two distinct abnormalities in patients with c8 alpha-gamma
TRANSCRIPT

Two distinct abnormalities in patients with C8 alpha-gammadeficiency. Low level of C8 beta chain and presence ofdysfunctional C8 alpha-gamma subunit.
F Tedesco, … , V Agnello, J M Sodetz
J Clin Invest. 1990;86(3):884-888. https://doi.org/10.1172/JCI114789.
The sera from three C8 alpha-gamma deficient patients previously reported to have a selective C8 alpha-gamma defectwere analyzed by SDS-PAGE and Western blot using two polyclonal antisera to C8 alpha-gamma and a monoclonalantibody to C8 alpha. All three sera exhibited C8 alpha-gamma bands that dissociated into alpha and gamma chainsunder reducing conditions. Quantitation of the alpha-gamma subunit in these sera by a sensitive ELISA revealed anamount approximately 1% of that found in normal human serum. A similar assay performed with a specific antiserum toC8 beta showed unexpectedly low levels of C8 beta in these sera, which were confirmed by hemolytic titration of C8 beta.The remarkable differences between C8 alpha-gamma and C8 beta in the C8 alpha-gamma deficient sera was that inspite of their comparable immunochemical levels, C8 beta still exhibited functional activity whereas C8 alpha-gamma wastotally inactive. That the residual C8 alpha-gamma was inactive was also proved by its inability to show lytic bands in anoverlay system after SDS-PAGE and subsequent removal of SDS. The implications of these findings for a novel conceptof C8 deficiency are discussed.
Research Article
Find the latest version:
https://jci.me/114789/pdf

Two Distinct Abnormalities in Patients with C8t-'y DeficiencyLow Level of C8ft Chain and Presence of Dysfunctional C8a-y Subunit
F. Tedesco, L. Roncelli, B. H. Petersen, V. Agnello, and J. M. SodetzIstituto di Patologia Generale, Universita di Trieste, Trieste, Italy; Istituto per l'Infanzia, Trieste, Italy; Eli Lilly and Company andWishard Memorial Hospital, Indianapolis, Indiana 46202; Lahey Clinic Medical Center, Burlington, Massachusetts 01803 andENRMVeterans Administration Hospital, Bedford, Massachusetts 01730; and Department of Chemistry,University of South Carolina, Columbia, South Carolina 29208
Abstract
The sera from three C8a-"y deficient patients previously re-
ported to have a selective C8a--y defect were analyzed bySDS-PAGEand Western blot using two polyclonal antisera toC8a-y and a monoclonal antibody to C8a. All three sera exhib-ited C8a-'y bands that dissociated into a and y chains underreducing conditions. Quantitation of the a-'y subunit in thesesera by a sensitive ELISA revealed an amount - 1% of thatfound in normal human serum. A similar assay performed witha specific antiserum to C8,0 showed unexpectedly low levels ofC8,B in these sera, which were confirmed by hemolytic titrationof C8ft. The remarkable differences between C8a-'y and C8# inthe C8a--y deficient sera was that in spite of their comparableimmunochemical levels, C8,8 still exhibited functional activitywhereas C8a-'y was totally inactive. That the residual C8a-ywas inactive was also proved by its inability to show lytic bandsin an overlay system after SDS-PAGEand subsequent removalof SDS. The implications of these findings for a novel conceptof C8 deficiency are discussed. (J. Clin. Invest. 1990. 86:884-888.) Key words: complement * C8 * inherited defect * C8 sub-units * combined deficiency
Introduction
The selective defect of the eighth complement component(C8)' is relatively commonamong the inherited deficiencies ofthe components and regulators of the complement system (1).Patients with this defect show an increased susceptibility tomeningococcal meningitis, indicating that C8 plays an impor-tant role as a component of the membrane attack complex andin the protection against neisserial infections (1, 2).
A distinctive feature of C8 deficiency is the presence of a
dysfunctional C8 molecule in all the sera of C8-deficient
Address correspondence and reprint requests to Dr. F. Tedesco, Isti-tuto di Patologia Generale, Universita di Trieste, via A. Fleming, 22,34127 Trieste, Italy.
Receivedfor publication 27 December 1989 and in revisedform 24April 1990.
