treating trauma-related symptoms and substance disorders with evidence-based practices kevin...
TRANSCRIPT

Treating Trauma-Related Symptoms
and Substance Disorders with Evidence-Based Practices
Kevin Koffler, MA, LMFTClinical Director
Sunspire Health Desert Palms
Treating Trauma-Related Symptoms and Substance Disorders with Evidence Based Practices
• What are Evidence-Based Practices, and Why Do They Matter?
• What is trauma, how do we assess for it, and how does it present itself in our clients?
• How does trauma-informed treatment differ from traditional substance abuse treatment?
• An introduction to Seeking Safety

What Are Evidence Based Practices- And Why Do They Matter?

Evidence
• Facts, theory, or subject matter that support or refute the claim that a given practice produces a specific clinical outcome. Evidence may include research findings and expert or consensus opinions.
(“COCE,” 2007)
Evidence-Based Thinking
• A process by which diverse sources of information (research, theory, practice principles, practice Thinking guidelines, and clinical experience) are synthesized by a clinician, expert, or group of experts in order to identify or choose the optimal clinical approach for a given clinical situation.
(“COCE,” 2007)

Evidence-Based Practice
• A practice which, based on research findings and expert or consensus opinion about available evidence,
• Practice is expected to produce a specific clinical outcome (measurable change in client status).
(“COCE,” 2007)

The Goal of Evidence Based Practice
• The goal of EBP is the integration of: (a) clinical expertise/expert opinion, (b) external scientific evidence, and (c) client /patient/ caregiver perspectives to provide high-quality services reflecting the interests, values, needs, and choices of the clients we serve. Conceptually, the trilateral principles forming the bases for EBP can be represented through a simple figure:
(ASHA, 2015)
Figure 1: Trilateral Diagram (ASHA, 2015)

Fidelity
• Fidelity is the extent to which a treatment approach as actually implemented corresponds to the treatment strategy as designed. Following the initial design with high fidelity is expected to result in greater success in achievingdesired client outcomes than deviating from the design (i.e., having low fidelity).
(“COCE,” 2007)
E
EBP’S at a Treatment Level:At Sunspire Health Desert Palms We Use:
• Motivational Interviewing (MI)
• Cognitive Behavioral Therapy (CBT)
• Dialectical Behavioral Therapy (DBT)
• Illness Management and Recovery (IMR)
• Matrix Model (For Relapse Prevention)
• Eye Movement Desensitization And Reprocessing (EMDR)
• Seeking Safety (SS)

Trauma


Think of a time that was particularly stressful (but not traumatic) in your life. Revisit this period as an observer watching the events unfold and then ask yourself, “What made this time particularly stressful?” It is likely that a part of your answer will include the difficulty of managing one situation before another circumstance came along demanding your time. Stressful times denote being bombarded with many things at one time, perceived or actual, without sufficient time or ability to address them emotionally, cognitively, spiritually, and/or physically. The same goes for trauma—rapid exposure to numerous traumas, one after another, lessens one’s ability to process the event before the next onslaught. This creates a cumulative effect, making it more difficult to heal from any one trauma.


