trabeculectomy with releasable page 229 - dos · pdf file · 2017-10-11of...
TRANSCRIPT

477DOS Times - Vol. 12, No. 6 December, 2006
Editor-in-chief
EDITORIAL 483
MEDICAL OPHTHALMOLOGYComprehensive Strategies for Macular Edema 485Harsha Bhattacharjee MS, Lokesh Jain MS,Debdulal Chakraborty DNB
Management Strategies in ChildhoodGlaucoma 494Abhishek B. Dagar MS, DNB, FICO, FPOS
Amblyopia 498Archana Gupta, Suma Ganesh MS,Manish Sharma MS, Sandeep Buttan
OPHTHALMIC TECHNIQUESMastering Scleral indentation 506Manisha Agarwal1 MS, Anuj Gogi, J.S. Guha MS
OPHTHALMIC PROCEDURESICG -Indocyanine Green Angiography 511Sanjeev Gupta MD, Amit Khosla MD
CASE REPORTCarotid Cavernous Fistula: A case report 521Harbansh Lal MS, Anita Sethi MD, FRCS,Shakir Hussain MD, DM, FINR, Shilpa Taneja DNB
HARDWARE HINTSAutorefraction 527Archana Sood MS
PEEP IN THE PASTA peep in the past: Allvar Gullstrand 535Lt. Col. Rakesh Maggon, Col. J.K.S. Parihar,Lt. Col. Vijay Mathur
COLUMNSLife Membership Form 545Abstract Form 551AIOS Membership Form 553
TEARSHEETD/D of posterior segment causes of poor visualgain after uneventful cataract extraction 561Sanjay Ahuja MD
Trabeculectomy with Releasable...Page 229

DOS Times - Vol. 12, No. 6December, 2006 478
Dear friends & colleagues
As winter sets in, its time to turn the heat on to continuing medicaleducation and conferences. Advances in technology and communicationhave made it possible to be at par with the west in terms of the latestinnovations in the field. In fact India is well on its way to be a globalsuper power, especially in technology related fields and medicine. We areproud that many of our ophthalmologists have achieved internationalrecognition and need to work together to make ophthalmology in Indiathe best in the world!
The ophthalmological societies, both at the state level and at the national level, are one wayof collectively working for the betterment of Indian ophthalmology. We should all try toparticipate and contribute in all the programmes, be it workshops, conferences or meetings. Tothis end we, the DOS executive, have been working hard to create programmes and newsletterswhich include both the basics and the recent advancements in ophthalmology to benefit boththe students and the practitioners. The enthusiastic participation and response from all of youcontinues to encourage us and we look forward to further strengthening our society by theinduction of new members and addition of newer ideas.
The parent body of all our societies is the All India Ophthalmological Society. This societyhas been the pioneer for all academic activities in our country. The annual conference has grownin leaps and bounds and now is truly world class with an attendance of around 4000 delegates,the best of national and international faculty and wonderful trade. This is one common arenafor people of all sub-specialities, and from all over the country to exchange thoughts and ideas,and is a great learning experience. We would request all of you to join the society and participatewhole-heartedly in all the programmes. For this purpose we are printing AIOS membershipform in this issue of DOS Times.
Though the AIOS and DOS conference are quite close, one should attend both as there is alot to be gained. Apart from one’s own specialty one should be aware of the advancements inother parts of the field as now the patients too, having internet access, demand “multifocalIOLs”, “Avastin injections”, Medpor implants etc! Even if one is not doing the procedures atleast we should be able to correctly guide the patients. We have invited faculty from all overIndia to participate in the DOS annual conference and for those of you who haven’t seen theFaculty topic form on the website, we have enclosed one in this issue. Those desirous ofparticipating in the conference can submit the forms and we will try to include them in theprogramme. Wishing you all Happy New Year and hope to see you in Hyderabad in Februaryand in New Delhi in April.
With best wishes.
Thanking you.Dr. Harbansh Lal
Secretary, DOS
EDITORIAL
Dr. Harbansh Lal

479DOS Times - Vol. 12, No. 6 December, 2006
Comprehensive Strategies for Macular EdemaHarsha Bhattacharjee MS, Lokesh Jain MS, Debdulal Chakraborty DNB
Sri Sankaradeva Nethralaya,Beltola, GuwahatiAssam
Macular edema is defined as retinal thickening fromaccumulation of fluid within 1 Disc diameter of the macula.It may be focal, diffuse or cystic and is characterized byextracellular accumulation of fluid, specifically in Henle’slayer and the inner nuclear layer of retina. Macular edemais a common cause of visual loss in a wide variety of ocularconditions. It is a non specific pathologic response to thedisruption to the normal permeability barrier that protectsthe retina.
Vogt first described the existence of microcyst at maculain 1918 using an ophthalmoscope with red-freeillumination. Friedenwald used the slit lamp to make thisobservation in 1929. Bangerte in 1945 emphasized thatmacular edema is not an uncommon condition which canbe detected early by slit lamp biomicroscopy. Irvinedescribed the association of macula edema followingcataract exraction.
Molecular and cellular alterations leading to macularedema
The breakdown of the blood-retinal barrier seems tobe the most important mechanism in explaining theextravasation of fluid although similar changes to theretinal blood flow may play a role. The blood retinal barrierconsists of the retinal pigment epithelium layer (outerblood retinal barrier) and the vascular endothelium (innerblood retinal barrier) that prohibit the passage ofmacromolecules and circulating cells from the vascularcompartment to the extracellular and therefore intraretinalspace.
In general, an increase in passive permeability throughthe endothelium can occur via three general mechanisms:
dysfunction of the intercellular junctionsincreased transcellular transportincreased endothelial cell destructionFluid homeostasis and endothelial permeability are
mostly regulated by intercellular junctions in the non-diseased retina. The inflammatory agents increasepermeability by binding to specific receptors thattransduce intercellular signals, which in turn causecystoskeletal reorganization widening of interendothelialclefts. Once leukocytes have adhered to the endothelium, a
coordinated opening of interendothelial cell junctionsoccurs.
Another important factor that is involved in theregulation of the of fluid homeostasis is the active cellulartransport of nutrients and fluid via pinocytosis. It isunclear how the molecular factors involved in pinocyticfluid transport are influenced by disease process.
Blood-retinal barrier breakdown is at least in part dueto endothelial cell damage and apoptosis. The proapoptoticmolecule Fas-ligand (FasL) induces apoptosis in cells thatcarry its receptor Fas (CD95).
Among the growth factors involved VascularEndothelial Growth Factor(VEGF) plays a dominant roleas a mediator of vascular leakage.
Metabolic alterations have a causal role in diabeticmaculopathy but also in inherited diseases such as theautosomal dominant form of macular edema or macularedema in retinitis pigmentosa. Furthermore, ischaemia ofthe inner or outer blood-retinal barrier leads to macularedema. Decreased perfusion of the retinal capillaries is seen,e. g. in vein occlusion and diabetic retinopathy, whereasischaemia along with decreased perfusion of the choroidwith associated serous retinal detachment occurs in severehypertensive retinopathy, in eclampsia or in rheumatoiddisorders. Following retinal vascular occlusion theintravascular pressure increases and leads to dysfunctionof the blood-retinal barrier.
Similarly, hydrostatic forces are effective in arterialhypertension or in eyes with low intraocular pressure andmay cause fluid accumulation in the macula. Mechanicaltraction such as in epiretinal membranes or invitreomacular traction syndromes promotes macularedema by physical forces.
Inflammation apparently plays a role in intermediateuveitis, postoperative cystoid macular edema (Irvine-Gasssyndrome), diabetic macular edema and various forms ofchoroidal inflammatory diseases including Vogt-Koyanagi-Harada syndrome and birdshot retino-choroidopathy. All prostaglandin-like pharmacologicalagents, even if applied topically, can induce macular edemavia a cytokine response similar to inflammatoryconditions.
DiagnosisDirect Ophthalmoscopy provides high magnification but
does not allow for stereoscopic visualization.Indirect Ophthalmoscopy provides an overall view of the
MEDICAL OPHTHALMOLOGY

DOS Times - Vol. 12, No. 6December, 2006 480
posterior pole and periphery and helps in detecting areasof extramacular thickening.
Biomicroscopic slit-lamp examination with fundus contactlens is of particular value in demonstrating even very mildcystic macular edema, as well as in identifying contributingdisease such as diabetic retinopathy or epiretinalmembrane
Biomicroscopy with the 78 and 90 diopter lenses can alsobe effectively used to diagnose subtle cystoid edema usingthe technique of light scattering. (Figure 1)
Fluorescein angiography: It is an essential tool in theevaluation of macular edema. In the normal eye, with anintact blood-retinal barrier, there is no detectable leakageof Fluorescein into the retina. Disruption of the blood-retinal barrier results in a variety of characteristicangiographic patterns of dye leakage that are oftendiagnostic of a particular retinal vascular disease. (Figure2and 3)
Hiedelberg Retina Angiograph 2:It is a confocal laserscanning system for digital fluorescein and indocyaningreen angiography. The size of field of view can be set to15x15, 20x20 and 30x30 degrees and provides highresolution and good view of macula. (Figure 4and 5)
Vitreous fluorometry: It quantitates fluorescein leakageusing a slit-lamp fluorophotometer, a techniquepopularized by Cunha-Vaz et al. In the normal eye onlysmall amounts of fluorescein enter the vitreous, but withdisruption of the blood-retinal barrier, increased fluoresceininto the vitreous leakage can be detected.
Optical coherence tomography (OCT) & Retinal thicknessanalysis (RTA): These provide objectiveand quantitative measures of retinalthickness. Although vascular leakageas demonstrated by fluoresceinangiography is important in theevaluation of CME, visual losscorrelate more reliably with thedegree of macular thickening thanwith the amount of macular leakageseen in fluorescein angiography. Boththese techniques use the projection of
a laser slit beam onto the retina with differential analysisof the reflected light yielding a high-resolution, cross-sectional image of the retina. Macular edema ischaracterized by localized accumulation of the fluid in theretina with an accompanying increase in retinal thickness.Retinal thickness analysis has the added advantage ofproviding multiple parallel cross-sectional images of theretina in a time interval sufficiently short to avoid motionartifacts, thereby allowing a three-dimensionalreconstruction of the retina. OCT is useful in documentinganatomic features of the vitreous and the retina, especiallyat the vitreoretinal interface.
Role of OCT in diabetic macular edemaDefining the disease pattern: Diabetic macular edema has
5 distinct patterns that can be defined on OCT alone. Theseare:1. Sponge- like retinal thickness2. Cystoid macular edema3. Serous retinal detachment4. Foveal tractional retinal detachment5. Taut posterior hyaloid membrane.
Echography: It is also a useful diagnostic adjunct if mediaopacities preclude good fundus visualization, or as asupplement to ophthalmoscopy. It may identify ordocument macular thickening and may help with etiologicclarification, for example, in cases of vitreomacular tractionsyndrome.
Fig.1: Technique of Slitlamp Biomicroscopy Fig.2: Procedure of Fundus FluoresceinAngiography
Fig.3: FFA showing Macular Edema
Fig.4 : Procedure of Hiedelberg RetinalAngiography 2
Fig.5: HRA2 showing Macular Edema

481DOS Times - Vol. 12, No. 6 December, 2006
Treatment Laser treatment
Laser therapy is well establishedin diabetic macular edema as well asmacular edema secondary to retinalvein occlusion.
Laser photo coagulation of diabeticmacular edema should only beconsidered when the edema isclinically significant (CSME). CSME asdefined by ETDRS includes any one ofthe following lesions:
retinal thickening at or within 500μm from the centre of the maculahard exudates at or within 500 μmfrom the centre of the macula,associated with thickening of theadjacent retinaan area or areas of retinalthickening at least one disc areain size, at least part of which iswithin one disc diameter of thecenter of the maculaFocal laser photo coagulation
reduces hypoxic areas and directlyoccludes leaky microaneurysms. Therationale for grid laser treatment indiffuse macular edema is that gridlaser may have its effect by thinningthe retina, bringing retinal vesselscloser to the choroidal vessels, andpermitting the retinal vessels toconstrict by autoregulation, therebydecreasing retinal blood flow andconsequently decreasing edemaformation.
Despite the lack of functionalimprovement (visual acuity) there isa reduction of retinal thickness(anatomical edema) after grid lasertreatment as shown in several studies.
It is well known that theanatomical endpoint (decrease in retinal thickness, or a‘dry macula” on angiography) in many cases differsconsiderably from the functional endpoint (visual acuityand reading ability). Grid laser has been shown to beefficacious in reducing vascular leakage; however, it doesnot improve visual acuity.
Panretinal photocoagulation (PRP) and focal macular lasertherapy
Although the DRS and ETDRS contain valuable
information for managing eyes with coexistentproliferative diabetic retinopathy (PDR) and macularedema, neither study gave clear recommendations for thesubgroup of patients with high-risk PDR and clinicallysignificant macular edema (CSME). This, along with thelack of other controlled multicenter clinical trials, has leftthese patients with no clear guidelines for treatment andwith a relatively guarded prognosis regarding maintenanceand improvement of visual acuity. One of the mainproblems in managing this group of patients is that PRPtends to cause worsening of CSME which usually leads to
Causes of Macular Edema
Disease group Disorder Pathogenesis
Metabolic Diabetes • Abnormal glucosealterations metabolism
• Aldose reductaseRetinitis pigmentosa • CME:leakage at the level
of RPEInherited CME(aut. dom.) • Müller cell disease:
leakage from perifoveolarcapillaries
Ischemia • Vein occlusion • Inner blood-retinal barrier• Diabetic retinopath (retinal capillary
hypoperfusion)• Severe hypertensive • Outer blood-retinal barrier
retinopathy (ischemic hypoperfusion• HELLP syndrome of the choroids: serous• Vasculitis, collagenosis detachment)
Hydrostatic Retinal vascular • Increased intravascularforces occlusions pressure
• Venous occlusion • Failure of the BRB• Arterial hypertension• Low IOP
Mechanical Vitreous traction on the • Epiretinal membrane withforces macula tangential traction
• Vitreomacular tractionsyndrome
Inflammation Intermediate uveitis • Mediated by prostaglandins• CME is indication for
treatmentPostoperative CME • Perivascular leuocytic
infilterationDiabetic macular edema • Diabetic leucostasis mediates
vascular leakage byendothelial cell apoptosis
Choroidal inflammatory • Vogt-Koyanagi-Haradadiseases syndrome
• Birdshotretinochoroidopathy
Pharmacotoxic e. g. • Mostly via prostaglandinseffects • Adrenaline (in aphakia)
• Betaxolol• Latanoprost

