trauma brain injury
DESCRIPTION
slide ini berisikan tentang trauma pada kepala.TRANSCRIPT

Head TraumaHead Trauma
Dr. Candy Lauwrenz SpS, MMKes, QIA

Head TraumaHead TraumaStatistics Statistics :: In USA, 150In USA, 150-300-300 peoples dead due to head injury per peoples dead due to head injury per
yearyear.. Mortality rate of TBI is about 25 /100.000 popMortality rate of TBI is about 25 /100.000 population ulation
annualyannualy Disability rate are three timeDisability rate are three time Main dead cause of young productive peoplesMain dead cause of young productive peoples Cost : $ 400 billion per yearCost : $ 400 billion per year - Income loss - Medical fee- Income loss - Medical fee - Insurance cost - Indirect cost- Insurance cost - Indirect cost
(Narayan, 2005)(Narayan, 2005) No data in IndonesiaNo data in Indonesia

Pathophysiology Pathophysiology
Traumatic Brain InjuryTraumatic Brain Injury
Primary vs. SecondaryPrimary vs. SecondaryInjuryInjury
Primary injury - directPrimary injury - direct
physical injury to neurons andphysical injury to neurons and
glial cellsglial cellsSecondary injury -Secondary injury -
physiological events after thephysiological events after the
primary injury primary injury furtherfurther damage.damage.

Primary InjuryPrimary Injury
ImpactImpact : epidural, subdural,: epidural, subdural, contusion, intracerebralcontusion, intracerebral hemorrhage, hemorrhage, skull fractures skull fractures
InertialInertial : concussion, diffuse axonal : concussion, diffuse axonal injury injury
Hypoxic/IschemicHypoxic/Ischemic

Secondary InjurySecondary Injury
Hypoxic-ischemic injury Hypoxic-ischemic injury Release of excitatory amino acids Release of excitatory amino acids Excess NMDA receptor activity Excess NMDA receptor activity Concurrent hypotension and Concurrent hypotension and
hypoxemia may be present hypoxemia may be present Inflammatory responseInflammatory response





1111
JJenis trauma enis trauma ::
EkstrakranialEkstrakranialLuka pada jaringan kulit bisaLuka pada jaringan kulit bisa : :
Luka tertutupLuka tertutup oleh karena benda oleh karena benda tumpul berupa hematoma.tumpul berupa hematoma.
Luka terbukaLuka terbuka akibat benda tajam / akibat benda tajam / runcing seperti luka sayat, luka runcing seperti luka sayat, luka tusuk, terpotongtusuk, terpotong..

1212

1313
Fraktur TengkorakFraktur TengkorakFraktur pada batok kepala : Fraktur pada batok kepala :
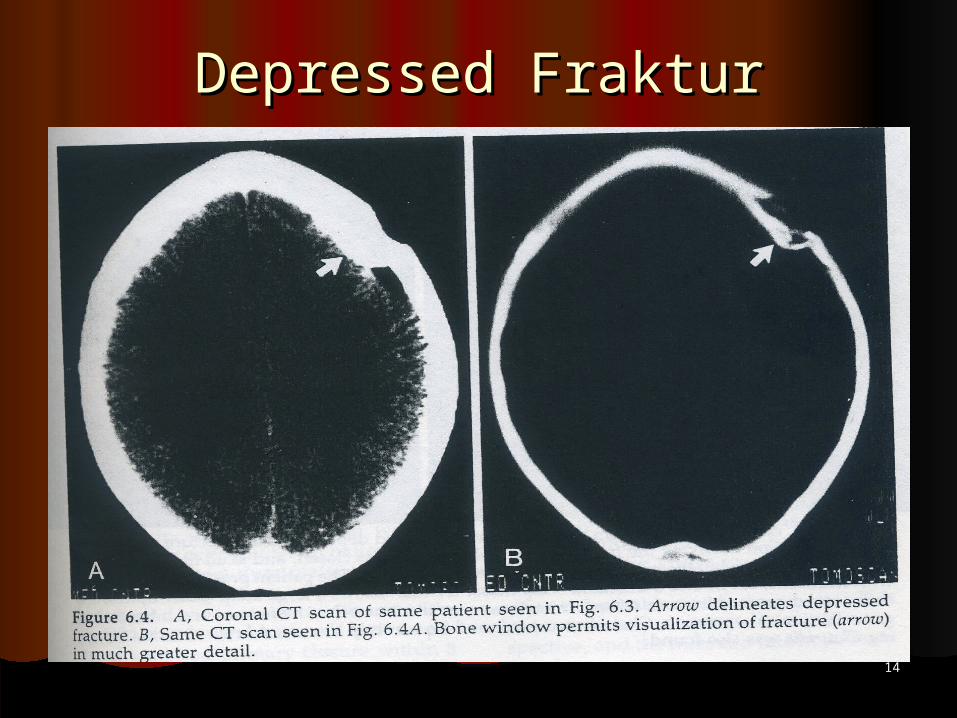
Linier frakturLinier frakturDepresed frakturDepresed frakturComminuted frakturComminuted fraktur
Fraktur pada basis tengkorakFraktur pada basis tengkorakLongitudinal frakturLongitudinal frakturTransversal frakturTransversal frakturCircular frakturCircular fraktur
JJenis trauma enis trauma ::
1414
Depressed FrakturDepressed Fraktur

