training and capacity development program to … and capacity development program to strengthen...
TRANSCRIPT

Draft before final consultation 1
Training and Capacity Development Program
to Strengthen Health Interventions in the
Pacific (SHIP)
Learn from work, at work, for work
Mahomed Patel National Centre for Epidemiology and Population Health
Research School of Population Health Australian National University
James Stuart
London School of Tropical Medicine and Hygiene & European Program for Interventional Epidemiology Training
United Kingdom
23 November 2013

Draft before final consultation 2
Table of Contents
1.0 Abbreviations and Acronyms .............................................................................................................. 3
2.0 Executive Summary ............................................................................................................................ 4
2.1 Mandate from Meetings of the Pacific Island Health Ministers ....................................................... 4
2.2 Program Goal and Purpose ............................................................................................................. 4
2.3 The challenge to integrate training and capacity development ....................................................... 4
2.4 Strengthening health interventions in the Pacific (SHIP) ................................................................. 5
3.0 Terms of Reference ............................................................................................................................ 5
4.0 THE MANDATE ................................................................................................................................... 6
4.1 Meetings of the Pacific Island Health Ministers............................................................................... 6
5.0 PROGRAM GOAL AND PURPOSE ......................................................................................................... 7
6.0 INTRODUCTION .................................................................................................................................. 8
6.1 Pacific Island Countries and Territories (PICTs) ............................................................................... 8
6.2 Pacific Regionalism ......................................................................................................................... 8
6.3 Secretariat of the Pacific Community (SPC) ..................................................................................... 8
6.4 WHO’s Division of Pacific Technical Support based in Suva, Fiji ....................................................... 9
6.5 The Pacific Public Health Surveillance Network (PPHSN) ................................................................. 9
6.6 Fiji National University’s College of Medicine, Nursing and Health Science (FNU) ......................... 10
6.7 Pacific Health Information Network (PHIN) ................................................................................... 10
6.9 PIHOA .......................................................................................................................................... 11
6.10 Building on the strengths of the development partners of the PPHSN .......................................... 11
7.0 SCOPE AND METHODS ..................................................................................................................... 12
8.0 FINDINGS ......................................................................................................................................... 13
8.1 Working definitions ...................................................................................................................... 13
8.2 Gaps and opportunities identified ................................................................................................ 15
8.3 Outcomes of the program: Strengthening Health Interventions in the Pacific (SHIP) ..................... 16
8.4 Theory of change: Integrating training with capacity development ............................................... 18
8.5 Options for study projects, classroom modules, trainees and trainers .......................................... 22
8.6 Intermediate program outcomes .................................................................................................. 25
8.7 Management structure, physical location and reporting requirements for full time-trainers and personal mentors ......................................................................................................................... 27
8.8 Management of the FETP trainers in the Indian Ocean ................................................................. 28
9.0 Monitoring and evaluation framework ............................................................................................. 28
10.0 GLOSSARY ........................................................................................................................................ 28
11.0 ANNEXES, for annexes 1 to 12, see separate issue ............................................................................ 29
Draft before final consultation 3
1.0 Abbreviations and Acronyms
AFD APSED
Agence française de développement Asia Pacific Strategy for Emerging Diseases
DDM Data for Decision-Making
EIS Epidemic Intelligence Service of US-CDC
EPIET European Program for Interventional Epidemiology Training
FETP Field Epidemiology Training Programs
FNU Fiji National University’s College of Medicine, Nursing and Health Science
IHR International Health Regulations (2005)
IOC Indian Ocean Commission
MAE Master of Applied Epidemiology Program, Australian National University
MDG Millennium Development Goals
NCD Non-communicable diseases
PIHOA Pacific Island Health Officers Association
PHD Public Health Division
PHIN Pacific Health Information Network
PICTs Pacific Island Countries and Territories
POLHN Pacific Open Learning Health Net of the WHO
PPHSN Pacific Public Health Surveillance Network
PPHSN-CB PPHSN-Coordinating Body
PRIPPP Pacific Regional Influenza Pandemic Preparedness Project
SHIP Strengthening Health Interventions in the Pacific
SPC Secretariat of the Pacific Community
TOC Theory of change
TPM Trainer and personal manager
USAPI United States Associated Pacific Island
US-CDC Centers for Disease Control, United States of America
WHO World Health Organisation
WHO EURO European Office of the WHO
WHO WPRO Western Pacific Regional Office of the WHO

Draft before final consultation 4
2.0 Executive Summary
2.1 Mandate from Meetings of the Pacific Island Health Ministers
Meetings of the Pacific Island Health Ministers in 2011 and 2013 acknowledged the weakness of staff in many countries to analyse, interpret and use health data effectively as an evidence-base for informing and evaluating policies, actions and programs. They called on regional development partners to help build training programs for all levels of the health workforce, and through this mechanism, to address a range of health priorities more effectively. These priorities included the need to renew commitments for supporting proven effective interventions against communicable diseases and for enabling development of the core capacities required to implement the International Health Regulations, to strengthen surveillance and response to the epidemic of the non-communicable diseases (NCDs), and to accelerate progress towards achieving the Millennium Development Goals (MDGs) 4 and 5 (Pacific strategy for scaling-up action on women’s and children’s health).
2.2 Program Goal and Purpose
The overall goal of the program is to improve population health outcomes in PICTs by increasing the effectiveness of essential public health services, and thus contribute to the vision of Healthy Islands Healthy People, the strategy for the SPC Public Health Division, 2013-2020.
The direct purpose of the program is to develop and implement a training program integrated with capacity development initiatives to strengthen public health interventions, actions and programs in PICTs.
This will be addressed through three broad strategies:
1. Assessing needs for training and capacity development to strengthen public health actions and programs in each PICT;
2. Identifying trainees and the study projects that they would design, develop and conduct, in order to strengthen public health actions and programs in each PICT;
3. Developing and implementing the curriculum including mechanisms identified to enable each trainee’s workplace to participate in, and learn and benefit directly from the study project.
2.3 The challenge to integrate training and capacity development
We identified two key challenges in designing and establishing a regional facility for training and capacity development in the Pacific. The first challenge was to integrate training with capacity development activities that could immediately strengthen public health actions and programs identified as priorities by individual Pacific Island Countries and Territories (PICTs). The second challenge was in establishing a regional facility that could coordinate and support training activities for all levels of the public health workforce.
We explored needs and priorities with senior public health decision-makers in PICTs and with development partners, and we developed a list of outcomes that are feasible in the Pacific context. We identified six desirable outcomes of the program:
1) graduates with specified competencies, as well as enhanced skills of their workplace team members; 2) effective responses to public health emergencies; 3) achievement of local and national IHR core capacities, 4) strengthening of other public health actions and programs; 5) building the knowledge-base for enhancing health outcomes; and 6) extended local, national, regional and global partnerships and networking.
We identified gaps and opportunities to be addressed by the program across a range of the essential public health functions (or operations), including needs identified at the Meetings of the Pacific Island Health Ministers. They included:

Draft before final consultation 5
1) the domains of communicable diseases consistent with IHR requirements as well as the epidemic-prone and endemic diseases not directly related to the IHR but identified as priorities by the country;
2) the NCDs; 3) activities to help accelerate progress to achieving MDG 4 and 5 (related to child health and maternal
and reproductive health), 4) environmental health, particularly water and sanitation.
The broader and important generic need was to strengthen management of health information systems, including data analysis and interpretation to provide the evidence-base for informing and evaluating public health actions, policies and programs.
2.4 Strengthening health interventions in the Pacific (SHIP)
The program will address the gaps and priorities identified by establishing a regional entity that will integrate training with capacity development in a way similar to that used in the FETP models that have been adopted in over 50 countries and regions around the globe. The entity will employ three full time trainers/personal mentors, harness the strengths and activities of development partners, build on the achievements of the Pacific Public Health Surveillance Network (PPHSN), and draw on the experience and support of the Field Epidemiology Training Programs (FETPs).
Trainees will include up to eight ‘fellows’ who will be enrolled to study and work full-time in their home-country over a period of two years, akin to the classical two-year FETP model. They will be expected to complete four study projects (see below) identified as priorities by senior national decision-makers. The projects should adhere to a specified standard that will be awarded a master level qualification by the FNU. However because of the demand for alternative shorter-term courses, part-time trainees will also be enrolled, and be expected to work on at least one of the study projects at a time in their home country for about 1-2 days per week. The training support will be through classroom-based modules followed by intensive in-country support to complete study projects for both groups of trainees. Six classroom modules will be delivered as three double modules over fifteen consecutive days at 3-4 month intervals in each twelve month period. Collectively these modules will cover the knowledge and the skills required to carry out the core public health operations of assessment, policy and planning, assurance. Each of the four first modules will be followed by a study project related to the following topics:
1) an emergency public health response (e.g. to a disease outbreak or natural or other disaster); 2) analysis of a database of a surveillance or other health information system, 3) establishment or evaluation of a surveillance or other health information system, or of a health
intervention program 4) an epidemiological study on operational research.
The workplaces of each trainee will be prepared and supported to provide an enabling environment for the trainees to conduct their study projects and to transfer their new knowledge and skills. The workplace team members will be encouraged to participate in the project and be beneficiaries of the program. Transfer of knowledge to, and active engagement of the workplace teams in the project will help generate performance results for the workplace and help develop individual and institutional capacity.
3.0 Terms of Reference
The feasibility study was funded by Agence française de développement (AFD), and the Terms of Reference for the feasibility study are to advise on developing capacity of the Pacific Public Health Surveillance Network (PPHSN) to train public health professionals in ways that can simultaneously help strengthen delivery of essential public health operations in PICTs as well as enhance regional coordination in responding to public health emergencies. Specifically to:
1. Develop regional capacities to train public health professionals in field epidemiology.