DOS Times - Vol. 12, No. 6December, 2006 482
further reduction in visual acuity.Conversely, treating macular edemafirst with focal or grid laser therapymay put the patient at risk of severevisual loss from PDR while waitingfor macular treatment to show effect.(Figure 6)
Focal laser photocoagulation isconsidered the gold standard oftreatment for CSME according to theETDRS. However, only 50% of eyeswere stabilized at 3 years, with 12% of treated eyes losing15 ETDRS letters at the 3-year follow-up. Lee and Olkshowed limited benefit of modified grid laserphotocoagulation for diffuse macular edema, with 60.9%of eyes unchanged and 24. 6% of eyes worse in 3 years. Thefailure of laser in a substantial subgroup of patients haspromoted interest in other treatment methods.
In the macular edema caused by retinal vein occlusion,treatment with a grid laser is generally consideredbeneficial when the perfused macular edema causes visualimpairment to the level of 20/40 or worse or shows nosigns of spontaneous improvement. Both in diabeticmacular edema and in macular edema secondary to branchvein occlusion, central laser surgery is not recommendedin eyes with ischemic maculopathy. Although definiteclinical data are lacking, the use of grid macular lasertreatment in the elderly population has additionaldrawbacks as it may induce or accelerate RPE atrophy inthe macular region.
In non-ischemic vascular occlusions, “rerouting” fromthe retinal to the choroidal vasculature (iatrogenicanastomosis by focal laser coagulation with high energy)has been postulated through laser photocoagulation.
Medical therapyMedical management of macular edema is best
established in postsurgical and predominantlyinflammatory oedema, e.g. in uveitis
Hyperglycemia, uncontrolled hypertension,nephropathy and fluid retention can cause worsening ofdiabetic macular edema. Thus, control of these factors maybe beneficial though there is no direct proven benefit.
Non-steroidal Anti-inflammatory Drugs (NSAIDs)target the inflammatory mediators that are responsiblefor edema formation and have been investigated in theprophylaxsis and therapy of postsurgical cystoid macularedema. It has been shown that topical administrationachieves better ocular penetration than systemicadministration and although they may not be an optimalstand-alone treatment they can be used as steroid sparingagents.
The rationale of carbonic anhydrase inhibitors as a
therapeutic agent in the treatment ofmacular edema is to improve theability of retinal pigment epithelialcells to pump fluid out of the retina.There are no available randomizedstudies that confirm beneficial effect ofcarbonic anhydrase inhibitors in thetreatment of macular edema
CorticosteroidsThe role of corticosteroids in the
treatment of macular edema is based primarily on theirinhibition of the biosynthetic pathways of leukotrienesand prostaglandins, the inflammatory mediatorsimplicated in the pathogenesis of CSME. Corticosteroidsinhibit the expression of inflammatory adhesion moleculesand contribute to stabilization of the blood-retinal barrier.Corticosteroids inhibit the expression of the vascularendothelial growth factor gene in human vascular smoothmuscle cells. Corticosteroids have also been shown toabolish the induction of vascular endothelial growth factorby platelet- derived growth factor and platelet- activatingfactor in a time- and dose-dependent manner.
The use of intravitreal triamcinolone acetonide (IVTA)has increased in the last few years after reports ofsuccessful treatment of macular edema secondary todiabetes, uveitis, and central retinal vein occlusion. IVTAcan dramatically reduce retinal thickness (RT) anddecrease cystic spaces shown by optical coherencetomography (OCT).
Intravitreal triamcinolone treatment has exhibitedencouraging results for patients with vascular occlusivediseases and macular edema. Park et al reported that at anaverage of 4. 8 months after 4-mg triamcinolone injections10 eyes with macular edema due to nonischemic CRVOsignificantly improved both anatomically and functionally;60% of eyes gained 2 lines of visual acuity.
Normalized retinal thickness, however, appears to beof limited duration with the restitution of edema withinseveral months. The limited duration of effect is most likelydue to elimination of drug by diffusion.
Jonas et al reported the transient effect of an intravitrealinjection of TA on macular edema associated with BRVO.They noted that while the difference between baselinevisual acuity and postinjection visual acuity at 1 monthwas statistically significant, no improvement of visualacuity was observed at any other time points. Anintravitreal injection of TA can be expected to achieve arapid effect. However, the effect of TA treatment on macularedema associated with BRVO would be transient
The recurrence of macular edema might be based onthe short half-life of TA in vitrectomized eyes (3. 2 days) oron the rebound phenomenon in TA.
Fig.6: Fundus Photograph showing Panretinalphotocoagulation

483DOS Times - Vol. 12, No. 6 December, 2006
Complications of intravitrealtriamcinolone acetonide deliverysystems comprise retinal detachment,vitreous haemorrhage, increasedintraocular pressure, cataractformation, and pseudohypopyon. It istherefore prudent that patients areasked about a history of a previoussteroid response. The incidence ofculture-positive endoph-thalmitisfollowing intravitreal triamcinoloneamounts to 0.87%.
A number of sustained-release corticosteroid deliverydevices have been devised to counter the recurrent natureof diabetic macular edema treated with intravitrealtriamcinolone acetonide. Retisert (fluocinolone acetonide;Bausch & Lomb; Rochester, New York) is an intraocularimplant that delivers 0. 59 mg of fluocinolone acetonide tothe posterior segment up to 3 years. It has been found toreduce the recurrence of macular edema in 58% of cases at3 years compared with 30% of eyes treated with laserphotocoagulation. Visual acuity improved by 3 or morelines in 28% of study eyes vs 15% of eyes treated withstandard of care. Posurdex (dexamethasone; Allergan, Inc.; Irvine, California) is another sustained deliveryintraocular implant that has been found to improve visualacuity in eyes with persistent macular edema at a dose of700 mcg compared with observation through 6 months.However the incidence of raised IOP and steroid inducedglaucoma is very high in both groups
Subteon injections of corticosteroids are widely usedin patients of cystoid macular edema with asymmetric orunilateral uveitis.
High-dose intravenous methylprednisolone (1 gmdaily for 3 days ) may be effective in the treatment ofpseudophakic CME not responding to other therapies asreported by few studies.
Anti-VEGF TherapiesIn recent years, extensive research initiatives have
greatly expanded our understanding of the underlyingmechanisms of macular edema. This information hassuggested new molecular targets for which noveltherapeutic agents have been developed. Several of theseagents are now undergoing clinical trials, the results ofwhich should begin to elucidate the potential of these newapproaches to preserve vision.
Potential New Drugs to Treat Macular Edema —Intravitreal Vascular Endothelial Growth Factor (VEGF) Inhibitors
In an effort to prevent the visual loss associated withmacular edema due to various causes, and to avoid theside effects associated with destructive treatments suchas laser therapy, studies have focused on blocking the
growth factors thought to initiate the abnormal vesselgrowth and vascular leakage of the retina. VEGF is generallyconsidered one of the most important of a diverse array ofmolecules that probably contribute to this complexbiological process.
Recent studies demonstrating efficacy of VEGFinhibitor therapy for choroidal neovascularization in eyeswith wet age-related macular degeneration (AMD) havegenerated increased interest in similar therapies for PDRand macular edema. In a recent multicenter clinical trial,eyes with diabetic retinal neovascularization treated withpegaptanib at doses of 0. 3 mg, 1 mg, or 3 mg were found tohave regression of neovascularization by 36 weeks.
Also under investigation for the treatment of diabeticmacular edema is ranibizumab, an anti-VEGF humanizedmonoclonal antibody. Bevacizumab the parent moleculefrom which Ranibizumab has been derived is an anti- VEGFantibody approved for use in colorectal carcinoma is beingused as an off label drug in macular edema and is showinggood results. (Figure 7)
Activated protein kinase C has been associated withincreased levels of VEGF and is also implicated in increasedretinal vascular permeability. PKC412 is an oral kinaseinhibitor that was found to reduce foveal thickening by66. 7 mcm at doses of 100-150 mg/d compared with placebowith a small but significant improvement in visual acuityat 3 months. Ruboxistaurin, a selective oral protein kinaseC beta inhibitor administered at doses of 4, 16, or 32 mg/dover 18 months, was also found to reduce retinal vascularleakage compared with placebo in patients with severediabetic macular edema.
Surgical approachesIt has been demonstrated that a surgically induced posterior
vitreous detachment in patients with a diffuse diabeticmacular edema leads to a reduction of macular edema witha subsequent increase in visual acuity. Although the exactmechanism is not known, removal of inflammatorymediators and better access of locally applied steroids arepostulated mechanisms of actions of vitrectomy.(Fig. 8& 9)
Vitrectomy including removal of the internal limiting membrane
Antiangiostatic Agents Available and in DevelopmentStops VEGF from binding to receptorPegaptanib (approved) Bevacizumab(off label)Ranibizumab (Phase III) VEGF Trap (phase II )
Stops VEGF or receptors from being madeCand 5 (phase II ) siRNA-027(phase I)
Stop VEGF effect after it binds to receptorsAnacortave acetate (phase III) Ad-PEDF (phase I-II)Squalamine (phase III) PTK inhibitors (preclinical)

DOS Times - Vol. 12, No. 6December, 2006 484
(ILM) aids the resolution of diffuse diabetic macular edemaand improvement of visual acuity and prevents epiretinalmembrane formation. Advantage of the ILM peeling overthe vitrectomy alone is the complete release of tractionalforces and inhibition of reproliferation of fibrous astrocytes,which seems to be prudent in the eyes of patients withdiabetes and advanced vitreoretinal interface disease ofthe macula. Similarly, favourable results were found inME from CRVO, chronic uveitis, post-surgical cystoid ME.
An increasing number of reports have shown theefficacy of pars plana vitrectomy (PPV) with or withoutarteriovenous sheathotomy or internal limiting membranepeeling for macular edema and visual loss associated withBRVO
In a recent study by Opremcak EM et al, 63 consecutivepatients of central retinal vein occlusion who underwent radialoptic neurotomy (RON) with adjunctive intraoculartriamicinolone were compared with previous series of 117patients with severe CRVO who underwent RON alone.
All patients had four quadrants ofintraretinal hemorrhage, venousdilatation and disk and macularedema. Anatomic resolution was seenin 93% of patients and 68% of patientsshowed an average of 3 lines ofimprovement in RON withintraocular triamcinolone group.Anatomic and visual outcomes werecomparable in both the groups. RONwith intraocular triamcinolone groupwas associated with a higherincidence of elevated IOP andendophthalmitis.
Miscellaneous therapiesOther potential targets in the
treatment of macular edema includepigment epithelium-derived factorand interferon alpha-2a. Pigmentepithelium-derived factor mayinterfere with VEGF-inducedvascular permeability and has been
found to occur in lower concentrations in the vitreous ofeyes with DME
Supplemental oxygen has also been found to reduceexcess foveolar thickness by 42% and improve visual acuityby at least 2 lines in a small study of patients with chronicME.
Case ReportsWe will like to present few of our interesting cases:Case1: Spontaneous resolution of BRVO (Fig. 10 and 11)A 33 year old male presented to us with chief
complaints of blurring of vision right eye for last one month,his visual acuity being 6/18. On examination he was foundto have inferior temporal BRVO. Patient was advisedroutine investigations including Echocardiography. On hisfollow up visit 2 months later he developed 360 degreeshard exudates around the hemorrhage. On his follow upafter 6 months his Visual acuity was 6/6 and fundusshowed regression of hemorrhage and exudates. On last
Fig.7: Intravitreal Injections Fig.8: OCT showing Vitreomacular tractionbefore Surgery
Fig.9: OCT of same eye after Surgery
Fig.10: Inferior temporal BRVO Fig.11: Same eye after spontaneous resolution
Fig.12: Gyrate Atrophy both eyes
485DOS Times - Vol. 12, No. 6 December, 2006
follow up his vision was 6/6 andcomplete resolution.
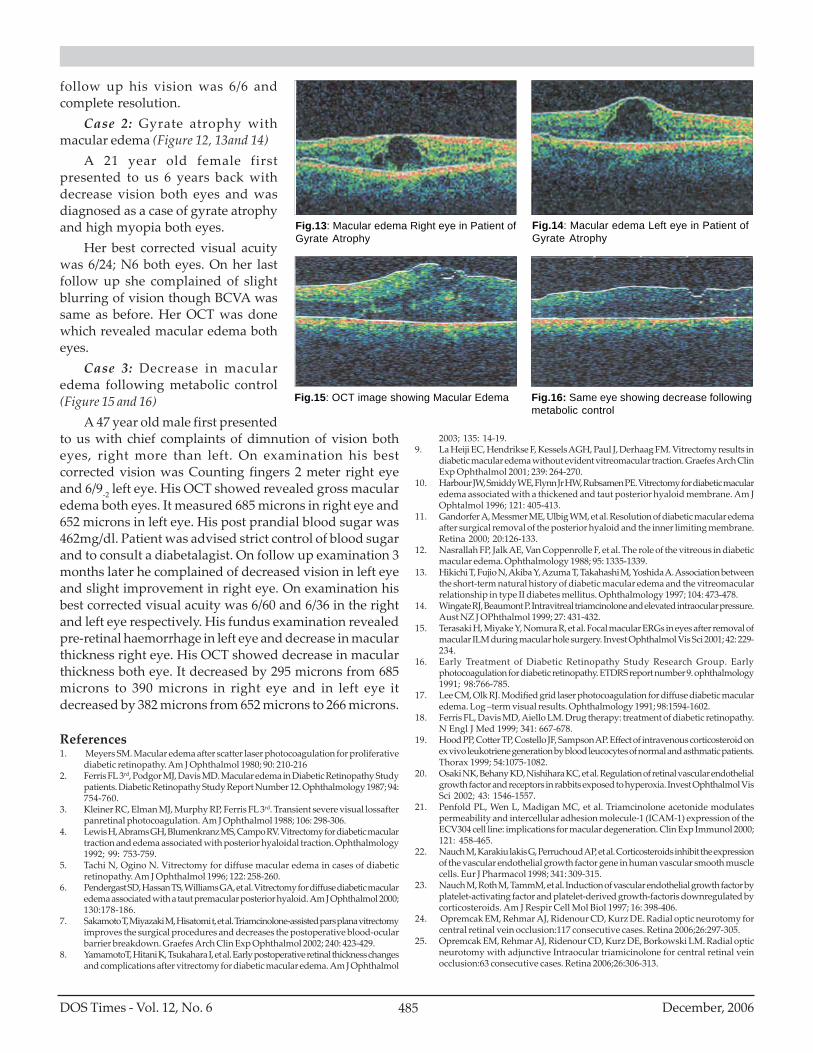
Case 2: Gyrate atrophy withmacular edema (Figure 12, 13and 14)
A 21 year old female firstpresented to us 6 years back withdecrease vision both eyes and wasdiagnosed as a case of gyrate atrophyand high myopia both eyes.
Her best corrected visual acuitywas 6/24; N6 both eyes. On her lastfollow up she complained of slightblurring of vision though BCVA wassame as before. Her OCT was donewhich revealed macular edema botheyes.
Case 3: Decrease in macularedema following metabolic control(Figure 15 and 16)
A 47 year old male first presentedto us with chief complaints of dimnution of vision botheyes, right more than left. On examination his bestcorrected vision was Counting fingers 2 meter right eyeand 6/9-2 left eye. His OCT showed revealed gross macularedema both eyes. It measured 685 microns in right eye and652 microns in left eye. His post prandial blood sugar was462mg/dl. Patient was advised strict control of blood sugarand to consult a diabetalagist. On follow up examination 3months later he complained of decreased vision in left eyeand slight improvement in right eye. On examination hisbest corrected visual acuity was 6/60 and 6/36 in the rightand left eye respectively. His fundus examination revealedpre-retinal haemorrhage in left eye and decrease in macularthickness right eye. His OCT showed decrease in macularthickness both eye. It decreased by 295 microns from 685microns to 390 microns in right eye and in left eye itdecreased by 382 microns from 652 microns to 266 microns.
References1. Meyers SM. Macular edema after scatter laser photocoagulation for proliferative
diabetic retinopathy. Am J Ophthalmol 1980; 90: 210-2162. Ferris FL 3rd, Podgor MJ, Davis MD. Macular edema in Diabetic Retinopathy Study
patients. Diabetic Retinopathy Study Report Number 12. Ophthalmology 1987; 94:754-760.
3. Kleiner RC, Elman MJ, Murphy RP, Ferris FL 3rd. Transient severe visual lossafterpanretinal photocoagulation. Am J Ophthalmol 1988; 106: 298-306.
4. Lewis H, Abrams GH, Blumenkranz MS, Campo RV. Vitrectomy for diabetic maculartraction and edema associated with posterior hyaloidal traction. Ophthalmology1992; 99: 753-759.
5. Tachi N, Ogino N. Vitrectomy for diffuse macular edema in cases of diabeticretinopathy. Am J Ophthalmol 1996; 122: 258-260.
6. Pendergast SD, Hassan TS, Williams GA, et al. Vitrectomy for diffuse diabetic macularedema associated with a taut premacular posterior hyaloid. Am J Ophthalmol 2000;130:178-186.
7. Sakamoto T, Miyazaki M, Hisatomi t, et al. Triamcinolone-assisted pars plana vitrectomyimproves the surgical procedures and decreases the postoperative blood-ocularbarrier breakdown. Graefes Arch Clin Exp Ophthalmol 2002; 240: 423-429.
8. YamamotoT, Hitani K, Tsukahara I, et al. Early postoperative retinal thickness changesand complications after vitrectomy for diabetic macular edema. Am J Ophthalmol
2003; 135: 14-19.9. La Heiji EC, Hendrikse F, Kessels AGH, Paul J, Derhaag FM. Vitrectomy results in
diabetic macular edema without evident vitreomacular traction. Graefes Arch ClinExp Ophthalmol 2001; 239: 264-270.
10. Harbour JW, Smiddy WE, Flynn Jr HW, Rubsamen PE. Vitrectomy for diabetic macularedema associated with a thickened and taut posterior hyaloid membrane. Am JOphtalmol 1996; 121: 405-413.
11. Gandorfer A, Messmer ME, Ulbig WM, et al. Resolution of diabetic macular edemaafter surgical removal of the posterior hyaloid and the inner limiting membrane.Retina 2000; 20:126-133.
12. Nasrallah FP, Jalk AE, Van Coppenrolle F, et al. The role of the vitreous in diabeticmacular edema. Ophthalmology 1988; 95: 1335-1339.
13. Hikichi T, Fujio N, Akiba Y, Azuma T, Takahashi M, Yoshida A. Association betweenthe short-term natural history of diabetic macular edema and the vitreomacularrelationship in type II diabetes mellitus. Ophthalmology 1997; 104: 473-478.
14. Wingate RJ, Beaumont P. Intravitreal triamcinolone and elevated intraocular pressure.Aust NZ J OPhthalmol 1999; 27: 431-432.
15. Terasaki H, Miyake Y, Nomura R, et al. Focal macular ERGs in eyes after removal ofmacular ILM during macular hole surgery. Invest Ophthalmol Vis Sci 2001; 42: 229-234.
16. Early Treatment of Diabetic Retinopathy Study Research Group. Earlyphotocoagulation for diabetic retinopathy. ETDRS report number 9. ophthalmology1991; 98:766-785.
17. Lee CM, Olk RJ. Modified grid laser photocoagulation for diffuse diabetic macularedema. Log –term visual results. Ophthalmology 1991; 98:1594-1602.
18. Ferris FL, Davis MD, Aiello LM. Drug therapy: treatment of diabetic retinopathy.N Engl J Med 1999; 341: 667-678.
19. Hood PP, Cotter TP, Costello JF, Sampson AP. Effect of intravenous corticosteroid onex vivo leukotriene generation by blood leucocytes of normal and asthmatic patients.Thorax 1999; 54:1075-1082.
20. Osaki NK, Behany KD, Nishihara KC, et al. Regulation of retinal vascular endothelialgrowth factor and receptors in rabbits exposed to hyperoxia. Invest Ophthalmol VisSci 2002; 43: 1546-1557.
21. Penfold PL, Wen L, Madigan MC, et al. Triamcinolone acetonide modulatespermeability and intercellular adhesion molecule-1 (ICAM-1) expression of theECV304 cell line: implications for macular degeneration. Clin Exp Immunol 2000;121: 458-465.
22. Nauch M, Karakiu lakis G, Perruchoud AP, et al. Corticosteroids inhibit the expressionof the vascular endothelial growth factor gene in human vascular smooth musclecells. Eur J Pharmacol 1998; 341: 309-315.
23. Nauch M, Roth M, TammM, et al. Induction of vascular endothelial growth factor byplatelet-activating factor and platelet-derived growth-factoris downregulated bycorticosteroids. Am J Respir Cell Mol Biol 1997; 16: 398-406.
24. Opremcak EM, Rehmar AJ, Ridenour CD, Kurz DE. Radial optic neurotomy forcentral retinal vein occlusion:117 consecutive cases. Retina 2006;26:297-305.
25. Opremcak EM, Rehmar AJ, Ridenour CD, Kurz DE, Borkowski LM. Radial opticneurotomy with adjunctive Intraocular triamicinolone for central retinal veinocclusion:63 consecutive cases. Retina 2006;26:306-313.
Fig.15: OCT image showing Macular Edema Fig.16: Same eye showing decrease followingmetabolic control
Fig.13: Macular edema Right eye in Patient ofGyrate Atrophy
Fig.14: Macular edema Left eye in Patient ofGyrate Atrophy

