transfusion med. prac
TRANSCRIPT
1
CLINICAL PRACTICE CLINICAL PRACTICE OF OF
TRANSFUSION MEDICINETRANSFUSION MEDICINE
DR. RAFIQ AHMAD
2
ContentsContents
Procurement and processing Clinical use of red cells, platelets, plasma, and
cryoprecipitate Adverse effects Alternatives Good transfusion practices
3
Saudi Food and Drug Authority enforces strict standards for screening donors for collection, processing and distribution of
blood and components Saudi Ministry of Health Blood Services are responsible for
donor recruitment collection, processing and distribution of blood components referral centers
Hospitals hospital blood banks hospital transfusion services - also responsible for supply of manufactured products (e.g. albumin, clotting factor VIII)
BasicsBasics
4
Types of donationsTypes of donations
1. Voluntary (including mobiles) -70% in RBB 1. Voluntary (including mobiles) -70% in RBB 2. Replacement – 30% in RBB2. Replacement – 30% in RBB3. Autologous and Directed Donations - rare3. Autologous and Directed Donations - rare
Autologous blood (patient’s own blood) may be collected in advance of elective surgery by blood center or at the treating hospital
Directed donations from parent to minor child, from selected donors for patients with rare blood types or platelet refractor-iness are available through the blood center