Draft before final consultation 6
2. Provide support to strengthen essential public health services in PICT members of SPC and PPHSN. 3. Sustainably improve PPHSN technical services and regional coordination during crisis situations by
developing a network of field epidemiologists in the Pacific, trained in the same good practices.
4.0 THE MANDATE
4.1 Meetings of the Pacific Island Health Ministers
The Meetings of the Pacific Island Health Ministers and long endorsed the activities of the Pacific Public Health Surveillance Network (PPHSN) and encouraged the network’s ongoing in-country and regional support systems based on training and capacity development initiatives to strengthen surveillance and responses to communicable disease threats. The activities of PPHSN were critical in enabling effective preparedness for the pandemic spread of SARS (severe acute respiratory syndrome) in 2003, for the anticipated influenza pandemic through the AusAID supported Pacific Regional Influenza Pandemic Preparedness Project (PRIPPP) and the response to pandemic influenza (H1N1), as well as to recent outbreaks of dengue and chikungunya infections.
Recent meetings of the Health Ministers acknowledged the challenges of responding to the triple burden of communicable diseases, non-communicable diseases (NCDs) and the health impacts of climate change. They noted the weakness of health staff in many Pacific Island Countries and Territories (PICTs) to analyse, interpret and use health data as an evidence-base for informing, implementing and evaluating public health policies, actions and programs. They therefore called on the assistance of existing coordinating and capacity-building mechanisms such as PIHOA, PHIN and the PPHSN, and of regional development partners to build training programs for all levels of the health workforce in ways that would strengthen their performance to address national and regional health priorities more effectively1. These priorities included the need to renew commitment for supporting proven effective interventions against communicable diseases, for supporting the development of the national core capacities required to implement the International Health Regulations (IHR) and the related Asia Pacific Strategy for Emerging Diseases (APSED), to strengthen surveillance and response for the epidemic of the non-communicable diseases (NCDs), to accelerate progress towards achieving the Millennium Development Goals (MDGs) 4 and 5 (Pacific strategy for scaling-up action on women’s and children’s health), and to act on the social determinants of health.
In response, the 18th meeting of the PPHSN-Coordinating Body (PPHSN-CB)2 in May 2012 approved the SPC, the Focal Point of the PPHSN-CB, to commission a study for assessing the feasibility of establishing a training and capacity development program in the Pacific to be modelled on the Field Epidemiology Training Program (FETP). The latter has been adopted in over 50 countries and regions across the world since the late 1970s, and is based on the highly successful model of competency-based training in public health that was initiated as the Epidemic Intelligence Service at the Centers for Disease Control in the USA (US-CDC) in the early 1950s. The PICT representatives attending the IHR meeting that followed immediately after the PPHSN-CB meeting supported and approved the need for the present study3.
1 “There is currently no single programme to systematically strengthen surveillance in the region. There is a need to strengthen both in-country and regional surveillance and response. This can be achieved through the full use of existing coordination and capacity-building mechanisms (e.g. PPHSN, PHIN, PIHOA), and full adoption of regional initiatives such as the Pacific Syndromic Surveillance System. Regional development partners can help to improve communications between countries, particularly in areas such as the International Health Regulations (2005) and health statistics. “, Honiara Outcome, Ninth Meeting of Ministers of Health for the Pacific Island Countries, WHO/SPC, June 2011. 2 As at November 2013, members of the PPHSN-CB are representatives of 7 PICTs (Cook Islands, Nauru, New Caledonia, Palau, Papua New Guinea, Tonga, and Vanuatu) and the following development partners:, WHO, Pacific Island Health Officers Association (PIHOA), Fiji National University/College of Medicine, Nursing and Health Sciences, the US Centers for Disease Control (CDC) in Hawaii, and the SPC which serves as the Focal Point of the PPHSN-CB. 3 International Health Regulations and PPHSN Meeting, Nandi, Fiji, 30 May – 1 June 2012.
Draft before final consultation 7
5.0 PROGRAM GOAL AND PURPOSE
The overall goal of the program is to improve population health outcomes in PICTs by increasing the effectiveness of essential public health services, and thus contribute to the vision of Healthy Islands Healthy People (Annex 1).
The direct purpose of the program is to develop and implement a training program integrated with capacity development initiatives to strengthen public health interventions, actions and programs in PICTs.
This will be addressed through three broad strategies:
4. Assessing needs for training and capacity development to strengthen public health actions and programs in each PICT;
5. Identifying trainees and the study projects that they would design, develop and conduct, in order to strengthen public health actions and programs in each PICT;
6. Developing and implementing the curriculum including mechanisms identified to enable each trainee’s workplace to participate in, and learn and benefit directly from the study project.
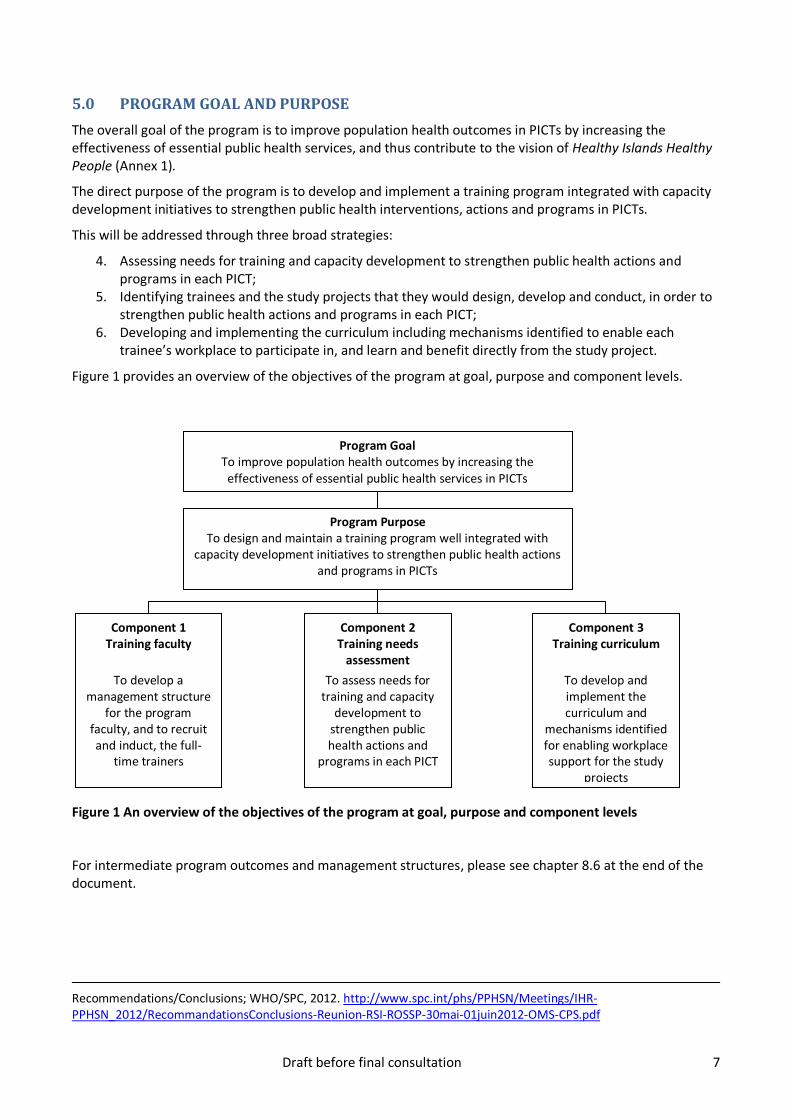
Figure 1 provides an overview of the objectives of the program at goal, purpose and component levels.
Figure 1 An overview of the objectives of the program at goal, purpose and component levels
For intermediate program outcomes and management structures, please see chapter 8.6 at the end of the document.
Recommendations/Conclusions; WHO/SPC, 2012. http://www.spc.int/phs/PPHSN/Meetings/IHR-PPHSN_2012/RecommandationsConclusions-Reunion-RSI-ROSSP-30mai-01juin2012-OMS-CPS.pdf
Program Goal To improve population health outcomes by increasing the
effectiveness of essential public health services in PICTs
Program Purpose To design and maintain a training program well integrated with
capacity development initiatives to strengthen public health actions and programs in PICTs
Component 2 Training needs
assessment
To assess needs for training and capacity
development to strengthen public health actions and
programs in each PICT
Component 3 Training curriculum
To develop and implement the curriculum and
mechanisms identified for enabling workplace support for the study
projects
Component 1 Training faculty
To develop a
management structure for the program
faculty, and to recruit and induct, the full-
time trainers

