traumatic brain injury: original research on repeat head ct bradley w. thomas, md lcdr mc usn...
TRANSCRIPT

Traumatic Brain Injury: Original Research on
Repeat Head CTBradley W. Thomas, MD
LCDR MC USNConstanta Trauma Symposium
12 JUNE 2013

Introduction
Traumatic brain injury (TBI) is the foremost
cause of death in children and young
adults

TBI Facts
5.3 million Americans (just over 2% of the population) currently live with a disability resulting from a TBI
1.5 million people sustain an TBI each year
50,000 die due to TBI each year Every 21 seconds a person in the US
sustains an TBI In 2003, the overall expense for
direct TBImedical care was estimated at
more than $56 billion per year
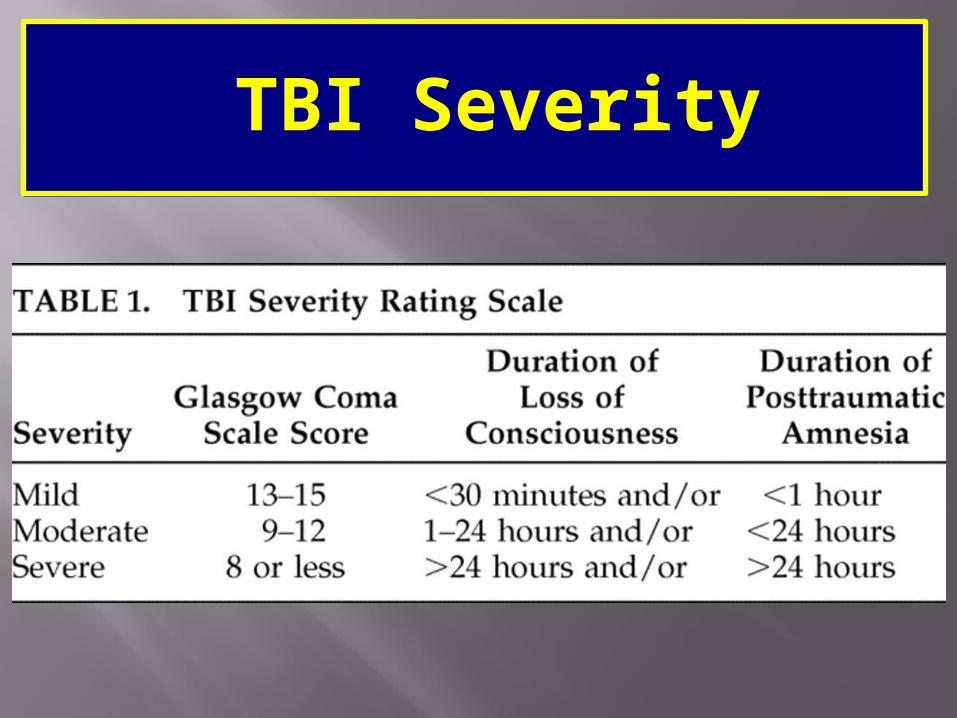
TBI Severity

TBI Treatment Modalities
Observation, Seizure Prophylaxis
Placement of ICP monitor Directed Mannitol/hypertonic Saline/ Chemical Paralysis to maintain CPP of 60mmHg
Ventriculostomy Craniotomy/Craniectomy

J Am Coll Surg. 2010 May;210(5):824-30, 831-2

This data was presented at the Southern Surgical Conference December 2009
No financial disclosures

• Initial evaluation of TBI*– Neurological examination– Initial brain computed tomography (IBCT)
• Subsequent evaluation – Unscheduled repeat brain CT (URBCT) for
neurologic deterioration is standard– Scheduled repeat brain CT (SRBCT) at
specified intervals is controversial
*Cushman. EAST Practice Management Guidelines for Management of Mild Traumatic Brain Injury.:http://www.east.org.

