top five papers in infectious disease pharmacotherapy · chart title quinolone ceftazidime cefepime...
TRANSCRIPT
Top Five Papers in Infectious
Disease Pharmacotherapy
Elizabeth Neuner, PharmD, BCPS (AQ-ID)
OSHP Spring Meeting
April 24th 2015
Learning Objectives
1. Review data from recent studies
assessing antimicrobial dosing strategies
and impact on clinical outcomes.
2. Discuss the impact of recent literature on
the selection of antimicrobials for various
health-care associated infections.

Methods
PubMed Search: Jan-Dec 2014
“Infectious Diseases”
N = 20,126
Houston ID Network: ID Pharmacotherapy
SIDP Survey
N = 27
Health-System
Pharmacists
SIDP = Society of Infectious Diseases Pharmacists
Other Excellent Papers
• Phe K, et al. AAC 2014;58(5):2740-6 (Polymixins Nephrotoxicity)
• Felton TW, et al. Clin Pharmacol Ther. 2014; 96(4): 438-48. (Pip-tazo)
• Spoorenberg V, et al. CID 2014; 58(2): 164-9. (UTI)
• DiazGranados CA, et al. NEJM 2014;371(7):635-45 (Influenza vaccine)
• Ahmed F, et al. CID 2014;58(1):50-57. (Influenza vaccine)
• Knoll GA, et al. JAMA 2014;312(20):2106-14. (BK virus)
• Afdhal N, et al. NEJM. 2014; 370(16): 1483-93. (Hepatitis C)
• Zeuzem S, et al. NEJM 2014;370:1604-1614. (Hepatitis C)
• Feld JJ, et al. NEJM 2014;370(17):1594-1603. (Hepatitis C)
• Corey GR, et al. NEJM 2014;370(23):2180-90. (Oritavancin)
• Moran GJ, et al. Lancet Infect Dis 2014;14(8):696-705. (Tedizolid)
• Boucher HW, et al. NEJM 2014;370(23):2169-79. (Dalbavancin)
• Ostrosky-Zeichner L, et al. CID 2014;58(9):1219-26. (Fungal infections)
• Beyda ND, et al. CID 2014;59(6):819-25. (Fungal infections)

β-Lactam PK in Sepsis: Background
• β-lactams commonly used in sepsis
• Dosing typically derived from healthy volunteers, less critically ill patients, and/or PK simulations
- PK-PD target: Time > MIC
• Critically ill patients have variable and often altered PK
- Larger volume of distribution
- Augmented renal clearance
- Low plasma albumin concentrations
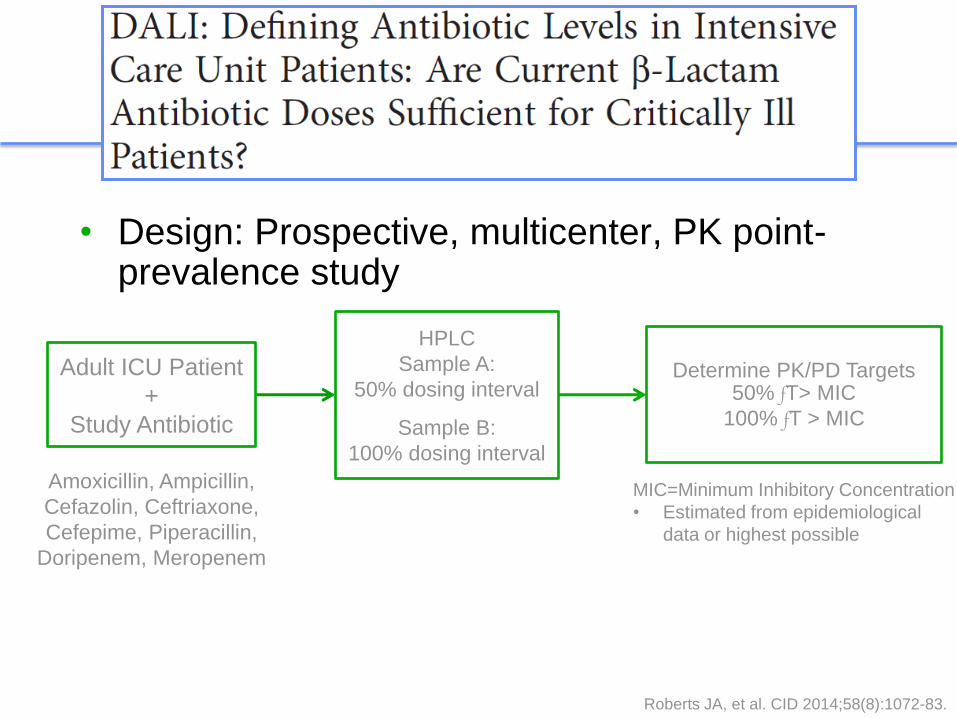
• Design: Prospective, multicenter, PK point-prevalence study
Roberts JA, et al. CID 2014;58(8):1072-83.
