trauma of the upper third of the face
TRANSCRIPT

j. max.-fac. Surg. 12 (1984) 2 5 5
J. max.-fac. Surg. 12 (1984) 255-261 © Georg Thieme Verlag Stuttgart • New York
Trauma of the Upper Third of the Face Management and Follow-up Charis Ioannides, Hans Peter M. Freihofer, Ingolf Bruaset
Dept. of Oral and Maxillo-Facial Surgery, (Head: Prof. H. P. M. Freihofer, M.D., D.M.D.) Nijmegen, The Netherlands
Accepted for publication 27. 2. 1984
Introduction
The incidence of nasofrontal and frontobasal fractures is much lower than that of fractures of the middle third of the face and mandible. The treatment of the former presents more difficulties and significant complications and sequel- lae can occur acutely or many years after injury. Functional problems arise because of the adjacent delicate structures (eye, lacrimal apparatus, etc.). In cases with frontobasal fractures the dura is often torn and the resulting communication with the exterior can lead to severe intra- cranial complications. Disruption of the medial canthal ligament or comminution of the anterior wall of the frontal sinus and of the nasal skeleton cause aesthetic problems. Complete neurological evaluation and, if possible, detailed radiographic examination (Claussen et al., 1977, 1979), are necessary. The fracture is often more extensive than the X- rays suggest. The treatment aims at: 1. Converting an "open" fracture into a dosed one in order to avoid intracranial complications. 2. Restoring the functional capacity of injured structures. 3. Restoring the aesthetic appearance. The therapeutic approach is sometimes multidisciplinary because of the complexity of the problems. Close coopera- tion of the maxillofacial surgeon with the neuro- and ophthalmological surgeons is mandatory so that an optimal result can be obtained. The best possible result should be attempted during the first operation (Merville and Derome, 1978). The importance and duration of secondary opera- tions, which are more difficult anyway, are thus kept to a minimum. Late complications can occur years after the injury. The patients should therefore be followed up for a long postoperative period. The aim of this paper is the presentation of our cases and experience in the management of these fractures. Conclu- sions which could lead to their optimal treatment are drawn.
Material and Methods
407 patients with facial fractures were operated on at the Department of Oral and Maxillo-Facial Surgery of the University Hospital in Nijmegen between July 1979 and July 1982. Among them, 23 (5.6 %) (4 women and 19 men), presented with nasofrontal and/or frontobasal fractures. The
Summary
Of 407 patients with facial fractures who were oper- ated on at the Department of Oral and Maxillo-Facial Surgery, University Hospital, Nijmegen, over a 3-year period, 23 had a fracture in the nasofrontal region with or without extension to the base of the skull. The problems and results of the treatment of these fractures are presented, with special reference to the manage- ment of the frontal sinus lesions, the lacrimal system, and the reconstruction of the nasal skeleton and canthal attachments. The postoperative complications and sequellae are discussed. Most prominent features are ocular problems and unsatisfactory nasal contour. Conclusions which could contribute to the proper therapeutic management are drawn.
Key-Words
Fracture, nasofrontal, frontobasal - Frontal sinus - Surgical management - Follow-up.
youngest patient was 7 and the oldest 78 years old, the mean age being 33.5 years (Fig. 1). The main causes were in traffic accidents, accounting for 16 of the injuries. Sport was the cause in 4, accidental fall in 2 and a suicide attempt in 1 case (Table 1). In 7 cases the fracture was situated in the frontal area, 6 could be classified as nasofrontal and 10 as frontobasal (Table 2). Several patients presented associated facial and non facial injuries (Table 3, 4). From the many classifications proposed, the one suggested by Pothe (1978) is of clinical interest. He divides fron- tobasal fractures into: 1. Direct open fracture with soft tissue injuries, in the
frontal region, liquor leakage and eventual brain pro- lapse. The indication for operation is absolute and urgent.
2. Indirect open fracture with persisting liquor leakage for 6 to 10 days. The term indirect refers to the communica- tion through the sinus. The indication for operation is absolute and the patient should be operated on within the time limits mentioned.
Pat ien ts
4-
:2-
_ ~ , _ 0 20 40 60 80
Age
Fig. 1 Ages of the 23 injured patients.
