tropical medicine/parasitic disease cases · 2018-02-06 · binax now is the only brand of malaria...
TRANSCRIPT

1
TROPICAL MEDICINE/PARASITIC DISEASE CASES
UNDIFFERENTIATED FEVER IN THE RETURNED TRAVELER: The differential diagnosis of undifferentiated fever in a returned traveler should include the following entities:
1. Malaria 2. Dengue Fever 3. Rickettsia - including Typhus 4. Typhoid Fever 5. Leptospirosis
MALARIA: Epidemiology:
~ 49% of the world’s population is at risk
~ 216 million cases and ~ 655,000 deaths occurred in 2010
most of the deaths occur among children < 5 years of age in sub-Saharan Africa
1,691 US cases (including 9 deaths) reported to the CDC in 2010 o the infecting species was identified and reported in 1,388 (82%) of cases o when the infecting organism was identified and reported:
P. falciparum was identified in 71% of cases P. vivax was identified in 23% of cases
o there were 1,479 imported cases where the region of acquisition was known: 959 (64.8%) were acquired in Africa 285 (19.3%) were acquired in Asia 230 (15.6%) were acquired in the Americas 5 (0.3%) were acquired in Oceania
Geographic Distribution: see map
the following areas have Chloroquine-sensitive P. falciparum: o Central America west of the Panama Canal o the Caribbean o Argentina and Paraguay o selected areas of North Africa and the Middle East
in all other areas P. falciparum is considered to be Chloroquine-resistant
all other malarial species are generally considered to be Chloroquine-sensitive with the exception of P. vivax from Papua New Guinea and Indonesia

2
Chloroquine-Resistant Malaria Mefloquine-Resistant Malaria

3
Parasitology/Life Cycle:
five species now cause human disease: o Plasmodium falciparum o Plasmodium vivax o Plasmodium ovale o Plasmodium malariae o Plasmodium knowlesi
vector: anopheline mosquitoes o feed from dusk to dawn; only females feed on vertebrates o mosquitoes must survive 9-22 days to be able to transmit infection o elevations over 6,000 feet not conducive to transmission
life cycle: Clinical Manifestations:
travel history: o fever in the traveler returning from the tropics o most cases occur within 1-2 months of travel
incubation: ~ 2 weeks (can vary due to chemoprophylaxis)
uncomplicated Malaria: o signs/symptoms: nonspecific
“flu-like” illness (headache, myalgias, abdominal discomfort, lethargy), fever rigors, diarrhea
unlikely findings: sore throat, lymphadenopathy, rash splenomegaly (minority of cases)

4
o laboratory findings: thrombocytopenia < 150,000/L (may be seen in up to 95%) WBC usually normal; lymphs; eosinophilia unusual anemia may be present positive blood films (thick - diagnosis; thin - speciation)
severe malaria (WHO definitions) – includes one or more of the following: o cerebral Malaria – high mortality o severe anemia o renal failure o pulmonary edema/ARDS o hypoglycemia o circulatory collapse or shock (algid malaria) o spontaneous bleeding o repeated generalized convulsions o lactic acidosis o macroscopic hemoglobinurias o post-mortem confirmation of diagnosis o impaired consciousness (less marked than unrousable coma) o prostration: in a child – inability to sit or feed o hyperparasitemia: 20% (varies according to circumstance)
Diagnosis:
blood smears: o thick film: diagnosis of malaria (~ 30x more sensitive than thin films) o thin film: speciation of malaria
Rapid Diagnostic Tests (RDTs): o first RDT recently approved by the FDA for use in the US (6/13/07):
BINAX NOW® detects specific malarial antigens within 15 minutes follow-up microscopy still required for both positive/negative tests
Binax NOW is the only brand of malaria RDT approved for use in the united States. The picture above demonstrates a positive test for Plasmodium falciparum. (Howden BP et al. Chronic falciparum malaria causing massive splenomegaly 9 years after leaving an endemic area. MJA 2005; 185: 186-188. ©Copyright 2005. The Medical Journal of Australia)

5
Red blood cell morphology in various forms of Plasmodium infections
Management/Treatment:
4 Important Questions: 1. Does the patient have malaria? 2. Does the patient have falciparum malaria or one of the rest? 3. Does the patient with falciparum malaria come from a chloroquine-resistant
area? 4. Does the patient have mild, moderate, or severe falciparum malaria?
Treatment regimens: http://www.cdc.gov/malaria/resources/pdf/treatmenttable.pdf

