treatment ofradiation-induced nodular...
TRANSCRIPT
Retrospective and prospective epidemiologicalstudies have shown that prior radiation exposure isan important factor in the development of thyroidcancer and multinodular goiter in adolescents andyoung adults (1 ) . In retrospective studies of youngpersons with thyroid cancer, a history of antecedentradiation therapy to the neck or upper chest canusually be elicited by specific questioning (2) . Inprospectivesurveysof selectedpopulationsof youngadults with known radiation exposure, the incidenceof neoplasticthyroid diseasecan be remarkablyhigh (1 ) . For example, in the 19 young MarshallIslanders whose thyroid glands were heavily irradiated during childhood by radioactive fission productsfrom a nuclear explosion in 1954, 15 or 78% developed nodular thyroid disease by 1967 (3) . Similarly, in a subgroup of persons in Rochester, NewYork, treated with x-rays in infancy for allegedthymic enlargement,almost 5% have developedthyroid cancer and 28% , nodular thyroid disease(4,5).
In studying the Rochester subgroup with a highrisk of developing nodular thyroid disease, the cmical managementof patientswith radiation-inducednodular lesions became an important consideration.The question that arose was whether all such lesionsshould be removed surgically or whether carefulfollowup alone or combined with suppressive thyroidtherapy would be sufficient. The present report dealswith the authors' experience with the clinical careof 29 patients in the Rochester series with radiationinduced nodular thyroid disease.
METHODS
Of the 105 young adults in the high-risk, thymusirradiated subgroup (5), 35 are known to have orto have had nodular goiters.All patientshad reported no thyroid problems on a mail questionnairein 1963. Twenty-nine of these patients are considered in this article; the other six have been lost tofollowup or have not been followed long enoughto merit inclusion in this study. Except for one glandthat was diffusely enlarged, the thyroid lesions in
all patients presented to palpation as solitary or multiple nodulesrangingin size from somethat werebarely palpable to one massive nodular goiter measuring 6 X 8 X 2 cm. Prior to start of therapy, allpatients were examined at least twice by the twosenior authors to check on the accuracy and reproducibility of the clinical findings. In each patientwith a palpably abnormal gland, the serum PB! and24-hr 131Juptake were determined, and a “scintiscan―of the gland was carried out. In all but one patient,there was no evidence of hypothyroidism.
In seven patients with nonfunctioning, fixed, stony,hard or rapidly enlarging nodules, surgery was performed. This was followed by suppressive therapywith L-thyroxin (0.2 mg daily) for 10 days; then,the daily dose was increased to 0.3 mg if the patienthad no toxic symptoms. Nineteen additional patientswith suppressive therapy were treated. without surgery. The remaining three patients who refusedtreatment were examined repeatedly several times ayear.
After 3 months of treatment with 0.3 mg L-thyroxin daily, the patients were reexamined to determine changes in the size of the gland and nodulesand to check for clinical evidence of toxicity. Thedose of 0.3 mg was well tolerated by all but onepatient whose daily dose had to be reduced to 0.2mg. If the thyroid lesions did not respond after 6months of therapy, the PB! and 1311uptake wererechecked to determine the degree of suppression ofthyroid function.
RESULTS
Surgery followed by suppressive therapy with thy
roxin (Table 1). Seven patients were treated surgically (Case 1603F in Table 3 was not included inthis group because of the long period of suppressivetherapy preceding surgery) . On the initial examination, the findingsin five patientswereconsistentwith
Received July 23, 1969; revision accepted Feb. 5, 1970.For reprints contact: Louis H. Hempelmann, The Uni
versity of Rochester School of Medicine and Dentistry, 260Crittenden Blvd., Rochester, N.Y. 14620.
496 JOURNAL OF NUCLEAR MEDICINE
TREATMENT OF RADIATION-INDUCED
NODULAR GOITERS
ZsoltG. de Papp,RalphA. Pincusand LouisH. Hempelmann
University of Rochester School of Medicine and Dentistry, Rochester, New York
by on February 6, 2020. For personal use only. jnm.snmjournals.org Downloaded from

CaseAgeMonthsNo/Sex(yr)Initial physical findings HistologyCurrent status postoperative
0347M 26 50 mo.
