transitional cell carcinoma
TRANSCRIPT

Genito-Urinary Tumors
Episode 6

Transitional Cell Carcinoma
• Primary neoplasms of the renal collecting
system represent 10% of the renal tumors, of
which approximately 80% are malignant. Most
are transitional cell carcinomas (TCCs).

Transitional Cell Carcinoma
• Bladder TCC is 50 times more common than
renal pelvic tumors. Often, TCCs are multiple,
involving any part or all of the collecting system.

Transitional Cell Carcinoma
•The male-to-female ratio is 3-4:1
•50-70 years.

Transitional Cell Carcinoma
Causative agents:
Exposure to a large variety of chemical carcinogens:
1. Tobacco.2. Aniline dyes.3. Benzidine.4. Aromatic amines. 5. Abuse of analgesics.6. Cyclophosphamide therapy, particularly after drug-
induced hemorrhagic cystitis.7. Recurrent or chronic infection and urinary calculi. Renal pelvic papillomas.

Transitional Cell Carcinoma
Causative agents:
• Chemical carcinogens act locally on the epithelium
causing chronic irritation → Hyperplastic Metaplastic
changes.
• Their action is enhanced by the contact time.
• Partial obstruction may account for increased exposure to
the upper tracts.

Transitional Cell Carcinoma
Pathology:
Broad classification:
(1) Exophytic papillary lesion (85%).
(2) Non-papillary, non-infiltrating.
(3) Infiltrating.
(4) Carcinoma in situ.

Transitional Cell Carcinoma
Pathology:
Spread:
1. Direct extension into the retroperitoneum.
2. Hematogenous.
3. Lymphatic.

Transitional Cell Carcinoma
Pathology:
Spread:
Metastases from ureteral TCC are far more common
than those from bladder cancer partly because the
ureteral wall is thin and acts as a poor barrier.

Transitional Cell Carcinoma
Hematuria.
• For upper tract TCC pain, abdominal mass
and pyuria.
• Dysuria and frequency are more commonly
reported with ureteral & bladder tumors.

Imaging
Transitional Cell Carcinoma
Transitional Cell Carcinoma
Plain X-Ray:
•Normal.
•Large renal outline may be seen in a completely
obstructed kidney.
•Displacement of renal calcifications, which occur in
analgesic nephropathy.
•Metastases.