5
Donor RegistrationDonor Registration
Each donation is registered by Identification, and a Record of Donation, consisting of two parts:
Questions about e.g. general health, travel
Questions by a skilled interviewer about “risk behaviors” e.g. illicit drug use
6
Donor ScreeningDonor Screening * Hb estimation
* Sickle cell testing * ABO grouping * Rh-D typing
Medical Examination * General Health * Pulse * BP * Temperature * Skin
7
Testing the Donation I.Testing the Donation I.
All donations are tested for some infectious agents:
HIV by antigen/antibody, and NAT HCV by antibody, and NAT HBV by HBsAg/antibody to HBc
total and NAT HTLV by antibody Syphilis by antibody (RPR/TPHA) Malaria by slide
8
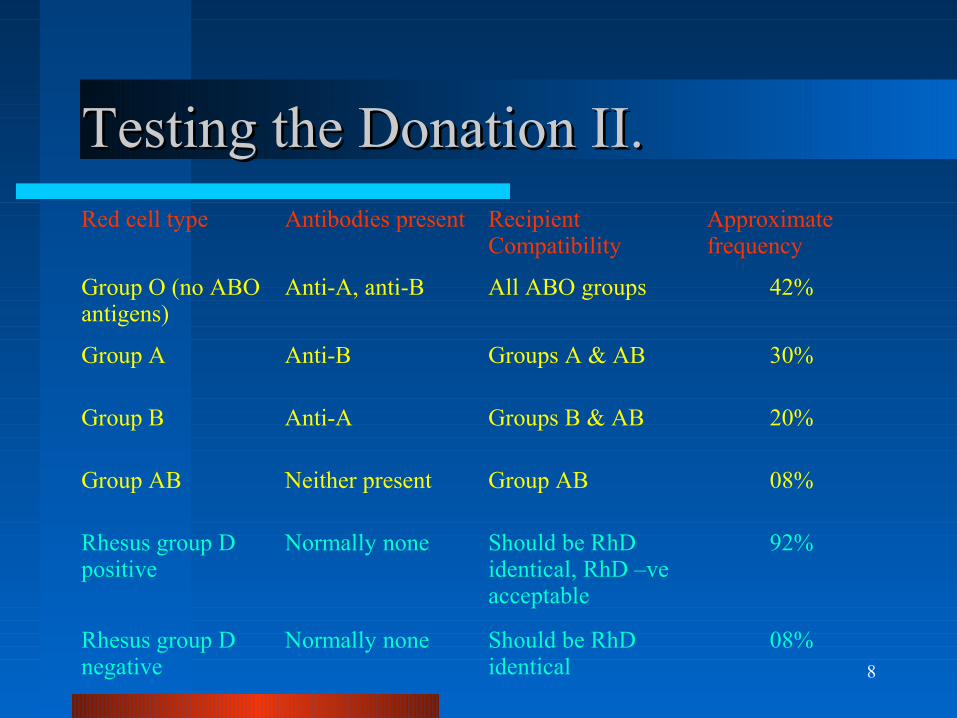
Testing the Donation II.Testing the Donation II.Red cell type Antibodies present Recipient
CompatibilityApproximate frequency
Group O (no ABO antigens)
Anti-A, anti-B All ABO groups 42%
Group A Anti-B Groups A & AB 30%
Group B Anti-A Groups B & AB 20%
Group AB Neither present Group AB 08%
Rhesus group D positive
Normally none Should be RhD identical, RhD –ve acceptable
92%
Rhesus group D negative
Normally none Should be RhD identical
08%
9
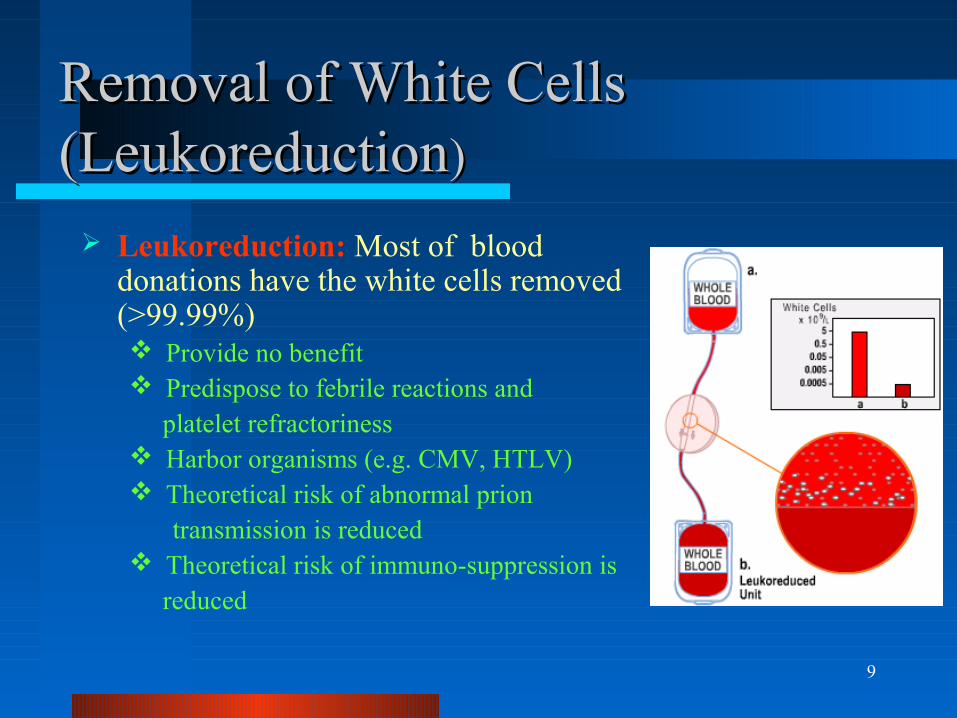
Removal of White Cells Removal of White Cells (Leukoreduction(Leukoreduction))
