understanding the evidence: preventing, detecting & managing pre-eclampsia & eclampsia
TRANSCRIPT

Understanding the Evidence:Preventing, Detecting &
ManagingPre-Eclampsia & Eclampsia

Objectives
1. Present evidence on pre-eclampsia and eclampsia (PE/E) interventions available for PE/E prevention, detection and management
2. Share emerging evidence and innovations on PE/E

Hypertensive Disorders among Global Maternal Mortality Causes
Eclampsia
Source: Khan et al., 2006; POPPHI, 2009

Declines in Maternal Deaths and Global MMR, 1990–2008
526,300
~440,000
342,900
422
~320
251
0
100
200
300
400
500
0
100000
200000
300000
400000
500000
600000
1980 1990 2008
Glo
bal M
MR
# m
ate
rnal death
s
# maternal deaths Global MMR
Source: Hogan et al., 2010

Declining MMR & Changing Causes of Maternal Deaths: Indonesia
Source: Indonesia Maternal Health Assessment, 2010

Hypertension in Pregnancy
Source: American Society of Hypertension, 2009
Hypertension complicates 5–7% of all pregnancies

PROBABLE DIAGNOSIS TYPICAL SIGNS AND SYMPTOMS
Chronic hypertension Diastolic BP 90 mm Hg or more prior to first 20 weeks of gestation
Pre-eclampsia superimposed on chronic hypertensionwomen with hypertension and no proteinuria early in pregnancy (<20 weeks’ gestation)
In women with hypertension and proteinuria before 20 weeks gestation any of the following are seen: New-onset or worsening proteinuria, or Sudden increase in blood pressure in a woman whose hypertension has previously
been well controlled
Gestational hypertensionTransient hypertension of pregnancy if PE is not present at the time of delivery and blood pressure returns to normal by 12 weeks postpartum (a retrospective diagnosis)
Two readings of diastolic BP 90 mm Hg or more but below 110 mm Hg 4 hours apart after 20 weeks gestation No proteinuria
Mild pre-eclampsia Two readings of diastolic BP 90 mm Hg or more but below 110 mm Hg 4 hours apart Proteinuria up to 2+
Severe pre-eclampsia Diagnosis of pre-eclampsia PLUS one or more of the following diagnostic criteria: Diastolic BP 110 mm Hg or more Proteinuria 3+ or more Hyperreflexia Headache (increasing frequency, unrelieved by regular analgesics) Blurred vision Oliguria (passing less than 400mL of urine in 24 hours) Upper abdominal pain (epigastric or right upper quadrant pain) Pulmonary oedema
Eclampsia Pre-eclampsia with: Convulsions Coma (unconscious)
Source: Prevention and management of pre-eclampsia and eclampsia Reference Manual for Healthcare Providers, MCHIP, 2011

69 (60 - 77)
0 20 40 60 80 100
Doppler combinations of FVWDoppler resistance indexDoppler pulsatility indexDoppler other ratiosDoppler bilateral notchingDoppler any/unilateral notchingSDS Page proteinuria 100 (88 - 100)KallikreinuriaMicroalbumin/creatinine ratioMicroalbuminuriaTotal albuminuriaTotal proteinuriaUrinary calcium/creatinine ratioUrinary calcium excretionSerum uric acidOestriolHCGFoetal DNAFibronectin totalFibronectin cellularAFPBMI<19.8BMI>24.2BMI>29
0 20 40 60 80 100
BMI>34
2529882119111224645316332127982
2289679821469726192933114345153307142219088
22281345705514
2681172732351373135
13709715272044021441082316200
11 (8 - 16)41 (29 - 53)23 (15 - 33)18 (15 - 21)
64 (54 - 74)66 (54 - 76)48 (29 - 69)55 (37 - 72)48 (34 - 62)63 (51 - 74)
19 (12 - 28)62 (23 - 90)70 (45 - 87)35 (13 - 68)50 (36 - 64)57 (24 - 84)36 (22 - 53)26 (9 - 56)24 (16 - 35)50 (31 - 69)65 (42 - 83)50 (30 - 70)9 (5 - 16)
83 (52 - 98)
80 (73 - 86) 75 (62 - 84)88 (80 - 93)93 (87 - 97)
86 (82 - 90)80 (74 - 85)87 (75 - 94)80 (73 - 86)92 (87 - 95)82 (74 - 87)
75 (73 - 77)68 (57 - 77)89 (79 - 94)89 (79 - 94)80 (66 - 89)74 (69 - 79)83 (73 - 90)82 (61 - 93)89 (86 - 92)88 (80 - 93)94 (86 - 98)96 (79 - 99)96 (94 - 98)
98 (98 - 100)
Sensitivity Specificity
Sn (95% CI)Test No of studies No of women Sp (95% CI)
Poor ability to Predict Pre-Eclampsia
Source: Meads CA, 2008.

