tumor board session
TRANSCRIPT

TUMOR BOARD SESSION
MULTIDISCIPLINARY APPROACH TO OPTIMAL
MANAGEMENT OF COLORECTAL CANCER
LIVER METASTASES
1

Panel & Disclosures
2
Arya Amini, MDAssistant Professor
Department of Radiation OncologyChief of Thoracic Radiotherapy
City of Hope
• Grant/Research Support from Genentech.• Consultant for Reflexion.• On the Speakers Bureau for AstraZeneca, and Takeda Pharmaceuticals.
Misagh Karimi, MDDirector of Operations
Assistant Clinical ProfessorDepartment of Medical Oncology & Therapeutics Research
City of Hope
• Nothing to disclose.
Aram Lee, MDAssistant Clinical Professor
Department of Interventional RadiologyCity of Hope
• Consultant for Genentech.• On the Speakers Bureau for Genentech.
Mustafa Raoof, MD, MS, FACSAssistant Professor
Department of SurgeryDepartment of Cancer Genetics and Epigenetics
City of Hope
• Nothing to disclose.

Case #1
▪ 58 yr old C female
▪ CRC with Synchronous liver mets
▪ 10/19/2020 presented with GI obstruction
▪ 10/19/2020 status post rectosigmoid resection and colostomy placement. Pathology showed invasive adenocarcinoma, low-grade (moderately differentiated). Tumor extends to serosal surface (pT4). Margins negative. No lymphovascular invasion. 20 lymph nodes evaluated and none showed metastasis. MSS by IHC.
▪ KRAS p.G12F;MMR pro by IHC, TMB 5; PDL-1 0 ; APC mutation;
▪ 11/17/2020 C1 FOLFOX Bev X 6 cycles with great PR
▪ 2/8/2021 switched to maintenance Cap Bev
3
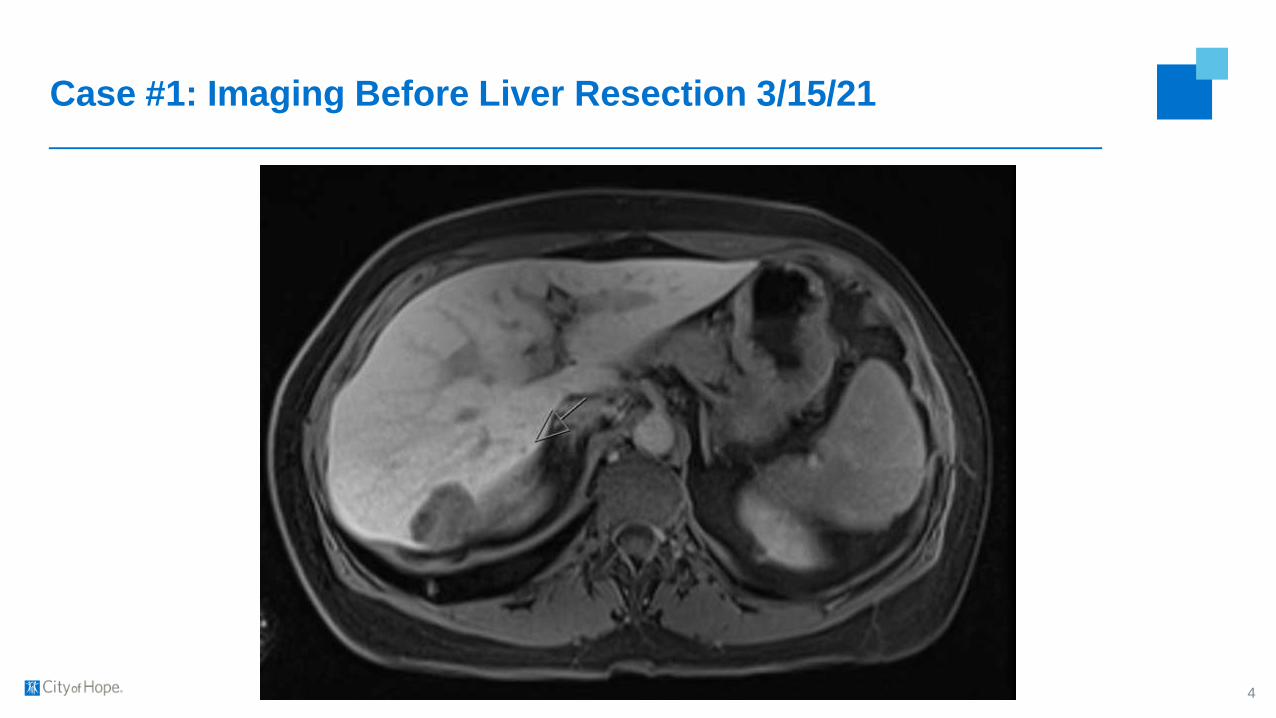
Case #1: Imaging Before Liver Resection 3/15/21
4