1515
1616

1717
IntIntrrakranialakranial
Trauma serebriTrauma serebri : :Komotio serebriKomotio serebriKontusio serebriKontusio serebriLaserasi serebriLaserasi serebri
JJenis trauma enis trauma ::

1818
Mekanisme trauma serebri :Mekanisme trauma serebri :
PPergeseran, otak dapat ergeseran, otak dapat bergesekan dengan tulang bergesekan dengan tulang tengkoraktengkorak
Tergencet & terjepit oleh Tergencet & terjepit oleh jaringan keras disekitarnyajaringan keras disekitarnya
Mengalami pantulan (counter Mengalami pantulan (counter coup)coup)

1919
Akibat trauma serebri berupa Akibat trauma serebri berupa
oedema serebrioedema serebriperdarahan subaraknoid, subdural, perdarahan subaraknoid, subdural,
epiduralepiduralpetechia / hematoma intraserebralpetechia / hematoma intraserebral laserasi / memarlaserasi / memarterpotongterpotong

Guidelines for the Guidelines for the ManagementManagement
Initial : Initial :
Airway and OxygenationAirway and OxygenationBreathingBreathingBlood Pressure ControlBlood Pressure ControlSeizures PreventionSeizures PreventionFluid and Nutrition Fluid and Nutrition Body TemperatureBody TemperatureExitation, vomitus, headacheExitation, vomitus, headache
(Fewel et al, (Fewel et al, 2003)2003)

CONSIDER ….CONSIDER ….
Cerebral Blood Flow (CBF)Cerebral Blood Flow (CBF)Mean Arterial Pressure (MAP)Mean Arterial Pressure (MAP)Intracranial Pressure (ICP)Intracranial Pressure (ICP)

2222
PENILAIAN GLASSGOW PENILAIAN GLASSGOW COMA SCALE (GCS) COMA SCALE (GCS)
TAMPAKAN SKALA NILAI
EYE OPENING SPONTAN 4
DIPANGGIL 3
RANGSANG NYERI 2
TIDAK ADA RESPONSE (DIAM)
1

2323

2424
PENILAIAN GLASSGOW PENILAIAN GLASSGOW COMA SCALE (GCS) COMA SCALE (GCS)
TAMPAKAN SKALA NILAI
VERBAL RESPONSE
ORIENTASI BAIK 5
JAWABAN KACAU 4
KATA-KATA TIDAK PATUT (INAPPROPRIATE)
3
BUNYI TAK BERARTI INCOMPREHENSIBLE
2
TIDAK BERSUARA 1

2525
PENILAIAN GLASSGOW PENILAIAN GLASSGOW COMA SCALE (GCS) COMA SCALE (GCS)
MOTOR RESPONSE
SESUAI PERINTAH 6
LOKALISASI NYERI 5
REAKSI PADA NYERI 4
FLEKSI (DEKORTIKASI) 3
EKSTENSI (DESEREBRASI)
2
TIDAK ADA RESPONSE (DIAM)
1

2626

2727

MANAGEMENT OF MANAGEMENT OF INCREASED ICPINCREASED ICP
Head elevationHead elevation HyperventilationHyperventilation Osmotic TherapyOsmotic Therapy SedationSedation Cerebrospinal Fluid Drainage ( Ventricular, Subdural Cerebrospinal Fluid Drainage ( Ventricular, Subdural
Drainage )Drainage )
beneficial in treating the hydrocephalus seen in beneficial in treating the hydrocephalus seen in thalamicthalamic hemorrhage with ventricular extension hemorrhage with ventricular extension
(Broderick et al, 1999; Fewel et al., 2003)(Broderick et al, 1999; Fewel et al., 2003)

ICP MONITORINGICP MONITORING
Placed in patient with GCS = 9Placed in patient with GCS = 9 Cerebral Edema on CT, Multipel Intracranial Cerebral Edema on CT, Multipel Intracranial
LesionsLesions The duration not exceed of 5 daysThe duration not exceed of 5 days Patient with suspected elevation ICP and Patient with suspected elevation ICP and
deteriorating level of conciousness are candidates deteriorating level of conciousness are candidates for invasive ICP Monitoringfor invasive ICP Monitoring
Intraventricular ICP monitoring and Intraventricular ICP monitoring and intraparenchymal fiber optic ICP device are two intraparenchymal fiber optic ICP device are two comcommonly used methods of monitoring ICPmonly used methods of monitoring ICP
(Orlando Regional Health Care, 2003)(Orlando Regional Health Care, 2003)

