uncovering red flags in physician contracts
TRANSCRIPT

1
Uncovering Red Flags in Physician Contracts
An MD Ranger On-Demand Educational Video

2
Objectives:
• Why identifying red flags in physician agreements is
important
• Identifying organizational behaviors and culture that
could lead to risky deals
• Finding risky elements in physician agreements

But first, a disclaimer
• MD Ranger doesn’t give legal advice
• Physician agreements should always be reviewed by
an attorney (or two)
• All matters regarding potential legal/compliance
issues should go to counsel
• A formal review and approval process is foundational
to compliance
3

Physician contracts across the
organization
• It’s likely your facility has dozens, if not hundreds, of
financial relationships with physicians
• These personal services agreements may include
emergency call coverage, medical directorships,
administrative positions, hospital-based services,
diagnostic test reading fees, leadership and hospital-
based clinics
4

Physician payment rates regulated to
prevent fraud and abuse
• Stark Law limits physician self-referrals
• Anti-Kickback Statute prohibits paying for or
incentivizing referrals
• False Claims Act allows government to pursue
reparations for claims made while provider violated
either of above two laws
• Whistleblowers are often the source of investigations
5

Penalties steep for non-compliance
• Stark Law: single civil violation could result in a fine
of up to $15,000 for each service, plus overpayment
obligation and potential for high civil monetary
penalties assessment
• AKS: single criminal violation could result in a fine of
up to $25,000 for each instance (bill, encounter,
payment, etc.) and imprisonment of up to five years,
and, even absent conviction, violators may face
exclusion from federal health care programs.
• False Claims Act: amplifies above penalties
6
Identifying red flags is important
because
• Physician relationships key to running a successful
healthcare organization
• Financial and legal risks of having non-compliant
agreements huge
• Ensuring accurate documentation and approval
process for all physician agreements should be
central component of physician contracting
compliance programs
7

Risky Organizational Behaviors
8

Compliance-oriented culture?
• Some organizations have a strong
compliance-oriented culture, others do not
• If you notice your organization commonly
behaves in one or more ways that we’ll
discuss, you could be at greater risk for non-
compliant physician agreements
9

Assuming you must pay physicians
when they ask
• Strong physician relationships are key to a successful
organization and they promote clinical excellence
• However, not all payments are commercially
reasonable
• Establish both commercial reasonableness and a
rate at FMV
• Always explore alternative ways to compensate
10

Negotiating consistently high rates
with physicians
• As you review physician contracts, note how many
contracts fall above the 75th percentile
• There could be good reasons why several contracts
are above the 75th or even the 90th percentile, but
paying at this range should not be standard practice
• Also, benchmarks can change, so be careful setting
rates at the edge
11

Spending more in aggregate on
physician contracts
• Non-employed physician contracts are a sizable
chunk of a hospital’s operating budget, usually falling
between 4-6% of total operating expenses
• Use benchmarks to compare your organization’s
physician spending to peers, and see if you are
average
• Above average payments could indicate potentially
non-compliant agreements
• Checking into high spending is good financial
management
12
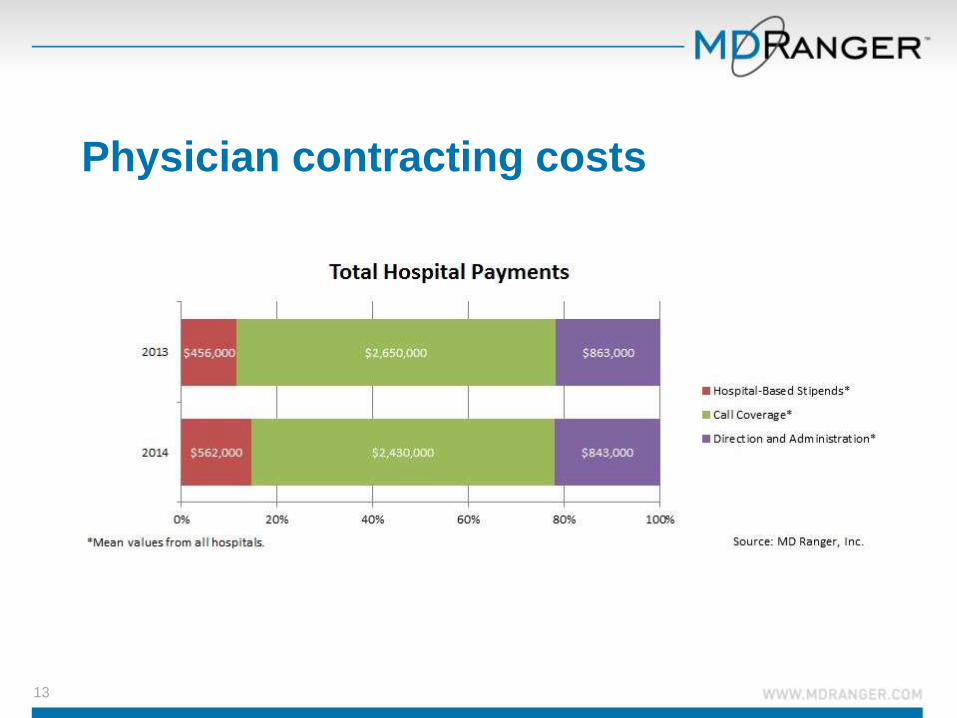
Physician contracting costs
13

