling molecules)
in a biological sample to identify metabolic phenotypes185. Metabolomics
0.0
2.5
5.0
7.5
Odds Ratio
Any sensitization
0-6yrs
Food sensitization
0-6yrs
Aeroallergen sensitization
0-6yrs
Allergic rhinitis
6yrs
Nasal eosinophilia
6yrs
Associations between u-EPX and atopic endpoints

DMSc Thesis by Bo Chawes
34
is unique for investigating the pathophysiological transition zone
between health and disease by representing the far end from gene
expression to systemic metabolism and might, therefore, be able to
unmask an altered homeostasis in early life prior to symptom onset.
Metabolomic profiling of urine has recently been utilized in asthma
research, but studies are few, have small sample sizes, account
inconsistent for race, medication and diet, and apply different
profiling platforms. The first childhood study published in 2011 showed
that nuclear magnetic resonance (NMR) profiling of 70 metabolites in
urine was capable of separating 4-16 year-old children with stable
asthma (N=73) and asthma exacerbations (N=20) from healthy controls
(N=42)186. Subsequently, a liquid chromatography mass spectrometry (LC-MS)
study of 41 children with atopic asthma and 12 controls showed that
asthmatics had reduced excretion of metabolites correlated with immune
modulation187. Lastly, another LC-MS based study of asthmatic adolescents
reported signs of metabolic derangements associated with oxidative
stress among severe uncontrolled cases (N=35) vs. mild-moderate cases
(N=22)188. Hitherto, no negative studies have been published raising a
concern for publication bias, and no study has yet investigated the
early life metabolome in serum or urine of healthy neonates before
symptoms emerge. Currently, additional urine samples from the COPSAC
biobank collected at age one month is undergoing LC-MS metabolomic
profiling.

DMSc Thesis by Bo Chawes
35
BIOMARKERS IN EXHALED BREATH FENO Nitric oxide was first discovered in human exhaled breath in 1991189 and
was for the first time shown to be elevated in asthmatics in 1993190.
Nitric oxide is produced from L-arginine by the nitric oxide synthases
(NOS), where the inducible iNOS activity is particularly enhanced in
epithelial cells like eosinophil granulocytes during asthmatic airway
inflammation191. Therefore, FeNO is proposed as a noninvasive marker of
eosinophilic airway inflammation – an inflammometer – and elevated
levels have been reported in preschool192–194 and school-aged children195
with asthma-like symptoms as well as in children with stable asthma
prior to exacerbations196. We, therefore, hypothesized that elevated FeNO
in healthy neonates could be a marker of a low-grade disease activity
prior to symptom penetrance.
Children from approximately 5 years of age can cooperate adequately to
assessment of FeNO by an online chemiluminescence technique at a
constant exhalation flow of 50 ml/s194,197. It is also feasible and
reproducible to measure FeNO in younger children and infants, but for
such purpose an offline technique is applied where expired air is
sampled into a reservoir and subsequently connected to an analyzer193,198.
The sampling procedure in the offline technique is important in order to
obtain an accurate measurement, as FeNO is flow dependent with higher
values at lower flow rates and vice versa. Two techniques have been
proposed in infants to standardize offline FeNO measurements and account
for the flow dependency: the single-breath199 and the tidal-breathing
techniques200.
The single-breath technique is used in sedated infants in relation to
spirometric testing by the raised volume rapid thoracoabdominal
compression “squeeze” technique41, where a constant forced expiratory
flow rate during sampling can be achieved by regulating the squeeze
jacket pressure199. In the tidal-breathing technique, which can be
performed in sedated or unsedated infants, exhaled air is sampled at
repeated steady breathing cycles through a face mask attached to a two-
way valve with a resistor interposed between the valve and the bag
DMSc Thesis by Bo Chawes
36
assuring a fixed expiratory resistance200. The repeated cycles and fixed
resistance diminish breath-to-breath flow variability and limit nasal
nitric oxide contamination of the sample201. Whereas FeNO values obtained
sequentially from forced expiration maneuvers and tidal breathing have
been compared in school-aged children with allergic asthma (mean age
11.7 years, N=101)202, no previous large scale study has compared the
techniques in neonates. We, therefore, measured FeNO by both techniques
in 253 healthy neonates from the COPSAC2000 cohort and showed that levels
were highly correlated, but the single-breath technique yielded slightly
higher FeNO values than the tidal-breathing technique with increasing
differences conditional on increasing FeNO values (V). It is recommended
to refrain from lung function testing prior to FeNO measurement203, and
our data was obtained in sedated neonates after spirometry, which may
have transiently altered the FeNO values. However, we did not detect
association between FeNO and the concomitantly measured neonatal lung
function incentives (IV), which aligns with a study of 45 1-year-old
children showing no FeNO difference before and after sedation or pre vs.
post lung function testing204. Based on that, we suggest measuring FeNO in
unanaesthetized infants by the least invasive tidal-breathing technique
for future studies (IV-V).
Currently, there are quite few studies of FeNO in neonates due to the
methodological obstacles inherent to the technique and determinants of
neonatal FeNO are largely unknown. Tobacco smoking is believed to lower
FeNO in adults due to airway epithelial changes205, but the relationship
between neonatal FeNO levels and smoke exposure in pre- and early
postnatal life is not fully elucidated. One study of 2-month-old infants
(N=187) found lower FeNO in infants exposed pre- and postnatally
compared to infants exposed only postnatally and never-exposed infants206,
whilst another study of 1-month-olds (N=98) showed higher FeNO in
infants exposed postnatally207, and a third study of unselected children
aged 2 to 6 months (N=110) found no association between FeNO and
concurrent tobacco-smoke expositure208. We did not detect an association
between neonatal FeNO and maternal smoking during pregnancy or with the
child’s hair nicotine level at age 1 year (V). This negative finding may
be due to the at-risk nature of the COPSAC2000 cohort as others have

DMSc Thesis by Bo Chawes
37
demonstrated an interaction between prenatal tobacco exposure, presence
of maternal asthma and neonatal FeNO207. Previous studies have not shown
influence from father’s history of asthma or allergies198,207,208, whereas
we detected significantly elevated FeNO in infants with atopic fathers
(V); e.g. children predisposed from both their father and mother. Some
studies have shown gender differences with higher FeNO in baby boys207,209,
whereas we did not observe such difference (V), which could also be
ascribed to all mothers having a history of asthma. Data from COPSAC2000
and other cohorts have not revealed relationships between other
environmental factors such as antibiotic and acetaminophen consumption
during pregnancy, socioeconomics, older siblings, furred pet exposure,
breastfeeding or deviations in the airway microbiome (V) and neonatal
FeNO204,207.
It is plausible that neonatal FeNO is mainly an inherited trait and that
well-known childhood asthma genes such as Filaggrin210,211, ORMDL345, and
DENND1B212 influence FeNO levels in early life. Accordingly, we
investigated and discovered that children carrying the DENND1B rs2786098
C allele have elevated neonatal FeNO with increasing levels per risk
allele (V) (Figure 5). It is unknown how DENND1B gene variants may
influence nitric oxide production, but DENND1B is expressed by immune
cells such as dendritic cells, which take part in the linkage of innate
and adaptive immune responses in the process of developing tolerability
or immunity213. Thus, DENND1B gene variants may induce a skewing of the
immature immune response towards a proinflammatory state, which could
up-regulate iNOS and result in elevated FeNO levels very early in life.
Interestingly, the DENND1B single nucleotide polymorphism has also been
shown to confer a risk of other complex inflammatory diseases such as
Chrons disease214 and primary biliary cirrhosis215 indicating that the
DENND1B associated childhood asthma endotype may have communalities with
other NCDs characterized by immune dysregulation.

DMSc Thesis by Bo Chawes
38
Figure 5. Relationship between neonatal FeNO levels, DENND1B risk variants (A), and paternal atopic diseases (B) (modified from V).
Recently, a large meta-GWAS study identified that genetic variants in
rs8069176, which are associated with ORMDL3 expression, influenced FeNO
levels in children aged 5-15 years216. We found no association between
neonatal FeNO and ORMDL3 variants or Filaggrin null-mutations (V)
highlighting the dissimilar etiology of FeNO in neonatal life vs. later
in childhood. No other previous studies have investigated the
association between childhood asthma genes and neonatal FeNO levels. In
addition, genetic studies of the nitric oxide synthesis pathway in
relation to neonatal FeNO have not yet been performed, but variants in
NOS2216 (encoding iNOS) and arginases (ARG2), which compete for L-
arginine, have been shown to correlate with FeNO level in a large sample
of American children aged 6-11 years, with stronger influences in the
subset of children with asthma217. Subsequently, it was shown that DNA
methylation of iNOS contributed to FeNO level and interacted with the
degree of particulate air pollution218. Together, these and our findings
suggest that infant FeNO concentration is largely influenced by the
child’s genetic makeup and gene-environment interactions.
Studies investigating the clinical value of FeNO in early life for
distinguishing between different respiratory diseases are scarce and
typically include children within a wide age range where a diagnosis is
Neonatal FeNO stratified by DENND1B risk variants and paternal atopy
A B
CC AC AA No paternal atopy Paternal atopyn=162 n=60 n=12 n=134 n=112
0
10
20
40
60
70
50
30
0
10
20
40
60
70
50
30
FeNO
lev
el,
ppb

DMSc Thesis by Bo Chawes
39
already established and treatment initiated. Thus, a Dutch study of 218
infants aged 1 to 25 months showed that FeNO levels differentiated
between children with recurrent wheezing, cystic fibrosis,
bronchopulmonary dysplasia and healthy children, with the highest levels amongst recurrent wheezers193. Similarly, a study conducted in Switzerland
including 391 children aged 3 to 47 months showed significantly raised
FeNO in children with frequent recurrent wheezing compared to children
with recurrent cough without wheezing194.
Recently, data from the Generation R birth cohort showed that elevated
FeNO measured by the tidal breathing technique in 294 6-month-old
infants predicted development of wheezing in the 2nd year of life209. This
is an interesting finding, but it does not unravel whether subclinical
airway inflammation precedes wheezing as the same study showed that a
previous history of upper or lower respiratory tract infection was
negatively associated with FeNO, which has also been demonstrated in
other infant FeNO studies206,208,209. In addition, the initiation of inhaled
corticosteroids is also well-known to lower FeNO values219.
Currently, only two studies have examined FeNO in neonates with naïve
airways prior to any respiratory symptoms or prescription of anti-
asthmatic drugs: a study by Latzin et al198 and our study (IV). The Latzin
study prospectively monitored severe respiratory symptoms at age 0-1
year in 164 infants and showed that neonatal tidal breathing FeNO values
were positively associated with symptom development, but only among
children of atopic and/or smoking mothers198. In the COPSAC2000 at-risk
cohort, we also observed that raised neonatal FeNO preceded recurrent
wheeze (Figure 6), episodic viral wheezing and number of wheezy episodes
in the 1st year of life, but not at age 1-6 years (IV). The study is
limited by only 4% of the cohort having recurrent wheeze at age 0-1
year, whilst the additional associations with episodic viral wheeze and
number of wheezy episodes increase confidence in the findings. These
results, supported by the Latzin study198, suggest that a low-grade airway
disease process in early life characterized by elevated FeNO heralds
onset of a distinct transient wheeze endotype in at-risk children.

DMSc Thesis by Bo Chawes
40
Figure 6. Kaplan Meier curve showing the association between neonatal FeNO and risk of recurrent wheeze (modified from IV).
The identified wheeze endotype was unrelated to atopy since FeNO was not
associated with the development of increased levels of total IgE,
specific IgE or blood eosinophil count (IV). This aligns with a study
showing similar FeNO concentration in sensitized and non-sensitized
infants220 suggesting that elevated FeNO in this age group is not a marker
of eosinophilic inflammation, which is further supported by bronchial
biopsy findings revealing very few eosinophils in the airways of
symptomatic infants221. It has been proposed that congenitally small
airway dimensions predispose to an increased propensity of early
Cumulated risk of recurrent wh
eeze
Age (years)0 1 2 3 4 5 6
FeNO <= 3rd quartile
FeNO > 3rd quartile
193
60
179
52
153
47
135
45
120
40
112
39
109
38
No. at risk
0.00
0.05
0.10
0.15
0.20
0.25
Risk of recurrent wheeze stratified on neonatal FeNO

DMSc Thesis by Bo Chawes
41
transient wheezing222. However, we found no association between neonatal
FeNO and indices of infant spirometry suggesting that the wheeze
endotype defined by elevated FeNO is independent of lung function and
airway caliber. Further studies are needed to characterize the FeNO
related disease mechanism and target this particular wheezy endotype.
EXHALED BREATH CONDENSATE The discovery of FeNO as a marker of airway inflammation has led to
further research into the development of novel noninvasive techniques to
explore the composition of exhaled breath in relation to respiratory
illnesses. One of those techniques is exhaled breath condensate (EBC),
where expired air is sampled through a cooling system at tidal breathing
and subsequently condenses223. The breath condensate is believed to
constitute aerosolized airway lining fluid and contains water vapor and
microdroplets, where a large range of mediators can be determined224. A
recent systematic review summarized the findings from EBC pediatric
asthma trials225, which were purely cross-sectional in nature comparing
healthy vs. asthmatic children, different degrees of asthma severity,
and acute vs. stable asthma. In general, the EBC of asthmatic children
had lower pH and showed signs of increased oxidative stress with
elevated hydrogen peroxide (H2O2) and nitric oxide products (NOx) and
decreased antioxidant glutathione suggesting a homeostatic imbalance
between oxidants and antioxidants in the airways. Studies of more
complex EBC molecules yielded ambiguous results, but overall found
elevated eicosanoids (e.g. 8-isoprostane and cysteinyl leukotrienes) and
Th2-related cytokines (e.g. IL-4) in particular amongst children with
coexisting sensitization and during exacerbations. Although these
results seem promising several methodological issues such as cooling
temperature, collection time, condenser material, noseclip, saliva trap,
resistor, filter, dilution marker, deaeration, assay sensitivity, within
subject reproducibility, etc.223, hamper comparisons and validity of the
results. Thus, two recent longitudinal trials did not find that EBC
biomarker analysis identified children progressing from preschool
wheezing to asthma226 or predicted forthcoming asthma exacerbations227.
Additional potential biomarkers have been sought by applying metabolic
profiling to EBC – “breathomics”. An NMR based metabolomics analysis

DMSc Thesis by Bo Chawes
42
showed that the metabolic biochemical fingerprint was slightly better
than the combination of FeNO and FEV1 to discriminate between 25 children
with asthma and 11 controls (7-15 years)228. A mass spectrometry based
approach was also able to distinguish between 8-17 year-old children
with asthma (N=42) vs. controls (N=15) and between severe (N=11) vs.
non-severe asthma (N=31)229.
It is feasible and safe to collect EBC in infants as early as one month
of age230, but hitherto no longitudinal study has examined the early life
composition of EBC in relation to asthma and allergies later in
childhood. There is a need for refined EBC collection techniques in
neonates and improved and validated chemical analytical platforms.
Thereafter, EBC studies in healthy symptom-free neonates are warranted
to investigate whether a deficient antioxidant capacity, a
proinflammatory state and/or a distinct metabolic phenotype
characterizes children on a trajectory towards asthma and allergy.
VOLATILE ORGANIC COMPOUNDS (VOCS) The EBC technique is constrained to assessment of soluble volatile
components and non-volatile components in expired air, whereas an
analysis of the entire fraction of exhaled volatile organic compounds
(VOCs) requires alternative approaches. The electronic nose contains a
panel of semi-selective sensors, which upon adsorption of volatile
molecules to the surface change their electrical properties. The
physical changes of the sensors are recorded by an electronic interface
resulting in a unique breath-o-gram fingerprint of the child, but
without information on the specific VOCs recorded. Identification of the
spectrum and amount of specific VOCs involved can be determined by
sampling exhaled air in a resistance-free bag system, which is
subsequently emptied in a stainless steel sorption tube and analyzed by
thermal desorption GC-time-of-flight-MS231.
Studies of VOC profiles obtained by GC-MS in childhood wheezing and
asthma are still sparse and all originate from the same research group.
In 2010, the first published childhood study measured ~900 different
VOCs and showed that 8 selected components discriminated between 63
asthmatic and 57 healthy children with a 92% correct classification

DMSc Thesis by Bo Chawes
43
(sensitivity 89%, specificity 95%)232. Subsequently, a larger case-control
study of 3-year-old children with (N=202) and without (N=50) recurrent
wheeze also determined ~900 different VOCs and found that 28 selected
VOCs correctly classified 83% of the children (84% sensitivity, 80%
specificity)233. A small 1-year prospective study of 40 children with
asthma analyzed VOC profiles consecutively with 2-months intervals
showed that 6 VOCs discriminated between children with and without
exacerbations with 96% correct classification (sensitivity 100%,
specificity 93%)234. Finally, a prospective questionnaire-based study of
252 children aged 2-4 years, who had experienced >2 episodes of wheezing
ever, showed that 17 amongst ~3,000 determined VOCs related to oxidative
stress and lipid peroxidation, was able to correctly classify 80% of the
children as transient wheeze vs. asthma by age 6 years235. This finding is
supported by a similarly sized preschool cohort of recurrent wheezers,
where VOC profiles were shown to improve asthma prediction at school
age226.
Even fewer studies have evaluated the value of breath-o-grams obtained
by electronic noses to distinguish between healthy and asthmatic
subjects. A small study found that the electronic nose could
discriminate between young adults with (N=10) and without asthma (N=10),
but with a poor accuracy for separating mild vs. severe cases236. Only one
childhood study has been published so far, which showed that breath-o-
grams from 178 preschool children could differentiate between children
suffering acute wheeze from asymptomatic controls237.
These results seem promising and stimulating for further research into
the diagnostic and predictive value of VOC profiles in childhood
respiratory disorders, but further validation studies and consensus on
data modeling modalities are warranted. In the unselected COPSAC2010
cohort of 700 children238, we have repetitively sampled expired air for
breathomics by electronic nose and GC-MS profiling from as early as 1
week of age enabling analyses of whether a distinct smellprint
characterizes asymptomatic neonates who go on to develop wheeze and
asthma later in childhood.

DMSc Thesis by Bo Chawes
44
NEONATAL LUNG FUNCTION
Pulmonary function in infants and neonates can be determined by a range
of techniques including spirometry, plethysmography, the interrupter
technique, the forced oscillation technique, and the multiple-breath
inert gas washout technique239, among which spirometry is the best
validated and standardized test for neonates44 also permitting bronchial
challenge testing41,42. Assessments of lung function and bronchial
responsiveness in healthy neonates enable exploring whether a low-grade
disease process is active in the target organ already in the pre-
symptomatic era.
BRONCHIOLITIS, RECURRENT WHEEZE AND ASTHMA Respiratory infections with RSV, Rhinovirus and other viruses result in
common colds in most infants, while a minority develops acute
bronchiolitis, which is a leading cause of hospitalization and
respiratory insufficiency during infancy47. The wide dispersion of the
severity of clinical manifestations in response to common airway
pathogens could be due to underlying host factors such as diminished
neonatal lung function and bronchial hyperresponsiveness.
In the COPSAC2000 cohort, neonatal spirometry was performed prior to any
respiratory symptoms in 402 children and analyzed in relation to
prospectively diagnosed acute severe bronchiolitis, which was present
before age 2 years in 8.5% of the children (N=34) (VI). The prevalence
of bronchiolitis in COPSAC2000 is higher than the prevalence of 1-3%
reported in unselected populations240,241, but comparable the 7% diagnosed
cases in a cohort of 253 infants where 71% had a family history of
asthma or allergy242. Our data revealed that children experiencing acute
severe bronchiolitis compared to controls had a significant 2.5-fold
increased bronchial responsiveness to methacholine as neonates as well
as indicia of diminished baseline FEV0.5 and FEF50, which was however not
significant (Figure 7). Interestingly, the findings were largely
unchanged in post-hoc subgroup analyses restricted to RSV cases (2/3 of
the cases), non-RSV cases (1/3 of the cases), hospitalized cases (~60%),
and cases encountered before age 1 year (~64%), suggesting that a low-
grade disease activity characterized by neonatal bronchial

DMSc Thesis by Bo Chawes
45
hyperresponsiveness precedes acute severe bronchiolitis irrespective of
the viral trigger or age at infection.
Figure 7. Neonatal lung function indices and bronchial responsiveness in children developing acute bronchiolitis vs. healthy controls (modified from VI).
The association between premorbid pulmonary function in early infancy
and subsequent development of severe viral lower respiratory tract
illness (LRTI)/bronchiolitis is only investigated in a limited amount of
studies, which are heterogeneous in nature with respect to populations,
case definitions and applied lung function technique. In premature
infants born <32 weeks gestation, a small study using the single
occlusion technique showed increased airway resistance (Rrs), but no
difference in compliance (Crs) or functional residual capacity (FRC) at
36 weeks postmenstrual age in 15 of 39 premature neonates, who
experienced RSV-LRTI in their first year of life243. These findings were
sought replicated by the same research group after enrolling 159 similar
preterm infants, but Rrs was only significantly higher among severe cases
(both RSV and non-RSV), who were admitted to hospital244. An older study
of term infants reported trends of reduced maximum flow at FRC (VmaxFRC),
whilst no differences in Rrs, Crs or bronchial responsiveness to histamine
at age 5 weeks in children developing bronchiolitis before age 2 years
(N=17) compared to controls (N=236)242. However, the study had several
limitations including the use of a not volume-anchored infant spirometry
methodology, a retrospective questionnaire defined “doctor-diagnosed
bronchiolitis” at age 2 years, and very mild cases only requiring
0%
5%
10%
20%
40%
50%
30%
15%
25%
35%
45%
-3 -2 -1 0 1 2 3 4
Z-score, PD15 (PtcO2)
Neonatal lung function and acute severe bronchiolitis
0%
5%
10%
20%
40%
50%
30%
15%
25%
35%
45%
-3 -2 -1 0 1 2-4Z-score, FEV0.5 (ml)
0%
5%
10%
20%
40%
50%
30%
15%
25%
35%
45%
-3 -2 -1 0 1 2 3-4Z-score, FEF50 (ml)
A B Cp < 0.05
BronchiolitisControls

DMSc Thesis by Bo Chawes
46
hospitalization in 2/17 cases242. More recently, a Dutch study of 417
healthy 2-month-old infants measured passive respiratory mechanics by
the single occlusion technique and showed increased Rrs and decreased Crs
in RSV-positive children hospitalized with bronchiolitis (N=18) vs. non-
hospitalized RSV-positive children (N=84) representing both symptomatic
and asymptomatic cases245. Thus, in line with our study, others have shown
impaired pulmonary capacity in infants subsequently developing severe
LRTI/bronchiolitis, but our finding that bronchial hyperresponsiveness
associates with an increased propensity to severe bronchiolitis during
common viral infections still needs replication.
Apart from premorbid lung function, asthmatic heredity, environmental
risk factors, and occurrence of asthma-like symptoms in early life have
all been shown to increase the risk of subsequent RSV-hospitalization
during infancy246,247. These findings were also present in our study as
children suffering acute severe bronchiolitis were characterized by
increased prevalence of wheezy episodes before the bronchiolitis
incident, genetic and environmental asthma risk factors including male
gender, the ORMDL3 risk allele, intrauterine tobacco exposure, early age
at daycare start, and stigmata such as elevated total IgE and blood
eosinophil count (VI). Adjusting the analyses for all of these potential
confounders did not modify the association between preexisting bronchial
hyperresponsiveness and development of bronchiolitis.
The abovementioned association between asthma predisposition, asthma
comorbidity and bronchiolitis along with the increased prevalence of
bronchiolitis in asthma high-risk populations proposes that small airway
caliber and/or bronchial hyperresponsiveness is a shared phenotypic
trait in early life for both bronchiolitis and asthma. In support of a
shared topical low-grade disease activity, children of the COPSAC2000
cohort with asthma by age 7 years were also characterized by diminished
forced flow, volume, and increased bronchial responsiveness as neonates,
which progressed during childhood248. These findings argue against a
causal role of RSV, Rhinovirus and other common respiratory viruses in
the inception of childhood asthma and suggest that acute bronchiolitis

DMSc Thesis by Bo Chawes
47
during infancy may purely represent a severe early debut of asthma
persisting into school-age.
Previous studies of pre-illness infant lung function have shown that
children experiencing a wheezing LRTI in their first year of life had
preexisting lower respiratory conductance (tptef/tE) in one study (N=124)222
and lower forced expiratory flow at FRC in another study (N=97)249. In
addition, children suffering recurrent wheezing episodes in their first
1-2 years of life have been shown to have altered neonatal lung function
demonstrated in both high-risk cohorts (reduced VmaxFRC, N=69)250 and in
unselected populations (reduced VmaxFRC and airway hyperresponsiveness,
N=253)251. Furthermore, follow-up of the Tucson birth cohort study showed
that wheezing by age 3 years was still characterized by altered neonatal
tptef/tE252. Finally, data obtained from a large Norwegian cohort utilizing
infant tidal breathing flow-volume loops (N=802) and passive respiratory
mechanics (N=664) showed that lung function abnormalities at birth
increased the risk of asthma at age 10 years253. Together, evidence from
the COPSAC2000 studies and other cohorts pinpoints the existence of a low-
grade disease activity in the newborn naïve lung increasing the risk of
an exaggerated airway response to respiratory viruses and continuation
of obstructive airway symptoms throughout childhood.
Small airway caliber in early life characterized by altered forced flow
and volume is speculated to origin from anatomical differences, reduced
elastic recoil pressure of the lung, increased airway wall compliance or
subclinical inflammation222. Further narrowing of the peripheral airways
during respiratory infections in such susceptible individuals is thought
to result in exaggerated obstructive airway symptoms typical of acute
bronchiolitis as well as recurrent wheezing. It is unknown how increased
bronchial responsiveness predisposes and contributes to wheezing and
bronchiolitis; it may be driven by subclinical airway inflammation,
which in our cohort seems unrelated to elevated FeNO as neonatal FeNO
and PD15 were not associated (IV), or an increased airway sensitivity
driven by other pathophysiological mechanisms.

DMSc Thesis by Bo Chawes
48
SYSTEMIC LOW-GRADE INFLAMMATION C-reactive protein (CRP) is an acute-phase reactant with important
innate immunity functions, which is released from the liver triggered by
pro-inflammatory cytokines such as interleukin IL-6, IL-1β, and TNF-α during acute and chronic inflammatory disorders254. Newer assays with
increased sensitivity255 have enabled measurements of CRP levels in the
blood previously below the limit of detection. This biomarker is termed
high sensitivity CRP (hs-CRP) and is now well established as a sensitive
marker of systemic low-grade inflammation.
Elevated hs-CRP has been demonstrated in adult steroid naïve asthmatics
(N=22) compared to healthy peers (N=14)256 suggesting that current asthma
in adults has a low-grade systemic inflammatory component. In addition,
a cross-sectional analysis of 259 adults showed that raised hs-CRP was
associated with lower FEV1 and increased prevalence of bronchial
hyperresponsiveness257 indicating that the degree of airflow obstruction
and inflammation contributes to the systemic inflammatory process. Two
large community based prospective studies of 531258 and 2,442259 adults
confirmed the cross-sectional reciprocal relationship between hs-CRP and
lung function, but only the former showed an association between
increasing hs-CRP and declining FEV1 over a 10-year period258. Low-grade
inflammation has also been demonstrated in chronic obstructive pulmonary
disease, where transient elevations of hs-CRP were shown to predict
imminent exacerbations260.
Currently, only very few published studies have investigated the
interrelationship between low-grade inflammation and pulmonary function
outcomes in children261–263. All of these studies are cross-sectional, have
low numbers, and are conducted among children with a diagnosis of asthma
without a healthy control group. Two studies including 63 children aged
2-12 years with and without concurrent exacerbations263 and 60 steroid
naïve and steroid treated school-aged children261, respectively, showed an
inverse relationship between hs-CRP and FEV1. A third study investigating
62 school-aged children with controlled and uncontrolled asthma262 did not
detect such relationship, but reported higher hs-CRP levels in
uncontrolled cases, presumably reflecting an aggravated airway
inflammation.

DMSc Thesis by Bo Chawes
49
Thus, the existing literature on adults and children with symptomatic
asthma supports presence of low-grade systemic inflammation, which seems
dependent on the degree of disease related respiratory impairment.
However, it is unknown whether the inflammatory process predates onset
of symptoms in early life or if such systemic disease component is
related to reduced neonatal lung function. To address this gap in
knowledge, we measured serum levels of hs-CRP, the pro-inflammatory
cytokines IL-1β, IL-6, TNF-α, and the neutrophil chemotactic CXCL8 at the early age of 6 months and investigated the possible association with
neonatal lung function indices (VII). We detected a strong linear
inverse association between FEV0.5 at age 4 weeks prior to any respiratory
morbidity and hs-CRP level at age 6 months suggesting increasing grade
of systemic inflammation by diminished neonatal forced volume.
Additionally, a PCA variable reduction approach including all the
inflammatory biomarkers showed that reduced FEV0.5 was associated with an
up-regulated blood inflammatory profile. Identical trends were seen for
FEF50, whereas the PD15 values were unrelated to any biomarkers of
systemic inflammation (Table 3).
Table 3. Associations between neonatal lung function indices and low-grade inflammation at age 6 months (modified from VII). Results are β-coefficients with 95% CI in brackets. The PCA includes hs-CRP, IL-6, TNF-α and CXCL8.
Neonatal lung function and inflammatory biomarkers at age 6 months hs-CRP
PCA analysis
z-score
FEV0.5
-0.12**
[-0.21 to -0.04] -0.10*
[-0.19 to -0.01]
z-score
FEF50
-0.06 [-0.15 to 0.02]
-0.06 [-0.14 to 0.03]
Log-PD15 0.04 [-0.12 to 0.21]
0.03 [-0.14 to 0.19]
*p<0.05; **p<0.01
These unparalleled data from the COPSAC2000 cohort indicate that
diminished neonatal lung function is part of an asymptomatic low-grade
disease process with a measurable systemic component from the beginning
of life. Still, the findings should be interpreted with caution as

DMSc Thesis by Bo Chawes
50
causality cannot be determined by this study and several factors may
account for the observed relationship by affecting either the neonatal
lung function, the biomarker levels or both. Neonatal spirometry
assessments before any respiratory symptoms are unbiased from previous
or concurrent airway symptoms, whereas a recent history of asthma-like
symptoms263 or infections264, even mild viral upper respiratory
infections265, could result in elevated hs-CRP levels. Bacterial
colonization of the neonatal airway is associated with increased risk
and number of pneumonia during preschool-age266, showed a trend of
increased hs-CRP at age 6 months (VII), and could, therefore, also act
as effect modifier. In addition, the observed association could have
been affected by factors such as tobacco smoke exposure and high BMI,
which is known to negatively impact both neonatal lung function267 and hs-
CRP levels268. Finally, established genetic and environmental determinants
of childhood wheezing and asthma such as parental asthma and allergy,
male gender, socioeconomics, sibship size, breastfeeding, childcare
attendance, etc., may have influenced both the pulmonary function tests
and inflammatory biomarker levels. It is, therefore, difficult to
preclude residual confounding even though the association between FEV0.5
and hs-CRP persisted with a largely unchanged effect estimate after
adjusting for a multitude of covariates including father’s history of
asthma, eczema or allergy; maternal smoking during pregnancy; caesarean
section; gender; anthropometrics; household income; older siblings;
furred pets; neonatal bacterial airway colonization; breastfeeding
length; age at daycare start; any troublesome lung symptoms or viral
wheezing before biomarker assessment; and any infections 14 days prior
to biomarker assessment (VII). Overall, it is a major limitation that
evaluations of low-grade inflammation and neonatal lung function were
not done concomitantly as we can only speculate whether the association
concurs with an underlying disorder or reflects an inflammatory disorder
of the mother during pregnancy.
A possible explanation favoring a causal link between neonatal lung
function and hs-CRP is that diminished forced flow and volume represent
an asymptomatic airway inflammation with a detectable systemic
component. In support of this theory, cytokines and chemokines involved

DMSc Thesis by Bo Chawes
51
in asthmatic airway inflammation have been shown to eventuate
recruitment of inflammatory progenitor cells from the bone marrow as a
possible systemic immune-inflammatory pathway269. Local production of IL-6
and TNF-α triggering CRP release from the liver and/or IL-1β-related inflammasome activation in airway macrophages could also contribute to
sustained elevation of CRP and systemic low-grade inflammation270.
Persistently elevated CRP in early life may originate from or
precipitate an increased susceptibility to changes in the exposome
through its actions as a general scavenger protein with important immune
functions recognizing and eliminating bacteria and damaged human cells
through opsonization, phagocytosis, and cell-mediated cytotoxicity264. The
reduced lung function in asymptomatic neonates may, therefore, reflect
an altered airway microbiome and subclinical airway inflammation, which
precedes the debut of clinical symptoms and systemic low-grade
inflammation.
An alternative explanation to the causal link between reduced neonatal
lung function and systemic inflammation is that the conditions are
indirectly connected through shared genetic and environmental risk
factors. The observed association could be due to pleiotropic gene
effects and not the low-grade inflammation per se as some genetic loci
might confer an increased risk of both asthma and elevated CRP271.
Maternal stress and inflammation during pregnancy reflected in raised
CRP levels have been shown to increase the risk of eczema272, respiratory
infections, and recurrent wheezing in early childhood273. In addition,
elevated CRP during pregnancy is associated with fetal growth
restriction274,275, which may result in smaller lungs and airways in the
newborn and thereby explain the increased susceptibility to respiratory
infections and wheezing. The biological mechanisms may also encompass
other fetal developmental adaptions such as induction of a pro-
inflammatory state and immune dysregulation possibly influencing both
neonatal airway inflammation, the development of systemic low-grade
inflammation, wheezing and asthma276. Such inefficient immune-regulation
and sustained systemic inflammation probably arise from a complex
interplay between the newborn’s genetic makeup and the intrauterine and
early life environment, where alterations of the human microbiome277 and

DMSc Thesis by Bo Chawes
52
changing dietary habits278 are thought to play a key role. Independent of
the underlying pathobiology, our findings demonstrate the presence of a
low-grade systemic inflammatory disease process in early life, which is
associated with asymptomatic impaired neonatal lung function (VII).

DMSc Thesis by Bo Chawes
53
CONCLUSIONS AND FUTURE DIRECTIONSThe research presented in this thesis (I-VII) piggybacks on data
collected from the Danish COPSAC2000 high-risk birth cohort, which is
unique due to the extensive biobanking and lung function testing in the
neonatal period prior to any clinical signs of disease32. The series of
papers show evidence of a pre-symptomatic low-grade disease activity
measurable in several body compartments including cord blood, urine and
exhaled breath as well as reduced lung function and bronchial
hyperresponsiveness. Interestingly, we observed that each biomarker
showed distinct associations with different disease trajectories: low
cord blood 25(OH)-vitamin D was associated with development of recurrent
wheeze, but not asthma or allergies (I); high cord blood CCL22 was
associated with increased total IgE, but not specific IgE, allergic
rhinitis or asthma (II); elevated u-EPX was associated with allergic
sensitization and eczema, but not with wheezing, asthma or allergic
rhinitis (III); and elevated FeNO increased the risk of wheezing in
early childhood, but not thereafter, and was unrelated to allergic
endpoints (IV-V). These findings indicate that low-grade disease
activity before the emergence of symptoms is a generic trait in
childhood asthma and allergies, which implicates, that primary
preventive initiative should be launched in earliest life or even during
fetal life to work properly. Furthermore, our findings can be
interpreted in support of asthma and allergies constituting a
heterogeneous syndrome of several specific endotypes with distinct
clinical features, divergent underlying molecular causes, and different
prevention and treatment options279. The discovery and elucidation of such
disease endotypes is essential for improved understanding of the
biological pathways leading to symptoms, for the development of novel
therapeutics, and for achieving and practicing precision medicine30.
The presented findings are intriguing and for some part supported by
other studies, but much work remains to be done to describe the disease
processes and phenotypes characterized by the identified biomarkers and
reduced lung function. For instance, we are unable to determine whether
the bronchial hyperresponsiveness, which increases the susceptibility
for acute bronchiolitis (VI), is caused by subclinical airway

DMSc Thesis by Bo Chawes
54
inflammation. This would require concomitant assessments of neonatal
lung function and invasive bronchoscopy with biopsies and retrieval of
bronchoalveolar lavage fluid. An alternative and less invasive approach
could be sampling of epithelial lining fluid with a synthetic absorptive
matrix from the respiratory system to examine the immune-inflammatory
profile by e.g. a quantitative multiplexed assay for immune mediators280.
This can be done from the lower airways by bronchoscopic microsampling281
or noninvasive with little discomfort from the nasal mucosa104, which is
known to share both functional and immunological properties with the
bronchial mucosa26. Applying the latter methodology in our novel
unselected COPSAC2010 mother-child cohort238, we recently demonstrated an
altered topical immune response in the upper airways of asymptomatic
neonates colonized with pathogenic bacteria282, but these inflammatory
blueprints remain to be analyzed in relation to respiratory morbidity
later in childhood.
The list of biomarkers presented in this thesis is not exhaustive as
biomedical literature databases contain a wealth of articles
investigating other biomarkers in asthma and allergic disorders measured
in various body fluids. Additional biomarkers such as chitinase-like
protein YKL-40 would be interesting to exploit due to the apparent
association with airway inflammation, lung function and severe asthma
presentations in childhood283,284. However, new biomarkers are constantly
being proposed but unfortunately no noninvasive easily interpretable
clinical biomarker has yet been discovered to assesses the nature,
progression or treatment response of childhood asthma and allergy285,286.
This is predominantly due to lack of specificity and overlap between
disease subtypes as exemplified by FeNO, which is a well-established
biomarker of eosinophilic airway inflammation, but an unreliable tool
for gauging asthma control and tailoring treatment in clinical
practice219. Therefore, biomarker research has recently drifted from
quantification of single biomarkers towards more global omics approaches
combining various markers for added clinical value. Metabolomic analyses
of serum287, urine186 and EBC228 as well as VOC profiling of exhaled
breath232 are all promising advances in pediatric biomarker research,
which allow detection of suspected metabolites, unknown metabolites and

DMSc Thesis by Bo Chawes
55
biomarkers, and may ultimately unravel novel disease-related pathways.
Applying these technologies on biobank material collected from carefully
characterized longitudinal birth cohorts such as the COPSAC200032 and
COPSAC2010238 would facilitate a broader understanding of the early life
low-grade disease activity preceding clinical symptoms, which are
proposed in this thesis. In addition to sophisticated metabolomic
fingerprints, multiple data layers including genomics, epigenomics,
transcriptomics, proteomics, and deep clinical phenotyping data should
be integrated in a systems biology multiparametric approach in order to
disentangle the origins of asthma and allergies.
Furthermore, the discovery that children with reduced neonatal lung
function are characterized by systemic low-grade inflammation very early
in life (VII) holds the promise that exploring the origins of asthma and
allergy may also shed light on disease mechanisms involved in other NCDs
of modern times. The chronic NCDs encompass disorders such as
cardiovascular diseases, metabolic diseases, and chronic lung diseases,
which have been shown to rise in parallel in prevalence among
westernized cultures during the previous decades288. Recent studies
pinpoint that chronic low-grade inflammation is a common nominator of
virtually all NCDs29, which is reflected by elevated levels of hs-CRP in
highly endemic societies289 and accompanying the specific disorders like
cardiovascular disease290, diabetes mellitus291, chronic obstructive
pulmonary disease260, and asthma256. In our study (VII), we demonstrated
that such common immune distortion initiating a vicious cycle of
sustained low-grade inflammation including elevated hs-CRP is already
prevalent in the early life course before any clinical symptoms among
children at increased risk of asthma and allergies, which are the
earliest debuting NCDs292. Strategies to restore the early life
immunological health status may, therefore, not only have the capacity
to prevent development of childhood asthma and allergy, but could
potentially also prevent a range of other frequent NCDs debuting later
in life. A greater understanding of the low-grade disease activity
occurring before symptoms are established is the only solid step stone
for conducting successful randomized controlled trials to promote immune

DMSc Thesis by Bo Chawes
56
health during pregnancy and early childhood to combat the major global
challenge of asthma, allergy, and other NCDs.

DMSc Thesis by Bo Chawes
57
SUMMARY Asthma and allergies are today the most common chronic diseases in
children and the leading causes of school absences, chronic medication
usage, emergency department visits and hospitalizations, which affect
all members of the family and represent a significant societal and
scientific challenge. These highly prevalent disorders are thought to
originate from immune distortion in early childhood, but the etiology
and heterogeneity of the disease mechanisms are not understood, which
hampers preventive initiatives and makes treatment inadequate.
The objective of this thesis is to investigate the presence of an early
life disease activity prior to clinical symptoms to understand the
anteceding pathophysiological steps towards childhood asthma and
allergy. The thesis is built on seven studies from the Copenhagen
Prospective Studies on Asthma in Childhood (COPSAC2000) birth cohort
examining biomarkers of disease activity in 411 asymptomatic neonates in
cord blood (I-II), urine (III), exhaled breath (IV-V) and infant lung
function (VI-VII) in relation to the subsequent development of asthma
and allergy during the first 7 years of life.
In papers I-II, we studied cord blood chemokines and 25(OH)-vitamin D,
which represent a proxy of the inborn immature immune system, the
intrauterine milieu, and the maternal immune health during pregnancy.
High levels of the Th2-related chemokine CCL22 and high CCL22/CXCL11
ratio were positively correlated with total IgE level during preschool
age (II). This suggests an inborn Th2 skewing of the immune system in
healthy newborns subsequently developing elevated total IgE antibodies,
which is considered to increase the risk of asthma and allergies later
in life. Additionally, deficient cord blood 25(OH)-vitamin D levels were
associated with a 2.7-fold increased risk of recurrent wheeze at age 0-7
years (I). Together, these findings support the concept that early life
immune programming in the pre-symptomatic era plays an essential role
for promotion of or protection against asthma and allergies. Therefore,
preventive initiatives to restore immune health, such as vitamin D
supplementation, should be directed to the fetus and the earliest
postnatal life.
DMSc Thesis by Bo Chawes
58
The eosinophil granulocyte has a major role in the allergic inflammatory
cascade and eosinophilia is considered a hallmark of many allergic
phenotypes. In paper III, we examined neonatal urinary biomarkers
including eosinophil protein X (u-EPX), which is contained in the
eosinophil granules. Elevated u-EPX in asymptomatic neonates was
associated with development of allergic sensitization and nasal
eosinophilia, but not with wheezing or asthma (III). These findings
suggest the presence of an ongoing low-grade disease process in early
life characterized by eosinophil activation prior to appearance of
allergy-related conditions.
In papers IV-V, we investigated perinatal and genetic predictors of
neonatal fractional exhaled nitric oxide (FeNO) and the relationship
between neonatal FeNO and wheezing later in childhood. The a priori
selected determinants encompassed asthma genetic risk variants,
anthropometrics, demographics, socioeconomics, parental asthma and
allergy, maternal smoking, paracetamol and antibiotic usage during
pregnancy, and neonatal bacterial airway colonization. Among those, only
the DENND1B risk allele and paternal history of asthma and allergy were
associated with increased FeNO values (V) suggesting that raised FeNO in
neonatal life is primarily an inherited trait. The neonatal FeNO levels
were widely dispersed (1-67ppb) and children with values in the upper
quartile were at increased risk of recurrent wheezing in early
childhood, but not persistent wheezing, reduced lung function or
allergy-related endpoints (IV). This suggests that elevated neonatal
FeNO represents an early asymptomatic low-grade disease process other
than congenitally small airway caliber contributing to a transient
wheezing phenotype.
Reduced lung function in neonates is associated with wheezing and asthma
proneness, but it is unknown if such host factor also confers a risk of
acute bronchiolitis, which is considered an index event of asthma
persisting into school age. In paper VI, we investigated neonatal forced
flow, volume, and responsiveness to methacholine in relation to
occurrence of acute severe bronchiolitis at age 0-2 years. Children
developing bronchiolitis had a 2.5-fold increased bronchial

DMSc Thesis by Bo Chawes
59
responsiveness as neonates (VI) suggesting a preexisting joint
propensity of the airways to react adversely to common respiratory
viruses and to develop asthma. This finding proposes airway
hyperresponsiveness as yet another marker of low-grade disease activity
among asymptomatic neonates on a trajectory towards childhood asthma.
In paper VII, we examined whether neonates with impaired pulmonary
capacity also had signs of systemic inflammation prior to clinical
symptoms. Reduced FEV0.5 was significantly associated with elevated serum
hs-CRP and other blood inflammatory markers (VII) suggesting presence of
systemic low-grade inflammation from the beginning of life. Chronic low-
grade inflammation is a common nominator of virtually all the major non-
communicable welfare diseases (NCDs) of modernity whereof asthma and
allergies are the earliest debuting disorders. The novel finding of
systemic low-grade inflammation among neonates at increased risk of
asthma and allergy, therefore, implies that exploring the origins of
asthma and allergy may also unravel disease mechanisms involved in other
NCDs.
In conclusion, the series of papers presented in this thesis (I-VII)
evidence the presence of a pre-symptomatic disease process measurable in
several body compartments, which supports the notion of low-grade
disease activity in early life as a generic trait among neonates
developing asthma and allergy. This hypothesis piggybacking on single
biomarker assessments could be enforced and refined by applying novel
global omics approaches. In particular, metabolomic analyses of serum,
urine, and airway lining fluid from neonates as well as neonatal VOC
profiling of exhaled breath may facilitate a broader understanding of
the early low-grade disease activity preceding clinical symptoms.
Disentangling the introductory pathophysiological mechanisms and
underlying endotypes of disease is paramount for generating successful
preventive measures to alleviate the major global burden of asthma,
allergy, and other NCDs of modern time.

DMSc Thesis by Bo Chawes
60
DANISH SUMMARYAstma og allergi er i dag de hyppigste sygdomme i barndommen, de
hyppigste årsager til skolefravær, kronisk medicinering, lægekontakter
og indlæggelser. Sygdommene påvirker såvel barnet som alle øvrige
familiemedlemmer og repræsenterer en stor samfundsmæssig og
videnskabelig udfordring. Disse hyppigt forekommende sygdomme opstår
formodentlig på bagrund af en skævvridning af den immunologisk udvikling
i den tidlige barndom, men ætiologien og de heterogene sygdomsmekanismer
er ufuldstændigt forstået, hvilket kompromitterer sufficient
forebyggelse og behandling.
Formålet med denne afhandling er at undersøge tilstedeværelsen af
sygdomsaktivitet tidligt i livet, før kliniske symptomer udvikles, for
at kunne forstå de indledende patofysiologiske mekanismer, der fører til
astma og allergi i barndommen. Afhandlingen er baseret på syv studier
fra Copenhagen Prospective Studies on Asthma in Childhood (COPSAC2000)
fødselskohorten, der alle omhandler analyser af sygdomsaktivitet hos 411
raske neonatale børn i navlesnorsblod (I-II), urin (III), udåndingsluft
(IV-V) samt neonatal lungefunktion (VI-VII) i relation til udvikling af
astma og allergi i førskolealderen.
I I-II undersøgte vi niveauet af navlesnors chemokiner og 25(OH)-vitamin
D, som er et mål for det medfødte immature immunsystem, det intrauterine
miljø, samt moderens immunologiske helbred under graviditeten. Høje
niveauer af det Th2-relaterede chemokin CCL22 og høj ratio af
CCL22/CXCL11 var positivt korreleret med niveauet af total IgE i
førskolealderen (II). Dette antyder en medfødt Th2 skævvridning af
immunsystemet hos raske nyfødte, der udvikler forhøjede total IgE
antistoffer, som antages at øge risikoen for astma og allergi senere i
livet. Ligeledes observerede vi, at for lavt niveau af 25(OH)-vitamin D
i navlesnorsblodet var associeret med en 2,7-fold forøget risiko for at
udvikle tilbagevendende astmalignende symptomer i alderen 0-7 år (I).
Sammenholdt støtter disse fund det koncept, at immunprogrammering
tidligt i livet i den præsymptomatiske æra spiller en afgørende rolle
for, om barnet får en forøget eller formindsket risiko for at udvikle
astma og allergi. Dette betyder, at forebyggende tiltag, der sigter mod

DMSc Thesis by Bo Chawes
61
at forbedre immunstatus, såsom vitamin D supplement, skal initieres
allerede i graviditeten og den tidligste barndom.
Den eosinofile granulocyt har en afgørende rolle i den allergiske
inflammatoriske kaskade, og eosinofili er et vigtigt karakteristika ved
flere allergiske fænotyper. I III undersøgte vi neonatale biomarkører i
urinen inkluderende eosinofil protein X (u-EPX), der findes i de
eosinofile granula. Forhøjet u-EPX hos de asymptomatiske neonatale børn
var associeret med udvikling af allergisk sensibilisering og nasal
eosinofili, men ikke med astmalignende symptomer eller astma (III).
Disse fund indikerer tilstedeværelsen af en igangværende lavgrads
sygdomsproces karakteriseret ved eosinofil aktivering ganske tidligt i
livet, før der udvikles tegn på allergisk sygdom.
I IV-V analyserede vi perinatale og genetiske prædiktorer for niveauet
af fraktioneret ekshaleret nitrogen oxid (FeNO) hos neonatale børn og
sammenhængen mellem neonatal FeNO og astmalignende symptomer senere i
barndommen. De a priori udvalgte prædiktorer var velkendte astma risiko
genvarianter, antropometri, demografi, socioøkonomi, forældrenes astma,
allergi og eksem status, mors rygning samt forbrug af paracetamol og
antibiotika i graviditeten, og neonatal bakteriel kolonisering af
luftvejene. Blandt disse prædiktorer var det kun risiko allellen DENND1B
og faderens sygdomshistorik, der var associeret med forøget niveau af
FeNO (V), hvilket antyder, at forhøjet FeNO hos neonatale primært er et
medfødt karaktertræk. Der var stor spændvidde på de målte neonatale FeNO
niveauer (1-67 ppb), hvor børn med niveauer i den øvre kvartil havde en
øget risiko for at udvikle astmalignende symptomer i det første leveår,
men ikke mere persisterende symptomer, nedsat lungefunktion eller
allergirelaterede tilstande (IV). Dette antyder, at forhøjet neonatal
FeNO niveau repræsenterer en tidlig asymptomatisk lavgrads sygdomsproces
forskellig fra medfødt nedsat lungefunktion, der har betydning for
udvikling af en fænotype karakteriseret ved tidlige forbigående
astmalignende symptomer.
Nedsat neonatal lungefunktion er associeret med en øget risiko for
astmalignende symptomer og astma, men det er ikke belyst, hvorvidt det
også øger risikoen for akut bronkiolitis, der antages at være et event,
DMSc Thesis by Bo Chawes
62
der karakteriserer børn, som udvikler persisterende astma. I VI
studerede vi neonatale forcerede flow, volumen, og reaktivitet overfor
metacholin i forhold til udvikling af akut svær bronkiolitis i alderen
0-2 år. Børn, der udviklede bronkiolitis, havde en 2,5-fold øget
reaktivitet som neonatale (VI), hvilket indikerer en præeksisterende
fælles tilbøjelighed i luftvejene til at reagere uhensigtsmæssigt
overfor almindelige luftvejsvira og til at udvikle astma. Dette fund
antyder, at bronkial hyperreaktivitet er endnu en markør for en lavgrads
sygdomsaktivitet hos asymptomatiske neonatale børn, der senere udvikler
børneastma og astmarelaterede sygdomme.
I VII undersøgte vi, om neonatale børn med reduceret lungefunktion også
har tegn på systemisk inflammation, før de udvikler kliniske symptomer.
Vi fandt, at lav FEV0.5 var signifikant associeret med forhøjet serum hs-
CRP og andre inflammatoriske markører i blodet (VII), hvilket indikerer
tilstedeværelse af systemisk lavgrads inflammation fra livets
begyndelse. Kronisk lavgrads inflammation er en fællesnævner for stort
set alle de store hyppigt forekommende ikkesmitsomme livsstilssygdomme,
af hvilke astma og allergi er de sygdomme, der debuterer tidligst i
livet. Den nye opdagelse af systemisk lavgrads inflammation blandt
neonatale med en øget risiko for at udvikle astma og allergi indebærer
derfor, at undersøgelser af ophavet til astma og allergi måske også kan
afdække sygdomsmekanismer involveret i andre livstilssygdomme, der
debuterer senere i livet.
Studierne i denne afhandling (I-VII) påviser eksistensen af en
præsymptomatisk sygdomsproces, som kan måles i flere forskellige
kropssystemer, hvilket understøtter, at lavgrads sygdomsaktivitet
tidligt i livet er et generisk karakteristika hos neonatale børn, der
udvikler astma og allergi i barndommen. Denne hypotese, som baserer sig
på måling af single biomarkører, kunne udbygges og raffineres ved at
anvende nyere globale omics teknologier. Metabolomics analyser af serum,
urin og luftvejssekret samt VOC profilering af udåndingsluft fra
neonatale børn kunne formodentlig føre til en bredere forståelse af den
lavgrads sygdomsproces, der foregår tidligt i livet, lang tid før
børnene udvikler symptomer. En dybere forståelse af disse indledende

DMSc Thesis by Bo Chawes
63
patofysiologiske mekanismer og de underliggende sygdoms subtyper er
afgørende for at kunne udvikle succesfulde forebyggende tiltag for at
afhjælpe den store globale byrde, som astma, allergi og andre moderne
livsstilssygdomme udgør.