Draft before final consultation 8
6.0 INTRODUCTION
6.1 Pacific Island Countries and Territories (PICTs)
The Pacific Islands region is vast; while there are considerable differences across the region in culture, population size and economic characteristics, most PICTs face similar challenges. These include geographic Isolation, small and at times dispersed populations, rapid population growth in some countries, and high vulnerability to the impacts of climate change and natural disasters, and to economic shocks such as fluctuating international fuel and food prices. These challenges are exacerbated by constraints in the health workforce, and therefore in their ability to deliver effective essential public health functions.
With the support of the PPHSN, PICTs were able to prepare for and respond to global public health emergencies such as SARS (Severe Acute Respiratory Syndrome), pandemic influenza and more recently, to outbreaks of dengue and chikungunya fever. The current key challenge is to respond more effectively to both the epidemic prone and endemic communicable diseases, as well as to develop the core competencies needed to implement the IHR (2005). Thirteen PICTs are State Parties to IHR. By June 2012, six of these State Parties reported achieving these core capacities, while seven requested a two-year extension and assistance from development partners to meet these obligations.
Beyond communicable diseases the PICT are experiencing the double burden of Non-communicable diseases. The high burden of NCDs now calls for immediate and more broad-based public health actions is the epidemic of the NCDs. The social and economic costs of NCD’s have escalated particularly rapidly in the Polynesian and Micronesian countries, and are increasing in the Melanesian countries that continue to experience the high burden of communicable diseases. An added challenge is that some PICTs appear to be falling short in attaining the targets for MDGs 4, 5 and 6 (child health, maternal and reproductive health, and the communicable diseases respectively).
6.2 Pacific Regionalism
The Pacific Plan for Strengthening Regional Cooperation and Integration (2005) is the fundamental document underpinning Pacific regionalism. The Plan stipulates three related facets: regional cooperation, regional provision of public goods and services, and regional integration. While regional approaches help supplement local capacity, they do not impose a ‘one-size-fits-all’ model of regionalism, and allow for countries in the region to continue pursuing their own nationally based policies. Of particular importance in this context are the three principles for providing regional public goods:
1) alignment of development support with broader government health programs; 2) adherence to the principle of subsidiarity, i.e. regional program should not have a role where action
can be taken most efficiently and effectively at the national level; 3) ensuring consistency with principles and practices of development effectiveness – ownership,
alignment, harmonization across development partners, working for results, and mutual accountability.
6.3 Secretariat of the Pacific Community (SPC)
Two sections with the SPC are of immediate relevance to training and capacity development programs in population and health related fields: the Public Health Division (PHD) and the Statistics for Development Division (SDD).
Public Health Division
Healthy Islands – Healthy People is the strategic plan of the PHD for the decade 2013–2022. It is consistent with three key development outcomes identified by SPC members: sustainable economic development,

Draft before final consultation 9
sustainable human and social development and sustainable natural resource and environmental management and development.
The plan outlines PHD’s strategic direction, priorities and outcomes and how it intends to achieve them. It focuses on two main areas: building national capacity to deliver core public health functions, and providing selected regional public goods in health. The latter are defined as ‘public health services that are most effectively and efficiently provided through cooperation and collective action by two or more countries, realising economies of scale and/or better results’. The three priority work areas will be: prevention and control of NCDs, communicable disease surveillance and response, and prevention and control sexually transmissible infections, including HIV/AIDS.
The Statistics for Development Division
The Statistics for Development Division (SDD) of the SPC conducts five-yearly demographic health surveys (DHS) in collaboration with each PICT. The surveys include key indicators to measure progress towards achieving the MDG, as well as key public health indicators. The five yearly DHS highlights key findings in each PICT, and additionally provides a ‘Policy Note’ on the implications of the findings for national policies and programs. The SDD provides technical assistance to countries in the region for their 5-10 yearly censuses and vital statistics systems.
The SDD trains national staff in conducting and analysing these surveys, and provides opportunities to complete training fellowships at their offices in Noumea. Public health practitioners also require core skills in the collection, analysis and interpretation of these data, and in using them to inform and evaluate public health policies and programs. The proposed training program should build on the experience and capacity within SDD and integrate its classroom and in-country training activities.
6.4 WHO’s Division of Pacific Technical Support based in Suva, Fiji
The Multi-Country Cooperation Strategy for the Pacific (2013–2017) was launched in September 2012 as the guiding framework for coordination between WHO and countries to meet national health goals. The strategy identifies health and development challenges and priorities in the Pacific and establishes an overall strategic direction and approach for overcoming the challenges and achieving national goals. It includes specific strategies for each of the 21 PICTs, with a synopsis of country health plans and WHO’s role in those plans; it identifies the following five priority areas:
reducing maternal and child morbidity and mortality;
reducing morbidity and mortality from sexually transmitted infections, HIV, tuberculosis, malaria and neglected tropical diseases;
reducing morbidity, premature death and disabilities from NCDs;
reducing mortality due to epidemics, disasters and the health impact of environmental threats and climate change; and
universal access to essential health services and products and sustainable health care.
6.5 The Pacific Public Health Surveillance Network (PPHSN)
The PPHSN was established in 1996 under the auspices of SPC, WHO and the PICTs. Its goal was to strengthen disease surveillance and the timely detection and response to disease outbreaks at the national and regional levels. The network has provided rapid access to five key support systems for the PICTS:
PacNet (1997) is the electronic forum for communications and outbreak alert, and early result of the activities was the collaborative development of guidelines and manuals for surveillance preparedness and outbreak response.

