unit 1 – tbl: stridor and acute respiratory infections in children – drs bromwich and kovesi...
TRANSCRIPT

Unit 1 – TBL: Stridor and Acute Respiratory Infections in Children – Drs Bromwich and Kovesi
TBL: Acute Respiratory Distress and Acute Respiratory Infections in Children
Tom Kovesi M.D. F.R.C.P.(C), Pediatric Respirologist, Professor (Pediatrics), Children’s Hospital of Eastern Ontario, University of Ottawa
Matthew Bromwich M.D. F.R.C.S.(C), Pediatric Otolaryngology - Head and Neck Surgery, Assistant Professor (Surgery), Children’s Hospital of Eastern Ontario, University of Ottawa

Unit 1 – TBL: Stridor and Acute Respiratory Infections in Children – Drs Vaccani and Kovesi
Objectives
Explain why respiratory infections are common, and serious, in children. List reasons why children are more susceptible to respiratory infections. Recognize underlying conditions that may predispose children to respiratory
tract infections. Identify the causative organism(s), presentation of, diagnosis of, and
treatment of common pediatric respiratory infections respiratory tract infections: Epiglottitis, Croup, Pertussis, and Bronchiolitis,
Bacterial Pneumonia,Viral Pneumonia and Mycoplasma Pneumonia Describe the differences between sturtor, inspiratory stridor and expiratory
wheezing. Develop an approach to determining the cause of respiratory distress
associated with stridor or wheezing in children and recognize important non"infectious causes of stridor, such as laryngomalaica.
Identify life"threatening pediatric airway emergencies based on history and physical examination.

Predisposing Factors for Respiratory Infections (1): Endogenous Factors
Smaller airway size in infants Develop more respiratory distress when airways narrowed
during infections Less developed (and experienced) immune system (especially
premature infants) Underlying diseases - cystic fibrosis, primary Ciliary dyskinesia,
congenital & acquired immune deficiency, Gastroesophageal Reflux
Congenital anomalies - cardiac (pulmonary edema), neurological handicaps (aspiration)

Predisposing Factors (2): Environmental Factors
Crowding, poverty, poor access to health care & immunizations Malnutrition Day care Environmental tobacco smoke exposure
Smoking in older children & teens Air pollution Indoor Air Pollution
Biomass fuel heaters in developing world Aspirated foreign bodies
Pieces of toys, nuts, pieces of food, cut corners of plastic milk bags
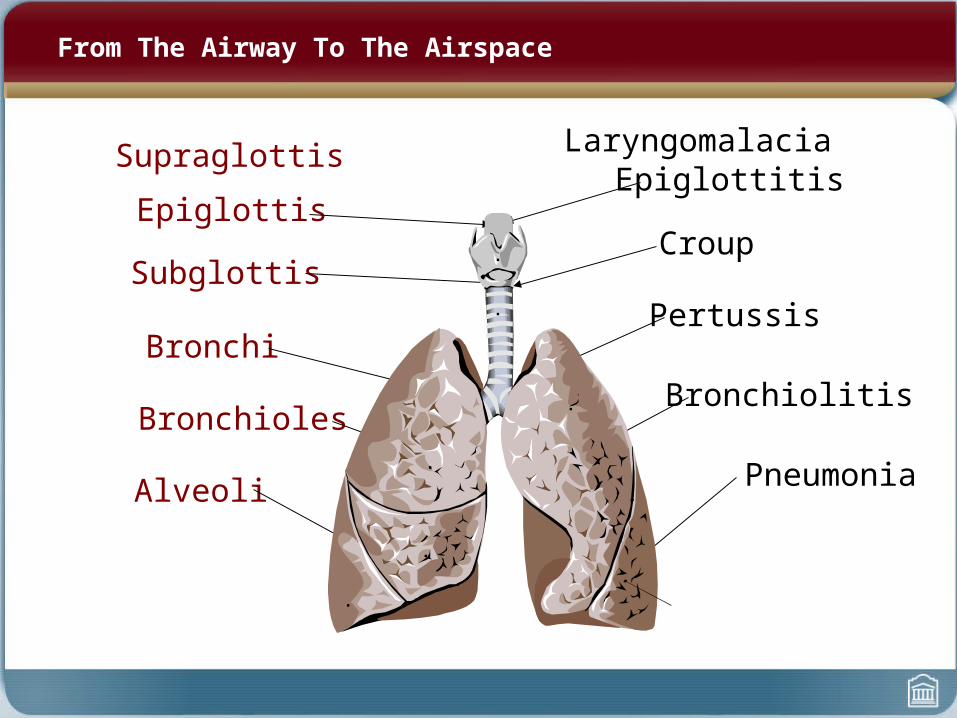
From The Airway To The Airspace
Epiglottitis
Croup
Pertussis
Bronchiolitis
Pneumonia
Epiglottis
Subglottis
Bronchi
Bronchioles
Alveoli
Supraglottis Laryngomalacia