Unscheduled repeat brain CT (URBCT) based on neurological deterioration – May delay treatment – May lead to secondary brain injury and poor
outcome
Scheduled repeat brain CT (SRBCT) – Increases expense– Increases labor– Risks associated with transport– May not improve outcome
Difficult to assess long term functional capacity and productivity following TBI
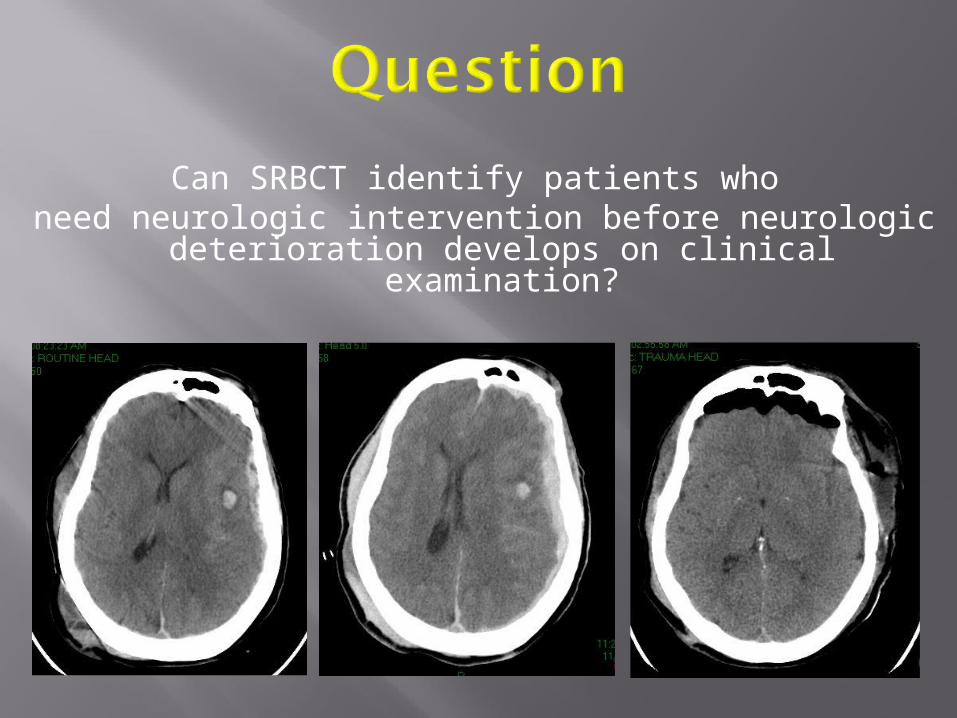
Can SRBCT identify patients who need neurologic intervention before neurologic deterioration develops on clinical examination?