1. Abbreviations used in this paper: C8, eighth component of comple-ment; C8D, C8a-wyD, and C8I3D, C8-, C8a-y-, and C8ft deficient;EACl-3, EACI-7, and EACl-8, sheep erythrocytes coated with anti-body and complement components up to C3b, C7, and C8; NHS,normal human sera.
(C8D) subjects that have been tested (2). This is rarely ob-served in other complement deficiencies with the exception ofa small group (10-15%) of patients lacking functional Cl-in-hibitor (3). On the basis of reconstitution experiments andimmunochemical analysis, two forms of dysfunctional C8,and consequently two groups of patients have been identified(4, 5). One form is associated with a dysfunction in the a--ysubunit and the other with a dysfunction in f3. The absence ofC8 activity in both groups is consistent with the fact that a-'yand j3 have specific functional roles and both are essential fornormal C8 hemolytic activity (6). For reasons that are pres-ently not clear, the inherited defect of C8ti is largely predomi-nant over that of C8a-,y and is essentially restricted to Cauca-sians, whereas the C8a-'y deficiency has been found exclu-sively in Blacks and North Africans (1, 2).
The possibility that C8 deficiencies result from the com-plete absence of a particular subunit is unlikely in view ofrecent findings by Tschopp and co-workers (7). Two C8#-defi-cient patients were found to have detectable but dysfunctionalC83 in their serum along with normal a--y. Partial character-ization indicated that the C8,3 was structurally abnormal.Thus, at least in some patients, dysfunctional C8,i is synthe-sized but in an altered form. Presumably this altered form isincapable of association with a-'y to produce functional C8.
In this study, we examined in more detail the molecularabnormality of the dysfunctional C8 in three C8a-,yD individ-uals and provide evidence for a further complexity of thisinherited defect. Data presented indicate that C8a-'y defi-ciency is a combined defect of both a-,y and fi, and that a smallamount of dysfunctional C8a-,y can be detected in the sera ofC8a--y deficient patients.
Methods
Sera. Three unrelated C8a-yD patients and two siblings with C8,BD,reported in previous publications (8-11), provided serum samples forthis investigation. The type of C8 deficiency was recognized by hemo-lytic reconstitution with the missing subunits and by identification ofthe subunit present in the various sera by SDS-PAGEand immuno-chemical procedures (4). A pool of normal human sera (NHS) wasprepared by mixing equal volumes of sera obtained from 20 blooddonors.
Complement reagents. HumanC8 was purified following the pro-cedure described in detail by Steckel et al. (12). The two subunits,C8a--y and C8(B, were dissociated from C8 in the presence of buffers ofhigh ionic strength and further purified by gel filtration through Seph-acryl S-300 (Pharmacia Fine Chemicals, Uppsala, Sweden), as reportedby Rao and Sodetz (13).
Erythrocyte intermediates and hemolytic assays. The preparationof EAC1-3 and EAC1-7 from IgM sensitized sheep red cells usingyeast-treated human serum and a C8,BD serum has been previouslydescribed (10). The hemolytic assays for C8a-'y and C8,3 were per-
884 F. Tedesco, L. Roncelli, B. H. Petersen, V. Agnello, and J. M. Sodetz
J. Clin. Invest.©The American Society for Clinical Investigation, Inc.0021-9738/90/09/0884/05 $2.00Volume 86, September 1990, 884-888
formed by incubating a mixture of 200 ,d of various sera dilutions and50 1Al of EACI-7 (1.5 X 107), suspended in either C8a--yD or C8#3Dsera, to a final dilution of 1/50 for 30 min at 370C. Preliminary exper-iments proved that the concentrations of the C8Dsera used for theseassays were not limiting for an optimal titration of the two C8 subunits.
Antisera. A goat antiserum against whole human C8 was purchasedfrom Atlantic Antibodies (Scarborough, ME). Antibodies to C8a-ywere prepared in two different ways. A goat antiserum prepared againstwhole human C8 was passed through an agarose-(a-y) affinity columnto isolate (a-'y)-specific Ig (14). A second antiserum with a higheravidity for a-,y was obtained by immunizing rabbits with purified a-yand passing the antiserum through an agarose-(() column to removetraces of anti-fl. Specific antibodies against fi were prepared similarly inrabbits using purified fi as the immunogen. Specificity was tested byOuchterlony and SDS-PAGEimmunoblotting.
