ultrasound in liver diseases · 31 liver cirrhosis ultrasonographic signs in more than 2/3 of cases...
TRANSCRIPT

1
Ultrasound in liver diseases
Geir Folvik, MD
Division of Gastroenterology
Department of Medicine, Haukeland University Hospital
Bergen, Norway
25. november 2019

Agenda
Benign liver diseases
– Benign focal liver lesions
– Fatty liver disease
– Liver cirrhosis
– Other benign liver disorders
Malignant liver diseases
– Hepatocellular carcinoma
– Cholangiocarcinoma
– Liver metastases
– Lymphoma
2

3
Benign liver diseases

4
Hemangioma
most common benign tumour of the liver (prevalence 5-10%)
small (< 2-3 cm)
– homogeneous
– hyperechogenic lesion
– well defined, often with irregular margins
– often found in a subcapsular or perivascular position
most often discovered by coincidence
larger hemangiomas can be atypical with heterogeneous echogenicity
typical vascular pattern
– peripheral nodular arterial enhancement followed by centripetal filling
contrast-enhanced ultrasonography(CEUS) and MRI > CT

5
Hemangioma

6
Hemangioma
typically peripheral nodular contrast
enhancement on CEUS
centripetal fill-in

9
Focal nodular hyperplasia/ Adenoma
FNH– second most common benign liver tumour (incidence of 1-3%)
– most often discovered by coincidence
– often almost isoechoic with a central stellate scar
– non-encapsulated, but well defined
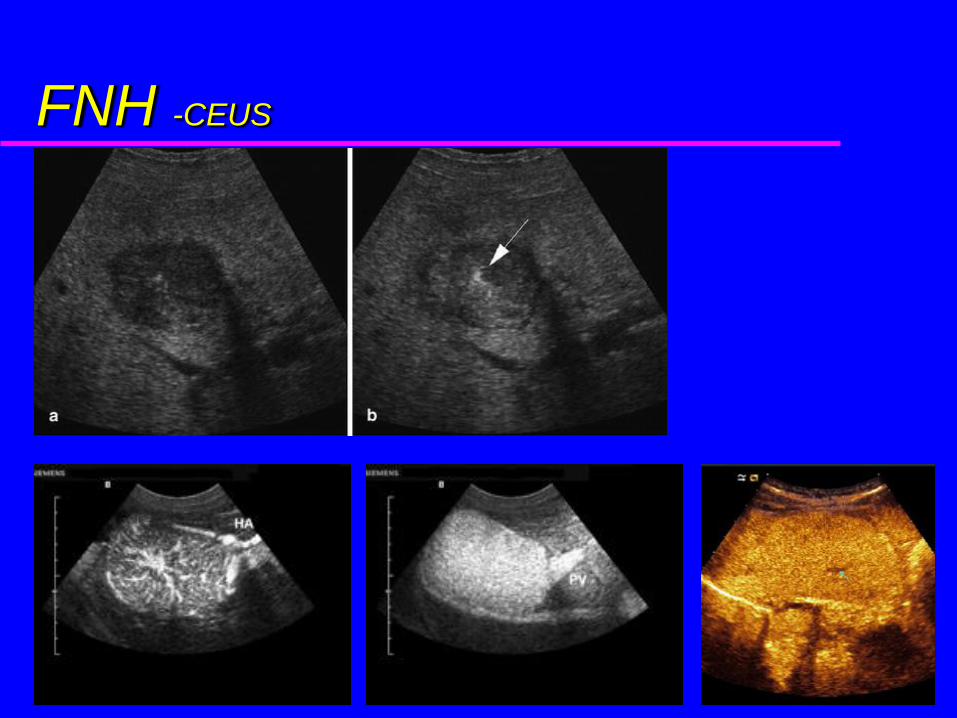
– typical centrifugal vascular filling to the periphery in the arterial phase on Color Doppler,CEUS, CT and MRI
Liver cell adenoma– adenomas less frequent than FNH
– encapsulated
– larger adenomas often inhomogeneous due to bleeding, necrosis and fibrosis
– RUQ pain due to mass effect or bleeding
– CEUS
– biopsy seldom indicated