DMSc Thesis by Bo Chawes
64
ACKNOWLEDGEMENTS The work presented in this thesis is based on investigations performed
at the COPSAC research clinic, Danish Pediatric Asthma Center, Copenhagen University Hospital, Gentofte, from 2007 to 2015. This work would not
have been possible without the invaluable support and guidance from
Professor Hans Bisgaard. Hans has been my mentor, friend, and a great
source of inspiration for more than a decade. He believed in me,
challenged me, and has, with his uncompromised ambitious approach to
pediatric research, lit a lifetime passion for research in me.
I would like to thank all the co-authors of the included manuscripts for
lots of fruitful discussions and constructive input. I owe thanks to
Johannes Waage for helping me with the figures included in the thesis
and to my mother for proofreading the text. I also wish to thank all my
dear colleagues at the COPSAC research unit - it would never have been
the same without you.
A special thank to all the children and parents in the COPSAC cohort
whose participation and dedication made these studies possible, and to
all funding agencies, who supported the studies financially
(acknowledged on www.copsac.com).
Finally, I wish to thank my love, wife, and best friend Anne for her
deep support, never ending patience, encouragement and understanding,
and our children Asbjørn, Ellen and Jens for being there - thank you for
letting me know what is important in life.

DMSc Thesis by Bo Chawes
65
REFERENCES 1. Bisgaard, H. & Szefler, S. Prevalence of asthma-like symptoms in young
children. Pediatr. Pulmonol 42, 723–728 (2007). 2. Newacheck, P. W. & Stoddard, J. J. Prevalence and impact of multiple
childhood chronic illnesses. J. Pediatr 124, 40–48 (1994). 3. Kocevar, V. S. et al. Variations in pediatric asthma hospitalization
rates and costs between and within Nordic countries. Chest 125, 1680–1684 (2004).
4. Eder, W., Ege, M. J. & von Mutius, E. The Asthma Epidemic. N. Engl. J. Med. 355, 2226–2235 (2006).
5. Masoli, M., Fabian, D., Holt, S. & Beasley, R. The global burden of asthma: executive summary of the GINA Dissemination Committee report. Allergy 59, 469–478 (2004).
6. Anandan, C., Nurmatov, U., van Schayck, O. C. P. & Sheikh, A. Is the prevalence of asthma declining? Systematic review of epidemiological studies. Allergy 65, 152–167 (2010).
7. Asher, M. I. et al. Worldwide time trends in the prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and eczema in childhood: ISAAC Phases One and Three repeat multicountry cross-sectional surveys. Lancet 368, 733–743 (2006).
8. Martinez, F. D. et al. Asthma and wheezing in the first six years of life. The Group Health Medical Associates. N. Engl. J. Med 332, 133–138 (1995).
9. Kulig, M. et al. Development of seasonal allergic rhinitis during the first 7 years of life. J. Allergy Clin. Immunol. 106, 832–839 (2000).
10. Marinho, S. et al. Rhinoconjunctivitis in 5-year-old children: a population-based birth cohort study. Allergy 62, 385–393 (2007).
11. Chawes, B. L. K., Kreiner-Møller, E. & Bisgaard, H. Objective assessments of allergic and nonallergic rhinitis in young children. Allergy 64, 1547–1553 (2009).
12. Bender Berz, J., Murdock, K. K. & Koinis Mitchell, D. Children’s Asthma, Internalizing Problems, and Social Functioning: An Urban Perspective. Journal of Child and Adolescent Psychiatric Nursing 18, 181–197 (2005).
13. Katon, W. J., Richardson, L., Lozano, P. & McCauley, E. The Relationship of Asthma and Anxiety Disorders. Psychosomatic Medicine 66, 349 –355 (2004).
14. Brasholt, M., Baty, F. & Bisgaard, H. Physical activity in young children is reduced with increasing bronchial responsiveness. J. Allergy Clin. Immunol 125, 1007–1012 (2010).
15. Glazebrook, C. et al. Asthma as a barrier to children’s physical activity: implications for body mass index and mental health. Pediatrics 118, 2443–2449 (2006).
16. Ng, D. K., Chan, C., Hwang, G. Y., Chow, P. & Kwok, K. A review of the roles of allergic rhinitis in childhood obstructive sleep apnea syndrome. Allergy Asthma Proc 27, 240–242 (2006).

DMSc Thesis by Bo Chawes
66
17. Meltzer, E. O. et al. Burden of allergic rhinitis: results from the Pediatric Allergies in America survey. J. Allergy Clin. Immunol. 124, S43–70 (2009).
18. Fowler, M. G., Davenport, M. G. & Garg, R. School functioning of US children with asthma. Pediatrics 90, 939–944 (1992).
19. Vuurman, E. F., van Veggel, L. M., Uiterwijk, M. M., Leutner, D. & O’Hanlon, J. F. Seasonal allergic rhinitis and antihistamine effects on children’s learning. Ann Allergy 71, 121–126 (1993).
20. Walker, S. et al. Seasonal allergic rhinitis is associated with a detrimental effect on examination performance in United Kingdom teenagers: case-control study. J. Allergy Clin. Immunol. 120, 381–387 (2007).
21. Akeson, N., Worth, A. & Sheikh, A. The psychosocial impact of anaphylaxis on young people and their parents. Clinical & Experimental Allergy 37, 1213–1220 (2007).
22. Boulet, L.-P., FitzGerald, J. M. & Reddel, H. K. The revised 2014 GINA strategy report: opportunities for change. Curr Opin Pulm Med 21, 1–7 (2015).
23. Barnes, P. J. Immunology of asthma and chronic obstructive pulmonary disease. Nat. Rev. Immunol. 8, 183–192 (2008).
24. Morishima, Y. et al. Th17-associated cytokines as a therapeutic target for steroid-insensitive asthma. Clin. Dev. Immunol. 2013, 609395 (2013).
25. Bacharier, L. B. & Geha, R. S. Molecular mechanisms of IgE regulation. J. Allergy Clin. Immunol. 105, S547–558 (2000).
26. Bousquet, J. et al. Allergic Rhinitis and its Impact on Asthma (ARIA) 2008 update (in collaboration with the World Health Organization, GA(2)LEN and AllerGen). Allergy 63 Suppl 86, 8–160 (2008).
27. Gelfand, E. W. Inflammatory mediators in allergic rhinitis. J. Allergy Clin. Immunol. 114, S135–138 (2004).
28. Howarth, P. H. et al. Objective monitoring of nasal airway inflammation in rhinitis. J. Allergy Clin. Immunol. 115, S414–441 (2005).
29. Renz, H. et al. Gene-environment interactions in chronic inflammatory disease. Nat. Immunol. 12, 273–277 (2011).
30. Collins, F. S. & Varmus, H. A new initiative on precision medicine. N. Engl. J. Med. 372, 793–795 (2015).
31. Bisgaard, H. & Bønnelykke, K. Long-term studies of the natural history of asthma in childhood. J. Allergy Clin. Immunol 126, 187–197 (2010).
32. Bisgaard, H. The Copenhagen Prospective Study on Asthma in Childhood (COPSAC): design, rationale, and baseline data from a longitudinal birth cohort study. Ann. Allergy Asthma Immunol. 93, 381–389 (2004).

DMSc Thesis by Bo Chawes
67
33. Bisgaard, H., Hermansen, M. N., Loland, L., Halkjaer, L. B. & Buchvald, F. Intermittent inhaled corticosteroids in infants with episodic wheezing. N. Engl. J. Med 354, 1998–2005 (2006).
34. Bisgaard, H. et al. Childhood asthma after bacterial colonization of the airway in neonates. N. Engl. J. Med 357, 1487–1495 (2007).
35. Bisgaard, H., Pipper, C. B. & Bønnelykke, K. Endotyping early childhood asthma by quantitative symptom assessment. J. Allergy Clin. Immunol 127, 1155–1164.e2 (2011).
36. Chawes, B. L. K., Bønnelykke, K., Kreiner-Møller, E. & Bisgaard, H. Children with allergic and nonallergic rhinitis have a similar risk of asthma. J. Allergy Clin. Immunol 126, 567–573.e1–8 (2010).
37. Abrahamsson, T. R., Sandberg Abelius, M., Forsberg, A., Björkstén, B. & Jenmalm, M. C. A Th1/Th2-associated chemokine imbalance during infancy in children developing eczema, wheeze and sensitization. Clin. Exp. Allergy 41, 1729–1739 (2011).
38. Højskov, C. S., Heickendorff, L. & Møller, H. J. High-throughput liquid-liquid extraction and LCMSMS assay for determination of circulating 25(OH) vitamin D3 and D2 in the routine clinical laboratory. Clin. Chim. Acta 411, 114–116 (2010).
39. Maunsell, Z., Wright, D. J. & Rainbow, S. J. Routine isotope-dilution liquid chromatography-tandem mass spectrometry assay for simultaneous measurement of the 25-hydroxy metabolites of vitamins D2 and D3. Clin. Chem. 51, 1683–1690 (2005).
40. Koller, D. Y. Sampling methods: urine/blood analysis. Am. J. Respir. Crit. Care Med. 162, S31–33 (2000).
41. Loland, L. & Bisgaard, H. Feasibility of repetitive lung function measurements by raised volume rapid thoracoabdominal compression during methacholine challenge in young infants. Chest 133, 115–122 (2008).
42. Loland, L. et al. Sensitivity of bronchial responsiveness measurements in young infants. Chest 129, 669–675 (2006).
43. Baraldi, E. & de Jongste, J. C. Measurement of exhaled nitric oxide in children, 2001. Eur. Respir. J. 20, 223–237 (2002).
44. American Thoracic Society & European Respiratory Society. ATS/ERS statement: raised volume forced expirations in infants: guidelines for current practice. Am. J. Respir. Crit. Care Med. 172, 1463–1471 (2005).
45. Bisgaard, H. et al. Chromosome 17q21 gene variants are associated with asthma and exacerbations but not atopy in early childhood. Am. J. Respir. Crit. Care Med 179, 179–185 (2009).
46. Brand, P. L. P. et al. Definition, assessment and treatment of wheezing disorders in preschool children: an evidence-based approach. Eur. Respir. J. 32, 1096–1110 (2008).
47. Bush, A. & Thomson, A. H. Acute bronchiolitis. BMJ 335, 1037–1041 (2007).
48. Smyth, R. L. & Openshaw, P. J. M. Bronchiolitis. Lancet 368, 312–322 (2006).

DMSc Thesis by Bo Chawes
68
49. Schoos, A.-M. M. et al. Disagreement between skin prick test and specific IgE in young children. Allergy (2014). doi:10.1111/all.12523
50. Ballardini, N., Nilsson, C., Nilsson, M. & Lilja, G. ImmunoCAP Phadiatop Infant--a new blood test for detecting IgE sensitisation in children at 2 years of age. Allergy 61, 337–343 (2006).
51. Wickman, M., Ahlstedt, S., Lilja, G. & van Hage Hamsten, M. Quantification of IgE antibodies simplifies the classification of allergic diseases in 4-year-old children. A report from the prospective birth cohort study--BAMSE. Pediatr Allergy Immunol 14, 441–447 (2003).
52. Chawes, B. L. K., Kreiner-Moller, E. & Bisgaard, H. Upper and Lower Airway Patency Are Associated in Young Children. Chest 137, 1332–1337 (2010).
53. Braun-Fahrländer, C. et al. Validation of a rhinitis symptom questionnaire (ISAAC core questions) in a population of Swiss school children visiting the school health services. SCARPOL-team. Swiss Study on Childhood Allergy and Respiratory Symptom with respect to Air Pollution and Climate. International Study of Asthma and Allergies in Childhood. Pediatr Allergy Immunol 8, 75–82 (1997).
54. Warner, J. A. & Warner, J. O. Early life events in allergic sensitisation. Br. Med. Bull. 56, 883–893 (2000).
55. Jones, C. A., Holloway, J. A. & Warner, J. O. Does atopic disease start in foetal life? Allergy 55, 2–10 (2000).
56. Lima, J. O. et al. Early expression of iepsilon, CD23 (FcepsilonRII), IL-4Ralpha, and IgE in the human fetus. J. Allergy Clin. Immunol. 106, 911–917 (2000).
57. Miller, D. L., Hiravonen, T. & Gitlin, D. Synthesis of IgE by the human conceptus. J. Allergy Clin. Immunol. 52, 182–188 (1973).
58. Avrech, O. M. et al. Efficacy of the placental barrier for immunoglobulins: correlations between maternal, paternal and fetal immunoglobulin levels. Int. Arch. Allergy Immunol. 103, 160–165 (1994).
59. Heinrich, J. et al. Allergens and endotoxin on mothers’ mattresses and total immunoglobulin E in cord blood of neonates. Eur. Respir. J. 20, 617–623 (2002).
60. Peters, J. L. et al. Relationships among prenatal aeroallergen exposure and maternal and cord blood IgE: project ACCESS. J. Allergy Clin. Immunol. 123, 1041–1046 (2009).
61. Ferguson, A. et al. Elevated cord blood IgE is associated with recurrent wheeze and atopy at 7 yrs in a high risk cohort. Pediatr Allergy Immunol 20, 710–713 (2009).
62. Scirica, C. V. et al. Predictors of cord blood IgE levels in children at risk for asthma and atopy. J. Allergy Clin. Immunol. 119, 81–88 (2007).
63. Karmaus, W., Arshad, H. & Mattes, J. Does the sibling effect have its origin in utero? Investigating birth order, cord blood

DMSc Thesis by Bo Chawes
69
immunoglobulin E concentration, and allergic sensitization at age 4 years. Am. J. Epidemiol. 154, 909–915 (2001).
64. Halonen, M. et al. Relationship of total serum IgE levels in cord and 9-month sera of infants. Clin. Exp. Allergy 21, 235–241 (1991).
65. Hansen, L. G., Halken, S., Høst, A., Møller, K. & Osterballe, O. Prediction of allergy from family history and cord blood IgE levels. A follow-up at the age of 5 years. Cord blood IgE. IV. Pediatr Allergy Immunol 4, 34–40 (1993).
66. Edenharter, G. et al. Cord blood-IgE as risk factor and predictor for atopic diseases. Clin. Exp. Allergy 28, 671–678 (1998).
67. Odelram, H., Björkstén, B., Leander, E. & Kjellman, N. I. Predictors of atopy in newborn babies. Allergy 50, 585–592 (1995).
68. Nambu, M., Shintaku, N. & Ohta, S. Relationship between cord blood level of IgE specific for Dermatophagoides pteronyssinus and allergic manifestations in infancy. Biol. Neonate 83, 102–106 (2003).
69. American Academy of Pediatrics. Committee on Nutrition. Hypoallergenic infant formulas. Pediatrics 106, 346–349 (2000).
70. Woodcock, A. et al. Early life environmental control: effect on symptoms, sensitization, and lung function at age 3 years. Am. J. Respir. Crit. Care Med. 170, 433–439 (2004).
71. Herrmann, M. E. et al. Prospective study of the atopy preventive effect of maternal avoidance of milk and eggs during pregnancy and lactation. Eur. J. Pediatr. 155, 770–774 (1996).
72. Hourihane, J. O. et al. The impact of government advice to pregnant mothers regarding peanut avoidance on the prevalence of peanut allergy in United Kingdom children at school entry. J. Allergy Clin. Immunol. 119, 1197–1202 (2007).
73. Jones, C. A., Warner, J. A. & Warner, J. O. Fetal swallowing of IgE. Lancet 351, 1859 (1998).
74. Bertino, E. et al. Relationship between maternal- and fetal-specific IgE. Pediatr Allergy Immunol 17, 484–488 (2006).
75. Depner, M. et al. Atopic sensitization in the first year of life. J. Allergy Clin. Immunol. 131, 781–788 (2013).
76. Kamemura, N. et al. Intrauterine sensitization of allergen-specific IgE analyzed by a highly sensitive new allergen microarray. J. Allergy Clin. Immunol. 130, 113–121.e2 (2012).
77. Bønnelykke, K., Pipper, C. B. & Bisgaard, H. Sensitization does not develop in utero. J. Allergy Clin. Immunol 121, 646–651 (2008).
78. Thornton, C. A. et al. Functional maturation of CD4+CD25+CTLA4+CD45RA+ T regulatory cells in human neonatal T cell responses to environmental antigens/allergens. J. Immunol. 173, 3084–3092 (2004).
79. Rowe, J. et al. Prenatal versus postnatal sensitization to environmental allergens in a high-risk birth cohort. J. Allergy Clin. Immunol. 119, 1164–1173 (2007).
80. Ownby, D. R., McCullough, J., Johnson, C. C. & Peterson, E. L. Evaluation of IgA measurements as a method for detecting maternal

DMSc Thesis by Bo Chawes
70
blood contamination of cord blood samples. Pediatr Allergy Immunol 7, 125–129 (1996).
81. Bønnelykke, K., Pipper, C. B. & Bisgaard, H. Transfer of maternal IgE can be a common cause of increased IgE levels in cord blood. J. Allergy Clin. Immunol 126, 657–663 (2010).
82. Moser, M. & Murphy, K. M. Dendritic cell regulation of TH1-TH2 development. Nat. Immunol. 1, 199–205 (2000).
83. Yabuhara, A. et al. TH2-polarized immunological memory to inhalant allergens in atopics is established during infancy and early childhood. Clin. Exp. Allergy 27, 1261–1269 (1997).
84. Prescott, S. L. et al. Development of allergen-specific T-cell memory in atopic and normal children. Lancet 353, 196–200 (1999).
85. Miles, E. A. et al. Peripheral blood mononuclear cell proliferative responses in the first year of life in babies born to allergic parents. Clin. Exp. Allergy 26, 780–788 (1996).
86. Ozdemir, C., Akdis, M. & Akdis, C. A. T regulatory cells and their counterparts: masters of immune regulation. Clin. Exp. Allergy 39, 626–639 (2009).
87. Schaub, B. et al. Impairment of T-regulatory cells in cord blood of atopic mothers. J. Allergy Clin. Immunol. 121, 1491–1499, 1499.e1–13 (2008).
88. Schaub, B. et al. Maternal farm exposure modulates neonatal immune mechanisms through regulatory T cells. J. Allergy Clin. Immunol. 123, 774–782.e5 (2009).
89. Von Mutius, E. Allergies, infections and the hygiene hypothesis--the epidemiological evidence. Immunobiology 212, 433–439 (2007).
90. Prescott, S. L., King, B., Strong, T. L. & Holt, P. G. The value of perinatal immune responses in predicting allergic disease at 6 years of age. Allergy 58, 1187–1194 (2003).
91. Sandberg, M. et al. Cord blood cytokines and chemokines and development of allergic disease. Pediatr Allergy Immunol 20, 519–527 (2009).
92. Mantovani, A. et al. The chemokine system in diverse forms of macrophage activation and polarization. Trends in Immunology 25, 677–686 (2004).
93. Pease, J. E. & Williams, T. J. Chemokines and their receptors in allergic disease. Journal of Allergy and Clinical Immunology 118, 305–318 (2006).
94. Abrahamsson, T. R., Sandberg Abelius, M., Forsberg, A., Björkstén, B. & Jenmalm, M. C. A Th1/Th2-associated chemokine imbalance during infancy in children developing eczema, wheeze and sensitization. Clin. Exp. Allergy 41, 1729–1739 (2011).
95. Fujisawa, T. et al. Presence of high contents of thymus and activation-regulated chemokine in platelets and elevated plasma levels of thymus and activation-regulated chemokine and macrophage-derived chemokine in patients with atopic dermatitis. Journal of Allergy and Clinical Immunology 110, 139–146 (2002).

DMSc Thesis by Bo Chawes
71
96. Jahnz‐Rozyk, K., Targowski, T., Paluchowska, E., Owczarek, W. & Kucharczyk, A. Serum thymus and activation‐regulated chemokine, macrophage‐derived chemokine and eotaxin as markers of severity of atopic dermatitis. Allergy 60, 685–688 (2005).
97. Abelius, M. S. et al. High Cord Blood Levels of the T-Helper 2-Associated Chemokines CCL17 and CCL22 Precede Allergy Development During the First 6 Years of Life. Pediatr. Res. 70, 495–500 (2011).
98. Sandberg, M. et al. Cord blood cytokines and chemokines and development of allergic disease. Pediatric Allergy and Immunology 20, 519–527 (2009).
99. Kotaniemi-Syrjänen, A. et al. Allergen-specific immunoglobulin E antibodies in wheezing infants: the risk for asthma in later childhood. Pediatrics 111, e255–261 (2003).
100. Rotsides, D. Z. et al. Asthma, allergy, and IgE levels in NYC head start children. Respir Med 104, 345–355 (2010).
101. Medoff, B. D. et al. CD11b+ myeloid cells are the key mediators of Th2 cell homing into the airway in allergic inflammation. J. Immunol. 182, 623–635 (2009).
102. Hartl, D. et al. Pulmonary chemokines and their receptors differentiate children with asthma and chronic cough. J. Allergy Clin. Immunol. 115, 728–736 (2005).
103. Miyahara, H., Okazaki, N., Nagakura, T., Korematsu, S. & Izumi, T. Elevated umbilical cord serum TARC/CCL17 levels predict the development of atopic dermatitis in infancy. Clinical & Experimental Allergy 41, 186–191 (2011).
104. Følsgaard, N. V. et al. Neonatal Cytokine Profile in the Airway Mucosal Lining Fluid Is Skewed by Maternal Atopy. Am. J. Respir. Crit. Care Med. 185, 275 –280 (2012).
105. Brodin, P. et al. Variation in the human immune system is largely driven by non-heritable influences. Cell 160, 37–47 (2015).
106. Theodoratou, E., Tzoulaki, I., Zgaga, L. & Ioannidis, J. P. A. Vitamin D and multiple health outcomes: umbrella review of systematic reviews and meta-analyses of observational studies and randomised trials. BMJ 348, g2035 (2014).
107. Sichert-Hellert, W., Wenz, G. & Kersting, M. Vitamin intakes from supplements and fortified food in German children and adolescents: results from the DONALD study. J. Nutr. 136, 1329–1333 (2006).
108. Hollams, E. M. Vitamin D and atopy and asthma phenotypes in children. Curr Opin Allergy Clin Immunol 12, 228–234 (2012).
109. Litonjua, A. A. & Weiss, S. T. Is vitamin D deficiency to blame for the asthma epidemic? Journal of Allergy and Clinical Immunology 120, 1031–1035 (2007).
110. Litonjua, A. A. Childhood asthma may be a consequence of vitamin D deficiency. Curr Opin Allergy Clin Immunol 9, 202–207 (2009).
111. Holick, M. F. Vitamin D deficiency. N. Engl. J. Med. 357, 266–281 (2007).

DMSc Thesis by Bo Chawes
72
112. Lee, J. M. et al. Vitamin D deficiency in a healthy group of mothers and newborn infants. Clin Pediatr (Phila) 46, 42–44 (2007).
113. Raby, B. A. et al. Association of vitamin D receptor gene polymorphisms with childhood and adult asthma. Am. J. Respir. Crit. Care Med. 170, 1057–1065 (2004).
114. Wjst, M. et al. Asthma families show transmission disequilibrium of gene variants in the vitamin D metabolism and signalling pathway. Respir. Res. 7, 60 (2006).
115. Topilski, I. et al. The anti-inflammatory effects of 1,25-dihydroxyvitamin D3 on Th2 cells in vivo are due in part to the control of integrin-mediated T lymphocyte homing. Eur. J. Immunol. 34, 1068–1076 (2004).
116. Cantorna, M. T., Zhu, Y., Froicu, M. & Wittke, A. Vitamin D status, 1,25-dihydroxyvitamin D3, and the immune system. Am. J. Clin. Nutr. 80, 1717S–20S (2004).
117. Matheu, V., Bäck, O., Mondoc, E. & Issazadeh-Navikas, S. Dual effects of vitamin D-induced alteration of TH1/TH2 cytokine expression: enhancing IgE production and decreasing airway eosinophilia in murine allergic airway disease. J. Allergy Clin. Immunol. 112, 585–592 (2003).
118. Pichler, J. et al. 1 alpha,25(OH)2D3 inhibits not only Th1 but also Th2 differentiation in human cord blood T cells. Pediatr. Res. 52, 12–18 (2002).
119. Jones, A. P. et al. 25-hydroxyvitamin D3 status is associated with developing adaptive and innate immune responses in the first 6 months of life. Clin. Exp. Allergy 45, 220–231 (2015).
120. Gregori, S. et al. Regulatory T cells induced by 1 alpha,25-dihydroxyvitamin D3 and mycophenolate mofetil treatment mediate transplantation tolerance. J. Immunol. 167, 1945–1953 (2001).
121. Chi, A. et al. Umbilical cord plasma 25-hydroxyvitamin D concentration and immune function at birth: the Urban Environment and Childhood Asthma study. Clin. Exp. Allergy 41, 842–850 (2011).
122. Vijayendra Chary, A. et al. Vitamin D deficiency in pregnant women impairs regulatory T cell function. J. Steroid Biochem. Mol. Biol. 147, 48–55 (2015).
123. Yim, S., Dhawan, P., Ragunath, C., Christakos, S. & Diamond, G. Induction of cathelicidin in normal and CF bronchial epithelial cells by 1,25-dihydroxyvitamin D(3). J. Cyst. Fibros. 6, 403–410 (2007).
124. Muehleisen, B. & Gallo, R. L. Vitamin D in allergic disease: shedding light on a complex problem. J. Allergy Clin. Immunol. 131, 324–329 (2013).
125. Rochat, M. K. et al. Maternal vitamin D intake during pregnancy increases gene expression of ILT3 and ILT4 in cord blood. Clin. Exp. Allergy 40, 786–794 (2010).
126. Nguyen, M. et al. 1,25-Dihydroxyvitamin D3 and fetal lung maturation: immunogold detection of VDR expression in pneumocytes type

DMSc Thesis by Bo Chawes
73
II cells and effect on fructose 1,6 bisphosphatase. J. Steroid Biochem. Mol. Biol. 89-90, 93–97 (2004).
127. Kho, A. T. et al. Vitamin D related genes in lung development and asthma pathogenesis. BMC Med Genomics 6, 47 (2013).
128. Camargo, C. A. et al. Maternal intake of vitamin D during pregnancy and risk of recurrent wheeze in children at 3 y of age. Am. J. Clin. Nutr. 85, 788–795 (2007).
129. Devereux, G. et al. Maternal vitamin D intake during pregnancy and early childhood wheezing. Am. J. Clin. Nutr. 85, 853–859 (2007).
130. Erkkola, M. et al. Maternal vitamin D intake during pregnancy is inversely associated with asthma and allergic rhinitis in 5-year-old children. Clin. Exp. Allergy 39, 875–882 (2009).
131. Morales, E. et al. Maternal vitamin D status in pregnancy and risk of lower respiratory tract infections, wheezing, and asthma in offspring. Epidemiology 23, 64–71 (2012).
132. Maslova, E. et al. Predicted vitamin D status in mid-pregnancy and child allergic disease. Pediatr Allergy Immunol 25, 706–713 (2014).
133. Chiu, C.-Y. et al. Low cord blood vitamin D levels are associated with increased milk sensitization in early childhood. Pediatr Allergy Immunol 25, 767–772 (2014).
134. Rothers, J., Wright, A. L., Stern, D. A., Halonen, M. & Camargo, C. A. Cord blood 25-hydroxyvitamin D levels are associated with aeroallergen sensitization in children from Tucson, Arizona. J. Allergy Clin. Immunol. 128, 1093–1099.e1–5 (2011).
135. Liu, X. et al. Gene-vitamin D interactions on food sensitization: a prospective birth cohort study. Allergy 66, 1442–1448 (2011).
136. Łuczyńska, A. et al. Cord blood 25(OH)D levels and the subsequent risk of lower respiratory tract infections in early childhood: the Ulm birth cohort. Eur. J. Epidemiol. 29, 585–594 (2014).
137. Mohamed, W. A. W. & Al-Shehri, M. A. Cord blood 25-hydroxyvitamin D levels and the risk of acute lower respiratory tract infection in early childhood. J. Trop. Pediatr. 59, 29–35 (2013).
138. Stelmach, I. et al. Cord serum 25-hydroxyvitamin D correlates with early childhood viral-induced wheezing. Respir Med 109, 38–43 (2015).
139. Weisse, K. et al. Maternal and newborn vitamin D status and its impact on food allergy development in the German LINA cohort study. Allergy 68, 220–228 (2013).
140. Jones, A. P., Palmer, D., Zhang, G. & Prescott, S. L. Cord blood 25-hydroxyvitamin D3 and allergic disease during infancy. Pediatrics 130, e1128–1135 (2012).
141. Camargo, C. A. et al. Cord-Blood 25-Hydroxyvitamin D Levels and Risk of Respiratory Infection, Wheezing, and Asthma. Pediatrics 127, e180 –e187 (2011).
142. Baïz, N. et al. Cord serum 25-hydroxyvitamin D and risk of early childhood transient wheezing and atopic dermatitis. J. Allergy Clin. Immunol. 133, 147–153 (2014).

DMSc Thesis by Bo Chawes
74
143. Belderbos, M. E. et al. Cord blood vitamin D deficiency is associated with respiratory syncytial virus bronchiolitis. Pediatrics 127, e1513–1520 (2011).
144. Baïz, N. et al. Cord serum 25-hydroxyvitamin D and risk of early childhood transient wheezing and atopic dermatitis. J. Allergy Clin. Immunol. 133, 147–153 (2014).
145. Stelmach, I. et al. The role of zinc, copper, plasma glutathione peroxidase enzyme, and vitamins in the development of allergic diseases in early childhood: The Polish mother and child cohort study. Allergy Asthma Proc 35, 227–232 (2014).
146. Devereux, G. et al. Early childhood wheezing symptoms in relation to plasma selenium in pregnant mothers and neonates. Clin. Exp. Allergy 37, 1000–1008 (2007).
147. Nwaru, B. I. et al. An exploratory study of the associations between maternal iron status in pregnancy and childhood wheeze and atopy. Br. J. Nutr. 112, 2018–2027 (2014).
148. Turner, S. W. et al. Associations between fetal size, maternal {alpha}-tocopherol and childhood asthma. Thorax 65, 391–397 (2010).
149. Blümer, N. & Renz, H. Consumption of omega3-fatty acids during perinatal life: role in immuno-modulation and allergy prevention. J Perinat Med 35 Suppl 1, S12–18 (2007).
150. Willers, S. M. et al. Maternal food consumption during pregnancy and asthma, respiratory and atopic symptoms in 5-year-old children. Thorax 62, 773–779 (2007).
151. Sausenthaler, S. et al. Maternal diet during pregnancy in relation to eczema and allergic sensitization in the offspring at 2 y of age. Am J Clin Nutr 85, 530–537 (2007).
152. Dunstan, J. A. et al. Fish oil supplementation in pregnancy modifies neonatal allergen-specific immune responses and clinical outcomes in infants at high risk of atopy: A randomized, controlled trial. Journal of Allergy and Clinical Immunology 112, 1178–1184 (2003).
153. Furuhjelm, C. et al. Fish oil supplementation in pregnancy and lactation may decrease the risk of infant allergy. Acta Pædiatrica 98, 1461–1467 (2009).
154. Palmer, D. J. et al. Randomized controlled trial of fish oil supplementation in pregnancy on childhood allergies. Allergy 68, 1370–1376 (2013).
155. Slifman, N. R., Venge, P., Peterson, C. G., McKean, D. J. & Gleich, G. J. Human eosinophil-derived neurotoxin and eosinophil protein X are likely the same protein. J. Immunol. 143, 2317–2322 (1989).
156. Kristjánsson, S. et al. Urinary eosinophil protein X in children with atopic asthma: a useful marker of antiinflammatory treatment. J. Allergy Clin. Immunol. 97, 1179–1187 (1996).
157. Cottin, V., Deviller, P., Tardy, F. & Cordier, J. F. Urinary eosinophil-derived neurotoxin/protein X: a simple method for assessing

DMSc Thesis by Bo Chawes
75
eosinophil degranulation in vivo. J. Allergy Clin. Immunol. 101, 116–123 (1998).
158. Pucci, N. et al. Urinary eosinophil protein X and serum eosinophil cationic protein in infants and young children with atopic dermatitis: correlation with disease activity. J. Allergy Clin. Immunol. 105, 353–357 (2000).
159. Bochenek, G., Nagraba, K., Nizankowska, E. & Szczeklik, A. A controlled study of 9alpha,11beta-PGF2 (a prostaglandin D2 metabolite) in plasma and urine of patients with bronchial asthma and healthy controls after aspirin challenge. J. Allergy Clin. Immunol. 111, 743–749 (2003).
160. Gore, C. et al. Urinary eosinophilic protein X, atopy, and symptoms suggestive of allergic disease at 3 years of age. J. Allergy Clin. Immunol. 112, 702–708 (2003).
161. Tauber, E. et al. Urinary eosinophil protein X in children: the relationship to asthma and atopy and normal values. Allergy 55, 647–652 (2000).
162. Oymar, K. & Bjerknes, R. Urinary eosinophil protein X in children with atopic dermatitis: relation to atopy and disease activity. Allergy 55, 964–968 (2000).
163. Wojnarowski, C. et al. Urinary leukotriene E(4), eosinophil protein X, and nasal eosinophil cationic protein are not associated with respiratory symptoms in 1-year-old children. Allergy 56, 883–888 (2001).
164. Oymar, K., Havnen, J., Halvorsen, T. & Bjerknes, R. Eosinophil counts and urinary eosinophil protein X in children hospitalized for wheezing during the first year of life: prediction of recurrent wheezing. Acta Paediatr. 90, 843–849 (2001).
165. Lugosi, E., Halmerbauer, G., Frischer, T. & Koller, D. Y. Urinary eosinophil protein X in relation to disease activity in childhood asthma. Allergy 52, 584–588 (1997).
166. Oymar, K. & Bjerknes, R. Urinary eosinophil protein X in children with asthma: influence of atopy and airway infections. Pediatr Allergy Immunol 12, 34–41 (2001).
167. Nuijsink, M., Hop, W. C. J., Sterk, P. J., Duiverman, E. J. & De Jongste, J. C. Urinary eosinophil protein X in childhood asthma: relation with changes in disease control and eosinophilic airway inflammation. Mediators Inflamm. 2013, 532619 (2013).
168. Labbé, A. et al. Prospective longitudinal study of urinary eosinophil protein X in children with asthma and chronic cough. Pediatr. Pulmonol. 31, 354–362 (2001).
169. Wolthers, O. D. Eosinophil granule proteins in the assessment of airway inflammation in pediatric bronchial asthma. Pediatr Allergy Immunol 14, 248–254 (2003).
170. Wedes, S. H. et al. Urinary bromotyrosine measures asthma control and predicts asthma exacerbations in children. J. Pediatr. 159, 248–255.e1 (2011).

DMSc Thesis by Bo Chawes
76
171. Severien, C., Artlich, A., Jonas, S. & Becher, G. Urinary excretion of leukotriene E4 and eosinophil protein X in children with atopic asthma. Eur. Respir. J. 16, 588–592 (2000).
172. Oh, J.-W., Shin, S.-A. & Lee, H.-B. Urine leukotriene E and eosinophil cationic protein in nasopharyngeal aspiration from young wheezy children. Pediatr Allergy Immunol 16, 416–421 (2005).
173. Oommen, A. & Grigg, J. Urinary leukotriene E4 in preschool children with acute clinical viral wheeze. Eur. Respir. J. 21, 149–154 (2003).
174. Marmarinos, A. et al. Urinary leukotriene E4 levels in atopic and non-atopic preschool children with recurrent episodic (viral) wheezing: a potential marker? J Asthma 1–6 (2014). doi:10.3109/02770903.2014.990092
175. Zanconato, S. et al. Dissociation between biological and clinical response to oral challenge in children with food allergy. Allergy 63, 1408–1410 (2008).
176. Nagakura, T. et al. GC/MS analysis of urinary excretion of 9alpha,11beta-PGF2 in acute and exercise-induced asthma in children. Clin. Exp. Allergy 28, 181–186 (1998).
177. Baek, H.-S., Choi, J.-H., Oh, J.-W. & Lee, H.-B. Leptin and urinary leukotriene E4 and 9α,11β-prostaglandin F2 release after exercise challenge. Ann. Allergy Asthma Immunol. 111, 112–117 (2013).
178. Bochenek, G., Nagraba, K., Nizankowska, E. & Szczeklik, A. A controlled study of 9alpha,11beta-PGF2 (a prostaglandin D2 metabolite) in plasma and urine of patients with bronchial asthma and healthy controls after aspirin challenge. J. Allergy Clin. Immunol. 111, 743–749 (2003).
179. O’Sullivan, S., Roquet, A., Dahlén, B., Dahlén, S. & Kumlin, M. Urinary excretion of inflammatory mediators during allergen-induced early and late phase asthmatic reactions. Clin. Exp. Allergy 28, 1332–1339 (1998).
180. Mattes, J. et al. Circadian variation of exhaled nitric oxide and urinary eosinophil protein X in asthmatic and healthy children. Pediatr. Res. 51, 190–194 (2002).
181. Hoffjan, S. et al. Genetic variation in immunoregulatory pathways and atopic phenotypes in infancy. J. Allergy Clin. Immunol. 113, 511–518 (2004).
182. Kabesch, M. et al. Polymorphisms in eosinophil pathway genes, asthma and atopy. Allergy 62, 423–428 (2007).
183. Elmose, C. et al. Genetic factors explain half of all variance in serum eosinophil cationic protein. Clin. Exp. Allergy 44, 1525–1530 (2014).
184. Kettunen, J. et al. Genome-wide association study identifies multiple loci influencing human serum metabolite levels. Nat. Genet. 44, 269–276 (2012).
185. Soininen, P. et al. High-throughput serum NMR metabonomics for cost-effective holistic studies on systemic metabolism. Analyst 134, 1781–1785 (2009).

DMSc Thesis by Bo Chawes
77
186. Saude, E. J. et al. Metabolomic profiling of asthma: diagnostic utility of urine nuclear magnetic resonance spectroscopy. J. Allergy Clin. Immunol. 127, 757–764.e1–6 (2011).
187. Mattarucchi, E., Baraldi, E. & Guillou, C. Metabolomics applied to urine samples in childhood asthma; differentiation between asthma phenotypes and identification of relevant metabolites. Biomed. Chromatogr. 26, 89–94 (2012).
188. Fitzpatrick, A. M., Park, Y., Brown, L. A. S. & Jones, D. P. Children with severe asthma have unique oxidative stress-associated metabolomic profiles. J. Allergy Clin. Immunol. 133, 258–261.e1–8 (2014).
189. Gustafsson, L. E., Leone, A. M., Persson, M. G., Wiklund, N. P. & Moncada, S. Endogenous nitric oxide is present in the exhaled air of rabbits, guinea pigs and humans. Biochem. Biophys. Res. Commun. 181, 852–857 (1991).
190. Alving, K., Weitzberg, E. & Lundberg, J. M. Increased amount of nitric oxide in exhaled air of asthmatics. Eur. Respir. J. 6, 1368–1370 (1993).
191. Lane, C. et al. Epithelial inducible nitric oxide synthase activity is the major determinant of nitric oxide concentration in exhaled breath. Thorax 59, 757–760 (2004).
192. Buchvald, F. & Bisgaard, H. FeNO measured at fixed exhalation flow rate during controlled tidal breathing in children from the age of 2 yr. Am. J. Respir. Crit. Care Med. 163, 699–704 (2001).
193. Gabriele, C. et al. Exhaled nitric oxide differentiates airway diseases in the first two years of life. Pediatr. Res. 60, 461–465 (2006).
194. Moeller, A. et al. Exhaled nitric oxide distinguishes between subgroups of preschool children with respiratory symptoms. J. Allergy Clin. Immunol. 121, 705–709 (2008).
195. Zacharasiewicz, A. et al. Clinical use of noninvasive measurements of airway inflammation in steroid reduction in children. Am. J. Respir. Crit. Care Med. 171, 1077–1082 (2005).
196. Pijnenburg, M. W., Hofhuis, W., Hop, W. C. & De Jongste, J. C. Exhaled nitric oxide predicts asthma relapse in children with clinical asthma remission. Thorax 60, 215–218 (2005).
197. Buchvald, F. et al. Measurements of exhaled nitric oxide in healthy subjects age 4 to 17 years. J. Allergy Clin. Immunol. 115, 1130–1136 (2005).
198. Latzin, P. et al. Elevated exhaled nitric oxide in newborns of atopic mothers precedes respiratory symptoms. Am. J. Respir. Crit. Care Med. 174, 1292–1298 (2006).
199. Wildhaber, J. H., Hall, G. L. & Stick, S. M. Measurements of exhaled nitric oxide with the single-breath technique and positive expiratory pressure in infants. Am. J. Respir. Crit. Care Med. 159, 74–78 (1999).

DMSc Thesis by Bo Chawes
78
200. Hall, G. L., Reinmann, B., Wildhaber, J. H. & Frey, U. Tidal exhaled nitric oxide in healthy, unsedated newborn infants with prenatal tobacco exposure. J. Appl. Physiol. 92, 59–66 (2002).
201. Kharitonov, S. A. & Barnes, P. J. Nasal contribution to exhaled nitric oxide during exhalation against resistance or during breath holding. Thorax 52, 540–544 (1997).
202. Jöbsis, Q., Schellekens, S. L., Kroesbergen, A., Hop, W. C. & de Jongste, J. C. Sampling of exhaled nitric oxide in children: end-expiratory plateau, balloon and tidal breathing methods compared. Eur. Respir. J. 13, 1406–1410 (1999).
203. American Thoracic Society & European Respiratory Society. ATS/ERS recommendations for standardized procedures for the online and offline measurement of exhaled lower respiratory nitric oxide and nasal nitric oxide, 2005. Am. J. Respir. Crit. Care Med. 171, 912–930 (2005).
204. Gabriele, C. et al. Methodological aspects of exhaled nitric oxide measurements in infants. Pediatr Allergy Immunol 18, 36–41 (2007).
205. Broekema, M. et al. Airway epithelial changes in smokers but not in ex-smokers with asthma. Am. J. Respir. Crit. Care Med. 180, 1170–1178 (2009).
206. Gabriele, C. et al. Smoke exposure, airway symptoms and exhaled nitric oxide in infants: the Generation R study. Eur. Respir. J. 32, 307–313 (2008).
207. Frey, U. et al. Maternal atopic disease modifies effects of prenatal risk factors on exhaled nitric oxide in infants. Am. J. Respir. Crit. Care Med. 170, 260–265 (2004).
208. Carlstedt, F., Lazowska, D., Bornehag, C.-G., Olin, A.-C. & Hasselgren, M. Exhaled nitric oxide and urinary EPX levels in infants: a pilot study. Clin Mol Allergy 9, 8 (2011).
209. Gabriele, C. et al. Exhaled nitric oxide and the risk of wheezing in infancy: the Generation R Study. Eur. Respir. J. 39, 567–572 (2012).
210. Palmer, C. N. A. et al. Filaggrin null mutations are associated with increased asthma severity in children and young adults. Journal of Allergy and Clinical Immunology 120, 64–68 (2007).
211. Bønnelykke, K., Pipper, C. B., Tavendale, R., Palmer, C. N. A. & Bisgaard, H. Filaggrin gene variants and atopic diseases in early childhood assessed longitudinally from birth. Pediatr Allergy Immunol 21, 954–961 (2010).
212. Sleiman, P. M. A. et al. Variants of DENND1B associated with asthma in children. N. Engl. J. Med 362, 36–44 (2010).
213. Lindstedt, M., Lundberg, K. & Borrebaeck, C. A. K. Gene family clustering identifies functionally associated subsets of human in vivo blood and tonsillar dendritic cells. J. Immunol. 175, 4839–4846 (2005).
214. Franke, A. et al. Genome-wide meta-analysis increases to 71 the number of confirmed Crohn’s disease susceptibility loci. Nat Genet 42, 1118–1125 (2010).

DMSc Thesis by Bo Chawes
79
215. Mells, G. F. et al. Genome-wide association study identifies 12 new susceptibility loci for primary biliary cirrhosis. Nat Genet 43, 329–332 (2011).
216. Van der Valk, R. J. P. et al. Fraction of exhaled nitric oxide values in childhood are associated with 17q11.2-q12 and 17q12-q21 variants. J. Allergy Clin. Immunol. 134, 46–55 (2014).
217. Salam, M. T. et al. Genetic variations in nitric oxide synthase and arginase influence exhaled nitric oxide levels in children. Allergy 66, 412–419 (2011).
218. Salam, M. T. et al. Genetic and epigenetic variations in inducible nitric oxide synthase promoter, particulate pollution, and exhaled nitric oxide levels in children. J. Allergy Clin. Immunol. 129, 232–239.e1–7 (2012).
219. Petsky, H. L. et al. Tailored interventions based on exhaled nitric oxide versus clinical symptoms for asthma in children and adults. Cochrane Database Syst Rev CD006340 (2009). doi:10.1002/14651858.CD006340.pub3
220. Tepper, R. S. et al. Expired nitric oxide and airway reactivity in infants at risk for asthma. J. Allergy Clin. Immunol. 122, 760–765 (2008).
221. Saglani, S. et al. Early detection of airway wall remodeling and eosinophilic inflammation in preschool wheezers. Am. J. Respir. Crit. Care Med. 176, 858–864 (2007).
222. Martinez, F. D., Morgan, W. J., Wright, A. L., Holberg, C. J. & Taussig, L. M. Diminished lung function as a predisposing factor for wheezing respiratory illness in infants. N. Engl. J. Med. 319, 1112–1117 (1988).
223. Horváth, I. et al. Exhaled breath condensate: methodological recommendations and unresolved questions. Eur. Respir. J. 26, 523–548 (2005).
224. Baraldi, E. & Carraro, S. Exhaled NO and breath condensate. Paediatr Respir Rev 7 Suppl 1, S20–22 (2006).
225. Thomas, P. S. et al. Exhaled breath condensate in pediatric asthma: promising new advance or pouring cold water on a lot of hot air? a systematic review. Pediatr. Pulmonol. 48, 419–442 (2013).
226. Klaassen, E. M. M. et al. Exhaled biomarkers and gene expression at preschool age improve asthma prediction at 6 years of age. Am. J. Respir. Crit. Care Med. 191, 201–207 (2015).
227. Van Vliet, D. et al. Prediction of asthma exacerbations in children by innovative exhaled inflammatory markers: results of a longitudinal study. PLoS ONE 10, e0119434 (2015).
228. Carraro, S. et al. Metabolomics applied to exhaled breath condensate in childhood asthma. Am. J. Respir. Crit. Care Med. 175, 986–990 (2007).
229. Carraro, S. et al. Asthma severity in childhood and metabolomic profiling of breath condensate. Allergy 68, 110–117 (2013).

