transplantation definition: to transfer (an organ or tissue) from one part or individual to another...
TRANSCRIPT
IMMUNOLOGY
Bios 328a textbook-based study of immunologySpring 2003
http://www.lehigh.edu/~sk08/Courses/Bios328/mainpage.htm

Transplantation• Definition: to transfer (an organ or
tissue) from one part or individual to another (Merriam-Webster)
• May take place between different parts of the same organism (autografting), different organisms of the same species (allografting), or even different species (xenografting)

The Basics• Tissue from another source is grafted into a
host
• The host either recognizes the graft as self and accepts it, or recognizes it non-self and an immune response develops
• The immune response destroys the graft and local vascular tissue (rejection)
http://www.novartis-transplant.com/medpro/ symposia/immunology_of_TX.html
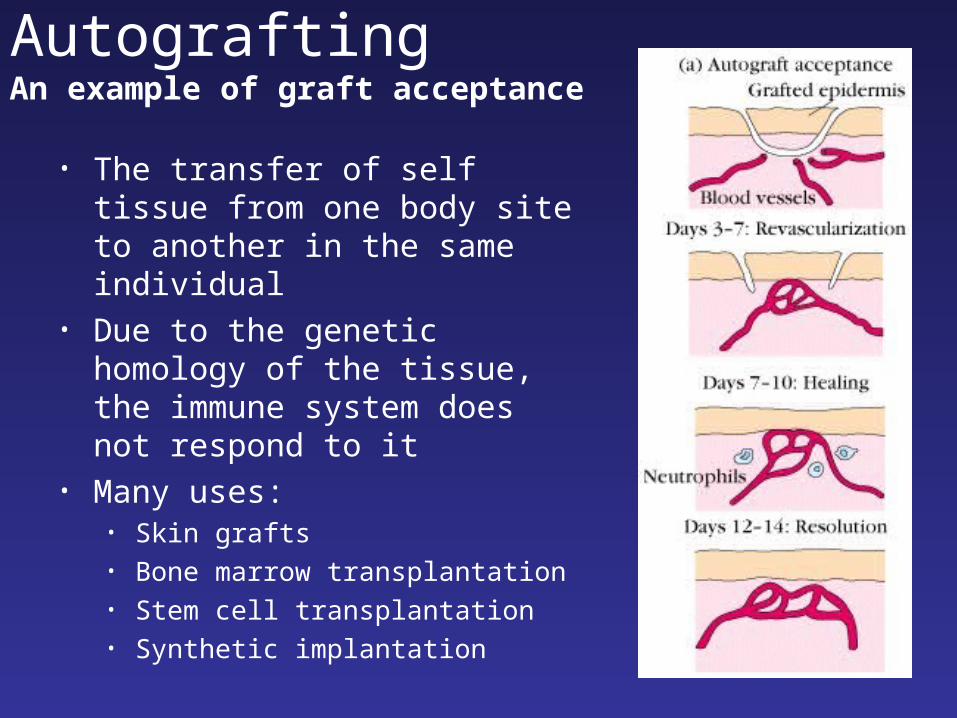
AutograftingAn example of graft acceptance
• The transfer of self tissue from one body site to another in the same individual
• Due to the genetic homology of the tissue, the immune system does not respond to it
• Many uses:• Skin grafts• Bone marrow transplantation• Stem cell transplantation• Synthetic implantation

RejectionWhen the immune system of the host detects
foreign graft tissue, it launches an attack, resulting in tissue rejection
Two Stages• Sensitization Stage• Effector Stage
Three Clinical Manifestations (more on this later)• Hyperacute• Acute• Chronic

Stage 1 – Sensitization Stage• Antigen recognition by T-cells triggers
lymphocyte proliferation
• ‘Antigen’ – portions of the graft’s HLA complex (MHC) are processed and presented
• Minor histocompatibility complexes also play a role – they don’t need to match exactly, but multiple mismatches can trigger rejection
• Important: major HCs can be recognized directly by T-cells, minor HCs must be processed and presented by APCs

Stage 2 – Effector Stage
The host immune system attacks the graft, destroying it with four methods (first two most important):
• CTL-mediated cytotoxicity
• Delayed-type hypersensitivity
• Antibody-dependent cell-mediated cytotoxicity
• Complement-mediated lysis

Clinical Transplantation
• Many human diseases and disorders are caused by defects in organs and tissue
• Transplanted organs can replace organs that are defective or damaged by disease.
• Improved surgical technique has made many different types of tissue grafting possible