Setting– Level I Trauma Center
Design– Retrospective observational study– IRB approved
Data– Trauma registry
Patients with TBI on initial brain CT (IBCT) – 50 month period beginning in November
2001– Medical record review
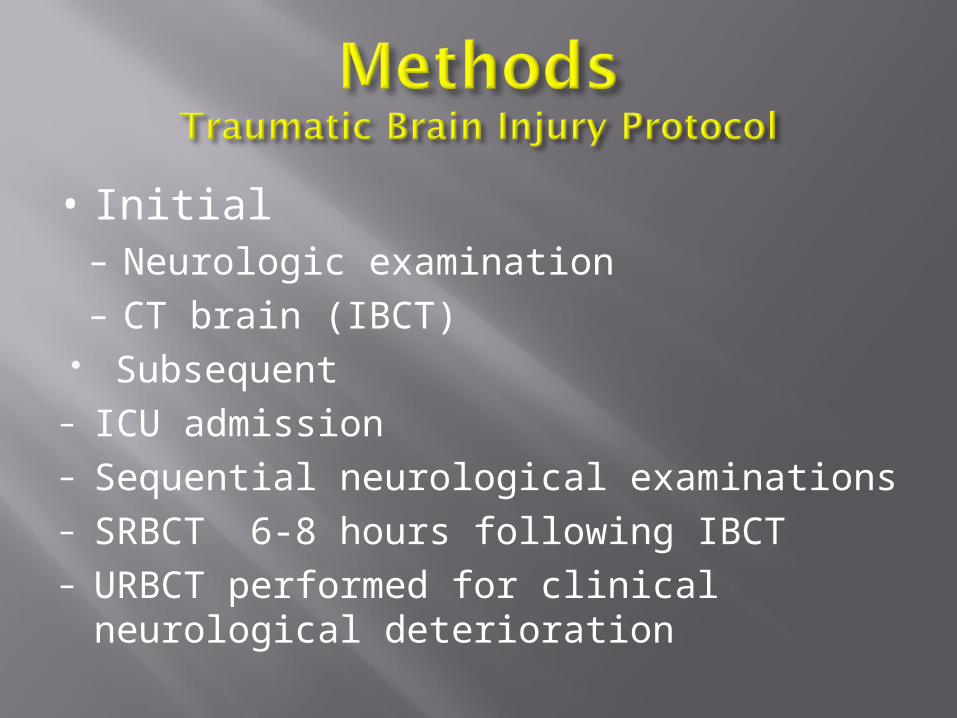
• Initial– Neurologic examination– CT brain (IBCT)
Subsequent– ICU admission– Sequential neurological examinations– SRBCT 6-8 hours following IBCT – URBCT performed for clinical neurological
deterioration

Demographics Age, sex
Mechanism of injury– Blunt injury only
Severity of injury Injury Severity Score (ISS) Admitting GCS
History Use of anticoagulants or anti-platelet
therapy

TBI admission data Type of TBI on IBCT
Subarachnoid hemorrhage Subdural hematoma Epidural hematoma Cerebral contusion Mixed
GCS on admission Mild (13-15) Moderate (9-12) Severe (3-8)

Post admission data Time from IBCT to SRBCT Frequency of SRBCT and URBCT
Outcome data Need for neurologic intervention ICU length of stay Hospital length of stay All cause hospital mortality

• Did patients undergo a neurologic intervention based on clinical change or SRBCT
• Was the 1st SRBCT worse or no worse

Medical intervention New onset administration of mannitol
or hypertonic saline
Surgical intervention Placement of an ICP monitor or
craniotomy

Statistical analysis was performed using SPSS version 17.0
Means are reported ± standard deviation
Chi square analysis and Wilcoxon rank sum test were used to compare groups where appropriate

9,669 patients admitted during the study period
1,019 patients had evidence of TBI on IBCT 132 patients excluded
87 (8.4%) immediate craniotomy 45 (4.5%)
–5 patients had no repeat head CT on file–29 patients died prior to repeat CT–1 loss of airway leading to anoxic injury–2 CVA secondary to other causes–8 patients had interventions based on unclear
indications 887 patients included


How did the results of SRBCT influence
patient management?

