too sick to be in the icu? toxic or healing environmentstoo sick to be in the icu? toxic or healing...
TRANSCRIPT
Too Sick to be in the ICU?
Toxic or Healing Environments
Martha A.Q. Curley, RN, PhD, FAAN
Ruth M. Colket Endowed Chair in Pediatric Nursing
Children’s Hospital of Philadelphia
Professor, School of Nursing
Anesthesia Critical Care Medicine
Perelman School of Medicine
University of Pennsylvania
Objectives
• Answer the question – are most ICUs toxic or healing? … what
about yours?
• Describe several strategies that can be used to create and/or
support healing ICU environments.
• Envision a “new normal” where the ICU is a healing milieu.
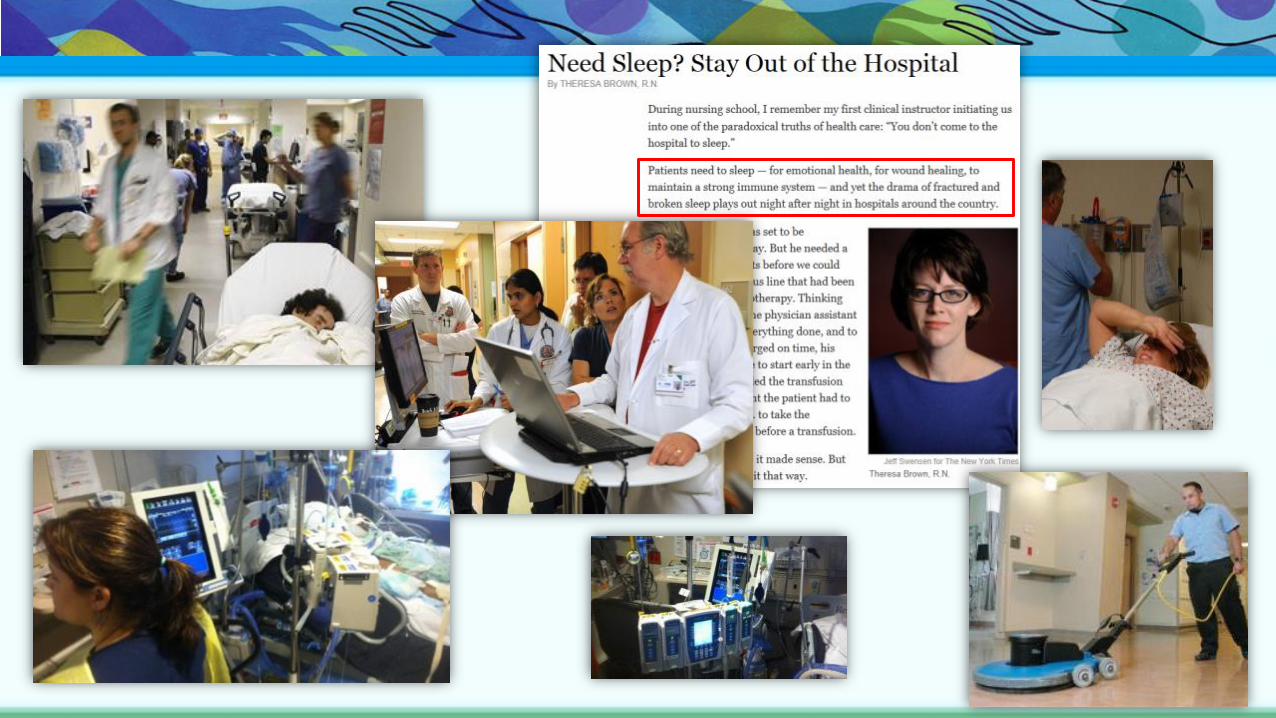
“What we must do … to put the
patient in the best condition for
nature to act upon him.”Florence Nightingale
Notes on Nursing, 1859
Create care environments that sustain and support the patient’s and
family’s capacity to heal.
“The very first requirement in a hospital
is that it should do the sick no harm.”
What ICU Nurses Do…
Domains of Practice • Diagnose and manage life-sustaining physiologic functions
• Manage crises
• Provide comfort measures
• Face death, provide end-of-life care and decision making
• Care for patients’ families
• Prevent hazards in a technological environment
• Communicate clinical assessments and improve teamwork
• Monitor quality, prevent, manage breakdown
• Provide clinical and moral leadership
Clinical Wisdom and Interventions in Acute and Critical Care (2011)
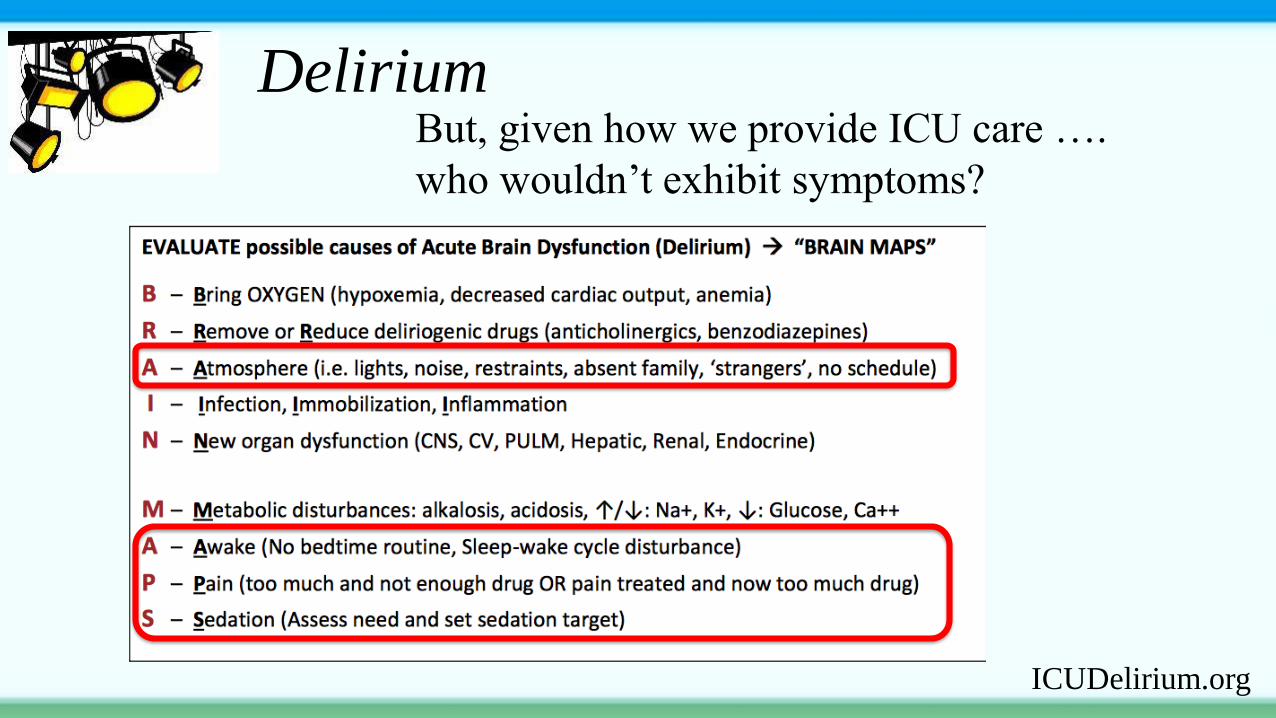
Delirium
ICUDelirium.org
But, given how we provide ICU care ….