Adult ICU Patient
+
Study Antibiotic
Amoxicillin, Ampicillin,
Cefazolin, Ceftriaxone,
Cefepime, Piperacillin,
Doripenem, Meropenem
HPLC
Sample A:
50% dosing interval
Sample B:
100% dosing interval
Determine PK/PD Targets 50% fT> MIC
100% fT > MIC
MIC=Minimum Inhibitory Concentration
• Estimated from epidemiological
data or highest possible
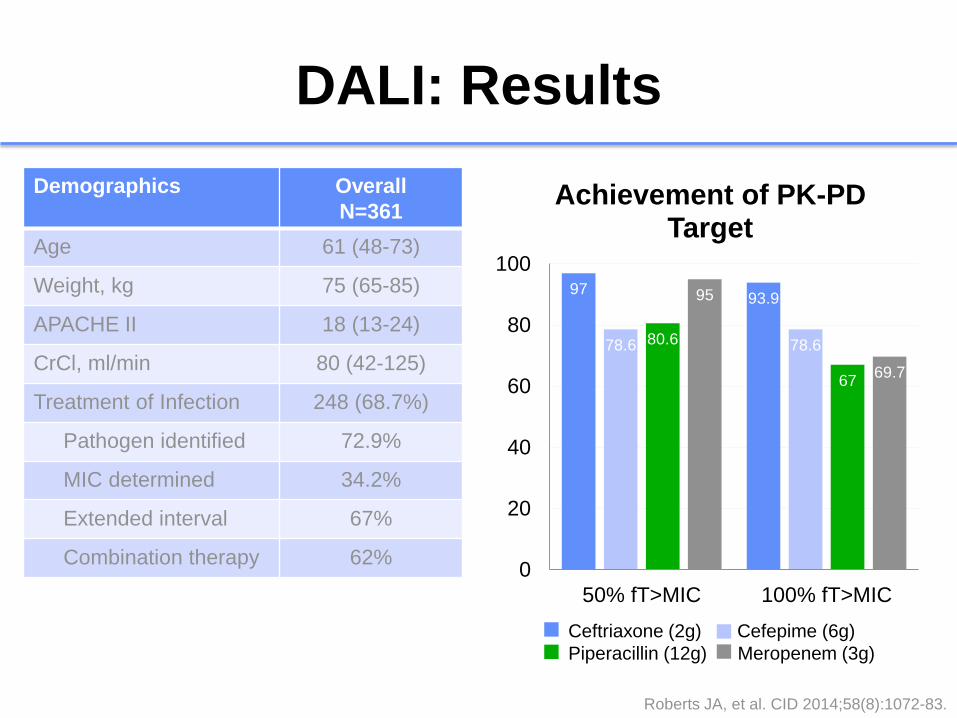
DALI: Results
Demographics Overall
N=361
Age 61 (48-73)
Weight, kg 75 (65-85)
APACHE II 18 (13-24)
CrCl, ml/min 80 (42-125)
Treatment of Infection 248 (68.7%)
Pathogen identified 72.9%
MIC determined 34.2%
Extended interval 67%
Combination therapy 62%
97 93.9
78.6 78.6 80.6
67
95
69.7
0
20
40
60
80
100
50% fT>MIC 100% fT>MIC
Achievement of PK-PD Target
Ceftriaxone Cefepime
Piperacillin Meropenem
Ceftriaxone (2g) Cefepime (6g)
Piperacillin (12g) Meropenem (3g)
Roberts JA, et al. CID 2014;58(8):1072-83.
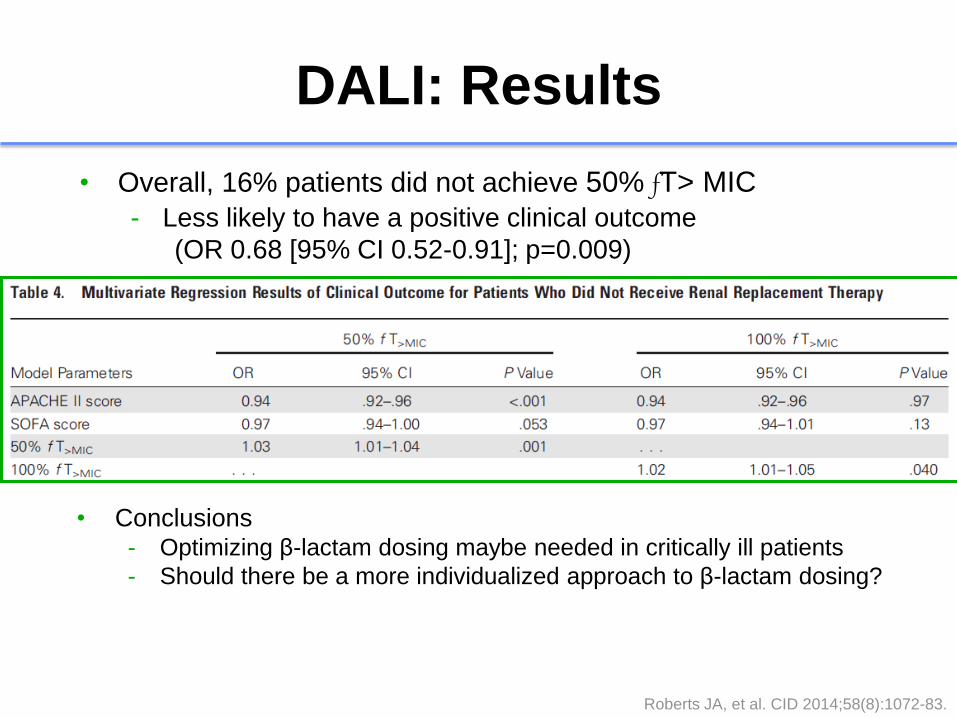
DALI: Results
• Overall, 16% patients did not achieve 50% fT> MIC
- Less likely to have a positive clinical outcome
(OR 0.68 [95% CI 0.52-0.91]; p=0.009)
• Conclusions - Optimizing β-lactam dosing maybe needed in critically ill patients
- Should there be a more individualized approach to β-lactam dosing?