Leukoreduction: Most of blood donations have the white cells removed (>99.99%) Provide no benefit Predispose to febrile reactions and platelet refractoriness Harbor organisms (e.g. CMV, HTLV) Theoretical risk of abnormal prion
transmission is reduced Theoretical risk of immuno-suppression is reduced
10
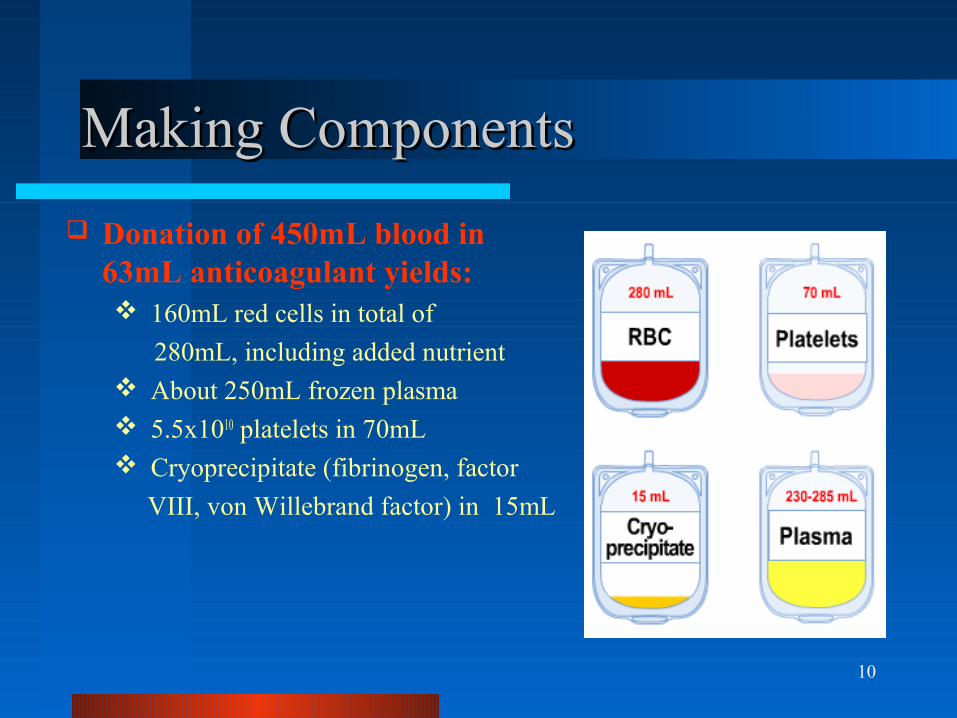
Making ComponentsMaking Components
Donation of 450mL blood in 63mL anticoagulant yields: 160mL red cells in total of
280mL, including added nutrient About 250mL frozen plasma 5.5x1010 platelets in 70mL Cryoprecipitate (fibrinogen, factor
VIII, von Willebrand factor) in 15mL
11
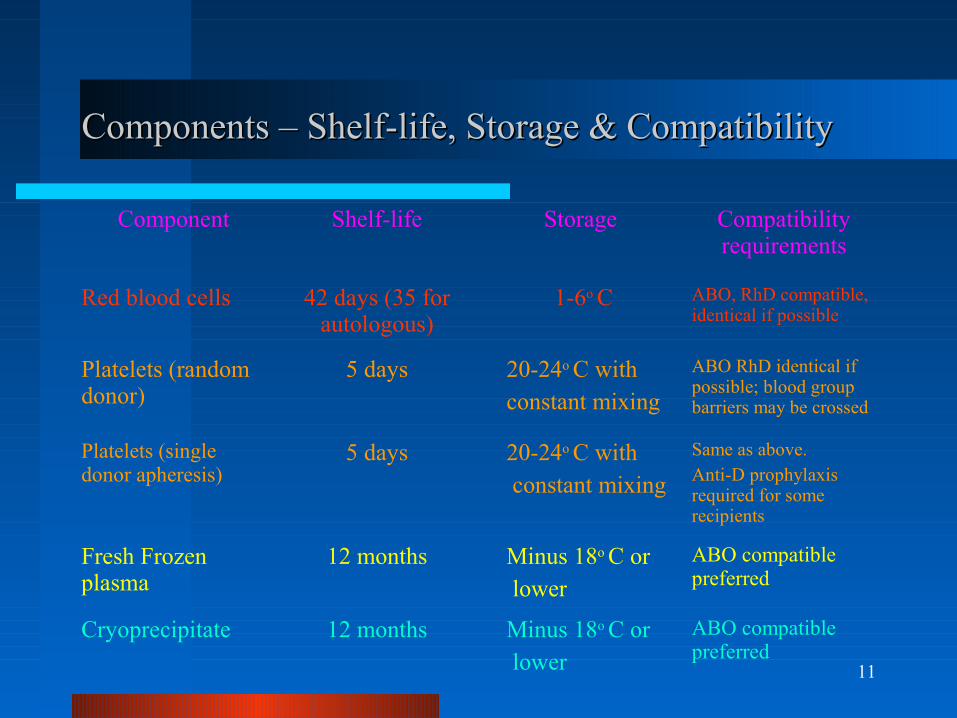
Components – Shelf-life, Storage & CompatibilityComponents – Shelf-life, Storage & Compatibility
Component Shelf-life Storage Compatibility requirements
Red blood cells 42 days (35 for autologous)
1-6o C ABO, RhD compatible, identical if possible
Platelets (random donor)
5 days 20-24o C with constant mixing
ABO RhD identical if possible; blood group barriers may be crossed
Platelets (single donor apheresis)
5 days 20-24o C with constant mixing
Same as above. Anti-D prophylaxis required for some recipients
Fresh Frozen plasma
12 months Minus 18o C or lower
ABO compatible preferred
Cryoprecipitate 12 months Minus 18o C or lower
ABO compatible preferred
12