6
Uncomplicated Disease (oral Rx)
*Complicated Disease (parenteral Rx)
**Drug-sensitive Malaria
Chloroquine Hydroxychloroquine
Quinidine + Doxycycline, Tetracycline, or Clindamycin Artesunate†, followed by Atovaquone/Proguanil, Doxycycline/Clindamycin, or Mefloquine Chloroquine
¶
Drug-resistant Malaria
Atovaquone/Proguanil Artemether/Lumefantrine Quinine + Doxycycline, Tetracycline, or Clindamycin Mefloquine
Quinidine + Doxycycline, Tetracycline, or Clindamycin Artesunate†, followed by Atovaquone/Proguanil, Doxycycline/Clindamycin, or Mefloquine
* Complicated disease => severe malaria (e.g., cerebral malaria, renal failure, ARDS, etc.) ** Terminal treatment with Primaquine is usually indicated for relapsing malaria (P. vivax, P. ovale) to prevent relapse (screen for G6PD-deficiency to avoid hemolytic anemia) † Investigational New Drug (IND): contact CDC for information
¶ Parenteral Chloroquine not available in the US; use parenteral Quinidine for cases of severe malaria, even if drug-
sensitive
indications for exchange blood transfusions: o presumed non-immune o severe disease (e.g., cerebral, ARF, ARDS) o parasitemia > 10% o failure to respond to 12-24 optimal therapy o HIV, hepatitis virus screened, compatible blood available o facilities for exchange available
Prevention:
see CDC website: http://www.cdc.gov/malaria/travelers/country_table/a.html o Awareness: know about the risk of malaria o Bites by mosquitoes: prevent or avoid o Compliance with appropriate chemoprophylaxis o Diagnose breakthrough malaria swiftly and obtain treatment promptly
7
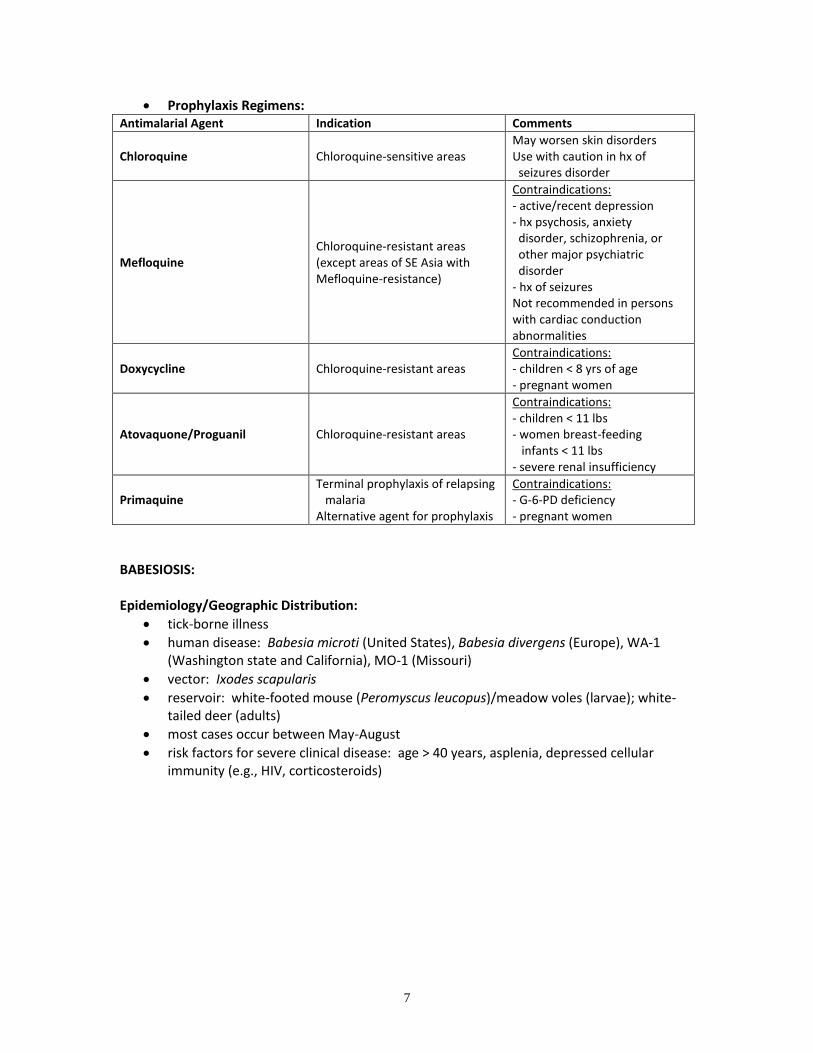
Prophylaxis Regimens: Antimalarial Agent Indication Comments
Chloroquine Chloroquine-sensitive areas May worsen skin disorders Use with caution in hx of seizures disorder
Mefloquine Chloroquine-resistant areas (except areas of SE Asia with Mefloquine-resistance)
Contraindications: - active/recent depression - hx psychosis, anxiety disorder, schizophrenia, or other major psychiatric disorder - hx of seizures Not recommended in persons with cardiac conduction abnormalities
Doxycycline Chloroquine-resistant areas Contraindications: - children < 8 yrs of age - pregnant women
Atovaquone/Proguanil Chloroquine-resistant areas
Contraindications: - children < 11 lbs - women breast-feeding infants < 11 lbs - severe renal insufficiency
Primaquine Terminal prophylaxis of relapsing malaria Alternative agent for prophylaxis
Contraindications: - G-6-PD deficiency - pregnant women
BABESIOSIS: Epidemiology/Geographic Distribution:
tick-borne illness
human disease: Babesia microti (United States), Babesia divergens (Europe), WA-1 (Washington state and California), MO-1 (Missouri)
vector: Ixodes scapularis
reservoir: white-footed mouse (Peromyscus leucopus)/meadow voles (larvae); white-tailed deer (adults)
most cases occur between May-August
risk factors for severe clinical disease: age > 40 years, asplenia, depressed cellular immunity (e.g., HIV, corticosteroids)

