transitioning to competence by design: geriatric medicine ... · 3. broadly describe the cbd...
TRANSCRIPT

Transitioning to Competence by Design: The Geriatric Medicine Journey
Dr. Evelyn Constantin
Assistant Dean, Postgraduate Medical Education, McGill University
CBME Lead, McGill University/RCPSC
Dr. Laura DiachunChair, Nucleus Committee for Geriatric Medicine

Faculty/Presenter Disclosure
• Faculty: Evelyn Constantin
• Relationships with financial sponsors:– Grants/Research Support: none– Speakers Bureau/Honoraria: none– Consulting Fees: none– Patents: none– Other: none

Disclosure of Financial Support• This program has received financial support from CIHR and RCPSC in the
form of operating grants and educational grants.• This program has received in‐kind support from nobody
• Potential for conflict(s) of interest:– none

Mitigating Potential Bias
• Not applicable
Objectives1. discuss the Royal College’s Competence by Design (CBD) program, including the
competence continuum and key components
1. compare the new CBD program to the current training system
2. evaluate the reasoning behind the changes to the new CBD system and the expectations of the transition to CBD
3. broadly describe the CBD implementation process and timelines, including the work and efforts of the CBD leads, the universities, the RCPSC and the specialty committees
4. explain geriatric medicine subspecialty programs’ progress with the planned transition to CBD
1. integrate Entrustable Professional Activities (EPA’s) of geriatric medicine into teaching
1. apply potential evaluation strategies to geriatric competencies.

CBME (COMPETENCY-BASED MEDICAL EDUCATION)
VS
CBD(COMPETENCE BY DESIGN)

Competency-Based Medical Education
7
CBME is “an outcomes-based approach to the design, implementation,
assessmentand evaluation of a medical educationprogram using competencies as the
organizing framework”.
© 2009 Royal College and The International CBME Collaborators Frank et al.,
2010

What is Competence by Design (CBD)?
8
• Multi-year, transformational change initiative to introduce CBME to residency education and continuing professional development;
• Focused on the learning continuum from the start of residency to retirement;
• Based on a competency model of education and assessment; and
• Designed to address societal health need and patient outcomes.

EPAs
Direct Observation
Assessment
Feedback
CBD in the workplace
Transition to CBME
• Launched in July 2018 – OTL and Anesthesia
• Royal College Specialty Committee Creation of new version of specialty specific requirements
• Program structure – learning experiences and program of assessment
• Entrustable Professional Activities (EPAs)
• Direct observation and feedback


Why CBME?
• Competency-based education for 40+ years
• Social contract with society
• Failure to fail – Lack of written documentation and assessment
data– Unfamiliarity with what evidence to document– Limited remediation options
Attributes of CBME
• Focus on outcomes
• Emphasis on abilities
• De-emphasis on time-based training
• Promotion of learner-centrednessFrank et al., 2010

