treating addiction as a chronic disease john f. kelly, ph.d. elizabeth r. spallin associate...
TRANSCRIPT

Treating Addiction as a chronic disease
John F. Kelly, Ph.D. Elizabeth R. Spallin Associate Professor of Psychiatry in Addiction Medicine
Harvard Medical School
Director Recovery Research Institute
MGH Center for Addiction Medicine
Faxton St. Lukes, October 17th 2014

Disclosure of Relevant Financial Relationships Content of Activity: Faxton St. Lukes Talk
Date of Activity: Octobr 17th 2014
Name Commercial Interests
Relevant Financial
Relationships: What Was Received
Relevant Financial
Relationships: For What Role
No Relevant Financial
Relationships with Any
Commercial Interests
x

RECOVERY RESEARCH INSTITUTE LAUNCHOCTOBER 30, 2013
WWW.RECOVERYANSWERS.ORG
www.recoveryanswers.org

MONTHLY NEWSLETTER

Sign up for Newsletter at:
www.recoveryanswers.org

OUTLINE
Definitions, terminology, and
stigma
Acute vs chronic care model
Conceptualizations of addiction and
recovery
Addiction recovery management
models

OUTLINE
Definitions, terminology, stigma, and
discrimination
HEALTH CARE IS CHANGING AND SUD IS (FINALLY) BECOMING AN IMPORTANT FOCUS IN THAT CHANGE


DEFINITIONS, TERMINOLOGY, STIGMA AND DISCRIMINATION
Should we use the term “Chronic disease”? Or, “alcohol/drug problem? Or call it “substance abuse/abuser”?
Does it really matter what we call it or them?
Is it chronic? Is it a “disease”?

WHAT IS A “DISEASE”?“a disordered or incorrectly functioning organ, part,
structure, or system of the body resulting from the effect of genetic or developmental errors, infection,
poisons, nutritional deficiency or imbalance, toxicity, or unfavorable environmental factors.” – Dictionary.com
“ a condition of the living animal or plant body or of one of its parts that impairs normal functioning and is typically manifested by distinguishing signs and symptoms” -Miriam Webster
It matters, because the words we use influence our conceptualizations and approaches to it (e.g., “War on drugs” “You use you lose” vs addiction as a public health problem)

“CHRONIC”?WHO (2014)
“Noncommunicable diseases (NCDs), also known as chronic diseases, are not passed from person to person. They are of long duration and generally slow progression. The four main types of noncommunicable diseases are cardiovascular diseases (like heart attacks and stroke), cancers, chronic respiratory diseases (such as chronic obstructed pulmonary disease and asthma) and diabetes.”

NOT ALL THOSE WHO MEET CRITERIA FOR SUD HAVE CHRONIC TRAJECTORIES…EPIDEMIOLOGIST’S ILLUSION VS. CLINICIAN'S ILLUSION
NSDUH and Dennis & Scott
0
10
20
30
40
50
60
70
80
90
100
12-13
14-15
16-17
18-20
21-29
30-34
35-49
50-64
65+
No Alcohol or Drug Use
Light Alcohol Use Only
Any Infrequent Drug Use
Regular AOD Use
Abuse
Dependence
Age Groups
Severity Category

14
REMISSION OF DEPENDENCE IS COMMON, BUT FOR SOME INDIVIDUALS’ DEPENDENCE CAN SPAN DECADES
Source: NIAAA 2001-2002 NESARC data (18-60+ years of age) and SAMHSA 2003 NSDUH (12-17 years of age).
High remission
rates
But for some, chronic, harmful course…

SUBTYPES – BUT IDENTIFICATION OF CLINICALLY MEANINGFUL SUBTYPES CHALLENGING…TYPOLOGY INVESTIGATIONS
Silkworth (1939) Jellinek (1960) Cloninger (1981) Babor (1992) Del Boca (1994) Del Boca (1996) Hesselbrock (2006) Moss (2007) Anton (2008)

Addiction Onset
Help Seeking
Full Sustained
Remission (1 year
abstinent)
Relapse Risk drops below
15%
4-5 years 8 years 5 years
Self-initiated cessatio
n attempt
s
4-5 Treatmen
t episodes/mutual-
help
Continuing care/mutual-
help
For more severely dependent individuals … course is chronic but remission most likely outcome
60% of individuals
with addiction
will achieve full
sustained remission (White, 2013)
Opportunity for earlier detection through
screening in non-
specialty settings like
primary care/ED

ADDICTION IS HEAVILY STIGMATIZED AND THE LANGUAGE WE USE MAY AFFECT STIGMA/DISCRIMINATION
• SUDs most stigmatized of all social/health problems Most
Stigmatized
• National surveys show stigma one of main reasons people with SUD do not seek specialty care (SAMHSA, 2009)Nationally
• WHO examined 18 most stigmatized conditions (eg. criminal, HIV, homeless) across 14 different countries (Room et al 2001)• Drug addiction- #1 - most stigmatized• Alcohol addiction- 4th most stigmatized
Internationally
• Ambivalence influenced by stigma and contributes to few accessing care (only 10% seek specialty care/yr)Poor access

LANGUAGE SURROUNDING CLINICAL CARE IN ADDICTION IS UNLIKE ANY OTHER AREA OF MEDICINE - MAY AFFECT QUALITY AND EFFECTIVENESS OF CARE
A patient suffering from diabetes has “an elevated glucose”. A patient with cardiovascular disease has “a positive exercise tolerance test” Someone inside the healthcare system
addresses the results. An “addict” isn’t “clean”—he has been
“abusing” drugs and has a “dirty” urine. Someone outside the system that cares for all
other health conditions addresses the results. In the worst case, the drug use is addressed by
incarceration.