8
Parasitology/Life Cycle: best understood in B. microti, see diagram Clinical Manifestations:
suspect in travelers to endemic areas, even without tick bite history
incubation: ~ 1-3 weeks; 6-9 weeks for post-transfusion cases
asymptomatic or mildly symptomatic (flu-like illness)
immunodeficient hosts may have a more severe disease (DIC, hypotension, shock, CHF, renal failure, ARDS)
Diagnosis:
blood smear: round, oval, or pear-shaped intraerythrocytic parasites seen on Wright or Giemsa stain on thin smear
PCR amplification of babesial DNA Treatment:
antimicrobial agents: o Quinine + Clindamycin 7-10 days o Atovaquone + Azithromycin x 7 days
exchange transfusion for severe babesiosis o high-grade parasitemia (≥ 10%) o significant hemolysis o renal/hepatic/pulmonary compromise
Prevention:
insect/arthropod repellents: Permethrin-based formulations, DEET (diethyltoluamide)
tick avoidance/surveillance

9
TYPHOID FEVER: Epidemiology/Geographic Distribution:
356 reported cases in the US in 2003
~ 75% of cases related to international travel during preceding 6 weeks
transmission is human-to-human: o contaminated food/water o raw fruit/vegetables (especially where night soil used) o shellfish (contaminated by raw sewage)
etiologic agents: Salmonella typhi; Salmonella paratyphi A, B, or C
endemic areas: Papua New Guinea, India, SE Asia, Middle East, Africa, Central/South America
Clinical Manifestations:
Incubation: 10-20 days (3-56 days); Paratyphoid (1-10 days)
Natural history of untreated disease o Week 1: non-specific symptoms
rising remittent fever, headache, malaise, constipation, mild cough o Week 2: toxicity, apathy, high sustained fever
slight abdominal distention, hepatosplenomegaly common (~ 50%) rose spots:
2-4 mm pink papules, fade with pressure; upper abdomen, lower chest
appear days 7-12 of infection; may be culture positive o Week 3: continued illness, more toxicity, weight loss common
continuous high fever with delirium abdominal distention, diarrhea, weakness, tachypnea, feeble pulse toxemia/myocarditis/intestinal hemorrhage/perforation => death
o Week 4: fever, mental status, abdominal distention slowly improving prolonged convalescence
other findings: o relative bradycardia (pulse-temperature dissociation) seen in less than 50% o leukopenia with neutropenia common
Diagnosis:
Cultures: o blood, bone marrow, rose spot, stool, urine o string test cultures may be helpful o chronic stool carriage may occur
Treatment:
- fluoroquinolones and 3 generation cephalosporins presently drugs of choice - treat for 7-14 days - corticosteroids may be useful in cases with associated altered mental status and shock