DOS Times - Vol. 12, No. 6December, 2006 486
Paediatric glaucoma encompasses complex, diversepathophysiological entities, with a pressure -sensitiveneurodegeneration of the optic nerve, and retinal ganglioncell death and loss1. The optic nerve damage is reflected bycupping of the optic nerve, visual field loss, and in latestages, blindness. It is seen in 1 in 10,000 live births, andmay be inherited in 10-27% cases. The inheritance isusually an incomplete, possibly, multifactorial, autosomalrecessive type. In the rest of the cases, it is heterogeneousand presents sporadically. It is bilateral in 70% of the cases,and may be asymmetric in presentation. The disease has aslight gender bias, 65% cases being male. Isolated primaryglaucoma is seen in 50- 70% cases, others being associatedwith structural maldevelopment.
This article, discusses the management of childhoodglaucoma in brief. It does not go into the details of differenttypes of glaucoma seen in children, rather, it is a review ofthe treatment options available, for childhood glaucomaas a whole.
In children the, the causes for glaucoma are multiple;the onset is variable, and outcomes are different1. A reviewof literature leaves us with incomplete information, andinadequate management guidelines.
Thick corneas in children may, sometimes, lead toartificially high measurements of the IOP3. The traditionalconcept of over diagnosing childhood glaucoma at IOPmeasurements, which are normal for adults, is nowredundant1,5. Falsely high IOP measurement is especiallytrue in children operated for cataract, who have increasedCentral Corneal Thickness (CCT) values4. It helps tocorrelate the CCT values with IOP measurements, beforediagnosing glaucoma in children2.
The current diagnostic criteria specifies repeated intra-ocular pressure (IOP) measurements of > 22 mmhg, withoptic nerve (ON) or retinal nerve fiber layer (RNFL)damage; or a IOP > 32 mmhg1,4,5.
Examination ProtocolThe examination protocol should include1:Age-appropriate visual acuity assessmentIOP measurementMeasurement of corneal diameter
Management Strategies in Childhood GlaucomaAbhishek B. Dagar MS, DNB, FICO, FPOS
Paediatric Ophthalmology ServicesVenu Eye Institute & Research Centre,1/31, Sheikh Sarai, Phase-2,New Delhi-17
Assessing of corneal clarityMeasuring CCTGonioscopyOphthalmoscopy- optic disc appearanceAxial length measurements
Ocular enlargement
Age (years) Corneal Diameter (mm)
New borns 9.5-10.5Up to 1 year 11.02-3 years 12.0
13 mm of corneal diameter is suggestive of glaucomaat any age.
Central Corneal Thickness (CCT)The CCT in children (0.554 ± 0.22 mm) is comparable
to that of adults (0.559 ± 0.39 mm)1,3.Thinning is seen inbuphthalmos. The CCT may be increased in acute episodesof IOP rise and in cases after cataract surgery2,6. A higherCCT falsely elevates IOP measurement, and this may leadto over diagnosing glaucoma in aphakic and pseudophakicchildren4,6.
Post- cataract surgery children comprise a majorchunk of paediatric glaucoma patients. There is an incidenceof up to 20% in aphakic cases, higher in those with vitreousdisruption6. Various reports show an incidence of 8 – 12 %in pseudophakes5. Most importantly, the frequencyincreases with long-term follow-ups, and all post-operative cases should be assessed for glaucoma on eachvisit5,6.
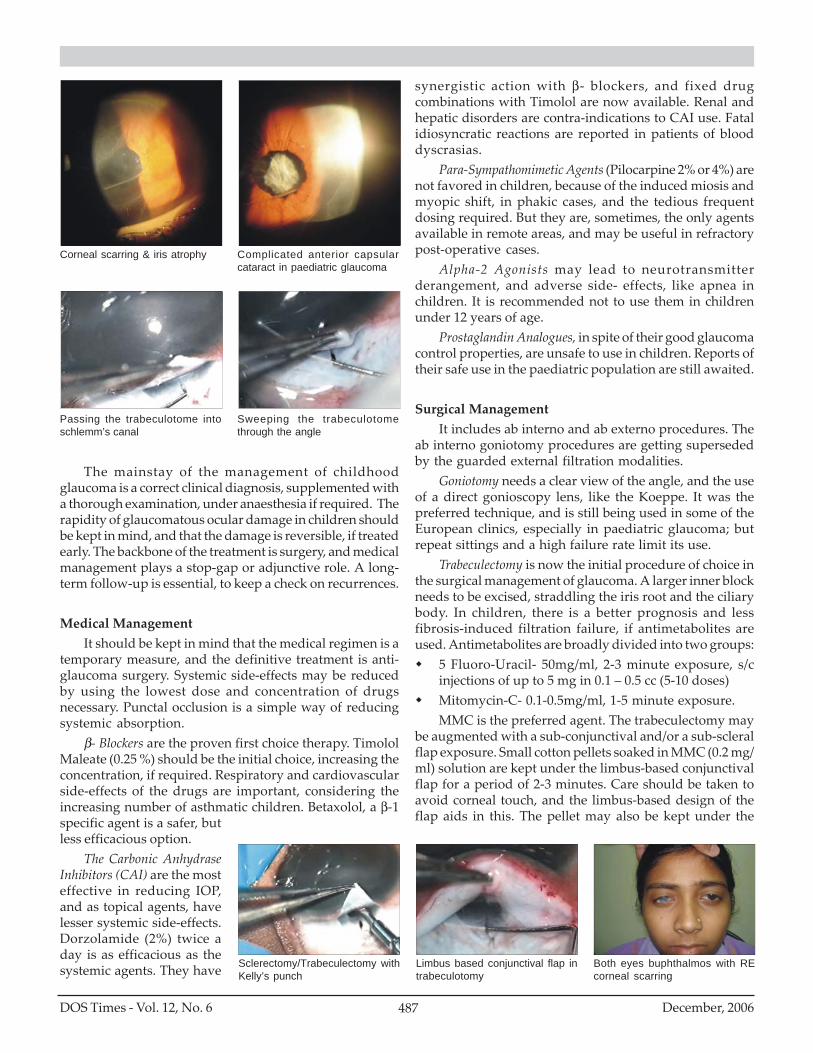
Haab’s striae in the cornea Haab’s striae & complicatedcataract
MEDICAL OPHTHALMOLOGY
487DOS Times - Vol. 12, No. 6 December, 2006
The mainstay of the management of childhoodglaucoma is a correct clinical diagnosis, supplemented witha thorough examination, under anaesthesia if required. Therapidity of glaucomatous ocular damage in children shouldbe kept in mind, and that the damage is reversible, if treatedearly. The backbone of the treatment is surgery, and medicalmanagement plays a stop-gap or adjunctive role. A long-term follow-up is essential, to keep a check on recurrences.
Medical ManagementIt should be kept in mind that the medical regimen is a
temporary measure, and the definitive treatment is anti-glaucoma surgery. Systemic side-effects may be reducedby using the lowest dose and concentration of drugsnecessary. Punctal occlusion is a simple way of reducingsystemic absorption.
β- Blockers are the proven first choice therapy. TimololMaleate (0.25 %) should be the initial choice, increasing theconcentration, if required. Respiratory and cardiovascularside-effects of the drugs are important, considering theincreasing number of asthmatic children. Betaxolol, a β-1specific agent is a safer, butless efficacious option.
The Carbonic AnhydraseInhibitors (CAI) are the mosteffective in reducing IOP,and as topical agents, havelesser systemic side-effects.Dorzolamide (2%) twice aday is as efficacious as thesystemic agents. They have
synergistic action with β- blockers, and fixed drugcombinations with Timolol are now available. Renal andhepatic disorders are contra-indications to CAI use. Fatalidiosyncratic reactions are reported in patients of blooddyscrasias.
Para-Sympathomimetic Agents (Pilocarpine 2% or 4%) arenot favored in children, because of the induced miosis andmyopic shift, in phakic cases, and the tedious frequentdosing required. But they are, sometimes, the only agentsavailable in remote areas, and may be useful in refractorypost-operative cases.
Alpha-2 Agonists may lead to neurotransmitterderangement, and adverse side- effects, like apnea inchildren. It is recommended not to use them in childrenunder 12 years of age.
Prostaglandin Analogues, in spite of their good glaucomacontrol properties, are unsafe to use in children. Reports oftheir safe use in the paediatric population are still awaited.
Surgical ManagementIt includes ab interno and ab externo procedures. The
ab interno goniotomy procedures are getting supersededby the guarded external filtration modalities.
Goniotomy needs a clear view of the angle, and the useof a direct gonioscopy lens, like the Koeppe. It was thepreferred technique, and is still being used in some of theEuropean clinics, especially in paediatric glaucoma; butrepeat sittings and a high failure rate limit its use.
Trabeculectomy is now the initial procedure of choice inthe surgical management of glaucoma. A larger inner blockneeds to be excised, straddling the iris root and the ciliarybody. In children, there is a better prognosis and lessfibrosis-induced filtration failure, if antimetabolites areused. Antimetabolites are broadly divided into two groups:
5 Fluoro-Uracil- 50mg/ml, 2-3 minute exposure, s/cinjections of up to 5 mg in 0.1 – 0.5 cc (5-10 doses)Mitomycin-C- 0.1-0.5mg/ml, 1-5 minute exposure.MMC is the preferred agent. The trabeculectomy may
be augmented with a sub-conjunctival and/or a sub-scleralflap exposure. Small cotton pellets soaked in MMC (0.2 mg/ml) solution are kept under the limbus-based conjunctivalflap for a period of 2-3 minutes. Care should be taken toavoid corneal touch, and the limbus-based design of theflap aids in this. The pellet may also be kept under the
Corneal scarring & iris atrophy Complicated anterior capsularcataract in paediatric glaucoma
Passing the trabeculotome intoschlemm’s canal
Sweeping the trabeculotomethrough the angle
Sclerectomy/Trabeculectomy withKelly’s punch
Limbus based conjunctival flap intrabeculotomy
Both eyes buphthalmos with REcorneal scarring

DOS Times - Vol. 12, No. 6December, 2006 488
scleral flap before doing the trabeculectomy. A thoroughsaline wash is mandatory before entering the anteriorchamber. Corneal epithelial damage, bleb-relatedcomplications, and a small risk of bleb endophthalmitisshould be kept in mind, when using antimetabolites.
Combining trabeculectomy with an ab externotrabeculotomy, the so-called “trab with trab” approachis, currently, the preferred approach in paediatricglaucoma. It may be augmented with antimetabolites inthe initial surgery, or they may be used in cases ofrefractory glaucoma, in repeat surgeries. Thetrabeculotomy provides an added drainage conduit andreduces filtration failure. The Schlemm’s canal is situatedjust posterior to the posterior surgical limbus, and itscircular fibers may be identified under high magnification.A 2mm vertical incision is given on the roof of the canal,after the scleral flap dissection. The Haans Trabeculotomeis inserted carefully, without any pressure, taking care notto create any false passages. It is then softly swept into theanterior chamber, again, with the least pressure, takingcare not to go behind the iris. It is then inserted and swepton the other side, completing a 180° trabeculotomy. A smallstreak of hyphema is expected, and may be washed outwith irrigation after the trabeculectomy. Thetrabeculectomy is then done by either the standard blockexcision, or with a Kelly’s punch. A peripheral iridectomy
is then done, and the scleral flap sutured back, after titratingthe flow from an irrigating side port. The conjunctival flaphas to be sutured back, and an absorbable suture may beused for this.
ConclusionContrary to popular belief, childhood glaucoma is a
manageable disease, and the optic nerve damage causedmay be reversible in children, if treated early. It should beremembered that ocular damage takes place very rapidlyin childhood glaucoma, and proceed to surgicalmanagement as soon as possible. A correct diagnosis mayrequire repeated examination under anaesthesia. Medicalmanagement may be handy as a stopgap measure and inthe postoperative period.
Bibliography1. A.W. Biglan. Glaucoma in children: are we making progress? JAAPOS 2006;10(1):7-
212. Peter. K. Rabiah. Frequency and predictors of glaucoma after paediatric cataract
surgery. Am J Ophthalmology 2004; 137: 30-37.3. M.H. Henriques et al. Corneal Thickness in Congenital Glaucoma. J Glaucoma
2004:13:185-188.4. J.W. Simon. Glaucoma in aphakic and pseudophakic children. JAAPOS 2005;9:326-
3295. J.E. Egbert. The natural history of glaucoma and ocular hypertension after paediatric
cataract surgery. JAAPOS 2006; 10:54-57.6. R. Bhola. Long term outcome of paediatric aphakic glaucoma. JAAPOS 2006; 10:243-
248.