1st SRBCT worsen=195
immediate intervention
n=14
intervention secondary to
subsequent SRBCTn=7
intervention secondary to clinical
changen=19
no interventionn=155
intervention preceded by clinical
change ± URBCTn=11
887 undergo SRBCT
1st SRBCT no worse
n=692
no immediate intervention
n=181
no intervention n=681
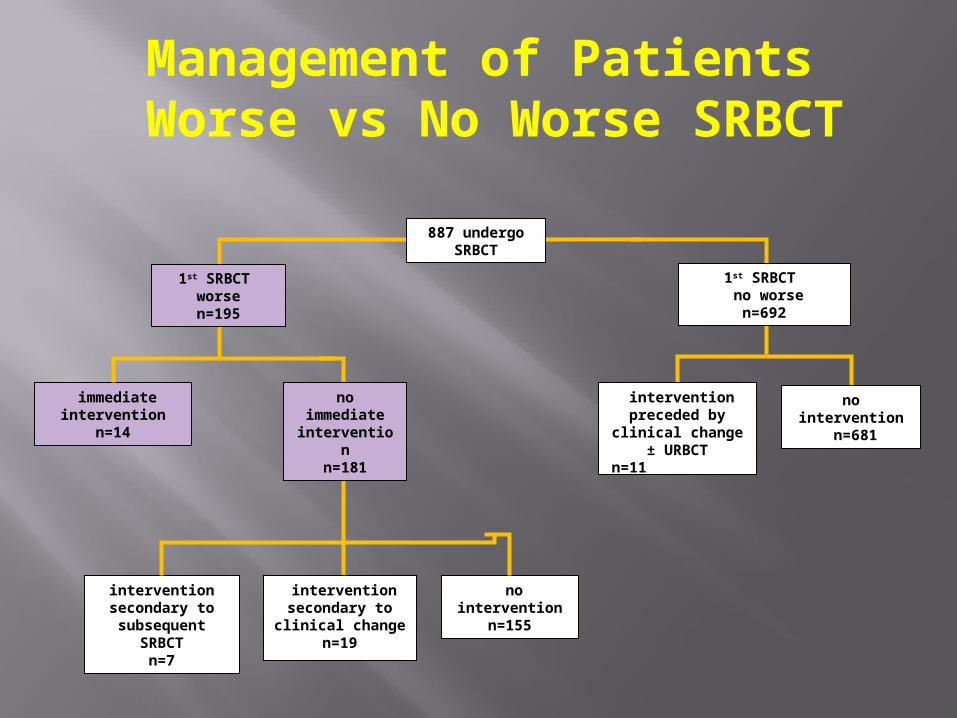
Management of Patients Worse vs No Worse SRBCT

1st SRBCT worsen=195
immediate intervention
n=14
intervention secondary to
subsequent SRBCTn=7
intervention secondary to clinical
changen=19
no interventionn=155
intervention preceded by clinical
change ± URBCTn=11
887 undergo SRBCT
1st SRBCT no worse
n=692
no immediate intervention
n=181
no intervention n=681
Management of Patients Worse vs No Worse SRBCT
1st SRBCT worsen=195
immediate intervention
n=14
intervention secondary to
subsequent SRBCTn=7
intervention secondary to clinical
changen=19
no interventionn=155
intervention preceded by clinical
change ± URBCTn=11
887 undergo SRBCT
1st SRBCT no worse
n=692
no immediate intervention
n=181
no intervention n=681
Management of Patients Worse vs No Worse SRBCT

1st SRBCT worsen=195
immediate intervention
n=14
intervention secondary to
subsequent SRBCTn=7
intervention secondary to clinical
changen=19
no interventionn=155
intervention preceded by clinical
change ± URBCTn=11
887 undergo SRBCT
1st SRBCT no worse
n=692
no immediate intervention
n=181
no intervention n=681
Management of Patients Worse vs No Worse SRBCT


1st SRBCT worsen=195
immediate intervention
n=14
intervention secondary to subsequent
SRBCTn=7
intervention secondary to
clinical changen=19
no interventionn=155
intervention preceded by
clinical change ± URBCT
n=11
887 undergo SRBCT
1st SRBCT no worse
n=692
no immediate intervention
n=181
no intervention n=681
Neurologic Change
No Neurologic Change
Total
SRBCT Worse 19 21 40/195 (20.5%)
SRBCT No Worse 11 681 11/692 (1.6%)
Chi square analysis shows greater likelihood for a patient with TBI to have aWorse SRBCT before they develop a neurologic change, p < 0.01
Analysis of Need for Neurologic Intervention Based on Worse SRBCT or Neurologic Change