10
TICK TYPHUS/AFRICAN TICK BITE FEVER: Epidemiology:
Geographical Distribution: o Rickettsia africae: South Africa, Zimbabwe
Hosts: o Arthropod vectors: Ticks (Amblyomma hebraeum) o Vertebrate reservoirs: cattle, hippopotamus, rhinoceros
Clinical Manifestations:
Incubation: 5-7 days
Eschar formation typically at site of infectious tick bite with regional lymphadenopathy
Fever, headache, malaise, conjunctival injection
Rash: o generalized, erythematous, maculopapular rash o most of body including palms, soles, and often face o may be hemorrhagic in severe disease
Complications, sequelae unusual Diagnosis: Serology - IFA, Latex agglutination, EIA, CFT Treatment:
Doxycycline 200 mg/d
Tetracycline 25 mg/kg/d
Chloramphenicol 2 g/d DENGUE FEVER: Epidemiology/Etiologic Agent:
single-stranded RNA Flavivirus
four serotypes (DEN-1 => DEN-4)
distribution: o widespread distribution throughout almost all tropical countries o 2.5 billion inhabitants at risk; > 100 million cases each year o an important disease seen in returned travelers
transmission: o vector: mosquito Aedes aegypti o breeds in relatively clean water usually stored for drinking or washing
Clinical Manifestations:
three overlapping clinical syndromes: o Undifferentiated fever:
occurs in young children a mild febrile illness lasting 1-3 days, often with upper respiratory signs
o Dengue fever syndrome: occurs in adolescents and adults incubation: 3-8 days sudden onset of fever (biphasic) with chills, severe headache
11
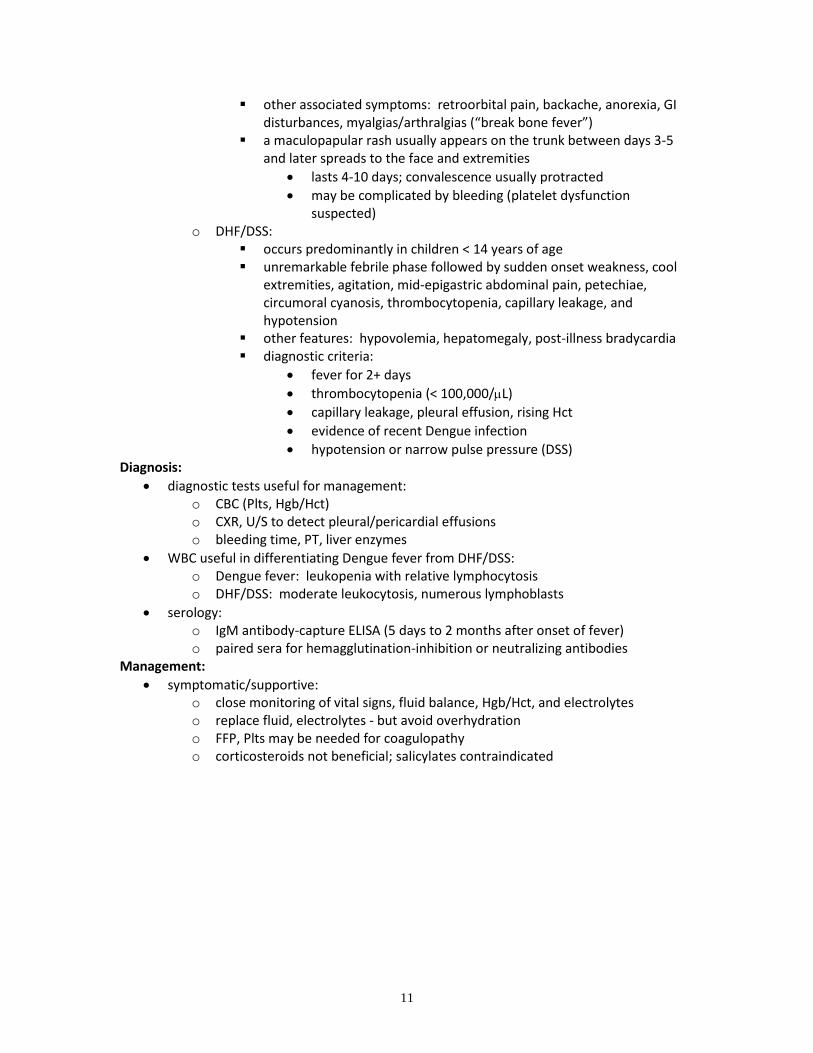
other associated symptoms: retroorbital pain, backache, anorexia, GI disturbances, myalgias/arthralgias (“break bone fever”)
a maculopapular rash usually appears on the trunk between days 3-5 and later spreads to the face and extremities
lasts 4-10 days; convalescence usually protracted
may be complicated by bleeding (platelet dysfunction suspected)
o DHF/DSS: occurs predominantly in children < 14 years of age unremarkable febrile phase followed by sudden onset weakness, cool
extremities, agitation, mid-epigastric abdominal pain, petechiae, circumoral cyanosis, thrombocytopenia, capillary leakage, and hypotension
other features: hypovolemia, hepatomegaly, post-illness bradycardia diagnostic criteria:
fever for 2+ days
thrombocytopenia (< 100,000/L)
capillary leakage, pleural effusion, rising Hct
evidence of recent Dengue infection
hypotension or narrow pulse pressure (DSS) Diagnosis:
diagnostic tests useful for management: o CBC (Plts, Hgb/Hct) o CXR, U/S to detect pleural/pericardial effusions o bleeding time, PT, liver enzymes
WBC useful in differentiating Dengue fever from DHF/DSS: o Dengue fever: leukopenia with relative lymphocytosis o DHF/DSS: moderate leukocytosis, numerous lymphoblasts
serology: o IgM antibody-capture ELISA (5 days to 2 months after onset of fever) o paired sera for hemagglutination-inhibition or neutralizing antibodies
Management:
symptomatic/supportive: o close monitoring of vital signs, fluid balance, Hgb/Hct, and electrolytes o replace fluid, electrolytes - but avoid overhydration o FFP, Plts may be needed for coagulopathy o corticosteroids not beneficial; salicylates contraindicated