489DOS Times - Vol. 12, No. 6 December, 2006
The term amblyopia is derived from the Greek word –ambly = dull, ops = vision. It is defined as a binocular ormonocular decrease in best-corrected visual acuity due topattern visual deprivation and or abnormal binocularinteraction during visual immaturity for which there isno obvious ocular pathology or visual pathway defect andwhich in appropriate cases is reversible.
Prevalence in the general population ranges from 2-2.5% and this increases to 4-4.5% in hospital-based settings.Chances of developing amblyopia increase to 5 times inpremature infants, small for gestational age babies and ifthere is a family history of amblyopia. Amblyopia is 6times more common in children with developmental delay.
For the purpose of understanding and prognosticatingamblyopia, it is important to identify the critical period ofvision development. There are 3 critical periods of visualdevelopment in children. The first period starts from birth to3-5 years. In this period, the development of visual acuityfrom 20/200-20/20 takes place. The second period can bedefined from birth to 7-8 years. This is the age when themaximum risk for deprivational amblyopia is there. Theperiod from the time of deprivation to teenage is the periodduring which recovery can be obtained.
Amblyopia can be classified as1. Strabismic amblyopia2. Anisometropic amblyopia3. Visual deprivation amblyopia4. Idiopathic amblyopia5. Amblyopia secondary to nystagmus
Strabismic AmblyopiaDevelops in patients with strabismus who strongly
favor one eye for fixation or who have no alteration offixation.
Stabismic amblyopia is more common in esotropiathan exotropia. One reason for this is that exotropia iscommonly intermittent. Also, in case of esotropia, the foveaof the deviating eye has to compete with the strongtemporal hemifield of the fixating eye, so is more likely toget suppressed.
AmblyopiaArchana Gupta, Suma Ganesh MS, Manish Sharma MS, Sandeep Buttan
Department of Pediatric Ophthalmology and Strabismus,Dr. Shroff’s Charity Eye Hospital,Daryaganj, New Delhi
Strabismic amblyopia is always unilateral, caused by theactive inhibition of the visual input originating in the fovea of thedeviating eye. In such cases, it is the consequence rather thanthe cause of strabismus.
It is important to remember that alternating suppressiondoes not result in amblyopia (fig 1).
Anisometropic AmblyopiaIs caused by the active inhibition of the fovea.
Anisometropic amblyopia develops in an attempt toeliminate sensory interference caused by superimpositionof a focused and a defocused image originating from thefixating point.
Contrast sensitivity is typically less. The anisiekoniaafter correction of anisometropia also may be anamblyopiogenic factor.
Amblyopia is more common in aniso-hypermetropiathan anisomyopia. This is because the retina of the morehypermetropic eye never receives a clear image. Converselyin case of anisomyopia, the less myopic eye can be used fordistance and the more myopic eye can be used for nearwork.
The amount of anisometropia that can induceamblyopia varies according to the type of refractive errorpresent (Table)
Amount of anisometropia
Hypermetropia >1DMyopia >3DAstigmatism >1D
Visual Deprivation AmblyopiaIt has been found that a lack of formed vision rather
than a lack of light in general leads to visual deprivationamblyopia . The critical period was found to be between 2to 3 months in humans.
Unilateral vision deprivation amblyopia is more severethan the bilateral form. This may be caused by mediaopacities, occlusion amblyopia, and unilateral ptosis (fig2). This is often accompanied by secondary esotropia orexotropia.
Bilateral vision deprivation amblyopia is less severeand may be caused by media opacities (fig 3), bilateraluncorrected high hypermetropia or astigmatism.
MEDICAL OPHTHALMOLOGY

DOS Times - Vol. 12, No. 6December, 2006 490
Meridional amblyopia is also a form of visualdeprivation amblyopia and this may be the reason somepeople do not improve even with the full correction of thecylindrical refractive error.
Idiopathic AmblyopiaIs a term used to describe apparently normal patients
with no apparent amblyopiogenic factors and no cause fordecreased vision. The mechanism has been postulated asfoveal suppression of the amblyopic eye due to a transientamblyopiogenic factor during infancy.
Organic AmblyopiaIs said to exist when adequate amblyopia treatment
improves vision only to a certain level but is unable torestore standard acuity to that eye. There is a possibilityof subtle sub ophthalmoscopic morphological changes notdetectable by routine clinical tests.
Amblyopia Secondary to NystagmusIt is difficult to determine whether nystagmus is the
cause or effect of amblyopia. The image blur or retinalpattern distortion causes structural and functional damageto the lateral geniculate nucleus and striate cortex.
Pathophysiology of AmblyopiaLateral Geniculate layers subserving the affected eye
have been found to be atrophic in amblyopia . The corticalocular dominance columns representing the amblyopic eyeare less responsive to stimulus and show changesmicroscopically.
There are two kinds of retinal ganglion cells – themagno cells and the parvo cells. Dissociation between theparvo and magnocellular systems occurs in amblyopia.
Clinical FeaturesHistory
It is important to elicit any history of squint, theduration of symptoms noted, patching or eye drops,previous ocular disease or surgery, family history ofstrabismus or other ocular problems.
Visual AcuityAmblyopia has been
defined in terms of visualacuity as a difference of 2lines or more between theeyes. The visual acuity maybe better with reducedillumination so testingshould be done under
standard conditions.Crowding Phenomena – the isolated letter visual
acuity is better than line acuity in amblyopia. Visualacuity testing should include both line and letter acuity.The visual acuity is recorded as the best corrected lineacuity, as the line acuity may not necessarily improve toletter acuity in amblyopic individuals. The letter acuityrepresents the true potential functional ability of the eye,which is masked by the amblyopic process.
Detection of Amblyopia in a Preverbal ChildThe presence of amblyopia in a preverbal child can be determined
if there is a fixation preference present .The child may stronglyresist occlusion of the fixating eye if the other eye is amblyopic.
The eye may be found to perform searchingnystagmoid movements when the fixating eye is covered.On cover test, if the fixating eye regains fixation in a fewseconds that cover is removed, a strong fixation preferenceis present and amblyopia is present. If the formerlydeviated eye holds fixation beyond the next blink,amblyopia is probably absent.
Neutral Density FiltersProfoundly reduce vision in eyes with central retinal
lesions and glaucoma but vision in amblyopic eyes is notreduced. This is believed to be due to a relative increase inmesopic visual acuity in amblyopic eyes.
Pharmacological effect on vision of amblyopic eyesA great deal of research is ongoing into the
pharmacological treatment of amblyopic eyes. Amblyopiaas it is now known is caused primarily by an active
Fig.1: Alternating strabismus
Fig.2: Unilateral cataract causessevere vision deprivationamblyopia
Fig.3: Bilateral vision deprivationamblyopia

491DOS Times - Vol. 12, No. 6 December, 2006
suppression of the amblyopic eye by the fixating eye,research has aimed at therapeutic intervention to targetthis suppression.
Levodopa is a neurotransmitter / neuromodulatorinfluencing visual system at retina and cortical cells.Levodopa/carbidopa has been found to facilitate visualrecovery when combined with occlusion therapy but longterm studies report reversal of effect once drug has beendiscontinued.
Management of amblyopiaThe value of normal visual function and the
effectiveness of treatment justify the difficulty andinconvenience of managing amblyopia in children.
PreventionInfants and young children are uniquely sensitive to
permanent central visual loss. The visual pathwayscontinue to develop from birth to age 10 till when the diseaseis amenable to treatment. It is important to identify factorsthat may predispose to amblyopia early in the child’s lifein order to improve treatment outcomes.
TreatmentHas to be individualized per patient.Treatable causes e.g cataract have to be removed in
case of vision deprivation amblyopia.The management can be broadly divided into 4 parts
1. Optical correction2. Occlusion3. Penalization4. Surgery
Management of congenital cataractThe best results in terms of attainment of vision are
seen when surgery is done before 8-10 weeks of age. Patientswith unilateral cataract are at a higher risk for developingamblyopia. A delay in surgery leads to less chances ofvision improving to more than 6/60 post operatively.Establishment and maintenance of accurate opticalcorrection is very important post operatively (fig 4);occlusion therapy may be required.
Postoperative management includes1. Management of Aphakia2. Management of Amblyopia3. Management of PCO4. Management of Low vision
Patching scheme for unilateral congenital cataract
Age Patching scheme
0-1 month No patching1-2 months 1-2 hours per day2-4 months 2-3 hours per day4-6 months 50% of waking hours6-12 months 80% of waking hours
Optical correctionThe amblyopic eye must have the most accurate optical
correction possible. This should occur prior to any occlusiontherapy because vision may improve with spectacles alone.
Full cycloplegic refraction should be given to patientswith accommodative esotropia and amblyopia.
Occlusion therapyIs the mainstay of amblyopia management (fig 5).
Occlusion can produce rapid and dramatic shifts in visualacuity.
Physiological benefit: decreases inhibitory signalsfrom the dominant eye. Occlusion may be full-time or part-time. Full time occlusion may also be defined as highpercentage occlusion, which includes 70 % of waking hours.
Part time occlusion may also be defined as lowpercentage occlusion including less than 70 percent ofwaking hours. Children need to be observed at intervals of1 week per year of age, if undergoing full-time occlusionto avoid occlusion amblyopia in the sound eye.
Always consider lack of compliance in a child wherevisual acuity is not improving. Compliance is difficult tomeasure but is an important factor in determining thesuccess of this therapy.
Full time versus part time occlusionFor treatment and prognosis, amblyopia can be
classified asSevere amblyopia : when the best corrected visual acuity
is less than 20/100.Moderate amblyopia : best corrected visual acuity 20/40 –
20/80
Fig.4: Aphakic glasses after con-genital cataract surgery
Fig.5: Occlusion

DOS Times - Vol. 12, No. 6December, 2006 492
Mild amblyopia : best corrected visual acuity 20/40 ormore
Severe amblyopiaChildren with severe amblyopia are usually prescribed
full time patching the regimen. Full time patching includespatching of all but one waking hour per day.
Moderate amblyopiaNo specific patching regimen recommended. A commonly accepted regimen is part time patching
upto 6 hrs/ day.The pediatric eye disease investigator group in a
prospective randomized control trial has found a similarmagnitude of improvement in visual acuity with 2 hoursof patching and 1 hour of intensive near work.
Side effects of patching treatmentSkin rashIncreased risk of accidents when the child is wearing apatchPrecipitation of or increase in the deviation of the angleof strabismusDiplopiaOcclusion induced amblyopia
Relation of age to response to therapyResponse to treatment and visual outcome are better
the younger the childHowever there have been reports that say that
amblyopia treatment may still be effective in children > 7yrs. A prospective trial is ongoing to evaluate the effect oftreatment in amblyopia in children 7-18 years of age. Thepreliminary report has found that in children 7-<13 yearsof age, 53% of the treatment group responded to treatment.The trial is still ongoing to record whether effectmaintained in the long term.
The end point of treatment may be defined as thespontaneous alternation of fixation or equal visual acuityin both eyes.
Maintenance patchingRecent reports have shown that amblyopia recurrence
rates are lower when patching is weaned before beingdiscontinued. Once the visual acuity difference in the twoeyes is one snellen line or less, patching should be decreased.
ConsiderReduction in time – tapering of occlusionOptical penalisation
Cycloplegic penalisationOr cessation of occlusion - if > 10 years age
PenalisationPenalization of the sound eye in the treatment of
amblyopia has shown a resurgence of interest with therecent studies showing comparable results with occlusiontherapy.
IndicationsMild to moderate amblyopiaOcclusion failuresMaintenance treatmentThe basic purpose is to decrease the vision of the sound
eye to less than the amblyopic eye.
TechniquesPharmacological - Atropine, homatropine or
cyclopentolateIn spectacles,the better eye can be penalised by–adding more plus to the spectacle lens–Ground glass/ adhesive paperAs a part of the amblyopia treatment studies, a
prospective randomized trial was conducted in childrenwith amblyopia and a best corrected visual acuity in theworse eye of 20/40 to 20/100; age group 3-7 years. The studygroup received atropine 1% eye drops once a day in theamblyopic eye for 6 months followed by 2 years of careand follow up compared with the control group thatreceived patching. The results showed a visual acuityimprovement of 75 % in the atropine group compared to74% in the patching group. The also found a comparableefficacy with weekend only atropine.
Advantages of penalization include a bettercompliance, better acceptability by the parents, a widervisual field is available using both the eyes, so more safetyfor the child, and the social stigma of the patch iseliminated.
However, the many disadvantages limit it’s use. Theseinclude side effects of the drug, photophobia, a chronicallydecreased near vision. In severe amblyopia, even aftercycloplegia, the vision in the sound eye will be better.Atropine penalization is contraindicated in children below 1 yearbecause of the risk of inverse amblyopia developing in the sound eye.
Prognosis of treatment in amblyopiaIt has been shown that after one year of occlusion
therapy, 73% cases show success but this decreases to 53%after 3 years. Risk factors for failure of occlusion therapyinclude.

493DOS Times - Vol. 12, No. 6 December, 2006
1. Type of amblyopia–Strabismic amblyopia has the best outcome,–High anisometropia and organic pathology the worst
2. Age at which therapy began–Younger age does better
3. Depth of amblyopia–The better the vision at the start of therapy, the better
the prognosis
References1. Von Noorden G V. Binocular Vision and Ocular Motility. Mosby. 6th ed2. Amblyopia Preferred Practice Pattern. American Academy of Ophthalmology.3. Lawrence D et al. Levodopa/carbidopa treatment for amblyopia in older children.
JAAPOS 1995;
Programme for DOS Monthly Clinical Meeting for December, 2006Venue: Lecture Theatre Complex, Behind New OPD Block,
Vardhman Mahavir Medical College, Safdarjang Hospital, New DelhiDate & Time: 23rd December, 2006 (Saturday) at 2:30 PM
Clinical CaseOrbital Lamphangioma ............................................................................ Dr. Sumi GuptaSafdarjung Suture in Euriblepharon ...................................................... Dr. Ashok Kumar
Clinical TalkRole of Antioxidants in ARMD-Newer perceptions ............................ Dr. B.P. Guliani
Mini Symposium : Practical Tips for the Beginners inChairman : Prof.K.P.S. MalikCo-Chairman: Dr. J.S. Titiyal
1. Non Phaco-SICS ........................................................................................... Dr. Ruchi Sangal2. Phaco Emulsification ................................................................................... Prof. K.P.S. Malik3. Foldable IOL’s ................................................................................................ Dr. Sangeeta Abrol
Discussion
4. Bhartiya P, Sharma P, Biswas NR, Tandon R, Khokhar SK.. Levodopa-carbidopa withocclusion in older children with amblyopia. J AAPOS. 2002 Dec; 6(6): 368-72.
5. Steele A L et al. Successful Treatment of anisometropic amblyopia with spectaclesalone. Journal of AAPOS; 10 (1); Feb 2006; 37-43.
6. The pediatric eye disease investigator group. A randomised trial of prescribed patchingregimens for treatment of severe amblyopia in children. Ophthalmology Nov 2003.Vol .110;11; 2075-2087.
7. The pediatric eye disease investigator group: A randomised trial of patching regimensfor treatment of moderate amblyopia in children. Arch Ophthalmol 121: 603-611,2003.
8. Epelbaum, Milliret C. The sensitive period for strabismic amblyopia in humans.Ophthalmology 1993. 100: 323-327.
9. Pediatric eye disease investigator group. An evaluation of treatment of amblyopiain children 7 - <18 years old. National Eye institute. Clinical studies database.
10. Pediatric Eye Disease Investigator Group: Randomised trial of treatment ofamblyopia in children aged 7-17 years. Arch Ophthalmol 2005. 123: 437-47.
11. The pediatric eye disease investigator group. A randomized trial of atropine versuspatching for treatment of moderate amblyopia in children. Arch Ophthalmol 120:268-278, 2002.