256 J. max.-fac. Surg. 12 (1984) Ch. Ioannides et al.
Fig. 2a Fig. 2b
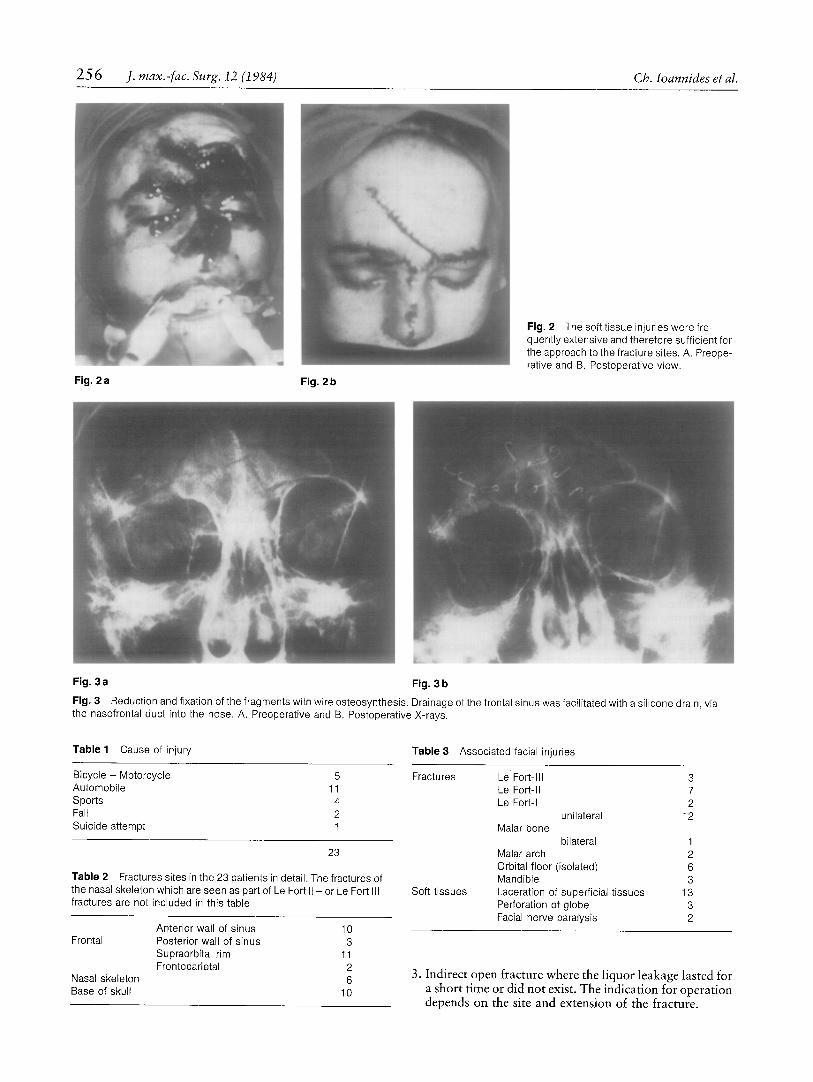
Fig. 2 The softtissue injuries were fre- quently extensive and therefore sufficient for the approach to the fracture sites. A. Preope- rative and B. Postoperative view.
Fig. 3 a Fig. 3 b
Fig. 3 Reduction and fixation of the fragments with wire osteosynthesis. Drainage of the frontal sinus was facilitated with a silicone drain, via the nasofrontal duct into the nose. A. Preoperative and B. Postoperative X-rays.
Table 1 Cause of injury Table 3 Associated facial injuries
Bicycle - Motorcycle 5 Fractures Le Fort-Ill 3 Automobile 11 Le Fort-II 7 Sports 4 Le Fort-I 2 Fall 2 unilateral 12 Suicide attempt 1 Malar bone
23
Table 2 Fractures sites in the 23 patients in detail. The fractures of the nasal skeleton which are seen as part of Le Fort II - or Le Fort III fractures are not included in this table
bilateral 1 Malar arch 2 Orbital floor (isolated) 6 Mandible 3 Laceration of superficial tissues 13 Perforation of globe 3 Facial nerve paralysis 2
Frontal
Nasal skeleton Base of skull
Anterior wall of sinus 10 Posterior wall of sinus 3 Supraorbital rim 11 Frontoparietal 2
6 10
Soft tissues
3. Indirect open fracture where the liquor leakage lasted for a short time or did not exist. The indication for operation depends on the site and extension of the fracture.