CanMEDS 2015 Physician Competency Framework
Copyright © 2015 The Royal College of Physicians and Surgeons of Canada. Reproduced with permission.
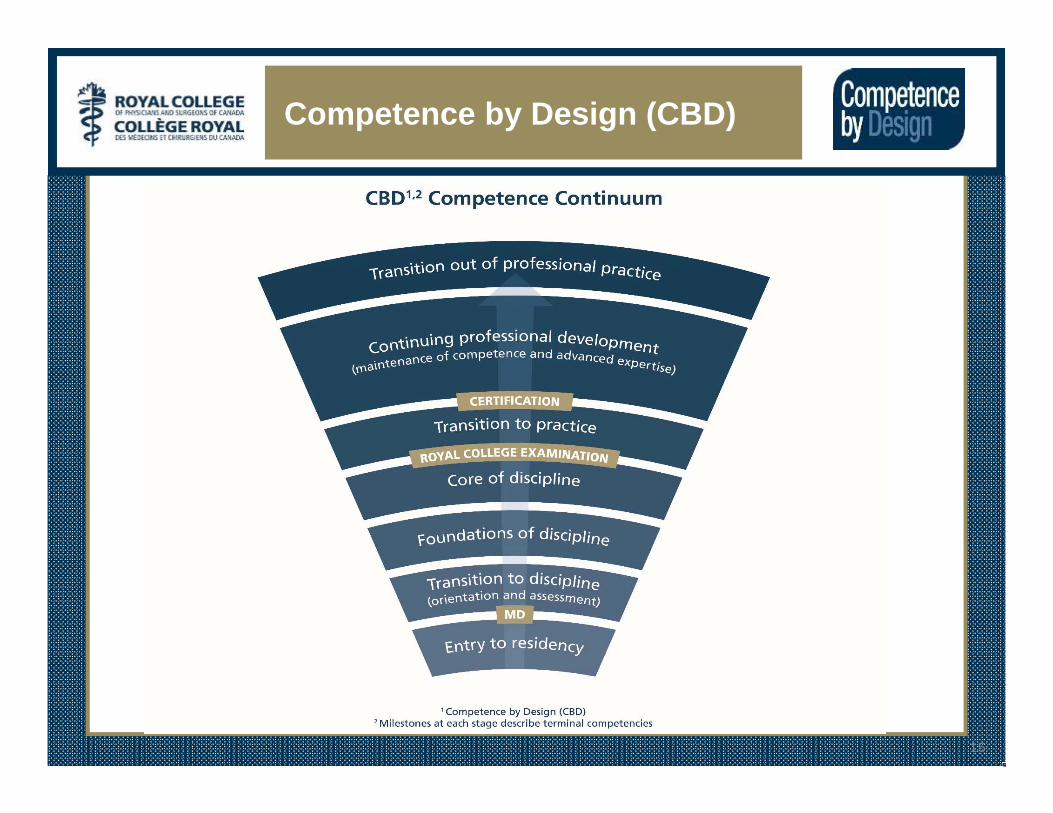
Competence by Design (CBD)
15

CBD Competence Continuum
16
Geriatrics
Core IM
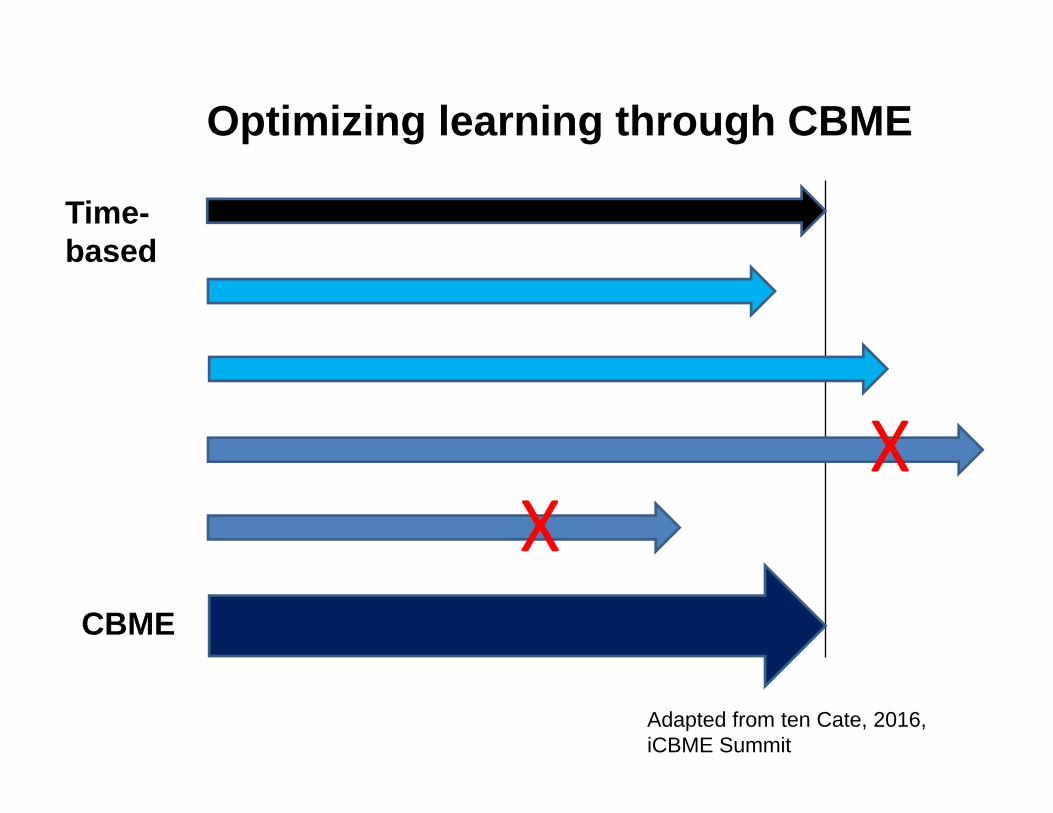
XX
Adapted from ten Cate, 2016, iCBME Summit
Time-based
CBME
Optimizing learning through CBME