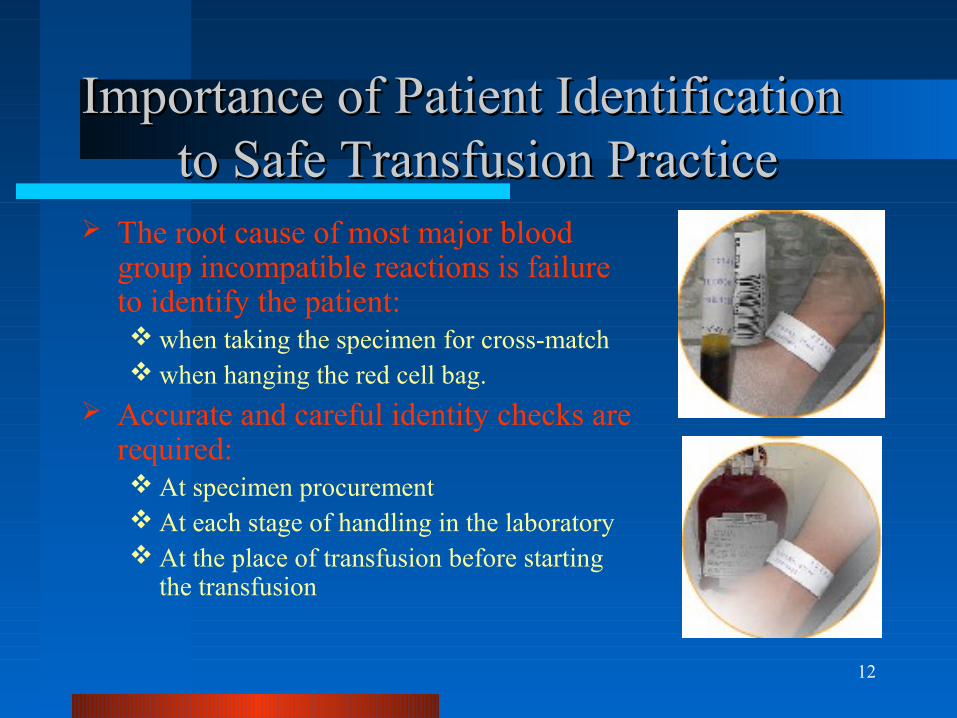
Importance of Patient Identification Importance of Patient Identification to Safe Transfusion Practiceto Safe Transfusion Practice
The root cause of most major blood group incompatible reactions is failure to identify the patient: when taking the specimen for cross-match when hanging the red cell bag.
Accurate and careful identity checks are required: At specimen procurement At each stage of handling in the laboratory At the place of transfusion before starting
the transfusion
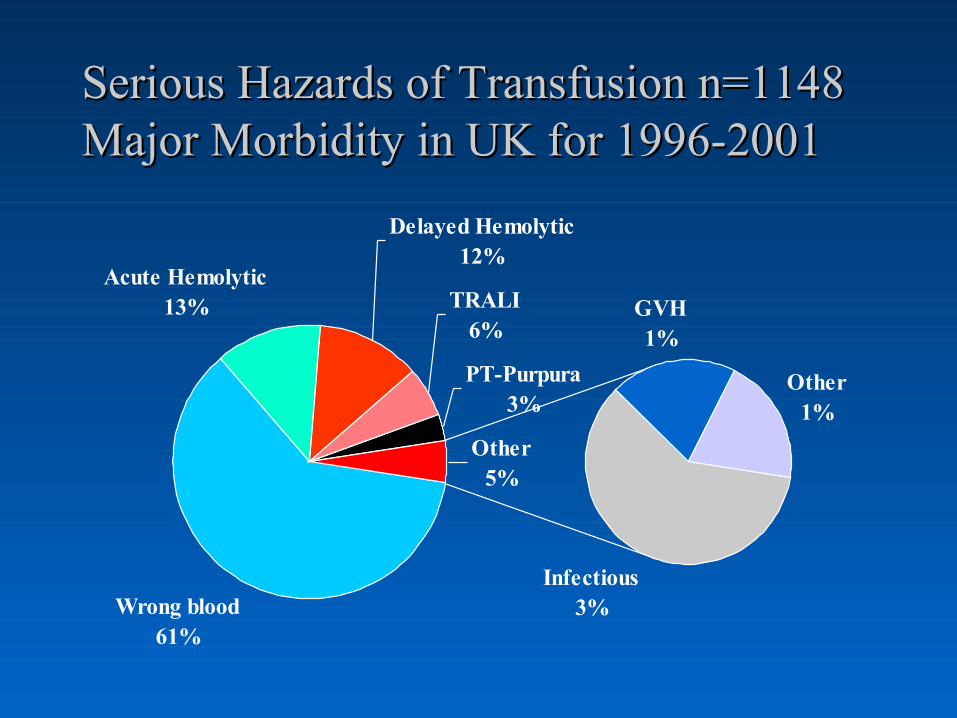
Serious Hazards of Transfusion n=1148 Serious Hazards of Transfusion n=1148 Major Morbidity in UK for 1996-2001Major Morbidity in UK for 1996-2001
Wrong blood61%
Acute Hemolytic13%
Delayed Hemolytic12%
TRALI6%
PT-Purpura3%
Infectious3%
GVH1%
Other1%
Other5%
14
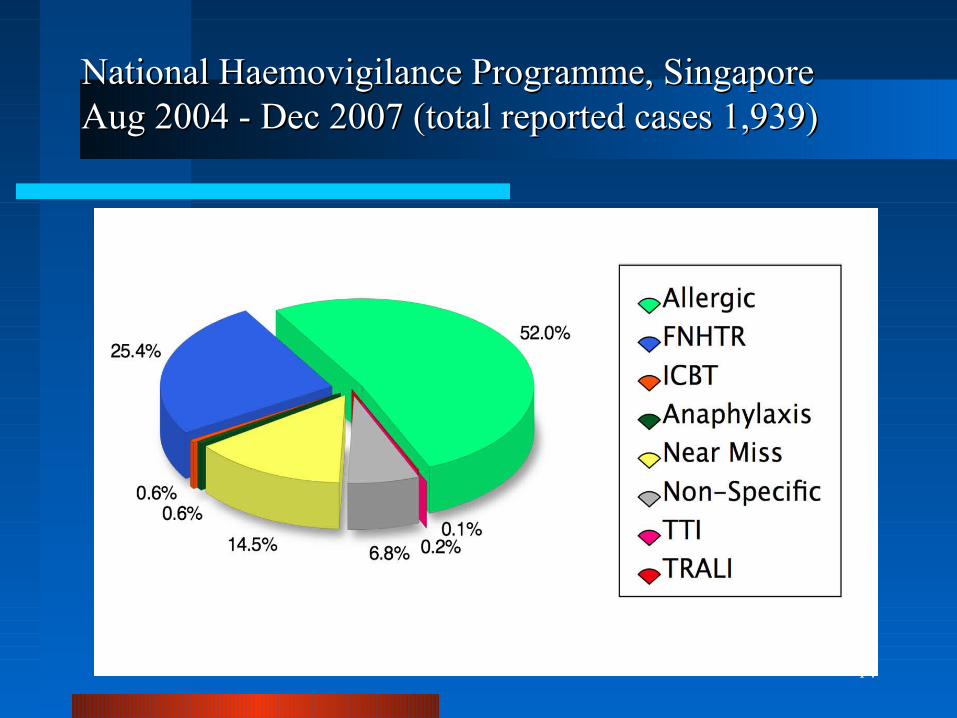
National Haemovigilance Programme, SingaporeNational Haemovigilance Programme, SingaporeAug 2004 - Dec 2007 (total reported cases 1,939)Aug 2004 - Dec 2007 (total reported cases 1,939)
15
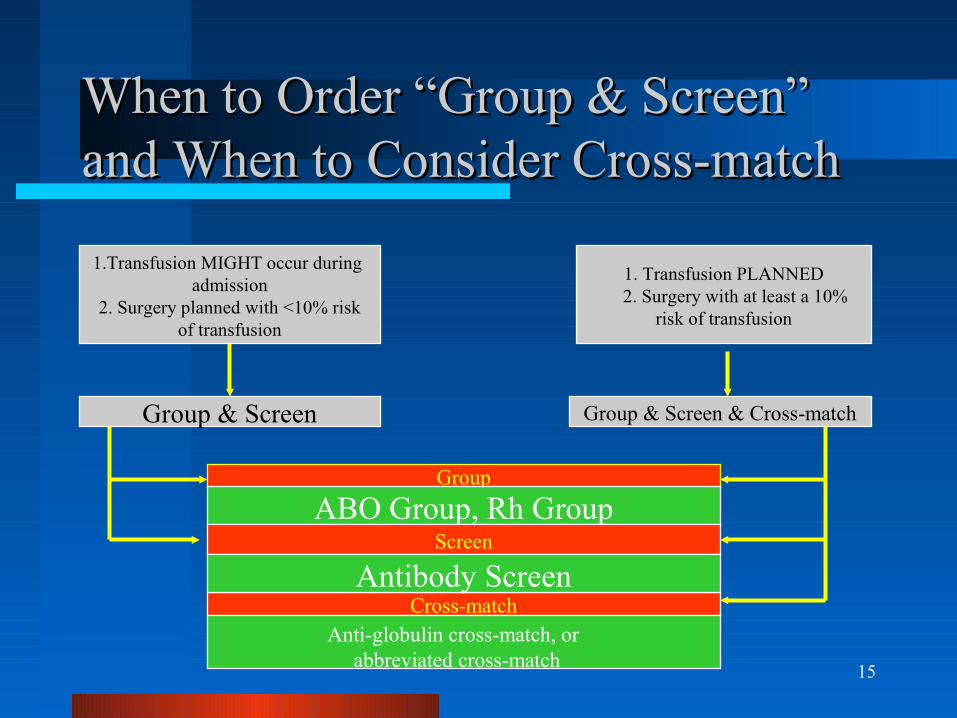
When to Order “Group & Screen” When to Order “Group & Screen” and When to Consider Cross-matchand When to Consider Cross-match
1.Transfusion MIGHT occur during admission
2. Surgery planned with <10% risk of transfusion
1. Transfusion PLANNED 2. Surgery with at least a 10%