Trauma of the Upper Third of the Face J. max.-fac. Surg. 12 (1984) 257
Fig. 4 a Fig. 4 b Fig. 4 c
Fig. 4 d
Fig. 4 Patient with an extensive frontobasal fracture. A. Preoperative clinical view. The soft tissue injury runs from the right nasal ala over the nose to the middle of the forehead. B, Frontal view of the patient 1 month postoperatively. The result is satisfactory. U nfortu nately the neurosurgeon extended the soft tissue injury cranially to gain access to the inner aspect of the skull thus increasing the aesthetic defect of the scar. C. One year postoperatively. The appearance of the scar has improved considerably. D. Preoperative X-rays showing fracture of medial orbital wall, nasal skeleton, frontal bone (anterior and posterior
Fig. 4 e
wall of frontal sinus) with loss of bone. The indication for operation was absolute because of the direct communication between brain and the exterior. E. X-ray postoperatively. The signs of craniotomy are clearly seen. It was used for the repair of the extensive injury to the dura, The frontal sinus mucosa was removed, the sinus was obliter- ated with cancellous bone and the anterior wall was reconstructed with a corticocancellous graft harvested from the right iliac crest, Certain fragments and the canthus were reduced and fixed with wire osteosynthesis.
An expectant attitude is justified. Basically this rationale is applied, with the modification, that an absolute indication for intervention in the second
Tab le4 Associated non-facial injuries
Upper extremities 3 Lower extremities 3 Clavicle 2 Ribs 1 Lung contusion 1
group is if the liquor leak persists after two weeks. Of the 23 cases 4 belonged to the first, 5 to the second and 14 to the third group. All our patients were operated on within 6 days after the accident. In order to gain access to the fracture sites, we used the pre- existing extensive soft tissue wounds in 11 cases (Fig. 2). An eyebrow incision was used in 7 and an anterior coronal flap in 1 case. Whenever possible, fragments were reduced and fixed with direct wiring (Tab. 5). In all cases of reconstruc- tion of the frontal sinus it was drained into the nasal cavity and the drain was left in situ for 4 to 6 weeks (Fig. 3). The damaged dura was repaired, in 2 cases via craniotomy and

2 5 8 J. rnax.-fac. Surg. 12 (1984) Ch. Ioannides et al.
Fig. 5 a
Fig. 5 Extensive frontobasat fracture. A. Loss of bone of the anterior wall of the frontal sinus. B. The dura injuries were repaired with lyophilized dura, the mucosa of the sinus was removed, the sinus was
Fig. 5 b
obliterated, certain fragments were reduced and the anterior wall was reconstructed with corticocancellous bone.
Table 5 Treatment performed
Reduction-wiring 15 Dura repair via craniotomy 2
via frontal sinus or frontal fracture 6 Canthopexy 6 Obliteration frontal sinus 3 Reconstruction (ant. wall of sinus, orbit, etc.) 6 Reconstruction nasal skeleton 4 Orbital exenteration 3 No treatment 4
in 2 cases via the frontal sinus, by using lyophilized dura for bigger defects and suturing the smaller ones (Fig. 4). In 3 cases there was extensive loss of bone in the anterior wall of the frontal sinus with corresponding damage to the mucosal lining and nasofrontal duct. In all three the mucosa was completely removed and the sinus was obliterated with cancellous bone, harvested from the right iliac crest. The cortical plates of the graft were used for the reconstruction of the anterior wall of the sinus (Fig. 5, 6). In 3 further cases reconstruction of the orbital walls was necessary. Twice, iliac crest cortical bone was used and once, a bone graft removed from the anterior wall of the contralatera] maxil- lary sinus. Disruption of the medial canthal ligament caused telecanthus (37-45 ram.) in 6 patients. In all cases the ligament was still attached to a (sometimes very small) bone fragment which was reduced and fixed via an indirect canthopexy to the contralateral side (Fig. 4). Lead plates fixed with transnasal wires were used to secure the result after the skin wounds had been sutured. The nasal skeleton was comminuted in 4 cases making its adequate reduction impossible. Reconstruction was neces- sary and bone grafts from the right iliac crest were used for this purpose (Fig. 6). Exenteration of the orbital contents had to be performed in 3 cases because of a perforation of the globe and/or damage to the optic nerve. Lacerations of the lacrimal apparatus were not treated primarily.
