ueda2016 symposium - managing special population in diabetic patient,vildagliptin evidence - ayman...
TRANSCRIPT

Managing special population in diabetic patient ...
Vildagliptin Evidence
Ayman El Sebaie, MRCP(UK)
Head of Nephrology & Endocrinology
Department
IMC

Diabetes is a huge and growing problem, and the costs to society are high and
escalating
IDF Diabetes 6th Atlas. International Diabetes Federation.http://www.idf.org/diabetesatlas. Accessed Nov 19th, 2013

Worldwide prevalence of diabetes is high and is expected to increase to 592 million
by 2035
IDF Diabetes 6th Atlas. International Diabetes Federation.
http://www.idf.org/diabetesatlas. Accessed Nov 19th, 2013

Agenda
• Vildagliptin with renal impairment patients
• Vildagliptin with elderly and very elderly population
• Vildagliptin safety

Agenda
• Vildagliptin with renal impairment patients
• Vildagliptin with elderly and very elderly population
• Vildagliptin safety

CHF = Congestive Heart Failure; ESRD = End-Stage Renal Disease; MI = Myocardial Infarction; TIA = Transient Ischemic Attack
Adapted from http://www.eatlas.idf.org/complications Accessed August 15, 2005
Eyes
(retinopathy, glaucoma,
cataracts)
Brain and Cerebral
Circulation
(stroke, TIA)
Heart and Coronary
Circulation
(angina, MI, CHF)Kidneys
(nephropathy, ESRD)
Peripheral Nervous
System
(peripheral neuropathy) Peripheral Vascular Tree
(peripheral vascular disease,
gangrene, amputation)
Tissue Damage in Many Organ Systems Leads to Serious Long-Term Complications in T2DM

Russo E, et al. Diabetes Metab Syndr Obes. 2013; 6: 161–170.

ESRD: End- Stage Renal Disease
Luk AO, et al. Diabetes Care. 2014 Jan;37(1):149-57

*Per 100,000
http://www.worldlifeexpectancy.com/cau
se-of-death/kidney-disease/by-country/
accessed 2012 Oct.


GN: Glomerulonephritis
Rashad S. Barsoum. Kidney International Supplements (2013) 3, 164–166

A1 A2 A3
Normal to
mildly
increased
Moderately
increased
Severely
increased
<30 mg/g
<3 mg/mmol
30-300 mg/g
3-30 mg/mmol
>300 mg/g
>30 mg/mmol
• CKD is defined as abnormalities of kidney structure or function, present for >3
months, with implications for health and CKD is classified based on cause, GFR
category, and albuminuria category (CGA).
KDIGO Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int Suppl. 2013;3:136-150.
http://www.kdigo.org/clinical_practice_guidelines/pdf/CKD/KDIGO_2012_CKD_GL.pdf Accessed February 26, 2013
G1 Normal or high ≥90
G2 Mildly decreased 60-89
G3aMildly to moderately
decreased45-59
G3bModerately to
severely decreased30-44
G4 Severely decreased 15-29
G5 Kidney failure <15
GF
R c
ate
go
ries (
ml/
min
/
1.7
3 m
²)
Desc
rip
tio
n a
nd
ran
ge
Persistent albuminuria categories
Description and range
Green: low risk (if no other markers of kidney disease, no CKD); Yellow: moderately increased risk; Orange: high risk; Red, very high risk.
Prognosis of CKD by GFR
and Albuminuria Categories:
KDIGO 2012
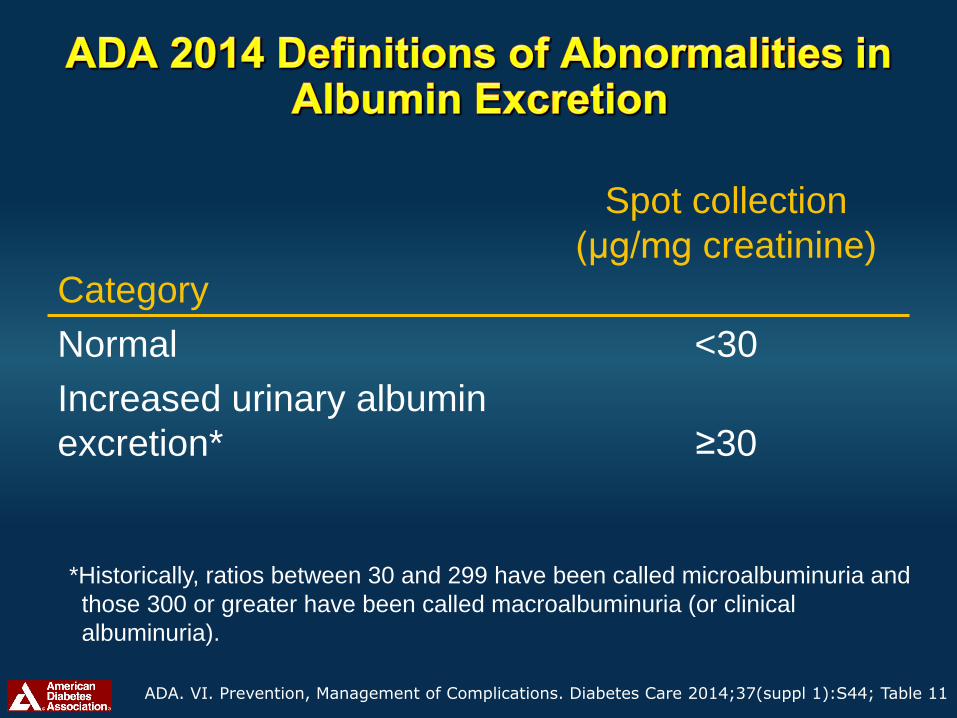
Category
Spot collection
(µg/mg creatinine)
Normal <30
Increased urinary albumin
excretion* ≥30
ADA. VI. Prevention, Management of Complications. Diabetes Care 2014;37(suppl 1):S44; Table 11
*Historically, ratios between 30 and 299 have been called microalbuminuria and
those 300 or greater have been called macroalbuminuria (or clinical
albuminuria).