Case #1
▪ 7/16/21 Signatera negative
▪ Cape Bev maintenance started 5/14/21
5

Case #1: 4-months post-resection
6

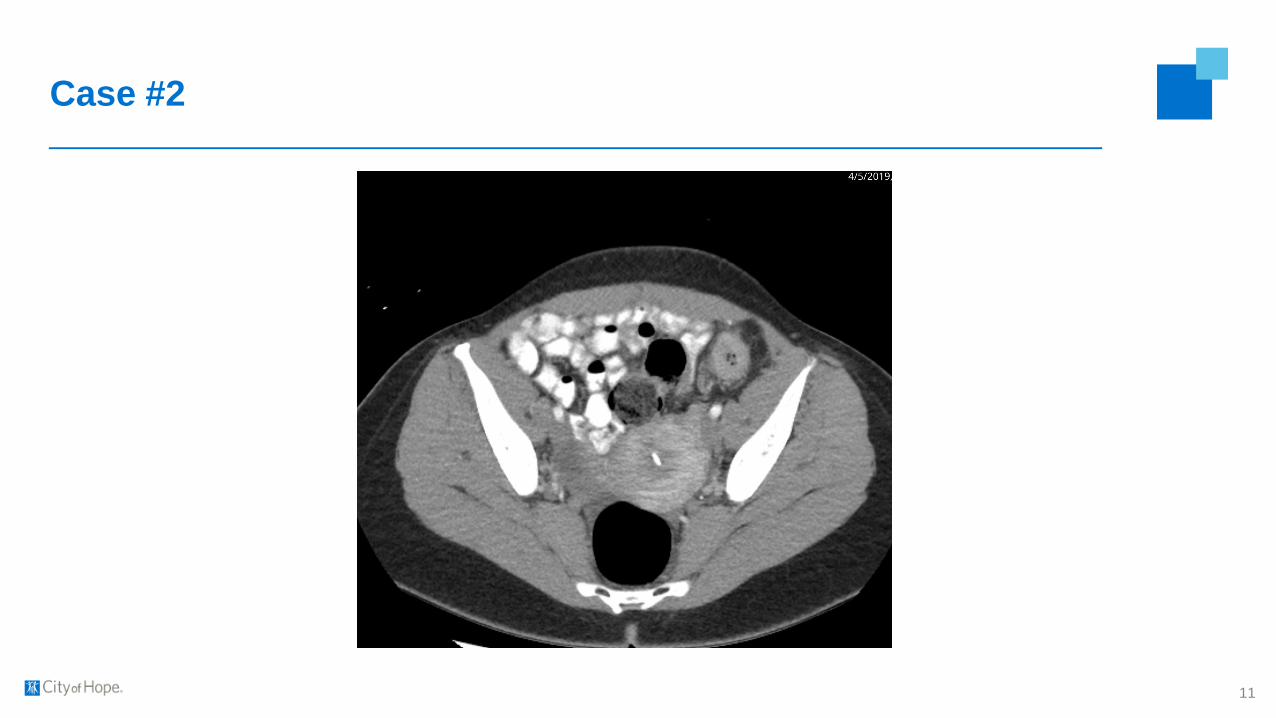
Case #2
▪ 40 yo F who presents with synchronous colorectal cancer liver metastases
▪ October 2018: Presented with intermittent abdominal pain, 3 months post-partum
▪ December 2018: Acute worsening of pain, evaluated in ER
▪ PMH: HTN
7

Case #2
8

Case #2
▪ March 2019, BRBPR, Hb 6.8
▪ Lower endoscopy on 4/6/19: Circumferential nearly obstructing colon mass in the descending
colon at 40 cm from the anal verge with contact bleeding and friability.
▪ Bx: Colon adenocarcinoma, KRAS WT, MSS, BRAF WT
▪ CEA 544
▪ Staging CT demonstrated the following:
9