Entrustable Professional Activities (EPAs)
Initiating a comprehensive geriatric assessment, identifying common geriatric syndromes, and suggesting a management plan
• Clinical task that a supervisor entrusts a trainee to perform independently, after trainee demonstrates competence in abilities
• EPAs often assessed by direct observation of trainee’s performance

Milestones and EPAs at each stage of progression
Milestone – Nested within an EPA, it represents an observable marker of an individual's ability along a developmental continuum• Used for planning and teaching• Based on CanMEDS Roles
Entrustable Professional Activity (EPA) - An essential task of a "discipline" that an individual can be trusted to perform independently in a given context• Used for assessment• Encompasses multiple milestones
“Entrustment”• Task-specific• Implies that
– a trust decision has been made– the learner would be able to perform the clinical
activity in the future• It’s not a personal judgment regarding “trust”• Helpful in providing constructive, deliberate
feedback around specific tasks
Damodaran et al., 2017

Entrustability
• To what degree autonomy can the trainee do this task?
• No longer (directly) about “how well did you do it?”, but rather “how much guidance did you need?”

Principles of Assessment in CBME
• Based on entrustment of specific clinical tasks
• Frequent use of direct and deliberate observation focused on milestones and competencies
• Multiple low-stakes assessment with documentation
• Day-to-day feedback and coaching to monitor progress
• Individualized learning plans, developed by resident, the PD, faculty coaches/advisors, and the Competence Committee

Program of Assessment• Integration of different methods to gather evidence about residents’ performance
• Based on frequent formative assessments
• Direct and indirect observation with feedback
• No intended redundancy in assessment
• What evidence are we gathering, and how are we gathering it?

Transition from‘now’ to ‘tomorrow’
CURRENT CBDTime-based training (e.g., PGY) Transitional stages and PGY + time
Direct observation / feedback Frequent direct observations with on-the-spot feedback
Objectives of training Rotations / blocksRotation goals and objectivesRequired training experiences
Rotations / blocksRotation goals and objectivesRequired training experiencesIndividualized learning
Rotation-specific ITERs Program of assessment: EPA forms + ITERs
Promotions Committees Competence Committees
Exams Exams
What does this mean for your program?• Revisiting curriculum and learning experiences
• Revisiting assessment methods– ITERs & EPA forms, establish a competence
committee
– Faculty and resident development
• Field testing EPA forms and other assessment forms– Frequent direct observation and feedback

Test Your Awareness – Group Activity
• https://youtu.be/8-hapS2SPz4

What is Direct Observation?
“Observing and giving feedback on clinical skills in the natural practice environment.”
“Assessing learners in natural settings offers the opportunity to see beyond what they know and into what they actually do, which is fundamentally essential to training qualified physicians.”
“…involves meaningful and timely feedback.”Russel 2009, Fromme 2009

The 5 Ws of Direct Observation• What – frequent direct and deliberate observations and
assessments using multiple tools (e.g., Mini-CEX, O-SCORE, narrative assessment)
• Why – to provide meaningful feedback
• Who – supervisors, rotation coordinators, senior residents and fellows, etc.
• Where – multiple settings (e.g., out-patient, in-patient, acute care, chronic care, simple, complex patient settings, etc.)
• When – as frequently as possible