Roberts JA, et al. CID 2014;58(8):1072-83.
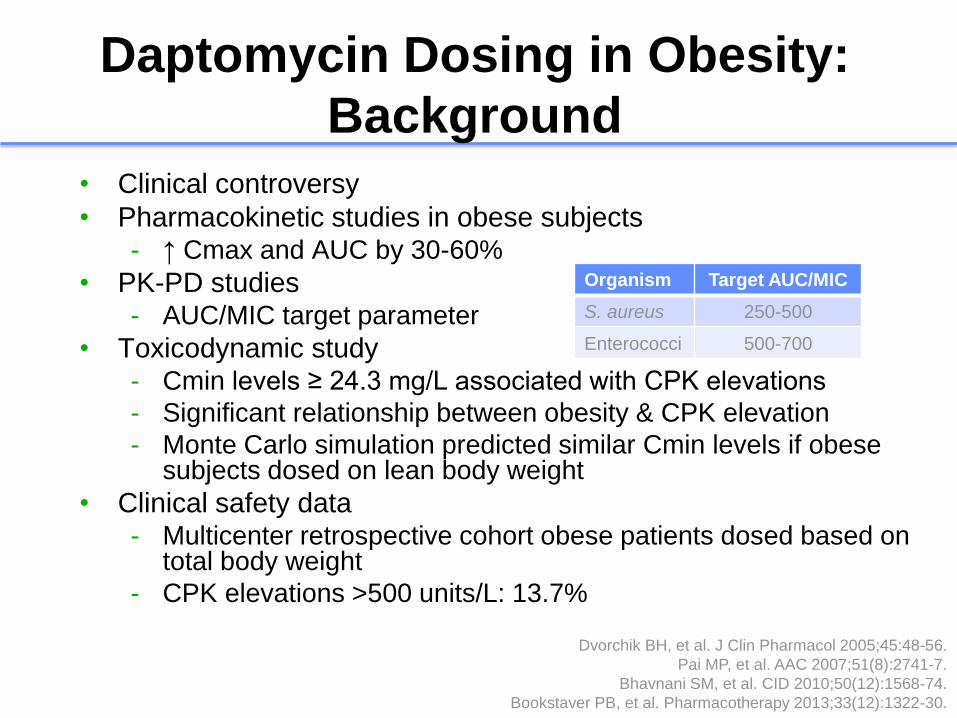
Daptomycin Dosing in Obesity:
Background
• Clinical controversy
• Pharmacokinetic studies in obese subjects - ↑ Cmax and AUC by 30-60%
• PK-PD studies - AUC/MIC target parameter
• Toxicodynamic study - Cmin levels ≥ 24.3 mg/L associated with CPK elevations
- Significant relationship between obesity & CPK elevation
- Monte Carlo simulation predicted similar Cmin levels if obese subjects dosed on lean body weight
• Clinical safety data - Multicenter retrospective cohort obese patients dosed based on
total body weight
- CPK elevations >500 units/L: 13.7%
Dvorchik BH, et al. J Clin Pharmacol 2005;45:48-56.
Pai MP, et al. AAC 2007;51(8):2741-7.
Bhavnani SM, et al. CID 2010;50(12):1568-74.
Bookstaver PB, et al. Pharmacotherapy 2013;33(12):1322-30.