12
AMEBIC LIVER ABSCESS: Epidemiology:
organism: Entamoeba histolytica
most infection/morbidity/mortality occurs in Central/South America, Africa, India
Risk factors for severe disease: neonates/children, pregnancy, post-partum, corticosteroids, malignancy, malnutrition
liver abscess is the most common form of extraintestinal amebiasis
adults >> children; M >> F; mortality < 1% in adults, up to 26% in children
patient population younger than in pyogenic liver abscess Life Cycle:
Clinical Manifestations:
presentation: o in returned travelers - symptoms occur within 5 months in 95% o fever (75-98%), RUQ pain < 10 days duration o pain: radiation to R shoulder, epigastric, pleuritic, intercostals o < 50% have an enlarged, painful liver o < 30% have active diarrhea before presentation o L-sided abscess: L-sided abdominal pain, L shoulder pain o rales R base, jaundice unusual (10-25%)

13
laboratory Data: o leukocytosis without eosinophilia; WBC > 10 x 109/L (75%) o mild anemia ~ 50% (more common in chronic presentation) o Alk phos (80%), ESR, ALT/AST in severe disease
complications: o rupture into pleural space/lung parenchyma (15%) => 6% mortality o rupture into peritoneal cavity (2-7%) => 18% mortality o rupture into pericardial space (< 1%) => 30% mortality
Diagnosis:
clinical Diagnosis
imaging techniques: Ultrasound, Radioisotope scans, CT, MRI o single R lobe liver lesion (70-80%) o L lobe liver lesion (5-21%) o multiple lesions can also occur
serology: o ~ 95% sensitivity, false-negatives occur during 1st week of symptoms o ELISA, IHA, CIE
Others: o Stool microscopy: < 50% yield o Abscess aspiration: “anchovy sauce”, trophozoites rare o X-rays: R hemidiaphragm, R costophrenic blunting
Treatment:
Metronidazole 750-800 mg tid x 10 days -or- Tinidazole 2 g qd x 3-5 days
other agents: Chloroquine, Dehydroemetine
follow-up above treatment with luminal agents to eradicate cysts: o Paromomycin 30 mg/kg/d in 3 divided doses x 10 days o Diiodohydroxyquin (iodoquinol) 650 mg tid x 20 days o Diloxanide furoate 500 mg tid x 10 days
recheck stools for asymptomatic cyst carriers 6 weeks after treatment
follow-up imaging not helpful: liver lesions persist for a long time STRONGYLOIDIASIS: Epidemiology:
widespread distribution in virtually all tropical and subtropical regions of the world
infection associated with poor sanitation and moist, temperate climates Geographic Distribution: see map