who wouldn’t exhibit symptoms?
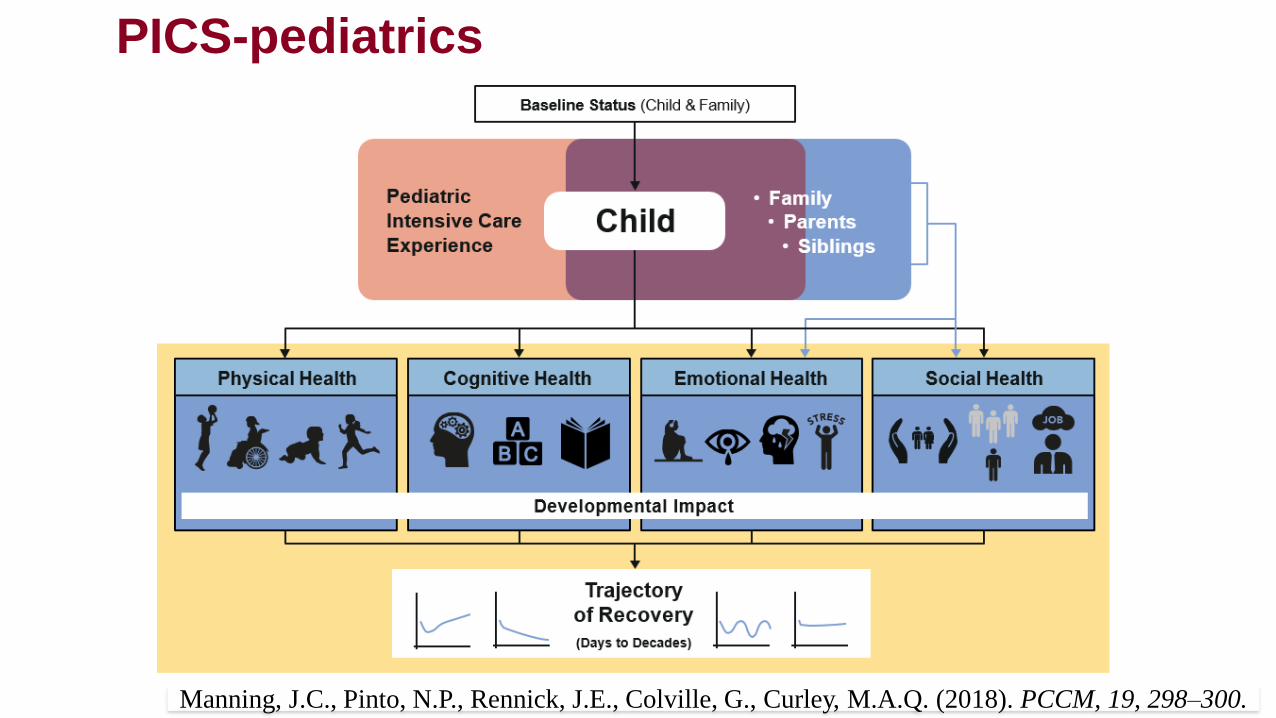
Manning, J.C., Pinto, N.P., Rennick, J.E., Colville, G., Curley, M.A.Q. (2018). PCCM, 19, 298–300.
PICS-pediatrics
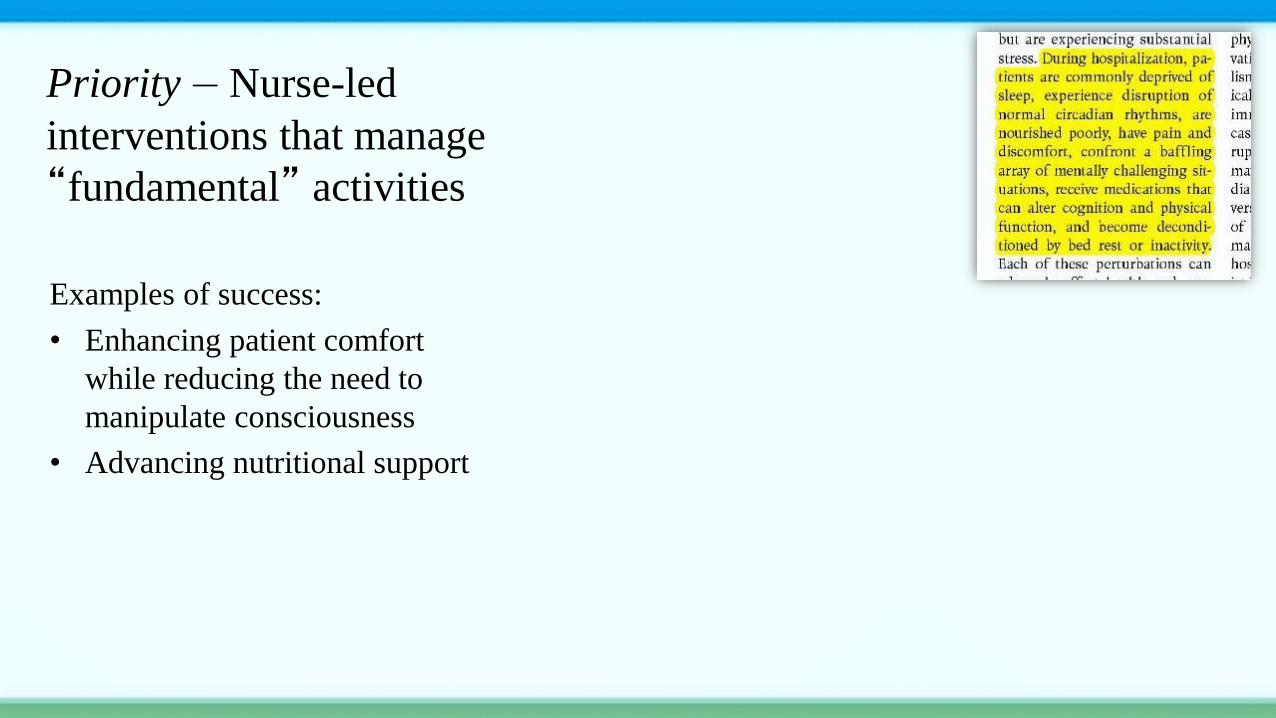
Examples of success:
• Enhancing patient comfort
while reducing the need to
manipulate consciousness
• Advancing nutritional support
Priority – Nurse-led
interventions that manage
“fundamental” activities
What can we do?