Draft before final consultation 10
LabNet (2000) offers PICTs access to reference laboratories for the identification and/or confirmation of pathogens for which they PICT may not have diagnostic capacity.
EpiNet (2001) was established as the network of the national response teams that were identified by each PICT; the team consists at least of a clinician, a laboratory scientist and an epidemiologist responsible for outbreak and emergency preparedness and response.
PICNet (Pacific Infection Control Network) (2006) was established for developing uniform surveillance and control systems for infections transmitted in health care facilities. This initiative was further reinforced by the Pacific Regional Influenza Pandemic Preparedness Project (PRIPPP); PICNet activities slowed down when the PRIPPP ended in June 2011 but are currently reinvigorated due to the ongoing threat of infections potentially transmitted in health care facilities (e.g. vector-borne diseases, antibiotic resistant bacterial infections).
The Pacific Syndromic Surveillance System (2010) is the latest initiative established in 2010 for the early detection of outbreaks.
The last available strategic plan of the PPHSN (2003-6) is shown in Annex 2. The development milestones of the PPPHSN over its first decade since formation are shown in Annex 3a. Annex 3b lists the key publications in ‘Inform’ACTION’, the regional bulletin published three times each year, and the PPHSN contributions through three special supplements of the Pacific Health Dialog (Journal of Community Health and Clinical Medicine for the Pacific Region produced with the assistance of Massey University and the Fiji School of Medicine).
In responding to the call of the Meetings of Pacific Health Ministers for development partners to help build training and capacity development, the PPHSN’s activities will need to extend beyond the control of communicable diseases to encompass a broader focus on the essential public health services; this will require a review of the governance and coordinating mechanisms of the PPHSN, as well as the need to develop a strategic work-plan consistent with the overall needs and priorities of the PICTs.
6.6 Fiji National University’s College of Medicine, Nursing and Health Science (FNU)
FNU had offered classroom-based training in public health for many years. However, over the last decade, FNU has taken a very flexible approach by responding to country’s requests to convene, support and accredit field-based training including outreach programs. The training is accredited with a variety of qualifications ranging from certificates to diplomas, bachelor and master level degrees. In addition, FNU has delivered several distance learning modules that included direct in-country support for designing, developing, implementing and reporting on public health studies. Three of the FNU programs are of immediate interest: the ‘Data for Decision-Making’ model and training in operational research (Annex 4a and 4b respectively), and training in analyzing data from health information systems.
6.7 Pacific Health Information Network (PHIN)
AusAID’s Knowledge Hub for Health Information Systems (HIS) developed a training package for managing HIS including analyzing and interpreting the data. The package was transferred to the FNU for implementation in collaboration with the Pacific Health Information Network. PHIN has developed a Regional Health Information Systems Strategic Plan (2012- 2017) that provides a framework for action to support HIS professionals achieve better health outcomes. In endorsing the six-year regional plan, HIS professionals, development partners, technical agencies and institutions recognised the urgent need to effectively address HIS issues and challenges in the region (a sentiment endorsed at the 9th Health Ministers Meeting held in Honiara in June 2011) and tasked the PHIN Implementation Working Group, with the support of and WHO - Western Pacific Regional Office (WPRO), with developing a detailed Implementation Plan to operationalise the Strategic Plan. It will therefore be important that training initiatives in HIS being proposed through this feasibility study are developed in collaboration with the PHIN Implementation
Draft before final consultation 11
Working Group to avoid any possible duplication or competition.
6.8 The United States Centre for Disease Control (US-CDC) and TEPHINET
The US-CDC with its home base in Atlanta, Georgia, developed the first model of field-based training in epidemiology through the highly successful Epidemic Intelligence Service (EIS) in 1951. Since the late 1970s, the US-CDC has worked with foreign ministries of health to establish this model of training referred to as the Field Epidemiology Training Program (FETP) around the world (Annex 6 and 7). US- CDC helped establish 50 FETP covering about 80 countries; collectively they have produced over 2,800 graduates and over 80% of them work in government in their home countries. As of February 2013, the US-CDC was supporting workforce development in 46 countries, including the placement of a full-time, in-country Resident Advisor for twenty one two-year FETPs serving 33 countries, and for three programs that are less than two years in length. The US-CDC has teams of physicians, epidemiologists, public health advisors, instructional designers, health communication specialists readily available to support workforce development and to provide general programmatic advice and support to foreign Ministries of Health.
Since 2008, the US-CDC’s Task Force for Global Health has been the focal point of the Training Programs in Epidemiology and Public Health Interventions Network (TEPHINET), a professional alliance of the FETPs. TEPHINET was founded in June 1997 with support from WHO, CDC and the Fondation Merieux (France). The network serves as a common ground for information exchange between FETP as well as with US-CDC and WHO, to facilitate and support development of training and research projects in epidemiology and public health, and to promote surveillance of communicable and non-communicable diseases. It convenes an annual scientific conference where FETP trainees and graduates have the opportunity to present their work; it also provides an ideal venue for trainees, graduates and staff to extend and strengthen their global networking. TEPHINET will soon have an accrediting body for its FETP membership, and the program being proposed for the Pacific is expected to adhere to these standards of accreditation and apply for membership of the network.
The Hawaii office of the US-CDC is a development partner and member of the PPHSN-CB, and has specified delegations in the USAPI. Staffs are active participants in training activities as well in emergency response and other support activities in USAPI, and in other PICTs.
6.9 PIHOA
The Pacific Island Health Officers Association (PIHOA) is a non-profit organization that is led by and represents the collective interests of the Ministers, Secretaries, and Directors of Health of the U.S.-Affiliated Pacific Islands (USAPI). PIHOA's mission is to improve the health and well-being of USAPI communities by providing, through consensus, a unified credible voice on health issues of regional significance. PIHOA enhances sharing of resource, information, and human expertise to support health improvements in the region; this includes health policy development, knowledge dissemination, communication enhancements, health services, research, continuing health professional development, quality assurance, and cooperative networking inside and outside the Pacific Basin.
PIHOA’s Strategic Plan 2013-17 is shown in Annex 5. Among the objectives priorities are to ”Support priority cost effective interventions, monitor their implementation and expand the evidence base through research and surveillance [and to] support local capacity to develop & use data to support policy”.
6.10 Building on the strengths of the development partners of the PPHSN
All development partners have conducted and continue to conduct a range of training programs to strengthen diverse aspects of public health services delivery and capacity in the region. Training is offered by the partners collaboratively, typically through the PPHSN, but also through bilateral and other multilateral

Draft before final consultation 12
arrangements. Of these, the training models of particular relevance to this feasibility study were:
1) The Field Epidemiology Training model being conducted by WHO and US-CDC in Papua New Guinea (March to November 2013), Cambodia and Laos (Annex 6a, b and c respectively),
2) PPHSN’s ‘Data for Decision Making’ (DDM) model (conducted between 2005 and 2009) (Annex 4a), 3) The operational research training model conducted by SPC and its international partners (2011-13)
(Annex 4b).
A summary of how these three programs are conducted, their duration and expected outcomes are summarized in Annex 6. We drew on the inputs, processes, outputs and outcomes defined for these programs, as well as on the FETP models adopted throughout the world (refer to summary in Annex 7a, b and c), to develop the first draft outcomes and the theory of change for the program in the Pacific. The final list of outcomes was subsequently revised to address the needs and priorities identified by PPHSN development partners and PICT representatives.
An additional highly relevant regional training program is WHO’s Pacific Open Learning Health Net (POLHN) implemented in partnership with PICTs and the FNU. POLHN is a unique facility offering a blended approach of on-line and face-to-face learning for health professionals. It is run through over 40 learning centres in the region, each providing networked computers with internet access, printer, scanner, data projector and educational materials in digital and print form. Health staff can enroll in one or more of self-paced courses, as well as get sponsorship for flexible learning courses that are accredited through the Fiji National University and the Pacific Paramedical Training Centre. Of particular relevance to public health are the materials offered for postgraduate courses in epidemiology, health research, health services management and public health. The URL for viewing details on POLHN and the range of courses offered are listed in Annex 8. Many of the courses will be relevant for the proposed training and capacity development program. The program should closely collaborate with POLHN in curriculum development as well as to identify mechanisms for the program’s new trainees to utilize the training materials and POLHN facilities. The support of POHLN will complement and supplement the knowledge and skills needed for participants enrolled in the SHIP program.
Development partners of the PPHSN have played a central role in supporting countries strengthen the surveillance and control of communicable diseases. This was achieved through engaging experienced technical staff of the partners through bilateral as well as multilateral mechanisms. Collectively, they have designed, developed, planned, implemented and evaluated a broad range training and capacity development in responding to country needs and priorities.
The most recent and impressive example of collaboration between the development partners was the planning, delivery and evaluation of the classroom training on syndromic surveillance and outbreak response in two settings: at the USAPI EpiNet workshop in Guam in August 2013, and in Kiribati in October 2013, both conducted in collaboration with staff from the University of Newcastle (Australia). Although follow-up support of participants to apply the new knowledge and skills was not planned before the workshop, all facilitators responded enthusiastically to requests by the trainees for ongoing support to either initiate or complete study projects at their workplace. The experience and lessons learned from these workshop have been carefully recorded, and will make an invaluable contribution for strengthening this model of training and support.
There is now the need for development partners to collaborate in the spirit of the PPHSN and extend their support to help address the challenges of NCDs, and more generally, to strengthen essential public health services by supporting public health policies policy development, actions and programs in the PICTs.
7.0 SCOPE AND METHODS
Our first task in this study was to develop working definitions of three key concepts used in the Terms of Reference of this study through a literature review: ‘field epidemiology’, ‘essential public health functions’ and ‘capacity development’. This was essential to develop a common understanding on what capacities were