10
FNH
11
FNH -CEUS

12
FNH -CEUS

15
Adenoma

16
Adenoma

17
Liver cysts
ultrasound is highly accurate in diagnosing liver cysts
anechoic with a clear posterior demarcation (but no wall)
posterior enhancement
often round in shape and smooth
occasionally RUQ pain due to mass effect or bleeding
polycystic liver disease– autosomal dominant disorder
– often multiple renal cysts (>50%)
– variation in size and shape
– hepatomegaly, cholestasis and portal hypertension (PHT)

18
Liver cysts

19
Liver cysts

20
Polycystic liver disease

21
Liver abscess
cystic pattern on ultrasound
spherical, oval or slightly irregular echo-poor lesions
often contain echogenic material including bubbles of gas
abscess wall more irregular than in simple cysts
fever, leucocytosis, CRP elevation and elevated LFT`s
ultrasound for percutaneous abscess drainage

22
Liver abscess

23
Liver abscess
CEUS

24
Lipoma and Fatty liver disease
Lipoma– a highly reflective hyperechogenic tumour with sharp
demarcation (”very bright”)
Fatty liver disease– steatosis or diffuse fatty liver -hyperechogenic liver
– focal fatty infiltration -hyperechogenic area
– in ”focal sparing” you will find a hypoechogenic area or lesion in a diffuse fatty liver

25
Lipoma -US og CT

26
Fatty liver ALCOHOL
NAFLD (obesity/ DM/ hyperlipidaemia)
drugs/ toxic substances
TPN
pregnancy
malnutrition/ bypass surgery
inborn errors of metabolism (”metabolic” diseases)
hepatomegaly
hyperechogenic with fine, closely packed echoes/ ”bright liver”
blood vessels and diaphragm often less distinct
increased attenuation => reduced visualisation ”in depth”
sensitivity 80-100% (depends of severity)

27
Focal fatty infiltration
hyperechogenic area
vessels are normal without displacement
no mass effect
can respect anatomical margins

28
Steatosis

29
Fatty liver with ”focal areas of sparing”

30
Fatty liver with ”focal areas of sparing”

31
Liver cirrhosis
ultrasonographic signs in more than 2/3 of cases
increased echogeneity (increased reflection due to fibrosis)
coarse and irregular echo-structure
portal vein walls often not defined
irregular contour because of surface nodularity -Lelio et al. Radiology 1989
– especially with high-frequency transducers and ascites
atrophy of the right lobe and hypertrophy of the caudate lobe
large regenerative nodules (DD: metastases/ tumours)

32
Liver cirrhosis
hepatic veins: often flattened flow-curve
thickened and layered wall of the gallbladder
ascites (Morrison`s pouch)
portal hypertension (PHT)
– alteration in or reversal of portal vein flow
– portal vein diameter increase in size to > 13-15mm
– splenomegaly
– collaterals/ recanalized paraumbilical vein
increased risk of HCC
– US screening +/- AFP every 6-12 months?

33
Liver cirrhosis

34
Liver cirrhosis

35
Enlarged caudate lobe

36
Flow-curve of the hepatic veins
Cirrhosis
Normal

Portal hypertension
Dilated portal vein
Reversed flow in the portal vein Open umbilical vein

38
Other benign disorders congestive liver failure
acute viral hepatitis
cholestatic liver disease
hematomas
regenerative nodules in cirrhosis
hydatid disease (echinococcal cysts)
amoebic abscess –hypoechogenic (history!)
schistosomiasis
Caroli`s disease
biloma (bile leakage)
granulomas usually not visualised

39
Congestive liver failure
congestive heart failure
dilatation of the hepatic veins
dilatation of vena cava
– compression/ Valsalva
hepatomegaly
ascites
portal hypertension
ESLD

40
PBC and PSC
periportal fibrosis
”end stage liver disease” (cirrhosis +/- PHT)
periportal lymph nodes
stones in the gallbladder or bile ducts
periportal fibrosis
irregular bile ducts
”end stage liver disease” (cirrhosis +/- PHT)
periportal lymph nodes
stones in the gallbladder or bile ducts

41
PBC

42
PSC

43
PSC

44
Stones in the gallbladder (PSC)

Hematoma– acute; highly reflective
– later; often inhomogeneous or hypoechogenic
– depends on age and severity of bleeding
45