Case #2
10
Case #2
11

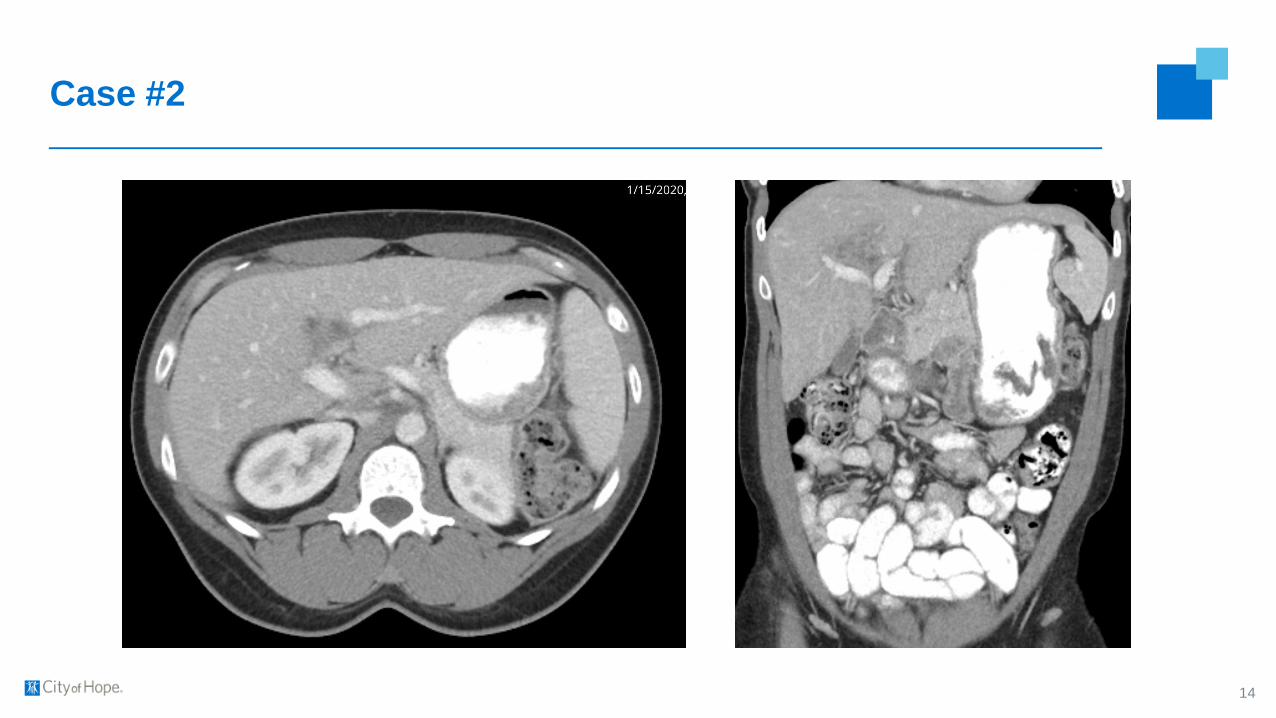
Case #2
▪ The patient was evaluated and treated at the outside hospital
▪ May 2019 – December 2020: FOLFOX + Avastin 12 cycles
▪ CEA 544 → 52
▪ CT demonstrated the following
12
▪ What would be the next step

Case #2
13
Case #2
14

Case #2
▪ FLR 30%, planned extended right
▪ March 2020, PVE (Right portal and segment 4)
▪ Chemotherapy changed to FOLFOX + Erbitux to get more response
▪ FLR 1 month later was 41%
▪ Continued tumor shrinkage but central mass still abutting the left portal inflow. CEA 544 → 52
→ 26
15
▪ What would be the next step

Case #2
▪ April 2020
▪ Extended Right hepatectomy, Segment 2 Ablation
▪ Hepatic Artery Infusion pump placement
▪ All liver disease resected except 1mm thick 1cm x 1cm residual disease on the left portal inflow
16
▪ What would be the next step

Case #2
17

Case #2
▪ Underwent SBRT, 40 Gy in 5 fractions
18
Case #3
▪ 55 yo M who presents with metastatic colorectal cancer with liver metastases
▪ Prior treatment history includes:
o FOLFOX cetuximab
o FOLFIRI bevacizumab
o FOLFIRI + HAI infusion with FUDR
▪ Due to continued progression he was referred for palliative Y90 radioembolization of his liver
metastases
19

Case #3
▪ Pre-Y90 radioembolization
20

Case #3
21
Intraprocedural hepatic angiogram Immediate post Y90 PET scan

Case #3
22
- Early post radiation changes in the right lobe- Tumor markers
- CEA 2657 -> 1626- CA19-9 893 -> 443
- Two enlarging central lesions in the untreated medial left lobe
- What treatment options should be considered?

Case #3
▪ Underwent SBRT, 40 Gy in 5 fractions
23

Questions
24