Draft before final consultation 13
to be targeted for development.
Our second task was to explore needs and priorities for training and capacity development expressed by senior public health decision-makers in PICTs, by representatives of the PPHSN-CB’s five Allied members, development partners and through interviews of the 24 trainees who participated in the USAPI EpiNet workshop on syndromic surveillance in Guam in August 2013.
The third task was to identify a list of outcomes that were feasible in the context of the PICTs. These were identified through a review of publications on the FETPs, our knowledge through engagement with FETPS around the world and the personal experiences of the two consultants as faculty members of the FETPs in Australia (the MAE Program) and in Europe (EPIET).These outcomes were reviewed and revised based on the results of the above interviews.
The final task was to develop a Theory of Change for relating the desired outcomes with appropriate and feasible training and capacity development activities, and using this information to craft the purpose, objectives and activities of the program.
8.0 FINDINGS
8.1 Working definitions
Field epidemiology
‘Field epidemiology’ is defined in the Dictionary of Epidemiology4, citing Gregg5 as:
‘the practice of epidemiology in the field - in the community, commonly in a public health service (i.e. a unit of government or a closely allied institution). Field epidemiology is how epidemics and outbreaks are investigated, and it is a tool for implementing measures to protect and improve the health of the public. Field epidemiologists must deal with unexpected, sometimes urgent problems that demand immediate solution’.
Field epidemiology is one of a range of tools and techniques needed to inform public health policies, actions, and programs. The Field Epidemiology Training Program (FETP) model has now been adopted in over fifty countries and regions around the world. A central attribute of this model is the way it partners and complements health department initiatives to enhance workforce skills, health system performance and the evidence-base for policies, programs and practice. In this model, short-term training courses in the classroom are followed by intensive mentoring support to trainees for designing and conducting study projects considered important by senior national health decision makers. The study findings are then used by trainees and their local supervisors to inform public health policies, actions and programs. Over a two-year period of the classical FETP model, classroom courses usually takes up 10-30% of the duration of the training, while the time dedicated to conducting study project in the field takes up the remaining 70-90% of the duration of training. The major public health domain covered by the FETPs have been in surveillance and response to communicable diseases, but have increasingly addressed other areas such as NCDs, injuries, environmental and occupational health and maternal and child health.
The cornerstone of the approach to training is the intensive mentoring support provided to trainees for conducting the study projects. Details of the models and how they are implemented in various countries and regions are shown in Annex 6 and 7.
Because of the relatively small size of the populations and public health workforce in the PICTs, individual staff members often wear ‘multiple hats’; they combine responsibilities of collecting and collating epidemiological data with the responsibility of interpreting the data to inform policies and programs, as well as for planning, implementing, monitoring, and evaluating the actions. The same individual or team is usually also responsible for the various public health domains, e.g. communicable diseases, non-communicable
4 A dictionary of epidemiology. Edited for the International Epidemiological Association by Miquel Port. 5th Ed. 2008 5 Field Epidemiology. Edited by Michael B Gregg. 3
rd Ed. Oxford University Press. 2008
Draft before final consultation 14
diseases, maternal and child health and environmental health. For this reason, the same individuals and teams have to be supported to strengthen their performance across multiple essential public health operations.
Essential public health operations
The potential scope of training and capacity development could be extremely broad when considering public health is defined as “the science and art of preventing disease, prolonging life and promoting health through the organized efforts of society”. Several conceptual models have been proposed to identify the functions through which the health sector contributes to the goals of public health. These functions (or operations) can be defined as a group of related services through which public health actions and programs are identified, formulated, implemented, monitored and evaluated. (WHO EURO has referred to these functions as ‘operations’ to emphasise the action-oriented nature of these essential functions/services).
Identifying these essential public health operations for the Pacific context are important for framing the scope of training and capacity development activities the program could address in the Pacific. For the purpose of this feasibility study, we drew on the essential operations proposed recently by WHO EURO
1. Surveillance of diseases and assessment of the population’s health. These include:
Surveillance in the area of civil registration (births and deaths);
Surveillance systems and disease registries in the areas of: communicable diseases, non-communicable diseases, maternal and child health, environmental health, social and mental health, occupational health and injury; and
Repeated surveys of health status and health behavior. 2. Systems and procedure for identifying priority health problems and health hazards such as detection
of outbreaks and environmental and workplace hazards. 3. Preparedness for managing public health emergencies. 4. Health protection which incorporates risk detection and assessments, and actions needed to ensure
environmental, occupational, food safety. 5. Primary and secondary disease prevention for communicable and non-communicable diseases and
injuries. 6. Health promotion to enable people to increase control of their health and its determinants and
thereby improve it. 7. Assuring a competent public health workforce. 8. Core governance, financing and quality assurance procedures for health policy planning and
implementation. 9. Core communications for public health aimed at improving the health literacy and status of
individuals and populations (incorporates education, media advocacy, and risk and crisis communications).
10. Research to inform policy development and service delivery.
Public health practitioners require three core public health skills to carry out these operations:
Assessment, or the ability to identify, define and prioritise public health challenges and needs systematically.
Policy development and planning to formulate appropriate solutions, i.e. public health actions and programs.
Assurance to ensure solutions are implemented, monitored and evaluated. The evaluation leads into the phase of assessing the extent to which public health needs and challenges had been addressed.
A senior public health practitioner requires all these skills to perform effectively. By contrast, junior level practitioners can function effectively by focusing on a selected subset of these functions/operations depending on the tasks defined in their job descriptions.
Draft before final consultation 15
The training and capacity development program should therefore offer a range of modules in ways that could address both the needs of senior as well as junior staff to perform tasks defined at their level of performance/proficiency.
Capacity development
Of the many definitions of capacity development, the following is applied in the context of this study: the combination of attributes and efforts needed to nurture, enhance and utilize the skills capabilities and assets of people and institutions at all levels of the health system – individual, workplace, organizational, national and regional – so that they can better deliver essential public health operation for improving population health outcomes.
Applying a systems approach to capacity development reveals that training individuals to accomplishing specific public health tasks is just one component of capacity development. It was therefore essential to detail how the program would use training as leverage to shift system behaviour and in this way strengthen individual and collective workplace capacity to develop and strengthen public health actions.
8.2 Gaps and opportunities identified
Based on discussions with development partners, senior decision-makers of PICTs and trainees who participated in the USAPI EpiNet workshop in Guam (August 2013), gaps and opportunities for the program were identified in the following domains of public health practice:
Communicable diseases:
o Achieving the core capacities required to implement the IHR/APSED: national coordination, surveillance, risk assessment, preparedness, rapid response, risk communications, and laboratory services.
o Activities to meet MDG 6 related to HIV/AIDS, tuberculosis and malaria. While the Global Fund supports training projects in many PICTs, they are not sustainable and have not been integrated with other more general training activities such as for management of surveillance and health information systems, and monitoring and evaluation of disease control programs;
o epidemic prone disease not covered by the IHR such as food and water-borne and vector-borne diseases; surveillance and control of these diseases are priority for adaptation to climate change;
o vaccine preventable disease, particularly those for which vaccines have become available in recent years against rotavirus, Haemophilus influenza b, pneumococcal disease and, human papilloma virus (HPV);
o The neglected tropical diseases such as leptospirosis, filariasis and leprosy.
NCDs: plans are being developed for comprehensive training in the surveillance and control of NCDs. However, as public health staffs in most countries are responsible for the surveillance and control of both communicable as well as NCDs, training for them should be integrated into a common package.
MDG 4 (child health) and MDG 5 (maternal and reproductive health). MDG performance across the region is mixed and generally weakest among the Melanesian while most Micronesian countries struggle to maintain some gains. The Polynesian countries which all started from a much higher base level, have been performing relatively well.
Environmental health, particularly water & sanitation
Individual PICTs vary in the specific public health domains they identified as priorities for training and capacity development through this program. For this reason the options listed above should be kept open so that each PICT has the opportunity to select priority areas for developing their programs.

Draft before final consultation 16
This list is not exhaustive and can be modified as the program develops.
The range of tasks that staff in small, intermediate-sized and large countries should be able to complete in addressing the essential public health operations are listed for consideration by the PPHSN-CB in Annex 9.
8.3 Outcomes of the program: Strengthening Health Interventions in the Pacific (SHIP)
Based on the gaps and opportunities identified, the purpose of the program would be to support countries strengthen the essential public health operations identified as their priorities. Because of this focus the program will extend beyond skilling people in applying the tools and techniques offered by field epidemiology, and include methods for strengthening the delivery of a broad range of essential public health services. It is for this reason that the title suggested for the program by a group of interviewees as the program to ‘Strengthen Health Interventions in the Pacific’ (SHIP).
Figure 2 shows a boat metaphor to illustrate the main outcomes of the training and capacity development program.
Figure 2: A boat metaphor is used to illustrate the main outcomes of the training program.
The outcomes of the program were identified at the individual, the workplace/national, as well as at the regional/global levels. These three levels correspond with workforce development, strengthened delivery of essential public health services consistent with national priorities, and networking regionally and globally respectively.
The extent to which each of these outcomes are realized in a particular PICT will depend on the aspirations expressed by the senior national decision-maker: they will identify the trainees and workplaces as well as priority study projects trainees will conduct and that will ideally align with the national health, strategic or operational plans.
Partnerships, networks and sharing of knowledge provide the sail that takes SHIP across and beyond the Pacific
The strength and competence of the workforce combined with the ability to respond to emergencies reflect the quality and design of SHIP
The balance of program content is the outrigger that keeps SHIP stable
The priorities of SHIP in each country are reflected in the direction of rudder