TABLE 1. SURGICALLYEXCISED NODULES*
Macrofollicularadenoma
Focal adenomatoushyperplasia
Colloid nodule andfollicular adenoma
Adenoma
Follicular adenomawith ossification
Adenomatous goiter
Papillary and follicubr carcinoma rt.lobe
New 4-cm cystic lesion 3 yr after thyroidectomy while on continuous suppression with Proloid 2 gr andL-thyroxin 0.2 mg; shrank to 3 cmon most recent exam
Not on thyroid for first 24 months postoperative; now on L-thyroxin 0.3mg; no new nodules
Private physician says no new nodules;1 gr thyroid
On 0.3 mg L.thyroxin, no palpablethyroid tissue
No thyroid treatment for first 40 monthspostoperative;on re-examination residual rt. lobe is enlarged; afterL-thyroxin therapy (0.3 mg daily)gland shrank
On 2 gr thyroid; only remnant of glandpalpable
On 0.3 mg L-thyroxin; no palpableresidual tissue; no metastases cvident
50-gm nodular gland, veryfirm, It. lower lobe nodule
1789F 17 Hard 0.8-cm nodule in rt.lobe
3024F 34 3-cm firm nodule in It. lobe.Nonfunctional on scan
164SF 26 3-cm firm nodule in rt lobe.Nonfunctional on scan
0368M 26 1.5-cm stony, hard nodulein It. lobe
1735M 24 Massive goiter > 125 gmpost-traumatic
0385M 31 Granular gland. Four yearslater, 2 cm stony, hardnodules in rt. lobe; soft3.5-cm nodule on left;both were nonfunctionalon scan.
60 mo.
10 mo.
27 mo.
58 mo.
39 mo.
20 mo.
* Nodules were functional on scintiscan unless otherwise indicated.
thoseof malignantdiseaseand, in the sixthpatient,an enormous goiter was present. The weight of theexcised thyroid tissue of the last patient exceeded125 gm. The lesions of all six patients proved to bebenign on histologic examination. In the seventhpatient (0385M), the initial examination revealed
a normal sized gland with multiple small lobulatedareas. Since no definite nodules or changes in consistency could be found, it was decided to followhim without therapy. The patient did not return forexamination by the authors for 4 years by whichtime two stony, hard, nonfunctioning nodules werepresent. A total thyroidectomy was performed anda papillar-follicular carcinoma was removed; therewas no evidence of metastasis. All patients weregiven levothyroxin to suppress function of the remaining thyroid tissue.
Repeated examination of five of the patients over
periods up to 60 months disclosed no recurrence ofthe nodular lesions. One female patient (Case 3024)did not return to us but her private physician reported that there was no recurrence of nodularity 10months after thyroidectomy. Three years after surgery, one patient (0374M) on suppressive therapy(Proloid 2 grains and thyroxin 0.2 mg), developed acystic lesion in the remnant of the thyroid gland.The cystic lesion transilluminated readily. Less than
1% of the 13lJ administered at this time was takenup by the gland indicating that thyroid function wascompletely suppressed. The patient refused a secondoperation.
Suppressive therapy without surgery. Nine patients
with solitary nodules, nine with multinodular glandsand one with a diffusely enlarged gland were treatedwith levothyroxin.
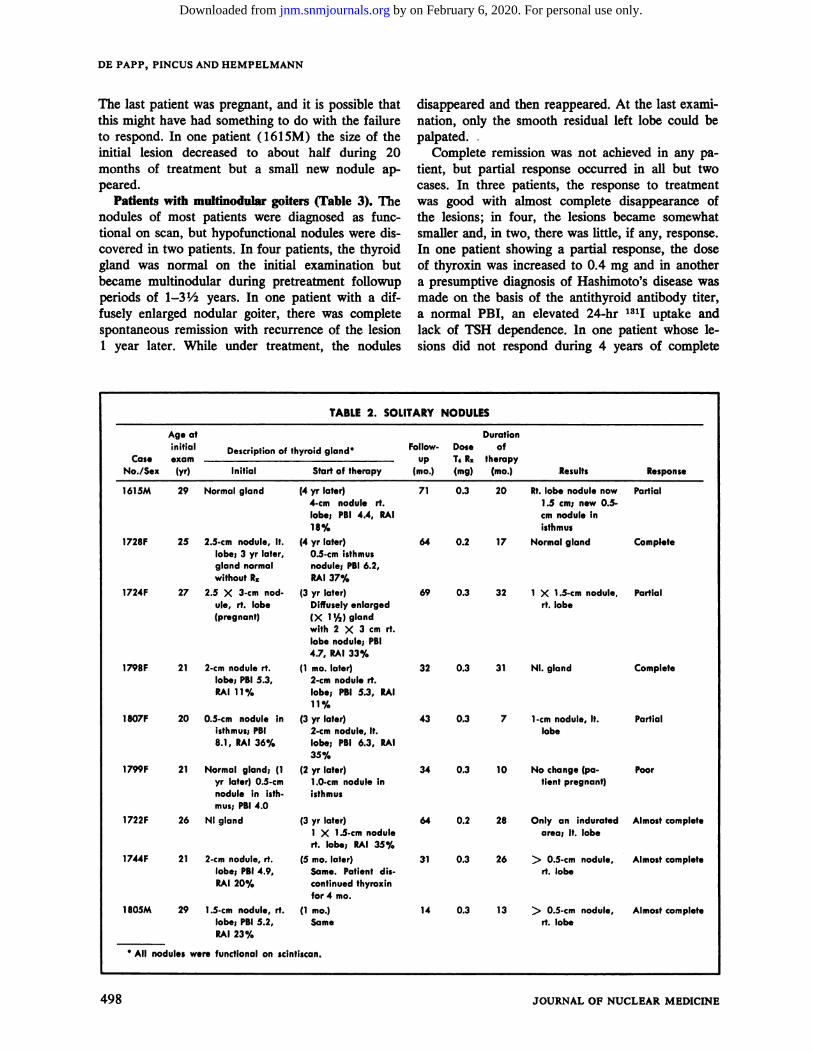
Patients with solitary nodules (Table 2). The nodules of all patients were “warm―on scintiscan. All
but the one patient mentioned above were able totolerate 0.3 mg of L-thyroxin daily. Even though thedaily dose was reduced to 0.2 mg, the thyroid nodules of this patient (Case 1722M) regressed almostcompletely. In one patient ( 1728F) there was acomplete spontaneous regression of a sizable noduleduring a 3-year observation period prior to treatment. When the lesions recurred 1 year later, treatment with thyroxin was begun.