Transitional Cell Carcinoma
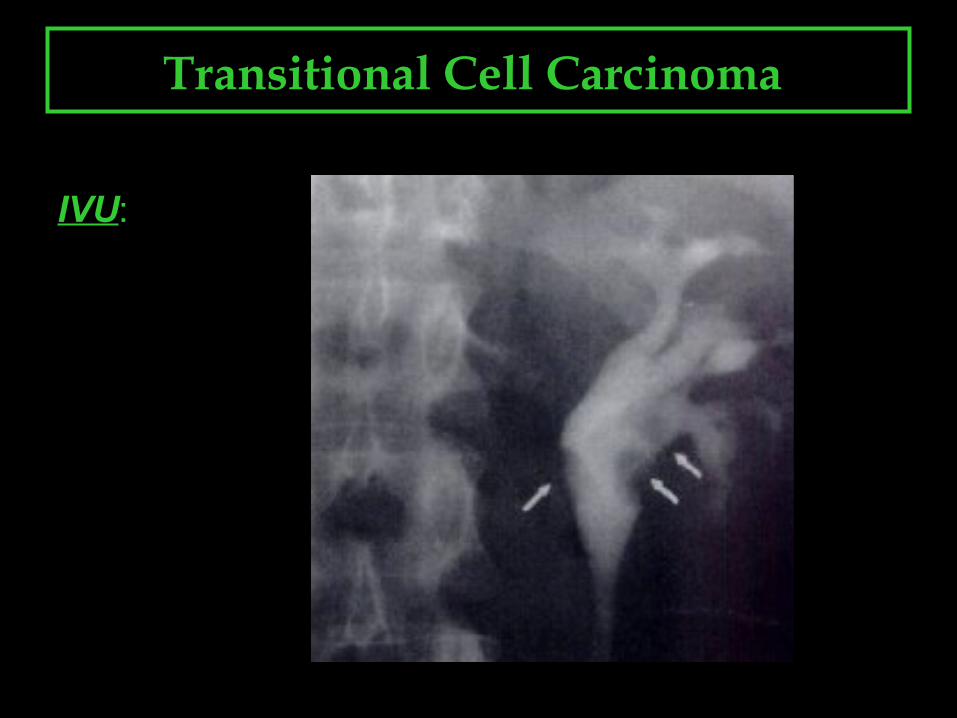
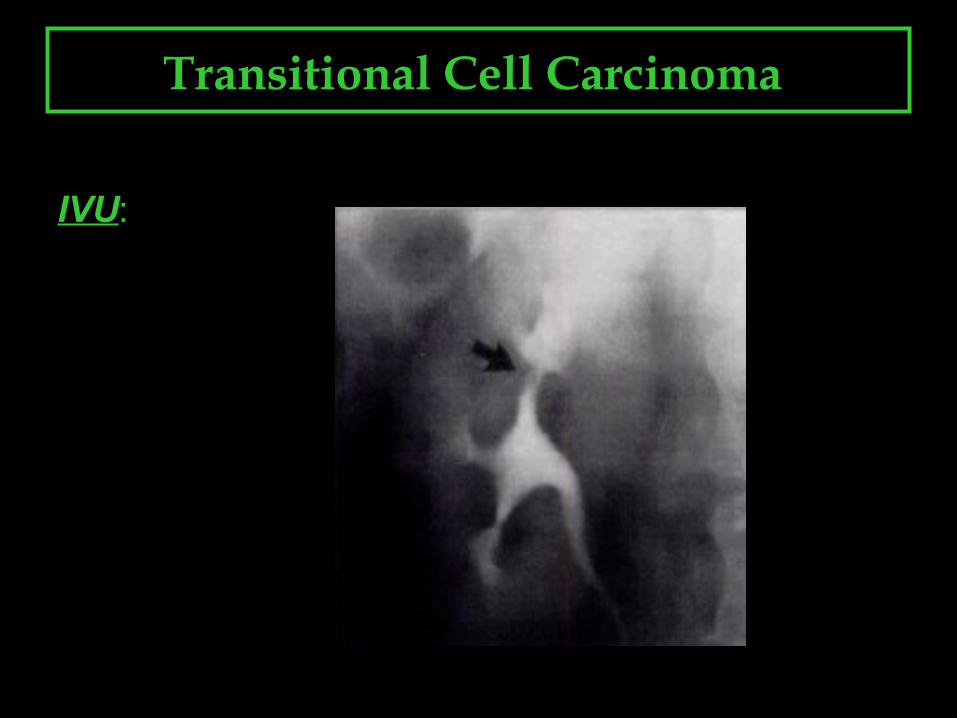
IVU:
• Single or multiple filling defects in renal pelvis/ureter.
• Stipple sign.
• Large renal outline may be seen in a completely obstructed
kidney.
• Displacement of renal calcifications, which occur in analgesic
nephropathy.
• Metastases.

Transitional Cell Carcinoma
IVU:

Transitional Cell Carcinoma
IVU:
Transitional Cell Carcinoma
IVU:

Transitional Cell Carcinoma
IVU:
Transitional Cell Carcinoma
IVU:

Transitional Cell Carcinoma
IVU:

Transitional Cell Carcinoma
Retrograde Pyelography :
• Focal expansion of ureters around
and distal to the mass called the
champagne, or goblet, sign.

Transitional Cell Carcinoma
Retrograde Pyelography :
• Focal expansion of ureters around
and distal to the mass called the
champagne, or goblet, sign.

Transitional Cell Carcinoma
Retrograde Pyelography :
• Focal expansion of ureters around
and distal to the mass called the
champagne, or goblet, sign.

Transitional Cell Carcinoma
Retrograde Pyelography :
•Occasionally, the catheter may coil below the
mass during retrograde catheterization; this is
called the Bergman sign.