DMSc Thesis by Bo Chawes
80
230. Moeller, A. et al. Measuring exhaled breath condensates in infants. Pediatr. Pulmonol. 41, 184–187 (2006).
231. Van Berkel, J. J. B. N. et al. Development of accurate classification method based on the analysis of volatile organic compounds from human exhaled air. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 861, 101–107 (2008).
232. Dallinga, J. W. et al. Volatile organic compounds in exhaled breath as a diagnostic tool for asthma in children. Clin. Exp. Allergy 40, 68–76 (2010).
233. Van de Kant, K. D. G. et al. Exhaled breath profiling in diagnosing wheezy preschool children. Eur. Respir. J. 41, 183–188 (2013).
234. Robroeks, C. M. et al. Exhaled volatile organic compounds predict exacerbations of childhood asthma in a 1-year prospective study. Eur. Respir. J. 42, 98–106 (2013).
235. Smolinska, A. et al. Profiling of volatile organic compounds in exhaled breath as a strategy to find early predictive signatures of asthma in children. PLoS ONE 9, e95668 (2014).
236. Dragonieri, S. et al. An electronic nose in the discrimination of patients with asthma and controls. J. Allergy Clin. Immunol. 120, 856–862 (2007).
237. Van der Schee, M. P. et al. Altered exhaled biomarker profiles in children during and after rhinovirus-induced wheeze. Eur. Respir. J. 45, 440–448 (2015).
238. Bisgaard, H. et al. Deep phenotyping of the unselected COPSAC2010 birth cohort study. Clin. Exp. Allergy 43, 1384–1394 (2013).
239. Beydon, N. et al. An official American Thoracic Society/European Respiratory Society statement: pulmonary function testing in preschool children. Am. J. Respir. Crit. Care Med. 175, 1304–1345 (2007).
240. Fjaerli, H.-O., Farstad, T. & Bratlid, D. Hospitalisations for respiratory syncytial virus bronchiolitis in Akershus, Norway, 1993-2000: a population-based retrospective study. BMC Pediatr 4, 25 (2004).
241. Nielsen, H. E. et al. Respiratory syncytial virus infection--risk factors for hospital admission: a case-control study. Acta Paediatr. 92, 1314–1321 (2003).
242. Young, S., O’Keeffe, P. T., Arnott, J. & Landau, L. I. Lung function, airway responsiveness, and respiratory symptoms before and after bronchiolitis. Arch. Dis. Child. 72, 16–24 (1995).
243. Broughton, S. et al. Diminished lung function, RSV infection, and respiratory morbidity in prematurely born infants. Arch. Dis. Child. 91, 26–30 (2006).
244. Drysdale, S. B. et al. Lung function prior to viral lower respiratory tract infections in prematurely born infants. Thorax 66, 468–473 (2011).
245. Zomer-Kooijker, K. et al. Decreased lung function precedes severe respiratory syncytial virus infection and post-respiratory syncytial virus wheeze in term infants. Eur. Respir. J. 44, 666–674 (2014).

DMSc Thesis by Bo Chawes
81
246. Goetghebuer, T., Kwiatkowski, D., Thomson, A. & Hull, J. Familial susceptibility to severe respiratory infection in early life. Pediatr. Pulmonol. 38, 321–328 (2004).
247. Stensballe, L. G. et al. Atopic disposition, wheezing, and subsequent respiratory syncytial virus hospitalization in Danish children younger than 18 months: a nested case-control study. Pediatrics 118, e1360–1368 (2006).
248. Bisgaard, H., Jensen, S. M. & Bønnelykke, K. Interaction between asthma and lung function growth in early life. Am. J. Respir. Crit. Care Med. 185, 1183–1189 (2012).
249. Tager, I. B. et al. Lung function, pre- and post-natal smoke exposure, and wheezing in the first year of life. Am. Rev. Respir. Dis. 147, 811–817 (1993).
250. Murray, C. S. et al. Lung function at one month of age as a risk factor for infant respiratory symptoms in a high risk population. Thorax 57, 388–392 (2002).
251. Young, S., Arnott, J., O’Keeffe, P. T., Le Souef, P. N. & Landau, L. I. The association between early life lung function and wheezing during the first 2 yrs of life. Eur. Respir. J. 15, 151–157 (2000).
252. Martinez, F. D., Morgan, W. J., Wright, A. L., Holberg, C. & Taussig, L. M. Initial Airway Function Is a Risk Factor for Recurrent Wheezing Respiratory Illnesses during the First Three Years of Life. Am Rev Respir Dis 143, 312–316 (1991).
253. Håland, G. et al. Reduced lung function at birth and the risk of asthma at 10 years of age. N. Engl. J. Med. 355, 1682–1689 (2006).
254. Voleti, B. & Agrawal, A. Regulation of basal and induced expression of C-reactive protein through an overlapping element for OCT-1 and NF-kappaB on the proximal promoter. J. Immunol. 175, 3386–3390 (2005).
255. Rifai, N., Tracy, R. P. & Ridker, P. M. Clinical efficacy of an automated high-sensitivity C-reactive protein assay. Clin. Chem. 45, 2136–2141 (1999).
256. Takemura, M. et al. High sensitivity C-reactive protein in asthma. Eur. Respir. J. 27, 908–912 (2006).
257. Kony, S. et al. Association of bronchial hyperresponsiveness and lung function with C-reactive protein (CRP): a population based study. Thorax 59, 892–896 (2004).
258. Shaaban, R. et al. Change in C-reactive protein levels and FEV1 decline: a longitudinal population-based study. Respir Med 100, 2112–2120 (2006).
259. Fogarty, A. W., Jones, S., Britton, J. R., Lewis, S. A. & McKeever, T. M. Systemic inflammation and decline in lung function in a general population: a prospective study. Thorax 62, 515–520 (2007).
260. Thomsen, M. et al. Inflammatory biomarkers and exacerbations in chronic obstructive pulmonary disease. JAMA 309, 2353–2361 (2013).
261. Deraz, T. E., Kamel, T. B., El-Kerdany, T. A. & El-Ghazoly, H. M. A. High-sensitivity C reactive protein as a biomarker for grading of childhood asthma in relation to clinical classification, induced

DMSc Thesis by Bo Chawes
82
sputum cellularity, and spirometry. Pediatr. Pulmonol. 47, 220–225 (2012).
262. Navratil, M. et al. Markers of systemic and lung inflammation in childhood asthma. J Asthma 46, 822–828 (2009).
263. Soferman, R., Glatstein, M., Sivan, Y. & Weisman, Y. HsCRP levels: measurement of airway inflammation in asthmatic children. Pediatr Int 50, 12–16 (2008).
264. Pepys, M. B. & Hirschfield, G. M. C-reactive protein: a critical update. J. Clin. Invest. 111, 1805–1812 (2003).
265. Melbye, H., Hvidsten, D., Holm, A., Nordbø, S. A. & Brox, J. The course of C-reactive protein response in untreated upper respiratory tract infection. Br J Gen Pract 54, 653–658 (2004).
266. Vissing, N. H., Chawes, B. L. K. & Bisgaard, H. Increased risk of pneumonia and bronchiolitis after bacterial colonization of the airways as neonates. Am. J. Respir. Crit. Care Med. 188, 1246–1252 (2013).
267. Bisgaard, H., Loland, L., Holst, K. K. & Pipper, C. B. Prenatal determinants of neonatal lung function in high-risk newborns. J. Allergy Clin. Immunol. 123, 651–657, 657.e1–4 (2009).
268. MacKenzie, K. E. et al. Hs-CRP is associated with weight, BMI, and female sex but not with endothelial function in children with type 1 diabetes. Pediatr Diabetes 10, 44–51 (2009).
269. Holt, P. G. & Sly, P. D. Interaction between adaptive and innate immune pathways in the pathogenesis of atopic asthma: operation of a lung/bone marrow axis. Chest 139, 1165–1171 (2011).
270. Hardyman, M. A. et al. TNF-α-mediated bronchial barrier disruption and regulation by src-family kinase activation. J. Allergy Clin. Immunol. 132, 665–675.e8 (2013).
271. Solovieff, N., Cotsapas, C., Lee, P. H., Purcell, S. M. & Smoller, J. W. Pleiotropy in complex traits: challenges and strategies. Nat. Rev. Genet. 14, 483–495 (2013).
272. Sonnenschein-van der Voort, A. M. M. et al. Influence of maternal and cord blood C-reactive protein on childhood respiratory symptoms and eczema. Pediatr Allergy Immunol 24, 469–475 (2013).
273. Morales, E. et al. Maternal C-reactive protein levels in pregnancy are associated with wheezing and lower respiratory tract infections in the offspring. Am. J. Obstet. Gynecol. 204, 164.e1–9 (2011).
274. Ernst, G. D. S. et al. C-reactive protein levels in early pregnancy, fetal growth patterns, and the risk for neonatal complications: the Generation R Study. Am. J. Obstet. Gynecol. 205, 132.e1–12 (2011).
275. Tjoa, M. L. et al. Elevated C-reactive protein levels during first trimester of pregnancy are indicative of preeclampsia and intrauterine growth restriction. J. Reprod. Immunol. 59, 29–37 (2003).
276. Macaubas, C. et al. Association between antenatal cytokine production and the development of atopy and asthma at age 6 years. Lancet 362, 1192–1197 (2003).

DMSc Thesis by Bo Chawes
83
277. Bisgaard, H., Bønnelykke, K. & Stokholm, J. Immune-mediated diseases and microbial exposure in early life. Clin. Exp. Allergy 44, 475–481 (2014).
278. Prescott, S. & Nowak-Węgrzyn, A. Strategies to prevent or reduce allergic disease. Ann. Nutr. Metab. 59 Suppl 1, 28–42 (2011).
279. Anderson, G. P. Endotyping asthma: new insights into key pathogenic mechanisms in a complex, heterogeneous disease. Lancet 372, 1107–1119 (2008).
280. Chawes, B. L. K. et al. A novel method for assessing unchallenged levels of mediators in nasal epithelial lining fluid. J. Allergy Clin. Immunol 125, 1387–1389.e3 (2010).
281. Ishizaka, A. et al. New bronchoscopic microsample probe to measure the biochemical constituents in epithelial lining fluid of patients with acute respiratory distress syndrome. Crit. Care Med. 29, 896–898 (2001).
282. Følsgaard, N. V. et al. Pathogenic bacteria colonizing the airways in asymptomatic neonates stimulates topical inflammatory mediator release. Am. J. Respir. Crit. Care Med. 187, 589–595 (2013).
283. Konradsen, J. R. et al. The chitinase-like protein YKL-40: a possible biomarker of inflammation and airway remodeling in severe pediatric asthma. J. Allergy Clin. Immunol. 132, 328–335.e5 (2013).
284. Ober, C. et al. Effect of variation in CHI3L1 on serum YKL-40 level, risk of asthma, and lung function. N. Engl. J. Med. 358, 1682–1691 (2008).
285. Leung, T. F., Ko, F. W. S. & Wong, G. W. K. Recent advances in asthma biomarker research. Ther Adv Respir Dis 7, 297–308 (2013).
286. Vijverberg, S. J. et al. Clinical utility of asthma biomarkers: from bench to bedside. Biologics 7, 199–210 (2013).
287. Ried, J. S. et al. Integrative genetic and metabolite profiling analysis suggests altered phosphatidylcholine metabolism in asthma. Allergy 68, 629–636 (2013).
288. Bach, J.-F. The Effect of Infections on Susceptibility to Autoimmune and Allergic Diseases. N. Engl. J. Med. 347, 911–920 (2002).
289. McDade, T. W. Early environments and the ecology of inflammation. Proc. Natl. Acad. Sci. U.S.A. 109 Suppl 2, 17281–17288 (2012).
290. Sabatine, M. S. et al. Prognostic significance of the Centers for Disease Control/American Heart Association high-sensitivity C-reactive protein cut points for cardiovascular and other outcomes in patients with stable coronary artery disease. Circulation 115, 1528–1536 (2007).
291. Hung, M.-J., Hsu, K.-H., Hu, W.-S., Chang, N.-C. & Hung, M.-Y. C-reactive protein for predicting prognosis and its gender-specific associations with diabetes mellitus and hypertension in the development of coronary artery spasm. PLoS ONE 8, e77655 (2013).

DMSc Thesis by Bo Chawes
84
292. Prescott, S. L. Early-life environmental determinants of allergic diseases and the wider pandemic of inflammatory noncommunicable diseases. J. Allergy Clin. Immunol. 131, 23–30 (2013).

DMSc Thesis by Bo Chawes
85
APPENDIX A: PAPER I-VII

Cord Blood 25(OH)-Vitamin D Deficiency and ChildhoodAsthma, Allergy and Eczema: The COPSAC2000 BirthCohort StudyBo L. Chawes1, Klaus Bønnelykke1, Pia F. Jensen1, Ann-Marie M. Schoos1, Lene Heickendorff2,
Hans Bisgaard1*
1 Copenhagen Prospective Studies on Asthma in Childhood, Health Sciences, University of Copenhagen, Danish Pediatric Asthma Center, Copenhagen University
Hospital, Gentofte, Denmark, 2 Department of Clinical Biochemistry, Aarhus University Hospital, Aarhus, Denmark
Abstract
Background: Epidemiological studies have suggested an association between maternal vitamin D dietary intake duringpregnancy and risk of asthma and allergy in the offspring. However, prospective clinical studies on vitamin D measured incord blood and development of clinical end-points are sparse.
Objective: To investigate the interdependence of cord blood 25-hydroxyvitamin D (25(OH)-Vitamin D) level andinvestigator-diagnosed asthma- and allergy-related conditions during preschool-age.
Methods: Cord blood 25(OH)-Vitamin D level was measured in 257 children from the Copenhagen Prospective Studies onAsthma in Childhood (COPSAC2000) at-risk mother-child cohort. Troublesome lung symptoms (TROLS), asthma, respiratoryinfections, allergic rhinitis, and eczema, at age 0–7 yrs were diagnosed exclusively by the COPSAC pediatricians strictlyadhering to predefined algorithms. Objective assessments of lung function and sensitization were performed repeatedlyfrom birth.
Results: After adjusting for season of birth, deficient cord blood 25(OH)-Vitamin D level (,50 nmol/L) was associated with a2.7-fold increased risk of recurrent TROLS (HR = 2.65; 95% CI = 1.02–6.86), but showed no association with respiratoryinfections or asthma. We saw no association between cord blood 25(OH)-Vitamin D level and lung function, sensitization,rhinitis or eczema. The effects were unaffected from adjusting for multiple lifestyle factors.
Conclusion: Cord blood 25(OH)-Vitamin D deficiency associated with increased risk of recurrent TROLS till age 7 years.Randomized controlled trials of vitamin D supplementation during pregnancy are needed to prove causality.
Citation: Chawes BL, Bønnelykke K, Jensen PF, Schoos A-MM, Heickendorff L, et al. (2014) Cord Blood 25(OH)-Vitamin D Deficiency and Childhood Asthma,Allergy and Eczema: The COPSAC2000 Birth Cohort Study. PLoS ONE 9(6): e99856. doi:10.1371/journal.pone.0099856
Editor: Yungling Leo Lee, National Taiwan University, Taiwan
Received March 7, 2014; Accepted May 19, 2014; Published June 12, 2014
Copyright: ! 2014 Chawes et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permitsunrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Data Availability: The authors confirm that all data underlying the findings are fully available without restriction. All data are included within the SupportingInformation files.
Funding: COPSAC is funded by private and public research funds listed on www.copsac.com. The Lundbeck Foundation; The Danish Strategic Research Council;the Pharmacy Foundation of 1991; Augustinus Foundation; the Danish Medical Research Council and The Danish Pediatric Asthma Centre provided the coresupport for COPSAC research center. No pharmaceutical company was involved in the study. The funders had no role in study design, data collection and analysis,decision to publish, or preparation of the manuscript.
Competing Interests: The authors have declared that no competing interests exist.
* E-mail: [email protected]
Introduction
Vitamin D deficiency caused by adaption of a more sedentaryindoor lifestyle and changing dietary habits has become a commonhealth problem in developed and developing countries world-wide[1] which has occurred in parallel with the ‘‘asthmaepidemic’’[2]. It is now evident that vitamin D possesses a panoplyof immune-regulatory functions that may protect against asthmaand allergy [3] and recent findings also suggest a role of vitamin Dfor fetal lung cell maturation and subsequent lung functiondevelopment [4]. These findings lend support to the hypothesisthat fetal vitamin D deficiency may promote a trajectory to
develop asthma and allergy [5]. A growing amount of studies haveattempted to prove this hypothesis but with inconsistent findings.
Some epidemiological studies have shown an associationbetween low maternal vitamin D intake during pregnancy andincreased risk of wheezy phenotypes in the offspring [6,7] whereasothers showed association with lower respiratory tract infectionsbut not with wheezy symptoms [8] or asthma [8,9]. Likewise, somestudies have shown that fetal vitamin D deficiency increases therisk of food allergy [10] and eczema [11,12] whereas others foundno association with allergic sensitization [12]. Thus, it remainsuncertain whether fetal vitamin D deficiency contributes to thedevelopment of childhood asthma, allergy and eczema. This maybe a result from the inaccuracy of determining fetal Vitamin D
PLOS ONE | www.plosone.org 1 June 2014 | Volume 9 | Issue 6 | e99856

exposure by questionnaire-based estimations of maternal dietaryintake of vitamin D and/or poorly defined case definitions.
The aim of the current study was to investigate the program-ming effect of cord blood vitamin D deficiency on the subsequentdevelopment of troublesome lung symptoms (TROLS), asthma,lower respiratory tract infections, lung function, allergy, andeczema during preschool age. We studied these aspects in thechildren from the Copenhagen Prospective Study on Asthma inChildhood (COPSAC2000) high-risk birth cohort [13–15] withlongitudinal clinical data determined from strict predefinedalgorithm-based clinical case definitions and repeated objectiveassessments of intermediary end-points.
Materials and Methods
Study DesignThe COPSAC2000 birth cohort is a single-center prospective
clinical study of 411 children born to mothers with physicianverified asthma recruited between 1998 and 2001 as previouslydescribed [13–15]. The children were enrolled at one month ofage and subsequently attended the clinical research unit forscheduled clinical investigations at six-monthly intervals as well asimmediately upon onset of any respiratory-, allergy- or skin-relatedsymptom. The pediatricians employed at the clinical research unit(not the family practitioners) were solely responsible for diagnosisand treatment of asthma, allergy, and eczema. At every visit a fullphysical examination was performed including lung functiontesting and history was obtained by parental interviews usingpredefined questions with closed response categories. Historyinformation was collected online during the visits and the objectivemeasurements were double checked against source data andsubsequently locked.
The study was conducted in accordance with the Declaration ofHelsinki and was approved by The Copenhagen Ethics Commit-tee (KF 01-289/96) and The Danish Data Protection Agency(2008-41-1754). Written informed consent was obtained from bothparents before enrollment.
Cord Blood Vitamin D MeasurementCord blood was collected by the midwives by needle puncture
from the umbilical cord vein obtaining an aliquot of approxi-mately 14 mL which was subsequently sent to the COPSACresearch unit, centrifuged for 10 min at 4300 rpm to separateserum, and thereafter frozen at 280uC until analysis.
The serum samples were transported on dry ice for duplicateanalyses for 25-hydroxyvitamin D2 (25(OH)-Vitamin D2) and25(OH)-Vitamin D3 at the Dept. of Clinical Biochemistry, AarhusUniversity Hospital, Denmark. Serum 25-hydroxyvitamin D levelswere analyzed by isotope dilution liquid chromatography-tandemmass spectrometry (LC-MS/MS) [16,17]. Calibrators traceable toNIST SRM 972 (Chromsystems, DE) were used. Mean coeffi-cients of variation (CV) for 25(OH)-Vitamin D3 were 6.4% and9.1% at levels of 66.5 and 21.1 nmol/L and for 25(OH)-VitaminD2 the CV values were 8.8% and 9.4% at levels of 41.2 and25.3 nmol/L. The average of the combined 25(OH)-Vitamin Dvalues was calculated and used in the analysis. If both 25(OH)-Vitamin D2 and 25(OH)-Vitamin D3 were under the detectionlevel, the combined value was defined as equal to 10 nmol/L.
Clinical Investigator-diagnosed End-pointsTroublesome lung symptoms (TROLS) were defined as
significant cough or wheeze or dyspnea and were explained to theparents as wheeze or whistling sounds, breathlessness, or recurrenttroublesome cough severely affecting the well-being of the child
and were recorded by the parents in a day-to-day diary chart as adichotomized daily score (yes/no) from birth till age 7 yrs [18].Recurrent TROLS was defined from the diaries at thescheduled or acute visits to the research clinic as five episodeswithin 6 months, each episode lasting at least three consecutivedays, or daily symptoms for four consecutive weeks [19,20].Children meeting these criteria were prescribed a 3-month trial ofbudesonide 200 mcg bid increasing to 6 and 12 months atsubsequent relapses.
Asthma at age 7 yrs was diagnosed according to internationalguidelines and was based on recurrent TROLS as defined above,symptoms judged by the COPSAC pediatricians to be typical ofasthma (e.g. exercise induced symptoms, prolonged nocturnalcough, recurrent cough outside common cold, symptoms causingwakening at night); in need of intermittent rescue use of inhaledb2-agonist; responding to a 3-month trial of inhaled corticosteroidsand relapsing when stopping treatment [14,15].
Lower respiratory tract infections (LRTI) includedoccurrence of pneumonia and/or acute bronchiolitis at age 0–3 yrs where such disorders are most prevalent. The diagnoses wereestablished at the acute visits to the clinic by the researchpediatricians based on clinical appearance regardless of identifiedpathogen(s) in accordance with predefined standard procedures[21] or if the child had been hospitalized for such disorders.
Allergic rhinitis was diagnosed at age 7 yrs based on clinicalinterviews of the parents on history of symptoms in the child’s 7th
year of life [22–24]. Rhinitis was defined as troublesome sneezingor blocked or runny nose in the past 12 months in periods withoutaccompanying cold or flu [25].
Eczema was diagnosed utilizing the Hanifin-Rajka criteria aspreviously detailed [26,27] obtaining age at onset data. Skinlesions were described at both scheduled and acute visits accordingto pre-defined morphology and localization.
Lung FunctionInfant spirometry was performed during sedation at age 1
month by applying the raised volume rapid thoraco-abdominalcompression technique as previously detailed [28–30]. The forcedexpiratory volume at 0.5 seconds (FEV0.5) and forced expiratoryflow at 50% of the forced vital capacity (FEF50) were used as lungfunction indices.
Spirometry at age 7 yrs was performed as previouslydetailed [31] using a pneumotachograph Masterscope Pneumosc-reen, system 754,916 spirometer (Erich Jaeger, Wurtzburg,Germany) for assessing FEV1 and maximal mid-expiratory flow(MMEF).
Bronchial responsiveness at age 1 month was assessed aspreviously detailed [29] by continuous measurements of transcu-taneuos oxygen saturation (PtcO2) during quadrupling methacho-line dose-steps and was defined as the provocative dose causing a15% drop in PtcO2 (PD15). Bronchial responsiveness at age 7 yrswas defined as the provocative dose of methacholine causing a20% drop in FEV1 from baseline (PD20) [31].
Allergy Intermediary End-pointsSpecific-IgE was measured at age K, 1K, 4, and 6 yrs against
16 common inhalant and food allergens (cat, dog, horse, birch,timothy grass, mugwort, house dust mites, moulds, hen’s egg,cow’s milk, fish, wheat, peanut, soybean, or shrimp) by Immuno-CAP assay (Pharmacia Diagnostics AB, Uppsala, Sweden).Allergic sensitization was defined as specific-IgE $0.35 kU/L[32,33] for (1) any of the tested allergens, (2) any inhaled allergen,and (3) any food allergen.
Cord Blood 25(OH)-Vitamin D and Childhood Asthma
PLOS ONE | www.plosone.org 2 June 2014 | Volume 9 | Issue 6 | e99856

Total-IgE was measured at age K, 1K, 4, and 6 yrs byImmunoCAP (Pharmacia Diagnostics AB, Uppsala, Sweden) witha detection limit of 2 kU/L [33].
CovariatesBlood sampling season was categorized as: winter (Dec-
Feb), spring (March-May), summer (June-Aug) and fall (Sep-Nov).Demographics included child gender, birth BMI, maternal age atbirth of proband, and household income (low: ,50,000J,medium: 50,000–80,000J, high.80,000J). Postnatal expo-sures were older siblings (yes/no), length of solely breastfeeding,age at start in daycare, and environmental tobacco exposuremeasured objectively as hair nicotine level at age 1 yr [34].
Statistical AnalysisThe combined cord blood 25(OH)-Vitamin D value was
analyzed as a continuous variable per 100 nmol/L decrease aswell as categorized as: deficient (,50 nmol/L), insufficient (50–75 nmol/L), sufficient (.75 nmol/L), based on biologicallyrelevant levels according to recent studies on multiple healthoutcomes [1].
Distribution of baseline characteristics within the study groupand the drop-out analysis was done with univariable parametricand non-parametric tests such as x2, Fischer’s exact test, t-test, andKruskal-Wallis rank sum test.
The association of cord blood 25(OH)-Vitamin D level with ageat onset end-points (recurrent TROLS, LRTI, eczema) wasestimated as hazard ratios by Cox regression and visualized byKaplan-Meier curves for the categorized 25(OH)-Vitamin Dlevels. The effect of 25(OH)-Vitamin D level on the cross-sectionalend-points, e.g. asthma and allergic rhinitis, was estimated as oddsratios by logistic regression. The association between 25(OH)-Vitamin D and cross-sectional continuous outcomes such as lungfunction incentives was explored by general linear models (GLM).The effect on outcome measures with repetitive assessments(allergic sensitization, total-IgE) was modeled using generalestimating equations (GEE) applied to compute the overall oddsratio utilizing compiled data from all four time points (K, 1K, 4,6 yrs). PD15, PD20 and total-IgE were log-transformed and z-scores were calculated for FEV0.5, FEV1, FEF50 and MMEF priorto analyses.
Additional adjusted effect estimates were calculated withmultivariable models including all covariates significantly associ-ated with cord blood 25(OH)-Vitamin D level (p#0.05) in themodels. All analyses were adjusted for blood sampling season [12].Results are reported with 95% confidence intervals (CI) inbrackets, a p-value#0.05 is considered significant. Analyses weredone using SAS version 9.2 (SAS Institute, Cary, NC).
The core data of the manuscript is available online in Data S1.
Results
Baseline CharacteristicsCord blood was available for 25(OH)-Vitamin D analysis in 257
(63%) of the 411 children in the COPSAC2000 cohort. Charac-teristics of the children with and without available cord bloodsamples are given in Table 1. Children in the drop-out groupwithout available cord blood came from families with significantlylower household income (p = 0.01), but did not differ from thestudy group in any other baseline characteristics studied.
The median cord blood 25(OH)-Vitamin D level in the studygroup was 47.6 nmol/L (range, 10–145 nmol/L). The distributionof cord blood 25(OH)-Vitamin D concentrations was: 132 (53%)children with deficient levels, 82 (32%) with insufficient, and 39
(15%) with sufficient levels. Concentration of cord blood 25(OH)-Vitamin D varied significantly with season of birth (p,0.01) withmost 25(OH)-Vitamin D deficient children born during winter andmost sufficient children born during summer. Children withdeficient vs. sufficient levels were born to younger mothers(median age at birth, 29.5 yrs vs. 30.8 yrs; p = 0.02), had fewersiblings (children with older siblings, 44% vs. 50%; p = 0.02), andhad a higher exposure to environmental tobacco smoke (medianhair nicotine level at age 1 yr, 0.84 vs. 0.47 ng/mg; p = 0.03).
Cord Blood 25(OH)-Vitamin D Level vs. Asthma-relatedOutcomes and LRTI
Recurrent TROLS was diagnosed in 24% (N = 61) of thechildren at age 0–7 yrs. The cumulative prevalence rates were 4%(N = 11) at age 0–1 yrs, 14% (N = 35) at 0–2 yrs, 16% (N = 42) at0–3 yrs, 19% (N = 50) at 0–4 yrs, 22% (N = 57) at 0–5 yrs, and23% (N = 59) at 0–6 yrs. Cord blood 25(OH)-Vitamin D levelswere lower in children developing recurrent TROLS as illustratedin Figure 1. Having deficient vs. sufficient cord blood 25(OH)-Vitamin D level was associated with a 2.7-fold increased risk ofrecurrent TROLS (hazard ratio (HR), 2.65; 95% CI = 1.02–6.86;p = 0.04). The association was borderline significant whenadjusting for multiple confounding factors but with unchangedeffect estimates (aHR, 2.50; 95% CI, 0.95–6.57; p = 0.06).
Asthma at age 7 yrs was diagnosed in 16% (N = 34) of thechildren. 25(OH)-Vitamin D levels in cord blood showed noassociation with asthma at age 7 yrs (Table 2). In addition, cordblood 25(OH)-Vitamin D level was not suppressed in the subgroupof children experiencing recurrent TROLS who were subsequent-ly diagnosed with asthma at age 7 yrs (N = 31): OR 2.25 (95% CI,0.60–8.49; p = 0.21) for deficient vs. sufficient levels.
LRTI occurred in 56% (N = 119) of the study group with amean of 1.2 (SD, 1.6) episodes per child till age 3 yrs. Cord blood25(OH)-Vitamin D deficiency did not modify time to first LRTI(Figure 2) nor was the number of episodes affected by cord blood25(OH)-Vitamin D level (Table 2).
Association between Cord Blood 25(OH)-Vitamin D Leveland Lung Function
Cord blood 25(OH)-Vitamin D level was not associated withforced flows assessed at age 1mo (FEV0.5, FEF50) or 7 yrs (FEV1,MMEF) nor bronchial responsiveness to methacholine at any agepoint (PD15, PD20) (Table 2).
Relationship between Cord Blood 25(OH)-Vitamin D andAllergic Outcomes (Table 3)
Specific-IgE. Allergic sensitization at any of the four mea-suring points (K, 1K, 4, 6 yrs) was present in 35% (N = 88) forany of the investigated allergens, in 26% (N = 64) for any foodallergens, and in 21% (N = 52) for any inhaled allergen. There wasno significant association between cord blood 25(OH)-Vitamin Dlevel and allergic sensitization throughout childhood althoughthere was a tendency of Vitamin D deficiency being associatedwith decreased risk of sensitization.
Total-IgE. Cord blood 25(OH)-Vitamin D level was notassociated with level of total-IgE throughout childhood.
Allergic rhinitis was diagnosed in 12% (N = 23) at age 7 yrs.Deficient vs. sufficient cord blood 25(OH)-Vitamin D level seemedto be associated with a reduced risk of allergic rhinitis at age 7 yrsbut this was not significant.
Cord Blood 25(OH)-Vitamin D and Childhood Asthma
PLOS ONE | www.plosone.org 3 June 2014 | Volume 9 | Issue 6 | e99856

Table 1. Baseline characteristics of children with and without available cord blood for 25(OH)-Vitamin D analysis.
Cord blood 25(OH)-Vitamin D (nmol/l), N = 257No cord blood available,N = 154
Deficient: ,50 Insufficient: 50–75 Sufficient:.75 P* P**
Vitamin D cord blood (N) 53% (136) 32% (82) 15% (39) - - -
DEMOGRAFICS
Maternal age at birth1, median (range) 29.5 yrs (20.9–38.9) 29.2 yrs (22.6–41.1) 30.8 yrs (22.1–37.8) 0.02 30.0 (19.2–41.2) 0.31
Household income2 (N) 0.25 0.01
Low, ,50.000E 28% (35) 25% (19) 13% (5) 37% (53)
Medium, 50.000–80.000E 52% (65) 55% (42) 53% (20) 38% (55)
High, .80.000E 21% (26) 20% (15) 34% (13) 25% (36)
Boy2 (N) 45% (61) 55% (45) 46% (18) 0.34 51% (79) 0.55
Birth BMI1, median (range) 12.8 kg/m2 (7.0–16.3) 12.7 kg/m2 (10.0–16.6) 12.8 kg/m2 (9.6–15.1) 0.98 12.6 kg/m2 (8.4–16.5) 0.35
Birth season1 (N) ,0.01 0.39
Winter 30% (41) 15% (12) 18% (7) 23% (35)
Spring 24% (33) 21% (17) 15% (6) 19% (30)
Summer 21% (28) 33% (27) 49% (19) 24% (37)
Fall 25% (34) 32% (26) 18% (7) 34% (52)
POSTNATAL EXPOSURES
Older siblings2 (N) 44% (55) 26% (20) 50% (19) 0.02 40% (58) 0.87
Breastfeeding3+4, median (range) 123 (0–243) 121 (0–274) 137 (0–266) 0.14 120 (0–244) 0.14
Daycare4+5, median (range) 339 (140–1074) 308 (156–674) 286 (179–578) 0.46 355 (127–1003) 0.16
Nicotine in hair 1 yr4, median (range) 0.84 ng/mg (0.06–30.9) 0.53 ng/mg (0.03–43.5) 0.47 ng/mg (0.1–12.9) 0.03 0.95 (0.03–103.9) 0.14
*P-value for the distribution of characteristics within the groups of 25(OH)-Vitamin D.**P-value for the distribution of characteristics between children with and without available 25(OH)-Vitamin D data.1Linear regression; 2Chi-Square test; 3Days solely breastfed; 4Kruskal-Wallis rank sum test; 5Age at start in daycare.doi:10.1371/journal.pone.0099856.t001
Figure 1. Kaplan Meier survival curve showing the risk of developing recurrent troublesome lung symptoms (TROLS) at age 0–7 yrsstratified by cord blood 25(OH)-Vitamin D level.doi:10.1371/journal.pone.0099856.g001
Cord Blood 25(OH)-Vitamin D and Childhood Asthma
PLOS ONE | www.plosone.org 4 June 2014 | Volume 9 | Issue 6 | e99856

Ta
ble
2.
Co
rdb
loo
d25
(OH
)-V
itam
inD
vs.
asth
ma-
rela
ted
ou
tco
mes
,lo
wer
resp
irat
ory
trac
tin
fect
ion
san
dlu
ng
fun
ctio
n.
Co
rdb
loo
d2
5(O
H)-
Vit
am
inD
,5
0v
s.
75
nm
ol/
LP
,5
0v
s.
75
nm
ol/
LA
dju
ste
d*
PP
er
10
0n
mo
l/L
de
cre
ase
PP
er
10
0n
mo
l/L
de
cre
ase
Ad
just
ed
*P
Ast
hm
a-r
ela
ted
ou
tco
me
s
Rec
urr
ent
TRO
LS,
0–7
yrs1
+22
.65
(1.0
2to
6.8
6)
0.0
42
.50
(0.9
5to
6.5
7)
0.0
62
.65
(0.8
3to
8.5
0)
0.1
02.
27(0
.65
to7.
90)
0.20
Ast
hm
a,7
yrs3
1.60
(0.4
9to
5.22
)0.
311.
63(0
.47
to5.
61)
0.38
1.18
(0.2
5to
5.58
)0.
841.
01(0
.18
to5.
80)
0.99
LR
TI4
Tim
eto
first
LRTI
,0–
3yr
s1.
08(0
.63
to1.
85)
0.78
1.08
(0.6
2to
1.87
)0.
791.
17(0
.54
to2.
52)
0.69
1.05
(0.4
6to
2.39
)0.
91
No
.o
fLR
TI,
0–3
yrs5
1.07
(0.6
6to
1.75
)0.
780.
94(0
.57
to1.
55)
0.81
1.08
(0.5
3to
2.20
)0.
830.
75(0
.35
to1.
58)
0.69
Lu
ng
fun
ctio
n
z-FE
V0.
5,1m
o6
+70.
02(2
0.10
to0.
15)
0.73
20.
01(2
0.14
to0.
13)
0.94
0.01
(20.
02to
0.04
)0.
400.
01(2
0.02
to0.
04)
0.70
z-FE
V1,
7yr
s0.
04(2
0.09
to0.
18)
0.54
0.07
(20.
08to
0.22
)0.
370.
02(2
0.02
to0.
06)
0.28
0.02
(20.
01to
0.06
)0.
24
z-FE
F50,
1mo
20.
03(2
0.15
to0.
09)
0.63
20.
06(2
0.18
to0.
07)
0.38
0.01
(20.
02to
0.04
)0.
420.
00(2
0.03
to0.
03)
0.82
z-M
MEF
,7
yrs
20.
04(2
0.17
to0.
09)
0.55
20.
05(2
0.18
to0.
09)
0.50
0.00
(20.
03to
0.03
)0.
902
0.01
(20.
04to
0.02
)0.
62
log
PD
15,
1mo
80.
02(2
0.05
to0.
09)
0.62
0.01
(20.
07to
0.03
)0.
920.
01(2
0.01
to0.
02)
0.66
0.00
(20.
01to
0.02
)0.
82
log
PD
20,
7yr
s90.
02(2
0.08
to0.
12)
0.68
0.03
(20.
07to
0.14
)0.
520.
01(2
0.02
to0.
04)
0.41
0.01
(20.
02to
0.04
)0.
40
*Ad
just
edfo
rm
oth
er’s
age
atb
irth
,b
loo
dsa
mp
ling
seas
on
,o
lder
sib
ling
s,an
dh
air
nic
oti
ne
leve
lat
age
1yr
.1TR
OLS
=Tr
ou
ble
som
elu
ng
sym
pto
ms;
2C
ox
reg
ress
ion
:h
azar
ds
rati
o(9
5%C
I);3Lo
gis
tic
reg
ress
ion
:o
dd
sra
tio
(95%
CI);
4Lo
wer
resp
irat
ory
trac
tin
fect
ion
s;5P
ois
son
reg
ress
ion
:in
cid
ence
risk
rati
o(9
5%C
I);6A
lllu
ng
fun
ctio
nan
alys
esar
ed
on
ew
ith
gen
eral
linea
rm
od
els:b
-co
effic
ents
(95%
CI);
7z
refe
rsto
the
calc
ula
ted
z-sc
ore
;8P
D1
5re
fers
toth
ep
rovo
cati
ved
ose
of
met
hac
ho
line
resu
ltin
gin
a15
%d
ecre
ase
intr
ansc
uta
neu
os
oxy
gen
satu
rati
on
(Ptc
O2)
fro
mb
asel
ine;
9P
D2
0re
fers
toth
ep
rovo
cati
ved
ose
of
met
hac
ho
line
resu
ltin
gin
a20
%d
ecre
ase
inFE
V1
fro
mb
asel
ine.
do
i:10.
1371
/jo
urn
al.p
on
e.00
9985
6.t0
02
Cord Blood 25(OH)-Vitamin D and Childhood Asthma
PLOS ONE | www.plosone.org 5 June 2014 | Volume 9 | Issue 6 | e99856

Cord Blood 25(OH)-Vitamin D Level and Risk of EczemaEczema was diagnosed in 42% (N = 109) of the study group.
Cord blood 25(OH)-Vitamin D level was not significantlyassociated with the risk of eczema during preschool age althoughthe effect estimates suggested an increased risk by deficient cordblood levels (See Table 3 and Figure 3).
Discussion
Principal FindingsDeficient cord blood 25(OH)-Vitamin D level was associated
with a more than doubled risk of developing TROLS duringpreschool age in children of the Danish COPSAC2000 high-riskbirth cohort study. This finding supports the theory that deficient25(OH)-Vitamin D exposure in utero has a programming effect onthe immune maturation thus predisposing to development ofchronic inflammation.
Strengths and Limitations of the StudyThe primary strength of the study is the seven years of clinical
assessments of our birth cohort with longitudinal clinical deepphenotyping and standardized diagnoses solely performed by theCOPSAC research pediatricians. Repeated objective measure-ments along with day-to-day respiratory symptom diary recordingsthrough the first seven years of life provided strong age at onsetdata which is a major advantage compared to studies using cross-sectional unspecific community-based diagnoses [6,7,11].
Another significant strength is the objective assessment of fetal25(OH)-Vitamin D exposure by measuring the concentration inthe cord blood. Even though cord blood 25(OH)-Vitamin D levelprimarily reflects recent exposure during 3rd trimester and may becontaminated by maternal blood, this biological measure is a moreaccurate estimate of fetal 25(OH)-Vitamin D exposure comparedto approximations from questionnaires on maternal dietary andsupplementary intake since only 10% of vitamin D is obtainedthrough diet [35].
It is also a strength of the analyses that environmental exposureassessments were comprehensive including hair nicotine level [34]as a validated objective measure of tobacco smoke exposureallowing for robust confounder adjustment. In agreement withother studies we found a marked seasonal variation in cord blood25(OH)-Vitamin D level [12] as well as significant influence ofvarious lifestyle factors such as passive smoking, maternal age atdelivery, and older siblings [6,7]. We adjusted for season of bloodsampling (i.e. sunlight exposure) which is a major determinant ofserum 25(OH)-Vitamin D level [12]. We did not adjust ouranalyses for ethnicity [1] as 98% of the study group is of Caucasianorigin.
The study is limited from the at-risk nature of the cohort as allmothers have a history of asthma which may limit thegeneralizability of our findings to other populations. However,this should not affect our ability to analyze the relationshipbetween 25(OH)-Vitamin D levels and development of asthmaand allergy-related traits within the cohort, and our findings are inline with studies of unselected populations [7,11].
We expected to see the largest effects in children with deficientcompared to sufficient cord blood 25(OH)-Vitamin D levels. Anessential limitation of the study is therefore the study sample size asonly 15% had sufficient cord blood levels, equivalent to 39participants, which results in lack of statistical power and alikelihood of overlooking the true effect of 25(OH)-Vitamin Dexposure in fetal life on development of childhood asthma andallergy.
InterpretationOur finding that deficient cord blood 25(OH)-Vitamin D level
was associated with a more than doubled risk of developingrecurrent TROLS during preschool age is in line with a range ofepidemiological studies utilizing maternal dietary vitamin D intakeduring pregnancy as a surrogate measure of fetal vitamin Dexposure [6,7,36]. However, studies of cord blood 25(OH)-Vitamin D are still sparse [9,11,12] and our study is the onlyone with a full clinical follow-up till age 7 yrs at a single research
Figure 2.Kaplan Meier survival curve showing the risk of developing lower respiratory tract infections (LRTI) at age 0–3 yrsstratified by cord blood 25(OH)-Vitamin D level.doi:10.1371/journal.pone.0099856.g002
Cord Blood 25(OH)-Vitamin D and Childhood Asthma
PLOS ONE | www.plosone.org 6 June 2014 | Volume 9 | Issue 6 | e99856

unit employed solely with research pediatricians. Among availablecord blood studies, one study found no association with recurrentwheeze [12], but only assessed the children at age 1 yr where sucha diagnosis is quite infrequent in an unselected population. In linewith our findings, an increased risk of deficient levels has beenreported for early transient wheeze [11] and for development ofwheeze till age 5 yrs [9].
It has been speculated that deficient neonatal vitamin D levelmainly increases the risk of early transient wheezing exerting theeffect through immune-modulatory mechanisms [3] whichincrease the frequency of respiratory tract infections and thusvirus-induced wheezing [8,9]. We found that low cord blood levelwas associated with a significantly increased risk of early recurrentTROLS, but saw no association with occurrence of earlychildhood respiratory infections.
We found no significant association between cord blood25(OH)-Vitamin D level and subsequent development of allergicsensitization or allergic rhinitis although the effect estimatesshowed a trend of decreased risk of allergic outcomes by deficientVitamin D levels which has also been suggested by others [37].
We did not see any significant association between fetal vitaminD exposure and development of eczema although low cord bloodlevels seemed to associate with an increased risk. This finding issupported by other cord blood studies demonstrating that deficientvitamin D levels increase the risk of eczema both physiciandiagnosed and questionnaire-based [11,12].
The immune-regulatory properties of vitamin D exertedthrough e.g. promotion of pro-inflammatory cytokines andinduction of regulatory T cells include an ability to shift theTh1/Th2 balance with capacity to inhibit both Th1 and Th2-typeresponses leading to opposite effects on disease development, i.e.enhancing vs. reducing the risk [38]. The complex interplaybetween the genetic makeup, the early life milieu, and the timingof sufficient vitamin D exposure during maturation of theimmature immune system may determine the direction of theimmune-modulatory properties of Vitamin D. Additional pro-gramming effects of fetal vitamin D exposure apart from immune-modulation might be alterations of the airway microbiome frome.g. induction of the endogenous antimicrobial peptide cathelicidinin bronchial epithelial cells [39].
Overall, our study suggests an association between deficient fetal25(OH)-Vitamin D exposure and development of recurrentTROLS during preschool age with a sizable effect estimate.However, despite the rigorously clinically determined diagnoses inthis study and the objective assessment of cord blood 25(OH)-Vitamin D, the question of causality cannot be answered by anobservational study. Thus, acknowledging that and the possibilityof residual lifestyle confounding, this study prompts the perfor-mance of randomized controlled trials of maternal supplementa-tion of vitamin D during pregnancy to shed light on the possiblecausative and thus modifiable effect of fetal vitamin D deficiencyfor development of asthma, allergy and eczema. Several random-ized controlled trials are currently being conducted by our groupand others (clinicalTrials.gov identification numbers:NCT00856947, NCT00920621).
ConclusionThis study shows an interdependence of 25(OH)-Vitamin D
deficiency in fetal life and occurrence of recurrent TROLS duringpreschool in children of the at-risk COPSAC2000 cohort. Furtherresearch is required to establish whether vitamin D supplemen-tation during pregnancy can prevent development and severity ofsuch disorders.
Ta
ble
3.
Co
rdb
loo
d25
(OH
)-V
itam
inD
vs.
alle
rgic
ou
tco
mes
and
ecze
ma
at0–
7yr
s.
Co
rdb
loo
d2
5(O
H)-
Vit
am
inD
,5
0v
s.
75
nm
ol/
LP
,5
0v
s.
75
nm
ol/
LA
dju
ste
d*P
Pe
r1
00
nm
ol/
Ld
ecr
ea
seP
Pe
r1
00
nm
ol/
Ld
ecr
ea
seA
dju
ste
d*
P
All
erg
ico
utc
om
es
An
yse
nsi
tiza
tio
n,s
pec
-Ig
E,0–
6yr
1+2
0.96
(0.4
3–2.
16)
0.93
0.96
(0.6
4–2.
31)
0.93
0.52
(0.1
7–1.
52)
0.23
0.64
(0.1
9–2.
12)
0.47
Foo
dse
nsi
tiza
tio
n,
spec
-Ig
E,0–
6yr
20.
86(0
.34–
2.18
)0.
740.
94(0
.35–
2.53
)0.
910.
47(0
.13–
1.68
)0.
250.
63(0
.16–
2.57
)0.
53
Inh
aled
sen
siti
zati
on
,sp
ec-I
gE,
0–6
yr2
0.97
(0.4
7–2.
01)
0.94
1.20
(0.5
4–2.
67)
0.65
0.36
(0.0
9–1.
55)
0.17
0.43
(0.0
9–2.
05)
0.29
Tota
l-Ig
E,0–
6yr
20.
98(0
.66–
1.45
)0.
910.
98(0
.65–
1.48
)0.
930.
86(0
.46–
1.60
)0.
630.
83(0
.42–
1.65
)0.
60
Alle
rgic
rhin
itis
,7
yr3
0.40
(0.1
2–1.
26)
0.32
0.44
(0.1
3–1.
49)
0.47
0.33
(0.0
6–1.
92)
0.22
0.29
(0.0
4–2.
14)
0.23
Ecz
em
a
Tim
eto
ecze
ma,
0–7
yr4
0.97
(0.5
6–1.
69)
0.97
1.13
(0.6
3–2.
01)
0.69
0.88
(0.4
1–1.
92)
0.76
1.04
(0.4
4–2.
41)
0.94
Ecze
ma,
7yr
31.
80(0
.56–
5.79
)0.
682.
00(0
.59–
6.76
)0.
941.
39(0
.33–
5.82
)0.
651.
25(0
.27–
5.82
)0.
78
*Ad
just
edfo
rm
oth
er’s
age
atb
irth
,b
loo
dsa
mp
ling
seas
on
,o
lder
sib
ling
s,an
dh
air
nic
oti
ne
leve
lat
age
1yr
.1Sp
ecifi
c-Ig
E$0.
35kU
/mL
agai
nst
any
of:
do
g,c
at,h
ors
e,b
irch
,tim
oth
yg
rass
,mu
gw
ort
,ho
use
du
stm
ites
,mo
lds,
milk
,eg
g,w
hea
t,so
yab
ean
,co
dan
dp
ean
ut;
2G
EEm
od
elin
clu
din
gd
ata
fro
mag
eK
,1K
,4an
d6
yrs:
OR
(95%
CI);
3Lo
gis
tik
reg
ress
ion
:o
dd
sra
tio
(95%
CI);
4C
ox
reg
ress
ion
:h
azar
dra
tio
(95%
CI).
do
i:10.
1371
/jo
urn
al.p
on
e.00
9985
6.t0
03
Cord Blood 25(OH)-Vitamin D and Childhood Asthma
PLOS ONE | www.plosone.org 7 June 2014 | Volume 9 | Issue 6 | e99856