Organism Target AUC/MIC
S. aureus 250-500
Enterococci 500-700
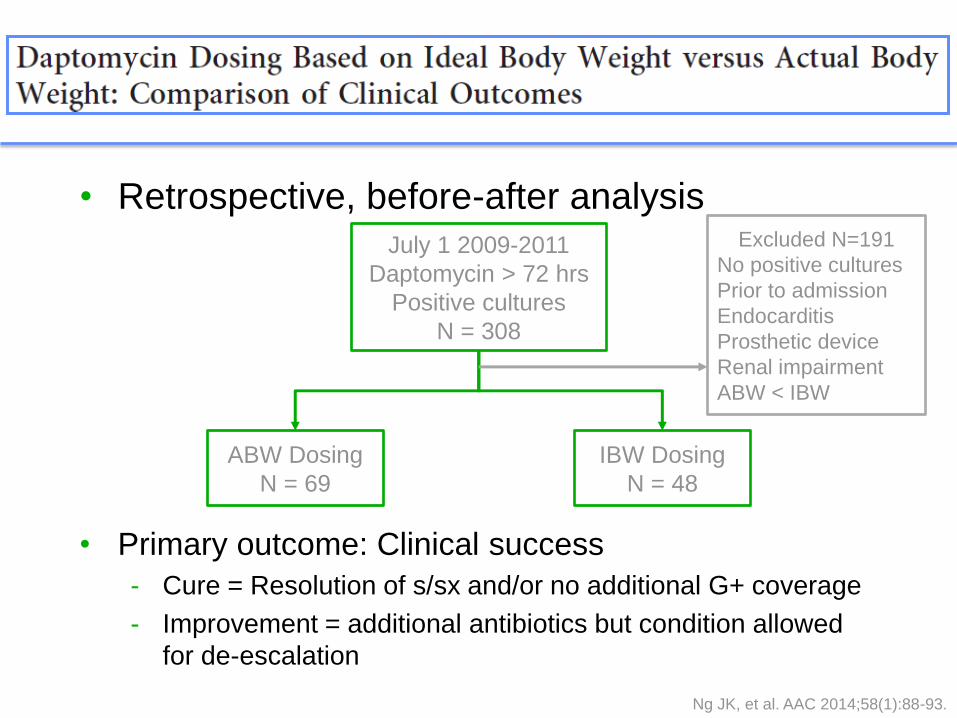
• Retrospective, before-after analysis
Ng JK, et al. AAC 2014;58(1):88-93.
July 1 2009-2011
Daptomycin > 72 hrs
Positive cultures
N = 308
Excluded N=191
No positive cultures
Prior to admission
Endocarditis
Prosthetic device
Renal impairment
ABW < IBW
ABW Dosing
N = 69
IBW Dosing
N = 48
• Primary outcome: Clinical success
- Cure = Resolution of s/sx and/or no additional G+ coverage
- Improvement = additional antibiotics but condition allowed
for de-escalation
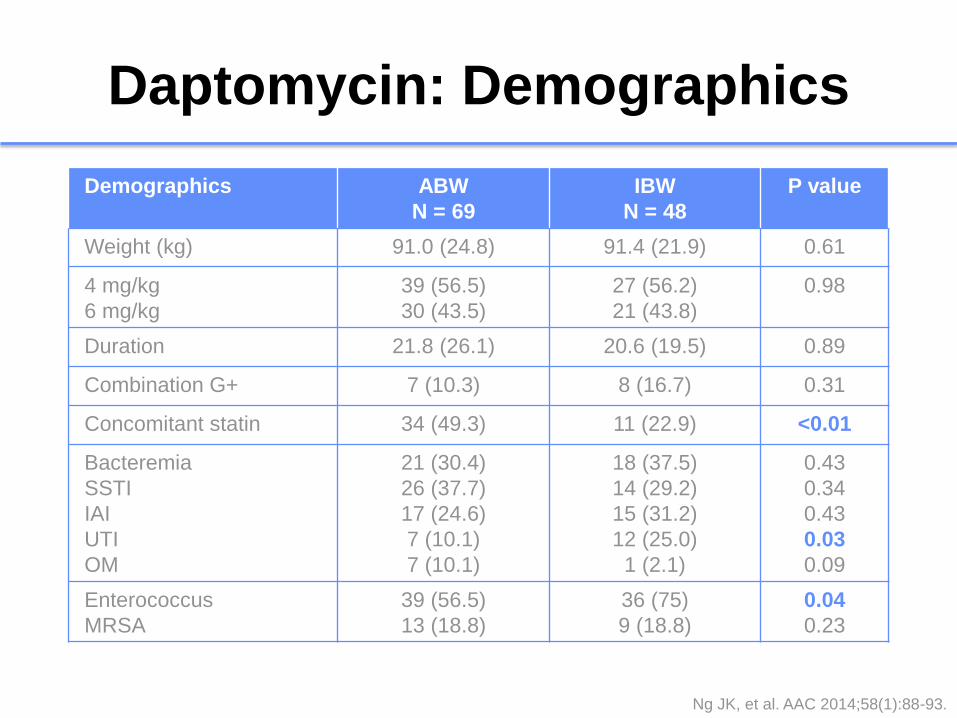
Daptomycin: Demographics
Demographics ABW
N = 69
IBW
N = 48
P value
Weight (kg) 91.0 (24.8) 91.4 (21.9) 0.61
4 mg/kg
6 mg/kg
39 (56.5)
30 (43.5)
27 (56.2)
21 (43.8)
0.98
Duration 21.8 (26.1) 20.6 (19.5) 0.89
Combination G+ 7 (10.3) 8 (16.7) 0.31
Concomitant statin 34 (49.3) 11 (22.9) <0.01
Bacteremia
SSTI
IAI
UTI
OM
21 (30.4)
26 (37.7)
17 (24.6)
7 (10.1)
7 (10.1)
18 (37.5)
14 (29.2)
15 (31.2)
12 (25.0)
1 (2.1)
0.43
0.34
0.43
0.03
0.09
Enterococcus
MRSA
39 (56.5)
13 (18.8)
36 (75)
9 (18.8)
0.04
0.23
Ng JK, et al. AAC 2014;58(1):88-93.