14
Parasitology/Life Cycle:
Autoinfection: a crucial differentiating characteristic o a small portion of rhabditiform larvae molt within the host’s intestine into the
filariform stage; penetrating the colonic wall or perianal skin, completing an internal cycle
Clinical Manifestations:
acute infection: o local reaction at entry site, pulmonary symptoms (from migrating larvae) o GI symptoms (diarrhea, constipation, anorexia, abdominal pain)
chronic infection: most often asymptomatic; irregular recurrence for years o GI symptoms, pruritus ani o dermatologic manifestations: urticaria, larva currens (“running” larva) o classic triad: urticaria, abdominal pain, diarrhea
hyperinfection/disseminated infection: o accelerated autoinfection – usually due to an altered immune system
(corticosteroids, hematologic malignancies, organ transplantation, HTLV-1, HIV, hypogammaglobulinemia, malnutrition)
o development/exacerbation of GI and pulmonary symptoms o increased numbers of larvae in stool/sputum o organisms may be confined (hyperinfection) or migrate beyond the range of the
pulmonary autoinfective cycle (dissemination) o GNR sepsis via “piggy-backing” of GNR/GPC/Candida on migrating larvae o mortality > 50%

15
Diagnosis:
unexplained eosinophilia may be the only clue
stool examination: problematic due to poor sensitivity
serology: ELISA testing
hyperinfection usually relatively easy to diagnose Treatment:
agents: o Ivermectin (drug of choice) o Albendazole o Thiabendazole (effective but significant associated toxicity)
longer course of treatment required for hyperinfection syndrome LOIASIS: Geographical Distribution: West/Central Africa Etiologic Agent: Loa loa Life Cycle/Transmission: see life cycle diagram
Vector: Chrysops fly
Reservoir: infected humans
Adult worms live/move around in connective tissues of reservoir hosts
Microfilariae: found in the peripheral blood, exhibit diurnal periodicity