Decreasing HbA1c Is a Real Challenge
With Renal Impairment Patients

Treat to target increases the risk of hypoglycemia in ACCORD, VADT and ADVANCE
1. ACCORD Study Group. N Engl J Med. 2008;358:2545–2559 2. Duckworth W, et al. N Engl J Med. 2009;360:129–1393. ADVANCE Collaborative Group. N Engl J Med. 2008;358:2560–2572
ACCORD1 VADT2 ADVANCE3
P <0.001
Even
ts (
%)
Standard Intensive
16
6
4
2
0
14
12
10
8
18
P <0.01
Standard Intensive
Even
ts p
er
10
0 p
ati
en
t-years
6
4
2
0
14
12
10
8
P <0.001
Standard Intensive
Even
ts p
er
10
0 p
ati
en
ts p
er
ye
ar
0.6
0.4
0.2
0
0.8
0.7
0.5
0.3
0.1

Hypoglycemia and Renal Impairment
• Longstanding type 2 diabetes in patients with advanced
kidney disease often requires insulin therapy.
• Insulin dosage is a real challenge in a renal impaired
population due to impaired catabolism and clearance of
insulin.
• The renal clearance of insulin shows little change if the
glomerular filtration rate (GFR) is above 40 mL/min, but it
falls precipitously with further progression of chronic kidney
disease, especially when GFR is less than 15–20 mL/min.
Lukashevich V, et al. Vasc Health Risk Manag. 2013;9:21-8.


Management of CKD in Diabetes
NICE Diabetes with Kidney Disease: Key Facts MARCH 2011

NICE Diabetes with Kidney Disease: Key Facts MARCH 2011

Russo E, et al. Diabetes Metab Syndr Obes. 2013; 6: 161–170.

SUs=sulfonylureas; T2DM=type 2 diabetes melllitus; *Requiring medical assistance or hospital admission
UK Prospective Diabetes Study Group. Diabetes.1995;44:1249–1258.
Cumulative Incidence of Hypoglycemia in T2DM over 6 Years in UKPDS
45
3.3
76
11.2
0
10
20
30
40
50
60
70
80
Sulfonylurea (n=922)
Insulin (n=689)
Sulfonylurea Insulin Sulfonylurea Insulin
Pati
en
ts (
%)
Any hypoglycema Major hypoglycemia*
HbA1c = 7.1% in all groups
70% increased risk
40% increased risk

Russo E, et al. Diabetes Metab Syndr Obes. 2013; 6: 161–170.
http://www.medscape.org/viewarticle/437273
http://www.elmhurst.edu/~chm/vchembook/604glycogenesis.html