Oropharynx Peritonsillar
cellulitis/abscess Retropharyngeal
abscess Larynx
Epiglottitis Croup
Lower Airway Bronchiolitis Pertussis Pneumonia Tuberculosis
Anatomical locations for Respiratory Distress in Children
Unit 1 – TBL: Stridor and Acute Respiratory Infections in Children – Drs Vaccani and Kovesi
Nasal Cavityo Anterior/Midnasal stenosiso Choanal atreasiao Adenoid Hypertrophy
Oral Cavityo Tonsillar Hypertrophyo Glossoptosis
Pierre-Robin Sequence
Larynxo Laryngomalaciao Vocal cord paralysiso Subglottic stenosis
Tracheao Tracheomalacia
InfectiousAnatomic

Assessing Respiratory Disease in Children (3)
Assess: Respiratory rate Retractions
o Tracheal tugo Intercostal retractionso Subcostal retractions
Accessory muscle useo Sternocleidomastoido Paradoxical respirations
Level of consciousness Cyanosis Pulsus paradoxicus

Bronchoscopy and Suspension

Anatomic: Bronchoscopy

Most common congenital cause of stridor Congenital collapse of tissue into airway from above vocal cords
Several potential causes: Short aryepiglottic folds, Arytenoid prolapse, Omega-shaped epiglottis Maybe… abnormal development of neural control of larynx in babies
Usually starts prior to 2 weeks of age Progresses for first few months of life Slow improvement after this time Usually all symptoms have gone by 18 months of age Very rarely – severe with apnea, failure to thrive, feeding difficulties
May need surgery
Laryngomalacia:
Unit 1 – TBL: Stridor and Acute Respiratory Infections in Children – Drs Vaccani and Kovesi

Symptoms of Laryngomalacia
• Inspiratory stridor• Stridor is not constant
– intermittent– variable intensity
• Increases with agitation and feeding• Decreases with neck extension or prone• Normal cry• Noisier asleep

Arytenoid Prolapse

Omega Epiglottis
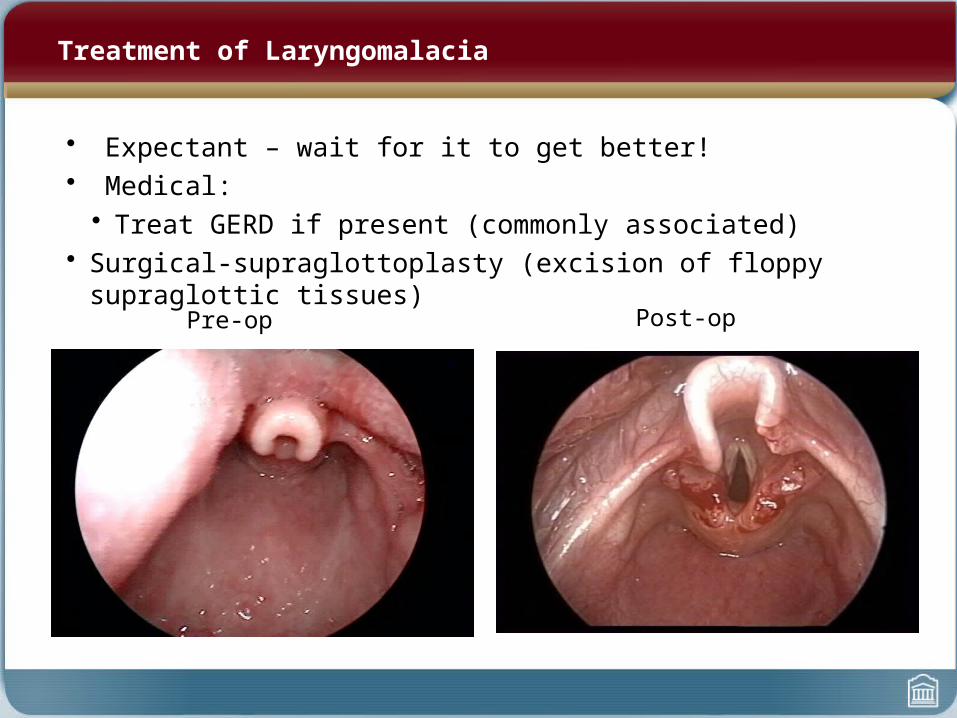
Treatment of Laryngomalacia
• Expectant – wait for it to get better!• Medical:
• Treat GERD if present (commonly associated)• Surgical-supraglottoplasty (excision of floppy supraglottic tissues)
Pre-op Post-op