A mouse monoclonal antibody was obtained following an estab-lished procedure (15) and found to recognize the a chain of C8. Asciticfluid was produced in pristane-primed Balb/c mice and used for theexperiments.
Biotin labeling of antibodies. The IgG fraction of the rabbit antiserato C8a-'y and C8fl was obtained by affinity cromatography throughprotein A-agarose (Zymed Laboratories, San Francisco, CA) using 0.2Mphosphate/0. 1 M citrate pH 3.5 as eluting buffer. The IgG weredialyzed against 0.2 MTris-HCl pH 8.0 and mixed with D-biotin-N-hydroxysuccinimide ester (Sigma Chemical Co., St. Louis, MO) (2mg/ml in DMSO)at a ratio of 1:4 (wt/wt) for 15 min at room tempera-ture. The excess biotin was removed by dialysis against 10 mMPBSpH7.4 containing 0.0 1%NaN3.
SDS-PAGEand immunoblotting. Normal and C8D sera were sub-jected to SDS-PAGEon a 10% gel under nonreducing conditions ac-cording to Laemmli (16), followed by electrophoretic transfer ontonitrocellulose (Schleicher & Schuell Inc., Dassel, FRG). After soakingthe nitrocellulose sheet in 50 mMTris-HCl pH 7.6 containing 0.5 MNaCl Tris buffered saline, 2%bovine serum albumin, and 0.5% Tween20 for I h at 37°C to block the free binding sites, the C8 bands wererevealed by successive incubations with the primary antibodies to C8or C8 subunits overnight at 4°C, followed by the biotin-labeled second-ary antibodies (Zymed Laboratories) for 2 h at 37°C and alkalinephosphatase conjugated to streptavidine (Jackson ImmunoresearchLaboratories, West Grove, PA) for 1 h at 37°C. The enzymatic reac-tion was developed using nitroblue tetrazolium (0.30 mg/ml) and 5-bromo-4-chloro-3-indolyl phosphate (0.15 mg/ml) (both purchasedfrom Sigma Chemical Co.), and diluted in 0.1 MTris-HCI pH 9.5containing 0. 15 MNaCI.
Hemolytic overlay. The functional activity of the C8a-'y subunitelectrophoresed by SDS-PAGEwas revealed following the proceduredeveloped by Orren et al. ( 17). Briefly, after the electrophoretic run thegels were soaked in an aqueous solution of 0.25% Triton X-100 for 1 hat 4°C to remove SDSand then in H20 for 1 h at 4°C, followed by a10-min wash with glucose veronal-buffered saline (18). The gel wascovered with a mixture of 1%agarose, 0.6% EACI-7, and 1/50 C8a--yDserum to obtain a 1-mm thick gel. The overlay was incubated at 37°Cin a humid box until the hemolytic bands developed. Further hemo-lysis was prevented by adding 2%glutaraldehyde in saline.
Quantitation of the C8 subunits by ELISA. The wells of microtiterplates (Dynatech, PBI, Milan, Italy) were coated with 200 LI of the IgGfraction of either anti-C8a-y (k1.6 ug/well) or anti-C8,B (0.5 ag/well) in0.1 M sodium bicarbonate buffer pH 9.6 overnight at 4°C. Afterblocking the residual free sites with PBS containing 1%bovine serumalbumin and 0.1% Tween 20, normal and C8Dsera were added at theappropriate dilutions and incubated for I h at 37°C and subsequentlyovernight at 4°C. The binding of the C8 subunits was revealed by theaddition of biotin-labeled anti-C8a-y or anti-C8,B antibodies. After anincubation of 2 h at 37°C, the reaction was revealed by the addition ofalkaline phosphatase conjugated to streptavidine for 30 min at 370C,and subsequently of p-nitrophenyl-phosphate (Merck, Bracco S. P. A.,Milan, Italy) at the concentration of 1 mg/ml in 0.1 Mglycine bufferpH 10.4 containing 1 mMMgCI2 as substrate for the enzyme. Reading
was performed in a Multiskan 340 apparatus (Flow Laboratories Inc.,Milan, Italy) at 405 nm.