Who is at Increased Risk for PE?
A personal or family history of PE/E
Pre-existing medical condition including obesity, chronic hypertension, or diabetes
Age: ≤19; >35 years Primigravida IUGR, abruption placenta or
fetal death in previous pregnancy
First pregnancy with a new partner
All pregnant women potentially at risk.
All need prevention and early detection of
PE.

Levels of PE/E Prevention
LEVEL STRATEGY DEFINITION
1. Primary Prevention
Prevention Avoiding the development of the disease
Avoiding pregnancy and conditions favorable to PE development
2. Secondary
Prevention
Detection, Screening
Detecting the disease before clinical PE symptoms appear
3. Tertiary Prevention
Treatment, Management
Treating the disease early to prevent complications
3. Management2. Detection
1. Prevention

PE/E Prevention
Prevention and prediction are difficult because: The cause is not well understood The associated factors are difficult to
influence Focus on symptomatic clinical
management to prevent maternal morbidity (e.g., eclampsia) and mortalitySource: Steegers EA et al., Lancet. 2010
3. Management2. Detection
1. Prevention

Taking Evidence to Scale
Seeking simple,
inexpensive and effective solutions that
reach all pregnant women
Photo credit: D
aniel Antonaccio
3. Management2. Detection
1. Prevention

Preventing Pre-Eclampsia
x x x
Almost 100 interventions tested in randomized trials
1. Prevention

Primary Prevention
Source: Prevention and management of pre-eclampsia and eclampsia reference manual, MCHIP, 2011
Intervention Pregnancy outcome Recommended?
Prevention of IUGRTheoretically contributes to primary prevention of PE (and IUGR) in the next generation
Yes
Family planning Potential to reduce pregnancies at risk for PE Yes
Pre-conceptual prevention and/or treatment of obesity
Potential to reduce PE Yes
Calcium supplementation Reduces PE in those at high risk and with low baseline dietary calcium intake No effect on perinatal outcome
High risk of gestational hypertension;
low dietary calcium intake
Low-dose aspirin Reduces PE Reduces fetal or neonatal deaths
Populations at increased risk
Magnesium or zinc supplementation
No PE reductionInsufficient evidence to
recommend*
Fish oil supplementation and other sources of fatty acids
No effect on low- or high-risk populationsInsufficient evidence to
recommend*
Heparin or low-molecular weight heparin
Reduces PE in women with renal disease and thrombophilia
Insufficient evidence to recommend*
Anti-oxidant vitamins (C, E) Reduced PE in one trial, but not all trials Insufficient evidence to recommend*
Protein or salt restriction No effect No
1. Prevention