Other Causes of Stridor in Children
• Congenital– Airway Hemangioma– Airway Webs
• Acquired– Subglottic Stenosis
• Most often: Post-intubation
– Laryngeal Papillomatosis
– Foreign Body– Vocal Cord Paralysis
• Unilateral or bilateral
Unit 1 – TBL: Stridor and Acute Respiratory Infections in Children – Drs Bromwich and Kovesi

Vocal cord paralysis
• Etiologies – most often, acquired:– Iatrogenic ( most common)
• Post cardiac surgery• Prolonged neonatal intubation: scarring
– Brainstem Disorders– Thoracic Masses and compression of recurrent laryngeal nerve– Idiopathic

Two types of vocal cord paralysis
• Unilateral: one cord paralyzed– Usually asymptomatic from respiratory
point of view– Able to create adequate airway
opening– Voice changes– Watch for aspiration
• Bilateral: both cords paralyzed– Unable to create adequate airway
• 80% require trach within first year• 50% resolve after 1 year with no
surgical intervention– Significant inspiratory stridor– Increased risk of aspiration– Marked respiratory distress is often
seen– Permanent surgical correction an
option after 1-2 years of age

Tracheomalacia
• Congenital• Causes expiratory wheeze;
biphasic wheeze if severe• Severe cases can cause:
• Apnea• Feeding Difficulties• Failure to thrive• Recurrent Pneumonias
(reduced mucociliary clearance)
• Associated with:• Other congenital
anomalies (cardiac, vascular rings)
• GERD

Foreign Bodies in the Airway
• Most common in toddler and preschool children
• Most often (but not always) – witnessed history of choking on something, with facial duskiness
• Presentation• Asphyxia – large airway• Respiratory distress• Persistent Pneumonia• Chronic cough• Persistent wheeze• Asymptomatic
• Whenever significant suspicion, needs a rigid bronchoscopy!
Peanut

Retropharyngeal Abscess
• Retropharyngeal lymph nodes drain adenoids and nasopharynx, and can get infected, resulting in abscess formation
• Usual cause: Group A, β-haemolytic Streptococci• Generally children < 2 years of age, following upper respiratory tract infection,
tonsillitis, otitis, adenitis• Can occur in older children from penetrating injury posterior wall of pharynx
(lollipop, fishbones)• Symptoms: fever, sore throat, difficulty and/or pain swallowing, difficulty
breathing, stridor, muffled voice, gurgling breathing• Signs: mass in posterior wall of pharynx, (generally unilateral), hyperextended
neck, enlarged cervical lymph nodes• Diagnosis: enlarged retropharyngeal space on lateral neck X-ray; CT neck
– Normal width retropharyngeal space in child < 15 years is < 7 mm• Treatment: surgical incision & drainage of abscess, intravenous Penicillin

Rules (Length of Retropharyngeal Space)
Normal:
- 7mm at C-2
- 14mm C-6 kids
- 22mm C-6 adults
OR:
>1/2 Vert Body
Retropharyngeal Abscess

Retropharyngeal Abscess

Epiglottitis
• Bacterial infection of supraglottic structures - epiglottis and aryepiglottic folds• Age 2 - 12 years• Caused by Hemophilus influenzae type b; • Rare since HiB (Hemophilus influenza type b) vaccination.• Symptoms progress rapidly:
– severe pain in throat leads to difficulty and avoidance of swallowing, causing drooling
– dyspnea, – muffled cough and voice, – high fever, – anxious expression, – child tends to sit leaning forward
• Risk for epiglottis sticking to laryngeal structures causing complete airway obstruction and asphyxia
• Similar symptoms caused by Bacterial Tracheitis (severe bacterial infection of the trachea with necrotic tissue & pus, caused by Staphylococcus aureus, and occasionally by Haemophilus influenzae)