The lesions in all but one patient responded totherapy by shrinking to less than half of the initialsize. In two patients under treatment, the lesionsdisappeared completely and in three others, almostcompletely. In three patients, the nodules were reduced in size to about half that observed at the onsetof treatment and, in one patient, the size of thenodulewas unchangedafter 10 monthsof therapy.
Volume 11, Number 8 497
by on February 6, 2020. For personal use only. jnm.snmjournals.org Downloaded from
AgeatDurationCase
No./Sexinitialexam(yr)Description
of thyroid glandFollowup
(mo.)DoseT@R1(mg)of
therapy(mo.) ResultsResponseInitialStart of therapy
1615M 29 Normal gland 71 0.3 20 Partial
DE PAPP, PINCUS AND HEMPELMANN
The last patient was pregnant, and it is possible thatthis might have had something to do with the failureto respond. In one patient ( 161 SM) the size of the
initial lesion decreased to about half during 20months of treatment but a small new nodule appeared.
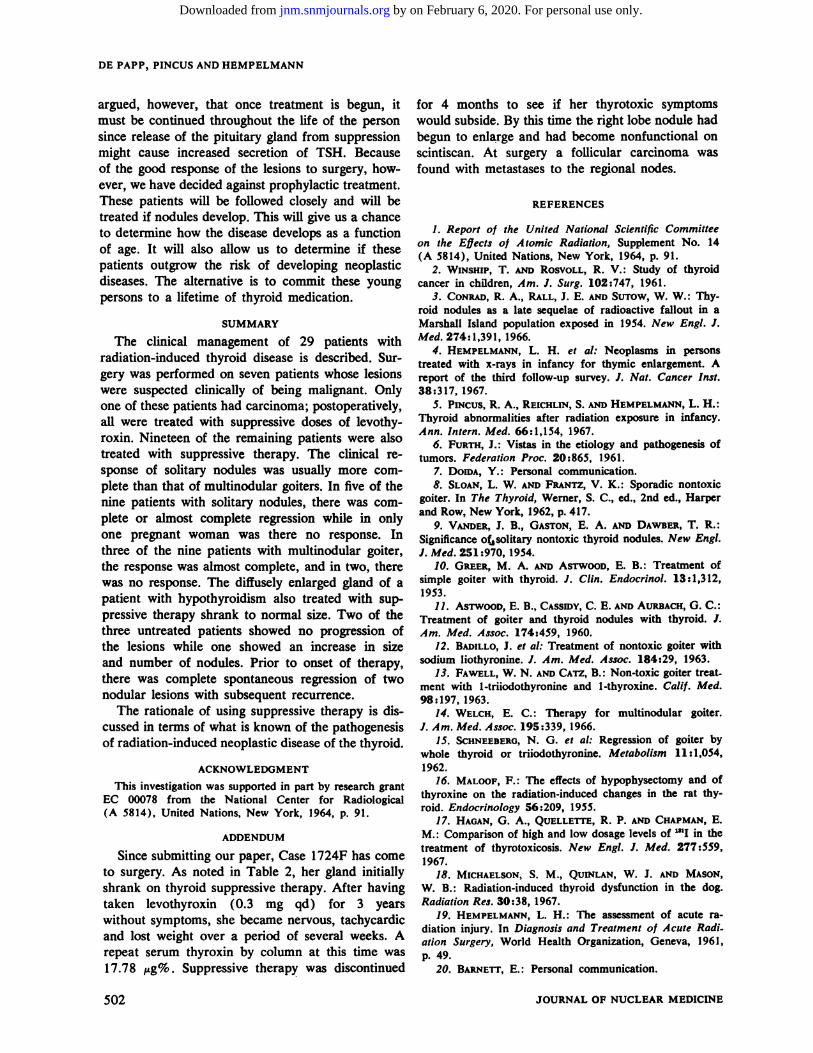
Patients with multinodular goiters (Table 3). The
nodulesof most patientswere diagnosedas functional on scan, but hypofunctional nodules were dis
covered in two patients. In four patients, the thyroidgland was normal on the initial examination butbecamemultinodularduring pretreatmentfollowupperiodsof 1—3½years. In one patient with a diffusely enlargednodular goiter, there was completespontaneous remission with recurrence of the lesion1 year later. While under treatment, the nodules
disappeared and then reappeared. At the last examination, only the smooth residual left lobe could be
palpated.Complete remission was not achieved in any pa
tient, but partial response occurred in all but twocases. In three patients, the response to treatmentwas good with almost complete disappearance ofthe lesions;in four, the lesionsbecamesomewhatsmaller and, in two, there was little, if any, response.