0.01 0.1 0.2 0.5 1 2 5 10
Progesterone 0.21 (0.03, 1.77)
Nitric oxide donors and precursors 0.83 (0.49, 1.41)
Diuretics 0.68 (0.45, 1.03)
Antiplatelets 0.81 (0.75, 0.88)
Antihypertensives v none 0.99 (0.84, 1.18)
Marine oils 0.86 (0.59, 1.27)
Magnesium 0.87 (0.57, 1.32)
Garlic 0.78 (0.31, 1.93)
Energy/protein restriction 1.13 (0.59, 2.18)
Isocaloric balanced protein supplementation 1.00 (0.57, 1.75)
Balanced protein/energy intake 1.20 (0.77, 1.89)
Nutritional advice 0.98 (0.42, 1.88)
Calcium 0.48 (0.33, 0.69)
Antioxidants 0.61 (0.50, 0.75)
Altered dietary salt 1.11 (0.46, 2.66)
Rest alone for normal BP 0.05 (0.00, 0.83)
Exercise 0.31 (0.01, 7.09)
Bed rest for high BP 0.98 (0.80, 1.20)
Ambulatory BP
1
4
4
43
19
4
2
1
2
1
3
1
12
7
2
1
2
1
0
128
170
1391
33439
2402
1683
474
100
284
782
512
136
15206
6082
631
32
45
228
0
Relative Risk (95% Confidence Interval)
RR (95% CI)Intervention No of RCTs No of women
Primary Prevention of PE
1. Prevention

Potential Impact ofCalcium
Calcium reduces PE by 48%
Potential of universal calcium supplementation: Prevent 21,500
maternal deaths Reduce DALYs
by 620,000
Source: Bhutta et al., Lancet, 2008
1. Prevention

Preventing PE: Calcium
Study Hofmeyr et al., 2010 (Cochrane)
Design 13 studies, most used 1.5–2g of calcium/dayMajority included: low-risk (n=15,143); low dietary calcium intake (n=10,678)
Results Reduced risk of: High blood pressure (35%)—greater for high-risk, low baseline calciumPE (31–65%)—greater for high-risk and low baseline calcium Preterm births (24%)—greater for high-risk (55%) Composite outcome maternal death or serious morbidity (20%)
No overall effect on stillbirth or neonatal death before hospital discharge
Supplementation (≥1g/day) halves the risk ratio of PE Greatest among women who are high risk or have low dietary calcium
intake No side effects reported
1. Prevention

Cochrane 2009: Calcium & PE
Source: Hofmeyr GJ, Lawrie TA, Atallah AN, Duley L, Cochrane Database Syst Rev. 2010
1. Prevention

Preventing PE: Calcium, WHO Reproductive Health Library, 2010
Useful in low-resource settings Women with low habitual calcium intake appeared to
benefit more No adverse effects, relatively safe Supports Cochrane findings calcium supplementation (>1
g/day) during pregnancy reduced risk, but interpret results with caution: High BP Half as likely to get PE
No evidence of significant difference for: Maternal outcomes (proteinuria, severe PE, eclampsia, maternal
death) Perinatal/neonatal (preterm birth, LBW, SGA, stillbirth or death
before discharge from hospital
greatest for women at high risk for PE; low baseline dietary calcium
Source: RHL Commentary by Palacios C and Pena-Rosas JP, 2010
1. Prevention

Daily Calcium Intake
472
346 363
499 498
352
860
0
500
1000
1500
World DevelopedCountries
Developingcountries
Africa Latin America Near East Far East
Minimum daily calcium intake, Adult WRA (1000−1200 mg/day)
Minimum daily calcium intake, Pregnant Women (1300−1500 mg/day)
Source: Calcium and Prevention of Pre-Eclampsia: Summary of Current Evidence, Monitoring, Evaluation and Research Task Force of
the PE/E working group 2010
1. Prevention