Draft before final consultation 17
The priorities of SHIP in each country are reflected in the direction of rudder
The six key outcomes are:
1. Development of a competent public health workforce
This outcome relates to the professional development of individual trainees, the co-workers with whom they share their new knowledge and skills and who contribute to their study projects, and other health professionals contributing to, and gaining from their study projects:
Individual trainees develop competencies to perform tasks consistent with their workplace functions and responsibilities. Through their activities, they contribute to Outcomes 2 to 6 below, as well as to the professional development of workplace colleagues.
Local (in-country) line managers or (supervisors) benefit by sharing the new knowledge and skills of trainees, and by contributing to trainees’ study projects.
Other health professionals, by collaborating in trainees’ study projects, gain from, and contribute directly to, the more effective functioning of health services. This group includes workplace colleagues, public health staff beyond the latter group, as well as clinicians (doctors, nurses and infection control staff in hospitals, primary health care practitioners), laboratory scientists, environmental health staff and Animal Health professionals.
All levels of health staff participating or collaborating in trainee’s study projects, where appropriate, may claim credits towards meeting their ‘Continuing Professional Development’ requirements for renewing their professional practice licenses (in countries where these are required, e.g. in Fiji).
2. Achievement of the core capacities required to implement the IHR/APSED at the local, national and regional levels; the core capacities include those related to national coordination of activities, planning, implementing, coordinating and evaluating preparedness, emergency response and surveillance systems across all levels of the health system, risk communication and workforce development.
3. Effective responses to public health emergencies at the local, national and/or regional levels. The emergencies include disease outbreaks, natural disasters, chemical accidents and threats to food safety. The lessons learned from these responses will be incorporated as part of a continuous quality improvement plan to strengthen systems of preparedness, surveillance and response as listed under Outcomes 2.
The strength and competence of the workforce combined with the ability to respond to emergencies reflect the quality and design of SHIP
4. Strengthening other public health actions and programs. This outcome refers to both the generic functions across public health services as well as to requirements for the more specialised public health services.
Skills needed to implement the generic functions include:
• to identify, define and prioritise public health risks, problems and needs; • to collate, analyse and interpret data from vital registrations (population census, births and
deaths); • to collate, analyse and interpret data from diverse health information systems, such as for
health care attendances, disease registers, environmental health surveys, demographic health surveys, reproductive health information system, and vaccination registers;
• to design, conduct and report on studies that inform, evaluate and/or provide the evidence-base for public health actions, policies, programs and public health practice;

Draft before final consultation 18
• to implement, monitor and evaluate disease prevention and control programs (e.g. for NCDs, programs on vaccinations, vector control, food safety, water and sanitation).
Specialized services that may be the subject of study projects could include:
• surveillance and control of communicable disease (emerging, epidemic-prone, endemic and neglected tropical diseases);
• surveillance and control of NCD’s; • environmental health; • mental health • occupational health; • maternal and reproductive health; and • child health, including school health services.
The balance of program content is the outrigger that keeps SHIP stable
5. Building the global knowledge base for enhancing health outcomes by sharing findings and lessons learned from trainees’ projects with the local community, and health professionals at national, regional and global level. Wherever possible, study findings are presented at scientific conferences, and published in newsletters/journals such as Pacific Health Dialog, Inform’ACTION, Western Pacific Surveillance and Response Journal (WPSAR, a WPRO’s publication) and/or other international peer-reviewed journals.
6. Extended local, national, regional & global interactions, partnerships and networking are generated by the above activities, enhancing collaborative learning to strengthen the performance and outcomes of public health services.
Partnerships, networks and sharing of knowledge provide the sail that takes SHIP across and beyond the Pacific
8.4 Theory of change: Integrating training with capacity development
How can we structure training activities so that it can simultaneously strengthen public health actions and programs and contribute to capacity development in a sustainable manner?
The ultimate objective of training individuals is to help improve performance of the public health workforce in ways that strengthen public health actions and programs. Individuals operate within a workplace, and workplaces operate within the broader health system. Capacity development is fundamentally about the dynamics of change and transformation of actors at all these levels of the health system – at individual, workplace, institutional and national levels. Therefore, training has to be used as a key point of leverage to shift system behaviour if it is to contribute to capacity development.
We developed a theory of change (TOC) to articulate the program logic and explain how training will impact immediately as well as in the longer term on strengthening public health actions and programs. We first identified the outcomes expected of program (described under ‘Outcomes of the program’ above), and then tracked backward to identify the series of changes (or pre-conditions) needed to achieve these outcomes. The TOC is summarized in figure 2.
1. The senior national decision-makers identify trainees (i.e. full-time, so-called “fellows” and/or part-time trainees) who will be trained and supported to complete selected study projects. These projects will be related to the training module being offered (e.g. the data analysis module); they will be selected based on needs that align with priorities identified in the national health plan or strategic plan, and are likely to generate the outcomes listed under ‘Outcomes of the program’ above. The resources for conducting the study are estimated, and mechanisms for mobilizing these are explored. These are explored with the

Draft before final consultation 19
senior national decision maker. Full-time fellows will be sponsored by the SHIP Programme. For other study resources, options could include self-funding (costs affordable by the PICT), funding already secured through a related national, bilateral or multi-lateral initiative, or a funding proposal to be prepared as part of the study project.
2. The curriculum will be developed as six modules (refer to the section on ‘Modules’ below) for enabling trainees to acquire the ‘domain-specific’ (or technical) knowledge and skills needed to carry out the essential public health operations, i.e. assessment, policy development and planning, and assurance. The detailed content of each module will be developed for the full program once the full-time trainers/mentors are appointed. A training needs assessment in collaboration with senior national decision-makers in each PICT, will be conducted by SPC and/or other development partners to ensure the training support for trainees from each PICT is customised to national priorities. The classroom curriculum will be delivered using a variety of active learning methods consistent with the principles of adult learning (Annex 10).
3. Trainees participate in the regional, two-week classroom training module. By the end of the module, the trainee develops the study proposal and presents it to the class to invite comments and suggestions for strengthening the proposal. The outputs expected from the study will be a systematic description and analysis of the issue/problem and a set of recommendations to address the public health need or problem. In this way, trainees develop the confidence and commitment to proceed with the study at the workplace.
4. On returning home, the trainee presents the proposal to the line supervisor and workplace team with the following objectives:
a. To clarify and emphasise the outcomes expected of the study, how it would benefit the local supervisor and workplace team, and how it would help strengthen public health actions and programs and ultimately local and national public health capacity.
b. to invite feedback from workplace team members for further strengthening the study proposal, and exploring how they could participate in, learn from, and contribute to, the study;
c. to get agreement with the team on the time and resources required for completing the project successfully.
d. For the line supervisor to offer encouragement, regular feedback, incentives and rewards for progress. The latter may include opportunities to present papers at international conferences, to participate in emergency responses in other countries, to participate in short term projects in offices of regional agencies such as SPC and WHO.
5. The trainee conducts the study over a specified period, say 6 or 9 months. The local supervisor ensures the workplace support is fully enabled. The personal mentor (full-time TPM appointed by the program) provides technical guidance and support for achieving learning and performance outcomes by communicating with the trainee through at least one on-site visit and fortnightly communications by phone, Skype and/or emails. It is possible that in some cases the mentor role may be delegated to another experienced epidemiologist in the country or from a regional partner agency, for example as part of a bilateral project being conducted by SPC or WHO. The trainee is given the option to enrol in an appropriate POLHN on-line module as a supplementary learning activity.
6. Through these processes, the trainee develops the domain-general (or soft skills) that complement the technical skills; the soft skills essential for public health include working collaboratively, advocating for public health, providing leadership and working with communities.
Steps 7 and 8 are not shown in figure 3 because they are iterations of the classroom – workplace support cycle to complete the study project.
7. Trainees return to the classroom to present their study findings and recommendations, and discuss and invite suggestions for enhancing their report. This provides an opportunity to reflect on and revise their report, consolidate their knowledge and skills, and identify and share lessons learned about conducting public health studies. Trainees then participate in a module that supports them to develop a logic model

Draft before final consultation 20
for resourcing, planning and implementing the study recommendations. Recommendations are reviewed applying criteria of effectiveness, affordability, feasibility, cost effectiveness, acceptability and equity. The logic model elaborates on the goals, objectives, outputs as well as verifiable indicators for monitoring and evaluation, and to the risk assessment and management framework for implementing the actions.
8. Trainees then return home to implement, monitor and evaluate the plan, once again enabling the workplace support and transferring knowledge and skills to local workplace team as described under 4 above. In this way trainees develop the competencies for strengthening public health actions and programs, while they contribute simultaneously to achieving other program outcomes (listed above).
9. Trainees write up the study to standards required for accreditation by the FNU; this standard will, in turn, depend on the level of experience and qualifications of the trainee, and the level of qualification, e.g. certificate, diploma or degree-level.
10. The trainee will be supported to present the study at scientific conferences, and prepare them for and appropriate publication such as Pacific Health Dialog, Inform’ACTION, WPSAR (WHO WPRO publication) and other international peer-reviewed journals.