National Kidney Foundation. KDOQI Clinical Practice Guideline for Diabetes
and CKD: 2012 update. Am J Kidney Dis. 2012;60(5):850-886.
~7.0%
to prevent or delay
progression of the
microvascular
complications of
diabetes, including
DKD
Not
<7.0%
in patients at risk
of hypoglycemia.
>7.0%
In individuals with
co-morbidities or
limited life
expectancy and risk
of hypoglycemia

Adapted from: Jindal A, et al. Endocrinol Metab Clin North Am. 2013 Dec;42(4):789-808
Diabetes indices and progresses
RI
RI increased risk of
hypoglycemia
Limited therapeutic
options Less control
Worsen of RI

CKD: Chronic Kidney Disease.
Jindal A, et al. Endocrinol Metab Clin North Am. 2013 Dec;42(4):789-808
Better glycemic and blood pressure control
Older oral hypoglycemic agents is either contraindicated or requires dosage adjustment in CKD
New medications for diabetes have been approved recently and many can be used safely in patients with CKD

Vildagliptin
Does it have evidence in diabetic renal
impaired patients !?!


Vildagliptin Use With Renal Impairment Patient
• Referring to EMA Recommendations and Locally
Approved Basic Prescribing Information:
EMA = European medical agency
Galvus Locally approved Basic Prescribing Information 2012



To assess long-term safety and efficacy of vildagliptin (50 mg qd) in
patients with T2DM and moderate or severe renal impairment (RI)
*Randomized: patients must remain on their current anti-diabetic therapy (stable dose for at least 4 weeks prior to visit 1) or remain untreated for the
duration of the study if patient is not on anti-diabetic therapy at study entry (unless patient meets criteria for rescue medication).
Total of 525 includes 10 patients with mild RI revealed during reclassification by MDRD method: 7 were randomized to vildagliptin, 3 to placebo, but
data from mild RI patients are not reported
1) Primary objective = safety and tolerability
2) Secondary objective = efficacy
(N=289) Vildagliptin 50 mg qd +
Placebo run-in plus
stable dose of current
therapy*
(N=226) Placebo +
24 weeks2 weeks
N=525
Adapted from Lukashevich V et al. Diabetes Obes Metab. 2011; 13:947-954
Adapted from W. Kothny,et al. Diabetes Obes Metab. May 2012
28 weeks double-blind treatment
current therapy (N=216)
current therapy (N=153)

-0.6
-0.2
-0.4
Moderate RI*
Vildagliptin 50mg QD
Placebo
Between-group Differance
-0.8
-0.1
-0.7
Severe RI*
Vildagliptin 50mg QD
Placebo
Between-group Differance
Duration :1 year
(p<0.0001)(p=0.005)
The overall safety and tolerability of vildagliptin 50 mg qd in patients with moderate
or severe RI was comparable with that of placebo.
Adapted from W. Kothny,et al. Diabetes Obes Metab. May 2012
RI: renal impairment
*Baseline in moderate and severe RI patient was 7.8% and 7.7% respectively
BL HbA1c BL HbA1c

-0.4
-0.7
Vildagliptin or Placebo Between-group difference
Moderate RI Severe RI
Hb
A1c A
dju
ste
d m
ea
n c
han
ge
(%)
fro
m b
ase
line
Duration :1 year
RI: renal impairment
Baseline in moderate and severe RI patient was 7.8% and 7.7% respectively
(p=0.005)
(p<0.0001)
Adapted from W. Kothny,et al. Diabetes Obes Metab. May 2012
(baseline=7.8%) (baseline=7.6%)

Moderate RI [n (%)] Severe RI [n (%)]
Event category
Vildagliptin 50
mg qd
(N=122)
Placebo
(N=89)
Vildagliptin
50 mg qd
(N=94)
Placebo
(N=64)
Any adverse event 103 (84.4) 76 (85.4) 80 (85.1) 56 (87.5)
Any serious adverse event 26 (21.3) 17 (19.1) 23 (24.5) 16 (25.0)
Any adverse event leading
to discontinuation6 (4.9) 5 (5.6) 9 (9.6) 4 (6.3)
RI, renal impairmentAdapted from W. Kothny,et al. Diabetes Obes Metab. May 2012