SUD STIGMA/DISCRIMINATION MODERATED BY TWO FACTORS…
CAUSE Did they cause it?
“It’s not their fault” (decreases stigma; increase compassion)
CONTROLLABILITY Can they help it?
“They can’t help it” (decreases stigma; increases compassion)

TWO COMMONLY USED TERMS…
Referring to someone as…
“a substance abuser” – implies perpetration/willful misconduct (they CAN help it)
“having a substance use disorder” – implies victim/medical malfunction (they CAN’T help it)


22
How we talk and write about these conditions and individuals suffering them does matter

Mr. Williams is a substance abuser and is attending a treatment program through the court. As part of the program Mr. Williams is required to remain abstinent from alcohol and other drugs. He has been doing extremely well, until one month ago, when he was found to have two positive urine toxicology screens which revealed drug use and a breathalyzer reading which revealed alcohol consumption. Within the past month there was a further urine toxicology screen revealing drug use. Mr. Williams has been a substance abuser for the past six years. He now awaits his appointment with the judge to determine his status.
Mr. Williams has a substance use disorder and is attending a treatment program through the court. As part of the program Mr. Williams is required to remain abstinent from alcohol and other drugs. He has been doing extremely well, until one month ago, when he was found to have two positive urine toxicology screens which revealed drug use and a breathalyzer reading which revealed alcohol consumption. Within the past month there was a further urine toxicology screen revealing drug use. Mr. Williams has had a substance use disorder for the past six years. He now awaits his appointment with the judge to determine his status.
Doctoral-level clinicians (n=561) randomized to receive one of two terms….

24
0.41 0.76 0.21 0.670.23 0.42 0.24 0.79 0.330.67 0.580.69.00
.10
.20
.30
.40
.50
.60
.70
.80
.90
Treatment Punishment Social Threat AttributionBlame
AttributionExoneration
Self-Regulation
Mea
n of
Sub
scal
e Sc
ores
Substance Abuser Substance Use Disorder
Figure 1. Subscales comparing the “substance abuser” and “substance use disorder” descriptive labels
Kelly, JF, Dow, SJ, Westerhoff, C. Does our choice of substance-related terms influence perceptions of treatment need? An empirical investigation with two commonly used terms (2010) Journal of Drug Issues

IMPLICATIONS
Exposure to the “abuser” term may activate an implicit more punitive cognitive bias
Learn from our friends in other fields : Individuals with “eating related problems” are
uniformly described as “having an eating disorder” NEVER as “food abusers”

STOP TALKING “DIRTY”: CLINICIANS, LANGUAGE, AND QUALITY OF CARE FOR THE LEADING CAUSE OF PREVENTABLE DEATH IN THE UNITED STATESKELLY, JF, WAKEMAN, SE, SAITZ, R. AMERICAN JOURNAL OF MEDICINE (IN PRESS)
Avoid stigmatizing terminology such as “dirty” vs “clean” utox screens, instead of “negative/positive”.
Recommendations: Use “person first” language - refer to individuals with
addiction as people with a “substance use disorder” not as substance “abusers” or “addicts.”
For those with consequences or risk, but not a disorder (often referred to inaccurately as “abuse”), use “hazardous”, “risky”, or “harmful” use, or for the full spectrum that includes risk to a disorder, “unhealthy” use.
…commit to a medically appropriate lexicon which conveys the same dignity and respect we offer to other individuals suffering from an array of medical problems.

OUTLINE
Acute vs chronic care model

Addiction Onset
Help Seeking
Full Sustained
Remission (1 year
abstinent)
Relapse Risk drops below
15%
4-5 years 8 years 5 years
Self-initiated cessatio
n attempt
s
4-5 Treatmen
t episodes/mutual-
help
Continuing care/mutual-
help
For more severely dependent individualscourse of addiction is chronic …
60% of individuals
with addiction
will achieve full
sustained remission (White, 2013)
Opportunity for earlier detection through
screening in non-
specialty settings like
primary care/ED

If really believed addiction is chronic we would not: View prior tx failure as a poor prognostic indicator Convey the expectation that all clients should achieve
complete, enduring sobriety following single, brief treatment episode
Punitively d/c clients for becoming symptomatic/confirming their diagnosis
Relegate continuing care to an afterthought Terminate the service relationship following acute care Treat serious and persistent SUD in serial episodes of
self-contained and unlinked interventions
BUT, WHAT IF REALLY BELIEVED ADDICTION WAS A CHRONIC DISORDER?
White and Kelly (2011)

CHRONIC NATURE OF SUBSTANCE DEPENDENCE MAKES IT WELL-SUITED TO ONGOING RECOVERY MANAGEMENT (RM) APPROACHES…
Addiction talked as chronic but still treated as acute condition:
Recovery management is a philosophy of organizing addiction treatment and recovery support services to enhance early pre-recovery engagement, recovery initiation, long-term recovery maintenance…(White & Kelly, 2011).