In one patient showing a partial response,the doseof thyroxinwas increasedto 0.4 mg and in anothera presumptive diagnosis of Hashimoto's disease wasmade on the basis of the antithyroid antibody titer,a normal PB!, an elevated 24-hr 131! uptake andlack of TSH dependence.in one patient whoselesions did not respond during 4 years of complete
(4 yr later)4-cm nodule rt.lobe; PBI 4.4, RAI18%
(4 yr later)0.5-cm isthmusnodule; PBI 6.2,RAI 37%
(3 yr later)Diffusely enlarged(X 1'@)glandwith 2 X 3 cm rt.lobe nodule; PSI4.7, RAI 33%
(1 mo. later)2-cm nodule rt.lobe; PBI 5.3, RAI11%
(3 yr later)2-cm nodule, It.lobe; PBI 6.3, RAI35%
(2 yr later)1.0-cm nodule inisthmus
(3 yr later)1 X 1.5-cm nodulert.lobe;RAI 35%
(5 mo.later)Same. Patient discontinuedthyroxinfor 4 mo.
(1 mo.)Same
Rt. lobe nodule now1.5 cm; new 0.5-cm nodule inisthmus
64 0.2 17 Normal gland
69 0.3 32 1 X 1.5-cm nodule.rt. lobe
32 0.3 31 NI. gland
43 0.3 7 1-cmnodule, It.lobe
34 0.3 10 No change (patient pregnant)
64 0.2 28 Only an induratedarea; It. lobe
31 0.3 26 > 0.5-cm nodule,rt.lobe
14 0.3 13 > 0.5-cm nodule,rt.lobe
1728F 25 2.5-cm nodule, It.lobe; 3 yr later,gland normalwithout R@
1724F 27 2.5 X 3.cm nodule, rt. lobe(pregnant)
1798F 21 2-cm nodule rt.lobe; PBI 5.3,RAI 11%
1807F 20 0.5-cm nodule Inisthmus; PBI8.1, RAI 36%
1799F 21 Normal gland; (1yr later) 0.5-cmnodule in isthmus;PBI4.0
1722F 26 NI gland
1744F 21 2-cm nodule, rt.lobe; PBI 4.9,RAI 20%
1805M 29 1.5-cm nodule, rt.lobe; PBI5.2,RAI 23°!.
Complete
Partial
Complete
Partial
Poor
Almostcomplete
Almostcomplete
Almostcomplete
. All nodules were functional on scintiscan.
498 JOURNAL OF NUCLEAR MEDICINE
TABLE 2. SOLITARY NODULES
by on February 6, 2020. For personal use only. jnm.snmjournals.org Downloaded from

AgeatDoseDurationCase
No/Sexinitialexam(yr)Descriptionof
thyroid gland°Followup
(mo.)L-thyroxin(mg)of
therapy(mo.) ResultsResponseInitialStart of therapy
1603F 36 62 0.3 48
TREATMENT OF RADIATION-INDUCED NODULAR GOITERS
4-cm nodule, It.lobe; 2 smallnodules in enl.rt.lobeRAI24%; all nodules @warm―
Treatmentstartedafter initial exam
(3 yr later)Rt.lobe,4cm;other nodules Unchanged; PBI, 3.2
mg; RAI 14%; onenodule hypofunctional
(3 yr later)Nodules, 2.3 cm inboth lobes
(3 yr later)3 distinctnodules
No change in nodules;completesuppressionoffunction; 3% RAIuptake
Poor;subtotalthyroidectomyafter 4 yr ofRx;multiplemicrofollicularand papillaryadenomaswith chronicinflammationand fibrosis
Partial
Partial (Hashimoto'sdisease) antithyroid A.B.,h512
1694M 20 2-cm nodule, ii.lobe; 1-cm nodules in It. lobeand isthmus Pt.refused treatment initially
1642M 18 Normal
1784F 26 Diffuselyenlargedwith nodules inboth lobes; PSI6.2, RAI 26%;all nodules
1794F 25 2-cm nodule, It.lobe; 0.5-cmnodule, isthmus;PBI6.3,RAI 24%
3375M 30 Normal
64 0.3 6 Nodule in it. lobe0.4 16 2.5 X 1-cm;
other nodulessmaller
47 0.3 14 Onlyslightreduction in glandsize; all nodulesstill prominent
68 0.3 33 After R. for 1 yrnodules disappeored but reappeared 1 yr later;only residual leftlobe now palpable, no nodules
60 0.3 3ot 20.2 6of 20.2 5
18
28 0.3 13 3 nodules < 1 cmIf. lobe; no nodules in rt. lobe
68 0.3 33 After 1 yr of R.,nodulesdisoppeored but reappeored 1 yr later;now no nodulesand only residualIt. lobe palpable
61 0.3 33 Only 0.5-cm nodulein isthmus remains
40 0.3 10 Hard nodule, < 1cm remainsinisthmus;? palpa.ble IgI.lymph node
1674F 29 Glanddiffuselyenlarged Xnormal
Poor
Almostcomplete
1711F 18 Normal gland (2 yr later)1 X 2-cm nodulein It. lobe; (3@/2yrlater) multiple nodules; PBI4.6;RAI 62%; no TSHresponse
1783F 23 Normal
No nodules
(1 yr later)1.5 X 2-cm nodulein each lobe; PSI7.0; RAI 23%; ii.nodule hypofunctional on scan
(2 yr later)Complete spontaneous regression;(3 yr later)sameason initial exam
(2 yr later)Same as on initialexam
(2 yr later)2 nodules1 X 1.5-cm in isthmus;PSI5.0, RAI21%;both nodules warm
Partial
Almostcomplete
Almostcomplete
Partial
S All nodules were functional except where indicated.