PharmacologicalPharmacological
NeuroprotectionNeuroprotection
1.1. Glutamate receptor antagonists,Glutamate receptor antagonists,
2.2. Calcium antagonists Calcium antagonists
3.3. Free radical scavengers,Free radical scavengers, andand
4.4. Cyclosporin ACyclosporin A
1. Glutamate receptor 1. Glutamate receptor antagonistsantagonists
The amino acid L-glutamate is anThe amino acid L-glutamate is an extensively distributed, mostlyextensively distributed, mostly excitatory neurotransmitter in theexcitatory neurotransmitter in the CNS.CNS.
Extracellular glutamate >> Extracellular glutamate >> deleterious effects to neurons.deleterious effects to neurons.
Glutamate receptors : NMDA,Glutamate receptors : NMDA, AMPAAMPA and Kainate receptors.and Kainate receptors.

2. 2. Calcium AntagonistCalcium Antagonist
NimodipineNimodipineNot recommended for severely Not recommended for severely
headhead injuredinjured patients.patients.Treatment of the TBI patients Treatment of the TBI patients
withoutwithout signs of subarachnoid signs of subarachnoid bleeding is notbleeding is not indicated.indicated.

3. Free radical scavengers3. Free radical scavengers
TBI may lead to an increase in intracellularTBI may lead to an increase in intracellular free radical activity.free radical activity.
Antioxidatives agents:Antioxidatives agents:TirilazadTirilazad
No significant positive influence of No significant positive influence of treatmenttreatment
with tirilazad on outcome of severely TBIwith tirilazad on outcome of severely TBI (phase III)(phase III)
Polyethylene glycol-conjugated Polyethylene glycol-conjugated superoxidesuperoxide dismutase (PEG-SOD).dismutase (PEG-SOD).
Trend towards better outcome Trend towards better outcome comparedcompared placeboplacebo (phase III)(phase III)
4. Cyclosporin A4. Cyclosporin A Cyclosporin is a cyclic polypeptide,Cyclosporin is a cyclic polypeptide,
consisting of 11 amino acids.consisting of 11 amino acids. Transplantation medicine as anTransplantation medicine as an
iimmunosuppressantmmunosuppressant Protective effect on mitochondrialProtective effect on mitochondrial
ultrastructure, and most likelyultrastructure, and most likely mitochondrial function, and onmitochondrial function, and on cytoskeletal cytoskeletal derangements after TBIderangements after TBI (animals study).(animals study).
No clinical phase II or III trials evaluatingNo clinical phase II or III trials evaluating the efficacy of cyclosporin A in thethe efficacy of cyclosporin A in the treatment of human severe TBItreatment of human severe TBI

CiticholinCiticholin
Mechanisms:Mechanisms: Preserving cardiolipin (an exclusive innerPreserving cardiolipin (an exclusive inner
mitochondrial membrane component) andmitochondrial membrane component) and sphingomyelin;sphingomyelin;
Preserving the arachidonic acid content ofPreserving the arachidonic acid content of PtdCho and Ptd-ethanolamine;PtdCho and Ptd-ethanolamine;
Partially restoring PtdCho levels;Partially restoring PtdCho levels; Stimulating glutathione synthesis andStimulating glutathione synthesis and
glutathione reductase activity;glutathione reductase activity; Attenuating lipid peroxidation; andAttenuating lipid peroxidation; and Restoring Na/K-ATPase activity.Restoring Na/K-ATPase activity.
ConclusionsConclusions
Pathophysiological cascades initiated by Pathophysiological cascades initiated by injury ofinjury of brain have many features in brain have many features in common, and braincommon, and brain ischemia and ischemia and mitochondria dysfunction frequentlymitochondria dysfunction frequently are the are the common denominator.common denominator.
The effort of mitigating brain injury include:The effort of mitigating brain injury include:Maintenance of brain perfusion.Maintenance of brain perfusion.Maintenance to adequate oxygen delivery.Maintenance to adequate oxygen delivery.Optimizing source of brain energy.Optimizing source of brain energy.Neuroprotective strategyNeuroprotective strategy

ConclusionsConclusions
Neuroprotective Strategies:Neuroprotective Strategies:Non Pharmalogical (Hypothermia).Non Pharmalogical (Hypothermia).Pharmacological Neuroprotetion.Pharmacological Neuroprotetion.
CDP-Choline is one ofCDP-Choline is one of PharmacPharmacoological Neuroprotection canlogical Neuroprotection can used in the treatment of TBIused in the treatment of TBI

Outcome and Mortality depend Outcome and Mortality depend on :on :
Primary Cerebral damagesPrimary Cerebral damagesOptimal initial careOptimal initial careNeurosurgery consultation procedureNeurosurgery consultation procedure Immediate and percise surgery Immediate and percise surgery Post-operative ICUPost-operative ICUMedical rehabilitationMedical rehabilitation