In 4 cases of fracture of the anterior wall of the frontal sinus there were no functional and aesthetic problems. There was no displacement of the fragments, therefore no treatment was considered necessary.
Results
Of the 23 patients one died of cardiovascular complica- tions. The follow-up period of the other 22 ranged from 10 months to almost 4 years. Three patients still suffer from headaches. Radiographic examination, however, did not demonstrate any pathology. Eight patients presented ocular problems, mostly decreased visual acuity. One patient, suffering from diplopia which did not respond to orthoptic treatment, was operated on by the ophthalmological surgeon. The adhesions of the inferior rectus muscle were detached and the superior rectus muscle was advanced 2 ram. Most of the above-mentioned patients are still under observation at the Department of Ophthal- mology. One of the 6 patients where a canthopexy was performed showed a slight relapse. The intercanthal distance measured 31 ram. 1 week postoperatively. Six months later it had increased to 34 ram. Since this distance is still within normal limits, no further correction was considered neces- sary. Five patients, one of them having undergone an exentera- tion of the orbital contents, suffer from a mild or more severe epiphora. One of them developed dacryocystitis, due to an obstruction of the nasolacrimal duct. Secondary dacryocystorhinostomy has solved this problem. The other 4 patients did not wish any secondary correction. In 9 patients the sensibility of the frontal skin area is diminished or altered, due to damage to the supratrochlear or supraorbital nerves. Damage to the olfactory nerve was the cause of partial or total loss of the sense of smell in 11 patients. Three patients were not satisfied with the aesthetic appear- ance of their noses. Two were improved by secondary

Trauma of the Upper Third of the Face J. max.-fac. Surg. 12 (1984) 259
Fig. 6a Fig. 6 b
,
Fig. 6 c Fig. 6 d Fig. 6 e
Fig. 6 Patient kicked by her horse suffered severe injuries of the naso-fronto-orbital area. A. Preoperative clinical appearance. B. More detailed picture. One arrow shows the defect of the posterior wall of the sinus. The other arrows show the margins of the bone loss of the anterior wall of the frontal sinus. The nasal skeleton was also destroyed and the fracture at the medial orbital wall ran back as far as the optic foramen. C. Frontal view one year postoperatively. The
rhinoplasty with onlay grafts (Fig. 7), one by remodelling of the primary graft. Three more patients have a slight nasal deformity, but did not consider it severe and declined further operations. The appearance of the scars was not satisfactory in 5 patients. Three of them wished secondary corrections. In one patient who had concomitant midface fractures, an orbital asymmetry persists. The right orbit is displaced inferiorly and laterally. Secondary osteotomy is planned.
frontal sinus is obliterated with autologous bone; the frontal defect, the orbital walls and the nasal skeleton are reconstructed. The left eye was lost due to the injury and replaced by a prosthesis. D. Lateral view. Although the result was very satisfactory the patient wished correction of the slight prominence at the bridge of the nose. E. Total body scan of the patient 17 months postoperatively. Increased activity is still seen in the frontal area.
Finally, psychological changes such as phobia, loss of self- confidence or aggressiveness were seen in 5 patients. Two of them are still under psychiatric treatment.