risk of transfusion
Group & Screen Group & Screen & Cross-match
Group
ABO Group, Rh GroupScreen
Cross-matchAntibody Screen
Anti-globulin cross-match, or abbreviated cross-match
16
Red Blood Cell TransfusionRed Blood Cell Transfusion
This section covers: Contents of a unit of red cells Patient testing Selection of compatible units Expected outcome of transfusion Good transfusion practices Guidelines for use of red cells
17
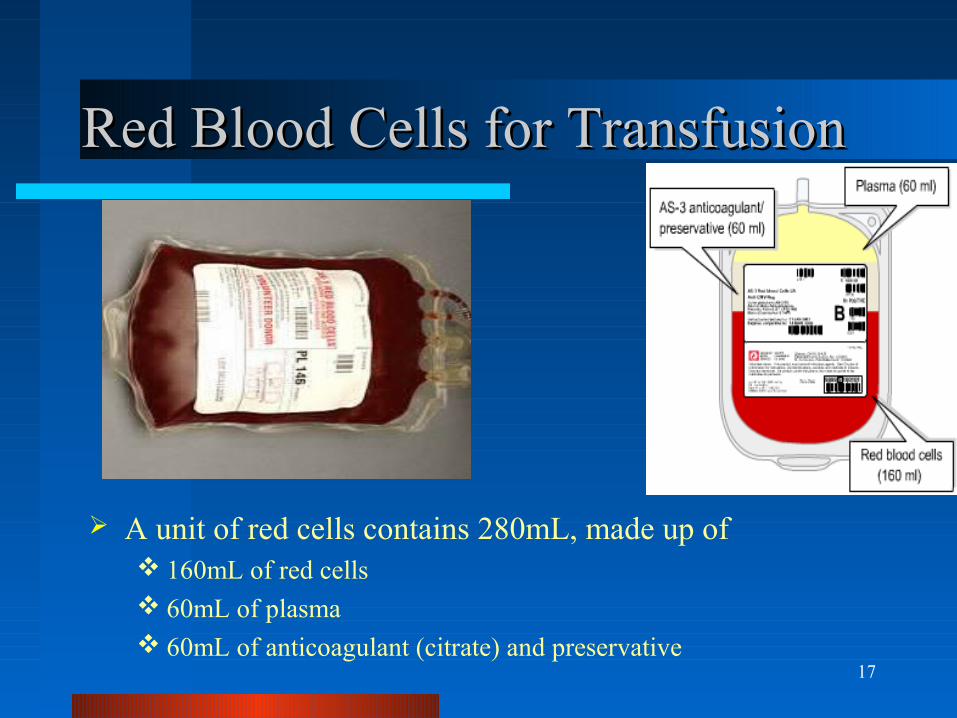
Red Blood Cells for TransfusionRed Blood Cells for Transfusion
A unit of red cells contains 280mL, made up of 160mL of red cells 60mL of plasma 60mL of anticoagulant (citrate) and preservative
18
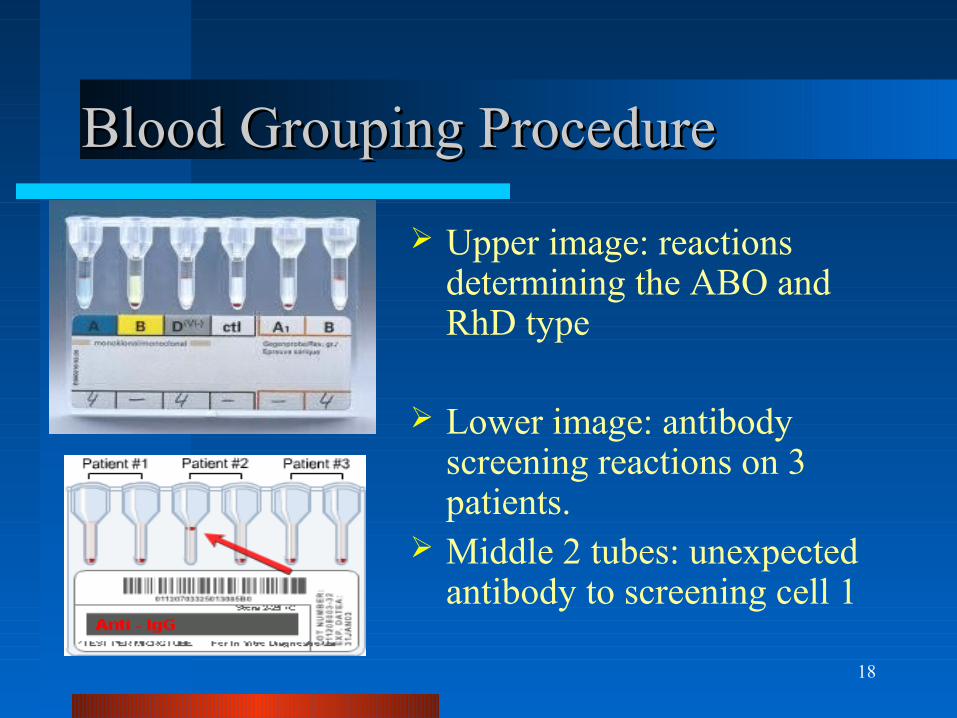
Blood Grouping ProcedureBlood Grouping Procedure
Upper image: reactions determining the ABO and RhD type
Lower image: antibody screening reactions on 3 patients.
Middle 2 tubes: unexpected antibody to screening cell 1
19
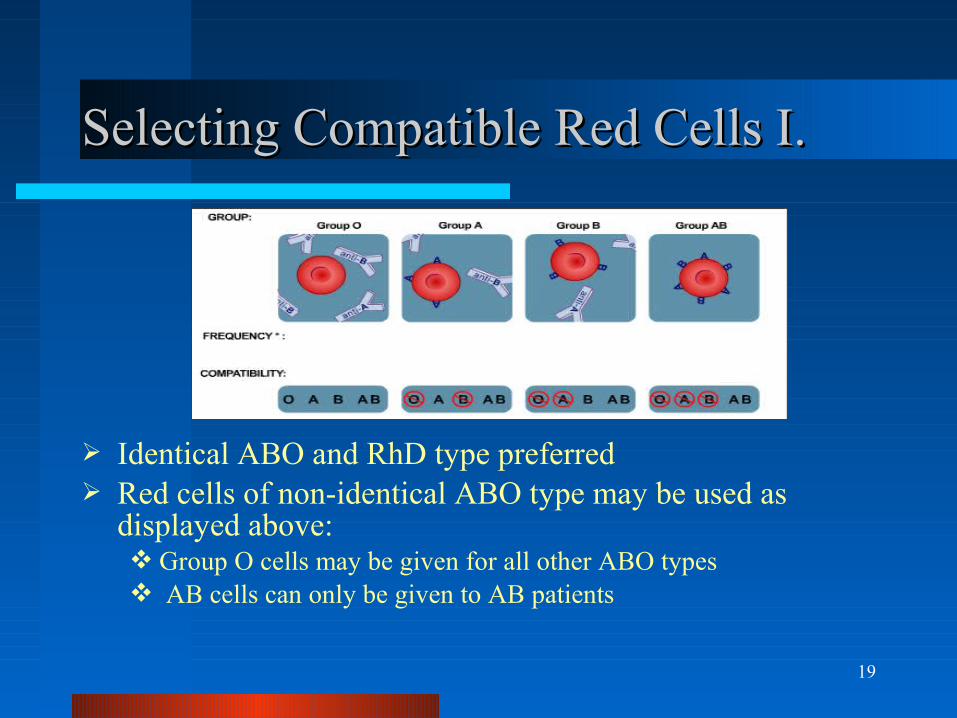
Selecting Compatible Red Cells I.Selecting Compatible Red Cells I.
Identical ABO and RhD type preferred Red cells of non-identical ABO type may be used as
displayed above: Group O cells may be given for all other ABO types AB cells can only be given to AB patients
20
Selecting Compatible Red Cells II.Selecting Compatible Red Cells II.