Depletion of C8from human sera by affinity chromatography. Aga-rose-(a-y) IgG was prepared by coupling affinity purified goat anti-a-yIgG to agarose by standard procedures using cyanogen bromide acti-vation ( 14). This resin recognizes and removes both free a-,y and intactC8 from serum.
Results
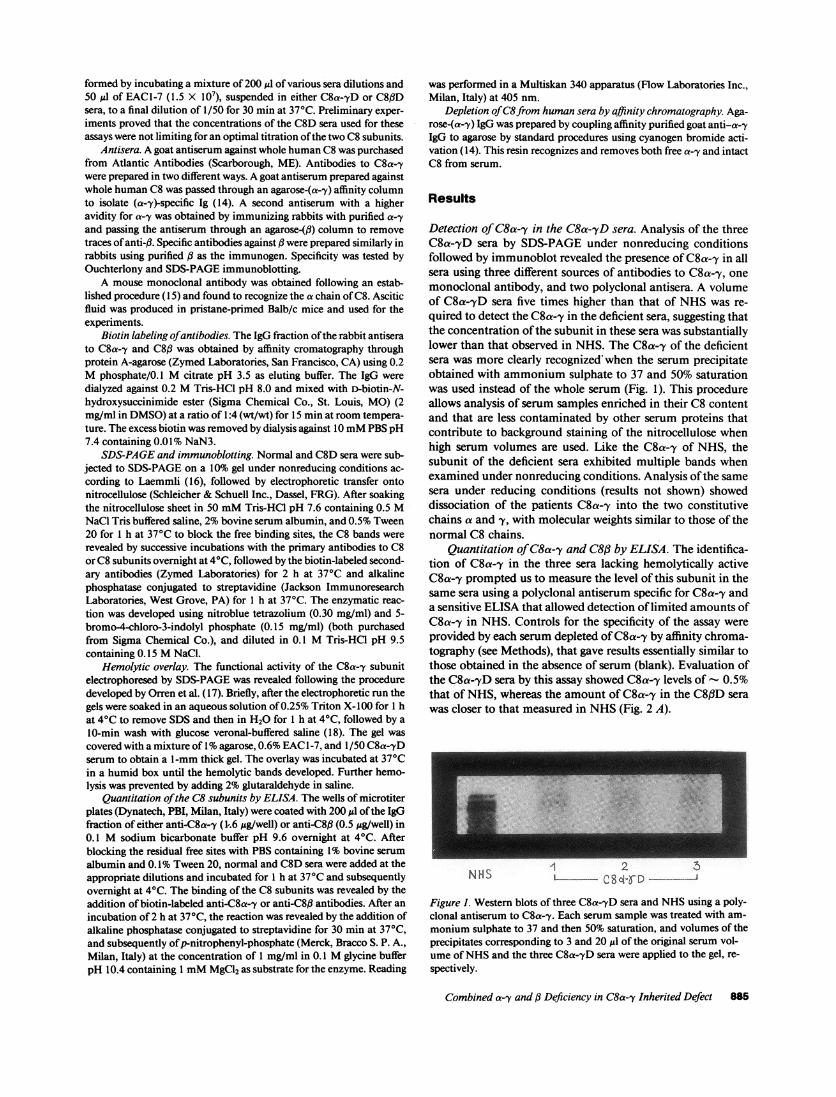
Detection of C8a-,y in the C8a-,yD sera. Analysis of the threeC8a-yD sera by SDS-PAGE under nonreducing conditionsfollowed by immunoblot revealed the presence of C8a-y in allsera using three different sources of antibodies to C8a-,y, onemonoclonal antibody, and two polyclonal antisera. A volumeof C8a-TyD sera five times higher than that of NHSwas re-quired to detect the C8a-y in the deficient sera, suggesting thatthe concentration of the subunit in these sera was substantiallylower than that observed in NHS. The C8a-'y of the deficientsera was more clearly recognized when the serum precipitateobtained with ammonium sulphate to 37 and 50% saturationwas used instead of the whole serum (Fig. 1). This procedureallows analysis of serum samples enriched in their C8 contentand that are less contaminated by other serum proteins thatcontribute to background staining of the nitrocellulose whenhigh serum volumes are used. Like the C8a-y of NHS, thesubunit of the deficient sera exhibited multiple bands whenexamined under nonreducing conditions. Analysis of the samesera under reducing conditions (results not shown) showeddissociation of the patients C8a-'y into the two constitutivechains a and y, with molecular weights similar to those of thenormal C8 chains.