OUTLINE
Conceptualizations of addiction and
recovery

ADDICTION IS A… A disease of the brain that affects the neuro-circuitry
of reward, memory, motivation, impulse control, and judgment
For recovery to occur, accurate risk appraisals must be conducted and frequent adaptive decisions made and actions taken (prefrontal cortex) to inhibit impulses and gradually correct dysregulated reward system (limbic system)
Rewards of use are immediate, concentrated, predictable; rewards of recovery are delayed, diffuse, and variable
Recovery is a demanding, effortful, process requiring constant vigilance to protect against the risk of relapse and can lead to frustration and exhaustion…
WHY DO PEOPLE HAVE A HARD TIME STAYING SOBER AND IN REMISSION?
General Adaptation Syndrome (Selye, 1956)
Alarm – Resistance – Exhaustion
“… after self-control efforts, subsequent attempts at self-control are more likely to fail. Continuous self-control efforts, such as vigilance, also degrade over time…These decrements appear to be specific to behaviors that involve self-control (Muraven & Baumeister, 2000).
Post-acute withdrawal and need to learn complex recovery coping skills – stressful; taxes available coping resources - affects relapse risk
Need to find ways to replenish cognitive resources to inhibit thoughts and impulses to use substances over time…
WHY DO PEOPLE HAVE A HARD TIME STAYING SOBER AND IN REMISSION?

In fact, the recovery construct, like the addiction construct, is made up of two reciprocal factors: “remission” and the consequences of that remission, “recovery capital”;
as longer remission is achieved, more capital accrues, BUT also, remission can be influenced the other way - as more recovery capital accrues so the chances of continued remission increase.
Kelly and Hoeppner (2014) A biaxial formulation of the recovery construct, Addiction Research and Theory

35
DECREASE STRESS AND REPLENISH COPING RESOURCES BY PROVIDING RM AND RECOVERY SUPPORT SERVICES
Recovery Management and Monitoring
Recovery Mutual-help organizations
Recovery High schools
Collegiate Recovery Support programs
Recovery Community Centers
Recovery Community Organizations

OUTLINEAddiction recovery
management models

Clinically, we’ve learned that
prized-based CM approaches can produce large effects while
contingencies in place …. But advantage
disappears by 6m once removed

Examples of Long-term recovery management programs
Physicians Health Programs
Hawaii Opportunity Probation with Enforcement (HOPE)
South Dakota “24/7”
Clinical Recovery Management Check-ups
Mutual-help organizations

PHYSICIANS HEALTH PROGRAMS
Emerged in 1970s, through the American Medical Association to help alcohol/drug impaired physicians
Services provided include:- professional intervention services- referral to formal evaluation- referral to formal treatment- long-term monitoring
Source: White, W.L., DuPont, R.L. & Skipper, G.E. (2007)

KEY INGREDIENTS OF PHPS motivational fulcrum: link recovery to positive rewards and
relapse to negative consequences (e.g., loss of license) comprehensive assessment and treatment: patient-oriented
treatment rather than a fixed model care management oversight role: PHPs directs care for
physicians so they can select appropriate resources high expectation for abstinence-based recovery: relapses are
seen as temporary setbacks/learning experiences assertive linkage to recovery support groups: active referrals
to 12-step and other recovery-focused mutual aid groups sustained monitoring support reintervention: periodic
interviews/random urine testing over 5 years reintervention at higher level of intensity: relapse and
reintervention are followed by reevaluation and more intensive/prolonged treatment
integrated comprehensive program: PHPs include these items in an integrated and long-sustained program
Source: Skipper, G.E. and DuPont, R.L. (2011)

PHPS 5-7YR STUDY OUTCOMES (N=904)
72% completed the contract; a further 22% signed a new one
(78% of these voluntarily)
79% licensed and working at 5-year follow-up
92% participated in AA or NA; 61% participated in continuing
groups
78% had zero positive tests across 5-7 yrs; 22% had at least one positive test at some point, however, only 1 in 200 drug screens were positive over the 5-7yr monitoring period
Source: Du Pont, R.L. et al. (2011)

HAWAII OPPORTUNITY PROBATION WITH ENFORCEMENT (HOPE) PROGRAM
Goal - to reduce drug use, new crimes, and incarceration
Drug-testing-and-sanctions approach
Does not mandate treatment; 12-step participation encouraged
Started as pilot program 2004 with 36 offenders now expanded to over 1500 participants 2009

PILOT STUDY BY THE INTEGRATED COMMUNITY SANCTIONS UNIT IN HONOLULU
Offenders in HOPE vs. comparison offenders
HOPE procedure:- initiation/overview conducted by judge- call HOPE hotline every morning- if selected for testing, must appear by 2pm- if fail to appear or test positive, “Motion to Modify Probation” issued- after immediate hearing, if offender has violated probation, sentenced to short jail stay (several days)- HOPE participation resumes upon release
Probation as usual:- no random drug testing- scheduled appointments with a probation officer once a month

AVERAGE NUMBER OF POSITIVE UAS, BY PERIOD. (HAWKEN ET AL. , 2009)
In a 12-month period 61% of HOPE participants had zero positive UAs
Note: Data are from PROBER. For comparison probationers, data reflect urinalysis results for
regularly scheduled UAs. For HOPE probationers UAs include regularly scheduled tests, and
random testing. Pre (3m) refers to the average number of missed appointments in the three
months before the study start date (baseline). Follow-up (3m) refers to the average number of
missed appointments in the three-month period following baseline and Follow-up (6m) refers to
the average number of missed appointments in the six-month period following baseline.