The RhD antigen is highly immunogenic
Transfusing RhD +ve blood to an RhD -ve patient should be avoided wherever possible
RhD –ve females with child-bearing potential should never receive any RhD +ve products unless there is no alternative
Such female RhD –ve patients should receive prophylactic treatment with anti-D
Patients with an unexpected antibody should receive only red cells lacking the corresponding blood group antigen
21
Transfusion of Red CellsTransfusion of Red Cells
A unit of red cells is expected to raise the hemoglobin 10 g/L
Transfuse a single unit over 2 hours and not more than 4 hours
Assess the outcome (clinical, hemoglobin level) before transfusing further
22
The 10 FactsThe 10 Facts
1. Base decisions on national guidelines2. Minimize blood loss and use conservation
measures3. In acute blood loss, use effective resuscitation
while assessing transfusion needs4. Hemoglobin level not the only consideration in
decision to transfuse5. Transfusion only one element in treatment6. Be aware of risks of transfusion
23
The 10 Facts contd…The 10 Facts contd…
7. Prescribe only when the benefits outweigh the risks
8. Clearly record the reason for transfusion
9. Monitor the first 15 minutes of the transfusion for adverse
events
10. Obtain informed consent for transfusion of any blood
product• Must be given voluntarily and clearly documented
• Patient must have the capacity to give consent
• Consent must be specific to the treatment proposed
• Patient must understand the nature, risks and benefits
24
Transfusion in Acute Blood LossTransfusion in Acute Blood Loss
Maintain hemoglobin over 70 g/L during active bleeding Anticipate need when hemoglobin drops below 80 g/L Consider maintaining higher level (80-100 g/L) with:
Impaired pulmonary function Increased oxygen consumption (e.g. fever) Unstable coronary disease Atherosclerosis Uncontrolled bleeding
Patients with levels above 100 g/L are unlikely to benefit
25
Transfusion in the Critically IllTransfusion in the Critically Ill
No general benefit (& possible harm) until hemoglobin falls to 70 g/L
Transfusion recommended below 70 g/L Consider higher levels (100 g/L) in
patients with unstable angina or acute M I
26
Transfusion and the Peri-operative PatientTransfusion and the Peri-operative Patient
Pre-operatively, consider alternatives in advance (at least 5 weeks) of surgery to allow planning
Intra-operatively, meticulous attention to surgical technique
Post-operatively, adhere to good transfusion practice, minimize blood taking for laboratory tests
27
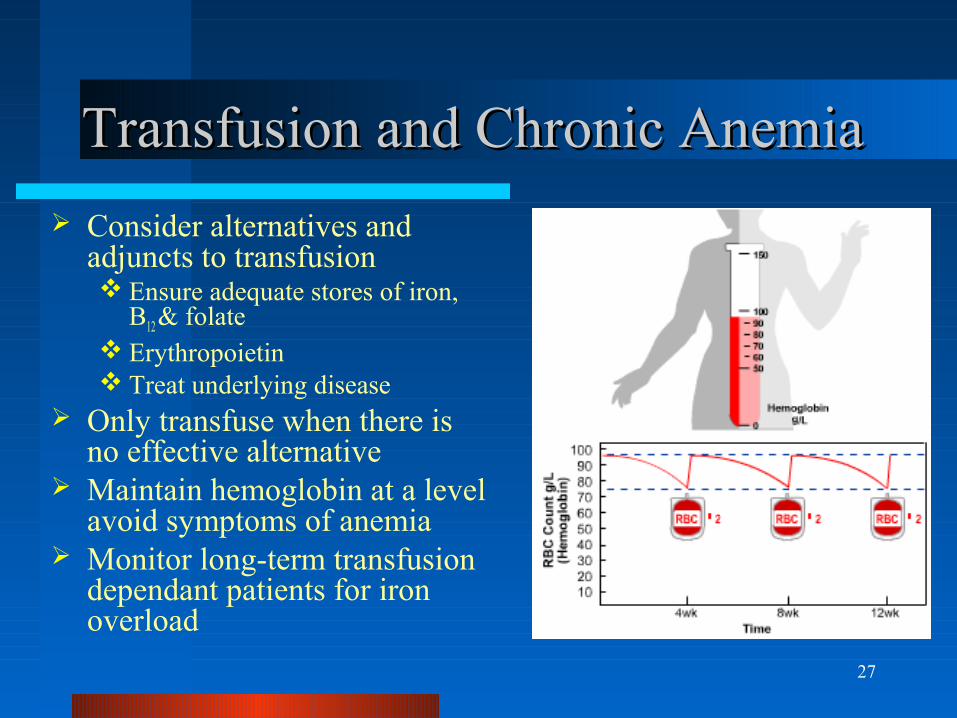
Transfusion and Chronic AnemiaTransfusion and Chronic Anemia
Consider alternatives and adjuncts to transfusion Ensure adequate stores of iron,