Supporting Information
Data S1 Core data of the manuscript.(XLS)
Acknowledgments
We gratefully express our gratitude to the children and families of theCOPSAC2000 cohort study for all their support and commitment. Weacknowledge and appreciate the unique efforts of the COPSAC researchteam.
Author Contributions
Conceived and designed the experiments: BLC KB HB. Performed theexperiments: BLC KB PFJ AMS. Analyzed the data: BLC KB PFJ AMSHB. Contributed reagents/materials/analysis tools: LH. Wrote the paper:BLC KB PFJ AMS LH HB. The guarantor of the study who has beenresponsible for the integrity of the work as a whole, from conception anddesign to conduct of the study and acquisition of data, analysis andinterpretation of data and writing of the manuscript: HB. Responsible fordata analysis, interpretation and writing the manuscript: BLC KB PFJAMS LH. Wrote the first draft of the manuscript: BC. No honorarium,grant, or other form of payment was given to anyone to produce themanuscript. All co-authors have contributed substantially to the analysesand interpretation of the data, and have provided important intellectualinput and approval of the final version of the manuscript.
References
1. Holick MF (2007) Vitamin D deficiency. N Engl J Med 357: 266–281.2. Eder W, Ege MJ, von ME (2006) The asthma epidemic. N Engl J Med 355:
2226–2235.3. Hollams EM (2012) Vitamin D and atopy and asthma phenotypes in children.
Curr Opin Allergy Clin Immunol 12: 228–234.4. Zosky GR, Berry LJ, Elliot JG, James AL, Gorman S, et al. (2011) Vitamin D
deficiency causes deficits in lung function and alters lung structure. Am J RespirCrit Care Med 183: 1336–1343.
5. Litonjua AA, Weiss ST (2007) Is vitamin D deficiency to blame for the asthmaepidemic? J Allergy Clin Immunol 120: 1031–1035.
6. Camargo CA, Jr., Rifas-Shiman SL, Litonjua AA, Rich-Edwards JW, Weiss ST,et al. (2007) Maternal intake of vitamin D during pregnancy and risk of recurrentwheeze in children at 3 y of age. Am J Clin Nutr 85: 788–795.
7. Devereux G, Litonjua AA, Turner SW, Craig LC, McNeill G, et al. (2007)Maternal vitamin D intake during pregnancy and early childhood wheezing.Am J Clin Nutr 85: 853–859.
8. Morales E, Romieu I, Guerra S, Ballester F, Rebagliato M, et al. (2012)Maternal vitamin D status in pregnancy and risk of lower respiratory tractinfections, wheezing, and asthma in offspring. Epidemiology 23: 64–71.
9. Camargo CA, Jr., Ingham T, Wickens K, Thadhani R, Silvers KM, et al. (2011)Cord-blood 25-hydroxyvitamin D levels and risk of respiratory infection,wheezing, and asthma. Pediatrics 127: e180–e187.
10. Liu X, Arguelles L, Zhou Y, Wang G, Chen Q, et al. (2013) Longitudinaltrajectory of vitamin D status from birth to early childhood in the developmentof food sensitization. Pediatr Res 74: 321–326.
11. Baiz N, rgent-Molina P, Wark JD, Souberbielle JC, nnesi-Maesano I (2013)Cord serum 25-hydroxyvitamin D and risk of early childhood transientwheezing and atopic dermatitis. J Allergy Clin Immunol.
12. Jones AP, Palmer D, Zhang G, Prescott SL (2012) Cord blood 25-hydroxyvitamin D3 and allergic disease during infancy. Pediatrics 130:e1128–e1135.
13. Bisgaard H (2004) The Copenhagen Prospective Study on Asthma in Childhood(COPSAC): design, rationale, and baseline data from a longitudinal birth cohortstudy. Ann Allergy Asthma Immunol 93: 381–389.
14. Bisgaard H, Hermansen MN, Loland L, Halkjaer LB, Buchvald F (2006)Intermittent inhaled corticosteroids in infants with episodic wheezing.N Engl J Med 354: 1998–2005.
15. Bisgaard H, Hermansen MN, Buchvald F, Loland L, Halkjaer LB, et al. (2007)Childhood asthma after bacterial colonization of the airway in neonates.N Engl J Med 357: 1487–1495.
16. Maunsell Z, Wright DJ, Rainbow SJ (2005) Routine isotope-dilution liquidchromatography-tandem mass spectrometry assay for simultaneous measure-ment of the 25-hydroxy metabolites of vitamins D2 and D3. Clin Chem 51:1683–1690.
17. Hojskov CS, Heickendorff L, Moller HJ (2010) High-throughput liquid-liquidextraction and LCMSMS assay for determination of circulating 25(OH) vitaminD3 and D2 in the routine clinical laboratory. Clin Chim Acta 411: 114–116.
18. Bisgaard H, Pipper CB, Bonnelykke K (2011) Endotyping early childhoodasthma by quantitative symptom assessment. J Allergy Clin Immunol.
19. Bisgaard H, Bonnelykke K, Sleiman PM, Brasholt M, Chawes B, et al. (2009)Chromosome 17q21 gene variants are associated with asthma and exacerbationsbut not atopy in early childhood. Am J Respir Crit Care Med 179: 179–185.
20. Chawes BL, Buchvald F, Bischoff AL, Loland L, Hermansen M, et al. (2010)Elevated Exhaled Nitric Oxide in High-risk Neonates Precedes Transient Earlybut not Persistent Wheeze. Am J Respir Crit Care Med 182: 138–142.
Figure 3. Kaplan Meier survival curve showing the risk of developing eczema at age 0–7 yrs stratified by cord blood 25(OH)-Vitamin D level.doi:10.1371/journal.pone.0099856.g003
Cord Blood 25(OH)-Vitamin D and Childhood Asthma
PLOS ONE | www.plosone.org 8 June 2014 | Volume 9 | Issue 6 | e99856

21. Vissing NH, Chawes BL, Bisgaard H (2013) Increased risk of pneumonia andbronchiolitis after bacterial colonization of the airways as neonates. Am J RespirCrit Care Med 188: 1246–1252.
22. Chawes BL, Kreiner-Moller E, Bisgaard H (2009) Objective assessments ofallergic and nonallergic rhinitis in young children. Allergy 64: 1547–1553.
23. Chawes BL, Kreiner-Moller E, Bisgaard H (2010) Upper and Lower AirwayPatency are Associated in Young Children. Chest 137: 1332–1337.
24. Chawes BL, Bonnelykke K, Kreiner-Moller E, Bisgaard H (2010) Children withallergic and nonallergic rhinitis have a similar risk of asthma. J Allergy ClinImmunol 126: 567–573.
25. Braun-Fahrlander C, Wuthrich B, Gassner M, Grize L, Sennhauser FH, et al.(1997) Validation of a rhinitis symptom questionnaire (ISAAC core questions) ina population of Swiss school children visiting the school health services.SCARPOL-team. Swiss Study on Childhood Allergy and Respiratory Symptomwith respect to Air Pollution and Climate. International Study of Asthma andAllergies in Childhood. Pediatr Allergy Immunol 8: 75–82.
26. Bisgaard H, Simpson A, Palmer CN, Bonnelykke K, McLean I, et al. (2008)Gene-environment interaction in the onset of eczema in infancy: filaggrin loss-of-function mutations enhanced by neonatal cat exposure. PLoS Med 5: e131.
27. Halkjaer LB, Loland L, Buchvald FF, Agner T, Skov L, et al. (2006)Development of atopic dermatitis during the first 3 years of life: the Copenhagenprospective study on asthma in childhood cohort study in high-risk children.Arch Dermatol 142: 561–566.
28. Chawes BL, Poorisrisak P, Johnston SL, Bisgaard H (2012) Neonatal bronchialhyperresponsiveness precedes acute severe viral bronchiolitis in infants. J AllergyClin Immunol 130: 354–361.
29. Loland L, Buchvald FF, Halkjaer LB, Anhoj J, Hall GL, et al. (2006) Sensitivityof bronchial responsiveness measurements in young infants. Chest 129: 669–675.
30. Loland L, Bisgaard H (2008) Feasibility of repetitive lung function measurementsby raised volume rapid thoracoabdominal compression during methacholinechallenge in young infants. Chest 133: 115–122.
31. Bisgaard H, Jensen SM, Bonnelykke K (2012) Interaction between Asthma andLung Function Growth in Early Life. Am J Respir Crit Care Med.
32. Ballardini N, Nilsson C, Nilsson M, Lilja G (2006) ImmunoCAP PhadiatopInfant—a new blood test for detecting IgE sensitisation in children at 2 years ofage. Allergy 61: 337–343.
33. Wickman M, Ahlstedt S, Lilja G, van Hage HM (2003) Quantification of IgEantibodies simplifies the classification of allergic diseases in 4-year-old children.A report from the prospective birth cohort study—BAMSE. Pediatr AllergyImmunol 14: 441–447.
34. Sorensen M, Bisgaard H, Stage M, Loft S (2007) Biomarkers of exposure toenvironmental tobacco smoke in infants. Biomarkers 12: 38–46.
35. Sichert-Hellert W, Wenz G, Kersting M (2006) Vitamin intakes fromsupplements and fortified food in German children and adolescents: resultsfrom the DONALD study. J Nutr 136: 1329–1333.
36. Miyake Y, Sasaki S, Tanaka K, Hirota Y (2010) Dairy food, calcium andvitamin D intake in pregnancy, and wheeze and eczema in infants. Eur Respir J35: 1228–1234.
37. Wjst M (2006) The vitamin D slant on allergy. Pediatr Allergy Immunol 17:477–483.
38. Litonjua AA (2009) Childhood asthma may be a consequence of vitamin Ddeficiency. Curr Opin Allergy Clin Immunol 9: 202–207.
39. Yim S, Dhawan P, Ragunath C, Christakos S, Diamond G (2007) Induction ofcathelicidin in normal and CF bronchial epithelial cells by 1,25-dihydroxyvi-tamin D(3). J Cyst Fibros 6: 403–410.
Cord Blood 25(OH)-Vitamin D and Childhood Asthma
PLOS ONE | www.plosone.org 9 June 2014 | Volume 9 | Issue 6 | e99856

doi: 10.1111/j.1365-2222.2012.04048.x Clinical & Experimental Allergy, 42, 1596–1603
ORIGINAL ARTICLE Clinical Mechanisms in Allergic Disease© 2012 Blackwell Publishing Ltd
Cord blood Th2-related chemokine CCL22 levels associate with elevatedtotal-IgE during preschool ageN. V. Følsgaard1, B. L. K. Chawes1, K. Bønnelykke1, M. C. Jenmalm2 and H. Bisgaard1
1Copenhagen Prospective Studies on Asthma in Childhood, Copenhagen University Hospital, Gentofte, Denmark and 2Department of Clinical andExperimental Medicine, Linköping University, Linköping, Sweden
Clinical &Experimental
Allergy
Correspondence:Professor Hans BisgaardCopenhagen Prospective Studies on
Asthma in Childhood
Copenhagen University HospitalLedreborg Alle 34
DK-2820 Gentofte, Copenhagen,Denmark.
E-mail: [email protected]
Cite this as: N. V. Følsgaard,B. L. K. Chawes, K. Bønnelykke,
M. C. Jenmalm and H. Bisgaard,Clinical & Experimental Allergy,2012 (42) 1596–1603.
SummaryBackground Early-life immune deviation is suspected in the inception of atopic disease.Objective To investigate the association between cord blood chemokines and thesubsequent development of atopic biomarkers and clinical end-points during the first6 years of life.Methods The Th1-associated chemokines CXCL10 and CXCL11 and the Th2-associatedchemokines CCL17 and CCL22 were assessed in cord blood of asymptomatic at-risk new-born children from the Copenhagen Prospective Study on Asthma in Childhood (COP-SAC2000) birth cohort and associated with the longitudinal development of biomarkersand clinical end-points of asthma, eczema, and allergic rhinitis during the first 6 years oflife.Results Cord blood CCL22 levels were significantly associated to total-IgE levels measuredat four time-points during the first 6 years of life; overall odds ratio, 1.54 [CI, 1.25–1.89;P < 0.0001]. CXCL10 and CXCL11 were not associated with development of any atopicdisorders or biomarkers.Conclusion and Clinical Relevance High cord blood levels of the Th2 related chemokineCCL22 were significantly associated with high total- IgE levels during the first 6 years oflife, but not with specific sensitization, asthma, eczema or allergic rhinitis. This suggestsan inborn skewing of the immune system in healthy newborns developing elevated total-IgE later in life.
Keywords cord blood, chemokine, CCL22, CCL17, CXCL11, CXCL10, preschool age, atopicdisorders, total-IgE, Th2 skewingSubmitted 02 March 2012; revised 30 April 2012; accepted 25 May 2012
Introduction
The ‘atopic diseases’ asthma, eczema, and allergic rhini-tis origin early in life, presumably as a result of a Th2skewing of the immune system [1, 2]. It is important tounderstand early-life immune mechanisms responsiblefor the inception of atopic disease to unravel diseasepathogenesis towards preventive measures and possiblycustomized therapies.
Cord blood is easily accessible at birth and provides aunique opportunity to investigate the immunity of thenewborn prior to disease onset. Circulating levels ofTh1 and Th2 cytokines are difficult to measure in cordblood due to low levels close to the detection limit ofthe currently available assays [3] and challenge models
generate an exaggerated and possibly un-physiologicalresponse. Chemokines are simple to measure with cur-rent technology and are equally robust markers of Th1/Th2 immunity [4–8] in manifest atopic disorders. How-ever, little is known about cord blood Th1- and Th2-related chemokine levels [4, 9]. We hypothesized thatlevels of Th2 related chemokines in the cord blood areassociated with the development of atopic disease andbiomarkers during preschool age.
The aim of this study was to investigate the possibleassociation between the cord blood chemokines Thymusand activation regulated chemokine, TARC (CCL17),Macrophage-derived chemokine, MDC (CCL22), inter-feron gamma-induced protein 10 kDa, IP-10 (CXCL10),and Interferon-inducible T cell alpha chemoattractant,

I-TAC (CXCL11) in asymptomatic at-risk newbornchildren from the Copenhagen Prospective Study onAsthma in Childhood (COPSAC2000) birth cohort inrelation to the subsequent development of atopic bio-markers and clinical end-points during the first 6 yearsof life.
Methods
The study is reported in accordance with the STROBEguidelines for observational studies [10].
Study population
Participants comprised children from the COPSAC2000cohort of 411 children born of mothers with doctor-verified asthma, the recruitment of whom waspreviously described in detail [11]. The pregnant womenvisited the COPSAC research centre during pregnancyfor information on the study procedures. Consentingmothers brought their 1-month-old child to theresearch clinic and subsequently attended the clinic at6-monthly intervals and immediately upon onset of anyallergy-, respiratory- or skin-related symptom until age7 years. Key exclusion criteria were gestational age< 36 weeks, severe congenital abnormality, neonatalmechanical ventilation or symptoms of lower airwayinfection before 1 month of age.
Ethics
The study was conducted in accordance with the guid-ing principles of the Declaration of Helsinki andapproved by the Ethics Committee for Copenhagen(KF01-289/96) and the Danish Data Protection Agency(2008/41-1754). Data validity was assured by compli-ance with Good Clinical Practice guidelines and qualitycontrol procedures.
Cord blood collection and analyses
The midwives received written instructions on the col-lection of cord blood using needle puncture from theumbilical cord vein: 14 mL cord blood was collected(7 mL in an EDTA tube and 7 mL whole blood) andsubsequently send to the COPSAC research unit, wherethe blood was centrifuged for 10 min at 2800 g toseparate serum and plasma, and thereafter frozen at!80°C until analysis at the Department of Clinical andExperimental Medicine, Linkoping University, Swe-den. The chemokines CXCL10, CXCL11, CCL17, andCCL22 were analysed in plasma with an in-house multi-plexed Luminex assay, as described in detail previously[4]. The limit of detection was 6 pg/mL for CXCL10,28 pg/mL for CXCL11, and 2 pg/mL for CCL17 and
CCL22. All samples were analysed in duplicates and thesample was re-analysed if the coefficient of variation(CV) was > 15%.
Atopic biomarkers
Blood was collected from the children at ages6 months, 18 months, 4 years, and 6 years during visitsat the research unit. All samples were stored at –80°Cuntil analysis.
Total-IgE levels were measured at ages 6 months,18 months, 4 years, and 6 years using ImmunoCAP(Pharmacia Diagnostics AB, Uppsala, Sweden) with adetection limit of 2 kU/L.
Specific IgE levels against 15 common inhalant andfood allergens (cat, dog, horse, birch, timothy grass,mugwort, house dust mites, moulds, hen’s egg, cow’smilk, fish, wheat, peanut, soybean, or shrimp) weremeasured at ages 6 months, 18 months, 4 years, and6 years using ImmunoCAP (Pharmacia Diagnostics AB)[12, 13].
Skin Prick Test was performed at 6 months,18 months, 4 years, and 6 years against 18 commoninhalant and food allergens (birch, timothy grass, mug-wort, horse, dog, cat, house dust mites, moulds, hen’segg, cow’s milk, fisk, wheat, rye, oat, peanut, soyabean,beef, and pork) with standard allergen solutions fromALK-Abello® (Bøge Alle 1, DK-2970 Hørsholm,Denmark), and in addition with pasteurised, fresh prod-ucts for cow’s milk and hen’s egg.
Allergic sensitization was defined as specificIgE " 0.35 kU/L [12, 13] for any of the tested aller-gens and/or a positive skin prick test defined as a weal" 2 mm at 6 and 18 months or " 3 mm at 4 or6 years. Allergic sensitization was analysed as a dichot-omized measurement.
Blood eosinophil count (109 cells/L) was assessed atages 6 months, 18 months, 4 years, and 6 years.
Nasal eosinophilia was examined by nasal scrapingsin the child’s 6th year of life and rated according toMeltzer’s semi-quantitative scale [14] as previouslydetailed [15].
Investigator-diagnosed clinical end-points
Allergic rhinitis was diagnosed at age 6 by the COPSACdoctors, based on parent interviews on symptom historyin the child’s 6th year of life [15]. Rhinitis was definedas troublesome sneezing or blocked or runny nose inthe past 12 months in periods without accompanyingvirus symptoms [16]. Allergic rhinitis was diagnosed inchildren sensitized to inhaled allergens of relevance tothe symptomatic periods.
Asthma at age 7 years was diagnosed as previouslydetailed, [17, 18] and was based on a history of recur-
© 2012 Blackwell Publishing Ltd, Clinical & Experimental Allergy, 42 : 1596–1603
Cord blood CCL22 related to total-IgE 1597

rent wheeze; symptom character judged by the studyphysicians to be typical of asthma; response to trials ofinhaled corticosteroids; and relapse when stoppingtreatment.
Eczema during the first 6 years of life was diagnosedusing the Hanifin–Rajka criteria as previously detailed[19]. Skin lesions were described at both scheduled andacute visits according to pre-defined morphology andlocalization.
Statistical analysis
We investigated the association between cord bloodlevels of the chemokines CXCL10, CXCL11, CCL17,CCL22 and the Th2/Th1 ratios CCL22/CXCL10, CCL17/CXCL10, CCL22/CXCL11, CCL17/CXCL11, and thedevelopment of atopic biomarkers and atopic clinicalend-points during the first 7 years of life. Modelsusing general estimating equations (GEE; PROC GEN-MOD in SAS version 9.1; SAS Institute, Inc., Cary, NC,USA) were applied to compute the overall odds ratiofor allergic sensitization, blood eosinophil count, andtotal-IgE using compiled data from all four measuringpoints (6 months, 18 months, 4 years, and 6 years).Logistic regression was used to calculate odds ratios ofthe cross-sectional end-points allergic rhinitis, nasaleosinophilia, and asthma. Hazard ratios of recurrentwheeze and eczema at ages 0–1 and 0–6 year werecalculated using Cox regression. Age at onset wasmodelled as a function of chemokine levels and ratios;
the children were retained in the analysis from birthuntil age at onset of disease, drop-out, or age at endof the observation period (i.e. 1 year for 0–1 year),whichever first. Levels of chemokines, total-IgE, andblood eosinophil count were log-transformed prior toanalysis to obtain normal distribution of data.
Results are reported with 95% CI in brackets. Robust-ness of results was investigated by adjusting for multi-ple testing according to the method by Bonferonicorrection for control of false discovery rate. All analy-ses were performed in SAS version 9.1 for Windows(SAS Institute, Inc.).
Results
Baseline
Cord blood samples were available for analyses from223 of the 411 children from the COPSAC2000 cohort.Children from low-income families were significantlyless likely to have cord blood sampled [P-value =0.008], whereas there were no differences between chil-dren with and without cord blood samples with respectto ethnicity, exposure to tobacco, alcohol, and maternalantibiotic use during 3rd trimester, mode of delivery,gestational age, gender or anthroprometrics (Table 1).
Levels of chemokines, total-IgE, blood eosinophilcount, and frequency of nasal eosinophilia, allergic rhi-nitis, asthma, eczema, and allergic sensitization in thestudy group are outlined in Table 2.
Table 1. Baseline demographics
Baseline demografics Entire COPSAC cohort N = 411
Cord blood
P-valueCollected N = 223 Not collected N = 188
Gender male 203 (49.4%) 112 (55.2%) 91 (44.8%) 0.71
Birth length* 133 (32.0%) 75 (33.6%) 58 (30.9%) 0.16
Birth weight† 129 (31.4%) 69 (30.9%) 60 (31.9%) 0.60
Mode of delivery‡ 85 (20.7%) 43 (19.3%) 42 (22.3%) 0.53
Occupation 0.15
Non-professional 128 (33.5%) 69 (33.7%) 59 (33.3%)
Professional 174 (45.6%) 100 (48.8%) 74 (41.8%)
Student 42 (10.9%) 22 (10.7%) 20 (11.3%)
Unemployed 14 (6.8%) 14 (6.8%) 24 (13.6%)
Household income 0.008
Low 112 (29.2%) 47 (22.8%) 65 (36.5%)
Average 182 (47.4%) 110 (53.4%) 72 (40.5%)
High 90 (23.4%) 49 (23.8%) 41 (23.0%)
Expositions
Smoking during third trimester 63 (15.3%) 36 (16.1%) 27 (14.4%) 0.61
Alcohol during third trimester 73 (17.8%) 40 (17.9%) 33 (17.6%) 0.91
Antibiotics third trimester 125 (30.4%) 67 (53.6%) 58 (46.4%) 0.85
*Lowest birth length tertile.†Lowest birth weight tertile.‡Caesarian section.
P-values were calculated using chi-square test.
© 2012 Blackwell Publishing Ltd, Clinical & Experimental Allergy, 42 : 1596–1603
1598 N. V. Følsgaard et al

Association between cord blood chemokine levels andatopic biomarkers
Total-IgE. Cord blood CCL22 levels were significantlyassociated with total-IgE levels at 6 months, 18 months,4 years, and 6 years (GEE model including all fourmeasuring points): odds ratio, 1.54 [CI, 1.25–1.89;P < 0.0001]. In addition, the Th2/Th1 ratios were alsoassociated with Total-IgE levels: CCL22/CXCL11: oddsratio, 1.31 [CI, 1.13–1.51; P = 0.0002] and CCL22/CXCL10 odds ratio, 1.22 [CI, 1.03–1.43; P = 0.02].However, the CCL22/CXCL10 ratio did not pass theBonferroni threshold for significance (Table 3). Therewas no association between CCL17, CXCL11 or CXCL10and Total-IgE levels. Figure 1 shows the individualizedassociation between cord blood CCL22 and total-IgE ateach measured time-point.
Specific IgE. No association was found between specificIgE and any cord blood chemokine levels (Table 3).
Blood eosinophil count. Cord blood CCL22 and CXCL11levels were associated with development of blood eosin-ophilia in the overall GEE model: Odds ratio, 1.15 [CI,1.00–1.32; P = 0.05] and odds ratio, 1.09 [CI, 1.00–1.20; P = 0.05], respectively. However, this was not sig-nificant after correction for multiple testing. There wasno association between CCL22/CXCL10, CCL22/CXCL11,CCL17/CXCL10, CCL17/CXCL11 ratios, CXCL10 orCCL17, and blood eosinophilia (Table 3).
Nasal eosinophilia at age 6 years was not associatedwith any of the tested chemokines or Th2/Th1 ratios(Table S1 online).
Association between cord blood chemokine levels andinvestigator-diagnosed clinical end-points
No association was found between levels or ratios ofany of the tested cord blood chemokines and develop-ment of eczema, asthma, troublesome lung symptomsor allergic rhinitis during the first 6 years of life(Tables S2–S5 online).
Discussion
Principle findings
Cord blood levels of the Th2 related chemokine CCL22and Th2/Th1 chemokine ratios in healthy newborns fromthe Danish COPSAC2000 birth cohort of asthmatic motherswere significantly associated with elevated total-IgElevels during the first 6 years of life. This suggests aninborn/intrauterine Th2 skewing of the immune system inchildren subsequently developing high levels of total-IgE.
Strengths and limitations
The major strength of this study is the 6-year longitudi-nal, stringent, and uniform clinical follow-up of a birthcohort. COPSAC is a single-centre study, where theCOPSAC doctors act as general practitioners for thechildren, diagnosing and treating all airway-, allergy-,and skin-related symptoms according to pre-definedalgorithms thus assuring consistency in diagnoses andreducing the risk of misclassification.
In addition, the atopic biomarkers; blood eosinophilcount, specific-, and total-IgE were assessed repeatedly
Table 2. Baseline levels of chemokines, atopic biomarker levels and occurrence of clinical end-points
Variable
Age-point
Birth (Cord blood) 6 Months 18 Months 4 Years 6 Years
CCL22 pg/mL; median (range) 441 (57–3581)CCL17 pg/mL; median (range) 211 (8.6–3949)CXCL11 pg/mL; median (range) 215 (35–2657)CXCL10 pg/mL; median (range) 35 (6.4–294)Blood eosinophil count (9 109/L)
median (range)
0.27 (0.06–1.45) 0.21 (0.04–1.19) 0.24 (0.01–3.0) 0.32 (0–3.5)
Total-IgE (kU/L); median (range) 4 (0.13–71) 7.7 (0.03–90) 27 (0.13–71) 46 (1.9–1564)Allergic sensitization*; % (N) 6.3 (14) 9.3 (21) 19 (42) 25 (56)
Sensitization ever; % (N) 36 (77)
Allergic rhinitis; 6 years; % (N) 8 (13)
Nasal eosinophilia† 6 years; % (N) 5 (8)
Asthma 7 years; % (N) 17 (32)
*Allergic sensitization = any sensitization for cat, dog, horse, birch, timothy grass, mugwort, house dust mites, moulds, hen’s egg, cow’s milk, fish,
wheat, peanut, soybean, or shrimp.†Nasal eosinophilia (> + 1 on Meltzer’s semi-quantitative scale).
© 2012 Blackwell Publishing Ltd, Clinical & Experimental Allergy, 42 : 1596–1603
Cord blood CCL22 related to total-IgE 1599

at four time-points till 6 years of age, increasing the sta-tistical power to detect true associations in GEE modelsaccounting for repeated within subject measurements.
A further strength of the study is the sensitivity of thechemokine assays allowing assessment of chemokinelevels in all available cord blood samples without stimu-lation, thus avoiding excessive un-physiologicalresponses accompanying challenge models. CirculatingTh1- and Th2-associated chemokine levels can be used asmarkers for the Th1/Th2 balance [4–8] making immune-regulatory chemokines potential biomarkers of currentand future disease [20]. Th1 responses increase the levels
of CXCR3 ligands CXCL10 and CXCL11, whereas Th2responses enhance the levels of CCR4 ligands CCL17 andCCL22 [21, 22]. CXCR3 is preferentially expressed on Th1cells and CCR4 on Th2 cells, thus further amplifying Th1and Th2 immunity, respectively [22].
Finally, the large cord blood sample size of 223 sam-ples increases the validity of the data.
Cord blood biomarkers may be biased by transferfrom maternal blood. This has been demonstrated forspecific- and total-IgE where maternal levels are often1000 times higher than cord blood levels and evenminimal amount of maternal blood may significantly
Fig. 1. Correlation between cord blood CCL22 and total-IgE at 6 months, 18 months, 4 years, and 6 years. All data are log-transformed.
Table 3. Association between cord blood chemokine levels and allergic sensitization, blood eosinophil count and total-IgE
Chemokines
Allergic sensitization* Blood eosinophil count Total-IgE
Odds ratio [95% CI] P-value Odds ratio [95% CI] P-value Odds ratio [95% CI] P-value
CCL22 1.35 [0.94–1.95] 0.10 1.15 [1.00–1.32] 0.05 1.54 [1.25–1.89] <0.0001
CCL22/CXCL10 1.08 [0.80–1.45] 0.62 1.07 [0.97–1.18] 0.16 1.22 [1.03–1.43] 0.02
CCL22/CXCL11 1.23 [0.90–1.68] 0.19 0.99 [0.91–1.09] 0.93 1.31 [1.13–1.51] 0.0002
CXCL10 1.15 [0.76–1.72] 0.51 1.01 [0.90–1.13] 0.83 1.05 [0.83–1.32] 0.67
CXCL11 0.94 [0.66–1.33] 0.71 1.09 [1.001–1.2] 0.05 0.93 [0.80–1.10] 0.43
CCL17 0.97 [0.76–1.24] 0.82 1.06 [0.98–1.13] 0.13 1.02 [0.90–1.15] 0.75
CCL17/CXCL10 0.95 [0.77–1.16] 0.61 1.03 [0.97–0.09] 0.27 1.00 [0.89–1.11] 0.99
CCL17/CXCL11 1.02 [0.72–1.44] 0.91 0.99 [0.90–1.10] 0.96 1.11 [0.93–1.34] 0.22
Results are based on GEE analysis; According to Bonferoni correction for multiple testing, only P-values < 0.006 are considered significant and
highlighted in bold.
*Allergic sensitization = any sensitization to cat, dog, horse, birch, timothy grass, mugwort, house dust mites, moulds, hen’s egg, cow’s milk, fish,
wheat, peanut, soybean, or shrimp.
© 2012 Blackwell Publishing Ltd, Clinical & Experimental Allergy, 42 : 1596–1603
1600 N. V. Følsgaard et al

affect cord blood levels [23, 24]. Such bias from mater-nal transfer seems not to be an issue for cord bloodchemokines that are often found in higher level in cordblood than maternal blood.
A limitation of our study is the high-risk nature ofthe COPSAC2000 cohort where all mothers have a his-tory of asthma, which requires replication in an unse-lected population. However, the analyses were based onwithin subject associations between cord blood chemo-kine levels and the subsequent development of atopicdisease and atopic biomarkers unlikely to be affectedby the increased risk of atopic diseases. This is sup-ported by a previous study where elevated cord bloodCCL22 levels preceded development of sensitisationindependent of atopic heredity [9].
A further limitation is that cord blood samples wereonly available from half of the cohort. However, theselected cohort was representative of the main cohortfor the majority of population characteristics.
Interpretation
Elevated cord blood levels of the CCL22 chemokine pre-ceding development of raised total-IgE during the first6 years of life suggests a triggering role of CCL22 inthe inception of elevated total-IgE in children on anatopic trajectory. The mechanism responsible for thelinkage between elevated CCL22 and raised total-IgEremains unknown, although CCL22 is described to playa central role in enhancing the Th2 responses. Thus,our data support the general hypothesis of an early-lifeTh2 skewing of the immune response [1, 3].
Cord blood CCL22 levels have previously been pro-posed as a predictor of elevated IgE levels and clinicallymanifest allergy development [6, 25]. However, only afew others have studied un-stimulated cord bloodchemokines. Our findings are supported by a previousreport from 56 children where cord blood CCL22 wasassociated with elevated IgE levels at age 6 [9]. Wefound no association between cord blood chemokinelevels and development of atopic symptoms of asthma,rhinitis or eczema. It is possible that CCL22 is involvedin a specific immunological mechanism only causingelevated total-IgE, but not specific sensitization or dis-ease. Cord blood CCL17 and CCL22 have been associ-ated with atopic dermatitis and asthma development incohorts of mixed atopic and non-atopic parental predis-position [9, 26]. As this study is the largest to date, it ispossible that previously reported association with atopicdisease were the result of a type 1 error. The discrep-ancy between these findings and our data might also bedue to the high-risk nature of the COPSAC2000 cohort.
The mechanism behind elevated cord blood CCL22remains unclear. However, such pronounced Th2/Th1imbalance in the newborn may be driven by genetic
variants and/or caused by unknown intrauterine envi-ronmental triggers impacting the fetal development.
We have previously shown that urine eosinophil pro-tein X in neonates precedes development of allergicsensitization and eczema, [27] and that raised exhalednitric oxide in neonates associates with development ofearly transient wheeze [28]. Importantly, these findingsand the current study supports the concept that earlyimmunological programming of immune function playsan essential role in the skewing of the immune response.Together such fingerprints of atopic disease develop-ment in newborns may contribute to construction ofclinically feasible prediction models in the future.
Conclusion
High cord blood levels of the Th2 related chemokineCCL22 were significantly associated with high total- IgElevels during the first 6 years of life. This suggests aninborn Th2 skewing of the immune system in healthynewborns developing elevated total-IgE later in life.
Acknowledgement
The authors thank the children and parents participat-ing in the COPSAC cohort as well as the COPSAC studyteam. We also thank Mrs Anne-Marie Fornander, Lin-koping University, for excellent technical assistance.
Source of funding and conflict of interest: COPSAC isfunded by private and public research funds listed onhttp://www.copsac.com. The Lundbeck Foundation; TheDanish Strategic Research Council; the Pharmacy Foun-dation of 1991; Augustinus Foundation; the DanishMedical Research Council and The Danish PediatricAsthma Centre provided the core support for COPSACresearch center. This study was also supported by theSwedish Research Council (K2011-56X-21854-01-06),the Cancer and Allergy Association and the Olle Engk-vist Foundation to MJ. No pharmaceutical companywas involved in the study. The funding agencies didnot have any role in design and conduct of the study;collection, management, and interpretation of the data;or preparation, review, or approval of the manuscript.
Authors Contribution: The guarantor of the study isHB who has been responsible for the integrity of thestudy as a whole, from conception and design to acqui-sition of data, analysis, and interpretation of data andwriting of the manuscript. NVF contributed to dataanalyses, statistical analysis, interpretation, and writingof the manuscript. MJ supervised the chemokine ana-lyses, data interpretation, and writing of the manu-script. BLKC and KB contributed to data analyses,interpretation, and writing of the manuscript. Allauthors made important intellectual contributions andcritical final revision of the manuscript.
© 2012 Blackwell Publishing Ltd, Clinical & Experimental Allergy, 42 : 1596–1603
Cord blood CCL22 related to total-IgE 1601

References
1 Leung T-F, Ng P-C, Tam W-H et al.Helper T-lymphocyte-related chemo-kines in healthy newborns. Pediatr Res2004; 55:334–8.
2 Hawrylowicz C, Ryanna K. Asthma andallergy: the early beginnings. Nat Med2010; 16:274–5.
3 Sandberg M, Frykman A, Ernerudh Jet al. Cord blood cytokines andchemokines and development of aller-gic disease. Pediatr Allergy Immunol2009; 20:519–27.
4 Abrahamsson TR, Sandberg Abelius M,Forsberg A, Bjorksten B, Jenmalm MC.A Th1/Th2-associated chemokine imbal-ance during infancy in children devel-oping eczema, wheeze and sensitization.Clin Exp Allergy 2011; 41:1729–39.
5 Fujisawa T, Fujisawa R, Kato Y et al.Presence of high contents of thymusand activation-regulated chemokinein platelets and elevated plasma levelsof thymus and activation-regulatedchemokine and macrophage-derivedchemokine in patients with atopic der-matitis. J Allergy Clin Immunol 2002;110:139–46.
6 Jahnz-Rozyk K, Targowski T, Pal-uchowska E, Owczarek W, KucharczykA. Serum thymus and activation-regu-lated chemokine, macrophage-derivedchemokine and eotaxin as markers ofseverity of atopic dermatitis. Allergy2005; 60:685–8.
7 Aggarwal A, Agarwal S, Misra R.Chemokine and chemokine receptoranalysis reveals elevated interferon-inducible protein-10 (IP)-10/CXCL10levels and increased number of CCR5+and CXCR3+ CD4 T cells in synovialfluid of patients with enthesitis-relatedarthritis (ERA). Clin Exp Immunol2007; 148:515–9.
8 Stumpf C, Auer C, Yilmaz A et al.Serum levels of the Th1 chemoattrac-tant interferon-gamma-inducible pro-tein (IP) 10 are elevated in patientswith essential hypertension. HypertensRes 2011; 34:484–8.
9 Abelius MS, Ernerudh J, Berg G, Matt-hiesen L, Nilsson LJ, Jenmalm MC.High cord blood levels of the T-helper2-associated chemokines CCL17 andCCL22 precede allergy development
during the first 6 years of life. PediatrRes 2011; 70:495–500.
10 von Elm E, Altman DG, Egger M, Po-cock SJ, Gøtzsche PC, VandenbrouckeJP. The strengthening the reporting ofobservational studies in epidemiology(STROBE) statement: guidelines forreporting observational studies. PLoSMed 2007; 4:e296.
11 Bisgaard H. The copenhagen prospec-tive study on asthma in childhood(COPSAC): design, rationale, and base-line data from a longitudinal birthcohort study. Ann Allergy AsthmaImmunol 2004; 93:381–9.
12 Ballardini N, Nilsson C, Nilsson M, Lil-ja G. ImmunoCAP Phadiatop Infant–anew blood test for detecting IgE sensi-tisation in children at 2 years of age.Allergy 2006; 61:337–43.
13 Wickman M, Ahlstedt S, Lilja G, vanHage Hamsten M. Quantification of IgEantibodies simplifies the classificationof allergic diseases in 4-year-old chil-dren. A report from the prospectivebirth cohort study–BAMSE. PediatrAllergy Immunol 2003; 14:441–7.
14 Howarth PH, Persson CGA, Meltzer EO,Jacobson MR, Durham SR, Silkoff PE.Objective monitoring of nasal airwayinflammation in rhinitis. J Allergy ClinImmunol 2005; 115:S414–41.
15 Chawes BLK, Kreiner-Møller E, Bisg-aard H. Objective assessments of aller-gic and nonallergic rhinitis in youngchildren. Allergy 2009; 64:1547–53.
16 Braun-Fahrlander C, Wuthrich B, Gass-ner M et al. Validation of a rhinitissymptom questionnaire (ISAAC corequestions) in a population of Swissschool children visiting the schoolhealth services. SCARPOL-team. Swissstudy on childhood allergy and respira-tory symptom with respect to air pollu-tion and climate. international study ofasthma and allergies in childhood. Pedi-atr Allergy Immunol 1997; 8:75–82.
17 Bisgaard H, Hermansen MN, Buchvald Fet al. Childhood asthma after bacterialcolonization of the airway in neonates.N Engl J Med 2007; 357:1487–95.
18 Bisgaard H, Hermansen MN, Loland L,Halkjaer LB, Buchvald F. Intermittentinhaled corticosteroids in infants withepisodic wheezing. N Engl J Med 2006;354:1998–2005.
19 Halkjaer LB, Loland L, Buchvald FFet al. Development of atopic dermatitisduring the first 3 years of life: thecopenhagen prospective study onasthma in childhood cohort study inhigh-risk children. Arch Dermatol2006; 142:561–6.
20 Hayglass KT. The quest for predictiveimmune biomarkers. Clin Exp Allergy2011; 41:1656–9.
21 Mantovani A, Sica A, Sozzani S, Alla-vena P, Vecchi A, Locati M. Thechemokine system in diverse forms ofmacrophage activation and polariza-tion. Trends Immunol 2004; 25:677–86.
22 Pease JE, Williams TJ. Chemokinesand their receptors in allergic disease.J Allergy Clin Immunol 2006; 118:305–18.
23 Bønnelykke K, Pipper CB, Bisgaard H.Sensitization does not develop in utero.J Allergy Clin Immunol 2008; 121:646–51.
24 Bønnelykke K, Pipper CB, Bisgaard H.Transfer of maternal IgE can be a com-mon cause of increased IgE levels incord blood. J Allergy Clin Immunol2010; 126:657–63.
25 Nakazato J, Kishida M, Kuroiwa R, Fu-jiwara J, Shimoda M, Shinomiya N.Serum levels of Th2 chemokines,CCL17, CCL22, and CCL27, were theimportant markers of severity in infan-tile atopic dermatitis. Pediatr AllergyImmunol 2008; 19:605–13.
26 Miyahara H, Okazaki N, Nagakura T,Korematsu S, Izumi T. Elevated umbili-cal cord serum TARC/CCL17 levelspredict the development of atopic der-matitis in infancy. Clin Exp Allergy2011; 41:186–91.
27 Chawes BLK, Bønnelykke K, BisgaardH. Elevated eosinophil protein X inurine from healthy neonates precedesdevelopment of atopy in the first 6years of life. Am J Respir Crit CareMed 2011. Available at: http://www.ncbi.nlm.nih.gov/pubmed/21680952(Accessed 28 July 2011).
28 Chawes BLK, Buchvald F, Bischoff ALet al. Elevated exhaled nitric oxide inhigh-risk neonates precedes transientearly but not persistent wheeze. Am JRespir Crit Care Med 2010; 182:138–42.
© 2012 Blackwell Publishing Ltd, Clinical & Experimental Allergy, 42 : 1596–1603
1602 N. V. Følsgaard et al

Supporting Information
Additional Supporting Information may be found inthe online version of this article:
Table S1. Association between chemokine levels atbirth and development of nasal eosinophilia at age 6.Nasal eosinophilia is measured by nasal scraping twicein the sixth year of life and defined as more than +1 onMeltzer’s semi-quantitative scale.
Table S2. Association between chemokines at birthand the development of eczema in the first 6 years oflife.
Table S3. Association between chemokine levels atbirth and recurrent wheeze.
Tabel S4. Association between chemokine levels atbirth and development of asthma at age 7.
Tabel S5. Association between Chemokine levels atbirth and development of allergic rhinitis at age 6.
Please note: Wiley-Blackwell are not responsible forthe content or functionality of any supporting materialssupplied by the authors. Any queries (other than miss-ing material) should be directed to the correspondingauthor for the article.
© 2012 Blackwell Publishing Ltd, Clinical & Experimental Allergy, 42 : 1596–1603
Cord blood CCL22 related to total-IgE 1603

Elevated Eosinophil Protein X in Urine from HealthyNeonates Precedes Development of Atopy in the First6 Years of LifeBo Lund Krogsgaard Chawes1, Klaus Bønnelykke1, and Hans Bisgaard1
1Copenhagen Prospective Studies on Asthma in Childhood, Health Sciences, University of Copenhagen, Copenhagen University Hospital,Gentofte, Copenhagen, Denmark
Rationale: Biomarkers predicting development of atopic disease areneeded for targeted preventive measures and to study if diseasepathology may be active before onset of symptoms.Objectives: To investigatewhether eosinophil proteinX, leukotriene-C4/D4/E4, and 11b-prostaglandin (PG) F2a (PGD2 metabolite)assessed in urine from healthy at-risk neonates precede develop-ment of atopic disease during the first 6 years of life.Methods: We measured eosinophil protein X (n ¼ 369), leukotriene-C4/D4/E4 (n¼367), and11b-PGF2a (n¼366) inurine from1-month-old childrenparticipating in theCopenhagenProspective Studies onAsthma in Childhood birth cohort. Clinical data on development ofallergic sensitization, allergic rhinitis, nasal eosinophilia, blood eo-sinophilia, eczema, troublesome lung symptoms (significant coughor wheeze or dyspnea), and asthma were collected prospectivelyuntil age 6 years. Associations between urinary biomarkers and de-velopment of atopic traits were investigated using general estimat-ing equations, logistic regression, and Cox regression.Measurements and Main Results: Eosinophil protein X in the urine ofthe asymptomatic 1-month-old neonates was significantly associ-ated with development of allergic sensitization (odds ratio, 1.49;95% confidence interval [CI], 1.08–1.89), nasal eosinophilia (oddsratio, 3.2; 95% CI, 1.2–8.8), and eczema (hazard ratio, 1.4; 95% CI,1.0–2.0), butnotwith allergic rhinitis, asthma, orbloodeosinophilia.Neither leukotriene-C4/D4/E4 nor 11b-PGF2a was associated withany of the atopic phenotypes.Conclusions: Eosinophil protein X in urine from asymptomatic neo-nates is a biomarker significantly associated with later developmentofallergic sensitization,nasaleosinophilia, andeczemaduringthefirst6 years of life. These findings suggest activation of eosinophil granu-locytes early in life before development of atopy-related symptoms.
Keywords: atopy; blood eosinophils; eczema; neonates; urinary eosin-ophil protein X
Identification of children at high risk of developing atopic disordersis amajor research challenge.Biomarkers predicting development ofatopic disease before the onset of symptoms are needed for targetedprevention and individualized intervention and treatment. Further-more, it is an important research question if the disease process maybe active before development of symptoms as we previously re-ported on increased fraction of exhaled nitric oxide in neonates laterdeveloping early wheeze (1) and pathogenic bacterial colonizationof the airways in neonates later developing asthma (2).
Urinary eosinophil protein X (u-EPX) released from acti-vated eosinophil granulocytes is seen in association with currentallergic sensitization (3) and has been associated with severity ofeczema (4) and acute and chronic childhood asthma (3, 5, 6).Urinary leukotriene (LT) C4/D4/E4 (u-LTC4/D4/E4), a measureof total body cysteinyl LT production, is elevated in subjectswith symptomatic allergic rhinitis (7) and in preschoolers withacute wheeze illnesses (8, 9). Prostaglandin (PG) D2, the majorcyclooxygenase product from activated mast cells, has been as-sociated with allergen-induced asthma illustrated by elevatedurinary level of 11b-PGF2a (u-11b-PGF2a), which is a majorstable PGD2 metabolite (10). Thus, u-EPX, u-LTC4/D4/E4, andu-11b-PGF2a are all well-known markers of established atopicinflammation, but it is unknown whether levels are elevatedvery early in life preceding symptom debut.
We measured u-EPX, u-LTC4/D4/E4, and u-11b-PGF2a inhealthy high-risk 1-month-old asymptomatic neonates to inves-tigate whether elevated level of these biomarkers precede sub-sequent development of atopic disease during the first 6 years oflife. We used the comprehensive longitudinal clinical data ontroublesome lung symptoms, asthma, eczema, rhinitis, allergicsensitization, blood, and nasal eosinophils in the CopenhagenProspective Study on Asthma in Childhood (COPSAC) birthcohort of high-risk babies.
(Received in original form January 19, 2011; accepted in final form June 11, 2011)
Supported by The Lundbeck Foundation, The Pharmacy Foundation of 1991, theDanish Medical Research Council, The Danish Pediatric Asthma Center, DanishLung Association, Hans Skoubys og hustru Emma Skoubys Fond, and Oda Ped-ersens Legat.
Contributions: The guarantor of the study is H.B., who has been responsible forthe integrity of the work as a whole, from conception and design to conduct ofthe study and acquisition of data, analysis and interpretation of data, and writingof the manuscript. B.L.K.C. drafted the manuscript. B.L.K.C. and K.B. were re-sponsible for data acquisition, analysis, interpretation, and writing the manu-script. All coauthors have contributed substantially to the analyses andinterpretation of the data, and have provided important intellectual input andapproval of the final version of the manuscript. H.B. had full access to the dataand had final responsibility for the decision to submit for publication.
Correspondence and requests for reprints should be addressed to Hans Bisgaard, M.D., D.M.Sc., Copenhagen Prospective Studies on Asthma in Childhood, HealthSciences, University of Copenhagen, Copenhagen University Hospital, Gentofte,Ledreborg Alle 34, DK-2820 Gentofte, Copenhagen, Denmark. E-mail: [email protected]
This article has an online supplement, which is accessible from this issue’s table ofcontents at www.atsjournals.org
Am J Respir Crit Care Med Vol 184. pp 656–661, 2011Originally Published in Press as DOI: 10.1164/rccm.201101-0111OC on June 16, 2011Internet address: www.atsjournals.org
AT A GLANCE COMMENTARY
Scientific Knowledge on the Subject
Urinary eosinophil protein X is elevated in subjects withpresent allergic sensitization and has been associated withseverity of eczema and acute and chronic childhood asthma.
What This Study Adds to the Field
Elevated level of urinary eosinophil protein X in symptom-free high-risk neonates precedes development of allergicsensitization, nasal eosinophilia, and eczema during pre-school age suggesting eosinophilic activation before thedevelopment of atopy-related illnesses.