RANDOMIZED CONTROLLED TRIAL OF HOPE (N=493) (HAWKEN ET AL., 2009)
HOPE vs. probation-as-usual One year follow up
ResultsHOPE in comparison with probation-as-usual:- 60% fewer no-shows- 70% fewer positive urine tests- 55% fewer new arrest rates- 53% lower revocation rate- 48% lower incarceration

SOUTH DAKOTA’S “24/7 SOBRIETY” PROJECT (LARRY LONG)
For repeat DUI offenders Started 1980s in 1 county; 2007 implemented
state-wide -replicated in North Dakota Objective verification of abstinence (twice
a day breath, blood or other bodily substance testing
Positive/missed tests results in immediate 24-hour incarceration
No treatment referral or requirement; 12-step attendance encouraged

24/7 SOBRIETY OUTCOMES
Urinalyses (July 1, 2007-July 20, 2011): N= 1,990 46,648 tests administered Pass Rate 96.9% SCRAM bracelets (Nov. 6, 2006-July 20, 2011): N=3,177 77.9% had no violations 22.1% participants had some type of violationDrug patches (July 1, 2007-July 20, 2011): N=94 Pass Rate 80%
Source: http://apps.sd.gov/atg/dui247/247stats.htm

A Example of the benefit of treating addiction like a chronic condition: 4-year outcomes from the Early Re-Intervention experiment using Recovery Management Checkups
N=446 adults with SUD, mean age = 38, 54% male, 85% African-American
randomly assigned to
quarterly assessment onlyquarterly assessment plus RMC
Recovery Management Checkups Linkage manager who used motivational interviewing to
review the participant’s substance use, discuss treatment barrier/solutions, schedule an appointment for treatment re-entry, and accompany participant through the intake
If participants reported no substance use in the previous quarter, the linkage manager reviewed how abstinence has changed their lives and what methods have worked to maintain abstinence
Source: Dennis & Scott (2012). Drug and Alcohol Dependence, 121, 10-17

RESULTS 1RETURN TO TREATMENT
• Participants in RMC condition sig. more likely to return to treatment sooner
Source: Dennis & Scott (2012). Drug and Alcohol Dependence, 121, 10-17

RESULTS 4DAYS ABSTINENT (0-1350)
Total days abstinent*880
900
920
940
960
980
1000
1020
1040
RMC Control
*p<.01
Of 18 vars tested, the only variables that predicted return to treatment was the
intervention


WHAT ABOUT MHOS’ ROLE IN CHRONIC RECOVERY MANAGEMENT?

SOCIETAL RESPONSE TO SUD AND RELATED PROBLEMS. WHY HAVE MHO’S GROWN DESPITE BETTER MORE EFFECTIVE
PROFESSIONAL TREATMENTS
While increases in quality and quantity of SUD treatment over past 40yrs….
…professional resources alone cannot cope; stigma and cost present further barriers to formal tx access
Addiction often has chronic course (8 yrs from 1 st tx to achieve FSR; Dennis et al, 2005); 4-5 yrs before risk of relapse <15%
In tacit recognition, most societies seen increases in MHOs during past 75 yrs (Kelly & Yeterian, 2008)
“The burden of alcohol problems is a heavy one; the specialized treatment sector is necessarily limited in size and quite costly.
The committee believes that only a shared effort can succeed in
lifting this burden to any significant degree” (IOM, 1990)

POTENTIAL ADVANTAGES OF COMMUNITY MUTUAL-HELP IN RECOVERY MANAGEMENT
Cost-effective -free; attend as intensively, as long as desired
Focused on addiction recovery management over long term
Widely available, easily accessible/flexible
Provide access at high risk times when professional services not available (e.g., nights/ weekends/holidays)
Entry threshold (no paperwork, insurance); anonymous (stigma)
Adaptive community based system that is responsive to undulating relapse risk

NameYear of Origin Number of groups in U.S. Location of groups in U.S.
Alcoholics Anonymous (AA) 1935
60,000all 50 States
Narcotics Anonymous (NA) 1940s
Approx. 20,000all 50 States
Cocaine Anonymous (CA) 1982
Approx. 2000 groups most States; 6 online meetings at www.ca-online.org
Methadone Anonymous (MA) 1990s Approx. 200 groups
25 States; online meetings at http://methadone-anonymous.org/chat.html
Marijuana Anonymous (MA) 1989 Approx. 500 groups
24 States; online meetings at www.ma-online.org
Rational Recovery (RR)
1988No group meetings or mutual helping; emphasis is on individual control and
responsibility-----------------------------------------------------
Self-Management and Recovery Training
(S.M.A.R.T. Recovery)
1994 Approx. 500 groups 40 States; 19 online meetings at
www.smartrecovery.org/meetings/olschedule.htm
Secular Organization for Sobriety, a.k.a.
Save Ourselves (SOS)1986 Approx. 500 groups
all 50 States; Online chat at www.sossobriety.org/sos/chat.htm
Women for Sobriety (WFS) 1976 150-300 groups
Online meetings at http://groups.msn.com/ WomenforSobriety
Moderation Management (MM) 1994 Approx.18 face-to-face meetings
12 States; Most meetings are online at www.angelfire.com/trek/mmchat/;
MHOs are prolific resources well-suited to RM approaches to SUD
Source: Kelly & Yeterian, 2008