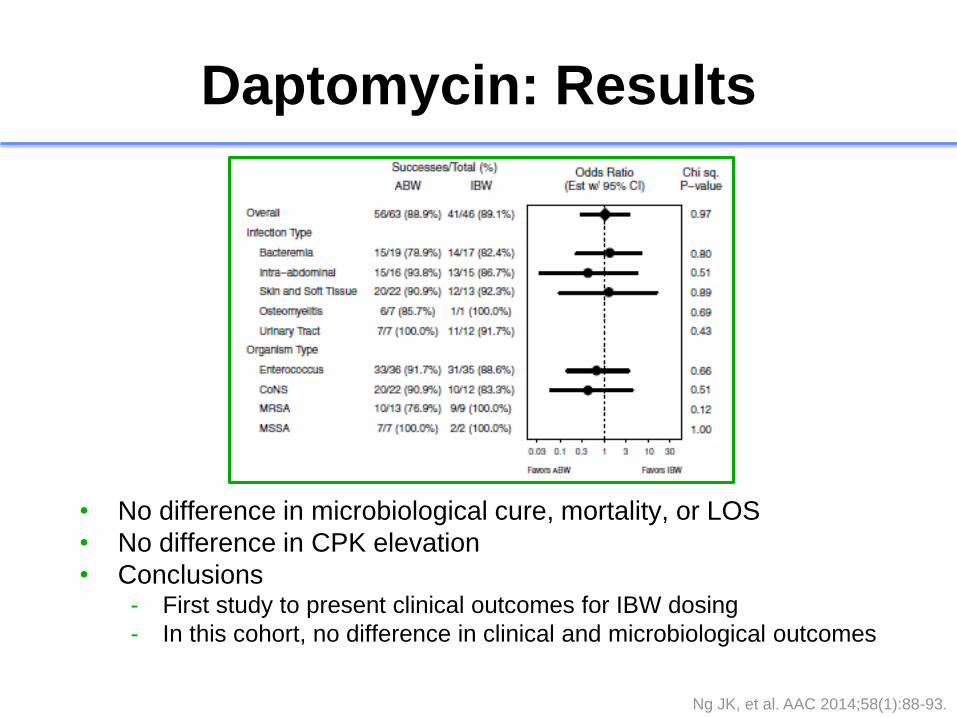
Daptomycin: Results
• No difference in microbiological cure, mortality, or LOS
• No difference in CPK elevation
• Conclusions - First study to present clinical outcomes for IBW dosing
- In this cohort, no difference in clinical and microbiological outcomes
Ng JK, et al. AAC 2014;58(1):88-93.
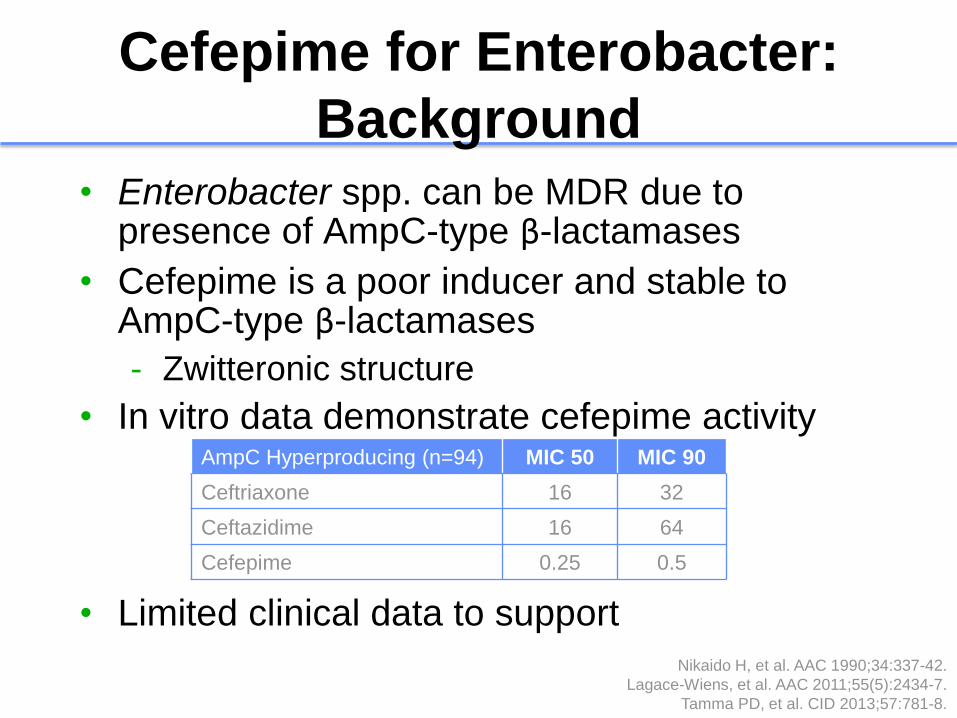
Cefepime for Enterobacter:
Background
• Enterobacter spp. can be MDR due to presence of AmpC-type β-lactamases
• Cefepime is a poor inducer and stable to AmpC-type β-lactamases
- Zwitteronic structure
• In vitro data demonstrate cefepime activity
• Limited clinical data to support
Nikaido H, et al. AAC 1990;34:337-42.