Change the paradigm
Creating healing ICU
milieus.
RESTORE Resilience
“R2”
Ann & Robert H. Lurie Children's Hospital of Chicago
1. Circadian rhythm & sleep history on PICU
admission (personalized sleep and activity
intervention)
2. Cycled day-night lighting and modulation of
sound to match the child’s routine
3. Minimal yet effective sedation
4. Night fasting with bolus enteral daytime
feedings
5. Early, developmentally-appropriate,
progressive exercise and mobility
6. Continuity in nursing care
7. ICU Parent diaries
R2 RESTORE Resilience
R21 HD093369
MPI: Curley, Kudchadkar, Zuppa

R2 RESTORE Resilience
R21 HD093369
MPI: Curley, Kudchadkar, Zuppa
• SPECIFIC AIM: To pilot-test RESTORE
resilience, an individualized chronotherapeutic
bundle, in pediatric patients supported on
mechanical ventilation for acute respiratory
failure in the PICU.
• Hypothesis: Pediatric patients managed per
RESTORE resilience will experience a more
restorative circadian rhythm evidenced by an
improved temporal sleep-wake pattern than
patients receiving usual care.
Secondary outcomes (exploratory):
1. Salivary melatonin levels on PICU day two and five
2. Nighttime EEG slow-wave activity during
endotracheal intubation
3. R2 feasibility, adherence, system barriers
4. Levels of patient comfort: PICU days free of pain,
agitation, delirium, iatrogenic withdrawal
5. PICU exposure to sedative medications (total dose
and length of exposure)