Clinical Transplantation

Milestones in Transplantation• 1682(!) – bone from a dog is used to repair a human skull• 1881 – earliest skin grafts (some using frog skin)• 1930 – Karl Landsteiner awarded Nobel Prize for discovery
of ABO blood groups• 1945 – P.B. Medawar publishes a paper linking graft
rejection and the immune system• 1954 – first successful kidney transplant between identical
twins• 1967 - first successful heart transplant• 1990 – first living-donor lung transplant• 1992 – a patient receives a baboon liver and survives for
two months• 1995 – An AIDS patient receives a bone marrow transplant
from a chimpanzee• 2002 – first liver transplant (between identical twins)
performed without immunosuppresion

Hyperacute rejection• Takes place within 24 hours of transplantation• Serum antibodies react to foreign MHC, triggering
the complement system• The inrush of neutrophils and the inflammation
causes clot formation in the blood vessels• The graft dies without being vascularized
But where do those serum antibodies come from?

Acute rejectionA two-stage process
• A good old fashioned immune response
• Within two weeks of transplantation, macrophages and lymphocytes swarm the tissue, triggering cytotoxicity, complement activation, and graft cell lysis
• The two week delay is indicative of the TH activation time

Chronic Rejection• Even if a graft escapes an immediate
rejection responses, it can undergo rejection years later
• Tissue typing and immunosuppressive drugs decrease the likelihood of chronic rejection, but they have a long way to go
• If the rejection cannot be managed, another transplant may be necessary
• Of course, due to the memory and specificity of the immune system, subsequent rejections occur even more quickly and vigorously

Zones of Immunological Privilege
• Transplants into zones of immunological privilege have proven highly successful
• For example, since there are few blood vessels in the cornea, there is a very low rate (about 20%) of corneal graft rejection
• There has even been some success transplanting fetal pig neural tissue into the brains of Parkinson’s disease patients
Graft-versus-host disease
• Lymphocytes from the donor are carried by the organ into the body of the graft recipient
• If the recipient is immunocompromised, the foreign lymphocytes can attack his tissue, resulting in skin rashes, intestinal problems, organ failure, and death
• Liver, spleen, and bone marrow transplants all carry the risk of GVHD

Barriers to Medical TransplantDifficulties posed by the immune system• The necessity of MHC matching makes it
harder to find compatible organs• Repeat graft recipients reject new organs
faster and more vigorously with each new transplant
Shortage of available organs• Many transplantable organs can only be taken
from cadavers• Organs must also be matched for size and
condition
Solutions?

Immunosuppressive TherapyNon-specific
• Drugs that interfere with the immune response
• This attenuates the rejection of donor tissue
• Decreased immune responsiveness increases susceptibility to pathogens and cancers
• Current therapies involve using multiple drugs in low doses: the goal of this is to minimize side effects while still preventing rejection
• Many immunosuppressives are derived from fungi…why? Cyclosporin A

Immunosuppressive TherapySpecific
• Treatments that produce an immunodeficiency specific to the donor alloantigens – an artificial hole in the repertoire
• Monoclonal antibodies can block T-cell activation and binding, extending the life of transplanted organs
• Soluble fusion proteins can be made with block costimulatory signals necessary for T-cell activation

XenotransplantationXenotransplantation – the transfer of tissue
from one species to another
• Usually refers to the implantation of animal tissue in humans
• Many different types of tissue may be transplanted
• Using animals for organs would provide a vast new source of organs for humans

Clinical Aspects• Attempts at kidney, heart, liver, and bone marrow
transplants from primates into humans have met with little success
• The earliest xenotransplantation of a chimpanzee kidney into a human took place in 1964
• In 1993, T.E. Starzl performed two liver transplants from baboons into patients suffering from liver failure (both died within 70 days)
• Pigs have also been considered as a source of organs, especially kidneys

Problems with Xenotransplantation• Even with immunosuppression, the
foreignness of animal tissue provokes a vigorous immune response
• Viruses and diseases which have no ill effects in animals have the potential to cause serious illness in humans
• Animal retroviruses may combine with human variants, producing dangerous new pathogens

Solutions?• Animals bred with human
histocompatibility genes (transgenic animals) would have organs immunologically indistinguishable from human organs
• Other transgenic organs might produce proteins that prevent destruction by the complement system

Summary• Graft antigens (in the form of MHC and
bound ligands) are recognized by host lymphocytes (most importantly TH-cells)
• The resulting cell-mediated response destroys the graft tissue, which undergoes necrosis
• In future transplants, serum antibodies may trigger antibody-mediated (hyperacute) rejection – specificity and memory