We hypothesized that elevated levels of u-EPX, u-LTC4/D4/E4,and u-11b-PGF2a very early in life reflects presymptom diseaseactivity preceding later development of atopic disease.
METHODS
Study Design
The COPSAC birth cohort is a prospective clinical study of 411 childrenborn to mothers with asthma previously described in detail (2, 11, 12).The symptom-free children were enrolled at 1 month of age and sub-sequently attended the clinical research unit for scheduled clinicalinvestigations at 6-monthly intervals and immediately on onset ofany respiratory or skin-related symptom. Key exclusion criteria weregestational age less than 36 weeks, severe congenital abnormality, neo-natal mechanical ventilation and symptoms of lower airway infectionbefore 1 month of age.
The study was conducted in accordance with the Declaration ofHelsinki and was approved by The Copenhagen Ethics Committee(KF 01–289/96) and The Danish Data Protection Agency (2008–41–1754) (11). Informed consent was obtained from both parents beforeenrollment.
Urine Inflammatory Markers
Urine was collected during visits to the COPSAC research unit at ages 1and 6 months into a sterile plastic bag adherent to the skin. The urinesamples were immediately transferred to 3.6-ml Nunc tubes, and the ali-quots were stored without addition of any preservatives at 2808C untilanalysis.
After thawing, levels of EPX, LTC4/D4/E4, and 11b-PGF2a weremeasured in the urine samples. u-EPX concentration was determinedby a double-antibody immunoassay (radioimmunoassay; PharmaciaUpjohn, AB, Uppsala, Sweden) in both the 1- and 6-month samples.The combined quantitative value of u-LTC4/D4/E4 levels was measuredby ELISA test kits (Neogen Corporation, Lexington, KY). Urinarylevel of 11b-PGF2a was also assessed by ELISA test kits (NeogenCorporation).
To standardize for variations in renal excretion, levels of all urinarymarkers were adjusted for creatinine excretion (13). Urinary creatininelevels were measured by buffered kinetic Jaffe reaction (Cobas Integra700 analyzer; Roche Diagnostics, Hvidovre, Denmark). All urine lab-oratory analyses were performed at Phadia ApS, Allerød, Denmark.
Atopic Intermediary End Points
Allergic sensitization was determined at ages 6 and 18 months and 4 and6 years by measurement of serum-specific IgE against 15 common in-halant and food allergens (cat, dog, horse, birch, timothy grass, mug-wort, house dust mites, molds, hen’s egg, cow’s milk, fish, wheat,peanut, soybean, and shrimp) by ImmunoCAP assay (Pharmacia Diag-nostics AB, Uppsala, Sweden). Sensitization was defined as specific-IgE greater than or equal to 0.35 kU/L (14, 15) for any of the testedallergens and was analyzed as a dichotomized measurement.
In a secondary analysis we stratified presence of allergic sensitizationas (1) food sensitization, being any sensitization for hen’s egg, cow’smilk, fish, wheat, peanut, soybean, or shrimp; (2) sensitization for in-haled allergens, being any sensitization for cat, dog, horse, birch, tim-othy grass, mugwort, house dust mites, or molds; (3) sensitization foroutdoor aeroallergens, being any sensitization for birch, timothy grass,or mugwort; and (4) sensitization for indoor aeroallergens, being anysensitization for cat, dog, house dust mites, or molds.
Blood eosinophil count (109 cells per liter) was assessed at ages 6and 18 months and 4 and 6 years. Nasal eosinophilia was investigatedby nasal scraping in the child’s sixth year of life and rated according toMeltzer’s semiquantitative scale (16) as previously detailed (17).
Clinical Investigator-diagnosed End Points
Allergic rhinitis was diagnosed at age 6 by the COPSACdoctors based onclinical interviews of the parents (not questionnaires) on history of symp-toms in the child’s sixth year of life (17–19). Rhinitis was defined as
troublesome sneezing or blocked or runny nose in the past 12 monthsin periods without accompanying cold or flu (20). Significance of symp-toms was judged by severity, length of periods, and time of year. Allergicrhinitis was diagnosed in children with rhinitis and sensitization to aero-allergens (cat, dog, horse, birch, timothy grass, mugwort, house dustmites, or molds) clearly related to the symptomatic periods.
Troublesome lung symptoms (significant cough or wheeze or dysp-nea) were recorded by the parents as a dichotomized daily score (yes orno) from birth until age 7 years (21). Recurrent troublesome lungsymptoms (recently termed “multitrigger wheeze” [22]) were definedfrom the diaries as five episodes within 6 months, each episode lastingat least 3 consecutive days, or daily symptoms for 4 consecutive weeks(1, 23). Children meeting these criteria were prescribed a 3-month trialof budesonide, 200 mg twice a day in a pressurized metered dose inhalerwith a spacer. Episodic viral troublesome lung symptoms (22) character-ized children suffering discrete symptomatic episodes, with the childbeing well between episodes, not fulfilling the criteria for recurrent trou-blesome lung symptoms, and treated intermittently solely with inhaledb2-agonist. Early transient troublesome lung symptoms was diagnosed inchildren with troublesome lung symptoms at age 0–3 years but withoutsymptoms at age 3–6 years; late-onset troublesome lung symptoms inchildren with troublesome lung symptoms with an age at onset at age3–6 years; and persistent troublesome lung symptoms in children whohad symptoms both at age 0–3 and 3–6 years.
Asthma at age 7 years was diagnosed by the COPSAC doctorsaccording to international guidelines and was based on recurrent trou-blesome lung symptoms, symptom character, and response to trialsof inhaled corticosteroids, as previously detailed (2, 12) (see www.copsac.com and the online supplement for further details on diagnosisof recurrent troublesome lung symptoms and asthma).
Eczema was diagnosed by using the Hanifin-Rajka criteria, as pre-viously detailed (24, 25). Skin lesions were described at both scheduledand acute visits according to predefined morphology and localization.
Statistical Analyses
Quantitative levels of u-EPX, u-LTC4/D4/E4, and u-11b-PGF2a at age1 month and u-EPX and blood eosinophil count at age 6 months wereused as explanatory variables. Models using general estimating equa-tions (GEE) (PROC GENMOD in SAS version 9.2; SAS Institute,Inc., Cary, NC) were applied to compute the overall odds ratio forallergic sensitization and the overall b-coefficient for blood eosinophilcount using compiled data from all four time points (6 and 18 mo, 4 and6 yr). Logistic regression was used to calculate odds ratios of the cross-sectional end points allergic rhinitis, nasal eosinophilia, asthma, and thepatterns of troublesome lung symptoms from 0–6 years. Hazard ratiosof recurrent troublesome lung symptoms and eczema at age 0–1 yearand 0–6 years were calculated by Cox regression. Age at onset wasmodeled as a function of the urinary biomarkers; the children wereretained in the analysis from birth until age at onset of disease, drop-out, or age at end of the observation period (i.e., 1 yr for 0–1 yr),whichever came first. Levels of urinary biomarkers and blood eosino-phil count were log-transformed before analysis.
Results are reported with 95% confidence interval (CI) in brackets;a P value less than or equal to 0.05 was considered significant. Allanalyses were done in SAS version 9.2 for Windows (SAS Insti-tute). Further details of the methods are outlined in the onlinesupplement.
RESULTS
Baseline Characteristics
This protocol for urinary inflammatory markers was initiated af-ter enrolling 42 of the 411 children of the cohort leaving 369 forurine analysis at age 1 month. Measurement of u-EPX was com-pleted for all 369 children, u-LTC4/D4/E4 for 367, and u-11b-PGF2a for 366, respectively. u-EPX was available for 337 childrenat age 6 months.
The study group consisted of 51% boys (n ¼ 187). In the firstyear of life, 4% of the children developed recurrent troublesomelung symptoms and 27% were diagnosed with eczema. A further
Chawes, Bønnelykke, Bisgaard: Urinary Inflammatory Markers and Childhood Atopy 657

17% developed recurrent troublesome lung symptoms and 15%eczema before age 6 years. Level of urinary markers, blood eo-sinophil count, and frequency of allergic sensitization, allergicrhinitis, nasal eosinophilia, and asthma are presented in Table 1.
There were no significant differences among the 42 subjectswithout urine samples and the 369 subjects in the study groupwith respect to sex, allergic sensitization, allergic rhinitis, nasaleosinophilia, asthma, eczema, or blood eosinophilia at age 6 years(see Table E1 in the online supplement).
u-EPX at Age 1 Month
Allergic sensitization. u-EPX at age 1 month was significantlyassociated with increased odds of allergic sensitization (GEEmodel including the four time points of 6 and 18 mo and 4 and6 yr; odds ratio, 1.49; 95% CI, 1.08–1.89; P ¼ 0.02) (Table 2),as illustrated by the plot of age-dependent odds ratios in Figure 1.Adjusting the analysis for maternal allergic sensitization assessedby specific-IgE measurements did not substantially modify theassociation (odds ratio, 1.45; 95% CI, 1.03–1.88; P ¼ 0.04). Anal-yses stratified for type of sensitization: food allergens, inhaledallergens, and outdoor and indoor aeroallergens showed similarresults (Table E2). Elevated u-EPX at age 1 month was associ-ated with an increased odds of sensitization irrespective of thetype of sensitization; the analysis was significant for foodsensitization (P ¼ 0.01), borderline significant for aeroallergensensitization (P ¼ 0.06) and sensitization to indoor inhaled aller-gens (P ¼ 0.08), but not significant for outdoor inhaled allergens(P ¼ 0.38) (Table E2).Allergic rhinitis and nasal eosinophilia. u-EPX at age 1 month
was strongly and significantly associated with nasal eosinophiliaat age 6 years (odds ratio, 3.2; 95% CI, 1.2–8.8; P ¼ 0.02). Inaddition, there was a tendency of increased odds for allergicrhinitis by age 6 years (Table 2).Blood eosinophilia. u-EPX at 1 month was significantly asso-
ciated with blood eosinophil count at age 6 years (b-coefficient,0.19; 95% CI, 0–0.38; P ¼ 0.05) (Table E3), but was not overallsignificantly associated with blood eosinophil count in the GEEmodel including all four measuring points (Table 2).Eczema. The cumulative risk of eczema during the first 6 years
of life for neonates with u-EPX level above and below the thirdquartile of the study group (149 mg/L) is illustrated in Figure E1,suggesting that elevated u-EPX is associated with developmentof eczema early in life. Accordingly, the risk of eczema duringthe first year of life increased significantly with increasing levelsof u-EPX at age 1 month (hazard ratio, 1.4; 95% CI, 1.0–2.0;P ¼ 0.05), but not thereafter (Table 3).Troublesome lung symptoms and asthma. u-EPX was not asso-
ciated with an increased risk of developing either recurrent,
episodic viral, early transient, late-onset, or persistent trouble-some lung symptoms during the first 6 years of life (Tables E3and E4), or with asthma by age 7 (Table 2, Table E4).
u-EPX at Age 6 Months
In the overall GEE model including all four time points (6 and18 mo and 4 and 6 yr), we found an increased odds of allergicsensitization, which was borderline significant (odds ratio, 1.21;95% CI, 0.98–1.54; P ¼ 0.10). Log (u-EPX/u-creatinine) ratio atage 6 months was significantly higher in subjects with current sen-sitization at age 6 months (mean difference, 10.28; 95% CI, 0.00–0.56; P ¼ 0.05).
u-EPX at age 6 months was significantly associated with devel-opment of allergic rhinitis at age 6 years (odds ratio, 2.3; 95% CI,1.0–3.5; P¼ 0.05). Apart from this, the analyses of u-EPX at age 6months showed similar association to the atopic end points asdescribed for u-EPX at age 1 month (Tables 2 and 3). In partic-ular, we found no association with any patterns of troublesomelung symptoms or asthma (Tables E3 and E4), and log (u-EPX/u-creatinine) ratio at age 6 months was not significantly increasedin childrenwith current troublesome lung symptoms at age 6months(mean difference, 10.10; 95% CI, 20.25 to 0.46; P ¼ 0.58).
u-LTC4/D4/E4 and u-11b-PGF2a at Age 1 Month
No associations were found between these biomarkers and anyof the end points studied (Tables 2 and 3).
Blood Eosinophil Count at Age 6 Months
Blood eosinophil count at age 6 months was associated with sen-sitization at ages 4 and 6 years, but not significantly in the overallGEE model (Table 2). Blood eosinophil count at 6 months wasstrongly overall associated with eosinophil counts at ages 18 monthsand 4 and 6 years (∆b, 0.41; 95% CI, 0.31–0.51; P, 0.0001). Therewas no association of blood eosinophil count at age 6 months withthe development of allergic rhinitis, nasal eosinophilia, eczema,troublesome lung symptoms, or asthma (Tables 2 and 3).
DISCUSSION
Principal Findings
u-EPX in healthy 1-month-old neonates was significantly associ-atedwith development of allergic sensitization, nasal eosinophilia,and eczema during the first 6 years of life in children of theDanish COPSAC birth cohort suggesting early life eosinophilicactivation before symptom debut in children developing atopy-related conditions.
TABLE 1. BASELINE CHARACTERISTICS
Variable
Age Point
1 Mo 6 Mo 18 Mo 4 Yr 6 Yr
u-EPX, mg/L, median (range) 83.9 (5.4–1,298) 131 (14.8–2,293)u-LTC4/D4/E4, mg/L, median (range) 0.05 (0–19.4)u-11b-PGF2a, mg/L, median (range) 0.20 (0.03–1.5)Blood eosinophil count, 3109/L, median (range) 0.29 (0.02–1.6) 0.21 (0.02–1.2) 0.24 (0.01–3) 0.33 (0–3.5)Allergic sensitization, prevalence, % (n)* 7.1 (24) 11.6 (38) 26.6 (77) 36.3 (97)Allergic rhinitis, prevalence, % (n) 9.3 (24)Nasal eosinophilia, prevalence, % (n)† 6.7 (17)Asthma, prevalence, % (n)‡ 13.6 (41)
Definition of abbreviations: PG ¼ prostaglandin; u-EPX ¼ urinary eosinophil protein X; u-LT ¼ urinary leukotriene.* Allergic sensitization ¼ any sensitization for cat, dog, horse, birch, timothy grass, mugwort, house dust mites, molds, hen’s egg, cow’s milk, fish, wheat, peanut,
soybean, or shrimp.yNasal eosinophilia > 11 on Meltzer’s semiquantitative scale.zAsthma at age 7 yr.
658 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE VOL 184 2011

Strengths and Limitations of the Study
This study provides the first data of urinary inflammatorymarkers measured in healthy neonates before development ofany atopic symptom. Previous studies have solely investigatedsubjects with established atopy (3–10).
The differential associations with u-EPX associating with sev-eral atopic traits during preschool age and u-LTC4/D4/E4 andu-11b-PGF2a without association with any of the atopic endpoints make the risk of a chance finding unlikely.
It isamajorstrengthofthisstudythattheclinicalendpointswerecollected in a closely monitored single-center birth cohort studywithcomprehensivelongitudinaldataondevelopmentofatopicdis-orders. The risk of misclassification and variability in the clinicaldata was minimized because all diagnoses were controlled by theCOPSACdoctorswhoactedasgeneralpractitioners for thecohort.Riskof recall biaswasminimizedbecause the families attended theresearch unit at half-yearly sessions and at acute symptomatic peri-ods. Parental misinterpretation of symptoms was minimized be-cause all mothers have a history of asthma and high prevalenceof related atopic disorders, such as eczemaand rhinitis, and clinicalassessments were made at all visits by the COPSAC doctors.
The symptom diaries on troublesome lung symptoms (signif-icant cough or wheeze or dyspnea) maintained by the parentsday-to-day from birth until age 7 years is another significantstrength of the study increasing the sensitivity of the asthmadiagnosis (21). The diagnostic specificity was ensured by theresearch doctors making all diagnoses at the clinical researchcenter minimizing the risk of misclassification by differentdoctors. Furthermore, the asthma diagnoses were strictly basedon an algorithm including only children responding to inhaledcorticosteroids and currently in need of this treatment after re-peated attempts to withdraw the treatment (i.e., we have notincluded children with intermittent asthma in this end pointdefinition). Other studies with less specific diagnostic criteriainevitably led to a higher prevalence of asthma. However, ourapproach with a strong emphasis on diagnostic specificity hasproved powerful in both genetic (23, 26, 27) and clinical asso-ciation studies (1, 2).
The high-risk nature of the cohort is a limitation to the gen-eralizability of our findings and replication is needed in an un-selected population-based cohort.
Meaning of the Study
It is intriguing that elevation of the biomarker u-EPX in healthysymptom-free newborns precedes the development of atopy later
in childhood. u-EPX is a biomarker known to correlate well witheosinophil count in blood and bronchoalveolar lavage fluid (28).Therefore, our findings suggest eosinophilic activation beforeatopy-related symptoms develop.
Elevated level of u-EPX in healthy asymptomatic neonateswas associated with later development of allergic sensitizationand eczema during the first 6 years of life. Previous studies haveconsistently reported increased u-EPX in preschoolers withestablished allergic sensitization (3, 5) and atopic dermatitis(4, 29), and in children more than 5 years of age with a diagnosisof atopic asthma (5, 6, 30, 31). We found no association betweenu-EPX at ages 1 or 6 months and the later development oftroublesome lung symptoms or asthma, nor was u-EPX elevatedin 6-month-old children with current troublesome lung symp-toms, which is in agreement with a previous report of 1-year-oldwheezy infants (32) and probably reflects the fact that airway
Figure 1. Association between urinary eosinophil protein X in healthy1-month-old neonates and allergic sensitization during preschool age.The figure shows odds ratios of allergic sensitization at ages 6 and 18months and 4 and 6 years (filled dot ¼ odds ratio; vertical bar ¼ 95%confidence interval) and the overall odds ratio calculated by a generalestimating equation model. OR ¼ odds ratio.
TABLE 2. ASSOCIATION AMONG URINE BIOMARKERS AT AGES 1 AND 6 MONTHS, BLOOD EOSINOPHIL COUNT AT AGE 6 MONTHS,AND DEVELOPMENT OF ALLERGIC SENSITIZATION, BLOOD EOSINOPHIL COUNT, ALLERGIC RHINITIS, NASAL EOSINOPHILIA, ANDASTHMA DURING THE FIRST 6 YEARS OF LIFE
Allergic Sensitization,* 0–6 Yr† Blood Eosinophil Count, 0–6 Yr† Allergic Rhinitis, 6 Yr Nasal Eosinophilia, 6 Yr Asthma, 7 Yr
Inflammatory MarkersOdds Ratio(95% CI) P Value
b-Coefficient(95% CI) P Value
Odds Ratio(95% CI) P Value
Odds Ratio(95% CI) P Value
Odds Ratio(95% CI) P Value
u-EPX, 1 mo 1.49 (1.08 to 1.89) 0.02 0.08 (20.04 to 0.19) 0.18 1.6 (0.7 to 3.8) 0.25 3.2 (1.2 to 8.8) 0.02 1 (0.5 to 1.8) 0.99u- LTC4/D4/E4, 1 mo 1.14 (0.95 to 1.32) 0.14 0.02 (20.04 to 0.08) 0.56 1.3 (0.8 to 2.1) 0.27 1.2 (0.8 to 1.9) 0.37 1 (0.7 to 1.4) 0.87u-11b-PGF2a, 1 mo 1.003 (0.60 to 1.41) 0.99 20.01 (20.10 to 0.09) 0.90 0.6 (0.3 to 1.3) 0.20 1 (0.4 to 2.3) 0.96 0.7 (0.4 to 1.43 0.23u-EPX, 6 mo 1.21 (0.98 to 1.54) 0.10 0.08 (20.02 to 0.18) 0.01 2.3 (1 to 3.5) 0.05 3 (1.4 to 5.3) 0.04 1 (0.6 to 1.8) 0.93Blood eosinophil
count, 6 mo1.30 (0.90 to 1.69) 0.14 0.41 (0.31 to 0.51)‡ ,0.0001 0.8 (0.4 to 1.7) 0.59 0.9 (0.4 to 2.4) 0.90 1.1 (0.6 to 2.1) 0.71
Definition of abbreviations: CI ¼ confidence interval; PG ¼ prostaglandin; u-EPX ¼ urinary eosinophil protein X; u-LT ¼ urinary leukotriene.* Allergic sensitization ¼ any sensitization for cat, dog, horse, birch, timothy grass, mugwort, house dust mites, molds, hen’s egg, cow’s milk, fish, wheat, peanut,
soybean, or shrimp.yAllergic sensitization and blood eosinophil count are measured at ages 6 and 18 mo and 4 and 6 yr. Models for these end points are based on general estimating
equations; P values are robust score tests.z In this model the outcome was blood eosinophil count measured at ages 18 mo and 4 and 6 yr.
Chawes, Bønnelykke, Bisgaard: Urinary Inflammatory Markers and Childhood Atopy 659

eosinophils are scarce in this age group (33). In contrast, elevatedEPX in nasal lavage samples from a population of healthy4-week-old infants at high risk of atopy was significantly asso-ciated with the development of wheezing at age 6 months (34).However, this was a questionnaire-based survey with “a doc-tor’s diagnosis of wheezy bronchitis” as the main outcome mea-sure and the authors found no association between EPX andparental observations of wheeze (34).
We also found a significant association between u-EPX at age1 month and presence of nasal eosinophilia at 6 years of age,which has not been reported previously. Elevated u-EPX at ages1 and 6 months showed increased odds of allergic rhinitis at age 6years and the association was significant for the 6-month sample.A previous study found no association between u-EPX and al-lergic rhinitis (3), but this was based on questionnaire diagnosisin children at age 3 years (35 cases among 903 children) wherea diagnosis of rhinitis is infrequent and difficult to establish (35).
The mechanism behind this presymptom eosinophilic activa-tion is unknown. The origin of an early life eosinophilic activa-tion might be dermal or nondermal (29). A dermal contributionto elevated u-EPX is suggested by increasing levels of u-EPX inchildren with increasing severity of atopic dermatitis (4). How-ever, the gut mucosa has been proposed as a nondermal focus ofeosinophilic inflammation in infants with food allergy (36),which is plausible because food sensitization prevails duringinfancy. Neonates with elevated u-EPX may host a distinct dys-functional eosinophil cell immune phenotype with altered sur-face antibodies resulting in an increased liability to degranulateEPX and other eosinophil basic proteins. In addition, geneticvariants in the eosinophil pathway activation genes might mod-ulate immunoregulation (e.g., via IL-5, IL-10, IL-13, and IFN-g)of eosinophil granulocytes (37, 38) and contribute to increaseddegranulation of EPX.
Blood eosinophil count at age 6 months was strongly associ-ated with persistent blood eosinophilia until age 6 years, but in-terestingly, it showed poorer association with all other atopic endpoints than u-EPX at 1 and 6 months of age. This suggests thatu-EPX is a better assessment of eosinophil activity than theblood cell count.
We found no association between u-LTC4/D4/E4 and u-11b-PGF2a at age 1 month and any of the studied atopic end points.LTs and PGs are released during the immediate early phaseallergic reaction by degranulation of IgE-sensitized mast cells,but are also released within the first hours of the late-phasereaction from several inflammatory cells types, such as mono-nuclear cells and basophilic granulocytes (39). In contrast, EPXis solely secreted by activated eosinophils, which are the pre-dominant inflammatory cell type in the chronic late-phase re-action (16). The different cellular origin and temporal releasepattern of EPX, LTC4/D4/E4, and 11b-PGF2a in the inflammatorycascade might explain why only EPX seems to play a role in the
inception of atopy very early in life. Future cellular studies offunctional and regulatory aspects of the eosinophil granulocytemay help understand initiation of atopic disease early in life.
The clinical implication of our findings is that elevated u-EPXearly in life seems to herald the onset of atopy-related conditions,such as allergic sensitization to food and inhaled allergens, aller-gic rhinitis, nasal eosinophilia, and eczema, but not troublesomelung symptoms or asthma during preschool age. The lack of as-sociation with preschool troublesome lung symptoms may reflectthe heterogeneity of symptom triggers in this age group whereallergens serve a quantitatively minor role compared with trig-gers of troublesome lung symptoms and asthma later in life.
Conclusions
u-EPXmeasured in healthy asymptomatic 1-month-old neonateswas associated with the development of allergic sensitization, na-sal eosinophilia, and eczema during preschool age. This suggestsongoing disease pathology including activation of eosinophilgranulocytes preceding the development of childhood atopy-related disorders.
Author Disclosure: B.L.K.C. does not have a financial relationship with a commer-cial entity that has an interest in the subject of this manuscript. K.B. was a con-sultant for Merck and GlaxoSmithKline (GSK) and was on the Advisory Board forMerck. He received lecture fees from Merck and GSK. H.B. was a consultant forChiesi and was on the Advisory Board for Merck. He received lecture fees fromMerck and AstraZeneca (AZ). He was an expert witness for NeoLab and receivedgrant support from Novartis and Chiesi. He received grant support form theLundbeck Foundation and the Danish Medical Research Foundation.
Acknowledgment: The authors gratefully express their gratitude to the childrenand families of the COPSAC cohort study for all their support and commitment.The authors acknowledge and appreciate the unique efforts of the COPSAC researchteam. The authors thank Phadia ApS, and especially Bjarne Kristensen and all labo-ratory crew at Phadia ApS, Allerød, Denmark, for assistance with analyses of theurine samples.
References
1. Chawes BL, Buchvald F, Bischoff AL, Loland L, Hermansen M, HalkjaerLB, Bonnelykke K, Bisgaard H. Elevated exhaled nitric oxide in high-risk neonates precedes transient early but not persistent wheeze. Am JRespir Crit Care Med 2010;182:138–142.
2. Bisgaard H, Hermansen MN, Buchvald F, Loland L, Halkjaer LB,Bonnelykke K, Brasholt M, Heltberg A, Vissing NH, Thorsen SV,et al. Childhood asthma after bacterial colonization of the airway inneonates. N Engl J Med 2007;357:1487–1495.
3. Gore C, Peterson CG, Kissen P, Simpson BM, Lowe LA, Woodcock A,Custovic A. Urinary eosinophilic protein X, atopy, and symptomssuggestive of allergic disease at 3 years of age. J Allergy Clin Immunol2003;112:702–708.
4. Pucci N, Lombardi E, Novembre E, Farina S, Bernardini R, Rossi E,Favilli T, Vierucci A. Urinary eosinophil protein X and serum eo-sinophil cationic protein in infants and young children with atopicdermatitis: correlation with disease activity. J Allergy Clin Immunol2000;105:353–357.
TABLE 3. ASSOCIATION AMONG URINE BIOMARKERS AT AGES 1 AND 6 MONTHS, BLOODEOSINOPHIL COUNT AT AGE 6 MONTHS, AND THE DEVELOPMENT OF ECZEMA IN THE FIRST6 YEARS OF LIFE
Eczema, 0–1 Yr Eczema, 0–6 Yr
Inflammatory Markers Hazard Ratio (95% CI) P Value Hazard Ratio (95% CI) P Value
u-EPX, 1 mo 1.4 (1–2) 0.05 1.1 (0.8–1.5) 0.51u- LTC4/D4/E4, 1 mo 1 (0.8–1.2) 0.95 1 (0.8–1.1) 0.79u-11b-PGF2a, 1 mo 1.1 (0.7–1.5) 0.74 1.1 (0.8–1.4) 0.59u-EPX, 6 mo 1.5 (1.1–2) 0.02 1.3 (1–1.7) 0.04Blood eosinophil count, 6 mo 1.2 (0.8–1.7) 0.31 1.2 (0.9–1.6) 0.19
Definition of abbreviations: CI ¼ confidence interval; PG ¼ prostaglandin; u-EPX ¼ urinary eosinophil protein X; u-LT ¼urinary leukotriene.
660 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE VOL 184 2011

5. Oymar K, Bjerknes R. Urinary eosinophil protein X in children withasthma: influence of atopy and airway infections. Pediatr AllergyImmunol 2001;12:34–41.
6. Severien C, Artlich A, Jonas S, Becher G. Urinary excretion of leuko-triene E4 and eosinophil protein X in children with atopic asthma.Eur Respir J 2000;16:588–592.
7. Higashi N, Taniguchi M, Mita H, Ishii T, Akiyama K. Nasal blockageand urinary leukotriene E4 concentration in patients with seasonalallergic rhinitis. Allergy 2003;58:476–480.
8. Oh JW, Shin SA, Lee HB. Urine leukotriene E and eosinophil cationicprotein in nasopharyngeal aspiration from young wheezy children.Pediatr Allergy Immunol 2005;16:416–421.
9. Oommen A, Grigg J. Urinary leukotriene E4 in preschool children withacute clinical viral wheeze. Eur Respir J 2003;21:149–154.
10. Bochenek G, Nagraba K, Nizankowska E, Szczeklik A. A controlledstudy of 9alpha,11beta-PGF2 (a prostaglandin D2 metabolite) inplasma and urine of patients with bronchial asthma and healthy con-trols after aspirin challenge. J Allergy Clin Immunol 2003;111:743–749.
11. Bisgaard H. The Copenhagen Prospective Study on Asthma in Childhood(COPSAC): design, rationale, and baseline data from a longitudinalbirth cohort study. Ann Allergy Asthma Immunol 2004;93:381–389.
12. Bisgaard H, Hermansen MN, Loland L, Halkjaer LB, Buchvald F. In-termittent inhaled corticosteroids in infants with episodic wheezing. NEngl J Med 2006;354:1998–2005.
13. Koller DY. Sampling methods: urine/blood analysis. Am J Respir CritCare Med 2000;162:S31–S33.
14. Ballardini N, Nilsson C, Nilsson M, Lilja G. ImmunoCAP PhadiatopInfant: a new blood test for detecting IgE sensitisation in children at 2years of age. Allergy 2006;61:337–343.
15. Wickman M, Ahlstedt S, Lilja G, van Hage HM. Quantification of IgEantibodies simplifies the classification of allergic diseases in 4-year-oldchildren. A report from the prospective birth cohort study–BAMSE.Pediatr Allergy Immunol 2003;14:441–447.
16. Howarth PH, Persson CG, Meltzer EO, Jacobson MR, Durham SR,Silkoff PE. Objective monitoring of nasal airway inflammation inrhinitis. J Allergy Clin Immunol 2005;115:S414–S441.
17. Chawes BL, Kreiner-Moller E, Bisgaard H. Objective assessments ofallergic and nonallergic rhinitis in young children. Allergy 2009;64:1547–1553.
18. Chawes BL, Kreiner-Moller E, Bisgaard H. Upper and lower airwaypatency are associated in young children. Chest 2010;137:1332–1337.
19. Chawes BL, Bonnelykke K, Kreiner-Moller E, Bisgaard H. Childrenwith allergic and nonallergic rhinitis have a similar risk of asthma. JAllergy Clin Immunol 2010;126:567–573.
20. Braun-Fahrlander C, Wuthrich B, Gassner M, Grize L, Sennhauser FH,Varonier HS, Vuille JC. Validation of a rhinitis symptom question-naire (ISAAC core questions) in a population of Swiss school childrenvisiting the school health services. SCARPOL-team. Swiss Study onChildhood Allergy and Respiratory Symptom with respect to AirPollution and Climate. International Study of Asthma and Allergiesin Childhood. Pediatr Allergy Immunol 1997;8:75–82.
21. Bisgaard H, Pipper CB, Bonnelykke K. Endotyping early childhoodasthma by quantitative symptom assessment. J Allergy Clin Immunol2011;127:1155–1164.
22. Brand PL, Baraldi E, Bisgaard H, Boner AL, Castro-Rodriguez JA,Custovic A, de BJ, de Jongste JC, Eber E, Everard ML, et al. Defi-nition, assessment and treatment of wheezing disorders in preschoolchildren: an evidence-based approach. Eur Respir J 2008;32:1096–1110.
23. Bisgaard H, Bonnelykke K, Sleiman PM, Brasholt M, Chawes B,Kreiner-Moller E, Stage M, Kim C, Tavendale R, Baty F, et al.Chromosome 17q21 gene variants are associated with asthma and
exacerbations but not atopy in early childhood. Am J Respir Crit CareMed 2009;179:179–185.
24. Bisgaard H, Simpson A, Palmer CN, Bonnelykke K, McLean I,Mukhopadhyay S, Pipper CB, Halkjaer LB, Lipworth B, Hankinson J,et al. Gene-environment interaction in the onset of eczema in infancy:filaggrin loss-of-function mutations enhanced by neonatal cat expo-sure. PLoS Med 2008;5:e131.
25. Halkjaer LB, Loland L, Buchvald FF, Agner T, Skov L, Strand M,Bisgaard H. Development of atopic dermatitis during the first 3 yearsof life: the Copenhagen prospective study on asthma in childhoodcohort study in high-risk children. Arch Dermatol 2006;142:561–566.
26. Bonnelykke K, Pipper CB, Tavendale R, Palmer CN, Bisgaard H.Filaggrin gene variants and atopic diseases in early childhood assessedlongitudinally from birth. Pediatr Allergy Immunol 2010;21:954–961.
27. Sleiman PM, Flory J, Imielinski M, Bradfield JP, Annaiah K, Willis-Owen SA, Wang K, Rafaels NM, Michel S, Bonnelykke K, et al.Variants of DENND1B associated with asthma in children. N EnglJ Med 2010;362:36–44.
28. Cottin V, Deviller P, Tardy F, Cordier JF. Urinary eosinophil-derivedneurotoxin/protein X: a simple method for assessing eosinophil de-granulation in vivo. J Allergy Clin Immunol 1998;101:116–123.
29. Oymar K, Bjerknes R. Urinary eosinophil protein X in children withatopic dermatitis: relation to atopy and disease activity. Allergy 2000;55:964–968.
30. Kristjansson S, Strannegard IL, Strannegard O, Peterson C, Enander I,Wennergren G. Urinary eosinophil protein X in children with atopicasthma: a useful marker of antiinflammatory treatment. J Allergy ClinImmunol 1996;97:1179–1187.
31. Lugosi E, Halmerbauer G, Frischer T, Koller DY. Urinary eosinophilprotein X in relation to disease activity in childhood asthma. Allergy1997;52:584–588.
32. Wojnarowski C, Halmerbauer G, Mayatepek E, Gartner C, Frischer T,Forster J, Kuehr J. Urinary leukotriene E(4), eosinophil protein X,and nasal eosinophil cationic protein are not associated with re-spiratory symptoms in 1-year-old children. Allergy 2001;56:883–888.
33. Saglani S, Payne DN, Zhu J, Wang Z, Nicholson AG, Bush A, JefferyPK. Early detection of airway wall remodeling and eosinophilic in-flammation in preschool wheezers. Am J Respir Crit Care Med 2007;176:858–864.
34. Frischer T, Halmerbauer G, Gartner C, Rath R, Tauber E, Schierl M,Koller DY, Urbanek R, Forster J, Kuhr J. Eosinophil-derived pro-teins in nasal lavage fluid of neonates of allergic parents and the de-velopment of respiratory symptoms during the first 6 months of life.Collaborative SPACE team. Study on the Prevention of Allergy inChildren in Europe. Allergy 2000;55:773–777.
35. Kulig M, Klettke U, Wahn V, Forster J, Bauer CP, Wahn U. De-velopment of seasonal allergic rhinitis during the first 7 years of life.J Allergy Clin Immunol 2000;106:832–839.
36. Majamaa H, Laine S, Miettinen A. Eosinophil protein X and eosinophilcationic protein as indicators of intestinal inflammation in infants withatopic eczema and food allergy. Clin Exp Allergy 1999;29:1502–1506.
37. Hoffjan S, Ostrovnaja I, Nicolae D, Newman DL, Nicolae R, GangnonR, Steiner L, Walker K, Reynolds R, Greene D, et al. Genetic vari-ation in immunoregulatory pathways and atopic phenotypes in in-fancy. J Allergy Clin Immunol 2004;113:511–518.
38. Kabesch M, Depner M, Dahmen I, Weiland SK, Vogelberg C,Niggemann B, Lau S, Illig T, Klopp N, Wahn U, et al. Polymorphismsin eosinophil pathway genes, asthma and atopy. Allergy 2007;62:423–428.
39. Gelfand EW. Inflammatory mediators in allergic rhinitis. J Allergy ClinImmunol 2004;114:S135–S138.
Chawes, Bønnelykke, Bisgaard: Urinary Inflammatory Markers and Childhood Atopy 661

Elevated Exhaled Nitric Oxide in High-Risk NeonatesPrecedes Transient Early but Not Persistent WheezeBo L. K. Chawes1, Frederik Buchvald1, Anne Louise Bischoff1, Lotte Loland1, Mette Hermansen1,Liselotte B. Halkjær1, Klaus Bønnelykke1, and Hans Bisgaard1
1Danish Pediatric Asthma Center, Copenhagen University Hospital, Gentofte, Denmark
Rationale: Elevated fractional exhaled nitric oxide (FENO) concentra-tion has been suggested to predict early childhood wheeze andsensitization.Objectives: To investigate the association between FENO in asymp-tomatic neonates and the development of wheeze patterns andatopic intermediary phenotypes in the first 6 years of life.Methods: We measured FENO in 253 healthy 1-month-old neonatesfrom the Copenhagen Prospective Study on Asthma in Childhoodbirth cohort and monitored prospectively wheezy episodes by dailydiary cards during the first 6 years of life. Total IgE, specific IgE, andblood eosinophil count were assessed at age 6 months, 4 years, and 6years. Associations were studied by Cox regression, logistic regres-sion, and generalized linear models.Measurements and Main Results: Increased neonatal FENO level wassignificantly associated with the development of recurrent wheezein the first year of life (hazard ratio, 2.63; 95% confidence interval,1.1 to 6.2; P 5 0.026) but not thereafter. The association was unaffectedby environmental tobacco smoke exposure. FENO was not associatedwithelevatedlevelsof total IgE,specificIgE,orbloodeosinophil countatany age point and was unrelated to neonatal lung function.Conclusions: An elevated FENO level in asymptomatic neonates born tomothers with asthma preceded the development of transient earlywheezing, but not persistent wheezing during preschool age, and wasunrelated to atopy. This suggests an early disease process other thansmall airway caliber contributing to the transient wheezing phenotype.
Keywords: atopy; children; fractional exhaled nitric oxide; infants;wheeze
Fraction of exhaled nitric oxide (FENO) has been proposed asa noninvasive marker of eosinophilic airway inflammation (1),which can be measured in both school-aged (2) and preschool-aged children (3, 4), and in infants (5, 6). FENO is increased inchronic asthma (7), before exacerbations in children withasthma (8, 9), and in preschool children with recurrent wheeze(3, 4, 10). Increased FENO values in neonates have beensuggested to predict severe respiratory symptoms in the firstyear of life, but only in a particular subgroup of newborns withatopic and/or smoking mothers (6).
The aim of our study was to analyze the association betweenFENO in asymptomatic neonates and the development of wheezyphenotypes and intermediary atopic end-points during the first6 years of life. We studied the association between FENO in253 healthy 1-month-old neonates and subsequent developmentof wheeze patterns, blood eosinophil count, total immunoglobu-lin E (IgE), and allergic sensitization in the first 6 years of life.The children were included from the Copenhagen ProspectiveStudy on Asthma in Childhood (COPSAC) birth cohort born ofmothers with a history of asthma.
None of the results in this study has been previously reportedin abstract or any other form.
METHODS
Design
The study was nested in COPSAC: a single-center, prospective clinicalbirth cohort study of 411 children born to mothers with asthma,enrollment of which was previously described in detail (11–13). Keyexclusion criteria included the following: gestational age less than 36weeks, severe congenital abnormality, neonatal mechanical ventilation,and symptoms of lower airway infection before inclusion.
All subjects participated in a randomized controlled clinical trial ofintermittent treatment with inhaled budesonide versus placebo for 2-week periods during wheezy episodes in the first 3 years of life, showingno short-term or long-term treatment effect (11).
Oral and written informed consent was obtained from all parents ofparticipating children. The study followed the guiding principles of theDeclaration of Helsinki, and was approved by the Ethics Committeefor Copenhagen (KF 01–289/96) and the Danish Data ProtectionAgency (2008-41-1754).
Neonatal FENO Measurements
FENO was measured at 1 month of age by an offline technique (14),after the completion of neonatal lung function testing during sedation(15, 16). FENO measurement was performed in asymptomatic neonates,that is, before any respiratory symptoms or prescription of inhaledcorticosteroid.
A mask covering the mouth and nose attached to a two-way valvewas gently placed on the infant’s face during sedation. A respiratoryresistance of at least 5 cm H2O was achieved by a resistor fitted into the
AT A GLANCE COMMENTARY
Scientific Knowledge on the Subject
Elevated exhaled nitric oxide has been suggested to predictearly childhood wheeze and sensitization.
What This Study Adds to the Field
Increased exhaled nitric oxide level in asymptomaticneonates born to mothers with asthma precedes transientearly wheezing, but not persistent wheezing during pre-school age, and is unrelated to elevated levels of total IgE,specific IgE, and blood eosinophil count.
(Received in original form September 13, 2009; accepted in final form March 12, 2010)
Supported by private and public research funds (all COPSAC support is listed atwww.copsac.com); the Lundbeck Foundation, the Pharmacy Foundation of1991, the Augustinus Foundation, the Danish Medical Research Council, andthe Danish Pediatric Asthma Centre provided core support for COPSAC. Thefunding agencies did not have any role in study design, data collection andanalysis, decision to publish, or preparation of the manuscript.
Correspondence and requests for reprints should be addressed to Hans Bisgaard,M.D., D.M.Sci., Copenhagen Prospective Studies on Asthma in Childhood,Danish Pediatric Asthma Center, Health Sciences, University of Copenhagen,Copenhagen University Hospital, Gentofte, Ledreborg Alle 34, 2820 Gentofte,Denmark. E-mail: [email protected]
This article has an online supplement, which is accessible from this issue’s table ofcontents at www.atsjournals.org
Am J Respir Crit Care Med Vol 182. pp 138–142, 2010Originally Published in Press as DOI: 10.1164/rccm.200909-1377OC on March 18, 2010Internet address: www.atsjournals.org

expiratory side of the valve. The infant inhaled ambient air, butmeasurements were canceled if ambient NO exceeded 10 parts perbillion (ppb). When stable tidal breathing was assured, an impermeablebag (Quintron Instrument, Milwaukee, WI) was attached to theexpiratory side of the valve and 750 ml of mixed expired air wascollected. Within 15 minutes, the bags were attached to the inlet of theNO analyzer and air was continuously sampled from the bags at a flowof 110 ml/minute. The FENO level was measured with a chemilumines-cence analyzer (CLD 77 AM; EcoPhysics, Duernten, Switzerland). Thesensitivity was 0.1 ppb and rise time (0–90%) was 0.1 second. Theanalyzer was calibrated at least once daily with certified NO gas (100ppb) (AGA, Gothenburg, Sweden). FENO levels were calculated as themean of duplicate measurements in each infant.
Wheezy Phenotypes
Wheezy episodes. Wheeze was explained to the parents as wheeze orwhistling sounds, breathlessness, or cough severely affecting the well-being of the child, and was recorded by the parents in daily diaries ascomposite dichotomized scores from birth until age 6 years. Doctors atthe COPSAC research unit reviewed symptom definition and the diaryentries with the parents at 6-monthly clinical sessions and at acuteclinic visits for wheezy episodes defined from the diaries as threeconsecutive days with wheeze.
Recurrent wheeze. Recurrent wheeze was defined as five wheezyepisodes within 6 months, or daily symptoms for four consecutiveweeks. The symptom character was judged by the COPSAC doctor tobe typical of discrete wheezy episodes and included symptoms betweenepisodes, such as exercise-induced symptoms; prolonged nocturnalcough; persistent cough not associated with a common cold; symptomscausing wakening at night; and need for intermittent rescue use ofinhaled b2-agonist. Age at onset of recurrent wheeze was used as theprimary end point.
Episodic viral wheeze. Episodic viral wheeze (17) characterizedchildren suffering discrete wheezy episodes, with the child being wellbetween episodes and treated intermittently with inhaled b2-agonist.
Atopic Intermediary Phenotypes
Blood was sampled at age 6 months, 4 years, and 6 years for mea-surements of eosinophil count, total IgE, and specific IgE (18). Sen-sitization was defined as specific IgE equal to or greater than 0.35 kU/L(18, 19) for at least 1 of 15 tested airborne and food allergens.
Statistical Analysis
Changes in risk of recurrent wheeze due to FENO concentration wereanalyzed as hazard ratios by Cox regression. The children wereretained in the analysis from birth until age at diagnosis of recurrentwheeze, dropout, or age at end of the observation period (i.e., 1 yr for0–1 yr, 6 yr for 0–6 yr), whichever occurred first. The associationbetween FENO level and number of wheezy episodes at ages 0–1 and 0–6 years was analyzed by Poisson regression, based on robust varianceestimation. Logistic regression was used to calculate odds ratios (ORs)of episodic viral wheeze and allergic sensitization. Associations be-tween FENO, blood eosinophil count, and total IgE were studied bygeneralized linear models expressing results as b coefficients.
The models were adjusted for sex, age at measurement, environ-mental tobacco smoke exposure (maternal smoking in third trimester(yes/no), and nicotine in hair at age 1 year [20]) (6, 21), previousmiscarriages, number of siblings (22), child care attendance (22),minute volume (21, 23), and ambient NO level.
Results are reported per 20 ppb increase in FENO with 95%confidence intervals (95% CI) in parentheses; P < 0.05 was consideredsignificant. All analyses were done in SAS version 9.1 (SAS Institute,Inc., Cary, NC).
Further details of the methods are given in the online supplement.
RESULTS
COPSAC enrolled 411 infants and performed neonatal lungfunction testing in 402 at 1 month of age by the raised volumerapid thoracoabdominal compression technique (15, 16). Thiscurrent protocol was enacted approximately 1 year into the
enrollment period, leaving 286 infants eligible for FENO mea-surement. Measurements were canceled if the child woke upbefore expired air was collected (n 5 5), ambient NO exceeded10 ppb (n 5 21) (14), or technical problems arose (n 5 7),leaving 253 infants for analysis.
Baseline Characteristics
The study group consisted of 122 males (48%). Thirty-sevenmothers (15%) smoked during the third trimester of theirpregnancy. In the first year of life, 138 children suffered wheezyepisodes (median number of episodes, 2; quartile 1 [Q1]–Q3, 1–4; range, 1–8), whereas 172 children had at least one wheezyepisode until age 6 years (median, 6; Q1–Q3, 3–12; range, 1–59).Recurrent wheeze was diagnosed in 4% of the children beforeage 1 year, and in a further 17% before age 6 years. Anthro-pometrics, lung function data, total IgE levels, eosinophilcounts, age at child care start, and hair nicotine levels at age 1year are given in Table 1.
Infants not included in this nested study were comparable tothe study group with respect to anthropometrics at study date,mothers smoking during the third trimester, previous miscar-riages, number of siblings, and age at child care start (univariatetests; data available on request).
FENO and Wheezy Phenotypes
The cumulative risk of recurrent wheeze during the first 6 yearsof life for neonates with FENO concentration above and belowthe third quartile of the study group (22 ppb) is illustrated inFigure 1, suggesting that neonatal FENO is associated witha transient early wheezy phenotype. Accordingly, increasedFENO concentration measured at age 1 month was significantlyassociated with the development of recurrent wheeze in the firstyear of life (hazard ratio, 2.63; 95% CI, 1.1–6.2; P 5 0.026), butnot thereafter (Table 2). Adjusting the analyses for sex, age,maternal smoking in the third trimester, nicotine in hair at age 1year, previous miscarriages, number of siblings, child careattendance, minute volume, and ambient NO level did not alterthe results substantially (Table 2).
Elevated neonatal FENO level was also associated with thedevelopment of episodic viral wheeze in the first year of life
TABLE 1. STUDY GROUP ANTHROPOMETRICS, LUNG FUNCTIONDATA, TOTAL IGE, BLOOD EOSINOPHIL COUNT, CHILD CAREATTENDANCE, AND HAIR NICOTINE LEVELS
n MedianInterquartile
Range Range
Age at study date, d 253 44 35–55 20–96Weight at study date, kg 253 5.0 4.5–5.5 3.0–8.2Length at study date, cm 253 56.4 54.5–58.2 47.9–64.5FENO, ppb 253 16 12–22 1–57Minute volume, ml 253 622.2 526.5–684.0 230.3–990.1Ambient NO, ppb 253 6 4–7 2–10Blood eosinophil count at
age 6 mo, 109/L220 0.3 0.2–0.4 0.1–1.5
Blood eosinophil count atage 4 yr, 109/L
190 0.2 0.2–0.4 0.05–1.7
Blood eosinophil count atage 6 yr, 109/L
178 0.3 0.2–0.5 0–3.5
Total IgE at age 6 mo, kU/L 222 4.0 2.2–9.3 0.1–80.7Total IgE at age 4 yr, kU/L 198 25.8 12.6–64.7 2.1–722.0Total IgE at age 6 yr, kU/L 189 42.7 18.7–110.0 0.8–2,423.7Age at child care start, d 238 342 244–411 140–1,074Nicotine in hair at
age 1 yr, ng/mg229 0.7 0.3–2.2 0.03–43.5
Definition of abbreviations: FENO 5 fraction of exhaled nitric oxide; ppb 5 partsper billion.
Chawes, Buchvald, Bischoff, et al.: Exhaled Nitric Oxide and Wheezy Disorder 139

(OR, 2.24; 95% CI, 1.3–3.9; P 5 0.010), but not until age 6 years(OR, 0.90; 95% CI, 0.5–1.6; P 5 0.701) (Table 3).
In addition, FENO concentration was associated with thenumber of wheezy episodes during the first year of life, but notuntil age 6 years. The incidence risk ratio of having wheezyepisodes during the first year of life was 1.36 (95% CI, 1.1–1.7;P 5 0.011) and 0.93 (95% CI, 0.8–1.1; P 5 0.135) until age6 years (Table 4).
FENO and Environmental Tobacco Smoke Exposure
There was no effect modification from environmental tobaccosmoke exposure on the association between neonatal FENO
levels and the development of recurrent wheeze in the first 6years of life; neither from mothers smoking as assessed byinterview in the third trimester of pregnancy nor when assessedby nicotine in the hair by age 1 year (P values for interactiongreater than 0.2 in all analyses).
FENO and Atopic Intermediary Phenotypes
Neonatal FENO concentration was not associated with levels oftotal IgE, blood eosinophil count, or allergic sensitization, atage 6 months, 4 years, or 6 years (see Tables E1–E3 in the onlinesupplement). Subsequently, we investigated whether total IgE,allergic sensitization, or blood eosinophils at age 6 monthsmodified the association between elevated FENO and the risk ofrecurrent wheeze. None of these intermediary phenotypesinteracted significantly with the association between FENO andearly wheeze (P values for interaction greater than 0.2 in allanalyses).
FENO and Lung Function
To further describe the endophenotype characterized by ele-vated neonatal FENO level, we did a post-hoc analysis of theassociation between FENO, infant lung function, and lungfunction at age 6 years. No association was observed betweenneonatal FENO and measures of infant lung function (FEV0.5,forced expiratory flow at 50% vital capacity [FEF50], and
provocative dose of methacholine causing a 15% fall inFEV0.5 [PD15]; Table E4), nor lung function at age 6 years(FEV1 and maximal midexpiratory flow [MMEF]; Table E5).
DISCUSSION
Principal Findings
FENO level in symptom-free 1-month-old neonates was associ-ated with the development of transient early wheeze, but notpersistent wheeze, in the COPSAC birth cohort of mothers withasthma. There was no association between infant FENO andneonatal lung function or lung function at age 6 years, or withthe development of total IgE, blood eosinophil count, or allergicsensitization, and no effect modification from environmentaltobacco exposure.
Strength and Limitations
The major strength of our study is the 6-year-long clinical follow-upof a birth cohort with prospective monitoring of respiratorysymptoms in daily diary cards and 6-monthly symptom reviewby doctors at the research unit. Risk of misclassification wasminimized as recurrent wheeze was diagnosed from the diariesaccording to predefined algorithms and the families solely attendedthe doctors employed at the clinical research unit for diagnosis andtreatment of any respiratory symptom rather than their familypractitioner.
The major limitation of our study is the setting of a high-riskcohort as all mothers have a history of asthma, which limits theexternal validity of the study. However, the analyses are basedon within-subject associations between FENO and subsequentdevelopment of wheezy phenotypes, which are unlikely to beaffected by the increased risk of atopic diseases.
TABLE 2. YEAR-BY-YEAR ANALYSIS OF ASSOCIATION BETWEENNEONATAL FRACTION OF EXHALED NITRIC OXIDE ANDDEVELOPMENT OF RECURRENT WHEEZE UNTIL AGE 6 YEARS
RecurrentWheeze
FENO per 20 ppb, Crude FENO per 20 ppb, Adjusted*
Hazard Ratio (95% CI) P Value Hazard Ratio (95% CI) P Value
0–1 yr 2.63 (1.1–6.2) 0.026 2.70 (1.0–7.4) 0.0500–2 yr 1.37 (0.7–2.7) 0.381 1.33 (0.7–2.6) 0.4150–3 yr 0.90 (0.4–1.8) 0.752 0.87 (0.4–1.7) 0.6870–4 yr 0.68 (0.3–1.3) 0.263 0.67 (0.3–1.3) 0.2330–5 yr 0.63 (0.3–1.2) 0.171 0.65 (0.3–1.2) 0.1920–6 yr 0.63 (0.3–1.2) 0.159 0.65 (0.3–1.2) 0.169
Definition of abbreviations: CI 5 confidence interval; FENO 5 fraction of exhalednitric oxide; ppb 5 parts per billion.
* FENO per 20 ppb adjusted for sex, age, maternal smoking in third trimester,nicotine in hair at age 1 year, number of previous miscarriages, number ofsiblings, age at start of child care, minute volume, and ambient NO.
Figure 1. Cumulative risk of recurrent wheeze during the first 6 yearsof life stratified by neonatal exhaled nitric oxide concentrations aboveand below the third quartile of the study group.
TABLE 3. ASSOCIATION BETWEEN NEONATAL FRACTIONOF EXHALED NITRIC OXIDE AND EPISODIC VIRAL WHEEZEIN FIRST 6 YEARS OF LIFE
EpisodicViralWheeze
FENO per 20 ppb, Crude FENO per 20 ppb, Adjusted*
Odds Ratio (95% CI) P Value Odds Ratio (95% CI) P Value
0–1 yr 2.24 (1.3–3.9) 0.010 2.11 (1.3–3.7) 0.0140–6 yr 0.90 (0.5–1.6) 0.701 0.91 (0.5–1.7) 0.751
Definition of abbreviations: CI 5 confidence interval; FENO 5 fraction of exhalednitric oxide; ppb 5 parts per billion.
* FENO per 20 ppb adjusted for sex, age, maternal smoking in third trimester,nicotine in hair at age 1 year, number of previous miscarriages, number ofsiblings, age at start of child care, minute volume, and ambient NO.
140 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE VOL 182 2010