Table 2. Dual-Diagnosis Focused Mutual-help Groups
Name Year of OriginNumber of
groups in U.S. Location of groups in U.S.
Double Trouble in Recovery
(DTR)1989 300
Highest number of groups in NY, GA, CA, CO, NM, FL
Dual Recovery Anonymous
(DRA)1989 445 Highest number of groups in
CA, OH, PA, MA
Dual Disorders Anonymous 1982 98 28 in IL
Dual Diagnosis Anonymous
(DDA) 76 38 in CA
Source: Kelly & Yeterian, 2008)

Table 3. Non-Substance Focused Addictive Behavior Mutual-help Groups
NameYear of Origin
Number of groups in U.S. Location of groups in U.S.
Gamblers Anonymous
(GA)1957 Approx. 1000 chapters all 50 States
Sex Addicts Anonymous
(SAA)1977 Approx. 700 meetings
most States; Online meetings at www.sexaa.org/online.htm; Telephone
meetings
Sex and Love Addicts
Anonymous (SLAA)
1976Approx. 1320 groups
worldwide
(including in all 50 States), Online meetings at
www.slaafws.org/online/onlinemeet.html
; Regional teleconference calls
Overeaters Anonymous
(OA)1960
Approx. thousands of meetings
all 50 States; Numerous online (www.oa.org/pdf/OnlineMeetingsList.pdf
) and telephone meetings (www.oa.org/pdf/phone_mtgs.pdf)
Source: Kelly & Yeterian, 2008)

Effectiveness: Do they help? Millions attend 12-step MHOs and
many continue long-term
Rigorous experimental, quasi-experimental, correlational, and observational studies support MHOs as stand alone or adjunct to treatment
Potentiate and extend treatment outcomes and reduce health
care costs
Work through mechanisms similar to those operating in formal tx
Clinical (12-step facilitation) strategies can enhance participation and outcomes


EVIDENCE OF BENEFIT - META ANALYSES OF AA 4 meta-analytic reviews
Emrick et al. 1993
Tonigan et al, 1996
Kownacki et al. 1999
Ferri, Amato, & Davoli, 2006

RESULTS AND LIMITATIONS Results from hundreds of studies reveal AA
confers a consistent moderate beneficial effect in par with professional treatment
Results from RCTs of AA itself, reveal mixed findings depending on whether individuals were coerced/mandated to attend AA meetings or not
Most attended following treatment –difficult to discern unique effects of AA…





Odds of Abstinence
4 Months
-Completed treatment -Attended 12-step meetings on a weekly or more basis
-Completed treatment -Did not attend 12-step meetings
-Remained in treatment-Did not complete treatment-Did not attend 12-step meetings
2 Months -Did not complete treatment -Did not attend 12-step meetings
-1 0 1 2 3 4 5 6 7 8 9
Fiorentine and Hillhouse (2000)

CBT TSF$0
$2,000
$4,000
$6,000
$8,000
$10,000
$12,000
$14,000
$16,000
$18,000
$20,000
$12,129
$7,400$5,735
$2,440
$17,864
$9,840Year 1Year 2Total
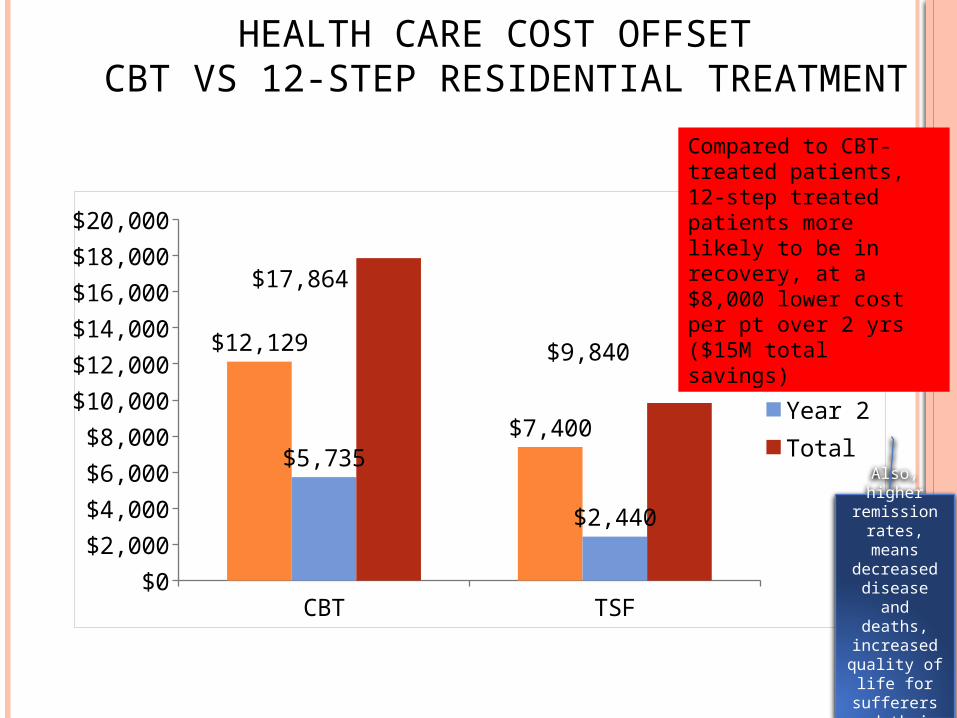
HEALTH CARE COST OFFSET CBT VS 12-STEP RESIDENTIAL TREATMENT
Compared to CBT-treated patients, 12-step treated patients more likely to be in recovery, at a $8,000 lower cost per pt over 2 yrs ($15M total savings)
Also, higher remission
rates, means
decreased disease and
deaths, increased quality of
life for sufferers and their families