Giving Feedback
• R2C2 feedback model (Sargeant 2016)– Relationship building– exploring Reactions to the feedback– Exploring understanding of feedback
Content– Coaching for performance change

\“Feedback considered good or helpful was specific, timely,
actionable and credible.” Watling et al., 2014
Key Principles for Giving Feedback
• Constructive• Direct• Specific• Timely• Focus on:
– Modifiable behaviours, decisions and actions
• Documentation
Anatomy of a Feedback Session
• The set-up • The feedback• The action plan• Summarize

EPAs
Direct Observation
Assessment
Feedback
CBD in the workplace

Competence Committee• Transition from Promotion Committee to Competence Committee
• Competence Committee Chair• Reviews all assessments
– (EPA forms, STACERs, required training experiences, OSCEs, etc…)
• Will meet minimum 4 times a year (and ad hoc prn)• Reports to RPC
– statement in Royal College documents; symbolic; no apparent operational change
• High‐stakes decision‐makers

PGME Initiatives/Resources
• CBME Program Leads• Competence Committee Chairs• Workshops and retreats for PDs and Admins and Faculty
• Multiple One‐on‐one sessions with PDs and Administrators
• Faculty Development Grant

3 things you need to do
• Observe (what did you see?)
• Feedback (what did you say?)
• Document (what did you write down?)

Additional information Royal College of Physician and Surgeons of Canada• Introduction to CBME and CBD
https://www.youtube.com/watch?v=pSBs9Mg-GIM
• Understanding Entrustable Professional Activities https://www.youtube.com/watch?v=5Ase3ETcsu0&sns=em
• Website – info about CBD implementation, competence committees, and other helpful resources http://www.royalcollege.ca/rcsite/cbd/competence-by-design-cbd-e

Questions???


Geriatric Medicine & CBME:Where are we now?
Laura DiachunChair, Nucleus Committee for
Geriatric Medicine

Faculty/Presenter Disclosure
• Faculty: Laura Diachun
• Relationships with financial sponsors:– Grants/Research Support: None– Consulting Fees: None– Patents: None– Other: None

Disclosure of Financial Support• This program has received financial support from nobody.
• Potential for conflict(s) of interest:– This is about geriatric education and I LOVE geriatric education
Mitigating Potential Bias
• My bias is that educating future geriatricians is of utmost importance. I am hoping not to mitigate this!
Objectives
1. Explain Geriatric Medicine’s progress with its planned transition to CBME
2. Identify Entrustable Professional Activities (EPAs) of Geriatric Medicine
3. Describe Geriatric Competencies and their potential evaluation strategies

National Endeavour
• March 2017‐present

Age Old Question
What exactly does a geriatrician do?

1) Regional variation in practice2) Site specific resources3) Language of origin
Challenging Considering:

Stage 1 – Transition to Discipline2‐6 weeks
Stage 2 – Foundations of Discipline6‐8 months
Stage 3 – Core of Discipline12 months
Stage 4‐Transition to Practice2‐4 months
1. Initiating a comprehensive geriatric assessment, identifying common geriatric syndromes, and suggesting a management plan
2. Assessing and proposing management for older adults with common Internal Medicine conditions
1. Performing a comprehensive geriatric assessment (CGA)
2. Diagnosing and managing common medical conditions in older patients
3. Assessing and managing common neuro‐cognitive disorders with typical presentations
4. Diagnosing and initiating management of delirium
5. Identifying issues with medication use and making suggestions for optimal prescribing
6. Completing falls risk assessments to include gait analysis and balance
7. Teaching and supervising junior learners
1. Managing older adults with functional decline using CGA
2. Managing older adults with multiple co‐morbidities across the spectrum of frailty
3. Assessing and managing patients with a complex and/or uncommon neuro‐cognitive presentations
4. Assessing and managing uncomplicated mental health conditions in older adults
5. Preventing and managing delirium
6. Assessing and managing complex psycho‐social issues unique to vulnerable older adults
7. Managing end‐of‐life in older adults
8. Teaching other learners
9. Running family and team meetings
10. Managing BPSD
11. Determining patients’ capacity for decision‐making
1. Managing the Geriatrician’s practice
2. Contributing to the improvement of health care delivery for older people in teams, organizations, and systems
3. Planning and completing personalized training experiences aligned with career plans and/or specific learning needs **NEW / ELECTIVE EPA**
Special assessments:Developing a personal learning plan
Advancing geriatric medicine through a scholarly project