Lateral Views of the Larynx
Normal Epiglottitis
Diagnosis: • lateral neck X-ray under medical supervision (“thumb sign” epiglottis, thickened aryepiglottic folds) • DO NOT examine throat with tongue depressor or upset the child

Epiglottitis

Treatment of Epiglottitis
Controlled intubation by experienced physician (emergency tracheostomy set available)
Then - culture epiglottis Treat with IV Cefuroxime
(2nd generation Cephalosporin, covers Haemophilus influenzae) Note: Bacterial tracheitis is diagnosed by bronchoscopy.
Treatment: o Intubationo Intravenous Cloxacillin, Vancomycin, or Cefuroxime

Croup (Viral Laryngotracheobronchitis)
• Age 3 months - 5 years• Causes:
– Parainfluenza virus type III (most common)– Influenza virus, – Respiratory syncytial virus (RSV)
• Symptoms - dramatic! – Coryza, – Loud, barky cough – Lots of stridor– Hoarseness– Fever– Cyanosis if severe– Worse at night
• Seasonality: especially fall & spring

Anterior views of the Larynx

More on Croup
• Diagnosis: – Usually clinical– If X-ray done, AP film of neck (“steeple sign”)
• Normal child may have a “steeple sign” if X-ray done in full inspiration
• Treatment: – Oxygen if needed – Oral Steroids (occasionally, nebulized
budesonide)– Nebulized epinephrine if stridor at
rest (to reduce swollen tissues)• Observe 2h afterwards for recurrence
– Traditionally: Cool mist (but not effective in studies)

Pertussis (Whooping Cough)
• The only true “bronchial infection” in children– Children get “bad colds” or bronchopneumonia (visible on CXR);
Otherwise, as children aren’t heavy smokers, “bronchitis symptoms” are invariably viral
• Caused by Bordetella pertussis (85% of cases; occasionally Bordetella parapertussis or Adenovirus can cause similar symptoms)
• Vaccine-preventable, but Pertussis vaccination about 90% effective– Older whole-cell vaccine was less effective, more side effects, and
vaccine effectiveness wanes over time; Adults remain a reservoir, spreading infection back to children
– New acellular vaccine now in widespread use• Infection and toxin production assist bacterial adhesion and lead to
cell necrosis, leads to severe dysfunction of cough receptors

Pertussis (Whooping Cough): Symptoms
• Catarrhal phase - coryza, mild cough - lasts about a week• Paroxysmal phase - severe paroxysms of coughing, leading to facial plethora,
vomiting – In older children, an inspiratory “whoop” at the end of a paroxysm of
coughing. – Paroxysms of coughing can cause apnea in small infants. – Lasts 6 weeks
• Convalescent phase - cough gradually abates, but re-activates with viral colds (never as bad as the initial episode) for up to a year
Severity
Time
Catarrhal Phase
Paroxysmal Phase
Convalescent Phase

Pertussis (Whooping Cough): Diagnosis and Treatment
• Diagnosis: – Nasopharyngeal aspirate (culture or PCR), serologic testing– Chest x-ray shows bronchopneumonia pattern– Occasionally, severe lymphocytosis (“leukemoid
pattern”)• Treatment:
– Macrolide antibiotics shortens the period of infectivity, but affects the cough only when given during the catarrhal phase
– Macrolides are also used to prophylax close contacts.
– Cough remedies have no effect
Casey PA. Altitude treatment for whooping cough. BMJ. 1991 May 18;302(6786):1212.