Calcium & Iron
Evidence (2005) Added calcium reduced the
initial uptake of heme iron by 20%
Reduced total iron absorbed by 25%
Nonheme iron absorption not significantly affected
“the long-term use of dietary calcium supplements… may further increase the risk of iron deficiency in women who are having difficulty in meeting their iron requirements.”
Implications (2010) Consider bioavailability of
calcium from supplements: Solubility, size of the dose Interacts with iron, zinc,
magnesium and phosphorus Inhibits iron absorption in a
dose-dependent and dose-saturable fashion separate time during the day
from daily iron+folic acid supplementation
Sources: Roughead, Z; Zito CA, Hunt JR 2005; RHL Commentary by Palacios C and Pena-Rosas JP, 2010
Photo
cred
it: Paul G
eor, w
ww
.sxc.h
u
1. Prevention

0 50
100 150
200 250 300 350 400 450 500
0.94 0.95 0.96 0.97 0.98 0.99
Effectiveness (proportion free of pre-eclampsia
Cos
t per
wom
an(
UK
£ 2
005)
No test, calcium to all
Source: Meads et al., Health Technol Assess. 2008
1. Prevention
Cost-effectiveness to Predict and Prevent PE: Test & Treatment
Second most cost-effective 'test-treatment' combination=Calcium supplementation to all women without any initial testing
Cost of an average case of PE approximately 9000 UK £

Preventing PE: Low-Dose Aspirin
Study Duley L et al., 2007 (Cochrane)
Bujold et al., 2010
Design 59 trials, n = 37,560 women, antiplatelet agents use
34 trials of women “at risk”: 12 at ≤16 weeks gestation; 22 after
Results Reduced risk of: PE (17%) SGA births Fetal, neonatal & infant deaths (14%)
Higher doses >75 mg of aspirin per day)
<16 weeks significant decrease: PE Severe PE IUGR Preterm birth
Daily prevents PE and IUGR for women at moderate or high-risk for PE
Greater benefits if started earlier in pregnancy (<16 weeks)
1. Prevention

Preventing PE: Vitamins C & E
Oxidative stress = Underlying mechanism for PE/E? Vitamins C & E for pregnant women at high-risk for PE Communities at risk of poor nutritional status in
developing countries 14–22 weeks gestation, daily supplements of vitamin
C (1000mg) & E (400 iu), n = 1365 Did not prevent PE, eclampsia, gestational
hypertension, LBW, SGA or perinatal deathsSource: Villar J et al., BJOG 2009
1. Prevention

Preventing PE: Vitamin D
Deficiency in pregnancy: Associated with adverse maternal and fetal outcomes Worldwide epidemic (18–84%)
Linkage to calcium absorption which increases during pregnancy, peaking in the third trimester
Recent studies found: Vitamin D deficiency <22 weeks is an independent predictor
of PE Vitamin D plus calcium supplementation started at 20–24
weeks significantly reduced BP but not PE Daily vitamin D intake (10–15 g/day) in Norway reduced the
adjusted risk for PE by 29% when adjusting for maternal BMISource: Haugen M et al., Epidemiology 2009; Mulligan et al., Am J Obstet Gynecol. 2010
1. Prevention

Detecting Pre-Eclampsia
No clinically-useful screening test to predict PE in either high-risk or low-risk groups (2004) Doppler ultrasonography 24-hour ambulatory blood pressure Placental and fetal peptides Renal dysfunction-related tests Endothelial and oxidant stress dysfunction-related tests
Ideal predictive test: Simple, innocuous, rapid, inexpensive, reproducible, and
noninvasive Easy to perform early in pregnancy
Source: Conde-Agudelo A, Villar J, Lindheimer M. Obstet Gynecol. 2004
2. Detection

Detecting Pre-Eclampsia: Measuring BP
Hypertension 10% of pregnancies, >20 weeks Diastolic BP 90 mm Hg
Most common: high BP before proteinuria
WHO ANC Guidelines 4 ANC visits/pregnancy BP history and measurement at each
visit Accuracy
Significant training needed to do BP well Robust and maintained equipment
Photo
cred
it: Sheena C
urrie
2. Detection