Stage 1 – Transition to Discipline2‐6 weeks
Stage 2 – Foundations of Discipline6‐8 months
Stage 3 – Core of Discipline12 months
Stage 4‐Transition to Practice2‐4 months
1. Initiating a comprehensive geriatric assessment, identifying common geriatric syndromes, and suggesting a management plan
2. Assessing and proposing management for older adults with common Internal Medicine conditions
1. Performing a comprehensive geriatric assessment (CGA)
2. Diagnosing and managing common medical conditions in older patients
1. Managing older adults with functional decline using CGA
2. Managing older adults with multiple co‐morbidities across the spectrum of frailty
1. Managing the Geriatrician’s practice

TD 1: Initiating a comprehensive geriatric assessment (CGA) and identifying common geriatric syndromes
Key Features:• This EPA focuses on components of the CGA, including conducting a comprehensive history and physical examination, documenting the clinical encounter, and identifying common geriatric syndromes
• This EPA also includes mental status assessments using Mini–Mental State Examination (MMSE) and a Montreal Cognitive Assessment (MoCA)
• This EPA does not include analysis and synthesis

F 1: Performing a comprehensive geriatric assessment (CGA)
Key Features:
• This EPA focuses on all components of the CGA, including analyzing and synthesizing diagnoses for common geriatric syndromes
• This EPA also includes incorporating medical and interprofessional team input, comprehensive care planning, awareness of community services, living environments and programs, and managing transitions of care, managing goals of care, discharge planning, and rehabilitation potential

C 1: Managing older adults with functional decline using comprehensive geriatric assessment (CGA)
Key Features:• This EPA builds on the competencies of the Foundations stage to
focus on generating a feasible management plan using CGA, including communicating prognosis, care planning, and managing transitions of care
• This EPA includes creating a prioritized problem list with a patient‐and/or family‐centered management plan that projects functional status trajectory of and assesses for rehabilitative potential
• The observation of this EPA includes the completion of a STACER and is divided into three parts: management plan; communication with patient and family; communication with referring source
TTP 1: Managing the Geriatrician’s Practice
Key Features:• This EPA includes managing service delivery, contributing to team
functioning, managing patient flow, demonstrating the ability to work simultaneously in more than one setting (covering more than one clinical service at a time, teaching, committees), completing medical and legal documents, time management, office management, billing and remuneration.
• This EPA is split into two components:1. Practice review/audit: review of the multiple components of practice including: combination of inpatient/consult service and outpatient experiences; time management; team functioning; and, office management over a specific timeframe (min of 2 weeks) to complete “independent practice”2. Shadow billing