DOS Times - Vol. 12, No. 6December, 2006 494
Scleral indentation is a procedure which enhancesdetection and allows dynamic evaluation of the peripheralretinal lesions. It can help you interpret clinical findingsby seeing changes in the fundus produced by movementsof the indentor. It's this dynamic aspect of scleralindentation that enables you to see things which mightotherwise go undetected. It is extremely useful indifferentiating flat from raised lesions, retinal break fromhemorrhage and in appreciating retinal flaps of horse shoetears.
Using binocular indirect ophthalmoscopy with scleralindentation, one can examine the ora serrata for 360 degreesin an eye that dilates well. We can use different types ofindentors (Fig.1) eg. wire vectis is often used for scleralindentation in premature babies to screen retinopathy ofprematurity (ROP).
TechniqueWhen using scleral indentation, remember that the
ora serrata begins less than 1cm behind the limbus. Whilestarting to learn scleral indentation we often forget thisand hold the indentor too much anteriorly leading toindentation of the ciliary body and causing immense painto the patient and discouraging us from continuing theprocedure.
Mastering Scleral indentationManisha Agarwal1 MS, Anuj Gogi2, J.S. Guha3 MS
1. Dr. Shroff’s Charity Eye Hospital5027, Kedar Nath Road, Daryaganj, New-Delhi
2. Gogi Eye Clinic, Ramghat Road, Aligarh3. Sai Retina Foundation
Navjyoti Eye Centre, Daryaganj, New-Delhi
Maximally dilate thepupilsRecline the patient -patient's head shouldbe at waist level.Stand 180 degree awayfrom the area of theretina you are trying toviewStart with the indirectophthalmoscope rheostat at low power and thenincrease it after the patient has adjusted to thebrightness.Ask the patient to look in the direction opposite to themeridian to be indented. The scleral indentor should just rest on the eye withthe shaft parallel to the eye without applying anypressure.
Fig.1: Various types of Indentors used for scleral Indentation
Fig.2: Altered red-gray reflex onscleral Indentration
Fig.3: The consensing lens, the patient’s pupil, the object of Interest inthe fundus and the scleral indentor are all in same axis
Fig.4: As the patient looks up towards 12 o’clock and as thesuperior lid retracts, slide the indentor posteriorly and nearlyparallel to the surface of the eye
OPHTHALMIC TECHNIQUES

495DOS Times - Vol. 12, No. 6 December, 2006
The ophthal-moscope lightilluminates theeye without thecondensing lensin place.The condensinglens is thenplaced only afterthe scleralindentor isproperly positio-ned and we seean altered red-gray reflex secondary to elevation ofthe retina by the indentor (Fig.2).Adjust the condensing lens to bring the indentedportion of the fundus into better focus.The force you need to apply to see the
fundus varies slightly with the amount ofpupil dilatation, the intraocular pressureand the fundus area you're examining. In anyevent, the force we need to indent the sclerais not as much as we think. We roughly usethe same pressure as we use in digitaltonometry.
Once we see the indented fundus, we canbring other parts of the anterior fundus intoview by moving the indentor.
The most important thing to rememberis that the examiner, the condensing lens, thepatient's pupil, the area of interest in thefundus and the scleral indentor should allbe in one axis (Fig-3).
Indent the sclera as parallel to the eye aspossible. If you can't see the mound offundus, and if your patient's eye holds itsposition, all you need to do is align theOphthalmoscope anteriorly or posteriorly.Generally, the inferior fundus is more
Fig.5: Indentration of 12 o’clock – indentor is placed on the upper lid just past the tarsal plate
difficult to examine byindentation than thesuperior fundus becausethe lower lid is thicker thanthe upper. When indentingthe lower eyelid, place theindentor about 3mm or4mm behind the lid margin.
"Examiner, thecondensing lens, thepatient's pupil, the area of interest in the fundus and thescleral indentor should all be in one axis"
Examination of the Vertical meridiansUsually one should begin scleral indentation at the 12
o'clock position. Have the reclined patient look down andplace the indentor on the superior lid, just past the tarsal
plate margin (Fig-4). Ask the patient tolook up, and as the superior lid retracts,slide the indentor posteriorly and nearlyparallel to the surface of the eye (Fig.5). Ifyou're right-handed, examine thesuperior fundus from the patient's rightside and the inferior areas from the leftside. If you're left-handed you may bemore comfortable reversing theprocedure.
Examination of the Horizontal meridiansIndent the sclera by applying the
indentor over the lid and moving the lidslightly or by carefully applying theindentor directly over the conjunctivaafter instilling topical anaesthetic drops(Paracaine 1%). (Fig.6&7)
Examination of the other quadrantsExamine the temporal fundus of
the left eye and the nasal area of the right
Fig.6: Instillation of local anesthetic dropsprior to placing the Indentor over theconjunctiva
Fig.7: Examination of the 3 and 9o’clock meridians by placing thescleral indentor on the conjunctivaafter anesthetic drops
Fig.8: Placement of the scleralindentor for indentration ofdifferent quadrants of the fundus

DOS Times - Vol. 12, No. 6December, 2006 496
eye from the patient's right side, and the right temporaland left nasal areas from the patient's left side. (Fig.8)
"Anyone can master Indirect Ophthalmoscopy and scleralindentation by
Practice, practice and then practice some more
References1. Learning scleral depression with binocular indirect
Ophthalmoscopy. Am J Ophthalmol.1979 Jan; 87(1): 97-9.2. A teaching pointer of indirect Ophthalmoscopy. Arch
Ophthalmol.1976 Feb; 94(2): 317.3. Havener WH. Schepens' binocular indirect ophthalmoscope. Am
J Ophthalmol.1958 Jun; 45(6):915-8.
ANNUALCONFERENCE
Delhi Ophthalmological Society (DOS)6-8 April, 2007
at Hotel Ashok, Chanakya Puri, New Delhi
497DOS Times - Vol. 12, No. 6 December, 2006
Choroidal circulation, though a significant part ofocular blood flow, was till recently not well known becauseof difficulties in choroidal imaging. Fluoresceinangiography has been used extensively in diseases of retinabut has limited applications for choroidal imaging due tocertain fundamental drawbacks such as:i) Masking of choroidal circulation by ocular pigments
and bloodii) Rapid leakage of fluorescein dye from the chorio-
capillaris eventually masking the choroidalvasculature.These have largely been overcome by the use of
indocyanine green angiography. Due to its infraredabsorption and emission, masking by pigments and bloodis minimized and because of its little leakage from chorio-capillaris, the choroidal vasculature is better visualised.
Indocyanine Green Dye1. Chemical Properties
Indocyanine green dye (ICG) is a sterile, water solubletricarbocyanine dye. It contains less than 5% sodiumIodide. The emperical formula is C43H47N2NaO6S2. It issupplied with an aqueous solvent and its pH in dissolvedstate is between 5.5 and 6.5
2. Optical PropertiesThe optical properties of ICG dye are such that it
absorbs and emits in the near-infrared range of thespectrum. The peak absorption and emission in blood ofICG is between 800 and 850 nm i.e. it maximally absorbsinfrared light at 805 mm and maximally fluoresces at 835nm. At these wavelengths, penetration through ocularpigments and media opacities is possible. Also the influenceof blood and hemoglobin on measurement of dyeconcentration at the 805 nm wavelength is small. Thesefactors results in better delineation of choroidalvasculature.
3. Pharmacologic PropertiesICG is administered via the intravenous route for
ophthalmic angiography. The 98% protein – bindingproperty of ICG is useful. The dye is retained within the
ICG -Indocyanine Green AngiographySanjeev Gupta MD, Amit Khosla MD
Siri Fort Laser Eye Centreat Sama Nursing Home8, Siri Fort Road,New Delhi
choriocapillaris resulting in better imaging of the choroidand any associated abnormalities. This gives it a majoradvantage over fluorescein, which extravasates rapidlythrough the choroidal capillaries into the extra-cellularspace preventing delineation of the choroidal anatomy.
4. PharmacokineticsICG dye is excreted exclusively by the liver. It does not
cross the blood brain barrier and placenta. Its dosage inophthalmic angiography is 25 mg / 2ml of aqueous solventfollowed by a 5 ml bolus of saline.
Adverse Reactions of ICGBecause ICG dye contains iodine, it should be used
with caution in patients with a history of allergy to iodides.
A Mild adverse ReactionA mild reaction is defined as a transient effect that
does not require any treatment. Complete and rapidresolution occurs without any sequelae. Mild reactions arenausea, vomiting, extravasation, sneezing and pruritis.
B Moderate Adverse ReactionIt is also a transient effect where some form of medical
treatment may be required with complete recovery. Theyare: urticaria, syncope, other skin eruptions, pyrexia, localtissue necrosis, nerve palsy.
C Severe Adverse ReactionDefined as one exhibiting prolonged effects that
requires intense treatment and also poses a threat to thepatient’s safety, and results in a variable recovery. Itinvolves the cardiac, respiratory, or neurologic system.They are:-Respiratory : Bronchospasm, Laryngospasm and
anaphylaxisCardiac : Circulatory shock, myocardial
infarction and arrest.Neurologic : Tonic-clonic seizure
High Risk PatientCertain patients have increased risk of adverse
reactions. They are:Persons with history of iodine allergy and otherallergies
OPHTHALMIC PROCEDURES

DOS Times - Vol. 12, No. 6December, 2006 498
Hepatic disease patient since the dye is excretedexclusively by liver.Patients undergoing hemodialysis for chronic renalfailure (cause unknown)Though ICG dye does not cross the placenta, it should
not be used in pregnancy as no studies on foetal toxicityhave been performed.
Mechanism of Adverse ReactionMild and moderate adverse reactions appear to be
pseudo allergic in nature. Non-immunologic release ofhistamine could explain these adverse reactions but therelease of other inflammatory mediators is anotherpossibility.
Severe reaction and death may be caused by a trueallergic reaction, an anaphylactic reaction.
ICG Vs. Fluorescein: Adverse reactions to ICG dye occurless frequently than with fluorescein :
Type of Reaction:
ICG Fluorescein
Mild 0.15% 1-10%Moderate 0.2% 1.6%Severe 0.05% 0.05%Death 1/333,333 1/222,000
Acquisition of ICG AngiogramsTo acquire a ICG angiogram, two kinds of system are available
Modified conventional fundus camera with infra-redfilters or scanning laser ophthalmoscope
Coventional Fundus CameraThe fundus camera system used for ICG angiography
is a standard retinal camera that has been modified withthe incorporation of infrared filters. The video camera usedis Kodak Mega Plus (1024 x 1024). The silicon based CCDchip used in the Megaplus camera is highly sensitive to theinfrared region of the light spectrum making it ideal forICG fluorescence imaging. For focusing a black and whiteCCD camera is used as ICG fluorescence is invisible tohuman eye. The field of view is 50°, 30° and 20°. Thelimitations of this system is speed - one frame/second.Therefore real-time video-angiography is not possible.
Scanning Laser Ophthalmoscope (SLO)Scanning laser ophthalmoscope uses an infrared laser
diode to illuminate the eye and the reflected light is blockedby a barrier filter. The wavelength of the laser diode and
the cut off wavelength of the barrier filter are matched tothe peak absorption and emission wavelength of the ICGdye in blood. It allows confocal imaging of the retina andchoroid with digital image acquisition and fast frame rate.The field of view varies from 10° to 30°. SLO has an addedadvantage of acquiring real time simultaneous ICG andfluorescein video-angiography.Its advantages are:a. Time sequence correlationsb. Exact overlapping of corresponding FA & ICG
angiographic imagesc. Time efficientThe disadvantages of SLO includes:a. Narrow field of viewb. High costc. Exposure to laser light
Normal Angiogram1. Early phase (Upto 20 seconds)It shows:
Hyperfluorescence of the optic disc associated withpoor perfusion of the vertical zone near the optic disc(watershed zone)Prominent filling of choroidal arteries and early fillingof choroidal veins.Early filling of retinal arteries
2. Early middle phase (20 sec. – 3 minutes)It shows:-
Filling of watershed zoneGradual fading of choroidal arterial filling with moreprominent filling of choroidal veins.Both retinal arteries and veins are visible
3. Late middle phase (3-6 minutes)It shows:-
Fading of choroidal vesselsDiffuse hyperfluorescence as a result of diffusion of dyefrom chorio-capillaris.Retinal vessels still visible
Late Phase (6-21 minutes)It shows :-
Virtually black optic disc and silhouetting of the large,relatively hypo-fluorescent choroidal vessels against thebackground fluorescence (result of staining of extra-choroidal space). Retinal vessels are no more visible.

499DOS Times - Vol. 12, No. 6 December, 2006
Clinical InterpretationThe approach for ICG angiography interpretation is
similar to that of fluorescein angiography. The first step isto determine whether an area of interest exhibitshyperfluorescence (increased fluorescence) orhypofluorescence (reduced fluorescence) compared to thesurrounding presumed normal regions of the fundus.
HypofluorescenceIs a relatively dark area on an ICG angiogram produced
either by tissue blockage of underlying dye fluorescence orsecondary to a vascular filling defect.
1. Blockage : (Blocked Fluorescence)Blocking in ICG angiography will depend on the nature
of the blocking material and on the background choroidalfluorescence. Melanin blocks most effectively and serousexudation least effectively. Blocking substances can bedivided into three main categories; pigment, hemorrhageand other materials including exudation, myelinated nervefibres and scar tissue.
a. Pigment: with ICG angiography heavypigmentation will result in marked hypofluorescence ofall posteriorly located structures. Lesser degree of melanindeposition results in varying levels of obstruction ofunderlying angiographic details.
b. Hemorrhage: Blood can be present in the variouslayers of the retina and choroid, be of varying thicknessand exist in various stages of evolution. With thin layersof blood, early phase ICG images often demonstrateminimal blockage of the large choroidal vessels. In the lateICG study, however, blockage by thin hemorrhage becomesmore prominent which is a result of the reduction of thedegree of background fluorescence from both the choroidand sclera.
Because pre-retinal and subretinal (including sub-retinal pigment epithelial ) hemorrhages tend to be thickerthan intra-retinal hemorrhages, they are more likely toblock fluorescence through out the study.
c. Exudation, Myelination and Scarring: Serous fluid, lipid,inflammatory infiltration and exudation produce variableblocking effect on ICG angiography but is less than thatseen with blood or pigment. An exception is myelinatednerve fibres, which may totally block underlyingfluorescence in both early and late phase of the ICGangiography.
2. Vascular Filling DefectVascular filling defects may be subdivided into (I)
physiologic, (2) vascular occlusion and (3) tissue atrophy.a) Physiologic: Early –watershed zone
Late– silhouette of large choroidal vessels againstbackground fluorescence.
These areas of hypofluorescence occur because of adisparity between the amount of dye present in one areaof fundus compared to an adjacent area.
b) Vascular occlusions: may involve both retinal andchoroidal circulations. Unlike fluorescein angiography,choroidal occlusions are more clearly demonstrated thanretinal vascular defects with ICG angiography.
c) Tissue atrophy: Atrophy of vascular beds occur inconditions such as pathologic myopia and age relatedmacular degeneration.
HyperfluorescenceHyperfluorescence is a relatively bright area on an ICG
angiogram. It may occur in presence of four conditions:pseudofluorescence, transmitted fluorescence, abnormalvessels and leakage.
Pseudofluorescence: It is seen prior to injection of dye andmay be produced by an area of high surface reflectivity inthe fundus or when the barrier and excitation filters of thecamera are not perfectly matched. Dehemoglobinized bloodat the margins of some pigment epithelial detachments inage related macular degeneration are the best example ofthis phenomenon.
Transmitted fluorescence: is most often seen with atrophyof RPE. This results in better definition of underlyingchoroidal vasculature and it is typically manifested as a“window defect” and most typically seen in maculardystrophies, trauma, congenital abnormalities or inspontaneous dehiscence or rip of the RPE. An uncommonform of transmitted fluorescence may be seen in pathologicmyopia.
Abnormal vessels: Although ICG angiography can imageabnormal vessels within the retinal circulation, it is moreadvantageous in imaging choroidal circulatory changes.These changed vessels may be of congenital origin,anomalous configuration, compensatory in response toinflammatory or occlusive changes, new proliferations orneovascularization, present with tumours, or the result ofidiopathic disorders.
Leakage: Leakage is an important form ofhyperfluorescence that is seen in the late stages of the ICGangiograms. Leakage does not typically become evidentuntil at least 10-15 minutes after injection of the dye.Abnormal choroidal vessels and physiologic barriers mayacquire permeability defects that lead to dye diffusion intospaces (pooling) or tissue (staining). Pooling may occurwithin the cystoid spaces of the retina, the subretinal space,and sub retinal pigment epithelial spaces, or in pathologicserous spaces as those seen in tumors. Staining may occuras a result of dye diffusion into the RPE or Bruch’s