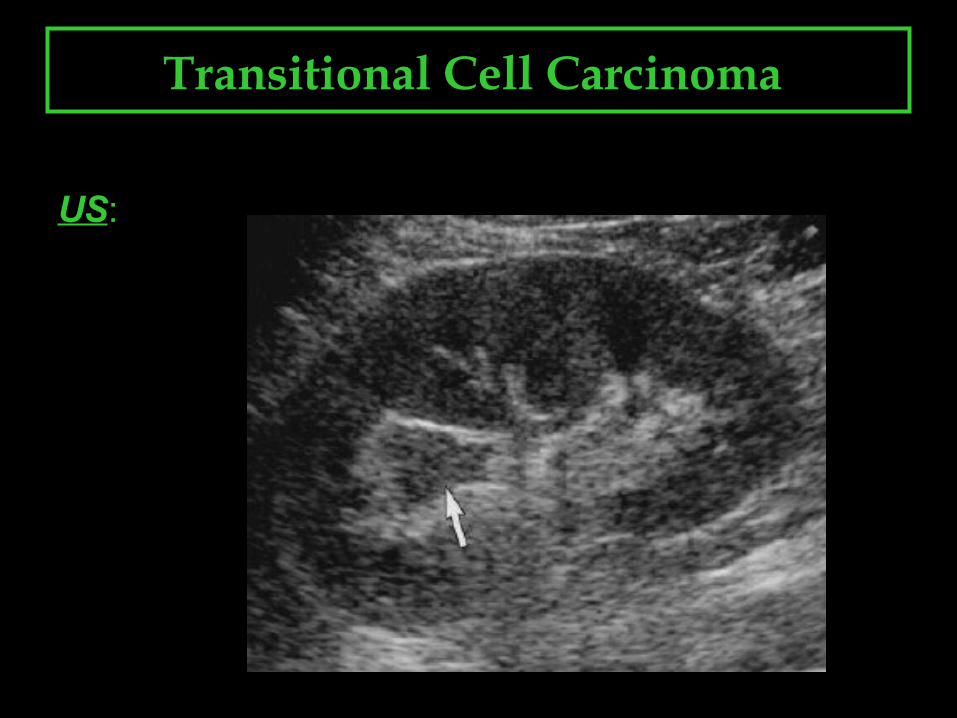
US:
• Hypoechoic renal collecting system mass splitting the
central echocomplex with varying degree of
infundibular dilatation.
• Focal hypoechogenicity of adjacent renal cortex
reflects local invasion.
• Occasionally, the central echocomplex may be only
segmentally amputated.
• Normal.
Transitional Cell Carcinoma

US:
Transitional Cell Carcinoma
US:
Transitional Cell Carcinoma

US:
Transitional Cell Carcinoma

US:
Transitional Cell Carcinoma

Transitional Cell Carcinoma
CT:
• Irregular filling defects of the pelvocalyceal system
and ureters, with obstruction and dilatation of the
ureter and pelvis proximal to the lesion.
• Ureteral wall thickening.
Transitional Cell Carcinoma
CT:
• NECT: TCC is hypoattenuating or isoattenuating relative to the
normal renal parenchyma, and it is hyperattenuating relative to
urine.
• CECT: Mild- to-moderate enhancement.
• DELAYED CECT/CTU: Hypoattenuating relative to opacified
urine.

Transitional Cell Carcinoma
CT:

Transitional Cell Carcinoma
CT:

Transitional Cell Carcinoma
CT:

Transitional Cell Carcinoma
CT:

Transitional Cell Carcinoma
CT:

Transitional Cell Carcinoma
CT:

Transitional Cell Carcinoma
CT:

Transitional Cell Carcinoma
CT:

Transitional Cell Carcinoma
MRI:
• TCC has lower signal intensity than the normally high-signal-
intensity urine on T2-weighted images.
• TCC is nearly isointense to renal parenchyma on T1- and T2-
weighted images.
• Moderate enhancement is seen with gadolinium contrast
material.
• MR urography.