B12 & folate Erythropoietin Treat underlying disease
Only transfuse when there is no effective alternative
Maintain hemoglobin at a level avoid symptoms of anemia
Monitor long-term transfusion dependant patients for iron overload
28
PlateletsPlatelets
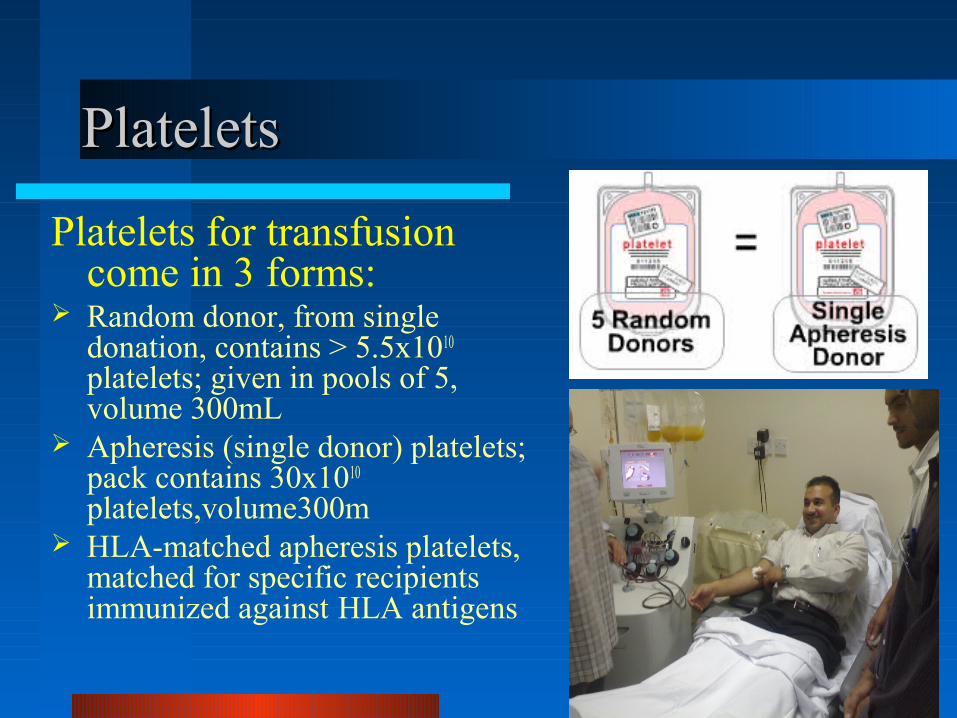
Platelets for transfusion come in 3 forms:
Random donor, from single donation, contains > 5.5x1010
platelets; given in pools of 5, volume 300mL
Apheresis (single donor) platelets; pack contains 30x1010
platelets,volume300m HLA-matched apheresis platelets,
matched for specific recipients immunized against HLA antigens
29
Platelets – Storage & TransfusionPlatelets – Storage & Transfusion
Shelf life 5 days Stored at 20-24o C with constant mixing Longer storage increases risk of septic reaction Recommended infusion time 60 minutes One pool of 5 units of random donor platelets, or
one apheresis platelet unit, should raise the platelet count by >30x109/L
Check post-transfusion platelet count within 1 hour of transfusion to determine response and detect refractoriness
30
Platelet transfusion responsePlatelet transfusion response
1. Calculation of Corrected Count Increment (CCI) in m² BSA/µL
CCI = Platelet count Increment X m² BSA/N
2. Post Platelet Recovery (PPR) in %age
PPR = Platelet count Increment X Blood Volume /N
N= Numbers of platelets transfusedNIH guidelines * 2 consecutive CCI of < 5000 platelets x m² BSA/µL indicates refractoriness after 1 hr
* PPR of < 20 % also indicates refractoriness

31
Platelets and Blood GroupPlatelets and Blood Group
ABO/RhD identical preferred ABO/RhD non-identical are
acceptable Rarely, incompatible plasma in
a platelet preparation may cause a hemolytic reaction due to high titre anti-A or anti-B
RhD –ve females of child-bearing potential receiving RhD +ve platelets require Rh-immunoglobulin prophylaxis
32
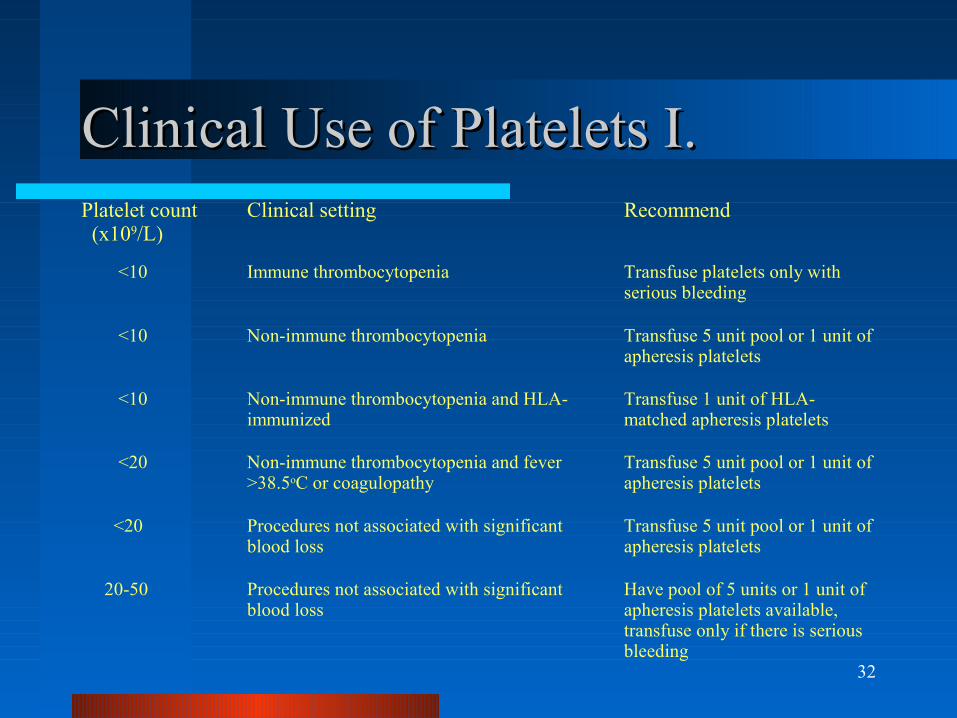
Clinical Use of Platelets I.Clinical Use of Platelets I.Platelet count (x109/L)
Clinical setting Recommend
<10 Immune thrombocytopenia Transfuse platelets only with serious bleeding
<10 Non-immune thrombocytopenia Transfuse 5 unit pool or 1 unit of apheresis platelets
<10 Non-immune thrombocytopenia and HLA-immunized
Transfuse 1 unit of HLA-matched apheresis platelets
<20 Non-immune thrombocytopenia and fever >38.5oC or coagulopathy
Transfuse 5 unit pool or 1 unit of apheresis platelets
<20 Procedures not associated with significant blood loss
Transfuse 5 unit pool or 1 unit of apheresis platelets
20-50 Procedures not associated with significant blood loss
Have pool of 5 units or 1 unit of apheresis platelets available, transfuse only if there is serious bleeding
33
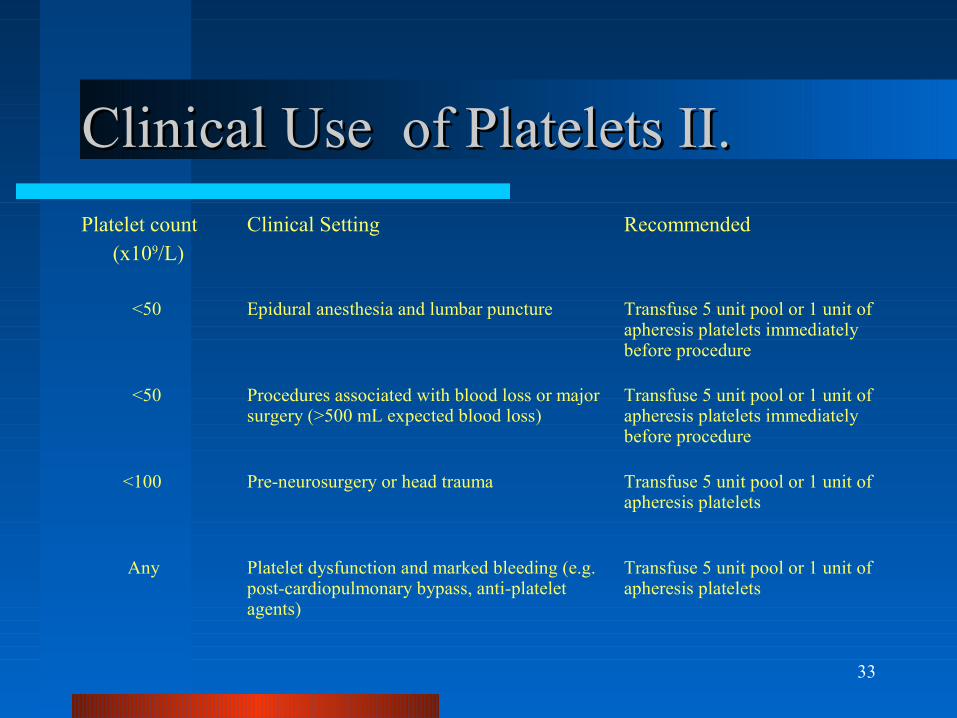
Clinical Use of Platelets II.Clinical Use of Platelets II.