Lagace-Wiens, et al. AAC 2011;55(5):2434-7.
Tamma PD, et al. CID 2013;57:781-8.
AmpC Hyperproducing (n=94) MIC 50 MIC 90
Ceftriaxone 16 32
Ceftazidime 16 64
Cefepime 0.25 0.5
• Retrospective review of all Enterobacter spp. bacteremias from 2005-2011
• Methods - Multivariable logistic regression models
adjusted for demographics and clinical characteristics
- Propensity-matched analysis
- Single or combination antimicrobial therapy
• Primary outcomes - Persistent bacteremia (≥ 1 day)
- In-hospital mortality
Siedner MJ, et al. CID 2014;58(11):1554-63.
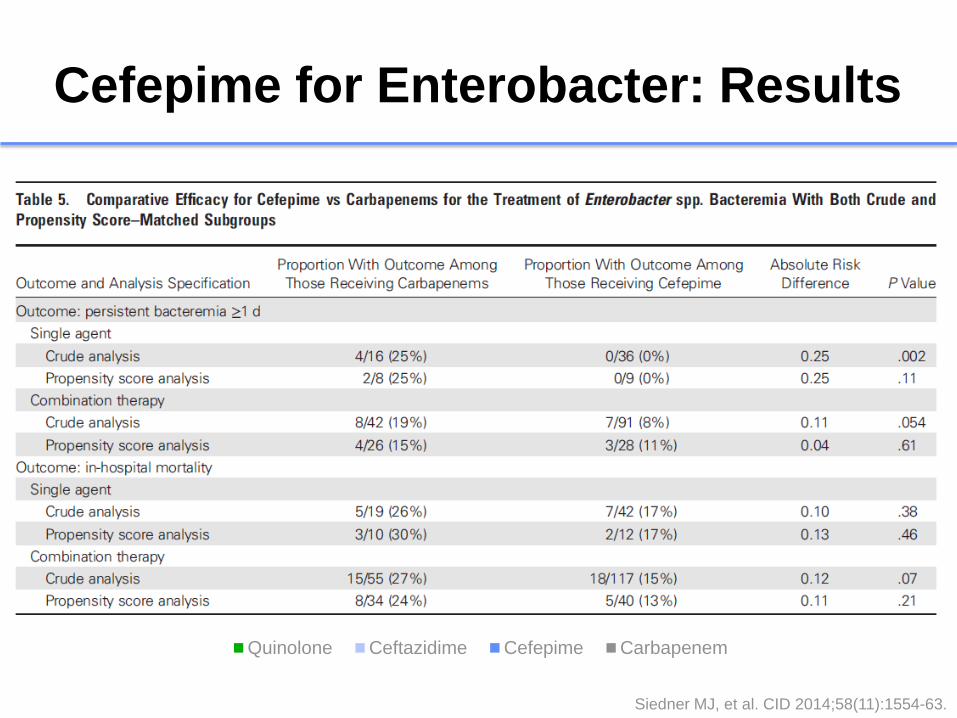
Cefepime for Enterobacter: Results
12 12
0
13
10 11
21
17
0
8
21
15
25
16
26
24
0
5
10
15
20
25
30
Category 1 Category 2 Category 3 Category 4
Pro
port
ion
of pa
tien
ts
Chart Title
Quinolone Ceftazidime Cefepime Carbapenem
Single-agent
persistent bacteremia
Overall persistent
bacteremia
Single-agent mortality Overall mortality
Siedner MJ, et al. CID 2014;58(11):1554-63.
Cefepime for Enterobacter: Results
• No statistically significant difference between cefepime or carbapenem for rates of persistent bacteremia or mortality
- Propensity score analysis
- Subset resistant to ceftriaxone or cephamycins
• Conclusion
- Cefepime has similar clinical and microbiological efficacy to carbapenems for Enterobacter spp. bacteremia
Siedner MJ, et al. CID 2014;58(11):1554-63.