Detecting Pre-Eclampsia: Proteinuria
Hypertension with proteinuria associated with poorer maternal and perinatal outcomes
Proteinuria among women with: Higher antenatal BP Deliver earlier More often require operative delivery
Magnitude of proteinuria is a poor predictor of the major maternal and fetal complications
Available tests: Urine dipstick test: Rapid, simple Boiling: Not feasible in high volume
sites Esbach: time-consuming, inpatient
Photo
cred
it: Danie
l A
nto
naccio
Source: Thornton CE et al., Clin Exp Pharmacol Physiol 2010; Thangaratinam S et al., BMC Med. 2009
2. Detection

Dipstick Urine Testing for Protein
Limited in reliability, sensitivity, specificity, and predictive value False negative rate of 48.6% during
ANC screening in South Africa—missed a significant number of patients with proteinuria
Widely used Only test available in low-income
and middle-income countries
Source: Steegers EA et al., Lancet. 2010; Gangaram R, Ojwang PJ, Moodley J, Maharaj D. Hypertens Pregnancy. 2005
Photo credit: D
aniel Antonaccio
2. Detection

Components of ANC in Africa: BP Measurement and Urine Analysis
0
10
20
30
40
50
60
70
80
90
100
Blood pressure measured Urine sample taken Burkina Faso-2003 Ethiopia 2005 Ghana 2003 Kenya 2003 Liberia 2007Malawi 2004 Nigeria 2003 Rwanda 2005 Senegal 2005 Tanzania 2004Uganda 2006 Zambia 2007 Egypt 2005
Source: DHS, years as noted above
2. Detection
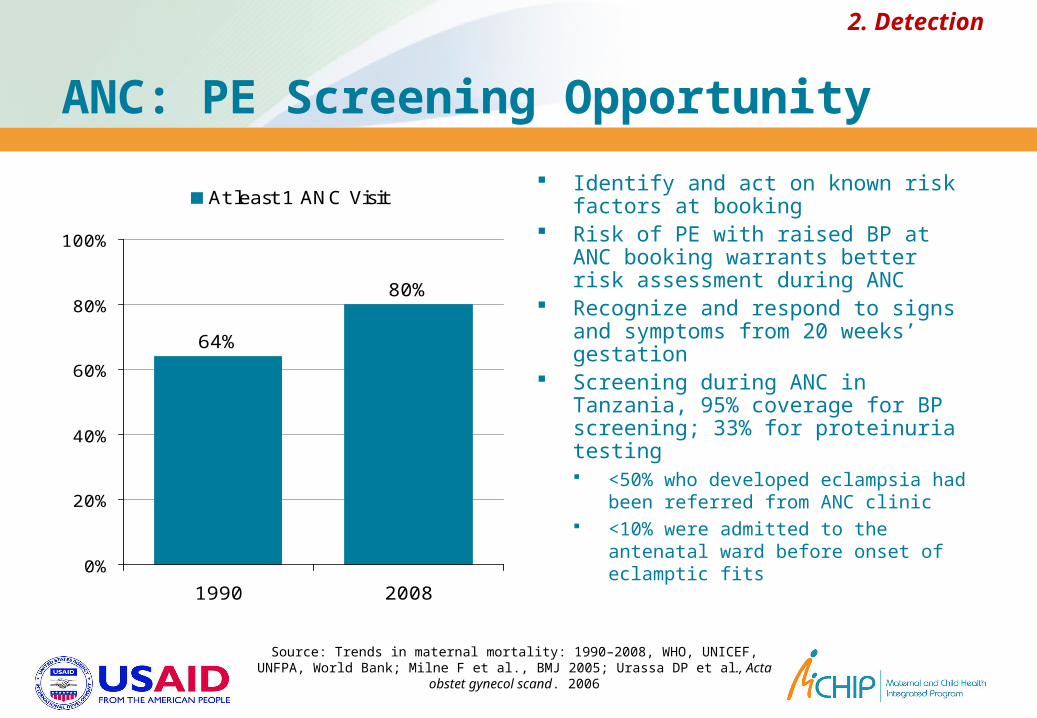
ANC: PE Screening Opportunity
64%
80%
0%
20%
40%
60%
80%
100%
1990 2008
At least 1 ANC Visit Identify and act on known risk factors
at booking Risk of PE with raised BP at ANC
booking warrants better risk assessment during ANC
Recognize and respond to signs and symptoms from 20 weeks’ gestation
Screening during ANC in Tanzania, 95% coverage for BP screening; 33% for proteinuria testing <50% who developed eclampsia had
been referred from ANC clinic <10% were admitted to the antenatal
ward before onset of eclamptic fits
Source: Trends in maternal mortality: 1990–2008, WHO, UNICEF, UNFPA, World Bank; Milne F et al., BMJ 2005; Urassa DP et al., Acta obstet gynecol
scand. 2006
2. Detection