Platelet count (x109/L)
Clinical Setting Recommended
<50 Epidural anesthesia and lumbar puncture Transfuse 5 unit pool or 1 unit of apheresis platelets immediately before procedure
<50 Procedures associated with blood loss or major surgery (>500 mL expected blood loss)
Transfuse 5 unit pool or 1 unit of apheresis platelets immediately before procedure
<100 Pre-neurosurgery or head trauma Transfuse 5 unit pool or 1 unit of apheresis platelets
Any Platelet dysfunction and marked bleeding (e.g. post-cardiopulmonary bypass, anti-platelet agents)
Transfuse 5 unit pool or 1 unit of apheresis platelets
34
Fresh Frozen PlasmaFresh Frozen Plasma
Fresh Frozen Plasma is a source of
clotting factors, with half lives in vivo
of between 6 hours & 3 days. Available in 2 forms:
250 mL recovered from regular donations 500 mL from apheresis donation
30 minutes required for thawing
35
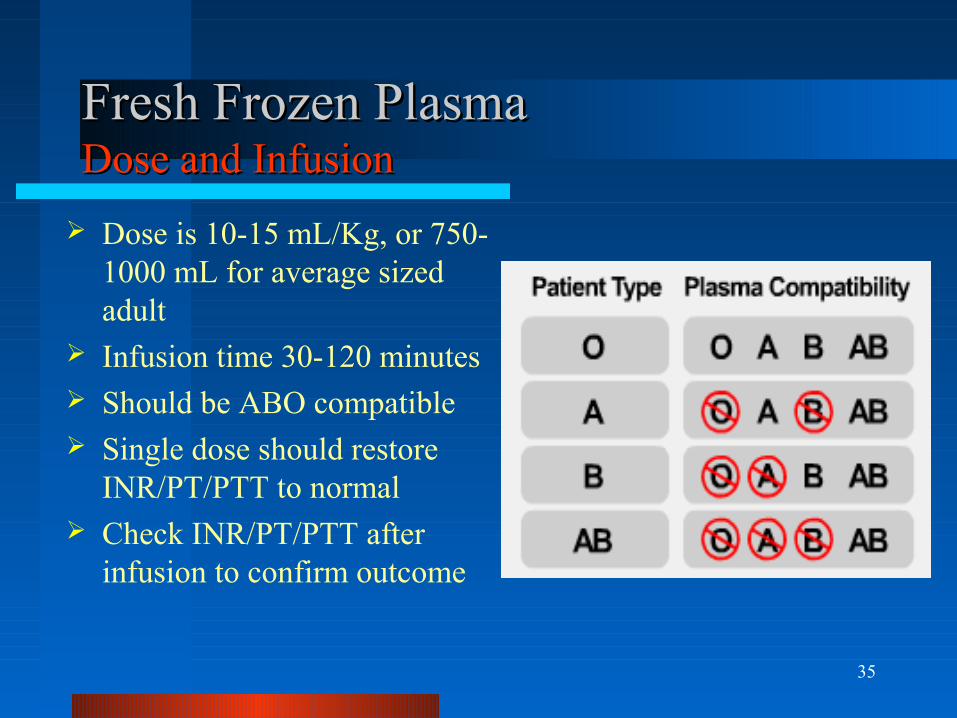
Fresh Frozen Plasma Fresh Frozen Plasma Dose and InfusionDose and Infusion
Dose is 10-15 mL/Kg, or 750-1000 mL for average sized adult
Infusion time 30-120 minutes Should be ABO compatible Single dose should restore
INR/PT/PTT to normal Check INR/PT/PTT after
infusion to confirm outcome
36
Reversal of Warfarin EffectReversal of Warfarin Effect
Warfarin effect can be reversed with vitamin K, 10 mg iv, and should be preferred to transfusion if time permits
If not, 750-1000 mL should be transfused
Expected result, INR/PT/PTT 1.5 x normal or less
Failure to get this result, re-consider diagnosis
Warfarin reversal effect
37
Misuse of Frozen Plasma - AuditMisuse of Frozen Plasma - Audit
CMAJ 2002; 166: 1539.CMAJ 2002; 166: 1539.
Almost half of 358 patients received FFP outside of guidelines– Appropriate 55%– Bleeding with INR<1.5 29%– Not bleeding 9%– INR not done 4%– Other 3%
38
CryoprecipitateCryoprecipitate
Cryoprecipitate containsFibrinogen – 250mgVon Willebrand FactorClotting Factor VIII (anti-hemophilic factor) – 80IU
1 unit per 8-10 Kg body weight, or 8-12 units for an average sized adult
Infusion time 10-30 minutes Each dose should raise fibrinogen by 500 mg/dL Check post-infusion fibrinogen level to confirm outcome
39
DoseDose
Fibrinogen dose = Fibrinogen increment x Plasma Volume/100/250
1 bag contains 250 mg/dL of fibrinogen
Cryoppt. dose) = factor VIII level increment x Plasma Volume/100/80
1 bag contains 80 IU of factor VIII
40
Clinical Use of CryoprecipitateClinical Use of Cryoprecipitate
Treatment of massive or microvascular bleeding with Fibrinogen < 1.0 g/L Status highly suggestive of hypofibrinogenemia without time for
laboratory confirmation Massive rapid defibrination in the obstetrical patient
Hereditary Disorders of Hemostasis For bleeding in von Willebrand’s syndrome patients ONLY if factor
concentrate is unavailable and DDAVP is ineffective
For the emergency management of factor VIII deficiency ONLY if manufactured factor VIII is unavailable
41
The end !!
Thank you