Bronchiolitis
Viral infection of the bronchioles Causes:
RSV (most common) Less often:
o Influenza o Parainfluenza viruso Rhinoviruso Adenovirus, Metapneumovirus, Bocavirus
Pathology: Viral infection causes intense inflammation, edema, mucous production,
and mucosal shedding of the bronchiolar epithelium Small-airways narrowing or obstruction leads to hyperinflation due to
gas-trapping and areas of atelectasis Bronchospasm may occur May have contiguous spread into interstitium, causing an interstitial
pneumonia

Bronchiolitis: Symptoms and Diagnosis
Symptoms: coryza and fever, followed by respiratory distress (tachypnea, retractions), wheezing,
cough; Cyanosis and lethargy if severe
Diagnosis: Nasopharyngeal aspirate for viral culture or rapid testing
(immunofluoresence assay) Chest radiograph shows:
o hyperinflation, o bronchial wall thickening. o If associated viral pneumonia:
atelectasis, interstitial infiltrates

Bronchiolitis X-ray
Note:• Hyperinflation• Bronchial wall
thickening• Patchy atelectasis

Bronchiolitis: Treatment
Oxygen Extra fluids 30-50% respond to bronchodilators (2-agonists, nebulized
epinephrine) Role of oral steroids controversial – most studies do not support their
use

Bronchiolitis - Prognosis
• Lower respiratory tract involvement during RSV infection associated with anti-RSV IgE (as opposed to anti-RSV IgG) antibodies
• Infants genetically predisposed to producing anti-viral IgE antibodies likely to develop other atopic diseases, so 50% infants with RSV bronchiolitis will later have asthma
• Severe bronchiolitis (especially adenovirus) in aboriginal children may lead to permanent lung damage, including permanent scarring of the bronchioles (bronchiolitis obliterans) and bronchiectasis

Pneumonia (General)
Typical Lobar Pneumonia Bronchopneumonia Due to bacteria: most often Strep
pneumoniae, Haemophilus influenzae
Atypical Interstitial Pneumonia Due to:
o Viruseso Mycoplasma
Children also get: Nosocomial Pneumonia Opportunistic infections
(immunocompromised children) Tuberculosis0
5
10
15
20
25
30
35
40
45
0-5 yrs 5-9 yrs > 9 yrs
Incidence (per 1000)
Commonest in 1st year of life

Diagnosing Pneumonia in Children
• Chest radiograph, CBC• Blood culture• Nasopharyngeal cultures for viruses, mycoplasma• Serology: Mycoplasma, Chlamydia, viruses• TB skin test• In severe cases: Bronchoscopy, Pleural fluid culture• CT Scan, Ultrasound Chest can identify and characterize
complications (lung abscess, empyema)

Lobar Pneumonia
Classic consolidation of one or more lobes, with alveolar spaces being filled with fluid, pus, and fibrin, with eventual organization and consolidation
Symptoms: Onset with URI in infants. May follow influenza, measles (developing
world) Rapid development high fever, lethargy, dyspnea, hacking cough ± sputum production headache, abdominal pain
Physical exam: classical signs pneumonia: crackles, reduced air entry, dullness ± meningismus Signs pleural effusion (if present)

Lobar Bacterial Pneumonia: X-ray and Organisms
CXR: lobar consolidation occupying one or more lobes +/- parapneumonic effusion, empyema
Common organisms: Streptococcus pneumoniae Haemophilus influenzae Group A Streptococcus Staphylococcus aureus

Right Middle Lobe - Lobar Pneumonia - Chest X-ray

Bronchopneumonia
Patchy areas of consolidation near bronchi, often throughout one or in multiple lobes
Suppurative neutrophilic exudate fills bronchi, bronchioles, and adjacent alveolar spaces
Chest X-ray shows patchy infiltrates next to major bronchi Typically follows URI. Symptoms:
Fever, chills Cough Chest Pain (older children) Fatigue Shortness of Breath, Rapid Shallow Breathing Sputum (older children)
Signs: difficulty breathing, productive cough, crackles Causes: Streptococcus pneumoniae, Hemophilus influenzae, β-haemolytic Strep
Group A

Complicated Pneumonia
Bacterial pneumonia can be complicated by: Pleural Effusion
o Parapneumonic Effusion (Transudate)o Empyema (Exudate) – suppurative material and bacteria accumulating
in pleural space Lung Abscess
o Necrosis and breakdown of lung tissue into cavities filled with pus and air (air-fluid level)
Pneumatoceleo Necrosis of breakdown of lung tissue producing air-filled cavity only
Necrotizing Pneumoniao Combination of empyema, consolidation, and multiple lung abscesses
within the consolidated lung Symptoms: rapid progression respiratory distress, cyanosis, shock