ADOLESCENT HEALTH CARE COST OFFSET 7-YEAR STUDY
N = 403 adolescents, age 13-18Follow-up: 6 months, 1, 3, 5, and 7 years12-step attendance associated with
better outcomes over the 7 yr period Avg annual medical costs for all participants over 7
years: $3085 per person per year 4.7% decrease in medical costs with each additional
12-step meeting attended = $145 annual savings per 12-step meetings attended
Source: Mundt, Parthasarathy, Chi, Sterling, Campbell (2012)
Mundt et all,, 2012, Drug and Alcohol Dependence

TOWARD TWELVE-STEP FACILITATIONEvidence: Millions have attended; half of AA members of 5 yrs
or more of sobriety; attendees report benefitting
Positive results from more than a hundred correlational/ quasi-experimental and experimental studies
Facilitating linkage enhances abstinence/remission and reduces health care costs
If we really believed addiction was a chronic disease and MHOs were shown to increase remission rates shouldn’t we try to link patients with them?

Can what we do in treatment increase
long-term engagement with MHOs and thereby enhance recovery
outcomes?

DOES FACILITATION DURING TX AFFECT RISK FOR DROPOUT?
Risk Factors
Treatment Settings Combined
High Supportive Treatment milieu
Low supportive Treatment milieu
n Dropout Rate n Dropout Rate n Dropout Rate 0 261 30 % (77) 151 30 % (45) 110 29 % (32) 1 548 30 % (163) 274 29 % (79) 274 31% (84) 2 582 38 % (221) 269 38 %(103) 313 38 % (118) 3 512 43 % (218) 176 40 % (70) 336 44% (148) 4 381 51 % (193) 119 42 % (50) 262 55% (143) 5 150 54 % (81) 36 47 % (17) 114 56% (64) 6-7 78 65 % (51) 16 50 % (8) 62 70% (43)
• Dropout rate = 40%• AA dropouts had 3x higher odds of relapse to alcohol/drug use

FACILITATION BY DROPOUT-RISK INTERACTION
Source: Kelly & Moos (2003) Dropout from 12-Step Groups: Prevalence, Predictors and Counteracting Treatment Influences, Journal of Substance Abuse Treatment,24, 241-250

PRECURSOR TO CURRENT TSF RESEARCH (SISSON AND MALAMS, 1981)
20 patients randomly selected from outpatient tx program for alcohol use disorder
Randomly assigned to:1: Standard referral
given information about AA including time, date, location of meetings, encouraged to attend meetings
2: Systematic encouragement and community access In addition to standard procedure, clients had phone
conversation with AA member during a session - client and AA member met before first meeting, member provided client with ride; client also received a reminder phone call from the member

PRECURSOR TO CURRENT 12-STEP FACILITATION RESEARCH
Results: 0% clients in standard referral attended a meeting
during the target week
100% clients in systematic encouragement and community access group attended meeting during target week
Mean AA meeting attendance rate for 4 week period: 0 for standard referral group vs 2.3 for systematic
encouragement group

TSF DELIVERY MODES
Stand alone Independent therapy
Integrated into an existing therapy
Component of a treatment package (e.g., an additional group)
As Modular appendage linkage component
TSF
OTH

TSF DELIVERY MODES
Stand alone Independent therapy
Integrated into an existing therapy
Component of a treatment package (e.g., an additional group)
As Modular add-on linkage component
TSF
OTH

I. PROJECT MATCH- RESULTS Similar on continuous outcomes (PDA/DDD) Across txs, AA attendees had better outcomes (Tonigan et al,
2002) AA valuable adjunct to treatment - even when not formally
emphasized Individuals assigned to TSF attended AA more frequently and
had substantially higher rates of continuous abstinence at 1yr and 3yrs