The percentage of patients achieving endpoint HbA1c <7.0% in the vildagliptin group (33/73
patients, 45.2%) was twice that in the placebo group (13/57 patients, 22.8%, P = 0.008).
Lukashevich V, et al. Vasc Health Risk Manag. 2013;9:21-8.
45.20%
22.80%
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
Insulin+ Vilda 50mg qd n=33/73 Insulin+ placebo n=13/57
Patients achieving endpoint HbA1c <7.0%
P = 0.008
post hoc sub-analysis of 24-week study

• A higher % of patients reported ≥ 2 events (72.7% with placebo versus 47.4% with vildagliptin).
• Severe hypoglycemia was reported at a similarly low rate in the two groups (2.0% with
vildagliptin and 2.6% with placebo).
47.40%
72.70%
0%
10%
20%
30%
40%
50%
60%
70%
80%
Insulin+ Vilda 50mg Insulin+ placebo
% of patients reported ≥ 2 events
2.00%
2.60%
0%
1%
1%
2%
2%
3%
3%
Insulin+ Vilda 50mg Insulin+ placebo
% of patients with severe hypoglycemia
Lukashevich V, et al. Vasc Health Risk Manag. 2013;9:21-8. post hoc subanalysis of 24-week study

Lukashevich V, et al. Vasc Health Risk Manag. 2013;9:21-8.

Vildaglitpin in managing T2D with renal impairment ...
Is goodoption for RI
patients
Provides effective glycemic control
Has low risk of
hypoglycimia

Agenda
• Vildagliptin with renal impairment patients
• Vildagliptin with elderly and very elderly population
• Vildagliptin safety
Optimizing the Management of T2D Patients....

Adapted from http://www.indexmundi.com/egypt/demographics_profile.html , https://www.cia.gov/library/publications/the-world-factbook/geos/eg.html , http://en.worldstat.info/World
accessed 22-2-2014

2013
≥60 Years
≤60 Years
International Diabetes Federation. Managing Older People with Type 2 Diabetes Global Guidelines.
http://www.idf.org/sites/default/files/IDF%20Guideline%20for%20Older%20People.pdf accessed 15-12-2013
2050
≥60 Years
≤60 Years
These changes present significant challenges to welfare, pension, and
healthcare systems in both developing and developed nations

• Diabetes-related complications are the major
causes of morbidity, disability and mortality in
older patients with type 2 diabetes:
• There is now overwhelming evidence that the
level and duration of glycemia influences the
development of diabetes-related complications
Sinclair 2004. Clinical guidelines for type 2 diabetes mellitus. EDWOP 2004
Microvascular: Neuropathy,Retinopathy,Nephropathy
Macrovascular: Cardiovascular disease, Stroke

Cost in US$ millions
Institutional care Outpatient careOutpatient medicines
and supplies
<45 years 45-64 years ≥65 years
American Diabetes Association. Diab Care 2008;31:596-615

• Advanced age
• Recent hospitalization
• Intercurrent illness
• Chronic liver, renal or
cardiovascular disease
• Endocrine deficiency
(thyroid, adrenal, pituitary)
• Loss of normal counter-
regulation
• Hypoglycaemic
unawareness
SU=sulfonylurea.
Adapted from Chelliah A, Burge MR. Drugs Aging. 2004; 21: 511–530.
I. Patient risk factors
• Poor nutrition or fasting
• Prolonged physical
exercise
• Alcohol (ethanol)
• Use of SU and / or insulin
• Drug interactions with SUs
III. Drug risk factors
II. Lifestyle risk factors

T2DM=type 2 diabetes mellitus.
Greco D, et al. Exp Clin Endocrinol Diabetes. 2010; 118: 215–219.
Decompensated
diabetes39%
Intercurrent
illness14%
Acute
cardiovascular events
13%
Chronic
complications of diabetes
17%
Severe
hypoglycaemia17%

Molecule with Smart Mechanism of Action

1Galvus Summary of Product Characteristics, Feb 2011, Section 4.5.
Vildagliptin is not metabolised by the
cytochrome P450 pathway1
Studies in healthy volunteers showed vildagliptin had no
clinically relevant pharmacokinetic interactions with
digoxin (Pgp substrate), warfarin (CYP2C9 substrate),
amlodipine, ramipril, valsartan or simvastatin1