Discussion
Fractures of the nasofrontal area extending or not to the base of the skull are relatively rare (Miller et al., 1978; Adkins et al., 1979; Lanigan and Stoelinga, 1980) corn-
260 J. max.-fac. Surg. 12 (1984) Ch. Ioannides et aI.
Fig. 7 a Fig. 7 b
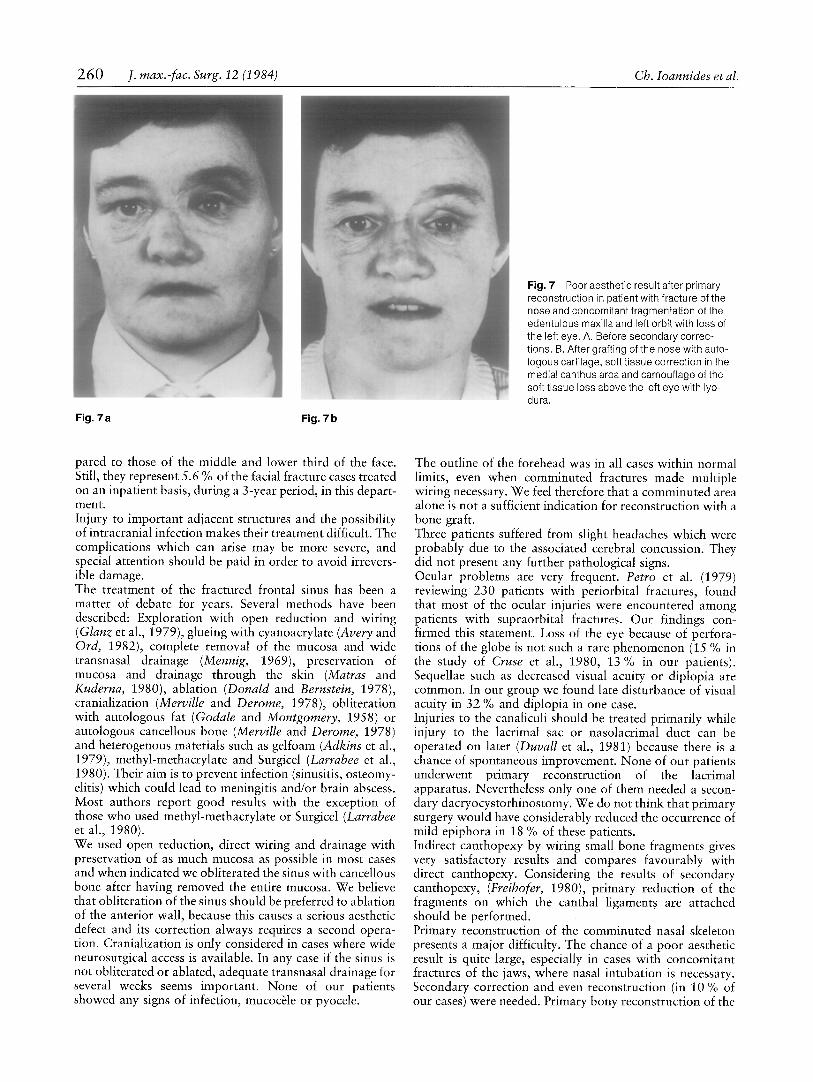
Fig. 7 Poor aesthetic result after primary reconstruction in patient with fracture of the nose and concomitant fragmentation of the edentulous maxilla and left orbit with loss of the left eye. A. Before secondary correc- tions. B. After grafting of the nose with auto- logous cartilage, soft tissue correction in the medial canthus area and camouflage of the soft tissue loss above the left eye with lyo- dura.
pared to those of the middle and lower third of the face. Still, they represent 5.6 % of the facial fracture cases treated on an inpatient basis, during a 3-year period, in this depart- ment. Injury to important adjacent structures and the possibility of intracranial infection makes their treatment difficult. The complications which can arise may be more severe, and special attention should be paid in order to avoid irrevers- ible damage. The treatment of the fractured frontal sinus has been a matter of debate for years. Several methods have been described: Exploration with open reduction and wiring (Glanz et al., 1979), glueing with cyanoacrylate (Avery and Ord, 1982), complete removal of the mucosa and wide transnasal drainage (Mennig, 1969), preservation of mucosa and drainage through the skin (Matras and Kuderna, 1980), ablation (Donald and Bernstein, 1978), cranialization (Merville and Derome, 1978), obliteration with autologous fat (Godale and Montgomery, 1958) or autologous cancellous bone (Merville and Derome, 1978) and heterogenous materials such as gelfoam (Adkins et al., 1979), methyl-methacrylate and Surgicel (Larrabee et al., 1980). Their aim is to prevent infection (sinusitis, osteomy- elitis) which could lead to meningitis and/or brain abscess. Most authors report good results with the exception of those who used methyl-methacrylate or Surgicel (Larrabee et al., 1980). We used open reduction, direct wiring and drainage with preservation of as much mucosa as possible in most cases and when indicated we obliterated the sinus with cancellous bone after having removed the entire mucosa. We believe that obliteration of the sinus should be preferred to ablation of the anterior wall, because this causes a serious aesthetic defect and its correction always requires a second opera- tion. Cranialization is only considered in cases where wide neurosurgical access is available. In any case if the sinus is not obliterated or ablated, adequate transnasal drainage for several weeks seems important. None of our patients showed any signs of infection, mucochle or pyocele.