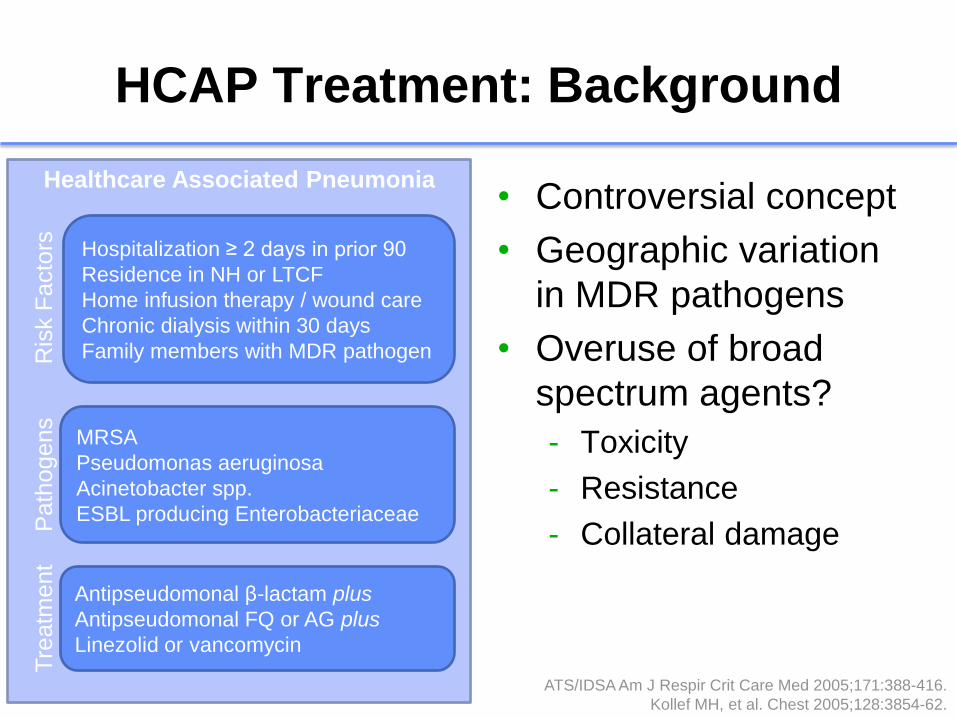
HCAP Treatment: Background
• Controversial concept
• Geographic variation
in MDR pathogens
• Overuse of broad
spectrum agents?
- Toxicity
- Resistance
- Collateral damage
ATS/IDSA Am J Respir Crit Care Med 2005;171:388-416.
Kollef MH, et al. Chest 2005;128:3854-62.
Healthcare Associated Pneumonia
Hospitalization ≥ 2 days in prior 90
Residence in NH or LTCF
Home infusion therapy / wound care
Chronic dialysis within 30 days
Family members with MDR pathogen
MRSA
Pseudomonas aeruginosa
Acinetobacter spp.
ESBL producing Enterobacteriaceae
Antipseudomonal β-lactam plus
Antipseudomonal FQ or AG plus
Linezolid or vancomycin
Ris
k F
acto
rs
Path
ogens
Tre
atm
ent
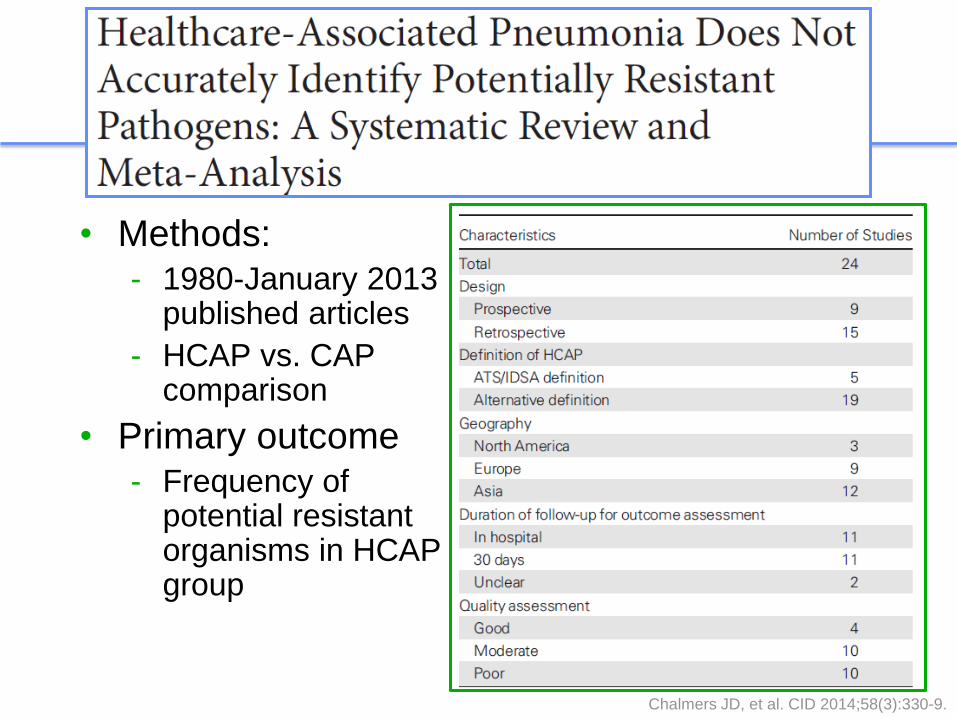
• Methods: - 1980-January 2013
published articles
- HCAP vs. CAP comparison
• Primary outcome - Frequency of
potential resistant organisms in HCAP group
Chalmers JD, et al. CID 2014;58(3):330-9.