6. Time to physiological stability (time on vasoactive
medication, duration of mechanical ventilation,
PICU and hospital length of stay)
7. Parent perception of being well-cared-for
Primary outcome: Circadian activity ratio (daytime
activity/total 24-hr activity) after endotracheal
extubation.
#1 – Circadian rhythm & sleep history on
PICU admission
R2
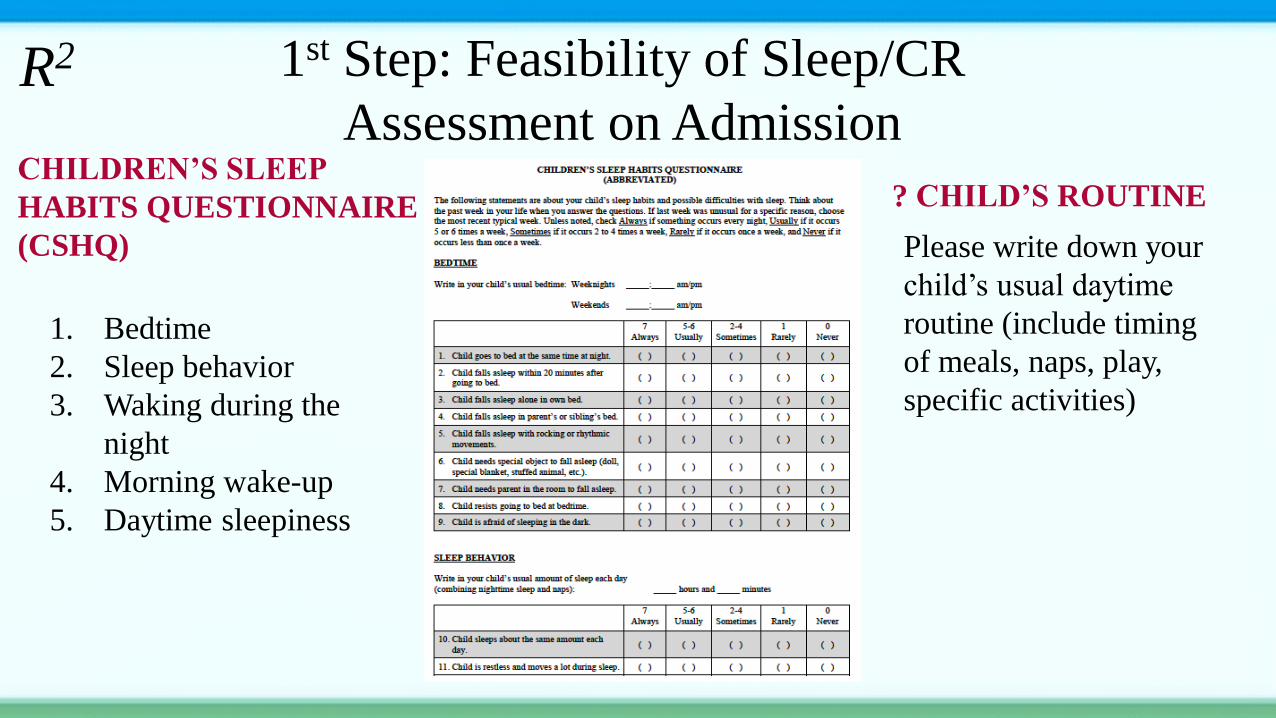
1st Step: Feasibility of Sleep/CR
Assessment on AdmissionCHILDREN’S SLEEP
HABITS QUESTIONNAIRE
(CSHQ)
1. Bedtime
2. Sleep behavior
3. Waking during the
night
4. Morning wake-up
5. Daytime sleepiness
Please write down your
child’s usual daytime
routine (include timing
of meals, naps, play,
specific activities)
R2
? CHILD’S ROUTINE
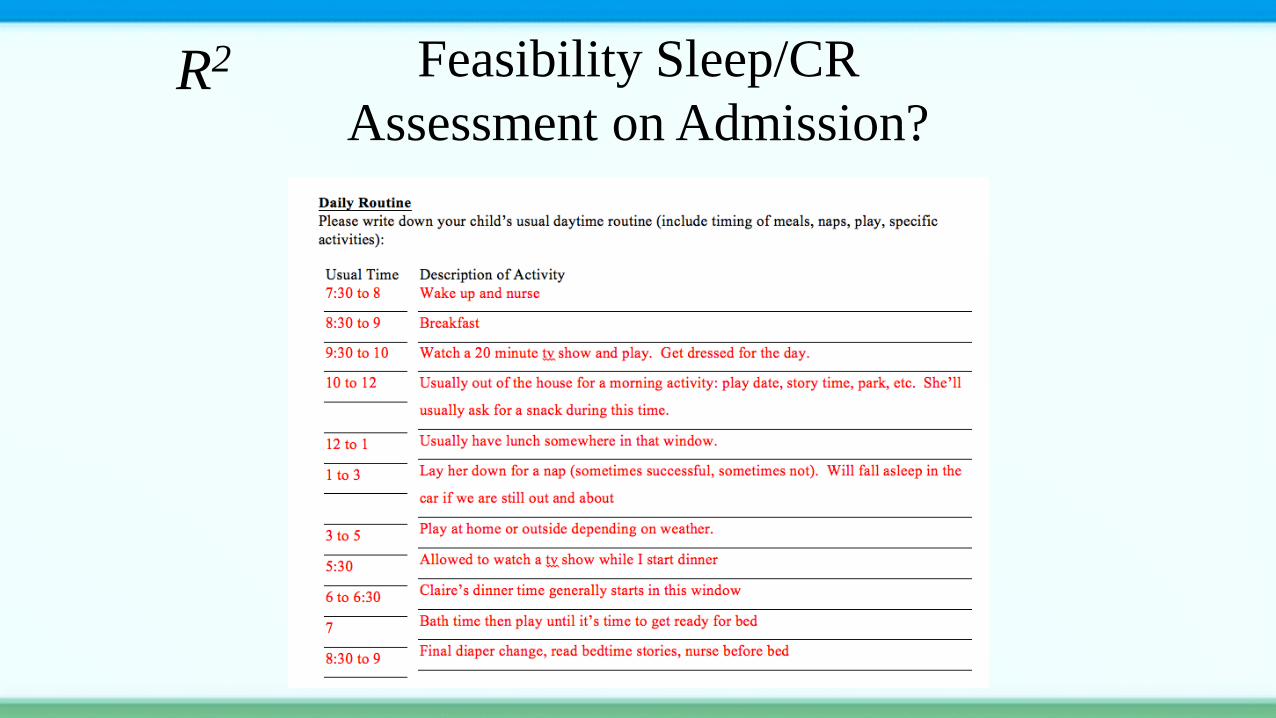
Feasibility Sleep/CR
Assessment on Admission?R2
CHILD’S ROUTINE
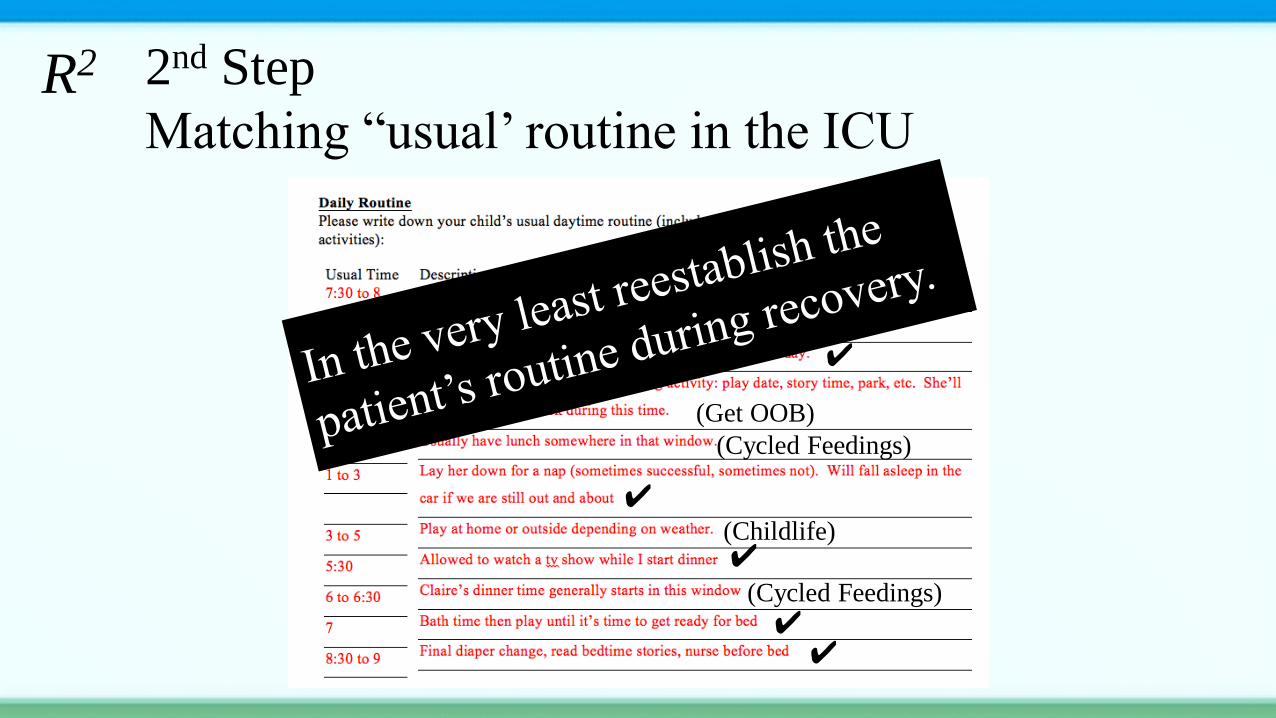
2nd Step
Matching “usual’ routine in the ICU R2
✔
✔
✔
✔
✔
✔
(Get OOB)
(Childlife)
(Cycled Feedings)
(Cycled Feedings)
(Cycled Feedings)
Decision-making
Participation
in Care
Aligns with Family Centered Care
R2 #2 Cycled day-night lighting and modulation of
sound to match the child’s routine
Cycled day-night lighting – building evidence
• Early morning bright light may enhance sleep, decrease
circadian rhythm disruption and decrease delirium.
• Optimizing physiologic light-dark patterns may decrease
sedative-analgesic needs and support recovery from critical
illness.