The Key Bacteria (1)
• Streptococcus pneumoniae (“Pneumococcus”) – Overwhelmingly the commonest cause of pneumonia in children– ½ of cases are lobar, ½ are bronchopneumonia – commonest cause of parapneumonic effusions, empyema, and
necrotizing pneumonia in children
• Hemophilus influenzae – 3/4 of cases are lobar– 80% cases children < 2 years of age– typable Hemophilus influenzae less common since vaccination– 75% are complicated by pleural effusion– High extra-pulmonary complication rate: meningitis, epiglottitis, septic
arthritis
The Key Bacteria (2)
• Group A Streptococcus – Generally children > 5 years of age
• 1/3 have antecedent strep throat. • Often follows varicella, influenza, measles
– ¾ of cases are bronchopneumonia, ¼ are lobar– Severe pneumonia; massive pleural effusion in at least 2/3 cases
• Staphylococcus aureus– Infants, malnourished children (developing world)– Lobar or segmental infiltrates – Severe pneumonia;
• massive pleural effusion & empyema (75%)• pneumothorax (40%) • pneumatoceles (45%) • lung abscesses

Mycoplasma Pneumonia
Cause: Mycoplasma pneumoniae Rare before 4 years of age; commoner in children over 5 years of age
and very common in adolescents and young adults Symptoms:
Usually - gradual onset fever, headache, malaise, myalgias, dry cough, sore throat, abdominal pain
Occasionally - sudden onset, sputum production may occur Crackles in 75%.
Diagnosis: CXR:
o peribronchial infiltrates, patchy atelectasis most common; o interstitial infiltrates may be seen
Other diagnostic tests: o serologyo PCR or culture of respiratory specimens o Cold agglutinins fairly sensitive but not specific

Mycoplasma Interstitial Pneumonia - Chest X-ray

More on Mycoplasma Pneumonia
Complications common: Arthritis Hemolytic anemia Meningitis
Treatment: Macrolide antibiotic (erythromycin, clarithromycin, or
azithromycin)
Chlamydia pneumoniae causes a similar infection in children, associated with a single, subsegmental lesion

Viral Pneumonia
Common organisms: RSV, Influenza, Parainfluenza, Adenovirus Pathology:
Organisms spread contiguously from upper respiratory tract to lower, causing epithelial necrosis, sloughing, and mucous hypersecretion, causing hyperinflation and areas atelectasis.
Alveolar involvement leads to interstitial mononuclear cell infiltrates & edema Symptoms:
URI anorexia, respiratory distress, cough, fever, cyanosis Wheezing is common
Chest radiograph: Hyperinflation bronchopneumonic/peribronchial infiltrates, interstitial infiltrates, patchy
areas of atelectasis, Treatment: fluids, oxygen

Pneumonia – an Ounce of Prevention
Influenza – influenza vaccination available in Ontario for people 6 months and older Overall, 30% reduction in influenza deaths in Ontario
Strep Pneumoniae: 90 serotypes, 23 account for 85-90% of invasive disease 7-valent protein-conjugated pneumococcal vaccine given at 2, 4, 6, 15 months
o Use resulted in 35% reduction in hospitalization for pneumonia in American children 1997-2006
23-valent polysaccharide vaccine for children 2 years and overo For high-risk children with underlying diseaseo Re-vaccinate in about 5 years
Haemophilus influenzae type b (HiB): Protein-conjugated HiB vaccine given at 2, 4, 6, 18 momths Use resulted in 99.7% reduction in invasive Haemophilus influenza disease
(including epiglottitis) in American children No effect on non-typable Haemophilus influenzae, Haemophilus species

Bacterial Pneumonia: Treatment
Mild-Moderate Pneumonias (Outpatient therapy) Children 1 – 4 years: amoxicillin +/-clavulinic Acid, 2nd-generation
cephalosporin (cefuroxime) Children 5-18 years: macrolide (clarithromycin, azithromycin) if
broncopneumonia, amoxicillin if lobar pneumonia Severe Pneumonia (Inpatient therapy)
IV 2nd-generation cephalosporin (cefuroxime) o IV Ceftriaxone or Vancomycin for Penicillin-resistant Pneumococci
IV cloxacillin for staphylococcus; vancomycin if Methicillin-resistant Pleural effusions or pneumothorax:
Drain with a chest tube if moderate-large Video-assisted Thoracoscopic Surgery (VATS) or fibrinolytics (TPase) by
chest tube if thick/loculated empyemas Pneumatoceles generally resolve on their own