Quantitation of C8a-,y and C8ff by ELISA. The identifica-tion of C8a-7y in the three sera lacking hemolytically activeC8a-y prompted us to measure the level of this subunit in thesame sera using a polyclonal antiserum specific for C8a-y anda sensitive ELISA that allowed detection of limited amounts ofC8a-'y in NHS. Controls for the specificity of the assay wereprovided by each serum depleted of C8a-,y by affinity chroma-tography (see Methods), that gave results essentially similar tothose obtained in the absence of serum (blank). Evaluation ofthe C8a-'yD sera by this assay showed C8a-,y levels of 0.5%that of NHS, whereas the amount of C8a-'y in the C8/3D serawas closer to that measured in NHS(Fig. 2 A).
NHS ~~1 2NHIdS LC8 cl-g D
Figure 1. Western blots of three C8a-,yD sera and NHSusing a poly-clonal antiserum to C8a-y. Each serum sample was treated with am-
monium sulphate to 37 and then 50% saturation, and volumes of theprecipitates corresponding to 3 and 20 Ml of the original serum vol-ume of NHSand the three C8a--yD sera were applied to the gel, re-
spectively.
Combined a-,y and ,3 Deficiency in C8a--y Inherited Defect 885

A
U,
-,
.A .2 .4 2.5 5 10 20 40 80
SERUM DILUTIONS (x103)10 20 40 80
SERUM DILUTIONS (x03)B
1.5
0 1.0-z
Co)
3; 0.5~
wU
B
-C
O
0
.5 1 2 4 8 16 32 64 128 256
SERUM DILUTIONS (x102)
Figure 2. Immunoenzymatic assay of C8a-'y (A) and C8# (B) inNHS(rn-*), two C8MD(A- A), and three C8a-yD sera (--*).The results are expressed as ELISA index that is equal to (OD sam-ple-OD blank)/OD blank, where blank indicates the result obtainedin the absence of the serum samples.
Since C8(3 is known to be present in the C8a-yD sera, wewanted to quantitate the amount of C8a-y relative to that ofC8,B in these sera next. Employing an ELISA specific for C8(l,the level of this subunit in the C8a-yD sera was found to bemarkedly reduced to - 1-3% of that in NHSwith a ratio ofC8a-y to C8,# varying between 0.2 and 0.5 in the three defi-cient sera (Fig. 2 B). A similar assay performed on the twoC8#lD sera revealed negligible amounts of C8,B (results notshown).
Table I. Comparison of the Hemolytic Activitiesand the Immunochemical Levels of C8a-y and C8fi Subunitsin NHSand C8a--yD Sera
Hemolytic activity Immunochemical levels(CH 50 U/ml) (% of NHS)
C8a-. C8ft C8a-y C8,
NHS 160,000 132,000 100 100C8a-'yDl 0 1,750 0.41 2.5C8a--yD2 0 1,200 0.56 2. 1C8a-yD3 0 1,000 0.50 0.98
1 .2 .4 .8 1.6 5 10 20 40 80 160
SERUM DILUTIONS (x103)
Figure 3. Hemolytic titration of C8a-'y (A) and C8# (B) in NHS( -rn) and three C8a-yD sera (e- .). The hemolytic system con-
tained 50 ul of EAC1-7 (1.5 X 107) and either C8a-yD or C8flD sera
to the final dilution of 1/50 in a total volume of 250 ,l.