HCAP Treatment: Results
PLR (95%CI) NLR (95%CI) AUC (95%CI)
All resistant 1.94 (1.67-2.24) 0.57 (0.50-0.66) 0.70 (0.69-0.71)
MRSA 1.97 (1.74-2.22) 0.44 (0.35-0.55) 0.74 (0.72-0.76)
Enterobacteriaceae 1.37 (1.26-1.49) 0.76 (0.69-0.84) 0.60 (0.58-0.62)
P. aeruginosa 1.68 (1.53-1.84) 0.62 (0.52-0.74) 0.68 (0.66-0.70)
Clinically Useful >10 <0.10 <0.75
• No significant increase in mortality associated with HCAP (OR 1.20; 95%CI 0.85-1.70; p=0.3)
• Conclusions - Current HCAP criteria do not accurately identify resistant
pathogens
- MDR risk factors may need to be pathogen specific
- Emphasize importance of local microbiology/epidemiology
Chalmers JD, et al. CID 2014;58(3):330-9.
PLR = positive likelihood ratio
NLR = negative likelihood ratio
AUC = area under the curve
Azithromycin & Cardiovascular
Events: Background
Ray WA, et al. NEJM 2012;366(20):1881-90.
Svanstrom H, et al. NEJM 2013;368(18):1704-12.
Rao GA, et al. Ann Fam Med 2014;12(2):121-7.
2012 2013 2014

• Retrospective population-based cohort
• Veterans Administration database
• Propensity score matching
Design
•Age ≥ 65 and diagnosis of pneumonia •Hospitalized October 2001 – September 2012 •IDSA/ATS recommended antibiotic for CAP within 48 hrs
Inclusion
• 30-day and 90-day all cause mortality
• Cardiovascular events within 90 days of admission
Outcomes
Mortensen EM, et al. JAMA 2014;311(21):2199-2208.
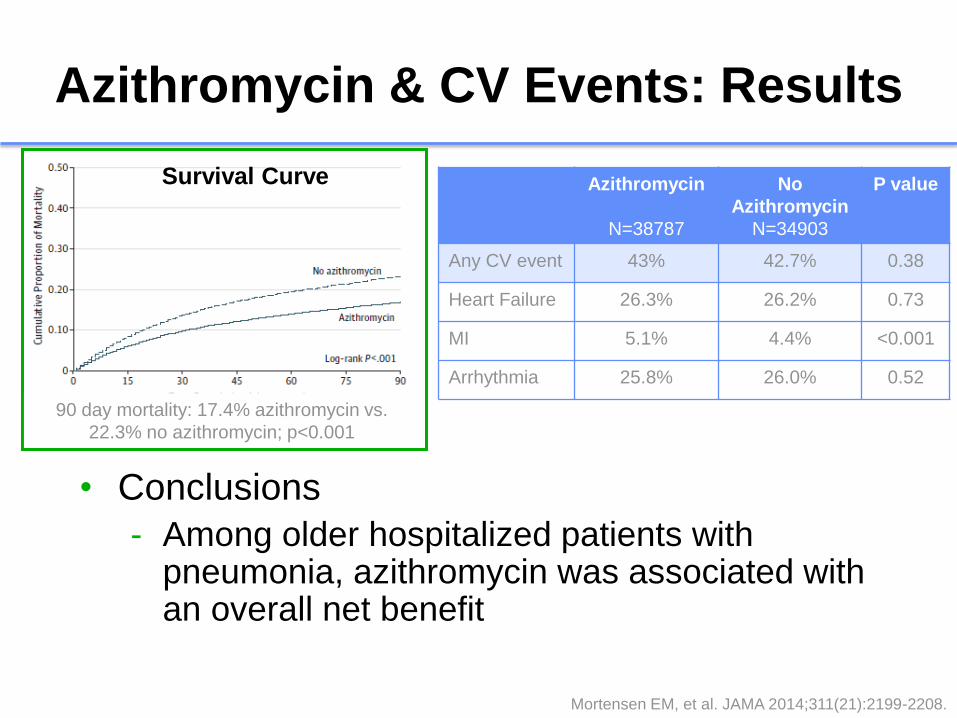
Azithromycin & CV Events: Results
Azithromycin
N=38787
No
Azithromycin
N=34903
P value
Any CV event 43% 42.7% 0.38
Heart Failure 26.3% 26.2% 0.73
MI 5.1% 4.4% <0.001
Arrhythmia 25.8% 26.0% 0.52
Survival Curve
90 day mortality: 17.4% azithromycin vs.
22.3% no azithromycin; p<0.001
• Conclusions
- Among older hospitalized patients with pneumonia, azithromycin was associated with an overall net benefit
Mortensen EM, et al. JAMA 2014;311(21):2199-2208.