Draft before final consultation 21
Figure 3: Learning at work, from work for work and the theory of change to explain the activities required to achieve the outcomes of the program.
Classroom module Curriculum based on skills needed to achieve workplace performance
outcomes
Learning Outcomes Domain-specific knowledge & skills
Confidence and commitment to perform effectively at the workplace
Workplace support
Local supervisor
Defines the outcomes expected of study project
Provides opportunities and resources to conduct projects
Offers encouragement, regular feedback, incentives and rewards
Workplace team members
Participate as co-learners and team members in study projects
Personal mentors
Provide intensive technical guidance and support for achieving learning and performance outcomes
How trainees will learn from work, at work, for work
Successful application and transfer of knowledge and skills through study
projects that also helps develop collective workplace capabilities
Development of domain-general skills needed in public health to work
collaboratively, advocate for public health, provide leadership, and work
with communities
Workplace performance outcomes
Effective delivery of essential public health services to strengthen actions and
programs (Trainee’s study report is documented to
a specified accreditation standard)
These outcomes (as identified by senior national decision-maker) will inform
curriculum development and objectives of the workplace support system
Societal outcomes
Improved population health
The needs to improve population health outcomes should be used to determine the expected workplace performance outcomes

Draft before final consultation 22
8.5 Options for study projects, classroom modules, trainees and trainers
Details on the scheduling of modules, the number of trainees per module and the number of study projects that the TPMs will be supervising in any particular month are summarised in the attached Excel spreadsheet (Annex 12).
Study projects
The classroom training modules and workplace support system are structured to help trainees develop and conduct the study projects in their home country. The project is aimed at a particular set of public health actions and programs, and that nurture competencies related to each of the three core functions of public health i.e. assessment, policy development and planning, and assurance.
Each fellow will complete at least one study project related to each of the following topics (i.e. at least 4 study projects altogether), while part-time trainees will complete only one or some, but not all projects:
1. An emergency public health response (e.g. to a disease outbreak or natural or other disaster). 2. Analysis of a database of a surveillance or other health information system. 3. Establish or evaluate a surveillance or other health information system, or a public health
intervention program. 4. An epidemiological study on operational or implementation research
In general studies will be aimed at strengthening public health actions and programs, and be of a standard acceptable for accreditation through the FNU.
Reports will be communicated to decision-makers and the public, and wherever possible, presented at international conferences and/or published in international journals
Modules
Six classroom modules will be conducted each twelve month period. Because of the high travel cost, the six modules will be delivered as three double modules over fifteen consecutive days at 3-4 month intervals. In this way travel cost for the trainers and the fellows can be reduced to three instead of six return trips from their home base each year.
Collectively the modules will cover the knowledge and the skills required to carry out the core public health operations of assessment, policy, planning, and assurance.
Box 1 outlines the structure and content of the modules and the number of days devoted to the respective topics. The following section describes how fellows and part-time trainees will complete their training and assignments.
Each of the first four modules will be systematically followed by developing a proposal for the related project, both for fellows and part-time trainees. While each module focuses on a particular set of public health topics, two to three days are set aside in each module either to support trainees prepare their proposal for their study project (at the end of that module), or for trainees to present their project in the classroom for review (immediately before the module).
Fellows will attend modules 1-6 in the first year, and then assist with teaching of modules in the second year. They will also be expected to attend one project review and presentation review in the second year. Part-time trainees will attend one module of their choice that is related to the study project to be conducted in their home country. Part-time trainees wanting to attend a second module can only do so after they have successfully completed the first study project.

Draft before final consultation 23
Box 1: Structure of the modules (number of days for the topic
Module 1. Public health priorities in the Pacific (2 days); preparing and responding to public health emergencies, including developing a project outline (5).
Module 2. Surveillance systems and data analysis (5); Proposal writing (3)
Module 3. Project review (2); Establishing, managing, and evaluating surveillance systems (4) plus project proposal (1)
Module 4. Epidemiological methods for operational research (5); Proposal writing (3)
Module 5. Project review (2); Influencing decision makers and strengthening public health actions and programs and risk communications (5)
Module 6. Scientific and oral communications (5); Presentation review (for fellows) or Proposal writing (for part-time trainees (3)
Trainees
The level of staff eligible for training and the tasks for which they will requires specified sets of competencies are shown in Annex 11. Three categories of trainees will attend the classroom modules:
a) Full time trainees (or fellows) will be enrolled in the program for two years, as in the classical FETP model. They will complete the six modules in one year and over the two years, complete the four studies as described under ‘Study Projects’ above. Fellows will work full-time on the projects in their home country.
b) Part time trainees will enrol in one module and follow this with a field project to be conducted over six to nine months (for the first four modules). They will work part-time in their home country, e.g. one to two days per week depending on the agreement made before enrolment into the program.
c) Participants who attend the module as part of their in-service training and who are not expected to follow through with a study project.
Each fellow and part-time trainee will have a line manager who is their country supervisor and will be assigned one of the TPMs for direct mentoring. Additional Project supervisors with expertise in the chosen project topic can be assigned with agreement of the country supervisor and coordinator. Such Project supervisors should primarily be drawn from regional expert resources, especially calling on the 5 PPHSN-CB Allied members, and/or on further PPHSN Allied Members. Would the appropriate expertise not be available within the PPHSN resources, other partnership could then be explore (e.g. academic institutions, research institutes non-yet affiliated with PPHSN)
An appropriate form of accreditation will be offered by FNU for successful completion of a study project. Arrangement for the FNU accreditation will need to be formalised; the Dean of FNU has agreed in principle that they will support accreditation for these training activities providing they meet the usual FNU requirements.
Completion of all six modules and four projects will be considered for a master degree accreditation. Completion of at least one module and one study project will be offered accreditation according to the pre-training qualifications, the quality of a project, and the number of study projects completed. As an example, this could be a certificate for one project, and a post-graduate certificate or diploma, or a Bachelor’s degree could be considered for completing more than one project. Once again, requirements for accreditation will have to be negotiated with FNU in all instances.

Draft before final consultation 24
Trainers/Personal mentors
We recommend three full time trainers/personal mentors (TPM) who will be employed in a full-time capacity to convene and conduct the training for classroom modules, as well as to act as personal mentors for the study projects. We consider three to be the minimum number given the extent and complexity of running a program across so many countries, and to provide intensive support for up to 20 trainees who may be conducting a study project in their home country. According on the option selected, this equates to up to 13-16 trainees per TPM (refer to Excel spreadsheet in Annex 12).
While the lead TPM will be based with SPC in Noumea, there are advantages in having the second TPM based in Fiji to link in with WHO and FNU. The third TPM could be based in either of these two countries or in one of the USAPI. The options for their management structure are discussed under Component 1 of the Program goals and purpose below. In order to accommodate the participation of the French speaking PICTs, the lead TPM will need to be fluent in both French and English.
Options on number of trainees
Eight options on numbers of full-time (fellows) and part-time trainees are shown as examples in the attached Excel spreadsheet (Annex 12). The examples are then used to estimate the total number of study projects for which the TPMs will have to provide intensive mentoring.
We recommend a cohort of 8 fellows who will be enrolled for two years as full-time trainees in the program; they will complete four study projects over the two years.
In options 3, 4, 5 and 6, we show the implication for the TPMs to support 8 part time trainees in each module who will complete follow-up study projects. In options 7 and 8, we show the implications for supporting 4 part-time trainees.
The options in Box 2 show the implications of choosing sequential or overlapping cohorts of fellows. In sequential cohorts, each new cohort starts every two years as the previous one finishes, whereas in sequential cohorts, a new cohort starts each year.
Recommendation: Options 1 &2 are not preferred as they only allow training of full-time fellows. Based on models from other FETPs, the trainee/TPM ratios in Options 3-6 are not within a range that can be expected to offer sufficient TPM support; they could, however easily be accommodated with the assistance of 3-5 additional Project supervisors, as discussed above, especially for mentoring part-time trainees. The range of 8-10 trainees per TPM in Options 7&8 is consistent with that seen in other FETPs. Overlapping cohorts are preferred, if resources permit, as this will lead to more rapid capacity and network building. We therefore recommend that strong consideration is given to Option 8.

Draft before final consultation 25
Box 2 Options on number of trainees, full-time fellows and part-time trainees
Number of fellows Number of part-time trainees
Ratio of trainees per Trainer/Personal Mentor
Option 1 8 every 2 years Nil 3-6
Option 2 8 every year Nil 3-6
Option 3 8 every 2 years 8 from year 2 onward 2- 3 trainees –Yr 1
Reaching to 13-16 from Yr 2 onward
Option 4 8 every year 8 from year 2 onward 2- 3 trainees –Yr 1
Reaching to 13-16 from Yr 2 onward
Option 5 8 every 2 years 8 from year 1 onward 13 trainees –Yr 1
Reaching 13-16 from Yr 2 onward
Option 6 8 every year 8 from year 1 onward 13 trainees –Yr 1
Reaching 13-16 from Yr 2 onward
Option 7 8 every 2 years 4 from year 1 onward Reaching 8-10 from yr 2 onward
Option 8 8 every year 4 from year 1 onward Reaching 8-10 from yr 2 onward
8.6 Intermediate program outcomes
The intermediate outcomes are described in terms of the objectives defined for the three components of the program presented in the beginning of the document (refer to page 8 “Program role and purpose”): 1) Training faculty 2) Training needs assessment, 3) Curriculum delivery.
Component 1: Training faculty
Objective 1: To develop a management structure for the three full time Trainers and Personal Mentors (TPMs), and to recruit them into the program
Intermediate outcome 1.1: Management structure, physical location and reporting requirements for full time-trainers and personal mentors (TPMs) established
Activities:
SPC should consider the options listed below (at the end of this section on ‘Immediate program outcomes’) to select what is most appropriate for the program.
Intermediate outcome 1.2: Three TPMs appointed to the program
Activities:
Apply the usual SPC requirements for recruiting and employing trainers