The hemolytic activities of C8a-7y and C8# in the C8a-,yDsera are differentially related to their immunochemical levels.Having found remarkably low amounts of both C8a-'y andC8# in the three C8a-'yD sera by ELISA, it was of importanceto examine how these levels related to the functional activity ofthese subunits in the same sera. Previous work has clearlyestablished that the C8j# of the C8a-'yD patients is fully activein reconstituting the lytic activity of the C8,BD sera (4, 5).Analysis of the C8a-7D sera for C8a-y (Fig. 3 A) and C8f# (Fig.3 B) hemolytic activities confirmed the results obtained withthe immunoenzymatic assays for C8(3 but not for C8a--y. Inparticular, all three C8a-yD sera had significant C8j# activity,but failed to lyse EACl-8ft. The serum of an additional unre-
lated C8a-yD patient, kindly provided by Dr. H. Jasin (De-partment of Internal Medicine, University of Texas South-western Medical School, Dallas, TX), was also found to haveextremely low levels of C8(l activity. Unfortunately, this serum
was not available in sufficient amounts to allow further inves-tigation. Comparing the results of the ELISA and of functionalassays (Table I), it is apparent that the immunochemical levelsof C8,B in the C8a-yD sera correlates with its functional activ-ity, accounting for 1-3% of the values found in NHS. In con-
trast, the hemolytic activity of C8a-y was absent in spite of a
886 F. Tedesco, L. Roncelli, B. H. Petersen, V. Agnello, and J. M. Sodetz
x
0z
ot-J(A
A

Figure 4. Detection offunctional C8a-y subunitby hemolytic overlay. 1,u of NHS(lane 6) and 6Ml of two C8,6D sera(lanes 1 and 3) and ofthree C8a-yD sera (lanes2, 4, and 5) were electro-phoresed by SDS-PAGEand the hemolytic bandswere revealed as de-scribed in Methods.
detectable immunochemical level, suggesting that C8a-y inthese sera is hemolytically inactive.
To obtain further evidence in favor of a dysfunctionalC8a-'y molecule being present in the C8a--yD sera, an addi-tional approach was followed based on the hemolytic detectionof C8a-y after SDS-PAGE. For this purpose, the sera wereelectrophoresed in duplicate on the same gel, and at the end ofthe run, one-half of the gel was processed for Western blottingwhile the second half was used for the hemolytic overlay afterremoval of SDS. Under these conditions, the C8a--y of bothNHSand C8f3D sera exhibited activity, as indicated by theappearance of lytic bands at the position of C8a--y migration(Fig. 4). No bands were detected in lanes loaded with the threeC8a--yD sera, although distinct C8a-'y bands appeared in thecorresponding lanes of the gel after immunoblotting (resultsnot shown).
Discussion
Patients with C8a--y deficiency represent a minority of thewhole group of C8D individuals and can be identified by thepresence of hemolytically active and immunochemically rec-ognizable C8,B in their sera (2). The lack of functional activityin these sera has been attributed to a selective defect of C8a-ythat could not be detected either functionally or immuno-chemically. Although this conclusion remains basically cor-rect, the present data indicate that the nature of the C8 defectin these sera is more complex than hitherto recognized.
An important finding of this study was the detection ofC8a-y in the deficient sera by Western blot analysis of thewhole serum using a monoclonal antibody and two polyclonalantisera to C8a-'y. The higher sensitivity of both the assaysystem employed in this investigation and the use of antibodiesspecific for C8a--y, possibly directed to additional epitopes notrecognized by antisera to whole C8, may have contributed toreveal previously undetected C8a-'y. A similar situation has
been described by Tschopp et al. (7) in two C8fiD sera in whichC8, was detected only by antisera specific for C8,B but not bythose to whole C8. Quantitation of C8a-'y by ELISA con-firmed the presence of this subunit in the C8a-'yD sera, albeitin a limited amount that did not exceed 2% of the level ob-served in NHS. The fact that the antiserum used for the ELISAdetected only C8a-y in NHSby Western blot proves the speci-ficity of the assay for C8a-y. This was further substantiated bythe finding that depletion of the residual C8a-'y by affinitychromatography resulted in C8a-'yD sera values similar tothose of the controls in the absence of serum.
The low levels of C8a-'y found in the C8a--yD sera do notcorrelate with the lack of hemolytic activity in these sera. NHScan in fact be diluted to contain an amount of C8a-y equal tothat of the C8a-yD sera and still induce complete lysis in aC8a-y-dependent lytic assay. This assay is in fact exquisitelysensitive and reveals functional C8a--y in NHSup to a dilutionof 1 to 100,000. The suggestion can therefore be made that theresidual C8a-y in the deficient sera is dysfunctional. This isalso proved by the inability of the subunit in the C8a-'yD serato resume lytic activity after SDS-PAGEin an overlay system,in spite of the fact that C8a-'y can be detected immunochemi-cally by Western blot.