Pooled safety and efficacy analysis of all randomised, double-blind
studies that:
• Dosed vildagliptin 50 mg twice daily
• Included patients ≥75 years
• Duration ≥24 weeks
• 10 studies were included, total n=12,326
No. patients receiving vildagliptin
<75 years ≥75 years
Safety
population
5984 132
Monotherapy Add-on therapy Monotherapy Add-on therapy
Efficacy
population2303 910 62 25
Vildagliptin is approved for 50 mg once or twice daily in combination with metformin or a TZD,
and vildagliptin 50 mg once daily in combination with a sulfonylurea.
Schweizer A, et al. Diabetes Obes Metab. 2011; 13: 55–64.

-1.1-1.2
-1.0
-0.8
-0.6
-0.4
-0.2
0.0
Ch
an
ge in
Hb
A1
c (
%)
fro
m b
ase
lin
e
n=
BL (%)=
25
8.5
*
Pooled analysis (24 weeks) of 3 add-on therapy studies, patients ≥75 years
HbA1c1
-0.2
-0.5
-0.4
-0.3
-0.2
-0.1
0.0
n=
BL (kg)=
Ch
an
ge in
weig
ht
(kg
)
fro
m b
ase
lin
e
25
82.8
Body weight1
n 31
Any events, n
(%)0 (0.0%)
Severe
events, n (%)0 (0.0%)
Hypoglycaemia2
Overall AEs, drug-related AEs and SAEs were all reported with a lower frequency in elderly patients receiving vildagliptin (133.9, 14.5 and 8.8 events per
100 SYE, respectively) than in elderly patients receiving comparators (200.6, 21.8 and 16.5 events per 100 SYE, respectively), and the incidence of
discontinuations due to AEs was similar in the 2 treatment groups (7.2 vs 7.5 events per 100 SYE, respectively). The incidences of AEs, drug-related AEs,
SAEs and discontinuations due to AEs were overall comparable between younger and older patients. The most notable difference was a higher incidence
of SAEs in the comparator group in patients ≥75 years vs <75 years.1Efficacy pool: all randomised, double-blind, controlled, parallel-group studies with duration ≥24 weeks and with patients ≥75 years. Only includes studies
with the approved dose of 50 mg twice daily. 2Safety pool: a pool of 38 Phase II and III studies (monotherapy and add-on therapy).
*P <0.05 vs baseline (within group). AEs=adverse events; bid=twice daily; BL=baseline; HbA1c=haemoglobin A1c; SAEs=serious adverse events.
Schweizer A, et al. Diabetes Obes Metab. 2011; 13: 55–64.

Vilda 50 mg bid
n=5984
Comparators
n=6041Vilda 50 mg bid
n=132
Comparators
n=169
Any AEs
n (%)147.9
4139 (69.2)
177.3
4174 (69.1)
133.9
86 (65.2)
200.6
114 (67.5)
Drug-related AEs
n (%)14.9
943 (15.8)
26.0
1325 (21.9)
14.5
18 (13.6)
21.8
24 (14.2)
SAEs
n (%)7.8
533 (8.9)
8.9
538 (8.9)
8.8
12 (9.1)
16.5
19 (11.2)
Discontinuation due to
AEs
n (%)
4.7
337 (5.6)
6.1
391 (6.5)
7.2
10 (7.6)
7.5
9 (5.3)
Deaths
n (%)0.3
24 (0.4)
0.3
21 (0.3)
0.0
0 (0.0)
1.7
2 (1.2)
AEs=adverse events; bid=twice daily; SAEs=serious adverse events; SYE-adj=subject year exposure-adjusted; vilda=vildagliptin.
Safety pool: a pool of 38 Phase II and III studies. Comparators group includes active comparator or placebo.
Schweizer A, et al. Diabetes Obes Metab. 2011; 13: 55–64.
Age <75 years Age ≥75 years

In this sub-analysis of data derived from a previously
described randomized, double blind, parallel-group, 24-week
study, 105 patients (50 randomized to vildagliptin 50 mg qd
and 55 to placebo) ≥ 75 years (mean age~78 years) with
T2DM and moderate or severe RI (mean baseline estimated
glomerular filtration rate~35 ml/min/ 1.73 m2) were included.
Schweizer, et al. Diabetes Ther. Experience with Vildagliptin in Patients ≥75 Years with Type 2 Diabetes and Moderate or Severe Renal Impairment.
2013 Dec;4(2):257-67.