Thinking your hospital is exceptional
• All hospitals are different, yet not so very different
that comparing like organizations isn’t helpful.
• Benchmarks shouldn’t be the end-all, be-all, but they
can be useful to understand how you compare to
peers
• Beware of overly-defensive reactions to benchmarks
at your organization
14

Physician Contract Attributes:
What’s Risky
15

The service might not be commercially
reasonable
• Just because you are paying a
physician for a service doesn’t
necessarily mean it’s commercially
reasonable
• Review commercial reasonableness
documentation during audit to ensure
argument still holds
• No documentation? Use MD Ranger
data to get a gut check• Percent paying
• Payment rates
• Number of positions
• Overall service payments
16

No proof of FMV
• All physician services agreements, in order to be
compliant, must have documentation that payments
are fair market value
• Likewise, all payments must be commercially
reasonable
• Lack of supporting documentation could mean that
the payment is not warranted or too high
• FMV documentation could be:• High quality market data
• Cost valuation
• Evidence of extraordinary efforts or circumstances17

Payments above the 75th percentile
with no justification/documentation
• Payments under the 75th percentile are generally considered
within FMV; however, your organization could have a different
policy regarding market ranges
• Many organizations use the median since it gives room for
growth or changes in benchmarks at contract renewal
• Typically it’s okay to have a few agreements above the 75th or
even the 90th percentile, if there is reasonable justification
• High payments with no or poor justification should be analyzed
further
18

Expired contracts
19
• Expired contracts mean that you do NOT have a
contract in place with the physician and you are
technically violating Stark if you continue to pay
• Remember: contract terms must be set in advance
• Calendar contract expirations and begin
renegotiations early (at least 90 days)

Payments with no contracts
• Cross check all payments to physicians from your AP
department as part of routine audits
• Payments to physicians with no contract in place is
extremely risky and is a violation of Stark, like an
expired agreement
20

Undocumented non-monetary
payments
21
• Are you providing non-monetary payments to
independent physicians that exceed the cap? • Parking spaces?
• Meals?
• Electronic health records?
• Overhead from charity events involving doctors?
• Joint marketing?
• Office artwork?
• Technology?
• Infrastructure?
• ….?

The service is not described in detail
on the contract
• Don’t forget important details, like number of hours in
administrative agreements
• Record keeping for time and performance of duties
• When in doubt, spell it out
22
Lack of time cards or call sheet
• Likewise, if no time cards or call sheets exist, your
red flag should fly
• Time cards are key for administrative contracts given
that physicians are typically paid hourly or monthly
based on a minimum and/or maximum number of
hours
23

Too many positions for a single
service
• Some medical directorships might need several
physicians serving in administrative roles (cardiology
is a good example)
• Many do not
• If you have more than one medical director per
service, investigate commercial reasonableness
• MD Ranger’s number of administrative positions
report can help!
24

Multiple contracts/payments to a
single provider or group
• Though payments might be warranted, check out
physicians or groups that receive multiple payments
• Compliance concerns mount when payments mount
25