Discovery of a combined deficiency of a--y and # in C8a-,ypatients is unexpected in view of the fact that the amount ofC8,B in these sera is sufficient to reconstitute the lytic activity ofC8,BD sera (4), and also that in C8,BD sera a--y is frequentlypresent at near normal levels. If inherited C8 deficiency mani-fests itself as a defect in either a-y or ,B, then one would alsoexpect to find near normal levels of ,B in C8a--yD. Results ofthis study clearly indicate that this is not the case. One expla-nation may be that in C8a--yD sera there are molecular defectsin both a-'y and ,B such that levels of each are reduced. Thisseems unlikely however, because only a-'y is functionally ab-normal. An alternative explanation is that ,3 depends on asso-ciation with normal a--y for proper biosynthesis and secretion
Combined a--y and , Deficiency in C8a--y Inherited Defect 887
..

or for stability in the circulation. Synthesis of an abnormal a-'ywould then produce a corresponding decrease in B3. This wouldcontrast with C8(3 deficiency, where neither the level nor thefunctional state of (3 have a major impact on levels of a-ey.Stability of free a-y in the bloodstream has been suggestedfrom biosynthetic studies showing that hepatocytes secrete ex-cess a-y relative to: ( 14), and from studies that found signifi-cant levels of free a-'y along with C8 in NHS(19, 20). Thus, itmay be that serum levels of ( are dependent on a-'y but theconverse is not necessarily true.
Weoriginally proposed that the inherited deficiency of C8be divided into two groups on the basis of immunochemicalanalysis and reconstitution experiments (4). The present find-ings of combined deficiency of C8a-y and C8(3 subunits inpatients with inherited defect of C8a-'y do not contradict ourprevious observation. The genetic and molecular defect re-sponsible for each type of C8 deficiency may still be restrictedto either a-ey or (3, but the consequences of these deficienciesdiffer with regard to the opposite subunit. In the combineddeficiency for instance, a defect in a-y would have an adverseeffect on serum levels of (3. At present, the nature of the molec-ular defects responsible for C8 deficiency is unknown. A majordeletion of the # gene has been excluded based on studies ofgenomic DNAfrom patients with C8(3 deficiency (21), whilefor the combined deficiency the defect may be in a or y. Amajor gene deletion in a seems unlikely in view of the closephysical linkage between a and (3 on chromosome 1 and theexpression of functional (3 in the C8a-yD (22). The exact na-ture of the a-'y defect must await further characterization of aand y genomic structures.
Acknowledgments
Weare indebted to Dr. C. Hershko, Department of Medicine, ShaareZedek Medical Center, Jerusalem, Israel, and Dr. H. Jasin, for theirgenerous supply of C8a-y-deficient sera. The authors wish to thank Dr.P. Bertoncin for helping in the affinity chromatography techniques.
This work was supported by the Italian Consiglio Nazionale delleRicerche grant on Progetto Finalizzato Ingegneria Genetica e BasiMolecolari delle Malattie, by the 40% grant of The Italian Ministerodella Pubblica Istruzione, and by National Institutes of Health grantsAl 16856 and GM42898.
References
1. Ross, S. C., and P. Densen. 1984. Complement deficiency statesand infection: epidemiology, pathogenesis and consequences of Neis-serial and other infections in an immune deficiency. Medicine (Balti-more). 63:243-273.
2. Tedesco, F. 1986. Complement deficiencies.8. The eighth com-ponent. In Hereditary and Acquired Complement Deficiencies in An-imals and Man. K. Rother and U. Rother, editors. Progr. Allergy.39:295-306.
3. Agostoni, A. 1989. Inherited Cl inhibitor deficiency. Comple-ment Inflammation. 6:112-118.
4. Tedesco, F., P. Densen, M. A. Villa, B. H. Petersen, and G.Sirchia. 1983. Two types of dysfunctional eighth component of com-plement (C8) molecules in C8 deficiency in man. Reconstitution ofnormal C8 from the mixture of two abnormal C8 molecules. J. Clin.Invest. 71:183-191.
5. Alper, C. A., D. Marcus, D. Raum, B. H. Petersen, and T. J.Spira. 1983. Genetic polymorphism in C8(3-chains. Evidence for twounlinked genetic loci for the eighth component of human complement(C8). J. Clin. Invest. 72:1526-1531.