What is Trauma?
• The term “trauma” refers to experiences that cause intense physical and psychological stress reactions. It can refer to “a single event, multiple events, or a set of circumstances that is experienced by an individual as physically and emotionally harmful or threatening and that has lasting adverse effects on the individual’s physical, social, emotional, or spiritual wellbeing”
(SAMHSA, 2012, p. 2)
Fight, Flight or Freeze
• When a person experiences a traumatic event, all of the sights, sounds and smells in their environment get instantaneously paired with a surge of adrenaline, stress and fear, leading them to do one of three things –
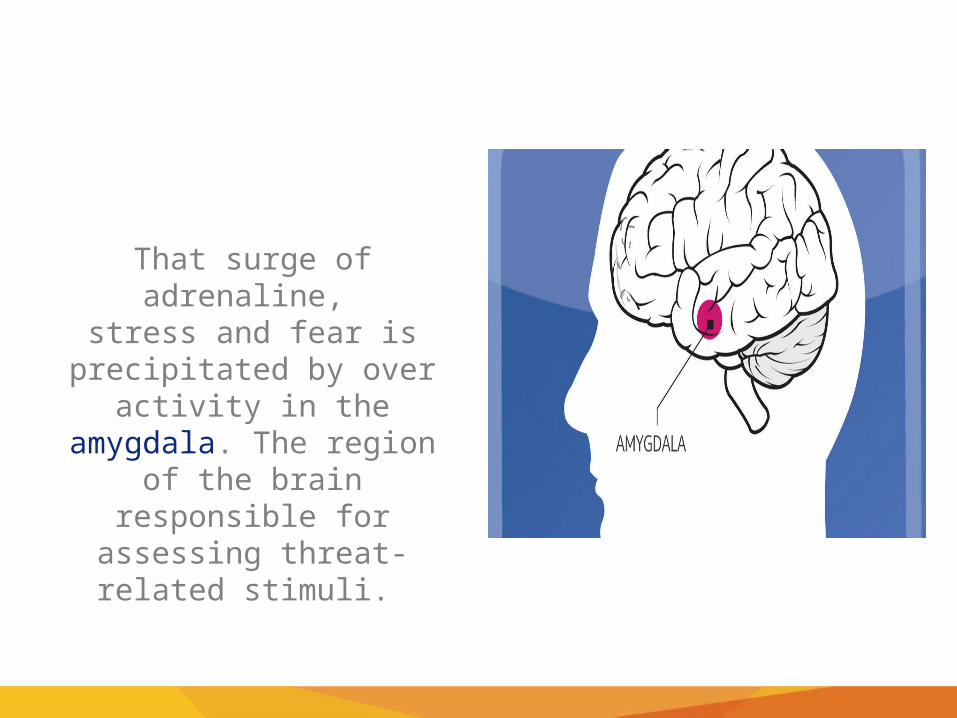
That surge of adrenaline, stress and fear is precipitated
by over activity in the amygdala. The region of the
brain responsible for assessing threat-related stimuli.
Consequently, when a person is exposed to one of the sights, sounds or smells they experienced during a
trauma, their amygdala interprets that as a threat and begins to overcompensate, sending a false signal to
the body letting it know it's in danger.

As a result of this process, a person may not understand why they suddenly feel anxious, or
fearful when they encounter a certain sight, sound or smell and they will likely go to great lengths to
avoid feeling that way.
How Do We Assess for Trauma
• Through doing standard trauma history profile to gather symptoms, problem behaviors and functional impairments utilizing the criteria listed in the DSM-5
• Through the use of outcome measure screening tools including the UCLA PTSD INDEX and the PCL-C
DSM-5 Diagnostic Criteria for PTSD Criterion A
Exposure to actual or threatened death, serious injury, or sexual violence in one (or more) of the following ways:
• Directly experiencing the traumatic event.
• Witnessing, in person, the event as it occurred to others.
• Learning that the traumatic event occurred to a close family member or friend. In cases of actual or threatened death of a family member or friend, the event must have been violent or accidental.
• Experiencing repeated or extreme exposure to aversive details of the traumatic event (e.g., first responders collecting human remains; police officers repeatedly exposed to details of child abuse).

DSM-5 Diagnostic Criteria for PTSD Cluster B
Presence of more than one of the following intrusion symptoms associated w/ the traumatic event(s), beginning after the traumatic event(s) has occurred:
• Recurrent, involuntary, & intrusive distressing memories of the event. • Repetitive play w/ trauma themes • Recurrent distressing dreams related to the event. • May have frightening dreams w/o recognizable content • Dissociative reactions (e.g., flashbacks) in which the individual feels/acts as
if the event were recurring. • Trauma-specific reenactment may occur in play • Psychological distress at cues resembling event. • Physiological reactions to cues resembling the event