t Treatmentwas discontinuedby the patient@sobstetricianduring pregnancy.
Volume 11, Number 8 499
TABLE 3. MULTINODULAR GOITERS
by on February 6, 2020. For personal use only. jnm.snmjournals.org Downloaded from
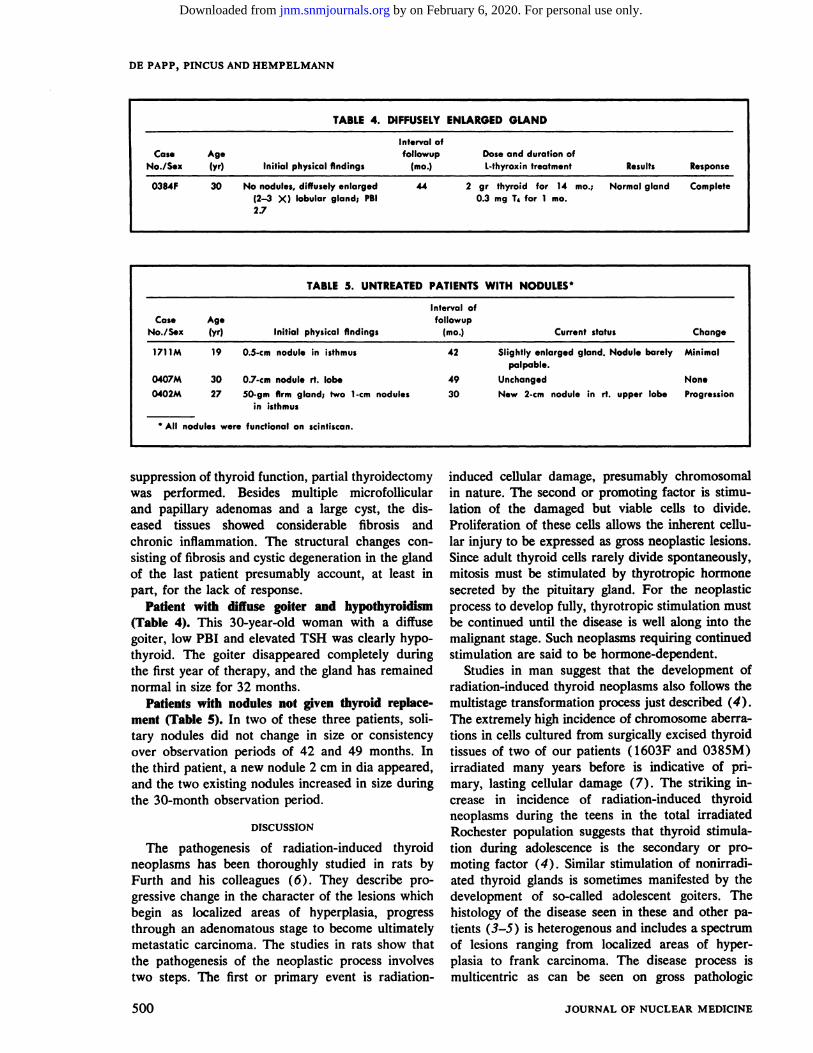
TABLE 4. DiFFUSELYENLARGED GLAND
Cas.AgeIntervalof
followupDose and durationofNo/Sex(yr)Initial physicalfindings (mo.)L-thyroxin treatment Results Response
0384F 30 No nodules,diffuselyenlarged 442 grthyroid for 14 mo.; Normal glandComplete(2—3X)lobulargland;PBI0.3mgT4 for1mo.2J
TABLE 5. UNTREATED PATIENTS WITH NODULES°
CaseAgeIntervalof
followupNo./Sex(yr)Initial physical findings (mo.)Current status Change
1711M190.5-cm nodule in isthmus42Slightly enlarged gland.NodulebarelyMinimalpalpable.0407M300.7-cm
nodule rt.lobe49UnchangedNone0402M2750-gmfirm gland; two 1-cm
in isthmusnodules30New2-cmnodule inrt.upperlobeProgression.