Draft before final consultation 26
Of the three trainers one will be appointed as a lead trainer. At least two of the three TPM should have a track record in the Pacific. The lead TPM should have experience and track record in setting up a similar program of training and capacity development and be fluent in both French and English.
Intermediate outcome 1.3: Induction plan for TPMs developed and implemented
Activities:
Develop agreement on how the TPM will engage and relate to each of the development partners.
Develop a tool for assessing needs for training and capacity development in each PICT.
Develop a draft curriculum for the six classroom modules.
Negotiate with FNU for university accreditation of fellows and part-time trainees.
Component 2: Training needs assessment
Objective 2: To assess needs for training and capacity development to strengthen public health actions and programs in each PICT
Intermediate outcome 2.1: Needs for training and capacity development identified with each PICT.
Activities:
Training needs assessment tool piloted, and data collected through a visit to each PICT.
Data from each PICT collated and analyzed.
Intermediate outcome 2.2: Fellows and part-time trainees to be enrolled for training from each PICT, their study projects and workplace support system.
Activities:
In collaboration with senior decision makers and country supervisor
Identify fellows and part-time trainees, their study projects and expected study outcomes.
Develop workplace support system to enable trainees to complete the project successfully, as well as methods to monitor and evaluate the support.
Intermediate outcome 2.3: Results of needs assessment and topics of study projects used to update training curriculum.
Activities:
Collate data from PICTs to update classroom curriculum.
Use information on each workplace support system to customize personal mentoring process for each trainee.
Component 3: Curriculum delivery
Objective 3: To implement the curriculum and enable mechanisms for in-country support to trainees’ study projects
Intermediate outcome 3.1: Schedule of modules and number of fellows and part-time trainees finalized for year 1.
Activities:
Collate data from outcomes of component 2 above.
Draft before final consultation 27
Intermediate outcome 3.2: List of projects, expected outcomes, responsibilities of each TPM finalized for year 1.
Activities:
Delegate a TPM for each trainee
Explore and arrange potential support for trainee that could be complemented or supplemented by an experienced epidemiologist/public health practitioner from a development agency, if appropriate (i.e. as previously so-called Project supervisor)
8.7 Management structure, physical location and reporting requirements for full time-trainers and personal mentors
The consultants do not have strong preference for one option over the other. The two key options are for the TPMs to be employed and managed by SPC as are other staff members, or to be employed by the SPC/PPHSN through an independent contractor. It is possible there may be further options.
Management by SPC
Strengths:
SPC has a broad mandate, membership and experience to provide, coordinate and drive development initiatives across PICTs.
SPC is in a prime position to understand both the national priorities and issues around strengthening essential public health services
SPC’s mandate and expertise overlaps with the TOR of this feasibility study, i.e. the need for the program to support countries to strengthen essential public health services, and to help strengthen regional coordination of emergency responses.
Potential challenges/concerns
PPHSN development partners may view the program as belonging to SPC rather than a regionally coordinated entity.
If TPMs are based at other locations eg Fiji, they may be “taken over” by the institutions in which they are based, with a risk of fragmentation of the training program coordination
Management by an independent contractor (e.g. Indian Ocean FETP hereunder)
Strengths:
An independent contractor would act under the direction of SPC and be accountable to SPC (refer to the arrangement of the FETP based in the Indian Ocean Commission (below).
The TPMs would be seen as truly independent and less susceptible to political influences.
The contracting agency could bring in a broad range of external expertise and support
Potential challenges/concerns
Potential for ‘external interference’ in regional dynamics particularly if the agency does not have expertise/first-hand experience with work, politics and dynamics in the region.
An external contractor accountable for the development and delivery of curriculum and training support will require a direct contractual and management relationship with SPC - so there is the potential for duplication in transaction costs and activities.

Draft before final consultation 28
8.8 Management of the FETP trainers in the Indian Ocean
The co-ordination of the Indian Ocean FETP is run by an external body, Epiconcept, which is linked to the Indian Ocean Commission (IOC) by a contract of services as prime contractor under the direction of the IOC. Technical support staffs including the FETP coordinators are available to the IOC and effectively work as staff of the IOC (not of Epiconcept).
Epiconcept’s senior staff and consultants can be involved as experts at the request of the IOC and in accordance with the terms of reference of the contract. EpiConcept staffs are therefore well integrated into the IOC.
The advantage for the IOC is that it has the necessary expertise on hand to carry out the coordination and supervision of the FETP and can also count on additional expertise (laboratory, IT, animal health ) whenever needed without having to go through a bidding process. This type of operation may be compatible with the operations of the SPC. SPC could draw up a contract with a provider for long-term and short-term technical assistance with the TPMs being positioned within the public health department of the SPC under the authority of the SPC Director.
9.0 Monitoring and evaluation framework
A detailed monitoring and evaluation framework should be developed with verifiable indictors based on the Theory of Change detailed above.
10.0 GLOSSARY
Capacity development is the combination of attributes (individual competencies, collective capabilities, assets and relationships) and efforts needed to nurture, enhance and utilize the skills and capabilities of people and institutions at all levels – locally, nationally, regionally and internationally – so that they can better progress towards sustainable development. When capacity development is successful, the result is more effective people and institutions better able to provide products and services on a sustainable basis. Capacity development is fundamentally about the dynamics of change and transformation of all the actors – at individual, organizational, sector-wide and societal levels. It encompasses a hierarchy of levels (individual, organizational, network/sectoral and the overall enabling environment) and to be successful, capacity-building efforts must respond to the relationship among these levels, all of which are systemically interlinked. These levels are interdependent.
Collective capability – the broad range of collective skills of organizations or systems needed to carry out a particular function or process. It is what enables an organization to do things and sustain itself. Capabilities can be understood as the building blocks of an organization’s overall capacity to perform.
A competency is defined as the “a cluster of related knowledge, skills, attitudes and behaviors that reflects a major portion of one's job, that correlates with performance on the job, that can be measured with well-accepted standards, and that can be improved with training and development”. A competency cannot be acquired only through classroom training/learning. To acquire a competency, the learner has to be motivated and supported to apply and experiment with the newly acquired knowledge and skills at the workplace, as outlined in figure 1; this approach is consistent with the current requirements for receiving FNU accreditation for the DDM modules.
Impacts are the long-term societal results of a project or program. Impacts typically refer to goal attainment and are sometimes referred to as higher-level outcomes.
Knowledge is a familiarity with someone or something, which can include facts, information, descriptions, or skills acquired through experience or education. It can refer to the theoretical or practical understanding of a subject. It can be implicit (as with practical skill or expertise) or explicit (as with the theoretical understanding of a subject). Knowledge acquisition involves complex cognitive processes: perception, communication, association and reasoning

Draft before final consultation 29
Outputs are the products produced as a result of a project’s activities, e.g. the number and type of training activities.
Outcomes are the effect or result of activities and outputs at the institutional or organizational level; they reflect uptake, adoption, or use of outputs by those who are supposed to benefit from the project. Outcomes are what things are changed because of the project or program.
Public health is the science and art of preventing disease, prolonging life and promoting health through the organized efforts of society.
Public health functions (or operations) are defined as any of a group of related activities or duties contributing to public health. (The term ‘operation’ was used by EURO-WHO to emphasize the action-oriented nature of these essential functions.
Skills are defined as proficiencies needed to carry out a group of functions (or operations) for achieving specified results, and that are acquired or developed through training or experience. Skills can often be divided into domain-specific (or technical) skills and domain-general (or soft) skills. In the context of public health, the former refers to the set of skills required to carry out the the core public health operations:
‘Assessment’, or the ability to identify, define and prioritise public health challenges and needs systematically.
‘Policy development and planning’ to formulate appropriate solutions, i.e. public health interventions, actions and programs.
‘Assurance’ to ensure these solutions are implemented, monitored and evaluated. The evaluation leads into the phase of assessing the extent to which public health needs and challenges had been addressed.
The domain-general (or soft skills) complement the technical skills required for the tasks and for many other activities; in public health they include specifically skills needed to work collaboratively, advocate for public health, provide leadership and work with communities.
System is an entity that maintains its existence and functions as a whole through the interrelationships of its parts or elements. The systems perspective would hold that no single factor or constituent element – incentives, financial support, trained staff, knowledge, structure – will by itself be an explanation for the development of capacity. Thus single interventions, e.g. training, are not likely to make a significant difference to system behaviour unless they represent a key point of leverage that can shift system behaviour.
11.0 ANNEXES, for annexes 1 to 12, see separate issue