:DSM-5 Diagnostic Criteria for
PTSD Cluster C
Persistent avoidance of stimuli associated w/ the traumatic event(s), beginning after the traumatic event(s) occurred, as evidenced by more than one of the following
• Avoidance of or efforts to avoid distressing memories, thoughts, or feelings about or closely associated with the traumatic event.
• Avoidance of or efforts to avoid external reminders (people, places, conversations, activities, objects, situations) that arouse distressing memories, thoughts, or feelings about or closely associated with the traumatic event.
:DSM-5 Diagnostic Criteria for
PTSD Cluster D
Negative alterations in cognitions & mood associated w/ the traumatic event(s), beginning or worsening after the traumatic event(s) occurred, as evidenced by more than two 2 of the following:
• Inability to remember an important aspect of the event (not due to head injury or substance use).
• Persistent & exaggerated negative beliefs or expectations about oneself, others, or the world (e.g., “I am bad,” “No one can be trusted”).
• Persistent, distorted cognitions about the cause or consequences of the event that lead the individual to blame himself/herself or others.
• Persistent negative emotional state (e.g., fear, anger, guilt, or shame).• Markedly diminished interest or participation in significant activities. • Feelings of detachment or estrangement from others. • Persistent inability to experience positive emotions

DSM-5 Diagnostic Criteria for PTSD Cluster E
Marked alterations in arousal & reactivity associated w/ the traumatic event(s), beginning or worsening after the traumatic event(s) occurred, as evidenced by more than two of the following:
• Irritable behavior & angry outbursts (w/ little or no provocation) typically expressed as verbal or physical aggression.
• Reckless or self-destructive behavior.
• Hypervigilance.
• Exaggerated startle response.
• Problems w/ concentration.
• Sleep disturbance

DSM-5 Diagnostic Criteria for PTSD
• Duration of the disturbance (Criteria B, C, D, & E) is more than 1 month.
• The disturbance causes clinically significant distress or impairment in social, occupational, or other important areas of functioning.
• The disturbance is not attributable to the physiological effects of a substance or other medical condition.

Since Clients Entering Treatment Can Be Poor Historians and/or are Avoiding Disclosure Due to Shame or Paranoid
Ideations, We Utilize the PCL-C
• It’s in the public domain, and doesn’t cost anything to use
• Provides standard measurements by having the patient answer a 17 item questionnaire
• Allows patients to disclose symptoms without discussing them in an interview
• Allows clinicians to measure progress made at reducing trauma-related symptoms more effectively.
IMMEDIATE AND DELAYED REACTIONS TO TRAUMA
Sources: Briere & Scott, 2006b; Foa, Stein, & McFarlane, 2006; Pietrzak, Goldstein, Southwick, & Grant, 2011.

Immediate Emotional Reactions
• Numbness and detachment Anxiety or severe fear
• Guilt (including survivor guilt) • Exhilaration as a result of surviving • Anger • Sadness • Helplessness • Feeling unreal; depersonalization (e.g., feeling as if you are watching
yourself) • Feeling out of control • Denial about self, discussion of traumatic events or reactions to them• Constriction of feelings
Delayed Emotional Reactions
• Irritability and/or hostility• Depression• Mood swings, instability• Anxiety (e.g., phobia, generalized anxiety)• Fear of trauma recurrence• Grief reactions• Shame • Feelings of fragility and/or vulnerability• Emotional detachment from anything that requires
emotional reactions

Immediate Physical Reactions
• Nausea and/or gastrointestinal distress
• Sweating or shivering
• Muscle tremors or uncontrollable shaking
• Elevated heartbeat, respiration, and blood pressure
• Extreme fatigue or exhaustion levels
• Greater startle responses
• Depersonalization
Delayed Physical Reactions
• Sleep disturbances, nightmares • Somatization • Faintness • Appetite and digestive changes • Lowered resistance to colds and infection• Persistent fatigue • Elevated levels of cortisol• Hyper arousal • Long-term health problems

Immediate Cognitive Reactions
• Difficulty concentrating
• Rumination or racing thoughts (e.g., replaying the traumatic event over and over again)
• Distortion of time and space (e.g., traumatic event may be perceived as if it was happening in slow motion, or a few seconds can be perceived as minutes)
• Memory problems (e.g., not being able to recall important aspects of the trauma)
• Strong identification with victims
Delayed Cognitive Reactions
• Intrusive memories or flashbacks • Reactivation of previous traumatic events • Self-blame • Preoccupation with event • Difficulty making decisions • Magical thinking: belief that certain behaviors, including avoidant
behavior, will protect against future trauma • Belief that feelings or memories are dangerous • Generalization of triggers (e.g., a person who experiences a home
invasion during the daytime may avoid being alone during the day) • Suicidal thinking