(A) p<0.001 (between-group difference).
(B) p = 0.970 (between-group difference).
BL= baseline
Schweizer, et al. Diabetes Ther. Experience with Vildagliptin in Patients ≥75 Years with Type 2 Diabetes and Moderate or Severe Renal Impairment.
2013 Dec;4(2):257-67.

Vildagliptin in the elderly: summary
HbA1c=haemoglobin A1c; SUs=sulfonylureas; T2DM=type 2 diabetes mellitus. 1Adapted from Cowie CC, et al. Diabetes Care. 2009; 32: 287–294; 2Araki A, Ito H. Geriatr Gerontol Int. 2009; 9: 105–114; 3Schweizer A, et al. Diabetes Obes Metab. 2011; 13: 55–64.
VILDAGLIPTIN

Agenda
• Vildagliptin with renal impairment patients
• Vildagliptin with elderly and very elderly population
• Vildagliptin safety

Vildagliptin safety is well assessed in different meta analysis

Safety of Vildagliptin is Well Established
• In meta – analysis of 38 clinical trials include more than 14.000 patients vildagliptin shows no increased risk of:
•Pancreatitis-related AEs
•ALT / AST or Bilirubin elevation
•Renal AEs and SAEs in patients with normal renal function and mild renal impairment patients
• Infection and skin related adverse events
vs. comparators (placebo, insulin and other OAD)
Ligueros-Saylan et al. DIABETES, OBESITY AND METABOLISM Volume 12 No. 6 June 2010

Schweizer A, et al. Diabetes Obes Metab. 2010; 12: 485–494.

• About 40% of patients had ≥ 2 documented CV risk factors in
addition to T2DM:
– dyslipidaemia
– hypertension
– age ≥65 years
• Over 15% had a high CV risk status:
– defined as a previous history of CCV events in the
Standard MedDRA Queries of ‘ischaemic heart disease,
cardiac failure, ischaemic cerebrovascular conditions
and/or embolic, thrombotic events.
Schweizer A, et al. Diabetes Obes Metab. 2010; 12: 485–494.
Patient Characteristics

Vildagliptin: In more than 14,000 patients No Increased Risk for Adjudicated CV Events,
Relative to All Comparators
AEs=adverse events; bid=twice daily; CI=confidence interval; CV=cardiovascular; M-H RR=Mantel-Haenszel risk ratio; qd=once daily; vilda=vildagliptin. #Vs comparators (all non-vildagliptin treatment groups). All-study safety population.
‡Guidance for Industry: Diabetes Mellitus - Evaluating Cardiovascular Risk in New Antidiabetic Therapies to Treat Type 2 Diabetes, U.S. Department
of Health and Human Services Food and Drug Administration Center for Drug Evaluation and Research (CDER), December 2008.
Schweizer A, et al. DOM 2010 in press.
Vildagliptin Reference M-H RR
n / N (%) n / N (%) (95% CI)
Vilda 50 mg qd# 10 / 1393 (0.72) 14 / 1555 (0.90) 0.88 (0.37–2.11)
Vilda 50 mg bid# 81 / 6116 (1.32) 80 / 4872 (1.64) 0.84 (0.62–1.14)
Risk Ratio
Incidences and Odds Ratios for
Adjudicated CV Events by Treatment
Vildagliptin better Vildagliptin worse
0.1 1 10
#Meta-analysis of vildagliptin 50 mg bid data vs all comparators according to the methodology set
by the US Food and Drug Administration‡ [50 mg bid odds ratio = 0.84 (95% CI 0.62–1.14)].

• 9,599 patients were treated with GALVUS® (50 mg once or twice
daily), as either monotherapy or in combination with another
OAD or insulin
• >40% had 2 or more CV risk factors (hypertension,
dyslipidaemia or age ≥60 years for females or 55 years for
males)
• Nearly a fifth (18%) had high CV risk status*
• 27% of patients ≥65 years
• 38% of patients had longstanding T2DM (>5 yrs)
• Almost half (49%) obese (BMI ≥30 kg/m2)
• 41.3% had renal impairment
Mclnnes Meta Analysis - 2014
• A recent meta-analysis has extended the assessment of GALVUS® CV safety to
• 40 Phase III and Phase IV studies (N=17,446), including trials in high-risk patients,
such as those with heart failure or moderate/several renal impairment [McInnes 2014]