Stage 1 – Transition to Discipline2‐6 weeks
Stage 2 – Foundations of Discipline6‐8 months
Stage 3 – Core of Discipline12 months
Stage 4‐Transition to Practice2‐4 months
1. Initiating a comprehensive geriatric assessment, identifying common geriatric syndromes, and suggesting a management plan
1. Assessing and managing common neuro‐cognitive disorders with typical presentations
2. Diagnosing and initiating management of delirium
1. Assessing and managing patients with a complex and/or uncommon neuro‐cognitive presentations
2. Managing BPSD
3. Preventing and managing delirium
F 3: Assessing, diagnosing and managing common neuro‐cognitive disorders with typical presentations
Key Features:• This EPA focuses on the initial assessment and diagnosis of patients with common
neurocognitive disorders but does not include patients with delirium or behavioural and psychological symptoms of dementia (BPSD)
• This EPA includes performing and interpreting cognitive assessment, physical examination and investigations, communicating diagnosis and prognosis, identifying potentially modifiable conditions, and recognizing the need for neuropsychological testing
• This EPA also includes managing patients with pharmacologic and non‐pharmacologic treatment options, utilizing community support programs, and demonstrating awareness of medicolegal aspects, and future planning
• The observation of this EPA is divided into three parts: cognitive assessment; communication with patient and/or caregiver; management
Assessment Plan
• Part A : Cognitive assessment
• Direct or indirect observation in the form of a case review by supervisor
• Case Mix: MCI; Alzheimer’s; vascular/mixed dementias; lewy body dementias
• Supervisor: geriatrician; geriatric psychiatrist; behaviouralneurologist; care of the elderly physician;
• Setting: Any clinical setting; simulation
• Collect 6 direct or indirect observations of achievement• At least 1 of each from the case mix • At least 3 by a geriatrician
Part B: Communication with patient/caregiver
• Direct observation by supervisor
• Communication Scenarios: communicating diagnosis with patient and family; communicating driving risk; communicating home safety risk; communicating about management of finances; communicating other safety issues [select all that apply]
Supervisor: geriatrician; geriatric psychiatrist; behavioural neurologist; care of the elderly physician
Settings: inpatient; outpatient
Collect 5 observations of achievement • At least 1 of the following types of communication: home safety, driving,
management of finances, or other safety issues• At least 1 communication of driving risk • At least 2 observations by a geriatric medicine specialists

Part C: Management
• Direct or indirect observation by supervisor
• Case Mix: MCI; Alzheimer’s; vascular/mixed dementias; lewy body dementias
• Supervisor role: geriatrician; geriatric psychiatrist; behavioural neurologist; care of the elderly physician;
• Settings: inpatient; outpatient; simulation
• Collect 5 observations of achievement. • At least 1 each of the case mix• At least 2 observations by a geriatric medicine specialist
C 4: Assessing and managing patients with complex and/or uncommon neuro‐cognitive presentations
Key Features:
• This EPA focuses on assessing and managing less common neuro‐cognitive disorders, such as non‐Alzheimer dementias and non‐vascular dementias
• This EPA includes performing a comprehensive neurological exam to support atypical features, as well as managing other factors that can complicate the presentation
• This EPA does not include the diagnosis of common and typical neuro‐cognitive disorders, the use of basic cognitive screening tests, or counseling about basic safety issues (e.g. driving, home safety, etc.)
• The observation of this EPA is divided into two parts: assessment and management of complex and/or uncommon neurocognitive disorders; and counseling and communication of diagnosis and prognostic issues specific to these less common disorders

EPAs and Observations
• 22 mandatory EPAs• Direct or indirect observations
– 6 TTD– 49 Foundation– 51 Core– 5 TTP

Royal College certification in Geriatric Medicine requires all of the following:
1. Royal College certification in Internal Medicine;
2. Successful completion of the Royal College examination in Geriatric Medicine;
3. Completion of all elements of the Geriatric Medicine Portfolio including: 1. Family meeting Structured Assessment for Clinical Encounter Report
(STACER) C102. Team meeting STACER (C10)3. Comprehensive Geriatric Assessment STACER in Foundations EPA 14. Comprehensive Geriatric Assessment STACER in Core EPA 15. ? Multi‐source feedback

CBD Document Suite
• Competency Training Requirements (CTR) (formerly OTR)
• Training Experiences document• Specific Standards for Accreditation
• ……. Coming soon to a program near you

Practice medicine within their defined scope of practice and expertise
– Apply knowledge of the clinical and biomedical sciences relevant to Geriatric Medicine
• Distinction between normal aging and disease states • Impact of age on common medical conditions• Principles of the diagnosis and management of common medical conditions in the older adult
• Principles of the diagnosis and management of the older adult with multiple, complex medical conditions or syndromes:
– Dementia, including behavioural and psychological symptoms– Mild cognitive impairment (MCI)– Falls and mobility issues– Bowel and bladder dysfunction etc

Time Line
• April 1, 2018 Document suite submitted for review
• June: Yay or nay decision• June‐Sept: documents submitted for translation
• Oct‐Nov: documents ready for dissemination• July 1 2019: Geriatric Medicine CBME implemented nationally
Questions?