The accuracy of the method may be limited as the expiratoryflow was not controlled. This was partly compensated by FENO
assessment in mixed exhaled air, which diminished breath-to-breath variations. In addition, sedation stabilized respirationand the expiratory resistance limited flow range and reducednasal contribution to the exhaled air. FENO levels in our studygroup were comparable to other studies despite differentmethodology (6, 24).
Meaning of the Study
Wheezy disorders are highly prevalent in early childhood (25)and one of the main reasons for hospitalization of preschoolchildren in westernized countries (26). Early age at onset (27)and recurrent severe symptoms (28) are important determinantsof persistent wheeze throughout childhood and subsequentdevelopment of asthma later in life. Thus, the challenge is todevelop noninvasive identification strategies applicable to earlychildhood before onset of first wheeze to improve preventionand treatment. Our findings suggest that neonatal FENO mea-surement cannot provide such risk assessment because it doesnot predict persistent wheeze.
The underlying mechanism causing raised FENO in neonatesbefore the development of transient wheeze is still unknown.This may not reflect atopic inflammation of the airways becausethere are few eosinophils in the airways even in symptomaticinfants (29). Accordingly, neonatal FENO was not associatedwith the development of increased levels of total IgE, specificIgE, or increased blood eosinophil count at the ages of 6months, 4 years, or 6 years. Cross-sectional studies have shownelevated FENO levels in older children with eosinophilia andallergic sensitization (30), but no difference in FENO level insensitized as compared with nonsensitized infants (31), suggest-ing that elevated FENO in this age group is not a marker ofatopic inflammation. In line with these findings, we observeda similar association between neonatal FENO and preschoolrecurrent wheeze in neonates with and without raised total IgE,specific IgE, or blood eosinophils. Therefore, it may be specu-lated that other inflammatory processes are driving transientearly wheeze and increased FENO.
Latzin and colleagues also reported that high FENO valuesafter birth in a subgroup of neonates born of atopic andsmoking mothers were associated with an increased risk ofsevere respiratory symptoms in the first year of life (6), but didnot monitor their study population after age 1 year. We foundthat elevated FENO in 1-month-old neonates born to motherswith asthma was associated with transient early wheezing, butnot persistent wheezing in our 6-year follow-up with dailysymptom recordings. In contrast to the findings of Latzin andcolleagues, we saw no effect from mothers smoking as assessedby interview in the third trimester of pregnancy, or whenassessed by nicotine in the hair by age 1 year.
Transient early wheezers present recurrent bronchial ob-struction early in life typically triggered by viral infections, andwith remittance during the first years of life (32). These childrenhave reduced pulmonary function at age 16 years as comparedwith children who never wheezed, but are as unlikely to wheezethrough adolescence as never-wheezers (33). Impaired neonatallung function measured before any lower respiratory tractinfection has been demonstrated in transient early wheezers(34), suggesting that congenitally small airway dimensions maypredispose to an increased wheeze propensity. We found noassociation between neonatal FENO and measures of infant lungfunction, suggesting that elevated FENO precedes a distincttransient early wheezing endophenotype independent of theunderlying lung function.
Asthma is likely to have several specific endophenotypesassociated with distinct clinical features, divergent underlyingmolecular causes, and distinct treatment responses (35). Iden-tifying these endophenotypes is essential for improved under-standing, prediction, and treatment of disease. At preschoolage, asthma-like symptoms represent a heterogeneous group ofdifferent endophenotypes. At present, these can only be disen-tangled retrospectively by their clinical presentation during thefirst 6 years of life (32). Elevated FENO in high-risk neonatesseems to precede a particular transient early endophenotypecharacterized by infant wheezy symptoms but is not associatedwith wheeze later in childhood. Further understanding of thisdisease mechanism may help to improve diagnosis and treat-ment of wheeze symptoms early in life.
Conclusion
An elevated FENO level measured in healthy neonates ofmothers with asthma before any wheezy symptom precedesthe onset of transient early wheezing, but not persistentwheezing, and is unrelated to underlying lung function changesor the development of increased total IgE, specific IgE, andblood eosinophil count. These findings suggest an early diseaseprocess other than small airway caliber contributing to transientearly wheeze.
Conflict of Interest Statement: B.L.K.C. does not have a financial relationship witha commercial entity that has an interest in the subject of this manuscript; F.B.does not have a financial relationship with a commercial entity that has aninterest in the subject of this manuscript; A.L.B. does not have a financialrelationship with a commercial entity that has an interest in the subject of thismanuscript; L.L. does not have a financial relationship with a commercial entitythat has an interest in the subject of this manuscript; M.H. does not havea financial relationship with a commercial entity that has an interest in the subjectof this manuscript; L.B.H. does not have a financial relationship with a commercialentity that has an interest in the subject of this manuscript; K.B. received$10,001–$50,000 from Merck as a website consultant and $1,001–$5,000 fromGlaxoSmithKline as a consultant on educational material, $1,001–$5,000 fromMerck in advisory board fees, $10,001–$50,000 from Merck and $5,001–$10,000 from GlaxoSmithKline in lecture fees; H.B. received $10,001–$50,000from Merck and $10,001–$50,000 from NeoLab in consultancy fees, $10,001–$50,000 from Merck, $10,001–$50,000 from NeoLab, $1,001–$5,000 fromChiesi, and $1,001–$5,000 from Nycomed in advisory board fees, $10,001–$50,000 from Merck and $10,001–$50,000 from AstraZeneca in lecture fees,$1,001–$5,000 from NeoLab, and $1,001–$5,000 from Chiesi for serving as anexpert witness, more than $100,001 from Novartis and more than $100,001from NeoLab in industry-sponsored grants.
Acknowledgment: The authors gratefully acknowledge all children and familiesparticipating in the COPSAC cohort study. The authors thank research assistantsLena Vind, Kirsten Hinsby Mathiesen, and Lotte Klansø.
References
1. American Thoracic Society, European Respiratory Society. ATS/ERSrecommendations for standardized procedures for the online andoffline measurement of exhaled lower respiratory nitric oxide andnasal nitric oxide, 2005. Am J Respir Crit Care Med 2005;171:912–930.
2. Buchvald F, Baraldi E, Carraro S, Gaston B, De JJ, Pijnenburg MW,Silkoff PE, Bisgaard H. Measurements of exhaled nitric oxide in
TABLE 4. ASSOCIATION BETWEEN NEONATAL FRACTIONOF EXHALED NITRIC OXIDE AND NUMBER OF WHEEZYEPISODES IN FIRST 6 YEARS OF LIFE
No. ofWheezyEpisodes
FENO per 20 ppb, Crude FENO per 20 ppb, Adjusted*
Incidence RiskRatio (95% CI) P Value
Incidence RiskRatio (95% CI) P Value
0–1 yr 1.36 (1.1–1.7) 0.011 1.24 (1.0–1.6) 0.0250–6 yr 0.93 (0.8–1.1) 0.135 0.96 (0.8–1.1) 0.253
Definition of abbreviations: CI 5 confidence interval; FENO 5 fraction of exhalednitric oxide; ppb 5 parts per billion.
* FENO per 20 ppb adjusted for sex, age, maternal smoking in third trimester,nicotine in hair at age 1 year, number of previous miscarriages, number ofsiblings, age at start of child care, minute volume, and ambient NO.
Chawes, Buchvald, Bischoff, et al.: Exhaled Nitric Oxide and Wheezy Disorder 141

healthy subjects age 4 to 17 years. J Allergy Clin Immunol 2005;115:1130–1136.
3. Buchvald F, Bisgaard H. FENO measured at fixed exhalation flow rateduring controlled tidal breathing in children from the age of 2 yr. AmJ Respir Crit Care Med 2001;163:699–704.
4. Moeller A, Diefenbacher C, Lehmann A, Rochat M, Brooks-WildhaberJ, Hall GL, Wildhaber JH. Exhaled nitric oxide distinguishes betweensubgroups of preschool children with respiratory symptoms. J AllergyClin Immunol 2008;121:705–709.
5. Gabriele C, Asgarali R, Jaddoe VW, Hofman A, Moll HA, De JongsteJC. Smoke exposure, airway symptoms and exhaled nitric oxide ininfants: the Generation R study. Eur Respir J 2008;32:307–313.
6. Latzin P, Kuehni CE, Baldwin DN, Roiha HL, Casaulta C, Frey U.Elevated exhaled nitric oxide in newborns of atopic mothers precedesrespiratory symptoms. Am J Respir Crit Care Med 2006;174:1292–1298.
7. Kharitonov SA, Yates D, Robbins RA, Logan-Sinclair R, ShinebourneEA, Barnes PJ. Increased nitric oxide in exhaled air of asthmaticpatients. Lancet 1994;343:133–135.
8. Zacharasiewicz A, Wilson N, Lex C, Erin EM, Li AM, Hansel T, KhanM, Bush A. Clinical use of noninvasive measurements of airwayinflammation in steroid reduction in children. Am J Respir Crit CareMed 2005;171:1077–1082.
9. Pijnenburg MW, Hofhuis W, Hop WC, De Jongste JC. Exhaled nitricoxide predicts asthma relapse in children with clinical asthma re-mission. Thorax 2005;60:215–218.
10. Gabriele C, Nieuwhof EM, Van Der Wiel EC, Hofhuis W, Moll HA,Merkus PJ, De Jongste JC. Exhaled nitric oxide differentiates airwaydiseases in the first two years of life. Pediatr Res 2006;60:461–465.
11. Bisgaard H, Hermansen MN, Loland L, Halkjaer LB, Buchvald F.Intermittent inhaled corticosteroids in infants with episodic wheezing.N Engl J Med 2006;354:1998–2005.
12. Bisgaard H, Hermansen MN, Buchvald F, Loland L, Halkjaer LB,Bonnelykke K, Brasholt M, Heltberg A, Vissing NH, Thorsen SV,et al. Childhood asthma after bacterial colonization of the airway inneonates. N Engl J Med 2007;357:1487–1495.
13. Bisgaard H. The Copenhagen Prospective Study on Asthma in Child-hood (COPSAC): design, rationale, and baseline data from a longi-tudinal birth cohort study. Ann Allergy Asthma Immunol 2004;93:381–389.
14. Baraldi E, De Jongste JC. Measurement of exhaled nitric oxide inchildren, 2001. Eur Respir J 2002;20:223–237.
15. Loland L, Buchvald FF, Halkjaer LB, Anhoj J, Hall GL, Persson T,Krause TG, Bisgaard H. Sensitivity of bronchial responsivenessmeasurements in young infants. Chest 2006;129:669–675.
16. Loland L, Bisgaard H. Feasibility of repetitive lung function measure-ments by raised volume rapid thoracoabdominal compression duringmethacholine challenge in young infants. Chest 2008;133:115–122.
17. Brand PL, Baraldi E, Bisgaard H, Boner AL, Castro-Rodriguez JA,Custovic A, de Blic J, De Jongste JC, Eber E, Everard ML, et al.Definition, assessment and treatment of wheezing disorders in pre-school children: an evidence-based approach. Eur Respir J 2008;32:1096–1110.
18. Ballardini N, Nilsson C, Nilsson M, Lilja G. ImmunoCAP PhadiatopInfant—a new blood test for detecting IgE sensitisation in children at2 years of age. Allergy 2006;61:337–343.
19. Wickman M, Ahlstedt S, Lilja G, van Hage HM. Quantification of IgEantibodies simplifies the classification of allergic diseases in 4-year-oldchildren: a report from the prospective birth cohort study BAMSE.Pediatr Allergy Immunol 2003;14:441–447.
20. Sorensen M, Bisgaard H, Stage M, Loft S. Biomarkers of exposure toenvironmental tobacco smoke in infants. Biomarkers 2007;12:38–46.
21. Frey U, Kuehni C, Roiha H, Cernelc M, Reinmann B, Wildhaber JH,Hall GL. Maternal atopic disease modifies effects of prenatal riskfactors on exhaled nitric oxide in infants. Am J Respir Crit Care Med2004;170:260–265.
22. Ball TM, Castro-Rodriguez JA, Griffith KA, Holberg CJ, Martinez FD,Wright AL. Siblings, day-care attendance, and the risk of asthma andwheezing during childhood. N Engl J Med 2000;343:538–543.
23. Hall GL, Reinmann B, Wildhaber JH, Frey U. Tidal exhaled nitric oxidein healthy, unsedated newborn infants with prenatal tobacco expo-sure. J Appl Physiol 2002;92:59–66.
24. Wildhaber JH, Hall GL, Stick SM. Measurements of exhaled nitric oxidewith the single-breath technique and positive expiratory pressure ininfants. Am J Respir Crit Care Med 1999;159:74–78.
25. Newacheck PW, Stoddard JJ. Prevalence and impact of multiple child-hood chronic illnesses. J Pediatr 1994;124:40–48.
26. Kocevar VS, Bisgaard H, Jonsson L, Valovirta E, Kristensen F, Yin DD,Thomas J III. Variations in pediatric asthma hospitalization rates andcosts between and within Nordic countries. Chest 2004;125:1680–1684.
27. Sears MR, Greene JM, Willan AR, Wiecek EM, Taylor DR, FlanneryEM, Cowan JO, Herbison GP, Silva PA, Poulton R. A longitudinal,population-based, cohort study of childhood asthma followed toadulthood. N Engl J Med 2003;349:1414–1422.
28. Lowe LA, Simpson A, Woodcock A, Morris J, Murray CS, Custovic A.Wheeze phenotypes and lung function in preschool children. Am JRespir Crit Care Med 2005;171:231–237.
29. Saglani S, Payne DN, Zhu J, Wang Z, Nicholson AG, Bush A, JefferyPK. Early detection of airway wall remodeling and eosinophilicinflammation in preschool wheezers. Am J Respir Crit Care Med2007;176:858–864.
30. Jouaville LF, Annesi-Maesano I, Nguyen LT, Bocage AS, Bedu M,Caillaud D. Interrelationships among asthma, atopy, rhinitis andexhaled nitric oxide in a population-based sample of children. ClinExp Allergy 2003;33:1506–1511.
31. Tepper RS, Llapur CJ, Jones MH, Tiller C, Coates C, Kimmel R, KislingJ, Katz B, Ding Y, Swigonski N. Expired nitric oxide and airwayreactivity in infants at risk for asthma. J Allergy Clin Immunol 2008;122:760–765.
32. Martinez FD, Wright AL, Taussig LM, Holberg CJ, Halonen M, MorganWJ; Group Health Medical Associates. Asthma and wheezing in thefirst six years of life. N Engl J Med 1995;332:133–138.
33. Morgan WJ, Stern DA, Sherrill DL, Guerra S, Holberg CJ, GuilbertTW, Taussig LM, Wright AL, Martinez FD. Outcome of asthma andwheezing in the first 6 years of life: follow-up through adolescence.Am J Respir Crit Care Med 2005;172:1253–1258.
34. Martinez FD, Morgan WJ, Wright AL, Holberg CJ, Taussig LM.Diminished lung function as a predisposing factor for wheezingrespiratory illness in infants. N Engl J Med 1988;319:1112–1117.
35. Anderson GP. Endotyping asthma: new insights into key pathogenicmechanisms in a complex, heterogeneous disease. Lancet 2008;372:1107–1119.
142 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE VOL 182 2010

Pediatric Pulmonology 50:109–117 (2015)
DENND1BGene Variants AssociateWith Elevated ExhaledNitric Oxide in Healthy High-Risk Neonates
Bo L.K. Chawes, MD, PhD,1 Anne Louise Bischoff, MD, PhD,1 Eskil Kreiner-Møller, MD,1
Frederik Buchvald, MD, PhD,1 Hakon Hakonarson, MD, PhD,2 and Hans Bisgaard, MD, DMSci1*y
Summary. Rationale of the Study: Increased neonatal fraction of exhaled nitric oxide (FeNO) isassociatedwith lung symptomsearly in life, while predictors of neonatal FeNO levels are unknown.The objective of this study was to investigate perinatal and genetic predictors of FeNO in healthyat-risk neonates. Methods: FeNO was measured during sedation by single-breath and tidal-breathing techniques in 253 one-month-old neonates from the Copenhagen Prospective Study onAsthma in Childhood (COPSAC2000) birth cohort. The risk factor analyses included geneticvariants in DENND1B, Filaggrin, and ORMDL3; anthropometrics; demographics; socioeconom-ics; paternal atopy; maternal smoking, and mother’s consumption of paracetamol and antibioticsduring 3rd trimester; and neonatal bacterial airway colonization. Results: FeNO values measuredby the single-breath versus tidal-breathing technique yielded slightly higher values (median,21.0 ppb; range, 2.0–74.0ppb vs. 16.0 ppb; 1.0–67.0ppb;P<0.0001) with increasing differencesconditional on increasing FeNO values (P<0.0001). The multivariable analysis including all riskfactors showed that the DENND1B rs2786098 C allele was associated with increasing levels ofFeNO (additive model;þ2.30 ppb per C allele; 95%CI, 0.10–5.00 ppb; P¼0.04) and that childrenof atopic fathers had elevated FeNO (þ2.90 ppb; 95% CI, 0.38–5.43ppb; P¼0.02). We did notdetect association between the remaining risk factors and neonatal FeNO levels. Conclusion:Increased FeNO in healthy newborns seems strongly influenced by genetics including father’satopy and child’s variants in the DENND1B locus at chromosome 1q31.3. Pediatr Pulmonol.2015;50:109–117. ! 2013 Wiley Periodicals, Inc.
Key words: asthma; genetics; nitric oxide; infant.
Funding source: Lundbeck Foundation; Pharmacy Foundation of 1991; AugustinusFoundation; Danish Medical Research Council and The Danish Pediatric Asthma Centre
INTRODUCTION
Fraction of exhaled nitric oxide (FeNO) is measured asa part of the routine clinical work up in many clinicalpediatric pulmonology centers to diagnose1 and monitorchildhood asthma.2,3 While assessment of FeNO level isstandard in children from approximately 5 years of age,4,5
it is also feasible and reproducible to measure FeNO inneonates.6,7
In a recent report from the Copenhagen ProspectiveStudy on Asthma in Childhood (COPSAC2000) birthcohort born to asthmatic mothers8 we observed a wideinter-subject variation in neonatal FeNO values (1–67 ppb) and subsequently showed that raised FeNOmeasured in asymptomatic healthy neonates prior toany respiratory symptoms is associated with the develop-ment of specific childhood wheezy endotypes.9 WhereasFeNO during school age is interpreted as a marker ofeosinophilic airway inflammation,10 the predictors ofelevated neonatal FeNO are poorly understood.The purpose of the current study was to explore the
previously reported wide range of neonatal FeNO levelsby investigating genetic and early life environmental
1Copenhagen Prospective Studies on Asthma in Childhood; COPSAC,Health Sciences, University of Copenhagen, Copenhagen University
Hospital, Gentofte, Ledreborg All!e 34, Gentofte 2820, Copenhagen,Denmark.
2Centre for Applied Genomics and Division of Human Genetics, The
Children’s Hospital of Philadelphia, University of Pennsylvania School ofMedicine, Philadelphia, Pennsylvania.
Conflict of interest: The authors have no conflicts of interest relevant to this
topic.
Dr. Chawes and Dr. Bischoff contributed equally to this manuscript.
ywww.copsac.com
#Correspondence to: Professor Hans Bisgaard, MD, DMSci, CopenhagenProspective Studies on Asthma in Childhood; COPSAC, Health Sciences,
University of Copenhagen, Copenhagen University Hospital, Gentofte,Ledreborg All!e 34, 2820 Gentofte, Copenhagen, Denmark. E-mail:[email protected]
Received 8 January 2013; Accepted 14 October 2013.
DOI 10.1002/ppul.22958Published online 17 December 2013 in Wiley Online Library(wileyonlinelibrary.com).
! 2013 Wiley Periodicals, Inc.

predictors of the FeNO levels measured in 253 neonatesfrom the COPSAC2000 birth cohort. Environmental riskfactors were selected a priori based on the existingliterature on predictors of neonatal FeNO, for example,parental atopic status and environmental tobacco smokeexposure,7,11,12 but also including well-know pre- andperinatal factors influencing development of wheezydisorders, for example, anthropometrics, socioeconom-ics, antibiotic and paracetamol consumption duringpregnancy, and bacterial colonization of the neonatalairway.13–16 Genetic analyses were performed accordingto a candidate gene approach including only well-known robust early-onset-asthma risk variants, that is,Filaggrin,17 ORMDL3,18 and DENND1B.19
MATERIALS AND METHODS
Study Design
Participants were included from the COPSAC2000
single center prospective clinical birth cohort studyrecruited in 1998–2001. This birth cohort included 411one-month-old high-risk neonates born to mothers with ahistory of asthma. Exclusion criteria were gestational age<36 weeks; any congenital abnormality and systemicillness; requirement of neonatal mechanical ventilation;and symptoms of lower airway infection prior to inclusion.Enrollment and baseline characteristics of the COP-SAC2000 cohort were previously described in detail.8,13,20
Ethics
The study followed the guiding principles of theDeclaration of Helsinki, and was approved by the EthicsCommittee of Copenhagen (KF 01-289/96) and TheDanish Data Protection Agency (2008-41-1754).8 Oraland written informed consent was obtained from allparents of participating children.
Neonatal FeNO Measurements
FeNO level was measured at 1 month of age aftercompletion of neonatal spirometry testing utilizing raised
volume rapid thoracoabdominal compression (RVRTC)technique during sedation with an oral dose of chloralhydrate 90mg/kg.21–24 Measurements and bag samplingwere performed in asymptomatic neonates prior to anyrespiratory symptoms, and by two separate techniques inall neonates.Single-Breath Technique25. After completion of baseline
lung functionmeasurement, a mask attached to a two-wayvalve was placed on the infants face covering the mouthand nose. A 250ml impermeable bag (Quintron Instru-ment, Milwaukee, WI) was connected to the expiratoryside of the valve with a resistor interposed assuring anexpiratory resistance of at least 5 cm H2O.Thereafter, a compression force, similar to the one used
for the previous spirometry assessment by inflation of asqueeze jacket wrapped around the infants thorax andabdomen, was applied, that is, leading to a standardizedforced expiration into the bag with flow similar to the oneobtained during spirometry measurements. The squeezemaneuver was repeated 10 times collecting five expira-tions into two bags.Tidal-Breathing Technique26.After completion of the last
squeeze maneuver, steady tidal breathing was assured inthe sedated infant. Using the same mask and two-wayvalve as for the single-breath technique, a 750mlimpermeable bag (Quintron Instrument) was attached tothe expiratory side of the valve, and two bags of expiredair were sampled during steady tidal breathing. Therespiratory frequency and the collection time wereregistered to calculate respiratory minute volume.During both techniques, the infant inhaled ambient air,
but if ambient nitric oxide (NO) exceeded 10 ppb, theFeNO measurement was cancelled.FeNO Measurements. Within 15min, the bags were
attached to the inlet of a NO-analyzer and the expired airwas sampled continuously from the bags with a constantflow of 110ml/min. Concentration of FeNO wasmeasured by a chemiluminescence analyzer (EcoPhysicsCLD 77 AM, Duernten, Switzerland). The sensitivity was0.1 ppb and rise time (0–90%) was 0.1 sec. The analyzerwas calibrated once daily using certified NO gas(100 pbb) (AGA, Gothenburg, Sweden).FeNO levels were analyzed and calculated as the mean
of duplicate measurements in each infant separate foreach sampling technique.
Pre- and Perinatal Risk Factors
Anthropometrics: Height and weight were assessedprior to neonatal FeNO measurement. Body mass index(BMI) was calculated and categorized as 7–12, 12–13,13–14, and 14–17 kg/m2 as previously reported.14
Socioeconomic status was evaluated from yearlyhousehold income at birth of the infant classified intothree groups as low (<53.000s), medium (53.000–80.000s), and high (>80.000s).
ABBREVIATIONS::BMI Body mass index
COPSAC Copenhagen prospective studies on asthma in childhoodFEF50 Forced expiratory flow at 50% of the functional vital
capacityFeNO Fractional exhaled Nitric OxideFEV0.5 Forced expiratory volume in 0.5 seconds.
GLM General linear modelsGWAS Genome-wide association study
NO Nitric oxideQQ-plot Quantile-quantile plotRVRTC Raised Volume rapid thoracoabdominal compression
110 Chawes et al.
Pediatric Pulmonology

Demographics comprised sex and older siblings at birth(yes/no).Paternal atopy was any history of asthma, allergic
rhinitis and/or atopic dermatitis (yes/no).Exposures during 3rd trimester of pregnancy included
smoking (yes/no), paracetamol [acetaminophen] (yes/no), and antibiotic usage (yes/no).Bacterial colonization of the airway was assessed at
age 1 month from hypopharyngeal aspirates performedimmediately after the FeNO sampling procedure aspreviously reported.13 Colonization with Streptococcuspneumoniae, Haemophilus influenzae, and/or Moraxellacatarrhalis was used as a binary endpoint (yes/no).
Genetics
Blood was sampled at age 6 months, centrifuged andseparated into serum and serum cells, and immediatelystored at !808C until analysis. After thawing, DNAwaspurified from the serum cells using the QIAamp DNABlood Maxi Kit (Qiagen, Inc., Valencia, CA).8
Filaggrin genotyping for the two common independentnull-mutations R501X and 2282del4 was performed aspreviously described.27 Children were assigned as havinga filaggrin mutation if they carried at least one of themutations.ORMDL3 genotyping: Allelic discrimination at the
rs7216389 single nucleotide polymorphism on chromo-some 17q12–21 was performed as previously detailed.18
DENND1B genotyping: Allelic discrimination at thers2786098 on chromosome 1q31.3 was performed asdescribed by Sleiman et al.19
Statistical Analysis Strategy
First, we investigated the distribution of the neonatalFeNO values by quantile–quantile plots (QQ-plot) andShapiro-Wilk’s test for normality.Second, we performed a Box-Cox transformation
analysis in the lambda-range from !3 to 3 investigatinglambda at 0.5 subsequent steps.Third, we tested agreement between the two FeNO
measuring techniques (single-breath vs. tidal-breathing)by calculating the mean difference between the measuredFeNO values, standard deviation of the difference, pairedt-tests, Bland–Altman plots and by fitting a regressionmodel for the difference between the methods conditionalon the average using both raw data and transformed dataaccording to the results of the Box-Cox analysis.Fourth, univariable risk factor analyses of neonatal
FeNO (sex; paternal atopy; household income; BMI;older siblings at birth; bacterial colonization at age1 month; smoking, usage of paracetamol and antibioticsin 3rd trimester; DENND1B, filaggrin, and ORMDL3)were performed using general linear models (GLM)utilizing the raw untransformed FeNO data and FeNO
values transformed according to the results of the Box-Cox transformation analysis. We used an additive modelwhen analyzing rs2786098 in the DENND1B gene usingthe A allele as reference and the C allele as risk factor(AA¼ 0; AC¼ 1; CC¼ 2). Association with theORMDL3 T allele was investigated in a recessive modelusing the CC and CT genotypes as reference.18 Allanalyses were adjusted for respiratory minute volume11,28
estimated from the bag volume (750ml), time in seconds ittook to fill the bag, and number of respirations: respiratoryminute volume¼ (750ml/no. respirations/time)# 60.Fifth, a multivariable analysis was performed with
complete cases only including all variables in the initialGLM model with subsequent backward elimination ofnon-significant variables using a cut-off at P< 0.10. Wechallenged the multivariable model by performing aforward selection procedure based on the largest value ofadjusted R2 with a P< 0.10 cut off, that is, when allcandidate effects for entry at a step have a statisticalsignificance level <0.10.In addition, we calculated coefficients of variation
(CV) between the duplicate measurements of FeNO in thetwo bags utilizing the raw data in the formula: CV¼standard deviation of the difference between bags/meanof the difference.Results are reported as b-coefficients with 95%
confidence intervals in brackets, a P-value $0.05 isconsidered significant. Analyses were done using SASversion 9.2 (SAS Institute, Cary, NC).
RESULTS
Baseline Characteristics
This current protocol was initiated 1 year after startingthe recruitment of the COPSAC2000 cohort leaving 286 of411 recruited infants eligible for neonatal FeNOmeasure-ments. FeNO levels were assessed with both techniques atone month of age in 253 of the 286 infants (Fig. E1Online).FeNO values, lung function data, bacterial airway
colonization, gender distribution, anthropometrics, de-mographics, older siblings at birth, paternal atopy,exposures during 3rd trimester of pregnancy, and geneticsare outlined in Table 1.Infants enrolled in the study compared to the rest of the
COPSAC2000 cohort had lower FEV0.5, less paracetamolconsumption in 3rd trimester, and higher household income(Table 1). Sincewe did not detect association between thesevariables and FeNO levels, we do not assume this selectionbias affected the main findings of the study.
Neonatal FeNO Measurements
Median neonatal FeNO level was 21.0 ppb (range; 2.0–74.0 pbb) measured with the single-breath technique and
DENND1B Gene Variants and Neonatal FeNO 111
Pediatric Pulmonology

16.0 ppb (range, 1.0–67.0 ppb) with the tidal-breathingtechnique. The coefficient of variation between theduplicate measurements of FeNO in the two bags was0.99 for the single-breath technique and 1.05 for the tidal-breathing technique.QQ-plots of the raw neonatal FeNO values (Fig. E2
Online) showed a skewed distribution of FeNO measuredby both techniques and the Shapiro–Wilk test indicatedthat the FeNO data was not normally distributed(P< 0.0001). ABox-Cox transformation analysis showedthat the best lambda value for normalizing data from bothmeasuring techniques was 0.5 corresponding to a squareroot transformation.
A paired t-test of the square root transformed FeNOvalues showed slightly higher values measured by thesingle-breath versus tidal-breathing technique (meandifference, 0.54; standard deviation of the difference,0.39; P< 000.1). Bland–Altman plots of the raw data andthe square root transformed data indicated that thedifference was dependent on the average of measuredFeNO levels with increasing difference conditional onincreasing average (Fig. E3Online), whichwas confirmedby fitting regression models for the raw data: estimate,0.27; 95% CI, 0.23–0.31; P< 0.0001, and the square roottransformed data: estimate 0.13; 95% CI, 0.09–0.16;P< 0.0001).
TABLE 1—Characteristics of the Study Population
Full cohort(N¼ 411)
Not enrolled inFeNO study(N¼ 158)
Enrolled inFeNO study(N¼ 253)
Studygroup (N) P-value"
FeNOSingle-breath, ppb, median (Q1–Q3) — — 21.0 (14.0–30.0) 252 —Tidal-breathing, ppb, median (Q1–Q3) — — 16.0 (12.0–22.0) 253 —Minute volume, ml, median (Q1–Q3) — — 616.4 (523.3–681.8) 253 —
Lung functionFEV0.5, Z-score, mean (SD) 0.0 (1.0) 0.15 (0.96) #0.09 (1.02) 250 0.011
FEF50, Z-score, mean (SD) 0.0 (1.0) 0.02 (0.99) #0.02 (1.01) 246 NS1
AnthropometricsAge at study date, days, median (Q1–Q3) 42.0 (33.0–55.0) 38.0 (32.0–50.0) 44.0 (35.0–56.0) 253 NS1
Weight at study date, kg, median (Q1–Q3) 4.9 (4.5–5.5) 4.8 (4.3–5.5) 5.0 (4.5–5.5) 253 NS1
Height at study date, cm, median (Q1–Q3) 56.3 (54.4–58.0) 56.0 (54.1–57.8) 56.4 (54.5–58.2) 252 NS1
BMI at study date, kg/m2, median (Q1–Q3) 15.6 (14.8–16.5) 15.4 (14.2–16.5) 15.6 (14.9–16.5) 252 NS1
DemographicsGender, female sex (%) 51 49 52 253 NS2
Older siblings at birth (%) 39 40 39 240 NS2
Household income (%) — — — 238 0.0022
Low <53.000s 29 40 23 — —Medium 53.000–80.000s 47 41 51 — —High >80.000s 23 19 26 — —Risk factors
Smoking, 3rd trimester (%) 15 16 15 253 NS2
Paracetamol, 3rd trimester (%) 55 68 47 253 <0.0012
Antibiotics, 3rd trimester (%) 30 31 30 253 NS2
Paternal atopy (%) 56 57 54 246 NS2
Bacterial colonization, 1 mo (%) 21 23 20 252 NS2
GeneticsDENND1B (%) 234 NS2
AA 4 3 5 — —AC 27 28 26 — —CC 69 69 69 — —
ORMDL3 (TT) (%) 29 28 30 241 NS2
Filaggrin mutation (%) 11 13 9 244 NS2
NS: P> 0.05.FeNO: Fraction of exhaled nitric oxide.FEV0.5: Forced expiratory volume in 0.5 sec.FEF50: Forced expiratory flow at 50% of the functional vital capacity.BMI: Body mass index."Comparison: enrolled versus not enrolled.1Unpaired t-test.2Chi-square test, where N< 5 Fishers-exact test.
112 Chawes et al.
Pediatric Pulmonology

We chose the raw untransformed FeNO values from theleast invasive tidal-breathing technique to investigatepossible risk factors influencing neonatal FeNO levels inour primary analyses and added auxiliary analyses withsquare root transformed FeNO values.
Risk Factor Analysis of Neonatal FeNO
Univariable Analyses. The univariable risk factor analy-ses showed higher levels of FeNO in children of atopicfathers (þ3.57 ppb; 95%CI, 1.20 to 5.97;P< 0.01) and inchildren with the DENND1B C allele (þ2.55 ppb per Callele; 95% CI, 0.38 to 4.71; P¼ 0.02) (Figs. 1 and 2).FeNO was higher in children of fathers with asthma andeczema (P< 0.01), borderline higher in children offathers with rhinitis and allergy (P¼ 0.08 for both),whereas we did not detect association between neonatalFeNO values and maternal rhinitis, allergy or eczema(Table E1 Online). We did not detect association betweenneonatal FeNO levels and sex; BMI; older siblings atbirth; tobacco, paracetamol, and antibiotic consumptionin 3rd trimester; household income; bacterial colonizationof the airway; Filaggrin mutations or ORMDL3 genevariants (Table 2).Ancillary analysis with square root transformed FeNO
values confirmed the results of the primary analyses withhigher FeNO estimates in children with atopic fathers(estimate, 0.45; 95% CI, 0.17–0.73; P< 0.01) and inchildren with the DENND1B allele (estimate per C allele,0.28; 95% CI, 0.03–0.54; P¼ 0.03). Also, utilizing FeNOvalues measured by the single-breath method yieldedcomparable results with higher values in children of
atopic fathers (þ4.81 ppb; 95% CI, 2.06 to7.56 ppb;P< 0.01) and in children with the DENND1B C allele(þ2.98 ppb per C allele; 95% CI, 0.42 to 5.54 ppb;P¼ 0.02).
Fig. 1. Neonatal FeNO measured by tidal-breathing methodstratified by paternal atopic status. Solid line: mean; dashedline: median.
Fig. 2. Neonatal FeNO measured by tidal-breathing methodstratified by DENND1B genotype. Solid line: mean; dashed line:median.
TABLE 2—Univariate Risk Factor Analysis of NeonatalFeNO
Neonatal FeNO, tidal-breathing technique, ppb
b-coefficient 95% CI P-value
Female sex 1.05 #1.32 to 3.43 0.38Household income
Low <53.000s ReferenceMedium 53.000–80.000s #1.63 #4.75 to 1.49 0.30High >80.000s 0.05 #3.50 to 3.60 0.98
Father, atopy 3.58 1.20 to 5.97 <0.01Bacterial colonization at
age 1 mo#1.99 #4.97 to 1.00 0.19
Smoking, 3rd trimester #1.46 #4.82 to 1.91 0.39Paracetamol, 3rd trimester #1.84 #4.21 to 0.54 0.13Antibiotics, 3rd trimester 0.38 #2.21 to 2.98 0.77Older siblings at birth 0.81 #1.71 to 3.33 0.53BMI, kg/m2, 4 weeks
7–12 Reference12–13 6.29 #13.92 to 26.49 0.5413–14 7.33 #12.20 to 26.86 0.4614–17 3.52 #15.42 to 22.47 0.71
DENND1B1 (additive model) 2.55 0.38 to 4.71 0.02Filaggrin mutation #0.50 #4.77 to 3.76 0.82ORMDL3 0.30 #2.39 to 2.99 0.83
1Per C allele.Variables significantly associated with neonatal FeNO are in bold(P< 0.05).
DENND1B Gene Variants and Neonatal FeNO 113
Pediatric Pulmonology

Multivariable Analysis. In the multivariable analysis withbackward selection, including all pre- and perinatal riskfactors and genetics, DENND1B gene variants(þ2.30 ppb per C allele; 95% CI, 0.10 to 5.00 ppb;P¼ 0.04) and paternal atopy (þ2.90 ppb; 95% CI, 0.38 to5.43 ppb; P¼ 0.02) remained predictors of increasedneonatal FeNO. The forward selection procedure stoppedat step 2 with paternal atopy (P¼ 0.01) and DENND1B(P¼ 0.05) included in the model resulting in R2¼ 0.037thus confirming the results from the backward selectionprocedure.
DISCUSSION
Principle Findings
Neonatal FeNO measured prior to any respiratorysymptoms exhibited a wide dispersion ranging between 1and 67 ppb. Neonatal FeNO levels were increased frompaternal atopy and DENND1B gene variants, suggestingthat the wide range of FeNO values in healthy high-risknewborns is mainly driven by genetics.
Strengths and Limitations of the Study
It is a strength of this study that one study physicianperformed all FeNO measurements following standardoperating procedures for both methods including criteriafor accepting and rejecting data. FeNO measurementswere completed in a high proportion of the eligiblechildren (88.4%) and measurements were done sequen-tially by both techniques in 99.6% of the children. AllFeNO values were double checked against source dataand the database was subsequently locked for furtherediting.This is the first study to measure and compare the two
different measuring techniques of neonatal FeNO and thelargest study of FeNO in neonates measured prior to anyrespiratory symptoms.The assessment of FeNO in neonates is complicated by
requirements of steady breathing at a constant flow. Amethodological limitation is that the exhaled flowwas notcontrolled during FeNO measurements by the tidal-breathing technique, but this was partially compensatedby the fact that the children were sedated ensuring steadytidal breathing which together with the fixed respiratoryresistance limited the flow range. The resistor fitted intothe expiratory side of the valve also ensured that the softpalate closed during sampling and thereby limited nasalcontamination of the breath sample.28,29 Finally weapplied the alternative technique of FeNO measurementsduring fixed flow repeating the RVRTC technique used forthe previous spirometric assessments assuring standard-ized flow similar to the one obtained during spirometry.23
The absolute FeNO values measured may also havebeen influenced by the previous infant spirometry that
could have altered expiratory flows during gas sampling.However, these conditions were the same for all theinfants and should not compromise our ability to studyrisk factors driving the inter-subject variation in thecohort.A limitation of the study is the low number of subjects
in the study cohort which precludes a Genome-wideassociation study (GWAS) approach to investigate geneticpredictors of neonatal FeNO. Instead we applied acandidate gene approach including only threewell-knownrisk variants of childhood asthma. The novel finding ofassociation between DENND1B gene variants and raisedneonatal FeNO is biologically plausible and wasidentified in the univariable and in the multivariableanalysis. The set of ancillary analyses showing compara-ble results including the untransformed FeNO valuesobtained by both techniques as well the square roottransformed FeNO values increase our confidence in thefindings. Adjustments for the multiplicity of testsperformed were not made; consequently, the apparentassociation with both DENNDIB and paternal atopy maybe chance findings. Replication in a large populationbased cohort is therefore needed.Another limitation of the study is the setting of a high-
risk cohort which limits the ability to generalize thefindings from the risk-factor analysis. Still, the medianFeNO levels of our study group are comparable tofindings from population based cohorts.7,11,25,26
Interpretation
It was an interesting observation that healthy neonatespresented a very wide range of FeNO values rangingbetween 1 and 67 ppb that led us to study what possiblepre- or perinatal factors could explain such variability.The risk factor analyses showed that neonates of atopicfathers and neonates carrying the DENND1B C allelehave increased neonatal FeNO levels, but the analysis wasinconclusive in regard to association between FeNO andother pre- and perinatal environmental risk factorsstudied.The C allele of the DENND1B single nucleotide
polymorphism has recently been found to confer anincreased risk of childhood asthma,19 but other complexinflammatory diseases such as Crohns disease30 andprimary biliary cirrhosis31 have also been associated withvariants in this gene suggesting a common immunedysregulation. The mechanism by which DENND1Bgene variants may influence NO production is unknown,but DENND1B is expressed by natural killer cells anddendritic cells which play an important role linking innateand adaptive immune responses in the process ofdeveloping tolerability or immunity.32 DENND1B genevariants may therefore induce a skewing of the immune
114 Chawes et al.
Pediatric Pulmonology

response and a dysregulated inflammatory responseleading to elevated FeNO levels very early in life.We have previously shown that raised neonatal FeNO is
associated with wheezing illnesses early in life but isunrelated to development of other asthma- and allergyrelated traits such as sensitization, allergic rhinitis,elevated total-IgE, and blood eosinophil count duringpre-school age.9 Neonatal FeNO is not associated withinfant pulmonary function9 suggesting that DENND1Brisk variants induce an early inflammatory diseaseprocess independent of small airway caliber contributingto the development of a specific endotype of childhoodasthma.Previous studies failed to detect association between
FeNO and paternal atopy;7,11 the discrepancy betweenthat and our finding could be explained by theCOPSAC2000 cohort being born to mothers with asthmaas previous studies showed that maternal atopy modifiesthe prenatal risk of elevated FeNO.7 We conjecture that inour COPSAC2000 cohort association between neonatalFeNO and maternal atopic disorders (e.g., eczema,allergic sensitization, and rhinitis) may not be evidentdue to all mothers having a history of asthma.Evidence of association between prenatal tobacco
smoke exposure and neonatal FeNO was inconclusive. Incontrast, others have reported that neonatal FeNO isaffected by both pre- and postnatal tobacco exposure.7,12
However, these results are ambiguous as one studyshowed that infants exposed pre- and postnatally totobacco smoke had lower FeNO than infants exposed onlyafter birth and never-exposed infants12 whereas anotherstudy reported higher FeNO in infants exposed tomaternal smoking after birth.7
Studies of FeNO in infants are scarce33 because mostmeasuring techniques are complicated and difficult toperform. The two techniques used in the current studyhave previously been shown to be feasible.25,26 Thesingle-breath technique ensures a high relatively constantexpiratory flow for the 10 exhalations used to sample airin each child, but not a constant inter-child expiratoryflow, which is considered a prerequisite in FeNOmeasurements as FeNO is flow-dependent.26 The tidal-breathing technique partly compensates this issue bysampling exhaled air in a bag during several breathingcycles producing roughly similar results compared tomeasurements donewith fixed expiratory flow.34 Our datashowed that the single-breath technique yielded slightlyhigher FeNO values than the tidal-breathing techniquewith increasing differences by increasing FeNO values.However, ancillary analyses utilizing FeNO obtainedfrom both techniques showed comparable associations topaternal atopy and DENND1B variants and we thereforesuggest usage of the least invasive tidal-breathingtechnique for future studies.
CONCLUSION
Variants in the DENND1B locus of chromosome1q31.3 and paternal atopy were found to be associatedwith elevated FeNO in healthy Danish high-risk neonates.Associations were not detected between FeNO and otherpre- and perinatal environmental factors studied suggest-ing that raised FeNO early in life is primarily an inheritedtrait. These findings however need replication in largepopulation-based GWAS cohorts.
ACKNOWLEDGMENTS
We gratefully express our gratitude to the children andfamilies of the COPSAC cohort study for all their supportand commitment. We acknowledge and appreciate theunique efforts of the COPSAC research team. COPSAC isfunded by private and public research funds all listed onwww.copsac.com. The Lundbeck Foundation; the Phar-macy Foundation of 1991; Augustinus Foundation; theDanish Medical Research Council and The DanishPediatric Asthma Centre provided core support forCOPSAC. The funding agencies did not have any rolein study design, data collection and analysis, decision topublish, or preparation of the manuscript.
Contributions
The guarantor of this study is H.B. who is responsiblefor the integrity of the work as a whole, from conceptionand design to conduct of the study and acquisition of data,analysis and interpretation of data and writing of themanuscript. A.L.B., B.C., E.K.M., F.B., H.H. andH.B. areresponsible for data acquisition, analysis, interpretation,and writing the manuscript. All co-authors have contrib-uted substantially to the analyses and interpretation of thedata, and have provided important intellectual input andapproval of the final version of the manuscript.The corresponding author had full access to the data
and had final responsibility for the decision to submit forpublication.
REFERENCES
1. Kharitonov SA, Yates D, Robbins RA, Logan-Sinclair R,Shinebourne EA, Barnes PJ. Increased nitric oxide in exhaledair of asthmatic patients. Lancet 1994;343:133–135.
2. Pijnenburg MW, Hofhuis W, Hop WC, de Jongste JC. Exhalednitric oxide predicts asthma relapse in children with clinicalasthma remission. Thorax 2005;60:215–218.
3. Zacharasiewicz A, Wilson N, Lex C, Erin EM, Li AM, Hansel T,Khan M, Bush A. Clinical use of noninvasive measurements ofairway inflammation in steroid reduction in children. Am J RespirCrit Care Med 2005;171:1077–1082.
4. Buchvald F, Baraldi E, Carraro S, Gaston B, De JJ, PijnenburgMW, Silkoff PE, Bisgaard H. Measurements of exhaled nitricoxide in healthy subjects age 4 to 17 years. JAllergy Clin Immunol2005;115:1130–1136.
DENND1B Gene Variants and Neonatal FeNO 115
Pediatric Pulmonology