Immediate Behavioral Reactions
• Startled reaction • Restlessness • Sleep and appetite disturbances • Engagement in high-risk behaviors • Argumentative behavior • Increased use of alcohol, drugs, and tobacco• Withdrawal and apathy

Delayed Behavioral Reactions
• Avoidance of event reminders• Social relationship disturbances• Decreased activity level • Difficulty expressing oneself• Increased use of alcohol and drugs• Withdrawal

Immediate Existential Reactions
• Intense use of prayer • Restoration of faith in the goodness of others
(e.g., receiving help from others) • Loss of self-efficacy • Despair about humanity, particularly if the event was
intentional • Immediate disruption of life assumptions
(e.g., fairness, safety, goodness, predictability of life)

Delayed Existential Reactions
• Delayed Existential Reactions Questioning (e.g., “Why me?”) • Increased cynicism• Disillusionment • Increased self-confidence (e.g., “If I can survive this, I can survive
anything”) • Loss of purpose Renewed faith • Hopelessness • Reestablishing priorities • Redefining meaning and importance of life • Reworking life’s assumptions to accommodate the trauma (e.g.,
taking a self-defense class to reestablish a sense of safety

So What Can This Look Like for Someone in Treatment?

The following examples reflect some of the types of cognitive or
thought-process changes that can occur in response to traumatic stress.

Cognitive Errors
Misinterpreting a current situation as dangerous because it resembles, even
remotely, a previous trauma (e.g., a client overreacting to an overturned canoe in 8 inches of water, as if she and her paddle
companion would drown, due to her previous experience of nearly drowning
in a rip current 5 years earlier).

Triggers
A trigger is a stimulus that sets off a memory of a trauma or a specific portion of a
traumatic experience. Imagine you were trapped briefly in a car after an accident.
Then, several years later, you were unable to unlatch a lock after using a restroom stall;
you might have begun to feel a surge of panic reminiscent of the accident, even
though there were other avenues of escape from the stall.

Flashbacks

Flashbacks
A flashback is re experiencing a previous traumatic experience as if it were actually happening in that moment. It includes
reactions that often resemble the client’s reactions during the trauma. Flashback experiences are very brief and typically last only a few seconds, but the emotional aftereffects linger for
hours or longer. Flashbacks are commonly initiated by a trigger, but not necessarily. Sometimes, they occur out of the blue.
Other times, specific physical states increase a person’s vulnerability to re experiencing a trauma
Excessive or Inappropriate Guilt
Attempting to make sense cognitively and gain control over a traumatic experience by assuming responsibility
or possessing survivor’s guilt, because others who experienced the same trauma did not survive.
Trauma Induced Hallucinations or Delusions
Experiencing hallucinations and delusions that, although they are
biological in origin, contain cognitions that are congruent with
trauma content (e.g., a woman believes that a person stepping onto
her bus is her father, who had sexually abused her repeatedly as
child, because he wore shoes similar to those her
father once wore).
Intrusive Thoughts or Memories
Experiencing, without warning or desire, thoughts and memories associated with the
trauma. These intrusive thoughts and memories can easily trigger strong emotional and
behavioral reactions, as if the trauma was recurring in the present. The intrusive thoughts and memories can come rapidly, referred to as flooding, and can be disruptive at the time of
their occurrence. If an individual experiences a trigger, he or she may have an increase in
intrusive thoughts and memories for a while.

Foreshortened Future
Trauma can affect one’s beliefs about the future via loss of hope, limited expectations about life, fear that life will end
abruptly or early, or anticipation that normal life events won’t occur (e.g., access to education, ability to have a significant and committed relationship, good opportunities for work).

When Assessing Trauma, the Clinician Must Consider:
• Was it a single, repeated or sustained trauma?• Was there enough time to process the experience?• How many losses did the trauma cause?• Was the trauma expected or unexpected?• Were the trauma’s effects on the person’s life isolated or
pervasive?• Who was responsible for the trauma, and was the act
intentional • What has happened since the trauma?