Managing PE/E
Anticonvulsants—magnesium sulfate Antihypertensives Timed delivery Clinical monitoring and vigilance
Diazepam Lytic Cocktail Rectal Avertinx x x
3. Management

Magnesium Sulfate: Treat Eclampsia
Collaborative Eclampsia Trial,1991–1992, 27 centers in 9 countries, n =1680
Compared 3 most popular treatments Magnesium sulfate Diazepam Phenytoin
Magnesium sulfate had a 52% and 67% lower recurrence of convulsions than diazepam and phenytoin respectively
Source: The Eclampsia Trial Collaborative Group Lancet 1995
3. Management

Magnesium Sulfate: Treat Severe PE & Prevent Eclampsia
Magpie Trial, 2002, 10,000 women, 33 countries
Reduced the occurrence of eclampsia by 58% Reduced maternal deaths by 46% (not
significant) No evidence of substantive harmful effects in
the short-term Increased flushing (side effect) by 19% Increased risk of Cesarean section by 5%Sources: Magpie Trial Collaboration Group Lancet. 2002
3. Management

Magnesium Sulfate & ReducedMaternal Mortality from PE/E
19%
11%
8%
8% 8%
0%
20%
40%
60%
80%
100%
2002 2003 2004 2005 2006
% o
f M
agnesi
um
Sulfate
Use
d
0%
5%
10%
15%
20%
25%
Case
fata
lity
rate
% MgSO4 use Case fatality rate
Magnesium Sulfate Use in Purulia, West Bengal, India, 2002–2006
3. Management

Preventing Recurrent Convulsions
Compared magnesium sulphate and diazepam
7 trials, 1441 women Reduced:
Recurrence of convulsions Maternal mortality Apgar scores <7 at 1 and 5
minutes
Other reviews confirm magnesium sulfate better than phenytoin or lytic cocktail
Source: Duley L, Henderson-Smart D. Cochrane Database Syst Rev. 2003
Magnesium sulfate saves more mothers’ lives than diazepam
when given for eclamptic fits.
For every 7 women treated with
magnesium sulfate (vs diazepam),
1 case of recurrent convulsions prevented
3. Management

Magnesium Sulfate and the Neonate
Better outcomes for babies of mothers who received magnesium sulfate for eclampsia (than diazepam or phenytoin) Greater vigor of the babies (5 minutes after birth) Lower chances of a long hospital stay in an
intensive care unit Fewer neonatal admissions to a special care unit Shorter duration of stay (in days) in the neonatal
care unit Fewer neonatal deaths
Source: Duley et al., 2003a
3. Management

Immediate Treatment: Severe PE/E
Severe PE/E patients who received the loading dose before referral: Reduced number of
convulsions Controlled convulsions Shortened time to full
consciousness Reduced maternal
mortality and stillbirths Loading dose useful at
home births and peripheral facilities
5%
18%
77%
0
50
100
150
200
<6 hours 6-12 hours >12 hours
# m
ate
rnal death
s
0%
20%
40%
60%
80%
100%
% m
ort
alit
y
# maternal deaths % mortality
Source: Rashida et al., 2004
Seizure to Treatment Interval
3. Management