46
Malignant liver diseases

47
Hepatocellular carcinoma
high prevalence in Africa and Southeast Asia (HBV and HCV)
strongly associated with cirrhosis and viral hepatitis
blood supply almost exclusively from an abnormal artery
< 2cm often hypoechogenic
large HCC (> 5 cm) often inhomogeneous with mixed echogenisity
– bleeding, necrosis and fibrosis
diffuse infiltration (DD: cirrhosis)
tumour thromb in the portal vein in about 35% using US
increased vascularity with Colour Doppler and CEUS
– ”feeding artery” and ”basket sign”
most often ”wash out” ( hypoechoic) in sinusoidal phase with CEUS
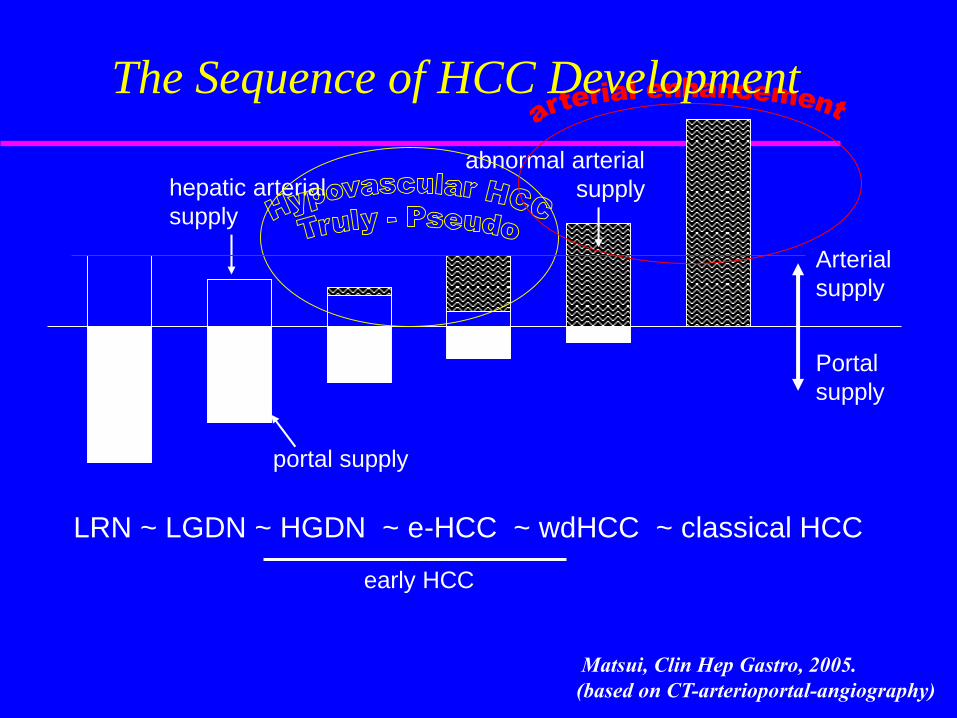
hepatic arterial
supply
abnormal arterial
supply
Arterial
supply
Portal
supply
portal supply
LRN ~ LGDN ~ HGDN ~ e-HCC ~ wdHCC ~ classical HCC
early HCC
Matsui, Clin Hep Gastro, 2005.
(based on CT-arterioportal-angiography)
The Sequence of HCC Development

49
Hepatocellular carcinoma

50
Hepatocellular carcinoma

51
Hepatocellular carcinoma

52
Hepatocellular carcinoma–”basket sign”

HCC -female 21 years of age with chronic HBV (Ethiopia 2012)
53

HCC -male 53 years of age with chronic HBV and
AFP=3000 (Ethiopia 2012)
54

55
??

56
Cholangiocarcinoma
often difficult to identify by ultrasound or other imaging techniques – ill-defined and often isoechoic
dilated bile ducts proximal to tumour– ”parallel sign”
solitary tumour with a slightly inhomogeneous echogenicity
localized thickening of the bile duct wall or just a ”major stricture”

57
Cholangiocarcinoma

58
Cholangiocarcinoma

59
Cholangiocarcinoma

60
Cholangiocarcinoma

61
Metastases
often multiple
hypo- and/or hyperechoic
halo
central necrosis
hypoechoic (wash-out) in parenchymal phase with CEUS

62
Metastases

63
Metastases

64
Liver metastases – from colorectal carcinoma

65
Metastases – from colorectal carcinoma

66
Liver metastases

67
Liver metastases
Late phase on CEUS

68
Lymphoma
– most often a diffuse infiltration (abnormal echogenicity?)
– seldom localized (10%)
– biopsy
– enlarged lymph nodes?

69
Diffuse malignant infiltration
myelomatosis/ plasma cell leukaemia– hepatomegaly