Evidence Based Treatment for Trauma Can Include:
• Prolonged Exposure (PE)
• Cognitive Processing Therapy (CPT)
• Eye Movement Desensitization Reprocessing (EMDR)
• Seeking Safety (SS)

These therapies prove to be effective in the treatment of PTSD due to their ability to
reduce the severity of symptoms by retraining the brain to no longer send out false signals

Seeking Safety Trauma Video

Secondary or Vicarious Trauma
Secondary trauma refers to trauma-related stress reactions and symptoms resulting from exposure to another individual’s
traumatic experiences, rather than from exposure directly to a traumatic event. Secondary trauma can occur among behavioral health service providers across all behavioral health settings and among all professionals who provide services to those who have experienced trauma(e.g., healthcare providers, peer counselors,
first responders, clergy, intake workers).
15 Minute Break

Introduction To Seeking Safety

Co-Morbidity of PTSD and SUD is Not Unusual
Women – 51% experience trauma, with 10% developing PTSD
Men – 61% experience trauma, with 5% developing PTSD
Najavits, L. M., (2002) Seeking Safety A Treatment Manual for PTSD and Substance Abuse.
New York: Guilford

Common Factors of SUD and Trauma-Related Symptoms
• Two main themes of both disorders are secrecy and control
• Each of the disorders makes the other more likely
• Both diagnoses have higher rates of personality disorders
• PTSD symptoms widely reported to become worse with initial abstinence
• Both situations produce a profound need to be in an altered state
Najavits, L. M., (2002) Seeking Safety A Treatment Manual for PTSD and Substance Abuse.

What is Seeking Safety?
Seeking Safety is an evidenced based treatment model that treats the co-occurring diagnosis’s of
SUD and TRAUMA RELATED SYMPTOMS

Delivering Seeking Safety Can Be Highly Flexible
• In group or individual treatment• Inpatient and outpatient settings• In long term residential care• For men and women• For Adolescents and TAY• For patients who do not necessarily meet formal criteria for
current PTSD and substance abuse• With other ongoing treatment approaches
Najavits, L. M.,(2002) Seeking Safety A Treatment Manual for PTSD and Substance Abuse.
New York: Guilford

Seeking Safety Treatment Manual
Seeking Safety is Based on Five Central Ideas
1. Safety as the priority for this first stage of treatment2. Integrated treatment of PTSD and SUD3. A focus on ideals4. Four content areas: cognitive, behavioral, interpersonal and
case management5. Attention to the therapist’s process
Najavits, L. M.,(2002) Seeking Safety A Treatment Manual for PTSD and Substance Abuse.
New York: Guilford

Najavitis Based Her Model on the Herman’s Three Stage Model of Recovery (1992)
1.Safety2.Mourning3.Reconnections• Safety Stage is the initial process of Najavits’ treatment
model and is the treatment stage presented in this training.• Mourning and Reconnections are later stages of recovery
that are initiated in therapy work separate from the Seeking Safety Skills Group.
Najavits, L. M.,(2002) Seeking Safety A Treatment Manual for PTSD and Substance Abuse. New York: Guilford
Safety As An Unbrella Term
Discontinue substance use, reduce suicidality, minimize exposure to
HIV and HCV, letting go of extreme symptoms, stopping self harming
behavior (such as cutting)
Najavits, L. M.,(2002) Seeking Safety A Treatment Manual for PTSD and Substance Abuse.
New York: Guilford

Treatment Focuses on the Here and Now
Treatment Focuses on Recovery Interventions that are Common to SUD
and Trauma-Related Symptoms

Safety Elements Within the Management of PTSD Symptoms Reflect Traditional Safety Elements
in Substance Abuse Recovery:
• Education
• Assessing the impact of condition
• Dealing with urges and cravings
• Focus on self care
• Attention to relapse prevention
Najavits, L. M.,(2002) Seeking Safety A Treatment Manual for PTSD and Substance Abuse.
New York: Guilford
The Goals of Seeking Safety
1. Develop commitment to practicing safety
2. Master coping skills (responses to symptoms)
3. Utilize safety planning (prevention)
4. Report unsafe behaviors (asking for help)
5. Utilize Safety contract (response to urges)
Najavits, L. M.,(2002) Seeking Safety A Treatment Manual for PTSD and Substance Abuse.New York: Guilford
25 Treatment Topics
• Safety• PTSD: Taking Back Your Power• Detaching from Emotional Pain
(Grounding)• When Substances Control You• Asking for Help• Taking Good Care of Yourself
• Compassion• Red and Green Flags• Honesty• Recovery Thinking• Integrating the Split Self
Najavits, L. M.,(2002) Seeking Safety A Treatment Manual for PTSD and Substance Abuse.New York: Guilford