The outline of the forehead was in all cases within normal limits, even when comminuted fractures made multiple wiring necessary. We feel therefore that a comminuted area alone is not a sufficient indication for reconstruction with a bone graft. Three patients suffered from slight headaches which were probably due to the associated cerebral concussion. They did not present any further pathological signs. Ocular problems are very frequent. Petro et al. (1979) reviewing 230 patients with periorbital fractures, found that most of the ocular injuries were encountered among patients with supraorbital fractures. Our findings con- firmed this statement. Loss of the eye because of perfora- tions of the globe is not such a rare phenomenon (15 % in the study of Cruse et al., 1980, 13 % in our patients). Sequellae such as decreased visual acuity or diplopia are common. In our group we found late disturbance of visual acuity in 32 % and diplopia in one case. Injuries to the canaliculi should be treated primarily while injury to the lacrimal sac or nasolacrimal duct can be operated on later (Duvall et al., 1981) because there is a chance of spontaneous improvement. None of our patients underwent primary reconstruction of the lacrimal apparatus. Nevertheless only one of them needed a secon- dary dacryocystorhinostomy. We do not think that primary surgery would have considerably reduced the occurrence of mild epiphora in 18 % of these patients. Indirect canthopexy by wiring small bone fragments gives very satisfactory results and compares favourably with direct canthopexy. Considering the results of secondary canthopexy, (Freihofer, 1980), primary reduction of the fragments on which the canthal ligaments are attached should be performed. Primary reconstruction of the comminuted nasal skeleton presents a major difficulty. The chance of a poor aesthetic result is quite large, especially in cases with concomitant fractures of the jaws, where nasal intubation is necessary. Secondary correction and even reconstruction (in 10 % of our cases) were needed. Primary bony reconstruction of the

Trauma of the Upper Thirdofthe Face J. max.-fac. Surg. 12 (1984) 261
nasal skeleton was performed only if a bone graft was harvested for other purposes also. It is suspected, that a less restrictive indication would have reduced the number of secondary operations. However, it remains a technically difficult procedure in cases with associated extensive mid- face fractures. We see no reason for surgical intervention if there are no functional and aesthetic problems and no displacement of the fragments. The 4 patients who belong to this group presented no sequellae at the late follow-up. The severity of superficial lesions, deep injuries and general condition of the patient do not always correlate (Matras and Kuderna, 1980). This was confirmed in our series. Therefore, thorough radiographic evaluation, if need be including computed tomography (Claussen et al., 1977, 1978) should be carried out in all cases, even if the clinical picture is not suggestive of serious injuries. If the general condition of the patient permits, one should try early to achieve an optimal result primarily. Sometimes, however, the condition is so critical that only the absolutely necessary steps can be taken. Besides haemostasis, preven- tion of infection by drainage seems to be the most impor- tant. Late primary management is still preferable to secon- dary surgery. Intra-cranial complications sometimes occur many years after the injury (Mennig, 1969; Pothe, 1980). Up to now we have not seen this in any of our patients. They will, how- ever, be followed for a long period in order to be able to diagnose and treat such complications early.
Conclusions
1. Nasofrontal and frontobasal fractures are severe injuries which often demand a multidisciplinary approach for their treatment.
2. The frontal sinus should be drained after reduction of the fragments. If reduction of the fragments is not possible, it can be primarily obliterated with autologous bone grafts.
3. The primary reduction of bone fragments without bone grafting in cases of a comminuted nasal skeleton often leads to a poor aesthetic result. Secondary corrections are then necessary.