16
Clinical Presentations:
Calabar Swellings: painless, non-pitting swelling of wrists/ankles lasting hours to days - may recur for years
adult worms migrating through the conjunctiva or skin
hypereosinophilia (may be > 20,000/L)
others: fatigue, arthralgias, localized abscess, meningoencephalitis Diagnosis:
day blood films to visualize microfilariae (use concentration techniques)
removal of adult worms from skin/conjunctivae Treatment:
Diethylcarbamazine (DEC): o dose: 5-10 mg/kg/d divided in 3 doses x 2-4 weeks o repeat treatment may be required for cure o side effects: fever, malaise, angioedema, pruritus o Precautions:
patients with significant microfilaremia (> 5000 microfilariae/mL)
small dose DEC/Ivermectin under corticosteroid cover
Mebendazole pretreatment (100-500 mg tid x 28 days)
pretreatment plasmapheresis of microfilariae beware of possible coinfection with Onchocerciasis
RABIES: Epidemiology/Virology:
almost all cases are transmitted from rabid animals through a bite
rarely transmission occurs from non-bite exposure or tissue transplantation
dogs account for 90% or more of reported cases in developing countries
since the late 1970s, wild animals have emerged as the source of human disease in the US: bats, raccoons, skunks, foxes
since the 1980s, bat variant rabies viruses have emerged as the dominant source associated with indigenous human deaths in the US
family Rhabdoviridae, genus Lyssavirus, ss-RNA virus Clinical Manifestations:
incubation: 1-3 months average (range 10 days to more than 1 year)
after initial symptoms => progressive worsening encephalopathy and death
classic forms: o encephalitic (furious) rabies:
hydrophobia, aerophobia, pharyngeal spasms, hyperactivity 80% of patients
o paralytic (dumb) rabies: quadriparesis with sphincter involvement, mimicking Guillain-Barré
syndrome little evidence of cerebral involvement until late in the course 20% of patients
17
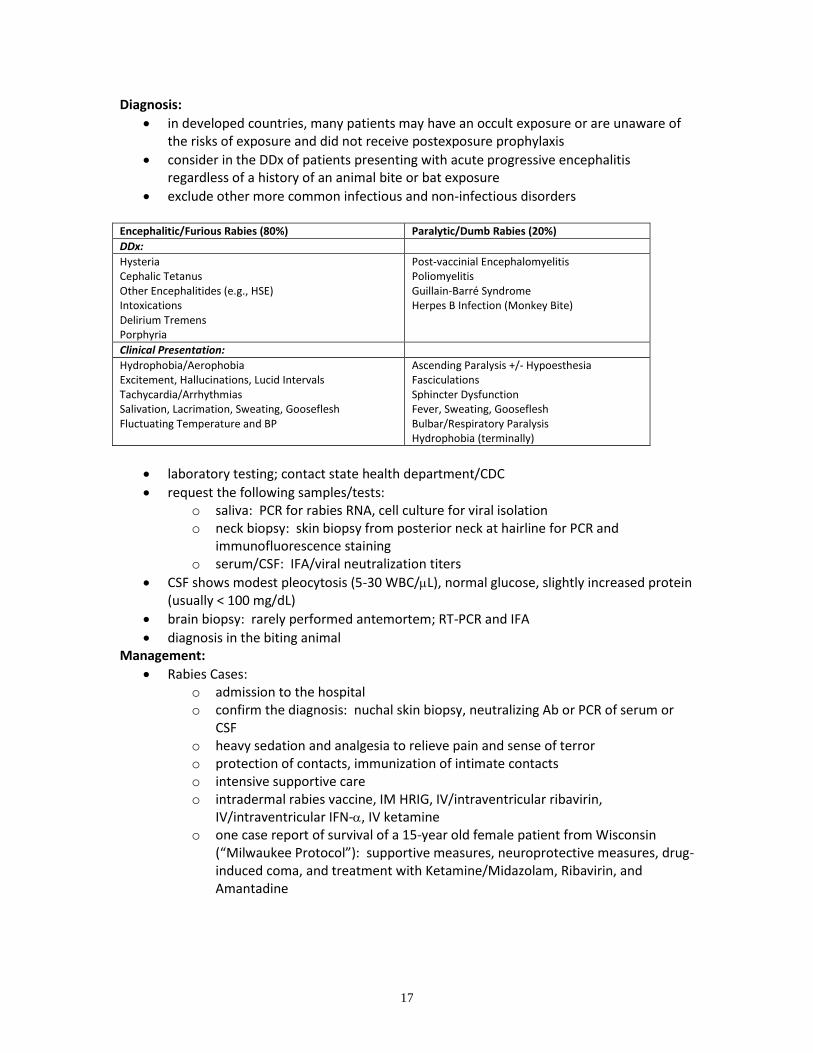
Diagnosis:
in developed countries, many patients may have an occult exposure or are unaware of the risks of exposure and did not receive postexposure prophylaxis
consider in the DDx of patients presenting with acute progressive encephalitis regardless of a history of an animal bite or bat exposure
exclude other more common infectious and non-infectious disorders Encephalitic/Furious Rabies (80%) Paralytic/Dumb Rabies (20%)
DDx:
Hysteria Cephalic Tetanus Other Encephalitides (e.g., HSE) Intoxications Delirium Tremens Porphyria
Post-vaccinial Encephalomyelitis Poliomyelitis Guillain-Barré Syndrome Herpes B Infection (Monkey Bite)
Clinical Presentation:
Hydrophobia/Aerophobia Excitement, Hallucinations, Lucid Intervals Tachycardia/Arrhythmias Salivation, Lacrimation, Sweating, Gooseflesh Fluctuating Temperature and BP
Ascending Paralysis +/- Hypoesthesia Fasciculations Sphincter Dysfunction Fever, Sweating, Gooseflesh Bulbar/Respiratory Paralysis Hydrophobia (terminally)
laboratory testing; contact state health department/CDC
request the following samples/tests: o saliva: PCR for rabies RNA, cell culture for viral isolation o neck biopsy: skin biopsy from posterior neck at hairline for PCR and
immunofluorescence staining o serum/CSF: IFA/viral neutralization titers
CSF shows modest pleocytosis (5-30 WBC/L), normal glucose, slightly increased protein (usually < 100 mg/dL)
brain biopsy: rarely performed antemortem; RT-PCR and IFA
diagnosis in the biting animal Management:
Rabies Cases: o admission to the hospital o confirm the diagnosis: nuchal skin biopsy, neutralizing Ab or PCR of serum or
CSF o heavy sedation and analgesia to relieve pain and sense of terror o protection of contacts, immunization of intimate contacts o intensive supportive care o intradermal rabies vaccine, IM HRIG, IV/intraventricular ribavirin,
IV/intraventricular IFN-, IV ketamine o one case report of survival of a 15-year old female patient from Wisconsin
(“Milwaukee Protocol”): supportive measures, neuroprotective measures, drug-induced coma, and treatment with Ketamine/Midazolam, Ribavirin, and Amantadine