R2 #2 Modulation of sound to match the child’s
routine & developmental level
Noise verses Meaningful Sound
• ICUs for all patient populations are too loud
– WHO recommendations: <35dBA (average), <45dBA (max)
– NICU specific: <45dBA (average), <65dBA (max)
– According to the EPA a 70dBA sound can cause awakening
• PICUs are loud! (Yu Kawai, J of ICM, September 2017)
– Median: 53 dB [IQR: 45-56]
– Hourly maximum: 68 dB [64-72]
– Peak: 123 dB
– Bed spaces louder during the day than at night [54 vs. 52 dB]
– Bed spaces closest to common areas were louder when occupied [55 vs. 53 dB]
and when unoccupied [51 vs. 44 dB]
Noise verses Meaningful Sound
• Patient care equipment is a major noise contributor in all ICUs
in all patient populations
• Staff-education interventions are effective in reducing noise
levels in ICUs for all patient populations
R2#2 Noise containment also good for staff
#3 Minimal but effective sedation
RESTORE: Nurse-Led Goal-Directed Sedation
R2
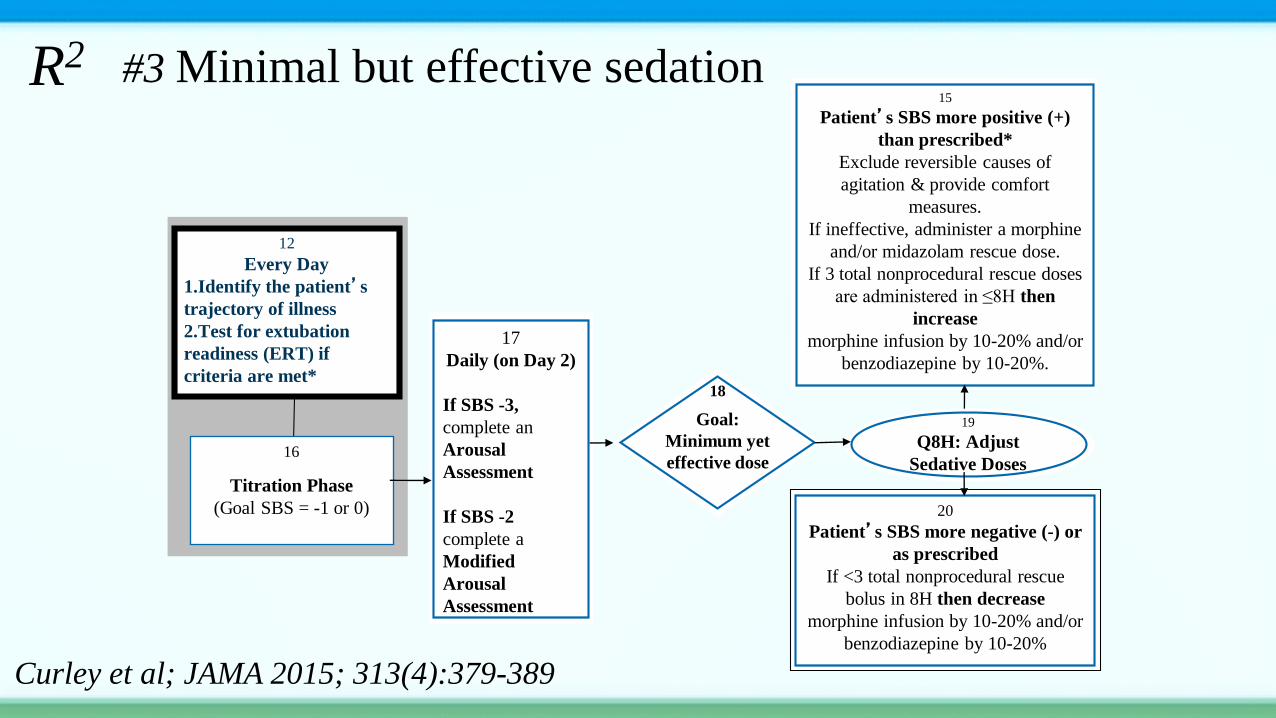
#3 Minimal but effective sedation
18
Goal:
Minimum yet
effective dose
19
Q8H: Adjust
Sedative Doses
15
Patient’s SBS more positive (+)
than prescribed*
Exclude reversible causes of
agitation & provide comfort
measures.
If ineffective, administer a morphine
and/or midazolam rescue dose.
If 3 total nonprocedural rescue doses
are administered in ≤8H then
increase
morphine infusion by 10-20% and/or
benzodiazepine by 10-20%.
20
Patient’s SBS more negative (-) or
as prescribed
If <3 total nonprocedural rescue
bolus in 8H then decrease
morphine infusion by 10-20% and/or
benzodiazepine by 10-20%
17
Daily (on Day 2)
If SBS -3,
complete an
Arousal
Assessment
If SBS -2
complete a
Modified
Arousal
Assessment
12
Every Day
1.Identify the patient’s
trajectory of illness
2.Test for extubation
readiness (ERT) if
criteria are met*
16
Titration Phase
(Goal SBS = -1 or 0)
Curley et al; JAMA 2015; 313(4):379-389
R2
#4 Night fasting with
bolus enteral daytime feedings (per child’s routine feeding schedule)
• Compared to slow continuous feedings, bolus feedings are
physiologic and a known driver of CR.
• There are little data supporting the benefits of continuous
versus bolus feeding in critically in children.