CHANGING NETWORK SUPPORT FOR DRINKING (LITT ET AL., 2009)
Network Support Project -to determine if tx can change social networks to ones supportive of sobriety
Alcohol dependent individuals (N=210) randomly assigned to 1 of 3 txs:
Network Support (NS) Meant to help patients change social network to include people in
support of abstinence; based on TSF treatment created for Project MATCH; 6 core sessions+ 6 elective sessions
Network Support +Contingency Management (NS+CM) Same network support as described above, plus drawings from a
“fishbowl” if soc. network enhancing tasks completed (eg. AA meeting, having coffee with a sober friend)
Case Management (CaseM, control condition) Based on intervention used in Marijuana Treatment Project; therapist
and participant worked together to indentify barriers to abstinence and develop goals and identify resources to be used to aid in achieving abstinence

CHANGING NETWORK SUPPORT FOR DRINKING- FINDINGS
Network Support:
• Higher PDA
• More total abstinent
• Lower consequences
• Lower DDD

TSF DELIVERY MODES
Stand alone Independent therapy
Integrated into an existing therapy
Component of a treatment package (e.g., an additional group)
As Modular add-on linkage component
TSF
OTH

STRATEGIES FOR FACILITATING OUTPATIENT ATTENDANCE OF AA (WALLITZER ET AL, 2008)
Approaches to assist in involvement in AA
169 adult alcoholic outpatients randomly assigned to one of three treatment conditions
All clients received treatment that included: 12 sessions Focus on problem-solving, drink refusal,
relaxation Recommendation to attend AA meetings

STRATEGIES FOR FACILITATING OUTPATIENT ATTENDANCE OF AA Treatment varied between 3 conditions in terms of how the therapist
discussed AA and how much information about AA was shared Condition 1: Directive approach
Therapist directed Client signed contract describing goals to attend AA meetings Therapist encouraged client to keep a journal about meetings Reading material about AA provided to client Therapist informs client about skills to use during meetings and about using a
sponsor 38% total material covered in sessions was about AA
Condition 2: motivational enhancement approach (more client centered)
Therapist obtains clients feelings and attitudes about AA Therapist describes positive aspects of AA, but states that it is up to the client how
much they will be involved Therapist intends to assist the client in making a decision in favor of AA 20% total material covered in sessions about AA
Condition 3: CBT treatment as usual, no special emphasis on AA Throughout treatment, therapist briefly inquires about AA and encourages client to
attend AA 8% total material covered in sessions about AA
Walitzer, Dermen & Barrick, 2009

STRATEGIES FOR FACILITATING AA ATTENDANCE DURING OUTPATIENT TREATMENT

Strategies for Facilitating AA Attendance during Outpatient Treatment

TSF DELIVERY MODES
Stand alone Independent therapy
Integrated into an existing therapy
Component of a treatment package (e.g., an additional group)
As Modular add-on linkage component
TSF
OTH

MAAEZ INTERVENTION (KASKUTAS ET AL, 2009) Making AA Easier- manual guided - designed to help clients
prepare for AA
Goal: to prepare for AA (encourage participation in AA, minimize resistance to AA, and educate about AA) MAAEZ intervention is conducted in a group format to help prepare
for group dynamic of AA
Facilitator goal: to inform clients about AA and facilitate group interaction Facilitator recommended to be an active member of AA, NA, or CA
Discussion format: MAAEZ allows and encourages feedback (referred to as “cross-talk” in MAAEZ), unlike AA which does not allow feedback

MAAEZ INTERVENTION- FINDINGS

TSF DELIVERY MODES
Stand alone Independent therapy
Integrated into an existing therapy
Component of a treatment package (e.g., an additional group)
As Modular add-on linkage component
TSF
OTH

EFFECTIVENESS OF CLINICIAN REFERRALS TO AA (TIMKO ET AL 2006; 2007)
Evaluation of procedures to effectively refer patients to 12-step meetings
Individuals with SUDs entering a new outpatient treatment program randomly assigned to a treatment condition and provided self reports on meeting attendance and substance use
Condition 1: standard referral Patients given locations and schedules of meetings and encouraged to attend
Condition 2: intensive referral Patients give locations and schedules of meetings, with the meetings preferred
by previous clients indicated
Therapist reviews a handout about program including introduction to 12-step philosophy and common concerns
Therapist arranged a meeting with a current member and client had a phone conversation with this member during a session
Therapist and client agreed on which meetings client will attend and client kept a journal of meetings attended and experiences

EFFECTIVENESS OF CLINICIAN REFERRALS TO AA- AA PARTICIPATION FINDINGS
Timko 2007

EFFECTIVENESS OF CLINICIAN REFERRALS TO AA- ABSTINENCE OUTCOME FINDINGS

Social
Psych
Neuro-biology
RELAPSE
Cue Induced
Stress Induced
Drug Induced
How might informal RM resources like MHOs reduce relapse risk and sustain the recovery process?
AA-related social network changes may help avoid cues, reduce and tolerate distress, and maintain abstinence minimizing drug-induced relapse risks
MHO
Kelly JF, Yeterian, JD, (2013). Mutual help groups. In McCrady and Epstein. Comprehensive Textbook on Substance Abuse.