18
Prevention:
vaccination
Post-exposure prophylaxis (not previously vaccinated): Treatment Regimen*
Local Wound Cleansing
Immediate thorough cleansing with soap and water
Human Rabies Immune Globulin (HRIG) 20 IU per kg body weight. Infiltrate as much of the full dose as possible into and around the wound. Administer the remainder intramuscularly at an anatomical site distant from vaccine administration
Vaccine 1.0 mL of Human Diploid Cell Vaccine (HDCV), Rabies Vaccine Adsorbed (RVA), or Purified Chick Embryo Cell Culture (PCEC) vaccine administered intramuscularly (deltoid area
†) on days 0, 3, 7, 14, and 28
‡
* These regimens are applicable for all age groups † The deltoid area is the only acceptable site of vaccination for adults and older children ‡ A four dose schedule can be used in patients who are not immunocompromised
MYIASIS: Geographical Distribution/Etiologic Agents:
Cordylobia anthropophaga: sub-Saharan Africa
Dermatobia hominis: Central & South America Life Cycle/Transmission:
C. anthropophaga: o fly eggs laid on clothing and linen o eggs hatch (activated by warmth, vibration) o larvae penetrate intact skin, develop in subcutaneous tissue, forming swellings
after 8-12 days o larvae later emerge from tissue, pupate, develop into adults
D. hominis: o fly eggs laid on other insects o when warmth is sensed (near host) eggs hatch o larvae penetrate host skin, a small nodule develops, larval development takes 6-
12 weeks o larvae later emerge, pupate, develop into adults
Prevention/Treatment:
C. anthropophaga: o iron clothes, linen, towels on both sides (to kill eggs) o apply vaseline, Canadian bacon, etc., larvae will emerge when suffocated o secondary infection common, antibiotics often required
D. hominis: o early (1st stage) larvae easy to remove o later stage larvae may require surgical removal

19
CYCLOSPORA: Epidemiology:
Cyclospora cayetanensis: coccidian, unicellular protozoan parasite
widely distributed geographically
a cause of prolonged travelers diarrhea
reported outbreaks: o Nepal - contaminated water o US outbreaks from 1995-2000 were traced to contaminated Guatemalan
raspberries o other contaminated produce: mesclun lettuce (1997), basil seasoning (1997,
1999), Guatemalan snow peas (2004) Life Cycle:
Clinical Manifestations:
incubation: ~ 7 days
diarrhea, flu-like symptoms, GI symptoms (flatulence, burping), fatigue, malaise
symptoms may be prolonged, especially in immunosuppressed (e.g., AIDS) Diagnosis:
stool examination - oocysts stain with modified acid-fast stains
oocysts can be distinguished from other coccidian parasites by their size (8-10 m) in comparison with cryptosporidia (4-6 m)

20
Treatment:
TMP-SMX DS 1 tab bid x 7 days
HIV-infected patients may require higher doses and maintenance therapy CYSTICERCOSIS: Epidemiology:
~ 50 million worldwide infections; most common parasitic infection of the brain
formerly common worldwide, wherever man/pigs coexisted
present areas of high prevalence: Central/South America (especially Mexico City), South Asia, China, selected areas in Africa
generally not seen in Islamic countries in SW Asia, N Africa
neurocysticercosis causes seizures in up to ~ 2-5% of emergency departments where large populations of immigrants are seen
Life Cycle/Transmission: Taenia solium
human disease transmitted by oral-fecal route
eggs ingested => hatch/develop into invasive larvae (oncospheres) => migrate across intestinal wall => disseminate in bloodstream preferentially to subcutaneous tissue, muscle, CNS
external autoinfection may occur
ingestion of pork is not necessary to develop cysticercosis

21
Clinical Manifestations:
neurocysticercosis: principal clinical problem o the majority of patients (~ 80%) are probably asymptomatic o parenchymal brain cysts: epilepsy, focal neurological deficits o meningeal cysts: chronic/relapsing meningitis, hydrocephalus o numerous cysts +/- inflammation: subacute encephalitis, increased intracranial
pressure, ultimately hydrocephalus o ventricular cysts: hydrocephalus, sometimes intermittent o spinal disease: various spinal cord syndromes, paraplegia o ocular disease: scotomata, blindness
others: subcutaneous/intramuscular disease, cardiac disease Diagnosis:
clinical neurological findings usually non-specific
search for subcutaneous cysticerci on examination
radiographic studies: calcified lesions, small enhancing lesions +/- a central bright spot, ring-enhancing lesions, larger cystic lesions
serology: o variable sensitivity/specificity, limited by cross reactivity o CSF serology helpful in meningitis
Treatment:
remains highly controversial
asymptomatic calcified/granulomatous lesions: no treatment
parenchymal cysts +/- little inflammation: o chemotherapy accompanied by steroids (Prednisolone or Dexamethasone)
Albendazole 15 mg/kg/d x 15 days (8 days equally efficacious) Praziquantel 50 mg/kg/d x 15 days
ventricular/spinal/ocular disease: probably surgery, some data using antihelminthics (always shunt those with hydrocephalus)
acute encephalitis/ocular disease: corticosteroids
control epilepsy medically