6. Sodetz, J. M. 1988. Structure and function of C8 in the mem-brane attack sequence of complement. In Current Topics in Microbi-ology and Immunology. E. R. Podack, editor. Springer-Verlag, Berlin.140:19-31.
7. Tschopp, J., F. Penea, J. Schifferli, and P. Spath. 1986. Dys-functional C8,6 chain in patients with C8 deficiency. Scand. J. Im-munol. 24:715-720.
8. Petersen, B. H., J. A. Graham, and G. F. Brooks. 1976. Humandeficiency of the eighth component of complement. The requirementof C8 for serum Neisseria gonorrhoeae bactericidal activity. J. Clin.Invest. 57:283-290.
9. Agnello, V., K. M. Pariser, and D. Babott. 1978. Association ofC8 deficiency with sickle-thalassemia hemoglobinopathy. J. Immunol.120: 1761 a. (Abstr.)
10. Tedesco, F., M. Bardare, A. M. Giovanetti, and G. Sirchia.1980. A familial dysfunction of the eighth component of complement(C8). Clin. Immunol. Immunopathol. 16:180-191.
11. Zimran, A., B. Rudensky, M. R. Kramer, F. Tedesco, M.Ehrenfeld, R. Raz, Z. Greif, M. Gelber, M. Lishner, E. Golan, and C.Hershko. 1987. Hereditary complement deficiency in survivors of me-ningococcal disease: high prevalence of C7/C8 deficiency in Sephardic(Moroccan) Jews. Q. J. Med. 240:349-358.
12. Steckel, E. W., R. G. York, J. B. Monahan, and J. M. Sodetz.1980. The eighth component of human complement: purification andphysicochemical characterization of its unusual subunit structure. J.Biol. Chem. 255:11997-12005.
13. Rao, A. G., and J. M. Sodetz. 1984. Purification of functionalsubunits of the eighth component of human complement (C8) undernondenaturing conditions. Complement. 1: 182-186.
14. Ng, S. C., and J. M. Sodetz. 1987. Biosynthesis of C8 by hepa-tocytes. Differential expression and intracellular association of the a-'yand ,B subunits. J. Immunol. 139:3021-3027.
15. Galfre, G., S. C. Howe, C. Milstein, G. W. Butcher, and J. C.Howard. 1977. Antibodies to major histocompatibility antigens pro-duced by hybrid cell lines. Nature (Lond.). 266:550-552.
16. Laemmli, U. K. 1970. Cleavage of structural proteins duringthe assembly of the head of bacteriophage T4. Nature (Lond.).227:680-685.
17. Orren, A., W. H. Lerch, and E. B. Dowdle. 1983. Functionalidentification of serum complement components following electro-phoresis in polyacrylamide gels containing sodium dodecyl sulphate. J.Immunol. Methods. 59:63-71.
18. Mayer, M. M. 1971. Complement and complement fixation. InExperimental Immunochemistry. E. A. Kabat and M. M. Mayer, edi-tors. Charles C. Thomas, Springfield, IL. 133-240.
19. Densen, P., and C. M. McRill. 1988. Differential functionalexpression of the C8 subunits: primary role of C8# in assembly ofintact C8. J. Immunol. 141:2674-2679.
20. Doglio, L. T., M. S. Gawryl, and T. F. Lint. 1988. Analysis ofhuman C8 with monoclonal antibodies: characterization of a mono-clonal antibody that recognizes free C8a-y subunit. J. Immunol.141:2079-2083.
21. Schneider, P. M., B. Dittmer, F. Tedesco, P. J. Spath, C.Rittner, and J. M. Sodetz. 1987. Genomic structure of the complementC8,l locus in individuals with inherited C8,B deficiency. Complement.4:22 la. (Abstr.)
22. Kaufman, K. M., J. V. Snider, N. K. Spurr, C. E. Schwartz, andJ. M. Sodetz. 1989. Chromosomal assignment of genes encoding the a,
,B, and y subunits of human complement protein C8: identification of aclose physical linkage between the a and the # loci. Genomics. 5:475-480.
888 Calvo, Obregon, Ruiz de OQa, Escobar del Rey, and Morreale de Escobar