5. Moeller A, Diefenbacher C, Lehmann A, Rochat M, Brooks-Wildhaber J, Hall GL, Wildhaber JH. Exhaled nitric oxidedistinguishes between subgroups of preschool children withrespiratory symptoms. J Allergy Clin Immunol 2008;121:705–709.
6. Gabriele C, Nieuwhof EM, Van Der Wiel EC, Hofhuis W, MollHA, Merkus PJ, de Jongste JC. Exhaled nitric oxide differentiatesairway diseases in the first two years of life. Pediatr Res2006;60:461–465.
7. Latzin P, Kuehni CE, Baldwin DN, Roiha HL, Casaulta C, Frey U.Elevated exhaled nitric oxide in newborns of atopic mothersprecedes respiratory symptoms. Am J Respir Crit Care Med2006;174:1292–1298.
8. Bisgaard H. The Copenhagen Prospective Study on Asthma inChildhood (COPSAC): design, rationale, and baseline data from alongitudinal birth cohort study. Ann Allergy Asthma Immunol2004;93:381–389.
9. Chawes BL, Buchvald F, Bischoff AL, Loland L, Hermansen M,Halkjaer LB, Bonnelykke K, Bisgaard H. Elevated exhaled nitricoxide in high-risk neonates precedes transient early but notpersistent wheeze. Am J Respir Crit CareMed 2010;182:138–142.
10. ATS/ERS recommendations for standardized procedures for theonline and offline measurement of exhaled lower respiratory nitricoxide and nasal nitric oxide, 2005. Am J Respir Crit Care Med2005;171:912–930.
11. Frey U, Kuehni C, Roiha H, Cernelc M, Reinmann B, WildhaberJH, Hall GL. Maternal atopic disease modifies effects of prenatalrisk factors on exhaled nitric oxide in infants. Am J Respir CritCare Med 2004;170:260–265.
12. Gabriele C, Asgarali R, Jaddoe VW, Hofman A, Moll HA, deJongste JC. Smoke exposure, airway symptoms and exhaled nitricoxide in infants: the Generation R study. Eur Respir J2008;32:307–313.
13. Bisgaard H, Hermansen MN, Buchvald F, Loland L, Halkjaer LB,Bonnelykke K, Brasholt M, Heltberg A, Vissing NH, Thorsen SV,Stage M, Pipper CB. Childhood asthma after bacterial coloniza-tion of the airway in neonates. N Engl J Med 2007;357:1487–1495.
14. Bisgaard H, Loland L, Holst KK, Pipper CB. Prenataldeterminants of neonatal lung function in high-risk newborns. JAllergy Clin Immunol 2009;123:651–657, 657.
15. Kreiner-Moller E, Sevelsted A, Vissing NH, Schoos AM, BisgaardH. Infant acetaminophen use associates with early asthmaticsymptoms independently of respiratory tract infections: theCopenhagen Prospective Study on Asthma in Childhood 2000(COPSAC (2000)) cohort. J Allergy Clin Immunol 2012;130:1434–1436.
16. Stensballe LG, Simonsen J, Jensen SM, Bonnelykke K, BisgaardH. Use of antibiotics during pregnancy increases the risk of asthmain early childhood. J Pediatr 2013;162:832–838.
17. Bonnelykke K, Pipper CB, Tavendale R, Palmer CN, Bisgaard H.Filaggrin gene variants and atopic diseases in early childhoodassessed longitudinally from birth. Pediatr Allergy Immunol2010;21:954–961.
18. Bisgaard H, Bonnelykke K, Sleiman PM, Brasholt M, Chawes B,Kreiner-Moller E, Stage M, Kim C, Tavendale R, Baty F, PipperCB, Palmer CN, Hakonarsson H. Chromosome 17q21 genevariants are associated with asthma and exacerbations but notatopy in early childhood. Am J Respir Crit Care Med2009;179:179–185.
19. Sleiman PM, Flory J, Imielinski M, Bradfield JP, Annaiah K,Willis-Owen SA, Wang K, Rafaels NM, Michel S, Bonnelykke K,ZhangH, KimCE, Frackelton EC, Glessner JT, Hou C, Otieno FG,Santa E, Thomas K, Smith RM, Glaberson WR, Garris M,Chiavacci RM, Beaty TH, Ruczinski I, Orange JM, Allen J,
Spergel JM, Grundmeier R, Mathias RA, Christie JD, von ME,Cookson WO, Kabesch M, Moffatt MF, Grunstein MM, BarnesKC, Devoto M, Magnusson M, Li H, Grant SF, Bisgaard H,Hakonarson H. Variants of DENND1B associated with asthma inchildren. N Engl J Med 2010;362:36–44.
20. Bisgaard H, Hermansen MN, Loland L, Halkjaer LB, Buchvald F.Intermittent inhaled corticosteroids in infants with episodicwheezing. N Engl J Med 2006;354:1998–2005.
21. Hayden MJ, Devadason SG, Sly PD, Wildhaber JH, Lesouef PN.Methacholine responsiveness using the raised volume forcedexpiration technique in infants. Am J Respir Crit Care Med1997;155:1670–1675.
22. Loland L, Buchvald FF, Halkjaer LB, Anhoj J, Hall GL, Persson T,Krause TG, Bisgaard H. Sensitivity of bronchial responsivenessmeasurements in young infants. Chest 2006;129:669–675.
23. Loland L, Bisgaard H. Feasibility of repetitive lung functionmeasurements by raised volume rapid thoracoabdominal com-pression during methacholine challenge in young infants. Chest2008;133:115–122.
24. Turner DJ, Stick SM, Lesouef KL, Sly PD, Lesouef PN. A newtechnique to generate and assess forced expiration from raisedlung volume in infants. Am J Respir Crit Care Med 1995;151:1441–1450.
25. Wildhaber JH, Hall GL, Stick SM.Measurements of exhaled nitricoxide with the single-breath technique and positive expiratorypressure in infants. Am J Respir Crit Care Med 1999;159:74–78.
26. Hall GL, Reinmann B, Wildhaber JH, Frey U. Tidal exhaled nitricoxide in healthy, unsedated newborn infants with prenatal tobaccoexposure. J Appl Physiol 2002;92:59–66.
27. Palmer CN, Irvine AD, Terron-Kwiatkowski A, Zhao Y, Liao H,Lee SP, Goudie DR, Sandilands A, Campbell LE, Smith FJ,O’Regan GM, Watson RM, Cecil JE, Bale SJ, Compton JG,DiGiovanna JJ, Fleckman P, Lewis-Jones S, Arseculeratne G,Sergeant A, Munro CS, El HB, McElreavey K, Halkjaer LB,Bisgaard H, Mukhopadhyay S, McLean WH. Common loss-of-function variants of the epidermal barrier protein filaggrin are amajor predisposing factor for atopic dermatitis. Nat Genet2006;38:441–446.
28. Kharitonov SA, Barnes PJ. Nasal contribution to exhaled nitricoxide during exhalation against resistance or during breathholding. Thorax 1997;52:540–544.
29. Silkoff PE, McClean PA, Slutsky AS, Furlott HG, Hoffstein E,Wakita S, Chapman KR, Szalai JP, Zamel N. Marked flow-dependence of exhaled nitric oxide using a new technique toexclude nasal nitric oxide. Am J Respir Crit Care Med1997;155:260–267.
30. Franke A,McGovern DP, Barrett JC,Wang K, Radford-Smith GL,Ahmad T, Lees CW, Balschun T, Lee J, Roberts R, Anderson CA,Bis JC, Bumpstead S, Ellinghaus D, Festen EM,GeorgesM,GreenT, Haritunians T, Jostins L, Latiano A, Mathew CG, MontgomeryGW, Prescott NJ, Raychaudhuri S, Rotter JI, SchummP, SharmaY,Simms LA, Taylor KD, Whiteman D, Wijmenga C, BaldassanoRN, Barclay M, Bayless TM, Brand S, Buning C, Cohen A,Colombel JF, Cottone M, Stronati L, Denson T, De VM, D’Inca R,DubinskyM, Edwards C, Florin T, Franchimont D, Gearry R, GlasJ, Van GA, Guthery SL, Halfvarson J, Verspaget HW, Hugot JP,Karban A, Laukens D, Lawrance I, Lemann M, Levine A,Libioulle C, Louis E, Mowat C, Newman W, Panes J, Phillips A,Proctor DD, Regueiro M, Russell R, Rutgeerts P, Sanderson J,SansM, Seibold F, Steinhart AH, Stokkers PC, Torkvist L, Kullak-Ublick G, Wilson D, Walters T, Targan SR, Brant SR, Rioux JD,D’Amato M, Weersma RK, Kugathasan S, Griffiths AM, Mans-field JC, Vermeire S, Duerr RH, Silverberg MS, Satsangi J,Schreiber S, Cho JH, Annese V, Hakonarson H, Daly MJ, ParkesM. Genome-wide meta-analysis increases to 71 the number of
116 Chawes et al.
Pediatric Pulmonology

confirmed Crohn’s disease susceptibility loci. Nat Genet 2010;42:1118–1125.
31. Mells GF, Floyd JA,Morley KI, Cordell HJ, Franklin CS, Shin SY,Heneghan MA, Neuberger JM, Donaldson PT, Day DB, DuckerSJ, Muriithi AW, Wheater EF, Hammond CJ, Dawwas MF, JonesDE, Peltonen L, Alexander GJ, Sandford RN, Anderson CA.Genome-wide association study identifies 12 new susceptibilityloci for primary biliary cirrhosis. Nat Genet 2011;43:329–332.
32. LindstedtM, Lundberg K, Borrebaeck CA. Gene family clusteringidentifies functionally associated subsets of human in vivo bloodand tonsillar dendritic cells. J Immunol 2005;175:4839–4846.
33. de Jongste JC, Alving K. Gas analysis. Am J Respir Crit Care Med2000;162:S23–S27.
34. Jobsis Q, Schellekens SL, Kroesbergen A, Hop WC, de JongsteJC. Sampling of exhaled nitric oxide in children: end-expiratoryplateau, balloon and tidal breathing methods compared. EurRespir J 1999;13:1406–1410.
SUPPORTING INFORMATION
Additional supporting information may be found in theonline version of this article at the publisher’s web-site.
DENND1B Gene Variants and Neonatal FeNO 117
Pediatric Pulmonology

Asthma and lower airway disease
Neonatal bronchial hyperresponsiveness precedes acutesevere viral bronchiolitis in infants
Bo L. K. Chawes, MD, PhD,a* Porntiva Poorisrisak, MD, PhD,a* Sebastian L. Johnston, MD, PhD,b and
Hans Bisgaard, MD, DMSca Copenhagen and Gentofte, Denmark, and London, United Kingdom
Background: Respiratory syncytial virus and other respiratorytract viruses lead to common colds in most infants, whereas aminority develop acute severe bronchiolitis often requiringhospitalization. We hypothesized that such an excessiveresponse to respiratory tract viral infection is caused by hostfactors reflected in pre-existing increased bronchialresponsiveness.Objective: We sought to compare bronchial responsiveness andlung function in 1-month-old neonates who later develop acutesevere bronchiolitis with those who do not.Methods: We measured infant lung function (n 5 402) andbronchial responsiveness to methacholine (n 5 363) using theraised-volume rapid thoracoabdominal compression techniquebefore any respiratory symptoms in 1-month-old neonates fromthe Copenhagen Prospective Study of Asthma in Childhoodbirth cohort born to mothers with asthma. The children wereprospectively monitored for respiratory symptoms and given adiagnosis of acute severe bronchiolitis according to a fixedalgorithm.Results: Thirty-four (8.5%) infants had acute severebronchiolitis before 2 years of age, 21 (62%) were hospitalized,
and 23 (67%) of the cases were associated with respiratorysyncytial virus. Children who later had acute severebronchiolitis irrespective of viral species had a 2.5-foldincreased responsiveness to methacholine (provocative dose ofmethacholine producing a 15% decrease in transcutaneousoxygen pressure [PD15]) at age 1 month compared with controlsubjects (median PD15 in cases vs control subjects, 0.13 vs 0.33mmol; P 5 .01), whereas differences in baseline airflow were notsignificant for forced expiratory volume at 0.5 seconds (mean zscore for cases vs control subjects, 20.18 vs 20.01; P 5 .36) andforced expiratory flow at 50% of forced vital capacity (mean zscore for cases vs control subjects, 20.37 vs 20.09; P 5 .13).Conclusion: Bronchial hyperresponsiveness in at-risk neonatesprecedes acute severe bronchiolitis in response to infectionswith respiratory tract virus. (J Allergy Clin Immunol2012;130:354-61.)
Key words: Bronchial responsiveness, infants, lung function mea-surements, viral bronchiolitis
Children with acute severe bronchiolitis in relation to airwayvirus infections, such as respiratory syncytial virus (RSV) andrhinovirus, have an increased risk of asthma and allergy at schoolage.1-4 This has led to the suggestion of a causal role of RSVand rhinovirus on the risk of asthma.5,6 On the other hand, asthmaheredity and troublesome asthma-like symptoms in early infancyare significant risk factors for subsequent RSV-related hospitali-zation during infancy,7,8 suggesting that host factors might deter-mine a shared predisposition to viral bronchiolitis and childhoodasthma. We hypothesized that pre-existing abnormal infant spi-rometry and bronchial hyperresponsiveness in neonates precedeslater development of acute severe bronchiolitis.We recently demonstrated that neonatal pulmonary function
was associated with asthma by age 7 years in the CopenhagenProspective Studies on Asthma in Childhood (COPSAC2000).
9
The present study investigates whether neonatal pulmonary func-tion is also associated with acute severe bronchiolitis in infants(ie, whether neonatal lung function is a shared host factor forboth asthma and acute severe bronchiolitis).This study was nested in COPSAC2000, a prospective clinical
study of a birth cohort of 411 neonates born of mothers with ahistory of asthma.10 The study included measurements of infantspirometry and bronchial responsiveness to methacholine at1 month of age in 402 of the 411 cohort participants. Thedeep phenotyping with close clinical, single-center follow-upof the birth cohort by the COPSAC physicians allowed prospec-tive identification of infants who developed acute severebronchiolitis.
From aCopenhagen Prospective Studies on Asthma in Childhood, Health Sciences, Uni-versity of Copenhagen and Danish Pediatric Asthma Centre, Copenhagen UniversityHospital, Gentofte, and bthe National Heart & Lung Institute, MRC and Asthma UKCentre in Allergic Mechanisms of Asthma and Centre for Respiratory Infections, Im-perial College London.
*These authors contributed equally to this work.The Copenhagen Studies on Asthma in Childhood (COPSAC) is funded by private andpublic research funds listed on www.copsac.com. The Lundbeck Foundation, the Dan-ish Strategic Research Council, the Pharmacy Foundation of 1991, the AugustinusFoundation, the Danish Medical Research Council, and the Danish Pediatric AsthmaCentre provided the core support for the COPSAC research center. S.L.J. is supportedby a Chair from Asthma UK (CH11SJ), MRC Centre Grant G1000758, ERC FP7 Ad-vanced grant 233015, and Predicta FP7 Collaborative Project grant 260895.
Disclosure of potential conflict of interest: S. L. Johnston has consultant arrangementswith AstraZeneca, Centocor, Sanofi-Pasteur, Synairgen, GlaxoSmithKline, and Chiesiand has a share optionwith Synairgen.H. Bisgaard has consulted forMerck andChiesi;has received lecture fees from Merck; receives research support from the LundbeckFoundation, the Pharmacy Foundation of 1991, the Augustinus Foundation, the DanishMedical Research Council, and the Danish Pediatric Asthma Centre; and has providedlegal consultation or expert witness testimony for the European Medicines Agency(EMEA) on guidelines on pediatric studies for documenting asthma drugs. The rest ofthe authors declare that they have no relevant conflicts of interest.
Received for publication November 17, 2011; revised April 25, 2012; accepted for pub-lication April 26, 2012.
Available online June 17, 2012.Corresponding author: Hans Bisgaard, MD, DMSc, Copenhagen Prospective Studies onAsthma in Childhood, Health Sciences, University of Copenhagen and Danish Pediat-ric Asthma Centre, Copenhagen University Hospital, Gentofte, Ledreborg All!e 34,2820 Gentofte, Denmark. E-mail: [email protected].
0091-6749/$36.00! 2012 American Academy of Allergy, Asthma & Immunologydoi:10.1016/j.jaci.2012.04.045
354

METHODSStudy population
Four hundred eleven infants born at term of mothers with a history ofphysician-diagnosed asthma were enrolled at 1 month of age in theCOPSAC2000 prospective birth cohort study.11-13 Key exclusion criteriawere symptoms of lower airway infection or neonatal mechanical ventilationbefore inclusion, gestational age of less than 36 weeks, and any congenital ab-normality or systemic illness.
EthicsThe study was conducted in accordance with the guiding principles of the
Declaration of Helsinki and was approved by the local ethics committee ([KF]01-227/97) and the Danish Data Protection Agency (2008-41-1754). Bothparents provided written informed consent before enrollment.
Neonatal lung function measurementInfant spirometry was assessed during sedation with an oral dose of 90 mg/
kg chloral hydrate at age 1 month by applying the raised-volume rapidthoracoabdominal compression technique in agreement with the AmericanThoracic Society and European Respiratory Society standards.14 An inflatable‘‘squeeze’’ jacket waswrapped around the sedated infant’s chest and abdomen.Repeated ventilations to predefined mouth pressures ensured expansion oflung volume before an instant inflation of the jacket caused a full exhalationduring which the flow was measured by using a pneumotachograph with anair-cushion facemask.10,15
The software identified forced vital capacity (FVC) as the first plateau onthe volume-time curve; only measurements with an FVC appearing after 0.5seconds and with the forced expiratory volume at 0.5 seconds (FEV0.5) beingless than or equal to the FVCwere accepted. Three to 5 acceptable curves wereobtained at each measurement; the curve containing the median value ofFEV0.5 was used for the analyses of both volume (FEV0.5) and flow (forcedexpiratory flow at 50% of forced vital capacity [FEF50]) parameters.
Baseline lung function measurement was repeated after a saline inhala-tion. Subsequently, methacholine was administered in quadrupling dosesteps administered through a dosimeter attached to a nebulizer (SPIRA 08TSM 133; Respiratory Care Center, H€ameenlinna, Finland), as previouslydetailed.15 Bronchial responsiveness was assessed by means of repeatedmeasurements of infant spirometry and continuous assessment of transcuta-neous oxygen pressure (PtcO2; TCM3; Radiometer, Copenhagen, Denmark).The provocative dose of methacholine producing a 15% decrease in transcu-taneous oxygen pressure (PD15) was estimated from the dose-responsecurves fitted with a logistic function. Our previous sensitivity analysesshowed PtcO2 determined bronchial responsiveness with greater sensitivitythan any of the forced flow indices of infant spirometry15,16; thereforePtcO2 (PD15) was used to assess bronchial responsiveness in the presentanalyses.
Acute severe bronchiolitis casesThe birth cohort was prospectively monitored closely for respiratory
symptoms with daily diary cards from 1 month of age and clinical
examinations performed by the COPSAC physicians at the research clinicevery 6 months and in cases of acute respiratory symptoms. Acute severebronchiolitis was defined as an acute respiratory tract illness with onset beforethe age of 2 years based on symptoms of coryza progressing over a few days tocough, tachypnea, chest retractions, and auscultative widespread crepitationand/or rhonchi.17-19
In cases in which the infants had been brought directly to the localpediatric emergency department for admission, hospital records wereretrieved and carefully reviewed to verify respiratory symptoms compat-ible with the abovementioned criteria for diagnosing acute severebronchiolitis.
Viruses were detected by means of PCR analysis of nasopharyngealaspirate samples for RSV; rhinoviruses; influenza viruses AH1, AH3, and B;parainfluenza viruses 1 to 3; coronaviruses 229E and OC43; picornaviruses;bocavirus; adenoviruses; and human metapneumovirus, as previouslydetailed.20
Bronchiolitis occurring before age 2 years irrespective of the viral trigger(ie, any bronchiolitis) was used as the primary end point, excludingchildren with acute asthma-like exacerbations. Secondary end points were(1) RSV-induced bronchiolitis, (2) non–RSV-induced bronchiolitis, (3) acuteasthma-like exacerbations, (4) bronchiolitis before age 1 year, and (5) anybronchiolitis, including acute asthma-like exacerbations.
Atopic comorbidityRecurrent episodes of troublesome lung symptoms were defined as 3
consecutive days recorded with significant cough and/or wheeze and/ordyspnea.21 The number of episodes of troublesome lung symptoms before de-velopment of acute severe bronchiolitis among cases was compared with thenumber of episodes in the control group occurring before the median age atdiagnosis of acute severe bronchiolitis in the cases.
Allergic sensitization was determined at age 18 months by means ofmeasurement of serum specific IgE levels against 15 common inhalant andfood allergens (cat, dog, horse, birch, timothy grass, mugwort, house dustmite, molds [Penicillium notatum,Cladosporium herbarum, Aspergillus fumi-gatus, and Alternaria tenuis], hen’s egg, cow’s milk, cod, wheat, peanut, soy-bean, or shrimp) using the ImmunoCAP assay (Pharmacia Diagnostics AB,Uppsala, Sweden). Sensitization was defined as a specific IgE level of 0.35kU/L or greater22,23 for any of the tested allergens and was analyzed as a di-chotomized measurement.
Total IgE levels were measured at age 18 months by using ImmunoCAP(Pharmacia Diagnostics AB), with a detection limit of 2 kU/L.22
Blood eosinophil counts (109 cells per liter) were assessed at age 18months.
Eczema was diagnosed by using the Hanifin-Rajka criteria, as previouslydetailed.24 Skin lesions were described at both scheduled and acute visits ac-cording to predefined morphology and localization.
GeneticsThe study population was genotyped for filaggrin-null mutations and
ORMDL3 and DENND1B variants, as described in detail in the Methods sec-tion in this article’s Online Repository at www.jacionline.org.
Statistical analysisLung function data (FEV0.5, FEF50, and PD15 [PtcO2]) were adjusted for
lifespan and birth length by using a generalized linear model, as previously de-tailed.16 Lifespan at examination date was calculated as the sum of estimatedgestational age inweeks at birth andweeks since birth. The lung functionmea-surements were log transformed before analysis to obtain normal distributionof data.
Generalized linear models were used to compare lung function data insubjects with and without acute severe bronchiolitis, assuming Gaussiandistribution of the data and using the identity link function as in multipleregression analyses. Adjustment for significant and borderline-significant
Abbreviations usedCOPSAC: Copenhagen Prospective Studies on Asthma in Childhood
FEF50: Forced expiratory flow at 50% of forced vital capacityFEV0.5: Forced expiratory volume at 0.5 secondsFVC: Forced vital capacityIQR: Interquartile rangePD15: Provocative dose of methacholine producing a 15% de-
crease in transcutaneous oxygen pressurePtcO2: Transcutaneous oxygen pressureRSV: Respiratory syncytial virus
J ALLERGY CLIN IMMUNOL
VOLUME 130, NUMBER 2
CHAWES ET AL 355

baseline characteristics and intermediary atopic markers was done by addingthe variables as covariates in the model.
The comparison of baseline characteristics and the development of atopicstigmata in cases versus control subjects were done by using univariateanalyses (ie, t tests and x2 tests). The number of episodes of troublesome lung
symptoms in cases versus control subjects was analyzed by using Poissonregression.
Analyses were done with SAS version 9.1 software for Windows (SASInstitute, Inc, Cary, NC). A P value of .05 or less was consideredsignificant.
TABLE I. Baseline characteristics of the study group
Control subjects(n 5 366)
Primary end point Secondary end points P value
Bronchiolitiscases*(n 5 34)
RSV-inducedbronchiolitiscases (n 5 23)
Non–RSV-inducedbronchiolitiscasesy (n 5 9)
Asthma-likecases (n 5 11)
Bronchiolitiscases vs
control subjects
Baseline characteristicsSex
Male (no.) 64.7% (22) 48.4% (177) — — — .07{Anthropometrics
BMI at birth (cm/kg2), median(IQR)
12.5 (11.6-13.7) 12.8 (12.0-13.7) — — — .25#
EnvironmentSmoking, 3rd trimester (no.) 35.3% (12) 13.1% (48) — — — .005{Alcohol, 3rd trimester (no.) 14.7% (5) 18.6% (68) — — — .58{Cat at birth (no.) 17.7% (6) 14.8% (52) — — — .65{Dog at birth (no.) 14.7% (5) 13.6% (48) — — — .86{Older siblings at birth (no.) 52.9% (18) 42.4% (155) — — — .23{Household income at birth (no.) .50!!Low, <53,000V 30.3% (10) 29.6% (101) — — —Medium, 53,000V-80,000V 54.6% (18) 46.6% (159) — — —High, >80,000V 15.2% (5) 23.8% (81) — — —Paternal history of asthma (no.) 24.2% (8) 16.5% (59) — — — .26{Age at start of day care (d),median (IQR)
296 (230-349) 341 (240-417) — — — .08#
Solely breast-fed (d), median(IQR)
120 (72-179) 122 (89-155) — — — .47#
Lung function at age 1 moFEV0.5 (z score), mean (SD) 20.18 (0.91) 20.01 (0.99) — — — .36#FEF50 (z score), mean (SD) 20.37 (1.05) 20.09 (1.00) — — — .13#PD15 (PtcO2 [mmol]), median(IQR)
0.13 (0.07-0.60) 0.33 (0.12-0.88) — — — .01#
GeneticsFilaggrin mutation 18.2% (6) 9.7% (34) — — — .13{ORMDL3 (TT) 48.5% (16) 26.7% (92) — — — .008{DENND1B genotype(rs2786098)
— — — .17**
AA 3.5% (1) 4.2% (14) — — —AB 13.8% (4) 27.5% (91) — — —BB 82.7% (24) 68.3% (226) — — —
Atopic intermediary markersAllergic sensitization!(18 mo [no.])
9.1% (3) 12.0% (38) 0% (0) 22.2% (2) 20.0% (2) .78""
Blood eosinophil count (18 mo[109/L]), median (IQR)
0.27 (0.18-0.43) 0.21 (0.13-0.32) 0.26 (0.18-0.43) 0.21 (0.15-0.38) 0.41 (0.22-0.48) .03#
Total IgE (18 mo [kU/L]),median (IQR)
15.3 (6.3-29.5) 8.2 (3.9-17.1) 15.5 (6.3-28.0) 10.2 (4.7-30.2) 7.0 (5.2-30.9) .03#
Episodes of troublesome lungsymptoms,§ median (IQR)
2 (1-6) 1 (1-2) 1 (1-5) 6 (3-7) 2 (1-4) .0005§§
Eczema (0-2 y [no.]) 38.2% (13) 38.4% (131) 30.4% (7) 66.7% (6) 40.0% (4) .98{Episode characteristics
Fever at diagnosisk (no.) — 59% (20) 57% (13) 56% (5) 36% (4) —Auscultation
Crepitations (no.) — 41% (14) 44% (10) 33% (3) 27% (3) —Rhonchi (no.) — 85% (29) 78% (18) 100% (9) 91% (10) —Hospitalization (no.) — 62% (21) 83% (19) 22% (2) 36% (4) —Days hospitalized, median(range)
— 3 (1-15) 4 (1-15) 2 (2-2) 2 (1-4) —
(Continued)
J ALLERGY CLIN IMMUNOL
AUGUST 2012
356 CHAWES ET AL

RESULTSStudy group selection
Infant spirometry was completed in 402 children, and bronchialresponsiveness to methacholine was assessed in 363 of the 411children in the cohort at age 1 month before the development ofany respiratory symptoms.Eleven children had an episode of acute asthma-like symptoms
not fulfilling all the diagnostic criteria for acute severe bronchi-olitis. These children were excluded because of a lack of objectivesigns of respiratory distress, such as tachypnea, chest retractions,or both (see Table I and Table E1 in this article’s Online Reposi-tory at www.jacionline.org for baseline characteristics of the ex-cluded children). These 11 children were excluded from both thecase and control groups, leaving 400 evaluable children (see FigE1 in this article’s Online Repository at www.jacionline.org forthe study group flow chart).
Bronchiolitis casesThirty-four (8.5%) of the 400 children in the selected cohort
had acute severe bronchiolitis before age 2 years (median age atdiagnosis, 327 days; interquartile range [IQR], 128-446 days). Ofthese 34 cases, 65% (n5 22) were boys, 59% (n5 20) had feverat the time of diagnosis (rectal temperature, >38.08C), 41%(n 5 14) had crepitations, and 85% (n 5 29) had rhonchi atauscultation. Median time from infant spirometry to diagnosis ofacute severe bronchiolitis was 267 days (range, 8-617 days). In 2of the 34 bronchiolitis cases, there were no available nasopha-ryngeal aspirates. RSVwas identified in 23 of the 32 bronchiolitiscases, whereas the remaining 9 cases were classified as havingnon–RSV-induced bronchiolitis (2 with picornavirus; 1 withbocavirus; 1 with rhinovirus; 1 with bocavirus and rhinovirus;1 with human metapneumovirus, picornavirus, influenza virus,parainfluenza virus, coronavirus, and bocavirus; and 3 withnegative nasopharyngeal suctions).
Hospitalization was required for 21 (62%) of the 34 bronchi-olitis cases, with a median duration of hospitalization of 10 days(IQR, 6-21 days). Half of the admitted children needed treatmentwith nasal continuous positive airway pressure, one third wereprescribed systemic corticosteroid treatment, and 90% receivednebulized b2-agonist. Children with acute severe bronchiolitiswho were not hospitalized received outpatient treatment with in-haled b2-agonists (92%), inhaled corticosteroids (62%), systemiccorticosteroids (31%), and antibiotics (77%).
Baseline characteristics of children with acutesevere bronchiolitis versus control subjects
Comparison of baseline characteristics of the bronchiolitiscases (n5 34) and control subjects (n5 366, Table I) showed thatmaternal smoking during the third trimester of pregnancywas sig-nificantly more common among infants with acute severe bron-chiolitis compared with control subjects (35% vs 13%,P 5 .005). The ORMDL3 TT genotype was also significantly as-sociated with the development of acute severe bronchiolitis dur-ing the first 2 years of life (cases vs control subjects, 49% vs27%; P 5 .008), whereas male sex (cases vs control subjects,65% vs 49%; P5 .07) and young age at the start of day care (me-dian age at start for cases vs control subjects, 296 vs 341 days;P5 .08) were borderline significant. We found no association be-tween cases and control subjects with respect to anthropometrics;maternal alcohol consumption during the third trimester of preg-nancy; the presence of a cat, a dog, or an older sibling in the homeat birth; household income; length of sole breast-feeding; paternalhistory of asthma; filaggrin-null mutations; and DENND1B ge-netic variants (Table I).Children with acute severe bronchiolitis had significantly
(P5 .0005) more episodes of troublesome lung symptoms beforebronchiolitis diagnosis (median, 2; IQR, 1-6) compared with con-trol subjects before the median age at bronchiolitis diagnosis
TABLE I. (Continued)
Control subjects(n 5 366)
Primary end point Secondary end points P value
Bronchiolitiscases*(n 5 34)
RSV-inducedbronchiolitiscases (n 5 23)
Non–RSV-inducedbronchiolitiscasesy (n 5 9)
Asthma-likecases (n 5 11)
Bronchiolitiscases vs
control subjects
Treatment — —Inhaled b2-agonist (no.) — 91% (31) 87% (20) 100% (9) 100% (11) —Inhaled corticosteroid (no.) — 47% (16) 48% (11) 44% (4) 81% (9) —Oral corticosteroid (no.) — 24% (8) 13% (3) 56% (5) 36% (4) —Intravenous corticosteroid (no.) — 9% (3) 13% (3) 0 10% (1) —Nasal CPAP (no.) — 9% (3) 13% (3) 0 0 —Antibiotics (no.) — 62% (21) 61% (14) 67% (6) 18% (2) —
Age at diagnosis (d), median(IQR)
— 327 (128-446) 199 (88-359) 462 (430-551) 383 (324-576) —
Time from lung function todiagnosis (d), median (range)
— 267 (8-617) 160 (8-500) 425 (91-617) 349 (191-677) —
Statistical tests: {x2 test; #t test; **log-additive model; !!Fisher exact test; ""1-way ANOVA; and §§Poisson regressionCPAP, Continuous positive airway pressure.*Two bronchiolitis cases are without available nasopharyngeal suction.!Two cases with picornavirus; 1 case with bocavirus; 1 case with rhinovirus; 1 case with bocavirus and rhinovirus; 1 case with human metapneumovirus, picornavirus, influenzavirus, parainfluenza virus, coronavirus, and bocavirus; and 3 cases with negative nasopharyngeal suctions."Any allergic sensitization (specific IgE >0.35 kU/L) against 15 common inhalant and food allergens (cat, dog, horse, birch, timothy grass, mugwort, house dust mite, molds, hen’segg, cow’s milk, fish, wheat, peanut, soybean, or shrimp).§Comparison of number of episodes in cases before development of acute bronchiolitis with number of episodes in control subjects occurring before median age at diagnosis ofacute bronchiolitis (327 days) in the cases.kRectal temperature >_38.08C.
J ALLERGY CLIN IMMUNOL
VOLUME 130, NUMBER 2
CHAWES ET AL 357

among the cases (median, 1; IQR, 0-2). Blood eosinophil countsand total IgE levels at age 18 months were significantly higher incases versus control subjects (blood eosinophil count: median,0.27 3 109 cells/L [IQR, 0.18-0.43 3 109 cells/L] vs0.213 109 cells/L [IQR, 0.13-0.323 109 cells/L], P5 .03; totalIgE level: median, 15.3 kU/L [IQR, 6.3-29.5 kU/L] vs 8.2 kU/L[IQR, 3.9-17.1 kU/L], P5 .03). Eczema and allergic sensitizationwere equally distributed among cases and control subjects.Children with RSV-induced bronchiolitis compared with those
with non–RSV-induced bronchiolitis were younger at diagnosis(199 vs 462 days, P < .01) and were more often admitted to thehospital (83% vs 22%, P < .01). There were no significant differ-ences in the development of atopic stigmata during the first 2years of life between cases with RSV-induced bronchiolitis andthose with non–RSV-induced bronchiolitis (all P > .05).A detailed description of the 34 bronchiolitis cases and the
control group is outlined in Table I.
Neonatal lung function in bronchiolitis cases versuscontrol subjects
Distributions of PD15 (PtcO2), FEV0.5, and FEF50 measured atage 1 month before any respiratory symptoms in children whosubsequently had acute severe bronchiolitis versus control sub-jects are shown in Fig 1. Children with acute severe bronchiolitisreacted to lower doses of methacholine compared with the controlgroup (median PD15 [PtcO2] dose in cases vs control subjects,0.13 vs 0.33mmol;P5.01; Fig 1,A). This phenomenon remainedsignificant (P 5 .02) after adjustment for significant andborderline-significant baseline characteristics, including atopicintermediary markers (sex, maternal smoking during the third tri-mester, age at the start of day care, ORMDL3 genotype, episodesof troublesome lung symptoms, and total IgE levels and blood eo-sinophil counts). Increased bronchial responsiveness to metha-choline in cases versus control subjects was confirmed in asensitivity analysis, including the excluded cases of acuteasthma-like symptoms not fulfilling all the diagnostic criteriafor acute bronchiolitis (P 5 .01). The distribution of FEV0.5 andFEF50 in Fig 1, B and C, suggested lower airflows in infantswith acute severe bronchiolitis compared with control subjects,but these trends were not significant (mean z score for FEV0.5 incases vs control subjects,20.18 vs20.01 [P5 .36]; mean z scorefor FEF50 in cases vs control subjects,20.37 vs20.09 [P5 .13]).
Subgroup analysis of PD15 (PtcO2) in cases with RSV-inducedbronchiolitis and those with non–RSV-induced bronchiolitis ex-cluding cases with acute asthma-like exacerbations and bronchi-olitis occurring before age 1 year suggested pre-existinghyperresponsive airways independent of these case definitions, al-though the statistical power was lost in some of these small
FIG 1. z Scores of neonatal bronchial responsiveness to methacholine (A),baseline FEV0.5 (B), and baseline FEF50 (C) in children with acute severebronchiolitis in the first 2 years of life compared with children who do nothave acute severe bronchiolitis.
TABLE II. Comparisonof lung functionat age1month in childrenwho laterhaveacute severebronchiolitis versushealthycontrol subjects
Control subjects (n 5 366) vs:Acute severe bronchiolitis
(n 5 34)
Lung function, age 1 mo Mean difference (95% CI) P value Adjusted mean difference* (95% CI) P value
FEV0.5 (z score) 20.17 (20.52 to 0.19) .36 20.12 (20.55 to 0.31) .59FEF50 (z score) 20.28 (20.65 to 0.08) .13 20.33 (20.76 to 0.10) .14logPD15 (PtcO2 [mmol]) 20.69 (21.24 to 20.15) .01 20.79 (21.44 to 20.13) .02
*Adjusted for sex, mother’s smoking during the third trimester of pregnancy (yes/no), age at start of day care, ORMDL3 genotype, blood eosinophil count and total IgE level at age18 months, and episodes of troublesome lung symptoms before diagnosis.
J ALLERGY CLIN IMMUNOL
AUGUST 2012
358 CHAWES ET AL

subgroups, including the specific RSV-induced bronchiolitis sub-group (P5 .12). Subgroup analyses of baseline FEV0.5 and FEF50values suggested similar trends of impaired neonatal airflow re-lated to the subsequent development of acute severe bronchiolitis(see Table II).
DISCUSSIONPrincipal findings
Neonatal bronchial hyperresponsiveness increases the riskof acute severe bronchiolitis in early life in the COPSAC2000
at-risk birth cohort. This demonstrates that neonatal airway hy-perresponsiveness is a pre-existing host factor common to laterdevelopment of both acute severe viral bronchiolitis and child-hood asthma.9
Strengths and limitations of the studyThis is the first assessment of premorbid neonatal lung
function and bronchial responsiveness in a birth cohort ofhealthy at-risk neonates combined with a close prospectiveclinical follow-up for subsequent development of acute severebronchiolitis.The risk of misclassification of the clinical end point of
acute severe bronchiolitis was minimized in this prospectivebirth cohort with close clinical monitoring, including dailydiary card recordings of respiratory symptoms, 6-month visitsto the clinic for clinical assessments by pediatricians, and visitsto the clinic at the time of acute respiratory symptoms. Theclinical research unit was acting as the primary health careresource for the cohort in relation to all respiratory symptoms,ensuring that diagnosis and treatment followed a predefinedalgorithm, including a standard clinical definition of acutesevere bronchiolitis.In particular, our clinical definition of acute severe bronchiol-
itis was based on objective assessment of tachypnea, chestretractions, and auscultative wide-spread fine crepitation and/orexpiratory rhonchi17-19 and not solely based on parental reporting.This approach enabled us to exclude cases of acute severe asthma-like exacerbations from the study group, which is importantbecause impaired pulmonary function early in life has been de-scribed in association with subsequent recurrent asthma-likesymptoms,25-29 and asthma.9 This selection process is essentialbecause the inclusion of children with acute severe asthma-likeexacerbations in the acute severe bronchiolitis group could havedriven our findings. Still, sensitivity analyses, including suchasthma-like exacerbations, provide similar conclusions, suggest-ing that the clinical distinction between acute bronchiolitis andacute asthma symptoms is arbitrary and the underlying patho-physiology is similar.
Bronchiolitis is difficult to differentiate from asthma-likesymptoms, and indeed, we suspect it to be the same entity.However, the literature suggests that these subtle clinical differ-ences represent different phenotypes. This is precisely the issuewe are questioning in our study. We choose a conservativedefinition of acute bronchiolitis using a strict predefined algo-rithm, including objective signs of respiratory distress, which is inline with recently published reviews.17-19
RSV-induced bronchiolitis has been associated with asthmalater in life, but it was our research hypothesis that bronchialhyperresponsiveness is the common cause of both bronchiolitisand asthma symptoms independently of viral species. In line withthis, it has been reported that also rhinovirus-induced bronchiol-itis increases the risk of asthma later in life.1,2 Children with RSVin our study were younger than the non-RSV cases but showedno differences in atopic stigmata. Furthermore, adjusting the anal-yses for atopic intermediary end points did not alter theassociations.In reverence to the long tradition of emphasizing the unique
quality of RSV, we analyzed a number of secondary bronchiolitisend points: (1) RSV-induced bronchiolitis, (2) non–RSV-inducedbronchiolitis, (3) acute asthma-like exacerbations, (4) bronchiol-itis before age 1 year, and (5) any bronchiolitis, including acuteasthma-like exacerbations. All these secondary analyses showsimilar patterns of pre-existing increased reactivity to methacho-line in cases versus control subjects. Some of these subgroupanalyses (eg, the RSV group) did not reach statistical significance,probably because of the lack of power from dividing the mainstudy group into smaller subgroups. The similarities of increasedbronchial responsiveness in all groups of infants presenting withsymptoms of acute severe airway obstruction independently oftrigger or age at onset suggest a common deficiency rather thanparticular trigger attributes. It is our interpretation that bronchialhyperresponsiveness is the common underlying phenotypic traitin infants presenting with acute severe airway obstruction inresponse to viral infections.It is our clinical practice only to admit infants if they need
support with feeding tubes; nasal continuous positive airwaypressure; suction of the upper airways; nebulized inhalations,such as isotonic saline; or b2-agonist or systemic steroids, de-pending on symptom severity. We are aware of the poor evidenceof this, but presumably, our clinical tradition builds from a con-cern over the ‘‘bronchiolitis phenotype’’ might indeed be an asth-matic reaction in which such treatment might be meaningful andin which no alternatives exist.It is a significant strength of this study that lung function was
assessed within a narrow age range around 1 month after birthbased on results of infant spirometry with the state-of-the-artraised-volume rapid thoracoabdominal compression technique inagreement with recognized international guidelines.14 This is the
RSV-induced bronchiolitis (n 5 23)Non–RSV-induced bronchiolitis
(n 5 9) Asthma-like cases (n 5 11) Bronchiolitis cases <1 y (n 5 20)
Mean difference (95% CI) P value Mean difference (95% CI) P value Mean difference (95% CI) P value Mean difference (95% CI) P value
20.10 (20.52 to 0.33) .66 20.31 (21.01 to 0.38) .37 20.15 (20.75 to 0.45) .62 0.02 (20.46 to 0.52) .9220.12 (20.56 to 0.31) .58 20.71 (21.42 to 20.01) .05 20.28 (20.91 to 0.35) .39 20.19 (20.67 to 0.29) .4320.42 (21.06 to 0.13) .12 21.37 (22.38 to 20.35) .01 20.76 (21.82 to 0.30) .16 20.98 (21.71 to 20.24) .01
TABLE II. (Continued)
J ALLERGY CLIN IMMUNOL
VOLUME 130, NUMBER 2
CHAWES ET AL 359

largest published sample of lung function assessments in neonatesperformed under standardized conditions comprising measure-ments in 402 asymptomatic infants.The relatively rare prevalence of acute severe bronchiolitis is a
limitation of the study. Interestingly, we did not find significantlylower airflow in the infants later having bronchiolitis symptoms.This might suggest that bronchial responsiveness is the primarypathology, leading to acute obstruction in response to virus later inlife, and that airflow limitation might not be the primary pathol-ogy. Alternatively, we might be unable to see differences inbaseline airflow because of the low number of cases, whichhampers the statistical power.The high-risk nature of the birth cohort might diminish the
generalizability of our findings because the absolute levels oflung function and bronchial responsiveness might not berepresentative of the general population, although this wouldnot affect the comparison of lung function within the cohort.A recent study of preterm infants reported that palivizumabprophylaxis significantly reduced the risk of recurrent wheeze inchildren without atopic predisposition, whereas there was noeffect in children with an atopic family history,30 suggesting adifferential effect of viral infection depending on atopic predis-position. Therefore our findings cannot be extrapolated beyonda high-risk population.
InterpretationThe significant association between bronchial hyperrespon-
siveness at 1 month of age in at-risk children and the laterdevelopment of acute severe bronchiolitis demonstrates a pre-existing propensity for an exaggerated airway response to com-mon respiratory tract viral infections.An older study reported trends of reduced airflow but no
increase in the bronchial responsiveness to histamine in infantssubsequently having bronchiolitis (n 5 17) compared withcontrol subjects (n 5 236). This study was limited from the useof infant spirometry, which was not volume anchored, testing theinfants at a wider age range up to 10 weeks, and from aretrospective questionnaire–defined end point of ‘‘doctor-diag-nosed bronchiolitis’’ recalled by the parents at follow-up by 2years of age.31
The association between airway hyperresponsiveness and thesubsequent development of acute severe bronchiolitis demon-strated in this study and our recent observation of an increasedrisk of asthma at age 7 years in children with neonatal bronchialhyperresponsiveness,9 together with observational evidence ofan association between acute severe bronchiolitis early in lifeand the development of asthma,1-4 suggests neonatal bronchialhyperresponsiveness as a shared host factor for bronchiolitisand asthma rather than a causal effect of bronchiolitis on asthmadevelopment.Notably, the incidence of acute severe bronchiolitis in our study
(8.5%) was higher than reported in some studies (1-3%)32-35 butcomparable with the incidence of 7% reported in a cohort of253 infants with a high prevalence (71%) of atopic predisposi-tion.31 This association between asthma predisposition and in-creased incidence of acute bronchiolitis in the infants supportsour research hypothesis that a host factor is responsible for acutebronchiolitis.Children with acute severe bronchiolitis had a high prevalence
of early troublesome lung symptoms before bronchiolitis, had
increased total IgE levels and blood eosinophil counts, were moreoften exposed to tobacco smoke in utero, were of the male sex,were carrying the ORMDL3 risk variant, and started day care atan early age compared with children not having such acute severebronchiolitis. We previously demonstrated the ORMDL3 risk al-lele is associated with neonatal increased bronchial reactivityand increased risk of asthma in early childhood in our cohort.36
Together these characteristics are all typical of children at riskof asthma, supporting that children with acute severe bronchiolitishave a premorbid constitution, including bronchial hyperrespon-siveness, which predisposes them to both an exaggerated responseto respiratory tract viral infection and later development ofasthma.Therefore it might be speculated that acute severe bronchiolitis
during infancy is not a specific disease entity but simply a severeearly debut of asthma persisting to school age.3,4
ConclusionBronchial hyperresponsiveness in asymptomatic at-risk
neonates precedes the later development of acute severe bron-chiolitis, suggesting a pre-existing common propensity of theairways to develop asthma and to react adversely to commonrespiratory tract viruses.
We express our gratitude to the children and families of the COPSAC cohortstudy for all their support and commitment. We acknowledge and appreciatethe unique efforts of the COPSAC research team. We thank S. Jensen forstatistical support.
Key messages
d RSV and other respiratory tract viruses lead to commoncolds in most infants, whereas a minority have acute se-vere bronchiolitis.
d Bronchial hyperresponsiveness in at-risk neonates pre-cedes acute severe bronchiolitis in response to respiratorytract viral infections.
REFERENCES1. Jackson DJ, Gangnon RE, Evans MD, Roberg KA, Anderson EL, Pappas TE, et al.
Wheezing rhinovirus illnesses in early life predict asthma development in high-riskchildren. Am J Respir Crit Care Med 2008;178:667-72.
2. Lemanske RF Jr, Jackson DJ, Gangnon RE, Evans MD, Li Z, Shult PA, et al. Rhi-novirus illnesses during infancy predict subsequent childhood wheezing. J AllergyClin Immunol 2005;116:571-7.
3. Sigurs N, Gustafsson PM, Bjarnason R, Lundberg F, Schmidt S, Sigurbergsson F,et al. Severe respiratory syncytial virus bronchiolitis in infancy and asthma and al-lergy at age 13. Am J Respir Crit Care Med 2005;171:137-41.
4. Stein RT, Sherrill D, Morgan WJ, Holberg CJ, Halonen M, Taussig LM, et al. Res-piratory syncytial virus in early life and risk of wheeze and allergy by age 13 years.Lancet 1999;354:541-5.
5. Kuehni CE, Spycher BD, Silverman M. Causal links between RSV infection andasthma: no clear answers to an old question. Am J Respir Crit Care Med 2009;179:1079-80.
6. Singh AM, Moore PE, Gern JE, Lemanske RF Jr, Hartert TV. Bronchiolitis toasthma: a review and call for studies of gene-virus interactions in asthma causa-tion. Am J Respir Crit Care Med 2007;175:108-19.
7. Goetghebuer T, Kwiatkowski D, Thomson A, Hull J. Familial susceptibility to se-vere respiratory infection in early life. Pediatr Pulmonol 2004;38:321-8.
8. Stensballe LG, Kristensen K, Simoes EA, Jensen H, Nielsen J, Benn CS, et al.Atopic disposition, wheezing, and subsequent respiratory syncytial virus hospital-ization in Danish children younger than 18 months: a nested case-control study. Pe-diatrics 2006;118:e1360-8.
9. Bisgaard H, Jensen SM, Bonnelykke K. Interaction between asthma and lungfunction growth in early life. Am J Respir Crit CareMed 2012 [Epub ahead of print].
J ALLERGY CLIN IMMUNOL
AUGUST 2012
360 CHAWES ET AL

10. Loland L, Bisgaard H. Feasibility of repetitive lung function measurements byraised volume rapid thoracoabdominal compression during methacholine challengein young infants. Chest 2008;133:115-22.
11. Bisgaard H. The Copenhagen Prospective Study on Asthma in Childhood (COP-SAC): design, rationale, and baseline data from a longitudinal birth cohort study.Ann Allergy Asthma Immunol 2004;93:381-9.
12. Bisgaard H, Hermansen MN, Loland L, Halkjaer LB, Buchvald F. Intermittent in-haled corticosteroids in infants with episodic wheezing. N Engl J Med 2006;354:1998-2005.
13. Bisgaard H, Hermansen MN, Buchvald F, Loland L, Halkjaer LB, Bønnelykke K,et al. Childhood asthma after bacterial colonization of the airway in neonates. NEngl J Med 2007;357:1487-95.
14. ATS/ERS statement: raised volume forced expirations in infants: guidelines forcurrent practice. Am J Respir Crit Care Med 2005;172:1463-71.
15. Loland L, Buchvald FF, Halkjaer LB, Anhøj J, Hall GL, Persson T, et al. Sensitiv-ity of bronchial responsiveness measurements in young infants. Chest 2006;129:669-75.
16. Bisgaard H, Loland L, Holst KK, Pipper CB. Prenatal determinants of neonatallung function in high-risk newborns. J Allergy Clin Immunol 2009;123:651-7.
17. Bush A, Thomson AH. Acute bronchiolitis. BMJ 2007;335:1037-41.18. Diagnosis and management of bronchiolitis. Pediatrics 2006;118:1774-93.19. Smyth RL, Openshaw PJ. Bronchiolitis. Lancet 2006;368:312-22.20. Bisgaard H, Hermansen MN, Bonnelykke K, Stockholm J, Baty F, Skytt NL, et al.
Association of bacteria and viruses with wheezy episodes in young children: pro-spective birth cohort study. BMJ 2010;341:c4978.
21. Bisgaard H, Pipper CB, Bonnelykke K. Endotyping early childhood asthma byquantitative symptom assessment. J Allergy Clin Immunol 2011;127:1155-64.e2.
22. Ballardini N, Nilsson C, Nilsson M, Lilja G. ImmunoCAP Phadiatop Infant—anew blood test for detecting IgE sensitisation in children at 2 years of age. Allergy2006;61:337-43.
23. Wickman M, Ahlstedt S, Lilja G, van Hage HM. Quantification of IgE antibodiessimplifies the classification of allergic diseases in 4-year-old children. A reportfrom the prospective birth cohort study—BAMSE. Pediatr Allergy Immunol2003;14:441-7.
24. Halkjaer LB, Loland L, Buchvald FF, Agner T, Skov L, Strand M, et al. Develop-ment of atopic dermatitis during the first 3 years of life: the Copenhagen prospec-tive study on asthma in childhood cohort study in high-risk children. ArchDermatol 2006;142:561-6.
25. Haland G, Carlsen KC, Sandvik L, Devulapalli CS, Munthe-Kaas MC, PettersenM, et al. Reduced lung function at birth and the risk of asthma at 10 years ofage. N Engl J Med 2006;355:1682-9.
26. Martinez FD, Morgan WJ, Wright AL, Holberg CJ, Taussig LM. Diminished lungfunction as a predisposing factor for wheezing respiratory illness in infants. N EnglJ Med 1988;319:1112-7.
27. Murray CS, Pipis SD, McArdle EC, Lowe LA, Custovic A, Woodcock A. Lungfunction at one month of age as a risk factor for infant respiratory symptoms ina high risk population. Thorax 2002;57:388-92.
28. Tager IB, Hanrahan JP, Tosteson TD, Castile RG, Brown RW, Weiss ST, et al. Lungfunction, pre- and post-natal smoke exposure, and wheezing in the first year of life.Am Rev Respir Dis 1993;147:811-7.
29. Young S, Arnott J, O’Keeffe PT, Le Souef PN, Landau LI. The association betweenearly life lung function and wheezing during the first 2 yrs of life. Eur Respir J2000;15:151-7.
30. Simoes EA, Carbonell-Estrany X, Rieger CH, Mitchell I, Fredrick L, Groothuis JR.The effect of respiratory syncytial virus on subsequent recurrent wheezing in atopicand nonatopic children. J Allergy Clin Immunol 2010;126:256-62.
31. Young S, O’Keeffe PT, Arnott J, Landau LI. Lung function, airway responsiveness,and respiratory symptoms before and after bronchiolitis. Arch Dis Child 1995;72:16-24.
32. Fjaerli HO, Farstad T, Bratlid D. Hospitalisations for respiratory syncytial virusbronchiolitis in Akershus, Norway, 1993-2000: a population-based retrospectivestudy. BMC Pediatr 2004;4:25.
33. Muller-Pebody B, Edmunds WJ, Zambon MC, Gay NJ, Crowcroft NS. Con-tribution of RSV to bronchiolitis and pneumonia-associated hospitalizationsin English children, April 1995-March 1998. Epidemiol Infect 2002;129:99-106.
34. Nielsen HE, Siersma V, Andersen S, Gahrn-Hansen B, Mordhorst CH, Nørgaard-Pedersen B, et al. Respiratory syncytial virus infection—risk factors for hospitaladmission: a case-control study. Acta Paediatr 2003;92:1314-21.
35. Shay DK, Holman RC, Newman RD, Liu LL, Stout JW, Anderson LJ. Bronchiol-itis-associated hospitalizations among US children, 1980-1996. JAMA 1999;282:1440-6.
36. Bisgaard H, Bønnelykke K, Sleiman PM, Brasholt M, Chawes B, Kreiner-MøllerE, et al. Chromosome 17q21 gene variants are associated with asthma and exacer-bations but not atopy in early childhood. Am J Respir Crit Care Med 2009;179:179-85.
J ALLERGY CLIN IMMUNOL
VOLUME 130, NUMBER 2
CHAWES ET AL 361