Immediate Treatment: Eclampsia
The sooner treatment starts, the better the survival rates
Treatment is relatively simple if instituted immediately Magnesium sulfate Antihypertensive Delivery
Delayed treatment especially beyond 2 hours requires intensive care for shock: DIC, renal shutdown, respiratory
failure, electrolyte disturbance, sepsis, pneumonia, multi organ failure
Even in best centers, mortality is high
Ensure magnesium sulfate loading dose
IM at the most peripheral
healthcare facilities—including for
homebirth.
It maybe all that you need for safe
transfer.
3. Management

Standard Magnesium Sulfate Regimens
1. IV: 4 g loading dose over 10 to 15 minutes followed by infusion of 1g/hour over 24 hours
2. IM: 4 g IV and 10 g IM as loading dose followed by5g IM every four hours for 24 hours
Source: Duley L, Matar HE, Almerie MQ, Hall DR. Cochrane Database Syst Rev. 2010
3. Management

Innovations for Low-resource Settings
1. Springfusor pump2. Pre-packaged kits3. Simplified regimens
Minimum effective dose Alternative routes of
administration (IV or IM) Duration of therapy
Source: Duley L, Matar HE, Almerie MQ, Hall DR. Cochrane Database Syst Rev. 2010
3. Management
Springfusor® syringe infusion pump

Single Dose for Treatment ofEclampsia: Bangladesh
A randomized trial, 401 patients Efficacy of loading dose vs. standard regime Recurrent convulsion rate 4% vs 3.5% Case fatality rate 4.5% vs 5% Better outcomes for women receiving a loading dose
at the community level before referral to a hospital (compared to those who received their loading dose in the hospital) Single loading dose sufficient Possible to treat—even at home
3. Management

Magnesium Sulfate: Challenges
1. No policies to promote use: Lack of guidelines mandating the use Not on national essential drugs list
2. No information: if in national guidelines, not widely disseminated or mandatory
3. Available only at highest-level facilities because of perceived need for close monitoring
4. Health workers are commonly not trained or authorized to administer magnesium sulfate; lack confidence and knowledge
5. Rare and inexpensive=no incentive for drug companies6. Inconvenient packs of 500–1000 mL; only 250 mL needed
Source: Reducing eclampsia-related deaths—a call to action, the Lancet, 2008
3. Management

PE/E Management: Antihypertensives
Reduce maternal risk without harming the fetus Help extend the pregnancy to improve fetal maturity
and outcomes. Indicated when the diastolic pressure is >110 mm Hg
Aim to bring it to 90–100 mm Hg to prevent cerebral hemorrhage
No clear choice of drugs Labetolol, hydralazine, and nifedipine currently widely
recommended
Once severe PE or eclampsia is diagnosed, at least the first dose of anti-hypertensive medications prior to transfer
3. Management

Managing PE/E: Timed Delivery
Induction of labor Associated with improved maternal outcome:
• Mild gestational hypertension• >37 weeks gestation
WHO Guidelines• Severe PE: Deliver <24 hours• Eclamptic convulsions/fits: Deliver <12 hours
Expectant management with early onset severe PE Gained a mean of 11 days gestation with improved
perinatal and neonatal survival rates Should not preclude timely delivery—the only
definitive cureSources: Steegers EA et al., Lancet. 2010; Sibai BM, Barton JR Am J Obstet Gynecol. 2007
3. Management

On the Horizon: 2003…2011?
“The technologies identified 5 years ago continue to be the key issues”
Nutritional supplements to prevent PE/E Antiplatelets to prevent PE/E Methods for early detection of PE/E or
elevated risk for PE/E Scaling up use of magnesium sulfate for
both prevention and treatment of eclampsiaSource: Tsu and Coffey, BJOG, 2009
3. Management2. Detection
1. Prevention