DOS Times - Vol. 12, No. 6December, 2006 500
membrane, tissue of the optic nerve,the choroid, or into tumors.Choroidal inflammation also inducestaining of these tissue secondary topermeability defects of the involvedvessels.
Clinical Applications of ICGAngiographyAge Related Macular Degeneration
In exudative ARMD, FAdemonstrates two kinds of choroidalneovessels (CNV) – well defined oroccult CNV. Recent studies have shown improved imagingof occult CNV by ICG angiography. Occult choroidalneovascularization can be subdivided into two groups onICG angiography.1. Focal CNV (Hot Spot):
Focal CNV or a hot spot is a solitary area of welldelineated focal neovascularization and is less than 1 discdiameter in size. It is seen in early to mid phase (Fig.1).2. Plaque:
A plaque is an area of occult CNV larger than 1 discdiameter in size. This may or may not be well defined. Ifthe staining remained well delineated throughout thecourse of the study and the full extent of lesion can bedetermined, a plaque is labeled as well defined. A plaque isclassified as ill-defined if the margins are indistinct or ifthere is blockage of any portion of the neovascularizationby blood. Approximately 60% of the plaques on ICGangiography are ill-defined (Fig.2).
When occult CNV is seen with pigment epithelialdetachment, it is called vascularized PED. ICG angiographyin these cases can show either focal or plaque or combinedlesion.
The relative frequency of these lesions are:-Focal CNV (Hot spot) — 29%Plaque — 61%Combined Lesion — 8%In combined types of occult CNV, hot spots may be
marginal, overlying or remote. Marginal spots are hotspots at the edge of plaque of neovascularization. Overlyingspots are hot spots on top of plaques of neovascularizationand remote spots are hot spots not in contiguity with aplaque of neovascularization.
On ICG angiography, the early staining vessels tend torepresent actively proliferating and highly permeableareas of neovascularization (active occult CNV), whereasthe late staining vessels are more likely to be quiescent orhypovascular areas of neovascularization (inactive occultCNV).
Although ICG angiography is helpful in demarcatingthe occult CNV in many cases, 60% of the plaques are stillill – defined. As the quality of images and their clinicalinterpretation improves, ICG angiography may be able toaddress issues regarding the natural course of plaques,hot spots with or without PED, and the timing and extentof photocoagulation in these cases.
AMD and Feeder VesselsICG can often identify the feeder vessel to a CNV,
especially when images are obtained with scanning laserophthalmoscope. The feeder vessel, once identified, can beclosed with laser treatment, with a success rate of 40% to70%.
Idiopathic Polypoidal Choroidal Vasculopathy (IPCV)Indocyanine green angiography demonstrates a
vascular network overlying the large normal choroidalvessels. Shortly after the vascular network is identified onICG-A, small hyperfluorescent polyps are visible withinthe choroid. These polypoidal structures are round andmost appear at the termini of individual vessels at theborder of the vascular network. The polypoidal structurescorrespond to the reddish-orange choroidal excrescencesseen on clinical examination. These polyps slowly leak dyeduring the course of ICG angiography (Fig.3).
Retinal angiomatous proliferation (RAP)Angiomatous proliferation originates from the retina
and extends posteriorly into the subretinal space,eventually communicating in some cases with choroidalnew vessels. This form of neovascular ARMD, termedretinal angiomatous proliferation (RAP) in this article, canbe confused with CNV. The most common clinical featuresof RAP include retinal and preretinal hemorrhages as wellas pigment epithelial detachments. RAP lesions can beidentified best in the mid or late phases of the ICGangiogram. They are focal areas of hyperfluorescence, so-called “hot-spots,” which increase in intensity as the ICGdye leaks into the surrounding intraretinal and subretinalspaces (Fig.4).
Fig.1: ICG Angiogram showing a focal choroidalneovessel
Fig.2: Late Phase ICG angiogram showing alarge choroidal neovascular plaque
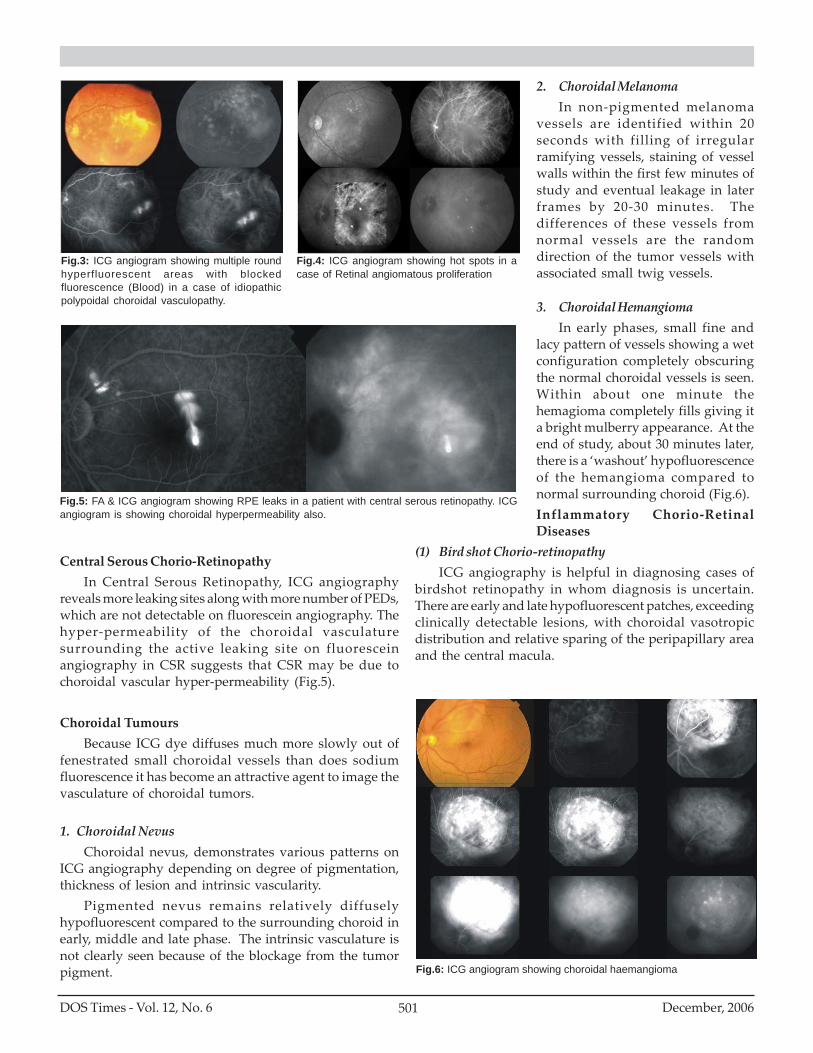
501DOS Times - Vol. 12, No. 6 December, 2006
Central Serous Chorio-RetinopathyIn Central Serous Retinopathy, ICG angiography
reveals more leaking sites along with more number of PEDs,which are not detectable on fluorescein angiography. Thehyper-permeability of the choroidal vasculaturesurrounding the active leaking site on fluoresceinangiography in CSR suggests that CSR may be due tochoroidal vascular hyper-permeability (Fig.5).
Choroidal TumoursBecause ICG dye diffuses much more slowly out of
fenestrated small choroidal vessels than does sodiumfluorescence it has become an attractive agent to image thevasculature of choroidal tumors.
1. Choroidal NevusChoroidal nevus, demonstrates various patterns on
ICG angiography depending on degree of pigmentation,thickness of lesion and intrinsic vascularity.
Pigmented nevus remains relatively diffuselyhypofluorescent compared to the surrounding choroid inearly, middle and late phase. The intrinsic vasculature isnot clearly seen because of the blockage from the tumorpigment.
2. Choroidal MelanomaIn non-pigmented melanoma
vessels are identified within 20seconds with filling of irregularramifying vessels, staining of vesselwalls within the first few minutes ofstudy and eventual leakage in laterframes by 20-30 minutes. Thedifferences of these vessels fromnormal vessels are the randomdirection of the tumor vessels withassociated small twig vessels.
3. Choroidal HemangiomaIn early phases, small fine and
lacy pattern of vessels showing a wetconfiguration completely obscuringthe normal choroidal vessels is seen.Within about one minute thehemagioma completely fills giving ita bright mulberry appearance. At theend of study, about 30 minutes later,there is a ‘washout’ hypofluorescenceof the hemangioma compared tonormal surrounding choroid (Fig.6).Inflammatory Chorio-RetinalDiseases
(1) Bird shot Chorio-retinopathyICG angiography is helpful in diagnosing cases of
birdshot retinopathy in whom diagnosis is uncertain.There are early and late hypofluorescent patches, exceedingclinically detectable lesions, with choroidal vasotropicdistribution and relative sparing of the peripapillary areaand the central macula.
Fig.6: ICG angiogram showing choroidal haemangioma
Fig.3: ICG angiogram showing multiple roundhyperfluorescent areas with blockedfluorescence (Blood) in a case of idiopathicpolypoidal choroidal vasculopathy.
Fig.4: ICG angiogram showing hot spots in acase of Retinal angiomatous proliferation
Fig.5: FA & ICG angiogram showing RPE leaks in a patient with central serous retinopathy. ICGangiogram is showing choroidal hyperpermeability also.

DOS Times - Vol. 12, No. 6December, 2006 502
(2) Acute Multifocal Posterior Placoid PigmentEpitheliopathy (AMPPPE)
ICG angiogram of the acute and subacute lesions inAMPPPE show marked choroidal hypofluorescence,especially in late phases of study. The early phase showslarge choroidal vessels perfusing beneath the areas ofhypofluorescence.
(3) Serpiginous ChoroidopathyIn acute stage there is marked and persistent
hypofluorescence during all phases with ill-definedborders in early phases becoming sharp, well demarcatedborders in late phase. Some hypofluorescent lesions havefaint haloes of hyperfluorescence surrounding them andthey do not correspond to any fluorescein or clinicallyevident abnormality of the retina or RPE.
(4) Multiple Evanescent White Dot SyndromeICG shows pattern of hypofluorescent spots through
posterior pole and peripheral retina which are more innumber and more apparent than fundus or fluoresceinappearance. The hypofluorescent spots appearsapproximately l0 minutes later and last through the studywith no leakage of dye.
Suggested Readings1. Symposium on diagnostic applications of indicator-dilution technics. Proceedings
of staff meetings of the Mayo clinic 1957;32:463-5082. Symposium on diagnostic applications of indicator dilution technics (continued).
Proceeding of the staff meetings of the Mayo clinic 1957;32:509-544.3. Proceedings of the staff meetings of the Mayo clinic 1960;35:729-7824. Diagnostic applications of indicator- dilution technics in congenital heart disease.
Circ. Res. 1962; X : 537-568.5. Freund KB, Yannuzi LA, Orlock DA et al. Interpretation of indocyanine green
angiography. American Academy of ophthalmology; Scientific exhibit, 1995.6. Destro M., Puliafito CA. Indocyanine Green videoangiography of choroidal
neovascularization. Ophthalmology 1989; 96: 846-853.7. Yannuzzi LA, Slakter JS, Sorenson JA et al . Digital indocyanine green video-
angiography and choroidal neovascularization. Retina 1992; 12: 191-223.8. Shiranga F, Shiragami C, Matsuo T. et al. Identification of ingrowth site of idiopathic
subfoveal choroidal neoascualrization by indocyanine green angiography.Ophthalmology 2000; 107 : 600-7.
9. Shiraga F, Ojima Y. Matsuo T, et al. Feeder vessel photocoagulation of subfovealchoroidal neovascularization secondary to age related macular degeneration.Ophthalmology 1998; 105: 662-9.
10. Reichel E, Duker JS, Puliafito CA. Indocyanine green angiograhy and choroidalneovasularization obscured by hemorrhage. Ophthalmology 1995 : 102: 1871 –6
11. Guyer DR, Yannuzi LA, Slakter JS. Sorenson JA, Hope Ross M. Orlock DR. Digitalindocyanine green angiography of central serous chorio-retinopathy. Archophthalmol 1994; 112: 1057-62.
12. Piccolino FC, Borgia L. Central serous chorio-retinopathy and indocyanine greenangiography. Retina 1994; 14: 231-4.
13. Shields CL, Shields JA, De Potter P. Patterns of indocyanine green videoangiographyof choroidal tumor. Br. J. Ophthalmol 1995; 790:237-245.
14. Piccolino FC, Borgia L, Zinicola E. Indocyanine green angiography of circumscribedchoroidal hemangioma. Retina 1996; 16:19-28.
15. Lafant BA, Mestdagh C, Kohno T. et al. Indocyanine green angiography in choroidalosteoma. Graefes Arch Clin Exp Ophthalmol 1997;235:330-7.
16. Yannuzzi LA, Sorenson JA, Guyer DR et al. Indocyanine green angiography : CurrentStatus : Eur J Ophthalmolol 1994; 4: 69-81.

503DOS Times - Vol. 12, No. 6 December, 2006
Carotid cavernous fistulas are abnormal arteriovenousconnections between carotid artery and the cavernoussinus. Associated symptomatology resulting due to theflow of high-flow arterial blood through the low-flowvenous system can be successfully treated by an established& accepted treatment of detachable balloon embolization.
Case ReportA 19 year old Male student presented to us with chief
complaints of progressiveswelling of right upper lidand protrusion of righteyeball for last one week.He gave history of RTA oneand a half months backwith treatment loss ofconsciousness, whichresulted in jaw and orbitalwall fracture. Fracturereduction was done andpatient was doingapparently well thereafterbut he noticed graduallyincreasing swelling andredness in his right eye
1. Deapartment of Ophthalmology2. Department of Neuroendovascular Therapy
Sir Ganga Ram Hospital, Rajinder Nagar,New Delhi
associated with headache and right eye retro-orbitalpain.There was no history of associated diminution ofvision, diplopia, postural variation of protrusion of righteye, fever, discharge, common cold or nose infection, insectbite or tinnitus
On examination patient was fully conscious andoriented with normal systemic examination. Left eye wasessentially normal with unaided vision 6/5P. Vision in righteye was 6/9 with edema of right upper eye lid and 7 mm ofaxial proptosis (as measured with Leuddesexophthalmometer) (Fig.1) . Along with diffuse edema ofboth right upper lid and right lower lid, prominent dilatedvessels were seen over the upper lid. The orbital tensionwas raised with marked inferior chemosis. There wasrestriction of RE movements in all gazes (Fig.2). Pupillaryreactions were normal in both eyes. Bruit was heard overright eyeball. Fundus examination showed dilated andtortuous vessels in the right eye as compared to the left eye(Fig.3a&3b). The IOP in both the eyes was 18 mmHg.
On investigating the patient, biochemical andhaematological investigation were normal. CT Brain withorbital cuts showed right swollen orbital soft tissues withprominent superior ophthalmic vein suggestive of rightsided carotico-cavernous fistula.
In collaboration with the Interventionalneurodiologist, Cerebral digital substraction angiographywas done under local aneasthesia. Bilateral CommonCarotid Arteries (CCAs), Internal Carotid Arteries (ICAs),and Vertebral Artery were selectively catheterized(Fig.4a,5a). On right ICA injection, there was rapid entry ofcontrast into the cavernous sinus (filling the opposite sidealso), drained by markedly dilated superior ophthalmicvein marked in (Fig.4a) and also other orbital veins,pterygoid plexus, petrosal sinuses and clival plexus. Therewas also some retrograde filling into the superficial middlecerebral veins with only faint filling of the right MiddleCerebral Artery (MCA) and right Anterior Cerebral Artery(ACA). The vertebro-basilar system was normal and therewas filling of cavernous sinus through the Carotid
Carotid Cavernous Fistula: A case report1Harbansh Lal MS, 1Anita Sethi MD, FRCS, 2Shakir Hussain MD, DM, FINR, 1Shilpa Taneja DNB
CASE REPORT
Fig.2: Restriction of right eye movements in all gazes
Fig.3a: Right eye FundusPhotograph
Fig.3b: Left eye FundusPhotograph
Fig.1: Right Eye

DOS Times - Vol. 12, No. 6December, 2006 504
Carotid Cavernous Fistula (CCF) on right carotidcompression. Features were suggestive of Right sidedCarotid Cavernous Fistula (CCF) (Type A).
Endovascular balloon occlusion of CCF was donethrough right femoral artery. Using a ‘Gold valve’detachable balloon (Fig.6).
Post-occlusion angiogram showed total obliterationof the CCF with total preservation of the right ICA, withrestoration of right MCA and right ACA filling from rightICA (Fig.4b & 5b). Four days post operatively, the patienthad a rapid resolution of proptosis (Fig.7) with restorationof eye movements (Fig.8) and 6/6 vision in the right eye.
DiscussionCarotid cavernous fistulas (CCF) can be categorized
according to pathogenesis (direct or indirect),hemodynamic profile (high-flow or low-flow) andangiographic anatomy(1). Barrow’s classification schemebased on angiographic anatomy is most widely used aseach type has a characteristic vascular supply whichdetermines the therapeutic approach and also predicts the
Fig. 6: Post-occlusion Right Lateral Digital Substraction angiogram (DSA)scan and plain X-ray showing position of detachable balloon with goldvalve
Digital Substraction angiogram (DSA) scan: Lateral view showingdye injection in right internal carotid artery (RICA) before (Fig.4a) andafter (Fig.4b) balloon occlusion respectively. Fig.4a shows dilatedsuperior ophthalmic vein (arrow)
Digital Substraction angiogram (DSA) Scan: Antero-posterior viewshowing dye injection in right internal carotid artery (RICA) before (Fig.5a)and (Fig.5b) after balloon occlusion respectively.
Fig.7: Pre-op 4 days Post-op
Fig.8: Restoration of right eye movements 4 days post-operatively
4a 4b 5a 5b