4. Ocular problems persist very often despite careful bony reconstruction. Late problems arising from the lacrimal apparatus on the other hand are scarce in spite of the fact that these lesions are not treated primarily.
Acknowledgement We thank the Dept. of Neurosurgery (Head: Prof. H. Walder, M. D.) and the Dept. of Ophthalmology (Head: Prof. A. F. Deutman, M.D.) for their cooperation in some of the cases described above.
References Adkins, W. Y., R. Douglas Cassone, F. Johnsons Putney: Solitary
frontal sinus fracture. Laryngoscope 89 (1979) 1099-1104 Avery, B. S., R. A. Ord: The use of butyl-cyanoacrylate as a tissue
adhesive in maxillo-facial and cranio-facial surgery. Br. J. Oral Surg. 20 (1982) 84
Claussen, C. D., F. W. Lohkamp, A. Krestel: Computed Tomography of Trauma Involving Brain and Facial Skull (Craniofacial injuries). J. of Comp. Ass. Tomog. 1 (1977) 472-481
Claussen, C, D., F. W. Lohkamp, H. Spenneberg, E. Gliick: Com- putertomographie bei ffontobasalen Sch~idelhirnverletzungen. Laryng. Rhinol. 57 (1978) 698-706
Cruse, C. W., P. K. Blevins, E. A. Luce: Naso-ethmoid orbital frac- tures. J. Trauma. 20 (1980) 551-556
Donald, P., L. Bernstein: Compound Frontal Sinus Injuries with Intracranial Penetration. Laryngoscope 88 (1978) 225-232
Duvall, A. J., D. A. Foster, D. P. Lyons, R. D. Letson: Medial Canthoplasty: Early and Delayed Repair. Laryngoscope 91 (1981) 173-183
Freibofer, H. P. M.: Experience with Transnasal Canthopexy. J. max.- fac. Surg 8 (1980) 119-224
Glanz, H., H. G. Schroeder, D. Kleinsasser: Sofortige Rekonstruktion der frakturierten Stirnh6hlenvorwand. Laryng. Rhinol. 58 (1979) 653-659
Godale, R., W. W. Montgomery: Experiences with the anterior osteo- plastic approach to the frontal sinus. Arch. Otolaryng. 68 (1958) 279
Lanigan, D. T., P. J. W. Stoelinga: Fractures of the supraorbital rim. J. Oral Surg. 38 (1980) 764-770
Larrabee, W. F., L. W. Travis, H. G. Tabb: Frontal Sinus Fractures - The i r Suppurative Complications and Surgical Management. Laryngoscope 90 (1980) 1810-1813
Matras, H., H. Kuderna: Combined cranio-facial fractures. J. max.- fac. Surg. 8 (1980) 52-59
Mennig, H.: Die oto-rhinologischen Komplikationen bei Kiefer- Gesichtsverletzungen und ihre Behandlungsprinzipien. In E. Reichenbach ed.: Traumatologie im Kiefer-Gesichtsbereich. Barth, Leipzig 1969
Merville, L. C., P. Derome: Concomittant Dislocations of the Face and Skull. J. max.-fac. Surg 6 (1978) 2-14
Miller, S. H., R. J. Lung, T. S. Davis, W. P. Graham, T. J. Kennedy: Management of Fractures of the Supraorbital Rim. J. Trauma. 18 (1978) 507-512
Petro, J., F. M. Tooze, C. R. Bales, G. Baker: Ocular Injuries Associ- ated with Periorbital Fractures. J. Trauma. 19 (1979) 730-733
Potbe, H.: Zu einigen Problemen bei der Therapie frontobasaler Frakturen. Stomatol. D.D.R. (1978) 545-547
Pothe, H.: Zur Problematik der verz6gerten Versorgung von Liquor- fisteln nach frontobasalen Frakturen. Beitr. Orthop. u. Traumatol. 27 (1980) 90-94
Pro~ Dr. H. P. M. Freihofer MD, DMD Afd. Kaakchirurgie St. Radboudziekenhuis Geert Grooteplein Zuid 14 Katholieke Universiteit NL-6500 HB Nijmegen