METHODSBronchial responsiveness
Baseline lung function was repeated after a saline inhalation. Subse-quently, methacholine was administered in quadrupling dose steps admin-istered through a dosimeter attached to a nebulizer (SPIRA 08 TSM 133,Respiratory Care Center), as previously detailed.E1 Bronchial responsivenesswas assessed by using repeated measurements of infant spirometry and con-tinuous assessment of PtcO2 (TCM3, Radiometer). The PD15 was estimatedfrom the dose-response curves fitted with a logistic function. Our previoussensitivity analyses showed PtcO2 to be more sensitive than any of theforced flow indices of infant spirometry.E1,E2 Therefore PtcO2 was used inthe analyses.
GeneticsBlood was sampled at age 6 months, centrifuged and separated into serum
and serum cells, and immediately stored at 2808C until analysis. Afterthawing, DNAwas purified from the serum cells by using the QIAamp DNABlood Maxi Kit (Qiagen, Valencia, Calif).E3
Filaggrin genotyping for the 2 common independent null mutationsR501X and 2282del4 was performed, as previously described.E4 Childrenwere defined as having a filaggrin mutation if they carried at least 1 ofthe mutations.
For ORMDL3 genotyping, allelic discrimination at the rs7216389 singlenucleotide polymorphism on chromosome 17q12-21 was performed, as previ-ously detailed.E5
For DENND1B genotyping, allelic discrimination at the rs2786098 onchromosome 1q31.3 was performed, as described by Sleiman et al.E6
REFERENCESE1. Loland L, Buchvald FF, Halkjaer LB, Anhøj J, Hall GL, Persson T, et al. Sensi-
tivity of bronchial responsiveness measurements in young infants. Chest 2006;129:669-75.
E2. Bisgaard H, Loland L, Holst KK, Pipper CB. Prenatal determinants of neonatallung function in high-risk newborns. J Allergy Clin Immunol 2009;123:651-7.
E3. Bisgaard H. The Copenhagen Prospective Study on Asthma in Childhood (COP-SAC): design, rationale, and baseline data from a longitudinal birth cohort study.Ann Allergy Asthma Immunol 2004;93:381-9.
E4. Palmer CN, Irvine AD, Terron-Kwiatkowski A, Zhao Y, Liao H, Lee SP, et al.Common loss-of-function variants of the epidermal barrier protein filaggrin area major predisposing factor for atopic dermatitis. Nat Genet 2006;38:441-6.
E5. BisgaardH,BonnelykkeK, Sleiman PM,BrasholtM, ChawesB,Kreiner-Møller E,et al. Chromosome 17q21 gene variants are associated with asthma and exacerba-tions but not atopy in early childhood.AmJRespirCrit CareMed2009;179:179-85.
E6. Sleiman PM, Flory J, Imielinski M, Bradfield JP, Annaiah K, Wills-Owen SA,et al. Variants of DENND1B associated with asthma in children. N Engl JMed 2010;362:36-44.
J ALLERGY CLIN IMMUNOL
AUGUST 2012
361.e1 CHAWES ET AL

FIG E1. Study group flow chart.
J ALLERGY CLIN IMMUNOL
VOLUME 130, NUMBER 2
CHAWES ET AL 361.e2

TABLE E1. Baseline characteristics and lung function results of children with acute severe bronchiolitis during the first 2 years of life,
excluding cases with acute severe asthma-like exacerbations but not fulfilling all diagnostic criteria for acute severe bronchiolitis, and
control subjects
Study group (n 5 411) Acute asthma-like exacerbations (n 5 11) Bronchiolitis (n 5 34) Control subjects (n 5 366)
SexMale sex (no.) 36.4% (4) 64.7% (22) 48.4% (177)
AnthropometricsBMI at birth (cm/kg2), median (IQR) 12.3 (11.3-14.8) 12.5 (11.6-13.7) 12.8 (12.0-13.7)
EnvironmentSmoking, 3rd trimester (no.) 18.2% (2) 35.3% (12)! 13.1% (48)Alcohol, 3rd trimester (no.) 0% (0) 14.7% (5) 18.6% (68)Cat at birth (no.) 20.0% (2) 17.7% (6) 14.8% (52)Dog at birth (no.) 10.0% (1) 14.7% (5) 13.6% (48)Older siblings at birth (no.) 45.5% (5) 52.9% (18) 42.4% (155)
Household income at birth (no.)Low, <53,000V 9.1% (1) 30.3% (10) 29.6% (101)Medium, 53,000V-80,000V 45.5% (5) 54.6% (18) 46.6% (159)High, >80,000V 36.4% (4) 15.2% (5) 23.8% (81)Paternal history of asthma (no.) 11.1% (1) 24.2% (8) 16.5% (59)Age at start of day care (d), median (IQR) 252 (194-376) 296 (230-349) 341 (240-417)Solely breast-fed (d), median (IQR) 122 (27-123) 120 (72-179) 122 (89-155)
Lung function at age 1 moFEV0.5 (z score), mean (SD) 20.16 (1.38) 20.18 (0.91) 20.01 (0.99)FEF50 (z score), mean (SD) 20.37 (0.96) 20.37 (1.05) 20.09 (1.00)PD15 (PtcO2 [mmol]), median (IQR) 0.09 (0.04-0.25) 0.13 (0.07-0.60)! 0.33 (0.12-0.88)
GeneticsFilaggrin mutation 20.0% (2) 18.2% (6) 9.7% (34)ORMDL3 (TT) 40.0% (4)* 48.5% (16)! 26.7% (92)
DENND1B genotype (rs2786098)AA 11.1% (1) 3.5% (1) 4.2% (14)AB 33.3% (3) 13.8% (4) 27.5% (91)BB 55.6% (5) 82.7% (24) 68.3% (226)
*Significant difference, children with acute asthma-like exacerbations versus control subjects.!Significant difference, bronchiolitis cases versus control subjects.
J ALLERGY CLIN IMMUNOL
AUGUST 2012
361.e3 CHAWES ET AL

Neonates with reduced neonatal lung function havesystemic low-grade inflammation
Bo L. K. Chawes, MD, PhD,a Jakob Stokholm, MD, PhD,a,c Klaus Bønnelykke, MD, PhD,a Susanne Brix, MSc, PhD,b and
Hans Bisgaard, MD, DMSca Copenhagen, Denmark
Background: Children and adults with asthma and impairedlung function have been reported to have low-grade systemicinflammation, but it is unknown whether this inflammationstarts before symptoms and in particular whether low-gradeinflammation is present in asymptomatic neonates with reducedlung function.Objective: We sought to investigate the possible associationbetween neonatal lung function and biomarkers of systemicinflammation.Methods: Plasma levels of high-sensitivity C-reactive protein (hs-CRP), IL-1b, IL-6, TNF-a, and CXCL8 (IL-8) were measured atage 6months in 300 children of the Copenhagen Prospective Studyon Asthma in Childhood2000 birth cohort who had completedneonatal lung function testing at age 4weeks. Associations betweenneonatal lung function indices and inflammatory biomarkers wereinvestigated by conventional statistics and unsupervised principalcomponent analysis.Results: The neonatal forced expiratory volume at 0.5 secondswasinversely associated with hs-CRP (b-coefficient,20.12; 95% CI,20.21 to20.04; P < .01) and IL-6 (b-coefficient,20.10; 95% CI,20.18 to20.01; P5 .03) levels. The multivariate principalcomponent analysis approach, including hs-CRP, IL-6, TNF-a,and CXCL8, confirmed a uniform upregulated inflammatoryprofile in children with reduced forced expiratory volume at 0.5seconds (P5 .02). Adjusting for bodymass index at birth,maternalsmoking, older children in the home, neonatal bacterial airwaycolonization, infections 14days before, andasthmatic symptoms, as
well as virus-induced wheezing, at any time before biomarkerassessment at age 6 months did not affect the associations.Conclusion: Diminished neonatal lung function is associatedwith upregulated systemic inflammatory markers, such ashs-CRP. (J Allergy Clin Immunol 2015;135:1450-6.)
Key words: Asthma, children, high-sensitivity C-reactive protein,proinflammatory cytokines, spirometry
C-reactive protein (CRP) is an acute-phase reactant found in theblood in response to acute and chronic inflammatory conditionsand has a broad clinical application in screening for infectious andimmune-mediated diseases.1 CRP has important innate immunityproperties and is released from the liver after triggering byproinflammatory cytokines, such as IL-6, IL-1b, and TNF-a.2
CRP assays3 with increased sensitivity (high-sensitivityC-reactive protein [hs-CRP]) have demonstrated low-gradeinflammation in patients with disorders such as cardiovasculardisease,4 obesity,5 and diabetes mellitus.6 Increased hs-CRPlevels have also been demonstrated during and shortly after viralrespiratory tract infections7 and in patients with symptomaticairway diseases, such as asthma8 and chronic obstructivepulmonary disease.9 In addition, impaired lung function inasthmatic children and adults has been associated with thepresence of systemic low-grade inflammation.10,11
We hypothesized that impaired lung function would beassociated with the systemic inflammatory process, even beforedevelopment of any respiratory symptoms. Therefore wemeasured plasma hs-CRP, IL-1b, IL-6, TNF-a, and CXCL8(formerly IL-8) levels at the early age of 6 months and relatedthese to neonatal lung function assessed at age 4 weeks in theCopenhagen Prospective Study on Asthma in Childhood2000(COPSAC2000) birth cohort.
METHODSStudy cohort
The study participants were 411 neonates born of mothers with a history ofasthma and enrolled at 4weeks of age in theCOPSAC2000 prospective birth cohortstudy.12-14 Exclusion criteria were any respiratory symptoms or respiratory sup-port before inclusion, gestational age of less than 36 weeks, and any congenitalabnormality or systemic illness, such as severe neonatal sepsis. The childrenattended the COPSAC research clinic at age 4 weeks for assessment of neonatallung function and subsequently at 6-month intervals, as previously detailed.12-14
EthicsThe study was conducted in accordance with the guiding principles of the
Declaration of Helsinki and was approved by the local ethics committee(KF 01-289/96) and the DanishData ProtectionAgency (2008-41-1754). Bothparents provided oral and written informed consent before enrollment.
Inflammatory biomarkersBlood was drawn in an EDTA tube from a cubital vein at the age of 6 months,
centrifuged to separate plasmaandplasmacells, and immediately stored at2808C
From aCopenhagen Prospective Studies on Asthma in Childhood, Health and MedicalSciences, University of Copenhagen & Danish Pediatric Asthma Center, GentofteHospital, University of Copenhagen; bthe Center for Biological Sequence Analysis,Department of Systems Biology, Technical University of Denmark; and cthe Depart-ment of Pediatrics, Naestved Hospital.
COPSAC is funded by private and public research funds listed on www.copsac.com. TheLundbeck Foundation (R16-A1694), the Danish State Budget (0903516), the DanishStrategic Research Council (0603-00280B), and the Danish Medical ResearchCouncil (10-082884 & 271-08-0815) provided the core support for COPSAC researchcenter. The funding agencies did not have any role in design and conduct of the study;collection, management, and interpretation of the data; or preparation, review, orapproval of the manuscript.
Disclosure of potential conflict of interest: B. L. K. Chawes has received research supportfrom A.P. Møller og Hustru Chastine Mc-Kinney Møllers Fond til almene Formaal(13-41). H. Bisgaard has received research support from the Danish Council for Stra-tegic Research (0603-00280B) and the Lundbeck Foundation (R16-A1694) and hasgrants pending from the European Commission. The rest of the authors declare thatthey have no relevant conflicts of interest.
Received for publication June 4, 2014; revised November 14, 2014; accepted for publi-cation November 14, 2014.
Available online January 8, 2015.Corresponding author: Hans Bisgaard, MD, DMSc, Copenhagen Prospective Studies onAsthma in Childhood, Health and Medical Sciences, University of Copenhagen &Danish Pediatric Asthma Center, Gentofte Hospital, University of Copenhagen, Ledre-borg All!e 34, DK-2820 Gentofte, Denmark. E-mail: [email protected].
0091-6749/$36.00! 2014 American Academy of Allergy, Asthma & Immunologyhttp://dx.doi.org/10.1016/j.jaci.2014.11.020
1450

Abbreviations usedBMI: Body mass index
COPSAC2000: Copenhagen Prospective Study on Asthma inChildhood
CRP: C-reactive proteinFEF50: Forced expiratory flow at 50% of the forced vital
capacityFEV0.5: Forced expiratory volume at 0.5 secondsFVC: Forced vital capacity
hs-CRP: High-sensitivity C-reactive proteinIQR: Interquartile rangePC1: First principal componentPCA: Principal component analysis
TROLS: Troublesome lung symptoms
until analysis. The samples were transported on dry ice to the laboratory,where levels of the a priori selected biomarkers were determined by usinghigh-sensitivity ELISAs based on electrochemiluminescence in a 4-plexsetting for IL-1b, IL-6, CXCL8, and TNF-a and as a single assay forhs-CRP. Samples were read in duplicates by using the Sector Imager 6000(Meso Scale Discovery, Gaithersburg, Md). The limit of detection (meansignal from blanks 1 3SD) was 9.54 pg/mL for hs-CRP, 0.15 pg/mL forIL-1b, 0.17 pg/mL for IL-6, 0.09 pg/mL for CXCL8, and 0.08 pg/mL forTNF-a.
Neonatal lung functionNeonatal spirometric results were measured at age 4 weeks, applying the
raised-volume rapid thoracoabdominal ‘‘squeeze’’ jacket compressiontechnique.15 Repeated ventilations to predefined mouth pressures ensuredexpansion of the lung volume before an instant inflation of the jacket causeda full exhalation during which the flow was measured by using apneumotachograph with an air-cushion facemask.16,17 The software identifiedforced vital capacity (FVC) as the first plateau on the volume-time curve, andmeasurements with FVC appearing after 0.5 seconds and the forced expiratoryvolume at 0.5 seconds (FEV0.5) being less than or equal to FVCwere accepted.Three to 5 acceptable curves were obtained for each measurement, and thecurve containing the median value of FEV0.5 was used for analysis ofFEV0.5 and forced expiratory flow at 50% of forced vital capacity (FEF50).
For neonatal bronchial responsiveness, after an initial saline inhalation,methacholine was administered in quadrupling dose steps with a dosimeterattached to a nebulizer (SPIRA 08 TSM 133; Respiratory Care Center,H€ameenlinna, Finland).17 Bronchial responsiveness was determined bymeansof continuous assessment of transcutaneous oxygen saturation (TCM3;Radiometer, Copenhagen, Denmark). The provocative dose of methacholinecausing a 15% decrease in transcutaneous oxygen saturation was estimatedfrom the dose-response curves fitted with a logistic function.
Troublesome lung symptomsTroublesome lung symptoms (TROLS) were defined as significant cough
or wheeze or dyspnea severely affecting the well-being of the child and recordedby the parents in a daily diary chart as a dichotomized score (yes/no) frombirth.18-20 At acute episodes of TROLS (>_3 consecutive days with TROLS), thechildren were seen at the COPSAC clinic for a clinical examination, including arhinopharyngeal aspirate for viral detection (picornaviruses, respiratorysyncytial virus, coronaviruses, parainfluenza viruses, influenza viruses, humanmetapneumoviruses, adenoviruses, and bocavirus).21
CovariatesCovariates included heredity (father’s history of asthma, eczema, or allergy
[yes/no]); anthropometrics (birth body mass index [BMI; 7-12, 12-13, 13-14,and 14-17 m/kg2]); demographics (sex, older children in the home at birth
[yes/no], and yearly household income [low at <V53,000, medium atV53,000-V80,000, and high at >V80,000]); prenatal and antenatal exposures(maternal smoking during the third trimester of pregnancy [yes/no] andcesarean section [yes/no]); postnatal exposures (bacterial airway colonizationwith Streptococcus pneumoniae, Haemophilus influenzae, or Moraxellacatarrhalis at age 4 weeks [yes/no],14 length of sole breast-feeding [0-3,3-6, and >6 mo], age at start in day care [0-9, 9-12, and >12 mo], and petsin the home in the first year of life: cat [yes/no] or dog [yes/no]); any TROLS(yes/no) and any episodes of TROLS with virus detected before biomarkerassessment (yes/no); and any infection 14 days before biomarker assessment(upper and lower respiratory tract infections, gastroenteritis, or fever withunknown cause [yes/no]).
StatisticsBiomarker null values were set to half of the lowest detected value for
the specific biomarker, values were log-transformed, and the mean ofthe duplicate measurements were used for association analyses. z Scoreswere calculated for FEV0.5 and FEF50, and the provocative dose ofmethacholine causing a 15% decrease in transcutaneous oxygen saturationwas log-transformed to obtain normality.
The associations between neonatal lung function indices and inflammatorybiomarkers were tested by using conventional statistics with general linearmodels and by using unsupervised pattern recognition with principalcomponent analysis (PCA). In the PCA analyses we extracted underlyingorthogonal components that described the systematic part of the variationacross the biomarkers using log-transformed and z score mediator levels.
All results are presented as raw estimates with 95% CIs and as estimatesobtained from partial regression analyses, adjusting for covariates associatedwith levels of hs-CRP by using a cutoff P value of .10 or less. Birth BMI andmaternal smoking during the third trimester were retained in the multivariablemodels independently of their association with hs-CRP because these areimportant determinants of neonatal lung function.22 Interaction with bacterialairway colonization, any TROLS, and acute episodes of TROLS with virusdetected was tested by adding cross-products to the models. A P value of.05 or less was considered significant. All analyses were done with SASsoftware, version 9.3 (SAS Institute, Cary, NC).
RESULTSInflammatory biomarker assessments
Measurements of IL-1b, IL-6, TNF-a, and CXCL8 levels wereperformed on 309 plasma samples collected at age 6 months, andmeasurements of hs-CRP levels were performed on 301 plasmasamples collected at age 6 months. One sample was lost fortechnical reasons while performing the 4-plex assay, resulting in300 children (73% of the original 411 cohort children) withavailable measurements for all 5 biomarkers. We found nosignificant differences in baseline characteristics betweenchildren with and without available biomarker assessments(see Table E1 in this article’s Online Repository at www.jacionline.org).
Median levels were as follows: hs-CRP, 1.39mg/L (interquartilerange [IQR], 0.46-4.61 mg/L); IL-1b, 0.01 ng/L (IQR, 0.001-0.04ng/L); IL-6, 0.20 ng/L (IQR, 0.11-0.31 ng/L); TNF-a, 2.34 ng/L(IQR, 1.92-2.88 ng/L); and CXCL8, 3.04 ng/L (IQR, 2.19-4.37 ng/L). IL-6 and TNF-a levels were strongly positively correlated withhs-CRP levels (P < .001 for both), whereas IL-1b and CXCL8levels were not correlated with hs-CRP levels (P >_ .62). Themeasured values of hs-CRP, IL-6, TNF-a, and CXCL8werewithinthe expected range,23 with very few null values, whereas IL-1blevels were much lower than expected,23 with null values for 72(23%) of 308 children. Because of this and the fact that IL-1bhas been shown to significantly degrade over time, even at2808C,24 IL-1b was not included in further analyses.
J ALLERGY CLIN IMMUNOL
VOLUME 135, NUMBER 6
CHAWES ET AL 1451

Determinants of hs-CRPChildren with older children in the home at birth had
significantly higher hs-CRP levels at age 6 months comparedwith children without older children in the home (median hs-CRPlevel, 2.20 mg/L [IQR, 0.63-5.05 mg/L] vs 1.16 mg/L [IQR,0.41-3.40 mg/L], P 5 .005). In addition, hs-CRP levels wereincreased in children who experienced an infectious episodewithin 14 days before biomarker assessment compared withchildren without apparent infections (4.29 mg/L [IQR,1.71-5.34 mg/L] vs 0.84 mg/L [IQR, 0.36-2.67 mg/L],P < .0001); in children experiencing TROLS at any time pointbefore biomarker assessment compared with children withoutTROLS (1.79 mg/L [IQR, 0.50-4.72 mg/L] vs 1.19 mg/L [IQR,0.46-4.14 mg/L], P 5 .05); and in children with acute episodesof TROLS with an airway virus detected (3.78 mg/L [IQR,1.00-5.42 mg/L] vs 1.16 mg/L [IQR, 0.41-3.85 mg/L],P < .0001). Children with bacterial airway colonization at age 4weeks compared with noncolonized children showed a trend ofincreased hs-CRP levels (2.68 mg/L [IQR, 0.84-5.17 mg/L] vs1.31 mg/L [IQR, 0.49-4.64 mg/L], P 5 .08). We did notdetect associations between hs-CRP levels and paternalhistory of asthma, eczema, or allergy; child’s sex; birthBMI; household income; maternal smoking during the thirdtrimester of pregnancy; birth by means of cesarean section;breast-feeding; day care attendance; and pets in the home(Table I).
Neonatal lung function and systemic low-gradeinflammation
hs-CRP. The conventional statistical approach showed astrong linear inverse association between FEV0.5 values at age 4weeks and hs-CRP levels at age 6 months (b-coefficient,20.12; 95% CI, 20.21 to 20.04; P 5 .004), suggestingincreasing grade of inflammation by diminished neonatal lungfunction (Fig 1). The association was unchanged by adjustmentfor older children in the home, bacterial airway colonization atage 4 weeks, infections 14 days before, and any TROLS, aswell as acute virus-related episodes of TROLS at any time beforebiomarker assessment, birth BMI, and maternal smoking in thethird trimester (b-coefficient, 20.12; 95% CI, 20.22 to 20.02;P 5 .02). Furthermore, we found no interaction with bacterialairway colonization (P5 .21), any TROLS (P5 .76), or any acuteepisodes of TROLS with a virus detected (P 5 .20).
FEF50 values also seemed inversely associated with hs-CRPlevels but was not significant (b-coefficient, 20.06; 95% CI,20.15 to 0.02; P 5 .14).
IL-6. Increasing FEV0.5 values were also significantlyassociated with decreasing IL-6 levels (b-coefficient, 20.10;95%CI,20.18 to20.01; P5 .03; Fig 2). Confounder adjustmentdid not substantially change the association (b-coefficient,20.11; 95% CI, 20.22 to 0.01; P 5 .07). We did not detect asignificant association between FEF50 values and IL-6 levels.
TNF-a and CXCL8. FEV0.5 and FEF50 measurementswere not associated with CXCL8 or TNF-a levels, although theb-coefficients suggested an inverse association between lungfunction indices and TNF-a levels (Table II).
PCA. Unsupervised PCA showed that hs-CRP, IL-6, TNF-a,and CXCL8 levels were positively correlated in the firstprincipal component (PC1), which explained 41% of the totalvariation in the data. The PCA approach is illustrated in the
TABLE I. Heredity; anthropometrics; demographics; prenatal,
perinatal, and postnatal exposures; TROLS; airway microbi-
ology; and infections before assessment of low-grade
inflammation in relation to hs-CRP levels at age 6 months
Characteristic No.
hs-CRP (mg/L)
at age 6 mo
Median (IQR)
P
value
Paternal asthma, allergy, or eczema .54
Yes 135 1.52 (0.46-4.61)
No 153 1.31 (0.46-4.44)
Sex .62
Male 155 1.37 (0.37-4.44)
Female 146 1.51 (0.49-4.81)
BMI at birth .56
7-12 m/kg2 78 1.06 (0.45-4.46)
12-13 m/kg2 73 1.80 (0.56-4.69)
13-14 m/kg2 74 1.41 (0.48-4.98)
14-17 m/kg2 76 1.25 (0.39-3.75)
Older children in home at birth .005
Yes 114 2.20 (0.63-5.05)
No 177 1.16 (0.41-3.40)
Household income at birth (yearly)* .17
Low 77 0.83 (0.38-3.57)
Average 144 1.31 (0.46-4.63)
High 70 2.27 (0.67-4.92)
Maternal smoking during third trimester .33
Yes 51 1.40 (0.41-4.46)
No 250 1.22 (0.64-5.02)
Cesarean section .20
Yes 60 1.81 (0.52-5.13)
No 205 1.31 (0.46-3-93)
Solely breast-feeding period .43
0-3 mo 64 2.16 (0.49-5.35)
3-6 mo 160 1.51 (0.46-4.31)
>6 mo 40 1.02 (0.55-3.87)
Age at start in day care .26
0-9 mo 89 1.80 (0.50-5.13)
9-12 mo 77 1.13 (0.36-3.40)
>12 mo 123 1.59 (0.50-4.82)
Cat in home in first year of life .42
Yes 46 1.74 (0.67-3.87)
No 248 1.41 (0.44-4.67)
Dog in home in first year of life .56
Yes 44 1.15 (0.50-3.65)
No 249 1.52 (0.49-4.69)
Bacterial airway colonization at age 4 wk! .08
Yes 51 2.68 (0.84-5.17)
No 189 1.31 (0.49-4.64)
Any TROLS at age 1-6 mo .05
Yes 141 1.79 (0.50-4.72)
No 160 1.19 (0.46-4.14)
Episodes of virus-induced TROLS atage 1-6 mo"
<.0001
Yes 57 3.78 (1.00-5.42)
No 244 1.16 (0.41-3.85)
Any infection 14 d before hs-CRPassessment§
<.0001
Yes 95 4.29 (1.71-5.34)
No 206 0.84 (0.36-2.67)
Values in boldface are P < .10.*Yearly household income at birth of neonate: low (<V53,000), medium(V53,000-V80,000), and high (>V80,000).!Bacterial airway colonization with S pneumoniae, H influenzae, or M catarrhalis atthe time of neonatal lung function testing."Picornaviruses, respiratory syncytial virus, coronaviruses, parainfluenza viruses,influenza viruses, human metapneumoviruses, adenoviruses, or bocavirus.§Any infection includes any upper or lower respiratory tract infection, gastroenteritis,or fever with unknown cause.
J ALLERGY CLIN IMMUNOL
JUNE 2015
1452 CHAWES ET AL

biplot (Fig 3), showing scores for PC1 and PC2 and loadings forthe biomarkers. Because of the univocal pattern in PC1, wefocused on PC1 in the further analyses. Confirming the findingsfrom conventional statistics, we found that FEV0.5 values wereinversely associated with PC1 values (P 5 .02) and remainedsignificant after confounder adjustments (P 5 .03). There wasno interaction with bacterial airway colonization, any TROLS,or any acute episodes of TROLS with a virus detected (all inter-action P >_ .20). The b-coefficients also suggested an inverse as-sociation between FEF50 and PC1 values, but the model was notsignificant (Table II).
Neonatal bronchial responsiveness and systemiclow-grade inflammation
Bronchial responsiveness to methacholine in neonatal life wasnot associated with biomarkers of low-grade inflammation at age6 months (Table II).
DISCUSSIONKey findings
Infants with reduced pulmonary capacity as neonates arecharacterized by systemic low-grade inflammation with anupregulated blood inflammatory response, including increasedhs-CRP levels. This association suggests that reduced neonatallung function is part of a condition with an ongoing asymptomaticairway inflammation and a measurable systemic component fromthe beginning of life.
Strengths and limitations of the studyA major strength of the study is the unique assessment of
neonatal lung function with the state-of-the-art raised-volumerapid thoracoabdominal compression technique performedstrictly in adherence with recognized guidelines15 in thefull mother-child birth cohort. The neonatal spirometricmeasurements were obtained in this cohort of asymptomaticchildren before any respiratory symptoms and are thus unbiasedfrom previous or concurrent airway symptoms.
Another significant strength of the study is the availability of arange of environmental exposure assessments, including bacterialairway colonization and the presence of a virus, enabling robustconfounder adjustment for factors with a possible influence onneonatal lung function and low-grade inflammation. However, it is alimitation that we did not assess the presence of bacteria and virusesat both lung function and inflammatory biomarker testing.
There were strong linear correlations between IL-6 and TNF-alevels and hs-CRP levels. Because IL-6 and TNF-a are the maintriggers of CRP release from the liver,2 these expectedcorrelations serve as a biological validation of the data. Thelack of correlation between CXCL8 and hs-CRP levels was notsurprising because CXCL8 primarily has a neutrophilicchemotactic function in the innate immune system and does notdirectly induce CRP release.25 The finding of significantlyincreased hs-CRP levels in children experiencing an infectiousepisode within 14 days before biomarker assessment furthervalidates the data because CRP is a reliable biomarker of airwayinflammation.1 Even after adjusting for this confounder, theassociation between neonatal lung function and hs-CRP levelsremained, with largely unchanged effect estimates.
Both the standard statistical approach and the unsuperviseddata-driven PCA approach showed similar associations,which strengthened confidence in our findings. Still, we didnot detect association between neonatal bronchial hyper-responsiveness and low-grade inflammation, which we wouldhave expected given our previous finding of associationbetween methacholine challenge results and subsequent asthmadevelopment.26
It is a limitation of the study that we were unable to detect abiologically meaningful signal from IL-1b, which is presumablycaused in part by the plasma storage time of up to 13 years beforeanalysis, during which samples had been thawed and frozen onseveral occasions. IL-1b is particularly sensitive to freeze-thawcycles and degrades by greater than 50% over time, even whensamples are stored at 2808C.24 It is well known that circulatingIL-1b levels are approximately 5 times less than TNF-a levelsin healthy adults,23 but in our case the median IL-1b levelwas 200 times less than the median TNF-a level (0.01 vs2.34 ng/L), and we were unable to detect an association betweenIL-1b and hs-CRP levels.
FIG 1. Scatter plot illustrating the relationship between neonatal lungfunction (z score of FEV0.5) and hs-CRP level at age 6 months(log-transformed values). Solid line, Regression line; shaded area, 95%confidence limits.
FIG 2. Scatter plot illustrating the relationship between neonatal lungfunction (z score of FEV0.5) and IL-6 levels at age 6 months (log-transformedvalues). Solid line, Regression line; shaded area, 95% confidence limits.
J ALLERGY CLIN IMMUNOL
VOLUME 135, NUMBER 6
CHAWES ET AL 1453
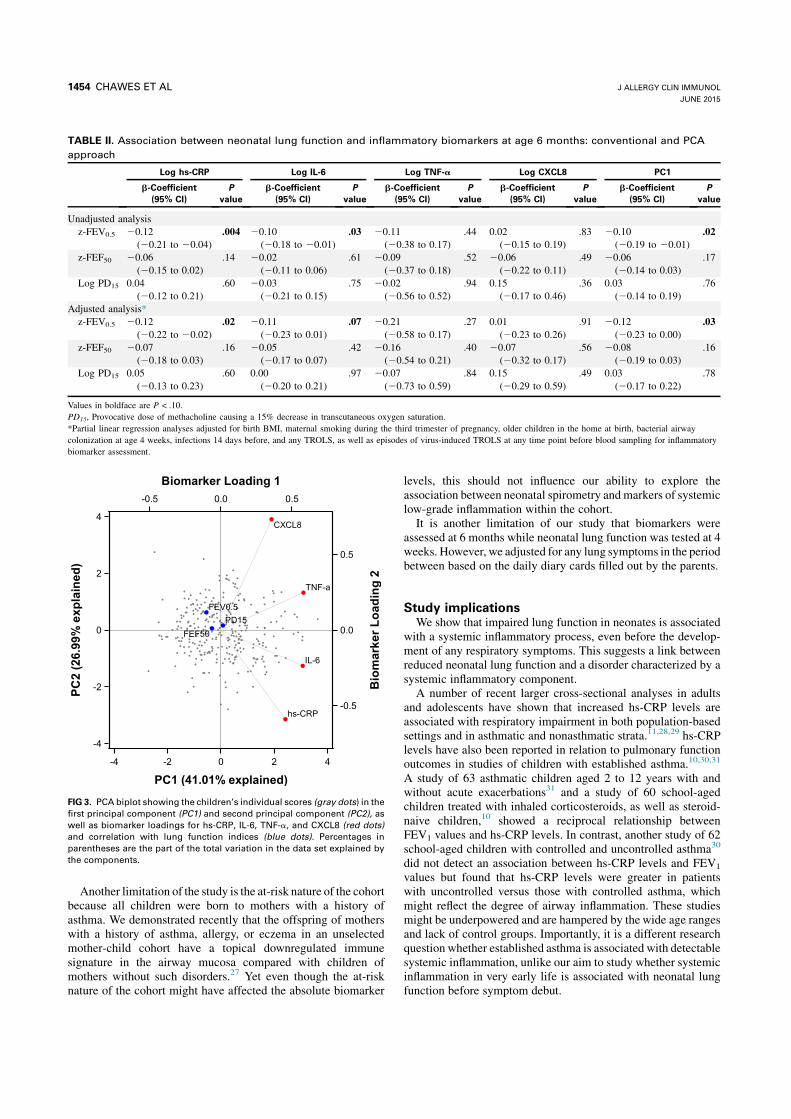
Another limitation of the study is the at-risk nature of the cohortbecause all children were born to mothers with a history ofasthma. We demonstrated recently that the offspring of motherswith a history of asthma, allergy, or eczema in an unselectedmother-child cohort have a topical downregulated immunesignature in the airway mucosa compared with children ofmothers without such disorders.27 Yet even though the at-risknature of the cohort might have affected the absolute biomarker
levels, this should not influence our ability to explore theassociation between neonatal spirometry and markers of systemiclow-grade inflammation within the cohort.
It is another limitation of our study that biomarkers wereassessed at 6 months while neonatal lung function was tested at 4weeks. However, we adjusted for any lung symptoms in the periodbetween based on the daily diary cards filled out by the parents.
Study implicationsWe show that impaired lung function in neonates is associated
with a systemic inflammatory process, even before the develop-ment of any respiratory symptoms. This suggests a link betweenreduced neonatal lung function and a disorder characterized by asystemic inflammatory component.
A number of recent larger cross-sectional analyses in adultsand adolescents have shown that increased hs-CRP levels areassociated with respiratory impairment in both population-basedsettings and in asthmatic and nonasthmatic strata.11,28,29 hs-CRPlevels have also been reported in relation to pulmonary functionoutcomes in studies of children with established asthma.10,30,31
A study of 63 asthmatic children aged 2 to 12 years with andwithout acute exacerbations31 and a study of 60 school-agedchildren treated with inhaled corticosteroids, as well as steroid-naive children,10 showed a reciprocal relationship betweenFEV1 values and hs-CRP levels. In contrast, another study of 62school-aged children with controlled and uncontrolled asthma30
did not detect an association between hs-CRP levels and FEV1
values but found that hs-CRP levels were greater in patientswith uncontrolled versus those with controlled asthma, whichmight reflect the degree of airway inflammation. These studiesmight be underpowered and are hampered by the wide age rangesand lack of control groups. Importantly, it is a different researchquestion whether established asthma is associated with detectablesystemic inflammation, unlike our aim to study whether systemicinflammation in very early life is associated with neonatal lungfunction before symptom debut.
TABLE II. Association between neonatal lung function and inflammatory biomarkers at age 6 months: conventional and PCA
approach
Log hs-CRP Log IL-6 Log TNF-a Log CXCL8 PC1
b-Coefficient(95% CI)
Pvalue
b-Coefficient(95% CI)
Pvalue
b-Coefficient(95% CI)
Pvalue
b-Coefficient(95% CI)
Pvalue
b-Coefficient(95% CI)
Pvalue
Unadjusted analysisz-FEV0.5 20.12
(20.21 to 20.04).004 20.10
(20.18 to 20.01).03 20.11
(20.38 to 0.17).44 0.02
(20.15 to 0.19).83 20.10
(20.19 to 20.01).02
z-FEF50 20.06(20.15 to 0.02)
.14 20.02(20.11 to 0.06)
.61 20.09(20.37 to 0.18)
.52 20.06(20.22 to 0.11)
.49 20.06(20.14 to 0.03)
.17
Log PD15 0.04(20.12 to 0.21)
.60 20.03(20.21 to 0.15)
.75 20.02(20.56 to 0.52)
.94 0.15(20.17 to 0.46)
.36 0.03(20.14 to 0.19)
.76
Adjusted analysis*z-FEV0.5 20.12
(20.22 to 20.02).02 20.11
(20.23 to 0.01).07 20.21
(20.58 to 0.17).27 0.01
(20.23 to 0.26).91 20.12
(20.23 to 0.00).03
z-FEF50 20.07(20.18 to 0.03)
.16 20.05(20.17 to 0.07)
.42 20.16(20.54 to 0.21)
.40 20.07(20.32 to 0.17)
.56 20.08(20.19 to 0.03)
.16
Log PD15 0.05(20.13 to 0.23)
.60 0.00(20.20 to 0.21)
.97 20.07(20.73 to 0.59)
.84 0.15(20.29 to 0.59)
.49 0.03(20.17 to 0.22)
.78
Values in boldface are P < .10.PD15, Provocative dose of methacholine causing a 15% decrease in transcutaneous oxygen saturation.*Partial linear regression analyses adjusted for birth BMI, maternal smoking during the third trimester of pregnancy, older children in the home at birth, bacterial airwaycolonization at age 4 weeks, infections 14 days before, and any TROLS, as well as episodes of virus-induced TROLS at any time point before blood sampling for inflammatorybiomarker assessment.
FIG 3. PCA biplot showing the children’s individual scores (gray dots) in thefirst principal component (PC1) and second principal component (PC2), aswell as biomarker loadings for hs-CRP, IL-6, TNF-a, and CXCL8 (red dots)and correlation with lung function indices (blue dots). Percentages inparentheses are the part of the total variation in the data set explained bythe components.
J ALLERGY CLIN IMMUNOL
JUNE 2015
1454 CHAWES ET AL

A possible explanation of the identified association betweenreduced neonatal lung function and increased hs-CRP levels isthat diminished forced volume is caused by airway inflammation.In vitro murine and human lung cell studies have established apossible role of the proinflammatory cytokines stimulatingCRP release, such as IL-6, TNF-a, and IL-1b, in thepathophysiology of obstructive airway inflammation.32,33
Persistently increased CRP levels might induce an increasedvulnerability to changes in the early-life environment throughits actions as a general scavenger protein with important innateimmune functions in the recognition and elimination of bacteriaand damaged human cells through opsonization, phagocytosis,and cell-mediated cytotoxicity.1 Therefore reduced neonatallung function might reflect subclinical bacterial airwaycolonization and airway inflammation predating detection ofclinical symptoms and systemic low-grade inflammation.Such a disease trajectory is well known in patients with cysticfibrosis, for example, in whom reduced lung function hasbeen shown to precede clinical disease penetrance34 and corre-lates with Pseudomonas aeruginosa airway colonization beforeexacerbations.35
Alternatively, reduced neonatal lung function does not lead tosystemic inflammation but is rather an independent characteristicof neonates with sustained low-grade inflammation in early life.Such inefficient immune regulation might be driven by thenewborn’s genotype interacting with the intrauterine andearly-life environment, thereby affecting the plasticity of thedeveloping immune system. In support of the latter theory, higherbaseline CRP levels have been demonstrated in westernizedpopulations, where obstructive airway disorders are moreprevalent compared with rural societies.36
We assessed lung function in the 4-week-old asymptomaticneonates and the inflammatory biomarkers at 6 months. We canonly speculate whether this concurs with the onset of anunderlying disorder or whether this possibly reflects a disorderbeginning even earlier in life, perhaps during pregnancy.
Children of the Danish COPSAC2000 at-risk cohort exhibitedan association between reduced neonatal lung function andupregulated systemic inflammatory biomarkers before symptomonset, suggesting that reduced lung function reflects an ongoinginflammatory disorder with a measurable systemic componentearly in life.
Key messages
d Asthmatic children and adults with diminished pulmo-nary function have increased levels of hs-CRP, a markerof systemic low-grade inflammation. However, it is un-known whether asymptomatic neonates with reducedlung function have signs of systemic inflammation.
d Neonates with impaired respiratory capacity are charac-terized by an upregulated blood inflammatory profile,including hs-CRP, suggesting the presence of systemiclow-grade inflammation in early life before symptomonset.
REFERENCES1. Pepys MB, Hirschfield GM. C-reactive protein: a critical update. J Clin Invest
2003;111:1805-12.
2. Voleti B, Agrawal A. Regulation of basal and induced expression of C-reactiveprotein through an overlapping element for OCT-1 and NF-kappaB on theproximal promoter. J Immunol 2005;175:3386-90.
3. Rifai N, Tracy RP, Ridker PM. Clinical efficacy of an automated high-sensitivityC-reactive protein assay. Clin Chem 1999;45:2136-41.
4. Sabatine MS, Morrow DA, Jablonski KA, Rice MM, Warnica JW, Domanski MJ,et al. Prognostic significance of the Centers for Disease Control/American HeartAssociation high-sensitivity C-reactive protein cut points for cardiovascular andother outcomes in patients with stable coronary artery disease. Circulation 2007;115:1528-36.
5. Nappo A, Iacoviello L, Fraterman A, Gonzalez-Gil EM, Hadjigeorgiou C, MarildS, et al. High-sensitivity C-reactive protein is a predictive factor of adiposity inchildren: results of the identification and prevention of dietary- and lifestyle-induced health effects in children and infants (IDEFICS) study. J Am Heart Assoc2013;2:e000101.
6. Hung MJ, Hsu KH, Hu WS, Chang NC, Hung MY. C-reactive protein forpredicting prognosis and its gender-specific associations with diabetes mellitusand hypertension in the development of coronary artery spasm. PLoS One 2013;8:e77655.
7. Melbye H, Hvidsten D, Holm A, Nordbo SA, Brox J. The course of C-reactiveprotein response in untreated upper respiratory tract infection. Br J Gen Pract2004;54:653-8.
8. Takemura M, Matsumoto H, Niimi A, Ueda T, Matsuoka H, Yamaguchi M, et al.High sensitivity C-reactive protein in asthma. Eur Respir J 2006;27:908-12.
9. Thomsen M, Ingebrigtsen TS, Marott JL, Dahl M, Lange P, Vestbo J, et al. Inflam-matory biomarkers and exacerbations in chronic obstructive pulmonary disease.JAMA 2013;309:2353-61.
10. Deraz TE, Kamel TB, El-Kerdany TA, El-Ghazoly HM. High-sensitivity C reactiveprotein as a biomarker for grading of childhood asthma in relation to clinicalclassification, induced sputum cellularity, and spirometry. Pediatr Pulmonol2012;47:220-5.
11. Kony S, Zureik M, Driss F, Neukirch C, Leynaert B, Neukirch F. Association ofbronchial hyperresponsiveness and lung function with C-reactive protein (CRP):a population based study. Thorax 2004;59:892-6.
12. Bisgaard H. The Copenhagen Prospective Study on Asthma in Childhood(COPSAC): design, rationale, and baseline data from a longitudinal birth cohortstudy. Ann Allergy Asthma Immunol 2004;93:381-9.
13. Bisgaard H, Hermansen MN, Loland L, Halkjaer LB, Buchvald F. Intermittentinhaled corticosteroids in infants with episodic wheezing. N Engl J Med 2006;354:1998-2005.
14. Bisgaard H, Hermansen MN, Buchvald F, Loland L, Halkjaer LB, Bonnelykke K,et al. Childhood asthma after bacterial colonization of the airway in neonates.N Engl J Med 2007;357:1487-95.
15. ATS/ERS statement: raised volume forced expirations in infants: guidelines forcurrent practice. Am J Respir Crit Care Med 2005;172:1463-71.
16. Loland L, Bisgaard H. Feasibility of repetitive lung function measurements byraised volume rapid thoracoabdominal compression during methacholine challengein young infants. Chest 2008;133:115-22.
17. Loland L, Buchvald FF, Halkjaer LB, Anhoj J, Hall GL, Persson T, et al.Sensitivity of bronchial responsiveness measurements in young infants. Chest2006;129:669-75.
18. Bisgaard H, Bonnelykke K, Sleiman PM, Brasholt M, Chawes B, Kreiner-MollerE, et al. Chromosome 17q21 gene variants are associated with asthma andexacerbations but not atopy in early childhood. Am J Respir Crit Care Med2009;179:179-85.
19. Bisgaard H, Pipper CB, Bonnelykke K. Endotyping early childhood asthma byquantitative symptom assessment. J Allergy Clin Immunol 2011;127:1155-64.e2.
20. Chawes BL, Buchvald F, Bischoff AL, Loland L, Hermansen M, Halkjaer LB, et al.Elevated exhaled nitric oxide in high-risk neonates precedes transient early but notpersistent wheeze. Am J Respir Crit Care Med 2010;182:138-42.
21. Bisgaard H, Hermansen MN, Bonnelykke K, Stokholm J, Baty F, Skytt NL, et al.Association of bacteria and viruses with wheezy episodes in young children:prospective birth cohort study. BMJ 2010;341:c4978.
22. Bisgaard H, Loland L, Holst KK, Pipper CB. Prenatal determinants of neonatallung function in high-risk newborns. J Allergy Clin Immunol 2009;123:651-7.
23. Jackman RP, Utter GH, Heitman JW, Hirschkorn DF, Law JP, Gefter N, et al.Effects of blood sample age at time of separation on measured cytokineconcentrations in human plasma. Clin Vaccine Immunol 2011;18:318-26.
24. de Jager W, Bourcier K, Rijkers GT, Prakken BJ, Seyfert-Margolis V. Prerequisitesfor cytokine measurements in clinical trials with multiplex immunoassays. BMCImmunol 2009;10:52.
25. Kohidai L, Csaba G. Chemotaxis and chemotactic selection induced with cytokines(IL-8, RANTES and TNF-alpha) in the unicellular Tetrahymena pyriformis.Cytokine 1998;10:481-6.
J ALLERGY CLIN IMMUNOL
VOLUME 135, NUMBER 6
CHAWES ET AL 1455

26. Bisgaard H, Jensen SM, Bonnelykke K. Interaction between asthma andlung function growth in early life. Am J Respir Crit Care Med 2012;185:1183-9.
27. Folsgaard NV, Chawes BL, Rasmussen MA, Bischoff AL, Carson CG, Stokholm J,et al. Neonatal cytokine profile in the airway mucosal lining fluid is skewed bymaternal atopy. Am J Respir Crit Care Med 2012;185:275-80.
28. Fogarty AW, Jones S, Britton JR, Lewis SA, McKeever TM. Systemic inflamma-tion and decline in lung function in a general population: a prospective study.Thorax 2007;62:515-20.
29. Shaaban R, Kony S, Driss F, Leynaert B, Soussan D, Pin I, et al. Change inC-reactive protein levels and FEV1 decline: a longitudinal population-based study.Respir Med 2006;100:2112-20.
30. Navratil M, Plavec D, Dodig S, Jelcic Z, Nogalo B, Erceg D, et al. Markersof systemic and lung inflammation in childhood asthma. J Asthma 2009;46:822-8.
31. Soferman R, Glatstein M, Sivan Y, Weisman Y. HsCRP levels: measurement ofairway inflammation in asthmatic children. Pediatr Int 2008;50:12-6.
32. DoganciA, SauerK,KarwotR, Finotto S. Pathological role of IL-6 in the experimentalallergic bronchial asthma in mice. Clin Rev Allergy Immunol 2005;28:257-70.
33. Hardyman MA, Wilkinson E, Martin E, Jayasekera NP, Blume C, Swindle EJ, et al.TNF-a–mediated bronchial barrier disruption and regulation by src-family kinaseactivation. J Allergy Clin Immunol 2013;132:665-75.
34. Ranganathan SC, Stocks J, Dezateux C, Bush A, Wade A, Carr S, et al. Theevolution of airway function in early childhood following clinical diagnosis ofcystic fibrosis. Am J Respir Crit Care Med 2004;169:928-33.
35. Pillarisetti N, Williamson E, Linnane B, Skoric B, Robertson CF, Robinson P, et al.Infection, inflammation, and lung function decline in infants with cystic fibrosis.Am J Respir Crit Care Med 2011;184:75-81.
36. McDade TW. Early environments and the ecology of inflammation. Proc Natl AcadSci U S A 2012;109(suppl 2):17281-8.
J ALLERGY CLIN IMMUNOL
JUNE 2015
1456 CHAWES ET AL

TABLE E1. Comparison of baseline characteristics between children with and without complete assessment of early-life low-
grade inflammation
Baseline characteristicChildren with biomarkerassessment (n 5 300)
Children without biomarkerassessment (n 5 111) P value
Paternal asthma, allergy, or eczema (no.) 47% (135) 46% (50) .84!Male sex (no.) 51% (154) 44% (49) .20!BMI at birth (m/kg2), mean (SD) 12.79 (1.34) 12.84 (1.22) .63"Older children in home at birth (no.) 39% (114) 40% (38) .91!Household income at birth* (no.) .12!
Low 27% (77) 38% (35)Average 49% (143) 41% (39)High 24% (70) 21% (20)
Maternal smoking during third trimester (no.) 17% (51) 11% (12) .12!Cesarean section (no.) 23% (60) 27% (25) .45!Solely breast-feeding length (d), median (IQR) 122 (90-155) 122 (74-164) .90§Age at start in day care (d), median (IQR) 345 (240-415) 307 (216-412) .27§Cat in home in first year of life (no.) 16% (46) 14% (14) .61!Dog in home in first year of life (no.) 15% (44) 10% (10) .16!
*Yearly household income at birth of neonate: low (<V53,000), medium (V53,000-V80,000), and high (>V80,000).!x2 Test."t Test.§Wilcoxon rank sum test.
J ALLERGY CLIN IMMUNOL
VOLUME 135, NUMBER 6
CHAWES ET AL 1456.e1