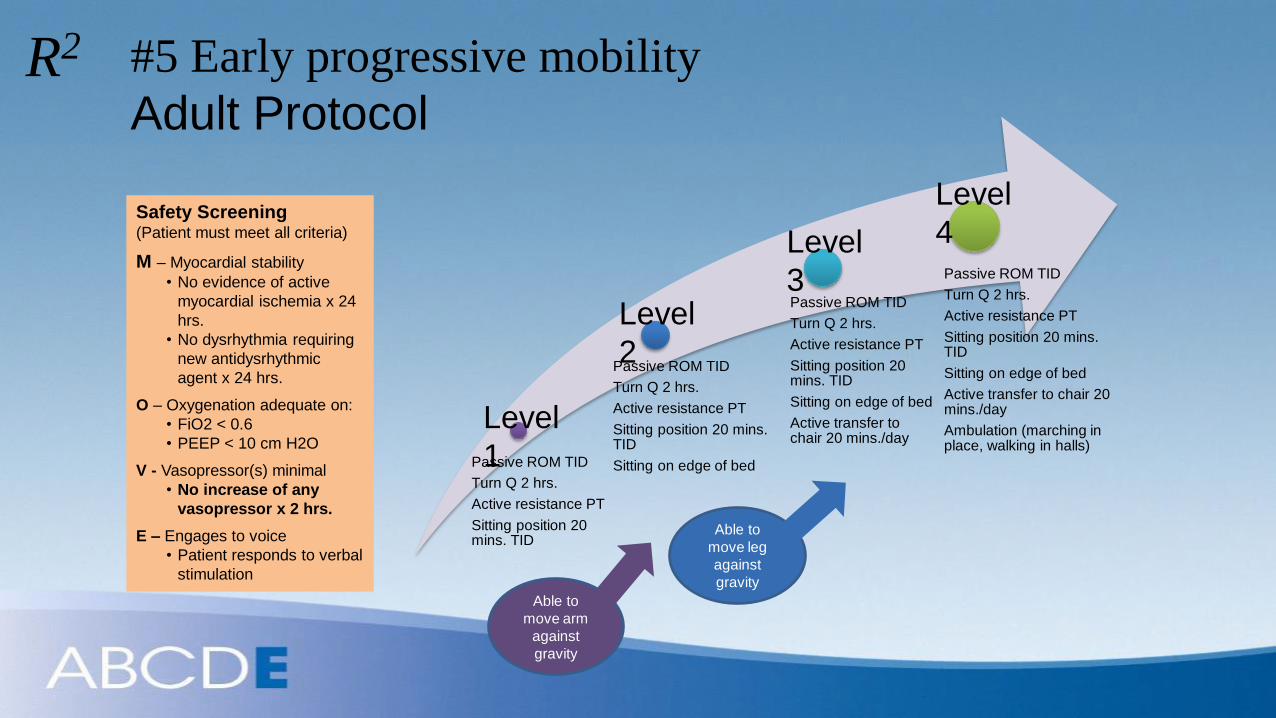
Passive ROM TID
Turn Q 2 hrs.
Active resistance PT
Sitting position 20 mins. TID
Passive ROM TID
Turn Q 2 hrs.
Active resistance PT
Sitting position 20 mins. TID
Sitting on edge of bed
Passive ROM TID
Turn Q 2 hrs.
Active resistance PT
Sitting position 20 mins. TID
Sitting on edge of bed
Active transfer to chair 20 mins./day
Passive ROM TID
Turn Q 2 hrs.
Active resistance PT
Sitting position 20 mins. TID
Sitting on edge of bed
Active transfer to chair 20 mins./day
Ambulation (marching in place, walking in halls)
Able to
move arm
against
gravity
Able to
move leg
against
gravity
#5 Early progressive mobility
Adult Protocol
Safety Screening (Patient must meet all criteria)
M – Myocardial stability
• No evidence of active
myocardial ischemia x 24
hrs.
• No dysrhythmia requiring
new antidysrhythmic
agent x 24 hrs.
O – Oxygenation adequate on:
• FiO2 < 0.6
• PEEP < 10 cm H2O
V - Vasopressor(s) minimal
• No increase of any