505DOS Times - Vol. 12, No. 6 December, 2006
Indirect CCF: Gradual onset with milder presentation.
EtiologyClosed head injury with or without a skull fracture is
the most common cause for direct (Type A) CCF, hence morecommon in young men. Rarely it is seen in older womenwith connective tissue disorders like fibromusculardysplasia, Ehler-Danlos syndrome, Osteogenesisimperfecta etc. (5,6,7).
In cases where no cause is found, spontaneous ruptureof a congenitally weakened or arteriosclerotic non-aneurysmal artery has been hypothesized.
Indirect CCF most coomonly present inperimenopausal female therefore a hormonal mechanismwith estrogen and other hormonal fluctuations has beensuggested(8, 9).
ManagementAn ocular bruit simply leaves no doubt about the
outcome(2).Barrow’s type A fistulas are direct communication
between the ICA and the cavernous sinus. Barrow’s typeB, C, D are indirect (dural) shunts because these fistulasarise from dural arteries and not directly from ICA. Type Bfistulas are between meningeal branches of ICA and thecarotid sinus. Type C fistulas are between meningealbranches of ECA and the carotid sinus. Type D shunts haveconnections between meningeal branches of both ICA andECA. Tomsick further subclassified type D into D1 and D2for unilateral and bilateral ICA and ECA supplyrespectively.
Indirect fistulas are five times more common thandirect ones(3). Amongst the indirect CCFs, Type D are thecommonest(4).
AnatomyCavernous sinus has a unique anatomy because it is
the only anatomic site where an artery passes through avenous space. Thus creation of an arteriovenous fistularequires only rupture of the artery and not simultaneoustrauma to adjacent parts of an artery and a vein (Fig.9).
Pathophysiology & C/FSymptoms and Signs can be correlated well with the
specific anatomy of the Cavernous Sinus. If the retrogradeflow occurs anteriorly to the directly communicatingsuperior ophthalmic vein, the ophthalmic manifestationsare pronounced. If the retrograde flow is more posteriorlytowards the cranial cavity then neurological symptomsand signs become more prominent (Fig.10).
PresentationDirect CCF: Acute onset with overt signs and
symptoms. Usually present with classical triad ofchemosis, pulsatile exophthalmos and ocular bruit.
Retrograde flow anteriorly i.e. towardsSuperior & Inferior ophthalmic veins
↓Dilated orbital venous spaces
↓Congested orbital soft tissues & muscles
↓Arterialization of conjunctival & scleral vessels
– Chemosis
↓Cranial nerve palsies – Ophthalmoplegia (III, IV, VI)
- Ptosis (III)- RAPD (II)
- Decreased Vision (II)
Retrograde flow posteriorly i.e. towardsMeningeal veins eg: sphenoparietal sinus
↓Superior & Inferior petrosal sinus
↓Dilated cerebral venous spaces
↓Disorientation
Ischaemic signs and symptomsCortical & Brain stem dysfunction
Fig.9: Tributaries and Draining channels of Cavernous Sinus(C.S.) - Cavernous Sinus, (ICA) - Internal Carotid A. (Intra carvernouscourse). (V.) - Vein, S. - Sinus, (MCV) - Middle cerebral vein, (F.O.) -Foramen Ovale, (S.F.) - Sphenoidal Foramen, (FL) - Foramen Lacerum
Fig.10: Pathophysiology of CCF

DOS Times - Vol. 12, No. 6December, 2006 506
diagnosis of direct fistulas.But an angiogram is necessary to localize the site of
fistula, for planning the treatment and for diagnosis ofIndirect fistulas.
Sympomatic direct CCF (type A) rarely resolvespontaneously. They almost always require urgenttreatment. The goal of treatment is to stop the retrogradeflow along with maintaining ICA patency. Percutaneoustransarterial endovascular occlusion of fistulas withdetachable balloons with preservation of patency of ICA isthe treatment of choice. Detachable coils too have been usedfor the same.
(Dural) Indirect CCFS, sometimes resolve spontenouslybecause of rethrombosis of the involved segment ofCavernous Sinus. Rate of spontaneous cure followingdiagnosed angiography has been reported to be almost43%(10).
Manual carotid Artery compression is used to treatdural fistulas with a cure rate of approx 30%(11, 12, 13).
In cases of high risk indirect CCF with retrogradecortical venous drainage, progressive ocular symptom,carotid bifurcation, atherosclerosis, neurologic deficittransvenons endovascular embolization has been triedwith success.
ConclusionHigh flow direct CCFs resulting due to the traumatic
fistulous connection between the ICA and the cavernoussinus may present to an ophthalmologist as an acuteproptosed red eye. We present the case to highlight theimportance of early diagnosis and treatment in such cases.
Bibliography1. Debrum GM, Vinuela F, Fox AJ, et al. Indications for treatment and
classification of 132 carotid-cavernous fistulas. Neurosurgery 1998;22:285-289.
2. Barrow DL, Spector RH, Braun IF et al. Classification and treatmentof spontaneous carotico-cavernous fistulas. J Neurosurg1985; 62:248-256.
3. Neurosurgery clinics of North America, Volume 11, Number 1,January 2000; 67-83.
4. Ernst RJ, Tomsick TA:Classification and angiography of carotidcavernous fistulas.In Tomsick TA(ed):Carotid Cavernous Fistulas.Cincinnati, Digital Educational Publishing, 1997, pp 13-21.
5. deCampos JM, Ferro MO, Buraco JA, et al:Spontaneous carotidcavernous fistula in osteogenesis imperfecta.J Neurosurg 56:590-593, 1982.
6. Halbach VV, Higashida RT, Dowd CF, et al:Treatment of carotidcavernous fistulas associated with Ehlers-Danlos Syndrome.Neurosurgery 26:1021-1027, 1990.
7. Heishima GB, Cahan LD, Mehringer CM, et al:Spontaneous arterio-venous fistulas of cerebral vessels in association with fibromusculardysplasia.Neurosurgery 18:454-458, 1986.
8. Newton TH, Hoyt WF:Dural arterioenous shunts in the region ofthe cavernous sinus.Neuroradiology 1:71-78, 1970.
9. Toya S, Shiobara R, Izumi Jet al: Spontaneous carotid-cavernousfistula during pregnancy or in the post-partum stage.JNeurosurg54:252-256, 1981.
10. Phelps CD, Thompson HS, Ossoinig KC:carotid-cavernousfistula(red-eye shunt syndrome).Am J Ophthalmol 93:423-436, 1982
11. Halbach VV, Higashida RT, Hieshima GB: Diagnosis and treatmentof dural arteriovenous fistulae.In Margulis AR, GoodingCA(eds):Diagnostic Radiology.San Francisco, University ofCalifornia press, 1987, pp303-308.
12. Halbach VV:Embolization of dural AVM’s.InValavanisA(ed):Interventional Neuroradiology.Paris, Springer-Verlag, 1993,pp35-57.
13. Higashida RT, Hieshima GB, Halbach VV, et al:Closure of carotidcavernous sinus fistulae by external compression of the carotidartery and jugular vein.Acta Radiol 369(suppl):580-583, 1986.
Monthly Meetings CalendarFor The Year 2006-2007
Dr. Shroff Charity Eye Hospital30th July, 2006 (Sunday)
Venu Eye Institute & Research Centre27th August, 2006 (Sunday)
Centre for Sight24th September, 2006 (Sunday)
Dr. R.P. Centre for Ophthalmic Sciences28th October, 2006 (Saturday)
Midterm Conference of DOS19th November, 2006 (Sunday)
Sir Ganga Ram Hospital26th November, 2006 (Sunday)
Safdarjung Hospital23rd December, 2006 (Saturday)
Army Hospital (R&R)28th January, 2007 (Sunday)Guru Nanak Eye Centre
24th February, 2007 (Saturday)Mohan Eye Institute
25th March, 2007 (Sunday)Annual Conference of DOS
6-8th April, 2007 (Friday, Saturday & Sunday)

507DOS Times - Vol. 12, No. 6 December, 2006
Autorefractometry is an alternative method ofassessing the error of refraction by use of a dedicatedoptical equipment. It is a relaible adjunct to theconventional technique of retinoscopic refraction, whichis time consuming and requires more expertise.
Automated objective refraction began in the late 1930sand has advanced to an extent that today theseinstruments are available and indipensables throughoutthe world. Commercialization of automated objectiveautomated refraction was the result of the electronic,electro-optical and computer revolutions. Far moreefficient, compact and powerful optical detectors(photodiodes and CCD cameras), light sources (highintensity light and infrared emitting diodes), computerdisplays, microelectronic processors, and computermicroprocessors have been incorporated into automatedrefractors. This has made automated objectivemeasurements of refractive status more repeatable ,reproducable faster, user and patientfriendly.
Optical Principles1. Schiener`s Principle (Figure 1)
The refractive error of the eye canbe determined by using doublepinhole apertures before the pupil.(Schiener;1619). A modern version ofthe Schieners principle isaccomplished with infrared lightemitting diodes(IR-LED)that areoptically presented in substitution forthe apertures in a schieners disc.
Autorefractors based on theSchieners principle are the mostcommon automated objectiverefractometers available. They arenulling refractors that opticallysubstitute IR-LEDs for the aperturesof a traditional schieners disc.Projection of NIR into the eye,collection of fundus relexes emittedfrom the eye, and determination ofrefractive status are accomplished
AutorefractionArchana Sood MS
Venu Eye Institute & Research Centre,1/31, Sheikh Sarai, Phase-2,New Delhi-17
using the concept of the Badal optometer. A specializedphotodetection device is employed to analyze the positionof fundus images created by the source optical train andimaged by the detection optical train at the photodetector.The corneal reflex is removed and the vitreoretinal reflexlikely attenuated by the corneal reflex block introducedinto the path of radiation returning from the fundus. Themeridional refractive errors are nulled and the twoprimary meridians of the eye are found by the secondnulling process. The sensetivity (signal/noise ratio)can bebrought to a peak at the point of neutralization.
2. Optometer Principle (Figure 2)This principle permits continuous variation of power
in the refracting instruments.
3. Retinoscopic principlesi) Autoretinoscope based ondirection of fundus streak motion(e.g. ophthalmometron)ii) Autoretinoscope based on speedof fundus streak motion(Nikon,Retinomax)
Autoretinoscopes are meridionalrefractors. The source of optical trainof an autoretinoscope imitates thefunction of a streak retinoscope.Motion of the incident rectangularbeams is usually created by a slotteddrum rotating about a source of NIR.These automated objective refractorsare nulling refractors if based onanalysis of the direction of motion ofthe retinoscopic fundus reflex, whenneutralization is achieved by use of aBadal optometer placed in thedetection optical train of theinstrument. Autoretinoscopes arenon nulling refractors if based on theanalysis of speed of motion of thefundus reflex, where the Badaloptometer is not required.
4. Best- focus principleWhen the image of a target is focussed on the retina,
the eye obtains an image having optimal contrast forprocessing by the visual system. Contrast is lost at the
Fig.1: Scheiner’s principle. Parallel rays oflight entering an emmetropic eye are focusedon the retina (A). Double apertures placed infront of the eye isolate two bundles of thelight passing through the pupil, which are fo-cused as a single spot on the retina in anemmetropic eye (B) and as two small sportsof l ight in the myopic (C) as well ashypremetropic eye (D).
HARDWARE HINTS

DOS Times - Vol. 12, No. 6December, 2006 508
retina when the image is defocussed.Hence if the detection of a change ofimage contrast at the fundus can beautomated, the vergence of incidentradiation necessary to bring aboutmaximum contrast can be captured.The refractive end point of a best focusautorefractor is obtained when thereferred image of a secondary fundussource attains highest contrast at aplane of a photodetection device. (e. g.Electronic Refrationometer, Collins),Dioptron.
Best focus autorefractors are bothnulling and meridional refractors.They find best focus in a meridianthrough the analysis of the contrastof the retinoscopic image. Best focuscorrelates with highest contrast.Neutralization is achieved by use of aBadal optometer placed in thecommon source/detection opticaltrain of the instrument, which refersthe image of the fundus reflex to theplane of a replica of the grating in a rotating drum. Thesensitiveity (signal/noise ratio) can be brought to peak atthe point of neutralization. Only a single photocell isrequired, which allowed Collins (1973) to apply the best-focus principle before photodetectors became sophisticated.The vitreoretinal reflex, corneal reflex, and coaxial reflexesfrom the extensive common optical path can be filtered bypolarization and removal of polarized NIR returning fromthe eye at the common beginning and end of the opticalpath. Coaxial optical elements may also be tipped withrespect to the detection train's optical axis, therebyreflecting unwanted NIR out of the detection system.
5. Knife- edge principleThe Foucault knife-edge test has long been used to
evalutate the refractive uniformity of mirrors and lenses.The knife-edge principle is related to retinoscopy and isthe basis of photorefraction. The image of a point source isfocused at the linear edge of a flat opaque surface, or knifeedge, from which the technique takes its name. When usedto test the refractive uniformity of a normal lens, the knifeedge is used as a source located in front of the lens, and amirror is placed behind the lens so as to retroreflect lightfrom the knife edge. By moving the retroreflector or theknife edge in an axial direction along the optic axis of thelens, the knife edge and its image can be made opticallyconjugate. Then, by the principle of reciprocity (orreversibility) in optics, all light returning through thesystem passes completely back into the source.Theoretically, no light should escape past the knife edge.
eg. Humphrey autorefractor
6. Ray- deflection principleWhen rays of light or NIR from a
small illuminated patch of fundus exitthe eye, they are refracted to an imageof the secondary fundus source alongthe optic axis of the eye. If the eye isemmetorpic, the rays exit the eyeparallel to each other. As hs alreadybeen noted, the rays are deflectedtoward a focus in front of the myopiceye in the far-point plane, and theyare deflected as if they came from theplane of a far point in back of thehyperopic eye. The angle of deflectionthat an exiting ray makes with respectto collimated parallel rays, therefore,indicates the type and magnitude ofthe eye's ametropia. eg. Canonautorefractor
7. Image-size principleThe size of the optical image on
the retina is a function of the refractive error. The refractivestatus may, therefore, be determined by measuring thesize of an annular secondary fundus source and, in thecase of astigmatism, the lengths and meridionalorientations of the major and minor axes of the ellipticalfundus reflex. To do this the detection system consists ofwhat is essentially a fundus camera: A CCD camera is usedas the detector. A computer analyzes the image to measurethe digital image of the secondary source created at thedetection surface of the CCD camera.
Topcon was first to apply the assessment of fundusreflex image size in the manufacture of autorefractors (figure 19-41A). An interesting instrument that also usesthe principle is the handheld autorefractor offered byGrand Seiko.
Interesting History factsCollins(1937) developed the first semiautomated
objective refractometer(electronic refractionometer). Safir(1964) automated the retinoscope and this work led to thefirst commercial autorefractor-the Ophthalmometron.6600 Autorefractor was the second commercialautorefractor (1969). Munnerlyn (1978) design using a bestcontrast principle with moving gratings led to theDioptron, an automated objective refractor.
Basic Optometer types1. Early subjective optometers
These instruments required the patients to adjust the
Fig.2: The optometer principle.Refractometerbased on this principle uses a single converginglens.(A)Light from a target on the far side ofthe lens may enter with zero(B), minus (C) orplus (D) Vergence. The scale used in optometerwould show the amount of ametropia in dioptres

509DOS Times - Vol. 12, No. 6 December, 2006
instrument for best focus or alignment of target parts. Theywere unsuccessful because of instrument accomodation. e.g Badal’s optometer, Young’s optometer
2. Early objective optometersThey were based on the optometer principle as well as
the schieners principle incorporated in most of them e. g.a. The Rodenstock refractometer
Based on schiener principle which depends on unitingtwo separate pathway of rays.b. Zeiss-Jena coincidence refractionometer
This instrument also uses the principle of the image onthe retina not lying on the axis of the system except whenthe axial test object is conjugate with the retina (schienerdisc principle)c. The Fincham coincidence optometer
A doubling device is used in the observation system.The target is viewed through a system of prisms, whichdivides the field into two halves. When it is not in a positionconjugate to the subject’s retina, the retinal image isdisplaced from the axis, otherwise the two halves arealigned.
Problems encountered with these devices are proximalaccomodation, small pupils, hazy media, ametropia andhigh astigmatism
Limitations of early optometers1. Alignment problems(both pinhole apertures must fitwithin the pupil)2. Irregular astigmatism(the best refraction over thewhole pupilmay be different in contrast to the two smallpinhole areas of the pupil).3. Accomodation(the instrument myopia alters theactual refractive status of the patient)
Modern refractometersThey can be grouped as:
a. Based on Instrument design and method
ObjectiveThe patient, s whole pupil is used in this system thus
avoiding some of the alignment and partly irregularastigmatism. The operator focusses a single spot of lighton the patient, s retina and measures the astigmatism bysuccessively focussing the two focal lines. In order tocontrol accomodation, the eye not being refracted is foggedby a trial lens through which the patient fixates at a distanttarget. e. g. Automated infrared optometers
(Nikon autorefractometer NR 1000F, AR2000, Canon
autoref R-1, Shin-Nippon SR 7000, Humphery automaticrefractometer, Dioptron, Nidek AR 2000)
Photorefractors (Fig 3)These devices capture images of the fundus reflexes
from the two eyes of the patient simultaneously, producedby a flash of visible light from a camera. The fundus reflexescan be captured on film, digitally, or by video and thensubjected to analysis.
Electrophysiological methods (Fig 4)Subjective
E. g. Laser speckle pattern refractiona. Multimeridonial refractometry
Computer actuated refractionInstruments having continuously variable
spherocylindrical power(Vision analyzer, SR 4 programmed subjective
refractor, Subjective autorefractor)b. Based on Operational method use1. Analysis of image quality
(Dioptron, Canon autorefractors, Hoya Autorefractors)
Fig.4: Laser speckle pattern refraction.
Fig.3: Grolman photographic system for objective refraction.