Treatment Topics (Continued)
• Commitment• Creating Meaning• Community Resources• Setting Boundaries in Relationships• Discovery• Getting Others to Support Your
Recovery
Najavits, L. M.,(2002) Seeking Safety A Treatment Manual for PTSD and Substance Abuse.New York: Guilford
• Coping with Triggers• Respecting Your Time• Healthy Relationships• Self-Nurturing• Healing from Anger• The Life Choices Game
(Review)• Termination
Detail to the Process Between the Counselor/ Therapist and Client
Attention to problematic countertransference reactions. • Avoid harsh confrontation• Voyeurism• Inability to hold patients accountable – misguided sympathy• Allowing patients to be scapegoated• Becoming a victim• Identification with patient’s PTSD which can result in excessive
support and overindulgence with patient’s vulnerability• Being afraid of patients
Najavits, L. M.,(2002) Seeking Safety A Treatment Manual for PTSD and Substance Abuse.New York: Guilford

Treatment Approach and Intervention Orientation
THE FOCUS IS ON SAFETY AS THE PRIMARY THEME
• Najavits’ model emphasizes “safety skills” in the management of PTSD symptoms, feelings of emotional turmoil, and self doubt
• Interactions with clients focus on supporting and facilitating safety themes in making behavioral choices, in response to emotions and reactions to situations
• In addition to Cognitive/Behavioral approaches, the teaching of grounding skills is used to enable the client to self sooth and disengage from destructive urges, emotional pain, and feelings of being overwhelmed.
Najavits, L. M.,(2002) Seeking Safety A Treatment Manual for PTSD and Substance Abuse. New York: Guilford
Important for Therapists New to Seeking Safety
• Direct process without taking charge
• Apply 80/20 rule
• Ask provocative questions – “How might this apply to your PTSD and substance use”
• Relate material to current and specific problems in patients’ lives
• Process barriers and obstacles
• Refer to Coping and Commitment SheetsNajavits, L. M.,(2002) Seeking Safety A Treatment Manual for PTSD and Substance Abuse.
New York: Guilford

How To Facilitate A Seeking Safety Session

Check In
Since your last session:
1. How are you feeling?
2. What good coping have you done?
3. Any substance use or other unsafe behavior?
4. Did you complete your commitment?
5. Community Resources Update
Quotation

Handouts

Seeking Safety Grounding Exercise
Demonstration
Check Out
1. Name one thing you got out of today’s session (and any problems with the session).
2. What is your new commitment?
3. What community resource will you call?
Questions And Answers

Final Check Out

For Further Information on Seeking Safety or Treatment of Trauma and SUD Evidence Based Treatment
• Official Seeking Safety Website: http://www.treatment-innovations.org/seeking-safety.html
• PTSD: National Center for PTSD (Resource for treatment information and access to outcome measures: http://www.ptsd.va.gov/professional/assessment/overview/index.asp
• SAMSHA National Center for Trauma-Informed Care: http://www.samhsa.gov/nctic
• National Child Traumatic Stress Network (For those Working with Adolescents or TAY): http://www.nctsn.org/resources
• Trauma Informed Care in Behavioral Health Services: http://store.samhsa.gov/product/TIP-57-Trauma-Informed-Care-in-Behavioral-Health-Services/SMA14-4816
• Understanding Evidence-Based Practices for Co-Occurring Disorders: http://store.samhsa.gov/product/Understanding-Evidence-Based-Practices-for-Co-Occurring-Disorders/SMA07-4278

Thank You.
[email protected] 760.992.3478
Kevin Koffler, MA LMFTClinical Director
C O N T A C T I N F O R M A T I O N: