transorbital approach without craniotomy to orbital … transorbital approach without craniotomy to...
TRANSCRIPT

Orbit, 2014; 33(5): 343–351! Informa Healthcare USA, Inc.
ISSN: 0167-6830 print / 1744-5108 online
DOI: 10.3109/01676830.2014.904374
ORIGINAL ARTICLE
Transorbital Approach Without Craniotomy toOrbital Tumors with Extradural Intracranial Extension
Helen Lew1, Daniel B. Rootman2, Nariman Nassiri2, Alice Goh2, andRobert A. Goldberg2
1Department of Ophthalmology, CHA Bundang Medical Center, CHA University, Bundang-gu, Seongnam,South Korea and 2Division of Orbital and Ophthalmic Plastic Surgery, Jules Stein Eye Institute,
David Geffen School of Medicine, University of California at Los Angeles, Los Angeles, California, USA
ABSTRACT
Purpose: To review indications and clinical outcomes in a series of orbitocranial tumors treated surgicallythrough a transorbital extradural approach without craniotomy.
Methods: In this retrospective case series, all patients who underwent surgery through a transorbital extraduralapproach without craniotomy for benign orbitocranial tumors involving the dura or extending into the anterioror middle cranial fossae were analyzed.
Results: Twenty-seven patients (20 females and 7 males) were included. Median age was 47.0 years (range: 6–74years) and median follow-up time was 43.5 months (range: 3–148 months). The median preoperativebest-corrected visual acuity (logMAR) was improved from 0.35 (range: 0–2.6) to 0.1 (range: 0–2.6) at the lastfollow-up (p50.03). The mean ± SD preoperative exophthalmos significantly decreased from 20.4 ± 3.4 mm to13.1 ± 3.5 mm at the last follow-up visit (p50.01). Four postoperative complications were noted and includedone case each of ptosis, numbness, diplopia (transient for 6 months), and cranial nerve VI palsy (transient for4 months).
Conclusions: The transorbital extradural approach provides access to the deep orbit and adjacent extraduralcranial spaces. Benign orbital tumors that have eroded through the orbital roof, are located in the orbital apexabutting the anterior cavernous sinus and tumors requiring debulking are all processes that can be potentiallyapproached through the transorbital extradural route. Compared to open craniotomy, the incision is smaller,the access more direct and specific risks of open craniotomy are reduced.
Keywords: Craniotomy, deep orbital approach, orbitocranial tumors, transorbital extradural approach,transcranial approach
INTRODUCTION
The orbit is a complex space within the skull basethat abuts both the anterior and middle cranial fossae.The bone separating these spaces can be extremelythin, and often orbital disease processes erodethrough these bony barriers to create a continuitybetween the orbit and the intracranial space.
Tumors spanning the orbit and the cranial vaultcan be approached both from above via craniotomy,or below transorbitally. A transcranial orbitotomy
provides a wide surgical field, and allows for directvisualization and protection of the dura. Thisapproach allows for excellent visualization of thespace above the optic nerve, including the lesserwing and anterior clinoid.1 However, transcranialapproaches to the orbit are often lengthy proceduresthat have significant risk of morbidity related to thecraniotomy, intracranial retraction and violation ofthe cranial space.2–6
Alternatively, transorbital strategies provide anadequate operative field extending to the orbital
Correspondence: Dr. Robert A. Goldberg, Jules Stein Eye Institute, 100 Stein Plaza, Los Angeles CA 90095, Tel: (310) 206-8250, Fax: (310)825-9263, E-mail: [email protected]
Received 24 August 2013; Revised 28 February 2014; Accepted 10 March 2014; Published online 4 September 2014
343
Orb
it D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y K
orea
Uni
vers
ity o
n 03
/22/
15Fo
r pe
rson
al u
se o
nly.
apex and skull base without an open craniotomy.7
With this approach the extradural anterior cranialfossa, middle cranial fossa, and anterior cavernoussinus can be accessed. In this study, we report theindications and clinical outcomes for the resection oforbitocranial lesions using a transorbital extraduralapproach without craniotomy.
METHODS
In this retrospective case series, medical records of allpatients with orbitocranial lesions managed at theJules Stein Eye Institute between January 1st, 1993,and July 30th, 2013, were reviewed. The InstitutionalReview Board at the University of California-LosAngeles approved the study protocol, and the tenetsof the Declaration of Helsinki were upheld.
The transorbital extradural approach was con-sidered for benign, well-encapsulated tumors withrelatively small areas of dural exposure. Thisapproach was not considered for invasive tumorswith extensive bony involvement, fibrous dysplasiaextending intradurally, apical tumors superior tothe optic nerve and optic nerve tumors requiringintracranial transection.
All surgeries were performed under general anes-thesia in an outpatient setting as described previ-ously.7 In brief, the lateral orbit is accessed througha modified lid crease incision. A subperiosteal planeis created extending from Whitnall’s tubercle to themid orbit along the rim and posteriorly to the inferiorand superior orbital fissures. The temporalis muscleis minimally distracted off of the lateral orbital rimand a lateral marginotomy is created. A high-speedcutting burr is used to remove the bone of the greaterwing of the sphenoid and the diploe of the trigone.
Under microscope guidance, the remaining boneof the outer table surrounding the lesion of interestis removed with a diamond burr, as this instrumentis less likely to tear the dura. The lesion can thenbe accessed for removal with microsurgical instru-mentation. Following resection, the marginotomy isreplaced utilizing suture fixation and the periostealincision at the arcus marginalis is closed by approx-imating the adjacent soft tissues. Intraoperative imageguidance is not utilized. Cerebrospinal fluid leakswere managed with surgical cellulose packingfollowed by placing small fat grafts as required.8,9
RESULTS
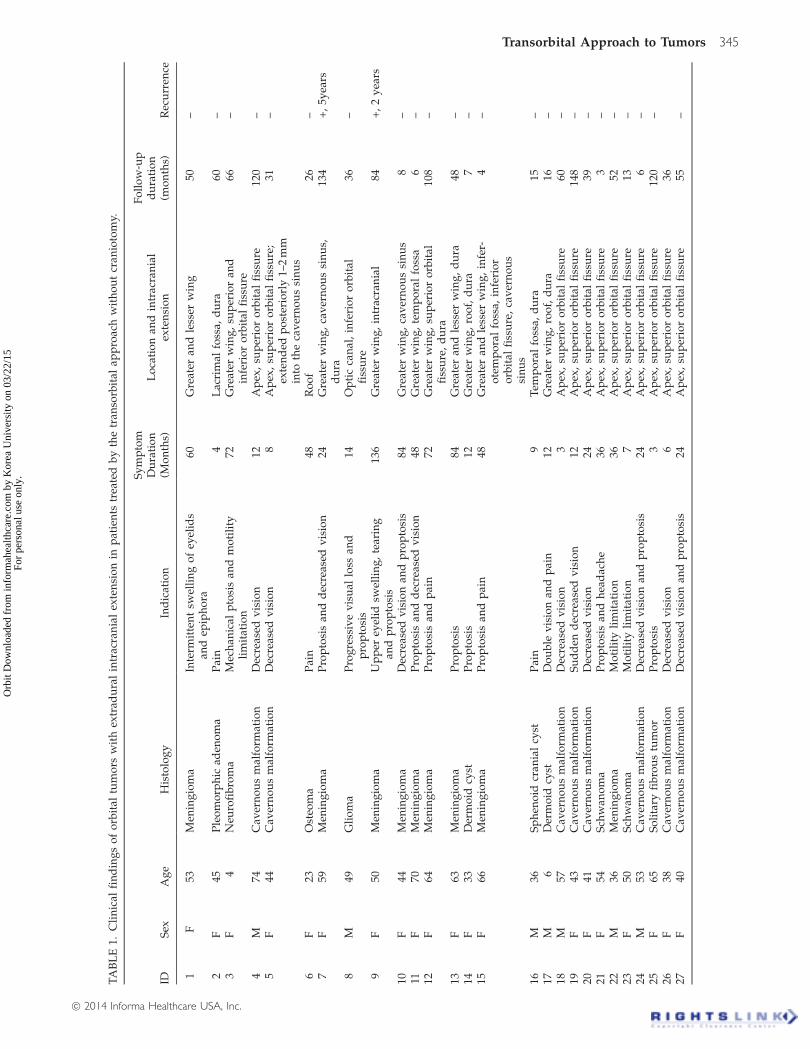
Twenty-seven consecutive patients (20 females and7 males) with orbital tumors extending to the anterioror middle cranial fossa were included in the sample(Table 1). Median patient age was 47.0 years (range:6–74 years). The median time from symptom onset to
surgery was 24 months (range: 3–136 months). Themedian follow-up was 43.5 months (range: 3–148months).
The median preoperative best-corrected visualacuity (BCVA; logMAR) was 0.35 (range: 0–2.6). Thisimproved to 0.1 (range: 0–2.6) at the last follow-upvisit (p50.03). The mean ± standard deviation pre-operative exophthalmos was 20.4 ± 3.4 mm. Thisimproved to 13.1 ± 3.5 mm at the last follow-up visit(p50.01). Preoperatively, a relative afferent pupillarydefect (RAPD) was noted in 13 (48.1%) patients. TheRAPD improved after surgery in eight eyes andremained unchanged in the rest.
Nineteen patients (70.4%) had normal eye move-ment before and after surgery. Six patients hadstrabismus before surgery. In four cases strabis-mus surgery was eventually required after tumorexcision, and in two cases the diplopia resolvedwithin 6 months of surgery. Postoperatively, twopatients experienced new onset diplopia due tocranial nerve VI palsy. In each case this was self-limited and resolved in 6 and 4 months, respectively.Other postoperative complications included numb-ness in one case and ptosis in one other.
Only two tumors recurred during the study period,and both were meningioma (after 2 and 5 years).They were both subsequently treated with surgicaldebulking and radiation.
CASE PRESENTATIONS
Patient 1
A 53-year-old woman presented with complaints ofdecreased vision, exophthalmos and swelling of lefteye for 4 years related to a known sphenoidmeningioma. On examination, BCVA in the affectedeye was 20/40, with decreased color vision (9/12plates) and a 2+ RAPD. There was 3 mm of relativeproptosis of the left eye, which was moderately firmto retropulsion. Motility was full. On funduscopy, theleft optic nerve was diffusely pale. Visual fieldtesting demonstrated spotty scotoma of the left eye.Magnetic resonance imaging (MRI) of the orbitsrevealed thickening and enhancement of the menin-ges with tumor extension through the superiororbital fissure (Figure 1). There was hyperostosis ofthe sphenoid bone.
With a goal of debulking the tumor to improveproptosis and congestion, deep transorbital surgerywas performed. The thickened bone of the greaterwing was removed with diamond and cutting burrsfollowing the dura to the superior orbital fissure.Abnormal bone was also removed between themiddle cranial fossa and the annulus of Zinn.A small leak was noted in the middle cranial fossadura. This was controlled with surgical cellulose and
344 H. Lew et al.
Orbit
Orb
it D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y K
orea
Uni
vers
ity o
n 03
/22/
15Fo
r pe
rson
al u
se o
nly.
TA
BL
E1.
Cli
nic
alfi
nd
ing
so
fo
rbit
altu
mo
rsw
ith
extr
adu
ral
intr
acra
nia
lex
ten
sio
nin
pat
ien
tstr
eate
db
yth
etr
anso
rbit
alap
pro
ach
wit
ho
ut
cran
ioto
my.
IDS
exA
ge
His
tolo
gy
Ind
icat
ion
Sy
mp
tom
Du
rati
on
(Mo
nth
s)L
oca
tio
nan
din
trac
ran
ial
exte
nsi
on
Fo
llo
w-u
pd
ura
tio
n(m
on
ths)
Rec
urr
ence
1F
53M
enin
gio
ma
Inte
rmit
ten
tsw
elli
ng
of
eyel
ids
and
epip
ho
ra60
Gre
ater
and
less
erw
ing
50–
2F
45P
leo
mo
rph
icad
eno
ma
Pai
n4
Lac
rim
alfo
ssa,
du
ra60
–3
F4
Neu
rofi
bro
ma
Mec
han
ical
pto
sis
and
mo
tili
tyli
mit
atio
n72
Gre
ater
win
g,
sup
erio
ran
din
feri
or
orb
ital
fiss
ure
66–
4M
74C
aver
no
us
mal
form
atio
nD
ecre
ased
vis
ion
12A
pex
,su
per
ior
orb
ital
fiss
ure
120
–5
F44
Cav
ern
ou
sm
alfo
rmat
ion
Dec
reas
edv
isio
n8
Ap
ex,
sup
erio
ro
rbit
alfi
ssu
re;
exte
nd
edp
ost
erio
rly
1–2
mm
into
the
cav
ern
ou
ssi
nu
s
31–
6F
23O
steo
ma
Pai
n48
Ro
of
26–
7F
59M
enin
gio
ma
Pro
pto
sis
and
dec
reas
edv
isio
n24
Gre
ater
win
g,
cav
ern
ou
ssi
nu
s,d
ura
134
+,
5yea
rs
8M
49G
lio
ma
Pro
gre
ssiv
ev
isu
allo
ssan
dp
rop
tosi
s14
Op
tic
can
al,
infe
rio
ro
rbit
alfi
ssu
re36
–
9F
50M
enin
gio
ma
Up
per
eyel
idsw
elli
ng
,te
arin
gan
dp
rop
tosi
s13
6G
reat
erw
ing
,in
trac
ran
ial
84+
,2
yea
rs
10F
44M
enin
gio
ma
Dec
reas
edv
isio
nan
dp
rop
tosi
s84
Gre
ater
win
g,
cav
ern
ou
ssi
nu
s8
–11
F70
Men
ing
iom
aP
rop
tosi
san
dd
ecre
ased
vis
ion
48G
reat
erw
ing
,te
mp
ora
lfo
ssa
6–
12F
64M
enin
gio
ma
Pro
pto
sis
and
pai
n72
Gre
ater
win
g,
sup
erio
ro
rbit
alfi
ssu
re,
du
ra10
8–
13F
63M
enin
gio
ma
Pro
pto
sis
84G
reat
eran
dle
sser
win
g,
du
ra48
–14
F33
Der
mo
idcy
stP
rop
tosi
s12
Gre
ater
win
g,
roo
f,d
ura
7–
15F
66M
enin
gio
ma
Pro
pto
sis
and
pai
n48
Gre
ater
and
less
erw
ing
,in
fer-
ote
mp
ora
lfo
ssa,
infe
rio
ro
rbit
alfi
ssu
re,
cav
ern
ou
ssi
nu
s
4–
16M
36S
ph
eno
idcr
ania
lcy
stP
ain
9T
emp
ora
lfo
ssa,
du
ra15
–17
M6
Der
mo
idcy
stD
ou
ble
vis
ion
and
pai
n12
Gre
ater
win
g,
roo
f,d
ura
16–
18M
57C
aver
no
us
mal
form
atio
nD
ecre
ased
vis
ion
3A
pex
,su
per
ior
orb
ital
fiss
ure
60–
19F
43C
aver
no
us
mal
form
atio
nS
ud
den
dec
reas
edv
isio
n12
Ap
ex,
sup
erio
ro
rbit
alfi
ssu
re14
8–
20F
41C
aver
no
us
mal
form
atio
nD
ecre
ased
vis
ion
24A
pex
,su
per
ior
orb
ital
fiss
ure
39–
21F
54S
chw
ano
ma
Pro
pto
sis
and
hea
dac
he
36A
pex
,su
per
ior
orb
ital
fiss
ure
3–
22M
36M
enin
gio
ma
Mo
tili
tyli
mit
atio
n36
Ap
ex,
sup
erio
ro
rbit
alfi
ssu
re52
–23
F50
Sch
wan
om
aM
oti
lity
lim
itat
ion
7A
pex
,su
per
ior
orb
ital
fiss
ure
13–
24M
53C
aver
no
us
mal
form
atio
nD
ecre
ased
vis
ion
and
pro
pto
sis
24A
pex
,su
per
ior
orb
ital
fiss
ure
6–
25F
65S
oli
tary
fib
rou
stu
mo
rP
rop
tosi
s3
Ap
ex,
sup
erio
ro
rbit
alfi
ssu
re12
0–
26F
38C
aver
no
us
mal
form
atio
nD
ecre
ased
vis
ion
6A
pex
,su
per
ior
orb
ital
fiss
ure
3627
F40
Cav
ern
ou
sm
alfo
rmat
ion
Dec
reas
edv
isio
nan
dp
rop
tosi
s24
Ap
ex,
sup
erio
ro
rbit
alfi
ssu
re55
–
Transorbital Approach to Tumors 345
! 2014 Informa Healthcare USA, Inc.
Orb
it D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y K
orea
Uni
vers
ity o
n 03
/22/
15Fo
r pe
rson
al u
se o
nly.

then covered with a 3� 4 mm fibro-fatty graft fromthe orbit.
The periorbita was then opened, and tumor wasexcised to the apex adjacent to the annulus of Zinn.Orbital fat was allowed to prolapse into the newspace. This provided further tamponade of the duralexposure and no CSF leak was noted at the end of thecase. At the conclusion of surgery, the orbit was softwith substantial improvement in proptosis andcongestion.
Histologic analysis of the excised mass confirmed adiagnosis of meningioma. The patient’s postoperativecourse was characterized by improvement in visualfield and a reduction in the amplitude of preoperativeRAPD. Transient mild ptosis persisted for 6 months.
One year postoperatively, BCVA was 20/20, with noAPD or ptosis and full motility. There was a smallamount of residual proptosis (2 mm).
Patient 2
A 45-year-old woman presented with painless eyelidswelling and proptosis on the left for 4 months.Imaging performed elsewhere revealed a lacrimalgland mass. Biopsy was performed and pathologicalanalysis suggested a diagnosis of pleomorphic aden-oma. Initial examination revealed BCVA in theaffected eye of 20/20, with full motility. There was1 mm of slightly firm proptosis on the left. The left
FIGURE 1. Preoperative contrast-enhanced transverse fat-suppressed, coronal T1-weighted MR images showing left spheno-orbitalmeningioma (A & B). Postoperative contrast-enhanced MR images demonstrating debulking of the tumor with bony removal over themiddle cranial fossa dura (C & D).
346 H. Lew et al.
Orbit
Orb
it D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y K
orea
Uni
vers
ity o
n 03
/22/
15Fo
r pe
rson
al u
se o
nly.
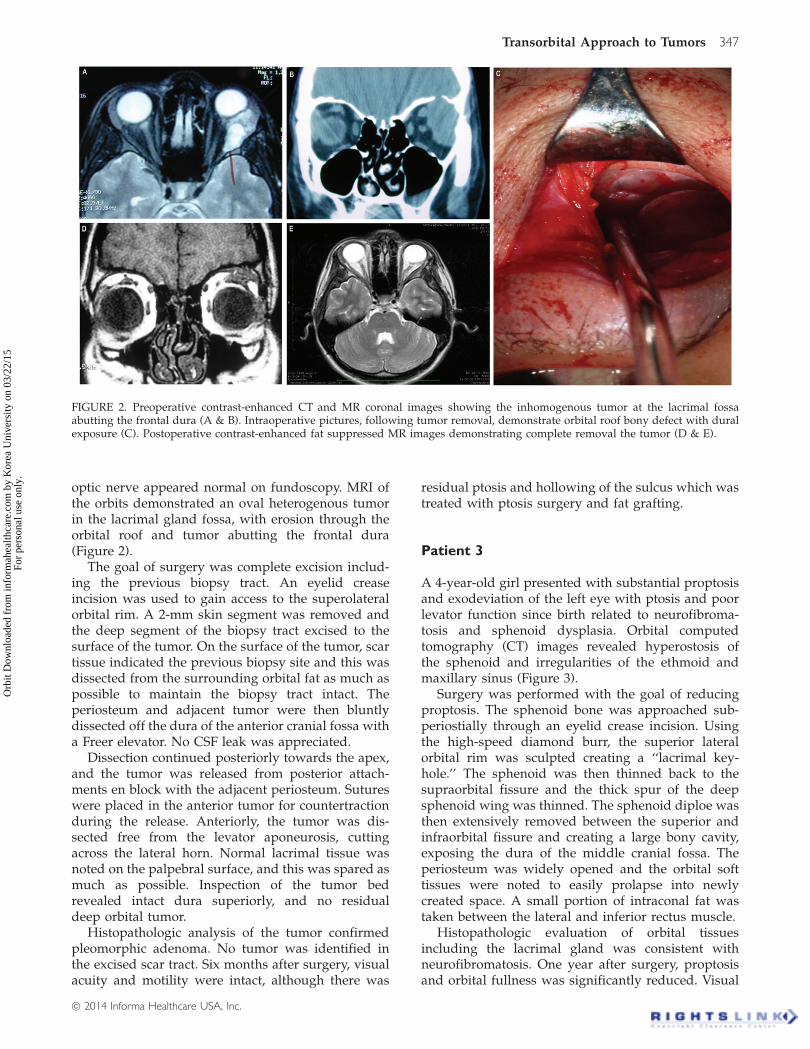
optic nerve appeared normal on fundoscopy. MRI ofthe orbits demonstrated an oval heterogenous tumorin the lacrimal gland fossa, with erosion through theorbital roof and tumor abutting the frontal dura(Figure 2).
The goal of surgery was complete excision includ-ing the previous biopsy tract. An eyelid creaseincision was used to gain access to the superolateralorbital rim. A 2-mm skin segment was removed andthe deep segment of the biopsy tract excised to thesurface of the tumor. On the surface of the tumor, scartissue indicated the previous biopsy site and this wasdissected from the surrounding orbital fat as much aspossible to maintain the biopsy tract intact. Theperiosteum and adjacent tumor were then bluntlydissected off the dura of the anterior cranial fossa witha Freer elevator. No CSF leak was appreciated.
Dissection continued posteriorly towards the apex,and the tumor was released from posterior attach-ments en block with the adjacent periosteum. Sutureswere placed in the anterior tumor for countertractionduring the release. Anteriorly, the tumor was dis-sected free from the levator aponeurosis, cuttingacross the lateral horn. Normal lacrimal tissue wasnoted on the palpebral surface, and this was spared asmuch as possible. Inspection of the tumor bedrevealed intact dura superiorly, and no residualdeep orbital tumor.
Histopathologic analysis of the tumor confirmedpleomorphic adenoma. No tumor was identified inthe excised scar tract. Six months after surgery, visualacuity and motility were intact, although there was
residual ptosis and hollowing of the sulcus which wastreated with ptosis surgery and fat grafting.
Patient 3
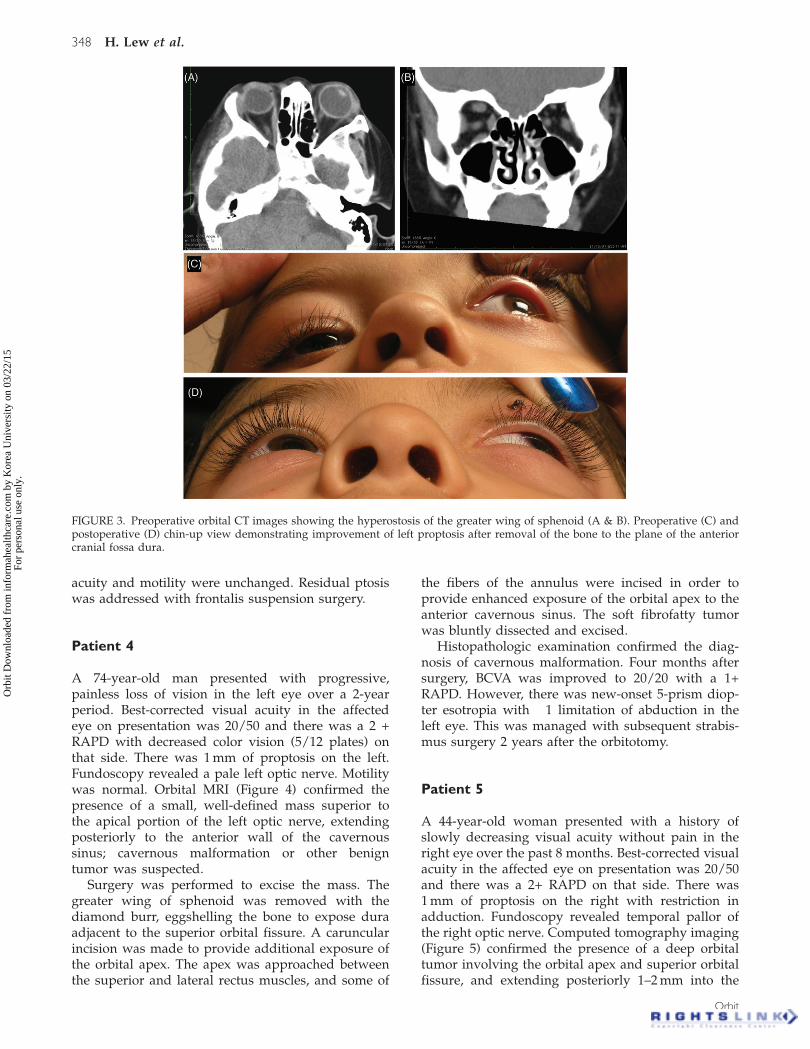
A 4-year-old girl presented with substantial proptosisand exodeviation of the left eye with ptosis and poorlevator function since birth related to neurofibroma-tosis and sphenoid dysplasia. Orbital computedtomography (CT) images revealed hyperostosis ofthe sphenoid and irregularities of the ethmoid andmaxillary sinus (Figure 3).
Surgery was performed with the goal of reducingproptosis. The sphenoid bone was approached sub-periostially through an eyelid crease incision. Usingthe high-speed diamond burr, the superior lateralorbital rim was sculpted creating a ‘‘lacrimal key-hole.’’ The sphenoid was then thinned back to thesupraorbital fissure and the thick spur of the deepsphenoid wing was thinned. The sphenoid diploe wasthen extensively removed between the superior andinfraorbital fissure and creating a large bony cavity,exposing the dura of the middle cranial fossa. Theperiosteum was widely opened and the orbital softtissues were noted to easily prolapse into newlycreated space. A small portion of intraconal fat wastaken between the lateral and inferior rectus muscle.
Histopathologic evaluation of orbital tissuesincluding the lacrimal gland was consistent withneurofibromatosis. One year after surgery, proptosisand orbital fullness was significantly reduced. Visual
FIGURE 2. Preoperative contrast-enhanced CT and MR coronal images showing the inhomogenous tumor at the lacrimal fossaabutting the frontal dura (A & B). Intraoperative pictures, following tumor removal, demonstrate orbital roof bony defect with duralexposure (C). Postoperative contrast-enhanced fat suppressed MR images demonstrating complete removal the tumor (D & E).
Transorbital Approach to Tumors 347
! 2014 Informa Healthcare USA, Inc.
Orb
it D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y K
orea
Uni
vers
ity o
n 03
/22/
15Fo
r pe
rson
al u
se o
nly.
acuity and motility were unchanged. Residual ptosiswas addressed with frontalis suspension surgery.
Patient 4
A 74-year-old man presented with progressive,painless loss of vision in the left eye over a 2-yearperiod. Best-corrected visual acuity in the affectedeye on presentation was 20/50 and there was a 2 +RAPD with decreased color vision (5/12 plates) onthat side. There was 1 mm of proptosis on the left.Fundoscopy revealed a pale left optic nerve. Motilitywas normal. Orbital MRI (Figure 4) confirmed thepresence of a small, well-defined mass superior tothe apical portion of the left optic nerve, extendingposteriorly to the anterior wall of the cavernoussinus; cavernous malformation or other benigntumor was suspected.
Surgery was performed to excise the mass. Thegreater wing of sphenoid was removed with thediamond burr, eggshelling the bone to expose duraadjacent to the superior orbital fissure. A caruncularincision was made to provide additional exposure ofthe orbital apex. The apex was approached betweenthe superior and lateral rectus muscles, and some of
the fibers of the annulus were incised in order toprovide enhanced exposure of the orbital apex to theanterior cavernous sinus. The soft fibrofatty tumorwas bluntly dissected and excised.
Histopathologic examination confirmed the diag-nosis of cavernous malformation. Four months aftersurgery, BCVA was improved to 20/20 with a 1+RAPD. However, there was new-onset 5-prism diop-ter esotropia with �1 limitation of abduction in theleft eye. This was managed with subsequent strabis-mus surgery 2 years after the orbitotomy.
Patient 5
A 44-year-old woman presented with a history ofslowly decreasing visual acuity without pain in theright eye over the past 8 months. Best-corrected visualacuity in the affected eye on presentation was 20/50and there was a 2+ RAPD on that side. There was1 mm of proptosis on the right with restriction inadduction. Fundoscopy revealed temporal pallor ofthe right optic nerve. Computed tomography imaging(Figure 5) confirmed the presence of a deep orbitaltumor involving the orbital apex and superior orbitalfissure, and extending posteriorly 1–2 mm into the
FIGURE 3. Preoperative orbital CT images showing the hyperostosis of the greater wing of sphenoid (A & B). Preoperative (C) andpostoperative (D) chin-up view demonstrating improvement of left proptosis after removal of the bone to the plane of the anteriorcranial fossa dura.
348 H. Lew et al.
Orbit
Orb
it D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y K
orea
Uni
vers
ity o
n 03
/22/
15Fo
r pe
rson
al u
se o
nly.

FIGURE 4. Preoperative contrast-enhanced transverse fat-suppressed MR images showing a contrast-enhancing deep apical tumorabutting the anterior cavernous sinus (A&B). Postoperative contrast-enhanced MR images following removal of the tumor (C&D).
FIGURE 5. Computed tomography imaging showing a deep orbital tumor involving the orbital apex and superior orbital fissure,extending posteriorly 1–2 mm into the cavernous sinus (A&B). Postoperative CT images following removal of the tumor (C&D).
Transorbital Approach to Tumors 349
! 2014 Informa Healthcare USA, Inc.
Orb
it D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y K
orea
Uni
vers
ity o
n 03
/22/
15Fo
r pe
rson
al u
se o
nly.

cavernous sinus. Cavernous malformation or otherbenign tumor was suspected.
Surgery was performed with the goal of reducingcompression of the optic nerve and orbital apex.An eyelid crease incision provided access to the lateralorbital rim and temporalis fossa. The periosteum wasreflected in both directions and a marginotomy wasfashioned extending from the mid orbit superiorly tothe take off of the zygomatic arch inferiorly. A high-speed diamond burr was used to remove the trigoneof the sphenoid bone. The dura of the middle cranialfossa was exposed surrounding the superior orbitalfissure. The operating microscope was broughtinto place and microsurgical instruments were usedto reflect the lateral rectus and carefully dissect thethird cranial nerve off of the tumor. The tumorwas delivered. The third cranial nerve was slightlydamaged in the process and repaired with 10–0 nylon.The marginotomy was re-approximated with wireand the skin was closed.
Histopathologic examination confirmed the diag-nosis of cavernous malformation. One year aftersurgery, BCVA had improved to 20/20 with a 1+RAPD. No residual proptosis or enophthalmos wasnoted.
DISCUSSION
A variety of surgical approaches have been describedto excise or biopsy tumors that involve the orbit aswell as the adjacent cranial cavity.10–18 The anatomy iscomplex, and each case presents a unique combin-ation of tumor location and anticipated pathology.Therefore, surgical treatment decisions are ideallyindividualized, and the experience and philosophy ofthe surgical team at individual centers will appropri-ately influence the decision making.
One of the central decisions in surgical planning isthe need for open craniotomy. An open craniotomy,whether transfrontal, pterional or suprabrow, pro-vides a wide view of the dura and extra-orbitalcompartment in the frontal and/or middle cranialfossa. There are a number of circumstances whenthis approach is preferred. For instance in caseswhere substantial dural involvement is documentedor suspected, the transcranial approach providesoptimal exposure. Additionally, processes involvingthe superior medial orbit, particularly superior to theoptic nerve, are difficult to visualize from an orbitalapproach and more easily exposed transcranially.Large orbitocranial tumors, particularly those thatmay be associated with a substantial bony defect ofthe roof following removal, are also appropriatelyapproached via craniotomy.
In experienced centers, the complication rate ofextradural craniotomy is low. However, an opencraniotomy remains a substantially invasive
procedure requiring an inpatient stay. Some of themajor complications including hemorrhage, meningi-tis, inadvertent nerve damage and CSF leak are sharedby the transcranial and orbital approaches.17–20
Others such as frontal branch facial nerve palsy,coronal hair loss and cutaneous scarring are specific totranscranial orbitotomy.
In appropriate cases the transorbital extraduralapproach can minimize some of these complications.It is a less invasive procedure compared to opencraniotomy, with smaller soft tissue and bony inci-sions. It can often be performed in an outpatientsetting, minimizing health care resource utilization(however, there should always be a low threshold toobserve the patient overnight if necessary). Althoughthe transorbital approach has certain advantages, itdoes involve many of the same potential intracranialand orbital risks as transcranial surgery. In addition,exposure is generally more limited so that intimateknowledge of the orbitocranial anatomy is aprerequisite.
Decisions as to which approach is more appropri-ate should be individualized. Benign, well encapsu-lated tumors and tumors that have relatively smalldural exposures are good candidates for the transor-bital approach. Larger tumors, tumors extendingsubstantially into the cavernous sinus, or those withinfiltrative features may not be appropriate.
The orbital surgeon approaching these orbitocra-nial tumors should be prepared to treat CSF leaks andto recognize more serious intracranial complicationssuch as intradural hemorrhage.8,9 A close workingrelationship with the neurosurgical team is ideal forcollaborative management of intraoperative or post-operative complications. Additionally, the surgeonshould be prepared to abandon the transorbitalapproach if intraoperative findings reveal a moreinfiltrative or anatomically difficult process thananticipated. Although we did not encounter such asituation in our series, our philosophy is to closethe incision and plan a second stage surgery in theneurosurgical operating room, rather than trying toconvert in the middle of the case.
Our experience with the transorbital extraduralapproach for orbitocranial tumors has been promis-ing. In our series, we did not encounter any vision,central nervous system, or life-threatening complica-tions. Long-term surgical outcome is highly depend-ent on pathology and as our study involved adisparate mix of entities, aggregate surgical outcomedata may be less informative than technique-relatedmeasures.
In summary, the transorbital extradural approachprovides access to the deep orbit and adjacentextradural cranial spaces. This approach is mostappropriate for benign orbital masses that haveeroded through the orbital roof and those found inthe orbital apex abutting or protruding into the
350 H. Lew et al.
Orbit
Orb
it D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y K
orea
Uni
vers
ity o
n 03
/22/
15Fo
r pe
rson
al u
se o
nly.
anterior cavernous sinus. Hyperostotic sphenoidmeningioma or fibrous dysplasia cases can also beadequately debulked via the transorbital extraduralroute. Compared to open craniotomy, the incision issmaller and a prolonged hospital stay is rarelyrequired. In addition, specific risks of the opencraniotomy are reduced. Careful case selection, atten-tion to anatomic details and appropriate collaborativerelationships with the neurosurgical service are allimportant elements for success.
DECLARATION OF INTEREST
The authors did not receive any financial supportfrom any public or private sources. The authors haveno financial or proprietary interest in a product,method, or material described herein. The authorsalone are responsible for the content and writing ofthe paper.
REFERENCES
1. Numa Y and Kawamoto K. Frontozygomatic Approach toIntraorbital Tumors. Skull base 2007;17:303–310.
2. Osguthorpe JD, Saunders RA, Adkins WY. Evaluation ofand access to posterior orbital tumors. Laryngoscope 1983;93:766–771.
3. Pelausa EO, Smith K, Dempsey I. Orbital complications offunctional endoscopic sinus surgery. J Otolaryngol 1995;24:154–159.
4. Remulla HD, Gliklich RE, Metson R, Rubin PA.Delayed orbital infection after endoscopic orbital decom-pression for dysthyroid orbitopathy. Ophthalmology 2000;107:947–950.
5. McCormick CD, Bearden WH, Hunts JH, Anderson RL.Cerebral vasospasm and ischemia after orbital decompres-sion for Graves ophthalmopathy. Ophthal Plast ReconstrSurg 2004;20:347–351.
6. Rose GE, Lund VJ. Clinical features and treatment of lateenophthalmos after orbital decompression. A condition
suggesting cause for idiopathic ‘‘imploding antrum’’(silent sinus) syndrome. Ophthalmology 2003;110:819–826.
7. Goldberg RA, Shorr N, Arnold AC, Garcia GH. Deeptransorbital approach to the apex and cavernous sinus.Ophthal Plast Reconstr Surg 1998;14:336–341.
8. Badilla J, Dolman PJ. Cerebrospinal fluid leaks complicat-ing orbital or oculoplastic surgery. Arch Ophth 2007;125:1631–1634.
9. Limawararut V, Valenzuela AA, Sullivan TJ. Cerebrospinalfluid leaks in orbital and lacrimal surgery. Surv Ophthalmol.2008;53:274–284.
10. Osguthorpe JD, Saunders RA, Adkins WY. Evaluation ofand access to posterior orbital tumors. Laryngoscope 1983;93:766–771.
11. Kennerdell JS, Maroon JC, Celin SE. The posteriorinferior orbitotomy. Ophthal Plast Reconstr Surg 1998;14:277–280.
12. Kingdom TT, Delgaudio JM. Endoscopic approach tolesions of the sphenoid sinus, orbital apex, and clivus.Am J Otolaryngol 2003;24:317–322.
13. Maroon JC, Kennerdell JS. Surgical approaches to theorbit: indications and techniques. J Neurosurg 1984;60:1226–1235.
14. Pelton RW, Patel BC. Superomedial lid crease approach tothe medial intraconal space: a new technique for access tothe optic nerve and central space. Ophthal Plast ReconstrSurg 2001;17:241–253.
15. Rohde V, Schaller K, Hassler W. The combined pterionaland orbitozygomatic approach to extensive tumors of thelateral and latero-basal orbit and orbital apex. ActaNeurochir 1995;132:127–130.
16. Sethi DS, Lau DP. Endoscopic management of orbital apexlesions. Am J Rhinol 1997;11:449–455.
17. Viale GL, Pau A. A plea for postero-lateral orbitotomy formicrosurgical removal of tumors of the orbital apex. ActaNeurochir 1988;90:124–126.
18. Scheuerle AF, Steiner HH, Kolling G, et al. Treatment andlong-term outcome of patients with orbital cavernomas.Am J Ophthalmol 2004; 138:237–244.
19. Hassler W, Eggert HR. External and intradural microsur-gical approaches to lesions of the optic canal and thesuperior orbital fissure. Acta Neurochir 1985;74:87–93.
20. McDermott MW, Durity FA, Rootman J, Woodhurst WB.Combined frontotemporal orbitozygomatic approach fortumors of the sphenoid wing and orbit. Neurosurgery 1990;26:107–116.
Transorbital Approach to Tumors 351
! 2014 Informa Healthcare USA, Inc.
Orb
it D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y K
orea
Uni
vers
ity o
n 03
/22/
15Fo
r pe
rson
al u
se o
nly.