• Primary End Point :
– Occurrence of MACE (myocardial infarction,
stroke and CV death).
• Secondary End Point :
– Assessments of the individual MACE
components and HF events (requiring
hospitalization or new onset) .
McInnes G, et al. Diabetologia. 2014;57(Suppl. 1):Abstract (presentation number 891)

CV safety of vildagliptin: an adjudicated meta-analysis of 40 studies
Incidences and risk ratios for adjudicated MACE and its individual components*
Vildagliptin
n/N (%)
Comparators
n/N (%)
M-H RR
(95% CI)
MACE composite
endpoint83/9599 (0.86) 85/7102 (1.20) 0.82 (0.61–1.11)
Myocardial
infarction38/9599 (0.40) 35/7102 (0.49) 0.87 (0.56–1.38)
Stroke 24/9599 (0.25) 25/7102 (0.35) 0.84 (0.47–1.50)
CV death 25/9599 (0.26) 28/7102 (0.39) 0.77 (0.45–1.31)
• This updated, large meta-analysis continues to indicate that vildagliptin is not
associated with an increased risk for adjudicated MACE relative to comparators.
• It now includes more patients with advanced renal impairment or CV disease
history including heart failure
Vildagliptin better Comparator better
0.01 0.10 1.0 10.0 100.0

Incidences and risk ratios for adjudicated MACE* in various subgroups
Vildagliptin
n/N (%)Comparators
n/N (%)
M-H RR
(95% CI)
0.74 (0.52–1.05)64/3928 (1.63)57/5310 (1.07)Male
0. 1 1.0 10.0 100.00.01Vildagliptin better Comparator better
i) MACE in subgroups by age, gender and CV risk status
Gender
1.06 (0.61–1.85)21/3174 (0.66)26/4289 (0.61)Female
0.63 (0.42–0.95)50/5119 (0.98)39/7239 (0.54)<65 years
1.09 (0.70–1.71)35/1983 (1.77)44/2360 (1.86)≥65 years
1.01 (0.51–2.00)16/3609 (0.44)19/5167 (0.37)No
0.78 (0.56–1.09)69/3493 (1.98)64/4432 (1.44)Yes
0.93 (0.66–1.30)62/3836 (1.62)66/4391 (1.50)Studies ≥52 weeks
Age (years)
High CV risk status**
ii) MACE in subgroup of long-term studies
*MACE, major adverse cardiovascular (CV) events–non-fatal myocardial infarction, non-fatal stroke or CV death; **High CV risk status ‘yes’
includes patients with a previous history of CV events in the standard MeDRA Queries of ‘ischemic heart disease, cardiac failure, ischemic
cerebrovascular conditions and /or embolic thrombotic events, arterial’. Vildagliptin = 50 mg qd/bid; M-H RR, Mantel-Haenszel risk ratio.
Adapted from McInnes G et al. Poster no 891 presented at the 50th EASD Annual Meeting, Sep 15–19, 2014, Vienna, Austria.

Vildagliptin
n/N (%)
Comparators
n/N (%)
M-H RR
(95% CI)
Vildagliptin
50 mg od/bid41/9599 (0.43) 32/7102 (0.45) 1.08 (0.68–1.70)
Vildagliptin
50 mg od20/2201 (0.91) 19/2451 (0.78) 1.19 (0.63–2.26)
Vildagliptin
50 mg bid21/7398 (0.28) 24/6229 (0.39) 0.99 (0.55–1.77)
Vildagliptin was not associated with increased risk of HF: Pooled safety data from ~17,000 T2DM patients
• Incidences and risk ratios for adjudicated heart failure events*
In patients with T2DM†, incidences of adjudicated heart failure events (New onset HF
or HF hospitalization) were similar in the vildagliptin and comparator treatment
groups
Vildagliptin better Comparator better
0.01 0.10 1.0 10.0 100.0
M-H RR=Mantel-Haenszel risk ratio
Evans M, et al. Poster presented at 50th EASD Annual Meeting, Vienna, Austria, 15–19 September 2014;
Evans M, et al. Diabetologia. 2014;57(Suppl. 1):Abstract (presentation number 888)

Vildagliptin Safety: summary
VILDAGLIPTIN