DOS Times - Vol. 12, No. 6December, 2006 510
2. Retinoscopic scanning(Ophthalmetron, Humphery autorefractor, Nikon 5000,
7000)3. Schiener disc refraction
(6600 Autorefractor, Nidek and Topcon autorefractors)Description of some important Modern Refractometers
Automated Infrared refractorsThe refraction is performed automatically by use of
near infrared light (NIR) at wavelengths between 800 and900nm, which is invisible to the patient. This propertyprevents photophobia, pupillary constriction andaccomodation. NIR is also efficiently reflected back fromthe fundus. The principle intraocular absorbers of visiblelight(melanin, haemoglobin and xanthophyll) arerelatively ineffective at absorbing NIR. Thus more NIR isreflected from the fundus than if visible light or other formsof electromagnetic radiation were used
A visible fixation light is provided in each instrumentin order to control the patient’s fixation and accomodation.Since the eye is not achromatic, an allowance has to bemade for the difference in ocular refraction between visiblelight and the wavelength of infrared radiation. This isusually about 800 to 900nm, for which the eye is 0. 75 to 1.00 DS hypermetropic relative to 550nm. Thus about 0. 5 to0. 75D allowance has to be made in addition to the effects ofchromatic aberration. This suggests that the infraredradiation is either being reflected from the capillary bed ofthe retina, about 0. 3mm in front of receptors or that it isreflected from several layers, the mean effect beingequivalent to reflection from a single plane in front of thereceptors.
It has been postulated that light which retains its planeof polarization on reflection by the fundus was reflectedfrom the anterior layers of the retina, while diffuselyreflected light may even be reflected from the sclera. Thiscould give a difference between those instruments usingpolarizing radiation, e. g. Dioptron and those withoutpolarization, e. g. Humphery autorefractor.
These instruments demonstrate one of the three basicprinciples upon which all current optometers are based.These basic principles and the optometers which utilizethem are:1. Scheiner Disc principle. The objective refractors based
on this optical principle are: Mark IX 6600autorefractor, Topcon RM-200 Band Nidek AR 2000.
2. Grating focus principle. Dioptronultima, DioptronNova and canon autoref R-1.
3. Retinoscopy illumination system is used in Nikon NR1000F and Ophthalmetron.A few of the objective autorefractometers available
commercially are discussed here.
1. DioptronIt is a fully objective infrared refractometer. Once
aligned with the eye it performs a spherocylinderrefraction, the results of which are printed out on a smallcard. It is based on a grating focus principle. the infraredlight is filtered from incandescent source. The instrumentfinds best focus in two arbitrary meridia, scans180 degreefor peaks, then measures successively in six meridian. Thecomputer then calculates the refractive correction by fittinga sine 2 curve to the 5 best data points.2. Nikon Autoref NR-1000F
This infrared optometer uses the principle ofretinoscopy in the illuminating system and the Schienerprincipal in the detection system. Speed of retinoscopicreflex is determined in each meridian as the instrumentsweeps through 360 in 0.5 seconds. Sphere, cylinder andaxis are calculated from the resulting data. Findings areshown on digital display.3. Canon Autoref. R-1. It is based on the 'grating focusprinciple'. Target consists of three gratings. The best focusfor the three separate gratings oriented 60 degree apart isdetermined during a 2 second sweep through the entirepower range. This has the fastest measurement time of allthe automated refractors. The refractions correction isautomatically calculated by fitting a sine 2 curve to thethree data points.4. Nidek AR 2000 Objective Automatic Refractor. It is aninfrared optometer that uses a straightforward Scheinersystem to measure through a 180 degree sweep in 1. 5seconds. Sphere, cylinder and axis are automaticallydtermined from the resulting curve.5. Humphrey Automatic Refractor. It hasspherocylindrical optical system using two variable acrosscylinders (Stokes lenses) in an optometer arrangement. Thewhole pupil is used during the refraction. A variation ofthe knife edge optical testing principle is used with thespherocylindrical optics being changed until no furtherrefractive error is detected. This is the only automatedobjective refractor to provide visual acuity measurementboth before and after the refraction.
Subjective InstrumentsSubjective instruments are not very commonly used
in the recent times.A few of the new subjective refractors which have been
available commercially are as follows:1. Vision Analyzer. It was introduced by Humphrey in
1975. in 1977 it was combined with the HumphreyLens Analyzer to form the over refraction system. TheVision Analyzer uses an innovative optical system andequally innovative methods for subjective refraction.
2. SR-IV Programmed Subjective Refractor. This

511DOS Times - Vol. 12, No. 6 December, 2006
instrument uses the optometerprincipal with an axially movingcylindrical lens to achievesmoothly variablespherocylindrical power over awide range. Clinical trials of theSR-IV indicate the Simulcrosssystem provides results that areat least as accurate as thoseobtained with conventionalsubjective techniques. But,undoubtedly the Simulcrosstesting is faster and easier for boththe patient and the operator.
3. Subjective Autorefractor-7. Thisinstrument has spherical opticsonly. Because no refinement of theastigmatic correction is possibleand because visual astigmaticcorrection is possible and becausevisual acuities can be determinedonly with spheres, the 'SubjectiveAutorefractor-7' can beconsidered only a screeninginstrument.
Conditions producing invalid autorefractive resultsAmetropias outside the range of the instrumentSmall pupilsAnt. seg abnormalities resulting in opacities, cloudyocular media, distorted pupils, irregular astigmatismas in keratoconus, corneal trauma, post refractivesurgeriesPost. seg problems like retinal detachment,staphylomas, retinopathiesAccommodative abnormalities as in latent hyperopia,psuedomyopia
Brief Abstract reviewPseudophakic autorefraction
Autorefraction can provide acceptably accuratepostoperative refraction values in pseudophakic eyesAutomated refraction with the Canon RK-1 Autorefkeratometer was evaluated by P. S Raj et al in 110 eyes (110patients) six to eight weeks after they had undergoneextracapsular cataract extraction with posterior chamberintraocular lens implantation and achieved a bestcorrected visual acuity of at least 6/12. Autorefractionreadings were obtained in 100 (91%) of these eyes. Theagreement between autorefraction and clinical refractiondata was 98% for spherical equivalence less than 0. 51dioptres (D), 95% for sphere power less than 0. 51D, 94%
for cylinder power less than 0. 51D, and 85% for cylinderaxis less than 11 degrees.
Paediatric autorefractionA comparison of autorefraction and subjective
refraction with and without cycloplegia was done byChoong YF et al in primary school children.
The accuracy of autorefraction was evaluated usingthree autorefractors comparing to subjective refraction indiagnosing refractive error in children. It was a cross-sectional community based study. with a study populationof 117 children sampled from primary schools. All subjectsunderwent autorefraction using three auto refractors andsubjective refraction with and without cycloplegia. mainoutcome measures: Spherical power, cylindrical power, andspherical equivalence (SE). Without cycloplegia, the meanSE were significantly different for Retinomax K plus2 (-1.55 diopters, SD 2.37 diopters;) and Canon RF10 (-1.11diopters; SD 2.61 diopters;) compared with monocularsubjective refraction (-0.80 diopters; SD 2.25 diopters;).Mean SE was significantly different for Grand SeikoWR5100K (-0. 79 diopters; SD 2. 40 diopters; compared withbinocular subjective refraction (-0.62 diopters; SD 2.51diopters; With cycloplegia, there was no significantdifference in mean SE between refraction methods. Undernoncycloplegic conditions, all three autorefractors have atendency towards minus over correction in children
Comparison between Subjective & Objective Instruments
Objective Subjective
Source of Light Infra-red light Visible LightTime Required 2-4 min 4-8 min
Information provided Less informative More informative (correctedvisual acuity)
Patient Co-operation Required less (only More Co-operation (Patienthas to look straight has to turn knob, focus target,at target) answer questioins about
appearance of target)
Ocular factors Better in Macular Can be done in hazy oculardieases with clear mediaocular media
Over refraction Difficult No problemcapability withspectacles , CL, IOL
Expected results Preliminary Gives refined subjectivesrefractive findings results.only. Practitionerhas to refine thefindings

DOS Times - Vol. 12, No. 6December, 2006 512
resulting in over diagnosis of myopia.However autorefractors wereaccurate under cycloplegic conditions.
Autorefraction and PRK treated eyesThe relative accuracy of
autorefraction and autokeratometry(autorefraction/autokeratometry)and subjective refraction in untreatedand photorefractive keratectomy(PRK)-treated eyes was studied byOyo Szerenyi et al. The results ofautorefraction/autokeratometryobtained by means of 2 contemporarydevices (Nidek ARK 2000 and CanonRk-3) were compared with those ofsubjective refraction in 48 untreatedeyes and in 78 eyes treated with (PRK).
A trend toward greater differences between subjectiveand objective methods in PRK-treated eyes was observed.Both autorefraction devices showed similarly higherdifferences from subjective readings in PRK-treated eyeswith regard to sphere (P < . 001) and cylinder (P = . 02), butnot axis (P =. 4). For autokeratometry, the mean differencefrom manual readings was highly significant when all Kreadings were considered together, but not so for theindividual differences in keratometric astigmatism (CanonRK-3 and Nidek ARK 2000 vs manual results: P =. 03 and P=. 93, respectively) and keratometric axis (Canon RK-3 andNidek ARK 2000 vs manual results: P =. 88 and P =. 19,respectively). Refractive and keratometric readingsobtained with the automated devices tested in this studyvaried more from those obtained with subjective methodswhen the eyes examined had been treated with PRK.Corneal topographical changes inherent in the wound-healing process may influence objective measurement withautomated devices.
Promising new method of IOL calculation: intraoperativeaphakic autorefraction
A recent study by Ianchulev et al shows promisingresults for an alternative method of IOL calculation usingoptical refractive biometry. The new method,intraoperative autorefractive retinoscopy, does not relyon axial length or keratometry readings, as do conventionalIOL calculations.
In the study, a pilot group of 22 patients underwentstandard cataract surgery and IOL implantation. Thepower of the IOL was calculated by conventional biometricmeasurements and IOL calculations. Intraoperativeautorefractive retinoscopy, which takes 2 or 3 minutes,was performed to obtain an aphakic refraction andspherical equivalent prior to lens implantation. Usinglinear regression, the aphakic spherical equivalent was
correlated to the final adjustedemmetropic IOL power to derive aformula for IOL calculation, known asthe optical refractive biometrymethod. A second validation series of16 eyes was used to directly compareoptical refractive biometry to theconventional IOL formula.
The study showed a statisticallysignificant relationship betweenaphakic spherical equivalent and finalIOL power. This relationship wassustained over an axial length range(21. 43 mm-25. 25 mm) and an IOLrange (12. 0 D-25. 5 D). In the validationseries, the optical refractive biometrymethod proved to be better thanconventional formulas at predicting
emmetropic IOL (plus or minus 1. 0 D) in post-LASIKpatients (83 percent vs. 67 percent, respectively).
In postrefractive surgery patients who developcataracts, IOL calculations are known to be inaccurate.This is largely due to inadequacies of measuring truecorneal power after refractive surgery. With this newmethod of IOL calculation, some limitations ofconventional biometry can be avoided, which could bebeneficial for these patients.
ConclusionAutomated refractors promise to relieve the
practitioner from the necessity of performing staticretinoscopy. But it is important to note that anautorefractionshould not be used as the final refractivecorrection without further confirmation. Hence theautorefractor should be used primarily to determineaninitial objective refraction prior to performance of thesubsequent subjective refraction.
References1. Campbell E. Charles, BenjaminJW, Howland CH. Objective
refraction:retinoscopy, autorefractionand photorefraction. Borish`sClinical refraction by William J Benjamin. I1st edition, W. B. SaundersCompany, Pennsylvania. 585-626.
2. Choong YF, Chen AH, Goh PP. A comparison of autorefractionand subjective refraction with and without cycloplegia in primarychildren school Am J Ophthalmol. 2006 Jul;142(1):68-74.
3. PS Raj, T Akingbehin and AM Levy Objective autorefraction inposterior chamber pseudophakia British Journal of Ophthalmology,1990, Vol 74, 731-733.
4. K. D. Oyo-Szerenyi, L. Wienecke, U. Businger and I. SchipperAutorefraction/autokeratometry and subjective refraction inuntreated and photorefractive keratectomy treated eyes.
5. Ianchulev T, Salz J, Hoffer K. Intraoperative optical refractivebiometry for intraocular lens power estimation without axial lengthand keratometry measurements. J Cataract Refract Surg.2005;31:1530-1536.
POTEC Auto refrakto-keratometer PRK-5000

513DOS Times - Vol. 12, No. 6 December, 2006
Allvar Gullstrand, eldestson of Dr. Pehr AlfredGullstrand, PrincipalMunicipal Medical Officer, andhis wife Sofia was born on June5, 1862, at Landskrona,Sweden. He passed hismatriculation in 1880 and thenwent to Uppsala University,which he left in 1885, andspent a year at Vienna. Hecontinued his medical studiesat Stockholm where he
graduated in medicine in 1888, and was appointed aLecturer in Ophthalmology in 1891. After holding variousappointments as Doctor and Lecturer and serving on theSwedish Medical Board, he was appointed the firstProfessor of Ophthalmology at Uppsala University in 1894.He occupied this post until 1913 and 1914 onwards held aPersonal Professorship in Physical and PhysiologicalOptics at Uppsala University. He was appointed EmeritusProfessor in 1927.
He was entirely self-taught in the fields covering hismost important work on geometric and physiologicaloptics. The basis of the science he developed was laid in1890 in his thesis Bidrag till astigmatismens teori(Contribution to the theory of astigmatism). The completeproof of this theory is found in the following three works:i) General theory of monochromatic aberrations and theirimmediate significance for ophthalmology, 1900, whichreceived awards from the Swedish Royal Academy ofSciences and the Swedish Medical Association; ii) The trueoptical image, 1906; and iii) The optical image inheterogeneous media and the dioptrics of the humancrystalline lens, 1908, which was awarded the CentenaryGold Medal of the Swedish Medical Association.
One of the first individuals to apply microscopy to theliving eye was Purkinje, who in the 1820s studied the iriswith an adjustable microscope by illuminating the field ofview. The uniocular slit lamp was born later when Louisde Wecker combined an eyepiece, objective and adjustablecondensing lens within a tube. Wecker's invention wasimproved upon by Siegfried Czapski, who addedbinocularity to the microscope. However, none of the unitsconstructed by these individuals had sufficient andadjustable illumination to be of much clinical benefit.
A peep in the past: Allvar GullstrandLt. Col. Rakesh Maggon, Col. J.K.S. Parihar, Lt. Col. Vijay Mathur
Department of OphthalmologyArmy Hospital (R&R), Delhi Cantt,New Delhi
Gullstrand developed a first true slit lamp to illuminatethe eye. The modern slit lamp bio-microscope became apowerful diagnostic tool capable of stereoscopicallyexamining optical sections of the anterior segment in greatdetail. The instrument was not only important as anessential diagnostic tool in the clinic, but also served togreatly advance the scientific knowledge ofOphthalmology.
Gullstrand contributed to knowledge of the structureand function of the cornea and to research on astigmatism.He improved corrective lenses for use after surgery forcataracts. His investigations led to a new concept of thetheory of optical images. He expanded the classic theory ofthe German physicist Hermann von Helmholtz to includethe redisposition of internal parts of the lens structure inaccommodation, a mechanism by which the eye can focusfor near or far vision within certain limits. Gullstrandshowed that although accommodation depends about two-thirds on the increase in convexity of the lens surface, theremaining one-third does not.
In 1911 he received the Nobel Prize for Physiology forhis work on the dioptric apparatus of the eye that heperformed jointly with Moritz von Rohr, and with thisthey placed the correction of refractive errors in the eye bymeans of eyeglasses on a strictly scientific basis. He wasmember of the Nobel Physics Committee of the SwedishAcademy of Sciences (1911-1929), and its Chairman (1922-1929). It is said that Albert Einstein was denied Nobel Prizefor his work on relativity only because Gullstrand wasnot convinced about the theory of relativity. In 1928 hewas awarded the Graefe Medal by German Society ofOphthalmology, an honour bestowed only once every tenyears. In 1885 he married Signe Christina Breitholtz. Theyhad one daughter, who died at an early age. Gullstranddied in Stockholm on July 28,1930.
PEEP IN THE PAST