vasopressor x 2 hrs.
E – Engages to voice
• Patient responds to verbal
stimulation
Level
1
Level
2
Level
3
Level
4
R2
Morandi A, et al.
Curr Opin Crit Care. 2011;17:43-49.
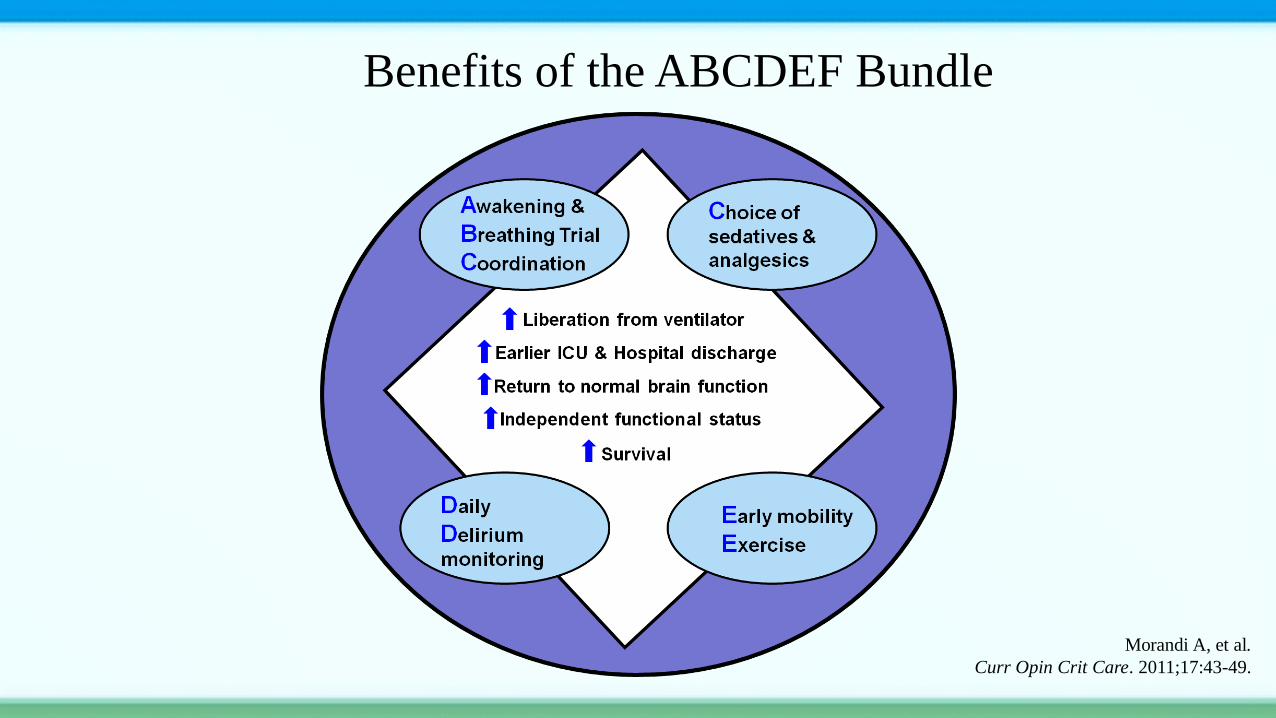
Benefits of the ABCDEF Bundle
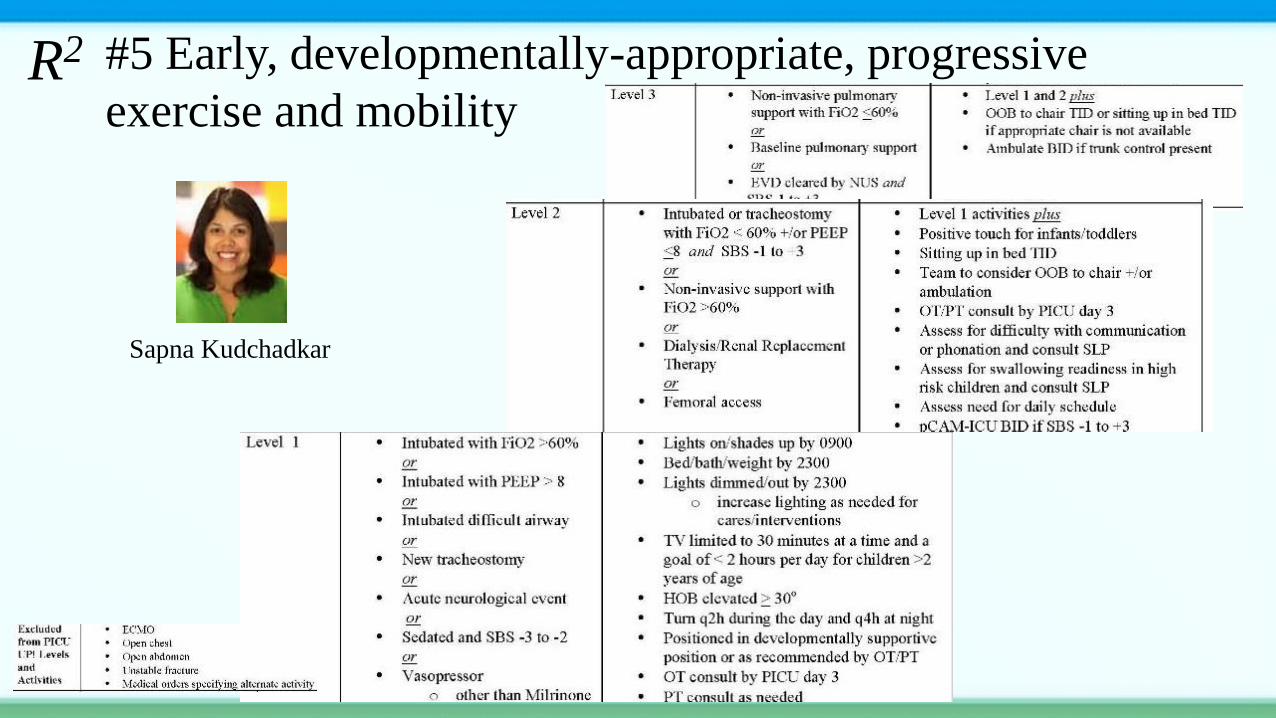
#5 Early, developmentally-appropriate, progressive
exercise and mobility
Sapna Kudchadkar
R2
#6 Continuity in Nursing CareModels of nursing care that allow reciprocal nurse-patient /family relationships
• Nurse “knowing” patients and families
– Limit the number of different clinicians assigned to care for each
patient; continuity in nursing care (CINC)
• Patients and families “knowing” nurses
– Unburden patients and families; preserve emotional energy, enhanced
communication and coordination of care
• Allow synergyPatient and family stability, complexities, predictability, resiliency. vulnerability,
participation in decision-making & care, resource availability