MHOS REMOTIVATE PEOPLE OVER TIME MHOs help maintain the salience of the negative
consequences of use by facilitating continuous re-exposure (personal stories) and reactivation of painful memories that stimulated the initial recovery attempt (“keep it green”)
MHOs provide exposure to recovering role models and observable evidence that recovery and happiness are attainable
MHOs impart knowledge/skills, realistic expectations of change
MHOs provide encouragement, cheerleading, applause to encourage people to continue; supervision/monitoring
MHOs provide access to new social network that can facilitate alternative sober rewarding activities


(9-mo) Self-efficacyNegative Affect
Baseline (BL) CovariatesAgeRaceSexMarital StatusEmployment Status
Prior Alcohol TreatmentMATCH Treatment groupMATCH study site
Alcohol Outcomes (PDA/DDD)
(15-mo) Alcohol Outcomes(PDA or DDD)
(3-mo) AA attendance
(BL) Self-efficacyNegative Affect
(9-mo) Self-efficacyPositive Social
(BL) Self-efficacyPositive Social
(9-mo) Religious/SpiritualPractices
(BL) Religious/SpiritualPractices
(9-mo) Depression(BL) Depression
(9-mo) Social Network“pro-abstinence”
(BL) Social Network“pro-abstinence”
(9-mo) Social Networkpro-drinking”
(BL) Social Network“pro-drinking”
Source: Kelly, Hoeppner, Stout, Pagano (2012) , Determining the relative importance of the mechanisms of behavior change within Alcoholics Anonymous: A multiple mediator analysis. Addiction 107(2):289-99

97
Self-efficacy (NA)5%
Depression3%
Spirit/Relig23%
Self-efficacy (Soc)34%
SocNet: pro-abst.16%
SocNet: pro-drk.24%
Aftercare (PDA)
Self-efficacy (NA)1%
Depression2% Spirit/Relig
6%
Self-efficacy (Soc)27%
SocNet: pro-abst.31%
SocNet: pro-drk.33%
Outpatient (PDA)
Self-efficacy (NA)20%
Depression11%
Spirit/Relig21%
Self-efficacy (Soc)21%
SocNet: pro-abst.
11%
SocNet: pro-drk.16%
Aftercare (DDD)
Self-efficacy (NA)1%
Depression5%
Spirit/Relig9%
Self-efficacy (Soc)39%
SocNet: pro-abst.17%
SocNet: pro-drk.29%
Outpatient (DDD)
DO MORE AND LESS SEVERELY ALCOHOL DEPENDENT INDIVIDUALS BENEFIT FROM AA IN THE SAME OR DIFFERENT WAYS?
effect of AA on alcohol use for AC was explained by social factors but also by S/R and through negative affect (DDD only)
Majority of effect of AA on alcohol use for OP was explained by social factors
Source: Kelly, Hoeppner, Stout, Pagano (2012) , Determining the relative importance of the mechanisms of behavior change within Alcoholics Anonymous: A multiple mediator analysis. Addiction 107(2):289-99

DO MEN AND WOMEN BENEFIT FROM AA IN THE SAME WAYS?
98

DO YOUNG ADULTS BENEFIT AS MUCH AND IN THE SAME WAYS AS OLDER ADULTS
Self-efficacy (NA)1%
Self-effi-cacy (Soc)
32%
Religiousness7%
Depression1%SocNet: pro-abst.
7%
SocNet: pro-drk.
52%
Younger Adults (PDA)
Self-efficacy (NA)3%
Self-efficacy (Soc)28%
Religiousness16%
Depression3%
SocNet: pro-abst.
25%
SocNet: pro-drk.
25%
Adults 30+ (PDA)
Self-efficacy (NA)1%
Self-ef-ficacy (Soc)38%
Religiousness6%Depression
3%SocNet: pro-abst.
10%
SocNet: pro-drk.
42%
Younger Adults (DDD)
Self-efficacy (NA)8%
Self-efficacy (Soc)29%
Religiousness19%
Depression12%
SocNet: pro-abst.14%
SocNet: pro-drk.18%
Adults 30+ (DDD)

MODERATED MEDIATION FINDINGS SUGGEST
AA-derived recovery benefits differ in nature and magnitude between more severely alcohol involved/impaired and less severely alcohol involved/impaired; men and women; and, young adults and adults 30+
Differences reflect differing needs based on recovery challenges related to differing symptom profiles, degree of subjective suffering and perceived severity/threat, life-stage based recovery contexts, and gender-based social roles & drinking contexts
Similar to psychotherapy literature (Bohart & Tollman, 1999) rather than thinking about how AA or similar organizations work, better to think how individuals use or make these organizations work for them – to meet most salient needs at any given phase of recovery

MODERATED-MECHANISMS: AA EFFECTS MODERATED BY SEVERITY, GENDER, AGE…
CONCLUSIONS
“Similar to the common finding that theoretically-distinct professional interventions do not result in differential patient outcomes, AA’s effectiveness may not be due to its specific content or process. Rather, its chief strength may lie in its ability to provide free, long-term, easy access and exposure to recovery-related common therapeutic elements, the dose of which, can be adaptively self-regulated according to perceived need. “
Kelly, Magill, Stout (2009)

IF WE REALLY BELIEVED ADDICTION WAS A CHRONIC DISEASE WE WOULD…
Stop talking dirty: adopt medical lexicon that is consistent with how we describe other conditions
Formulate, implement, and evaluate various sequences of services to determine the best practices in RM
Support development and testing of long-term cost-effective RM approaches that enhance patients’ self-care and provision of long-term professional monitoring akin to other CDM (e.g., linkage to MHOs and other self-care programs)