Allnodules were functional on scintiscan.
DE PAPP, PINCUS AND HEMPELMANN
induced cellular damage, presumably chromosomalin nature. The second or promoting factor is stimu
lation of the damagedbut viable cells to divide.Proliferation of these cells allows the inherent cellular injury to be expressedasgrossneoplasticlesions.Since adult thyroid cells rarely divide spontaneously,mitosis must be stimulated by thyrotropic hormonesecreted by the pituitary gland. For the neoplasticprocess to develop fully, thyrotropic stimulation must
be continued until the disease is well along into themalignant stage. Such neoplasms requiring continuedstimulation are said to be hormone-dependent.
Studies in man suggest that the development ofradiation-induced thyroid neoplasms also follows the
multistage transformation process just described (4).
The extremely high incidence of chromosome aberrations in cells cultured from surgically excised thyroidtissues of two of our patients ( 1603F and 0385M)
irradiated many years before is indicative of primary, lasting cellular damage (7). The striking in
crease in incidence of radiation-induced thyroidneoplasms during the teens in the total irradiatedRochester population suggests that thyroid stimulation during adolescence is the secondary or promoting factor (4) . Similar stimulation of nonirradi
ated thyroid glands is sometimes manifested by thedevelopment of so-called adolescent goiters. Thehistology of the disease seen in these and other patients (3—5)is heterogenous and includes a spectrumof lesionsranging from localized areas of hyperplasia to frank carcinoma. The disease process ismulticentric as can be seen on gross pathologic
suppression of thyroid function, partial thyroidectomywas performed. Besides multiple microfollicular
and papillary adenomas and a large cyst, the diseased tissues showed considerable fibrosis and
chronic inflammation.The structuralchangesconsisting of fibrosis and cystic degeneration in the glandof the last patient presumablyaccount,at least inpart, for the lack of response.
Patient with diffuse goiter and hypothyroidism(Table 4). This 30-year-old woman with a diffusegoiter, low PB! and elevated TSH was clearly hypothyroid. The goiter disappeared completely duringthe first year of therapy, and the gland has remainednormal in size for 32 months.
Patients with nodules not given thyroid replacement (Table 5). In two of these three patients, solitary nodules did not change in size or consistency
over observation periods of 42 and 49 months. Inthe third patient, a new nodule 2 cm in dia appeared,and the two existing nodules increased in size during
the 30-month observation period.
DISCUSSION
The pathogenesis of radiation-induced thyroidneoplasms has been thoroughly studied in rats byFurth and his colleagues (6). They describe progressive change in the character of the lesions whichbegin as localized areas of hyperplasia, progressthrough an adenomatous stage to become ultimatelymetastatic carcinoma. The studies in rats show thatthe pathogenesis of the neoplastic process involvestwo steps. The first or primary event is radiation
500 JOURNAL OF NUCLEAR MEDICINE
by on February 6, 2020. For personal use only. jnm.snmjournals.org Downloaded from

TREATMENT OF RADIATION-INDUCED NODULAR GOITERS
examination even in those lesions which cmnicallyappeared to be solitary nodules. Since the neoplasmsin these patients and in the total Rochester seriesresponded so well to treatment even when malignant,it may be speculated that the neoplastic process inyoung adults is still in the hormone-dependent stage.
In the present study, the question arose as totreatment of the nodular goiters in these youthful
subjects. Therapy was particularly important in thecase of the solitary nodules which, in the young, arereported to be malignant in many cases (8,9). Surgery was obviously indicated in those persons whoselesions were suspected of being malignant on clinicalgrounds, e.g., firm to palpation, fixed to adjacentstructures, unable to take up 1311or associated withenlarged regional lymph nodes. Alternative treatment of those lesions considered to be benign wasto follow the patient closely without treatment orwith suppression of thyroid function by adm@nistration of thyroid hormone. Because of the relativelybenign clinical course of all radiation-induced thyroid neoplasms and their good response to surgicalexcision, the first course, i.e., careful followup without treatment, did not seem unreasonable in selectedcases. Our experience in the present study, however,
indicated (see Table 5 and pretreatment period inTables 2 and 3) that usually, but not always (seeTable 5) , the existing nodules •in the untreated patients enlarged and new lesions appeared.
Although the alternative method of treatment,i.e., administration of thyroid hormone, has beenused in treating goiters since the turn of the century(9), suppressivetherapy of this type is often unsatisfactory in the treatment of sporadic nodulargoiter in older patients (10—15). In our youthfulpopulation with radiation-induced thyroid disease,however, there was reason to hope that replacementtherapy might cause regression by suppressing thyrotropinsecretionof the pituitary.The rationaleforthis type of therapy is : first, the role that thyrotropinstimulation is suspected of playing in the pathogenesisof the neoplastic disease and, second, the experiencein rats given 131!which make it seem likely that thyroid might prevent hyperplasia and subsequent neo
plastic transformation of the irradiated thyroid cells(16).
Our experience with these patients indicates thatsuppressive therapy is indeed useful in causing re
gression of thyroid nodules particularly when theypresent clinically as solitary lesions. In the earlystages, the disease process seems to be reversible asis indicated by the temporary spontaneous regression
of nodules in two patients. Suppressive therapy insuch early lesions caused complete clinical regression. In the more extensive and presumably more
advanced stages represented by multinodular goiter,the lesions frequently did not respond as well.Whether or not the thyroid cells at this stage havelost some of their dependency on thyrotropin stimulation is not known. It seems likely, however, that amajor factor in the failure of these lesions to respondis due to associated structural changes, e.g., fibrosis
and cystic degeneration, which is not affected bytreatment. Whether suppressive therapy will reducethe chance of malignant transformation of the lesionsis, of course, not known at this time. The develop
ment of a new nodule in Case 1615M and of a cystin Case 0347M while both patients were on thyroid
medication suggests that the treatment may not
block completelythe progressionof the disease.The case of hypothyroidism and presumed Hashi
moto's disease merit comment. That the large dosesof 131! used to treat hyperthyroidism can cause hypothyroidism in a substantial proportion of cases iswell known (17) . Even doses estimated to be 700—1,400 rads of beta and gamma rays in the Marshallese children exposed to fission products in 1954are presumed to be the cause of hypothyroidism intwo of the 19 children exposed before age 10 (3).
In adult dogs, clinical myxedema is reported todevelop several years after exposure of their upperbodies to x-ray exposures as low as 1,000 R (18).Similar partial body exposure of a man to radiationresulting from an accidental nuclear reaction wasalso followed by myxedema (19) . Therefore, the
hypothyroidism that developed in Case 0384F afterexposure to 800 R in infancy is compatible withother findings in irradiated man and animals. However, whether or not the development of Hashi
moto's diseasewas related to the x-ray treatmentis not known. This seems unlikely as analysis of
serum samples taken S years ago from the high risk
subgroup showed no abnormality of antithyroidtiter (20) . Also, the Marshallese patients showed
no abnormalities of antithyroid antibody titer.In conclusion, the matter of the prophylactic use
of suppressive therapy should be considered in allpersons with a high risk of developing nodulargoiters. In persons whose nodular lesions have beenexcised surgically, prophylactic use of thyroid hormone is clearly in order to prevent as far as possible regrowth of the non-neoplastic remnants orfurther neoplastic transformation of the gland. Inour patients with glands that are normal to palpation the issue is more complex. On theoretical
grounds, it can be argued that all of these subjectsshould have prophylactic treatment. Suppression ofthyroid function might prevent hyperplastic diseaseand, presumably,neoplastictransformationof theirradiated gland as it does in rats (10) . It can be
Volume 11, Number 8 501
by on February 6, 2020. For personal use only. jnm.snmjournals.org Downloaded from
DE PAPP, PINCUS AND HEMPELMANN
argued, however, that once treatment is begun, itmust be continued throughout the life of the person
since release of the pituitary gland from suppressionmight cause increased secretion of TSH. Becauseof the good response of the lesions to surgery, however, we have decided against prophylactic treatment.These patients will be followed closely and will betreated if nodules develop. This will give us a chance
to determine how the disease develops as a function
of age. It will also allow us to determine if thesepatients outgrow the risk of developing neoplasticdiseases. The alternative is to commit these young
personsto a lifetime of thyroid medication.
SUMMARY
The clinical management of 29 patients withradiation-induced thyroid disease is described. Surgery was performed on seven patients whose lesionswere suspected clinically of being malignant. Onlyone of these patients had carcinoma; postoperatively,all were treated with suppressive doses of levothyroxin. Nineteen of the remaining patients were alsotreated with suppressive therapy. The clinical response of solitary nodules was usually more complete than that of multinodular goiters. In five of thenine patients with solitary nodules, there was complete or almost complete regression while in only
one pregnant woman was there no response. Inthree of the nine patients with multinodular goiter,the response was almost complete, and in two, therewas no response. The diffusely enlarged gland of apatient with hypothyroidism also treated with suppressive therapy shrank to normal size. Two of the
three untreated patients showed no progression ofthe lesions while one showed an increase in sizeand number of nodules. Prior to onset of therapy,there was complete spontaneous regression of twonodular lesions with subsequent recurrence.
The rationale of using suppressive therapy is discussed in terms of what is known of the pathogenesisof radiation-induced neoplastic disease of the thyroid.
ACKNOWLEDGMENT
This investigation was supported in part by research grantEC 00078 from the National Center for Radiological(A 5814), United Nations, New York, 1964, p. 91.
ADDENDUM
Since submitting our paper, Case 1724F has come
to surgery. As noted in Table 2, her gland initiallyshrank on thyroid suppressive therapy. After havingtaken levothyroxin (0.3 mg qd) for 3 yearswithout symptoms, she became nervous, tachycardicand lost weight over a period of several weeks. Arepeat serum thyroxin by column at this time was17.78 /Lg%. Suppressive therapy was discontinued
for 4 months to see if her thyrotoxic symptomswould subside. By this time the right lobe nodule hadbegun to enlarge and had become nonfunctional onscintiscan. At surgery a follicular carcinoma was
found with metastases to the regional nodes.
REFERENCES
1. Report of the United National Scientific Committeeon the Effects of Atomic Radiation, Supplement No. 14(A 5814), United Nations, New York, 1964, p. 91.
2. WINSHIP, T. @i@wRosvoLL, R. V. : Study of thyroidcancer in children, Am. I. Surg. 102:747, 1961.
3. CONRAD, R. A., RALL, J. E. @i Strrow, W. W. : Thy
roid nodules as a late sequelae of radioactive fallout in aMarshall Island population exposed in 1954. New Engi. I.Med. 274:1,391, 1966.
4. HEMPELMANN,L. H. et a!: Neoplasms in personstreated with x-rays in infancy for thymic enlargement. Areport of the third follow-up survey. I. Nat. Cancer Inst.38:317, 1967.
5. PiNcus, R. A., REIcisuN, S. @NDHEMPELMANN, L. H.:Thyroid abnormalities after radiation exposure in infancy.Ann. Intern. Med. 66:1,154, 1967.
6. Fuim, I.: Vistas in the etiology and pathogenesisoftumors. Federation Proc. 20:865, 1961.
7. DomA, Y. : Personal communication.8. SLOAN, L. W. AND FRANTZ, V. K. : Sporadic nontoxic
goiter. In The Thyroid, Werner, S. C., ed., 2nd ed., Harperand Row,NewYork, 1962,p. 417.
9. VANDER,J. B., GASTON,E. A. ANDDAWBER,T. R.:Significance of@solitarynontoxic thyroid nodules. New Engi.I. Med. 251 :970, 1954.
10. GREEx, M. A. @NiASTWOOD, E. B.: Treatment ofsimple goiter with thyroid. I. Clin. Endocrinol. 13:1,312,1953.
11. As@rwooD,E. B., CASSIDY,C. E. ANDAURBACH,G. C.:Treatment of goiter and thyroid nodules with thyroid. I.Am. Med. Assoc. 174:459, 1960.
12. B@srnLLo,J. et a!: Treatment of nontoxic goiter withsodium liothyronine. I. Am. Med. Assoc. 184:29, 1963.
13. FAWELL, W. N. AND CA@rz, B. : Non-toxic goiter treat
ment with 1-triiodothyronine and 1-thyroxine. Calif. Med.98:197, 1963.
14. WELCH, E. C. : Therapy for multinodular goiter.
I. Am. Med. Assoc. 195:339, 1966.15. SCHNEEBERO,N. 0. et al: Regression of goiter by
whole thyroid or triiodothyroninc. Metabolism 11:1,054,1962.
16. MALOOF, F. : The effects of hypophysectomy and ofthyroxine on the radiation-induced changes in the rat thyroid. Endocrinology 56:209, 1955.
17. HAGAN,0. A., QUELLErrE, R. P. @imCHAPMAN,E.M. : Comparison of high and low dosage levels of @°‘Iin thetreatment of thyrotoxicosis. New Engl. I. Med. 277:559,1967.
18. MICHAELSON, S. M., QTJINLAN, W. J. AND MASON,
w. B.: Radiation-inducedthyroiddysfunctionin the dog.Radiation Res. 30:38, 1967.
19. HEMPELMANN, L. H. : The assessment of acute ra
diation injury. In Diagnosis and Treatment of Acute Radiation Surgery, World Health Organization, Geneva, 1961,p. 49.
20. BARNETr, E. : Personal communication.
502 JOURNAL OF NUCLEAR MEDICINE
by on February 6, 2020. For personal use only. jnm.snmjournals.org Downloaded from
1970;11:496-502.J Nucl Med. Zsolt G. de Papp, Ralph A. Pincus and Louis H. Hempelmann Treatment of Radiation-Induced Nodular Goiters
http://jnm.snmjournals.org/content/11/8/496This article and updated information are available at:
http://jnm.snmjournals.org/site/subscriptions/online.xhtml
Information about subscriptions to JNM can be found at:
http://jnm.snmjournals.org/site/misc/permission.xhtmlInformation about reproducing figures, tables, or other portions of this article can be found online at:
(Print ISSN: 0161-5505, Online ISSN: 2159-662X)1850 Samuel Morse Drive, Reston, VA 20190.SNMMI | Society of Nuclear Medicine and Molecular Imaging
is published monthly.The Journal of Nuclear Medicine
© Copyright 1970 SNMMI; all rights reserved.
by on February 6, 2020. For personal use only. jnm.snmjournals.org Downloaded from