The largest review to date shows that the majority of patients with no worse SRBCT required no further intervention
Patients with worse SRBCT had higher ISS, greater coagulopathy, longer length of stay and higher mortality
The vast majority (165/195, 92.8%) with worse SRBCT had no additional intervention
In 21/195 (10.7%) patients, a worse SRBCT prompted a number of interventions including diuresis for cerebral edema, ICP monitor placement and craniotomy
In 19/195 (10.5%) patients with a worse SRBCT subsequently developed neurologic change requiring an intervention
Patients with TBI are significantly more likely to have a worse SRBCT before they develop neurologic change that requires a neurologic intervention
• Retrospective study• CT findings subjective• Neurologic changes do not
necessarily mean secondary brain injury
• No long term follow-up
Treating a worse SRBCT before neurologic change occurs may prevent secondary brain injury
Protocol development for patients with worse SRBCT may improve outcome
Routine monitoring with SRBCT appears to be useful in managing patients with TBI

• Bee, Tiffany K. MD; Magnotti, Louis J. MD; Croce, Martin A. MD; Maish, George O. MD; Minard, Gayle MD; Schroeppel, Thomas J. MD; Zarzaur, Ben L. MD; Fabian, Timothy C. MD. Necessity of Repeat Head CT and ICU Monitoring in Patients With Minimal Brain Injury. J Trauma 2009 APR, pp. 66(4):1015-18.
• Brown CV, Weng J, Oh D, Salim A, Kasotakis G, Demetriades D, Velmahos GC, Rhee P. 2004 Dec. Does routine serial computed tomography of the head influence management of traumatic brain injury? A prospective evaluation. 2004 Dec, p. 57(6):1340.
• Brown CV, Zada G, Salim A, Inaba K, Kasotakis G, Hadjizacharia P, Demetriades D, Rhee P. 2007 Jun. Indications for routine repeat head computed tomography (CT) stratified by severity of traumatic brain injury. J Trauma. 2007 Jun, pp. 62(6):1339-44.
• Chao A, Pearl J, Perdue P, et al. Utility of routine serial computed tomography for blunt intracranial injury. J trauma; 2001; 51:870-5.
• Cushman JG, Agarwal N, Fabian TC, Garcia V, Nagy KK, Pasquale MD, Salotto AG and Group. EAST Practice Management Guidelines Work. 2001 Nov. Practice management guidelines for the management of mild traumatic brain injury: the EAST practice management guidelines work group. J Trauma. 2001 Nov, pp. 51(5):1016-26.
• Figg RE, Burry TS, Vander Kolk WE. 2003 Dec. Clinical efficacy of serial computed tomographic scanning in severe closed head injury patients. J Trauma. 2003 Dec, pp. 55(6):1061-4.
• Kaups KL, Davis JW, Parks SN. 2004 Mar. Routinely repeated computed tomography after blunt head trauma: does it benefit patients? J Trauma. 2004 Mar, pp. 56(3):475-80.
• Mendelow Ad, DarmiMZ, Paul KS, et al. Extradural haematoma: Effect of delayed treatment. Br Med J. 1979 May:1240-42.
• Sifri ZC, Homnick AT, Vaynman A, Lavery R, Liao W, Mohr A, Hauser CJ, Manniker A, Livingston D. 2006 OCT. A prospective evaluation of the value of repeat cranial computed tomography in patients with minimal head injury and an intracranial bleed. J Trauma. 2006 OCT, pp. 61(4):862-7.
• Sifri ZC, Livingston DH, Lavery RF, Homnick AT, Mosenthal AC, Mohr AM, Hauser CJ. 2004 Mar. Value of repeat cranial computed axial tomography scanning in patients with minimal head injury. Am J Surg. 2004 Mar, pp. 187(3):338-42.
• Stiell I, Wells G, Vandemheen K, et al. The Canadian CT Head Rule for patients with minor head injury. Lancet 2001;357:1391-6.
• Velmahos GC, Gervasini A, Petrovick L, Dorer DJ, Doran ME, Spaniolas K, Alam HB, De Moya M, Borges LF, Aladair AK. Routine Repeat Head CT for Minimal Head Injury is Unnecessary. J Trauma. 2006 Mar, pp. 60(3):494-499.