Fostering nursing clinical judgment, inquiry, caring practices, response to diversity,
advocacy, facilitator of learning , collaboration, and systems thinking.
R2
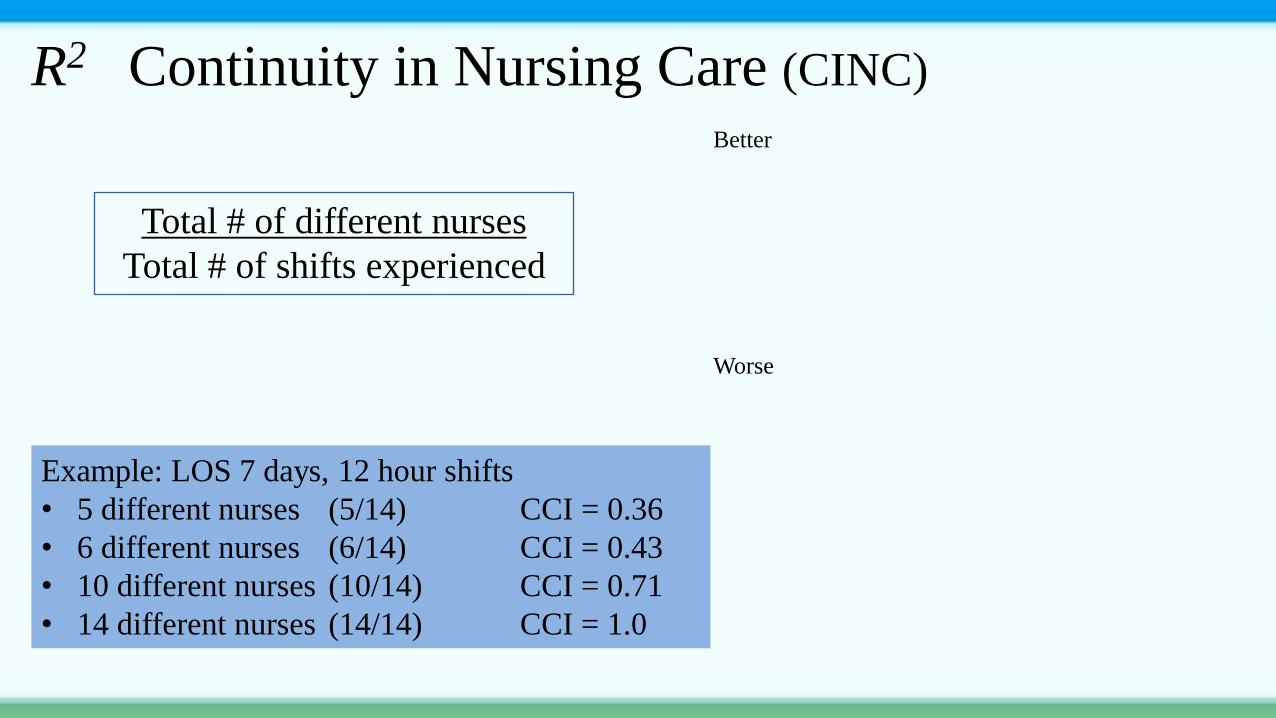
R2 Continuity in Nursing Care (CINC)
Total # of different nurses
Total # of shifts experienced
Example: LOS 7 days, 12 hour shifts
• 5 different nurses (5/14) CCI = 0.36
• 6 different nurses (6/14) CCI = 0.43
• 10 different nurses (10/14) CCI = 0.71
• 14 different nurses (14/14) CCI = 1.0
Better
Worse
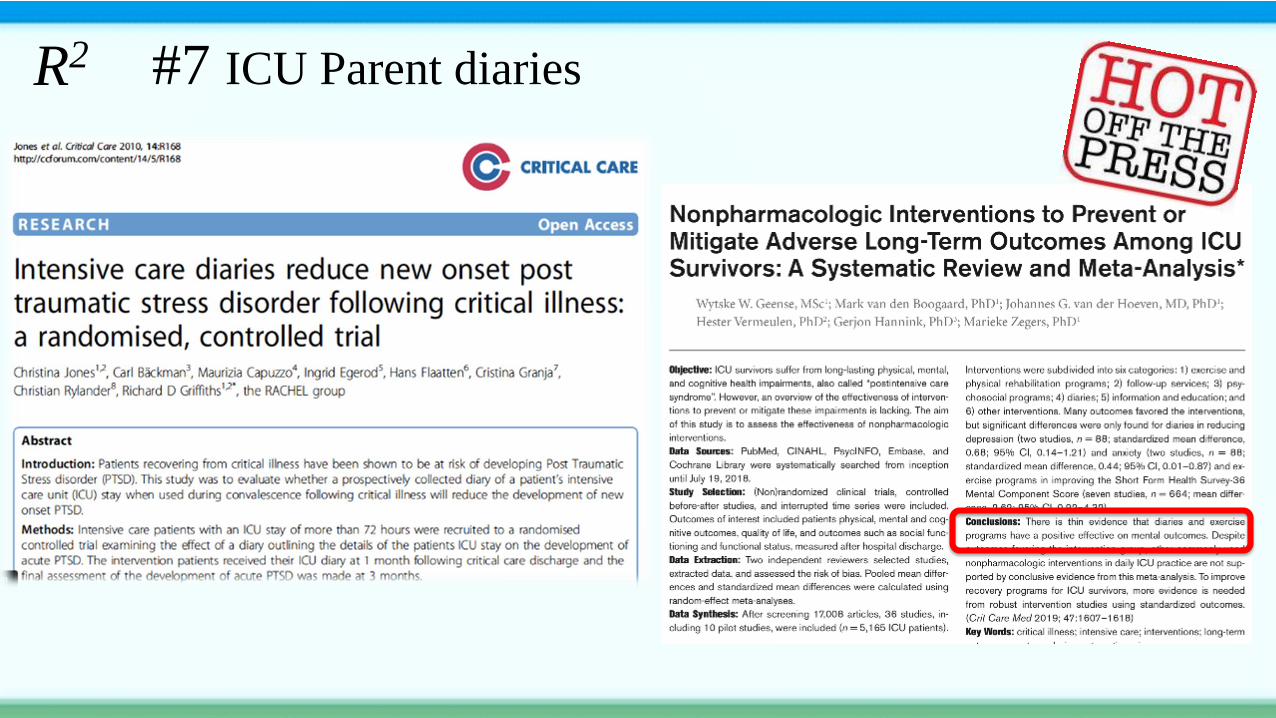
#7 ICU Parent diaries R2
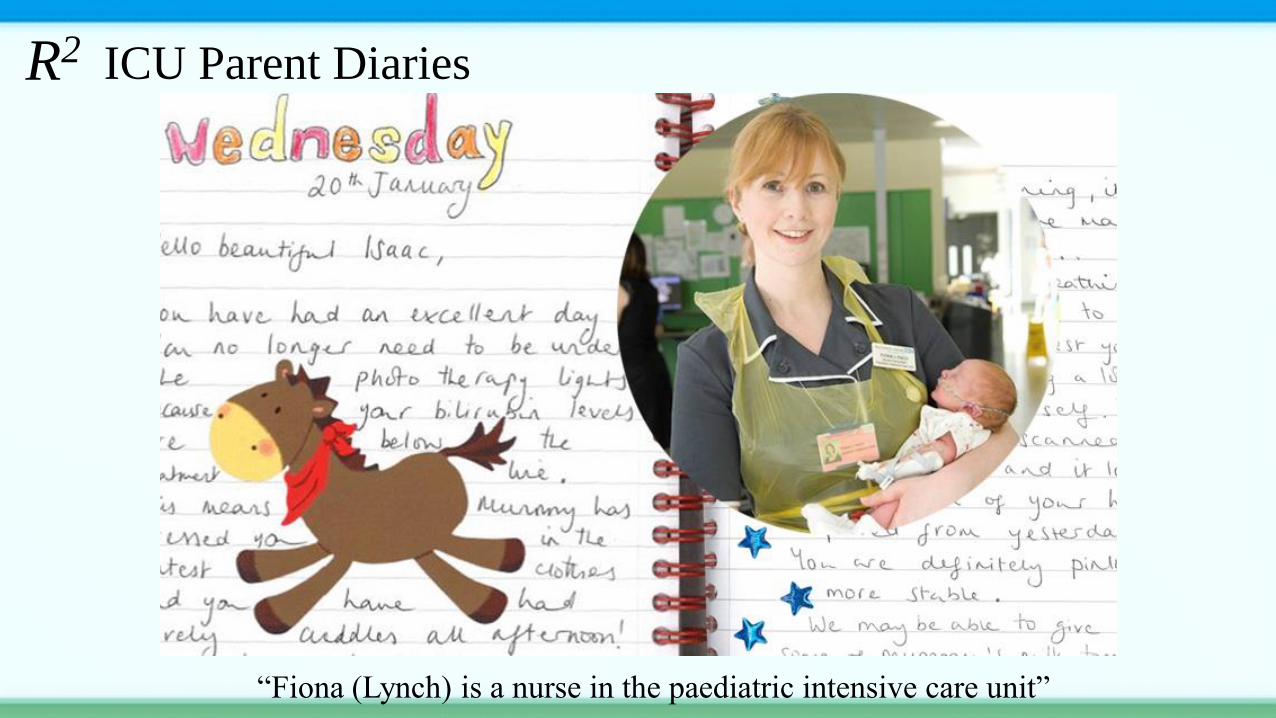
ICU Parent Diaries
“Fiona (Lynch) is a nurse in the paediatric intensive care unit”
R2
Benefits of creating healing milieus?
• Symptom management (agitation, delirium)
• Maintenance of circadian rhythms, sleep
• Time to physiologic stability
• Patient perception of being well-cared-for (FCCS)
• Short-term outcomes (lengths of stay, ventilator days)
• Long-term outcomes (post intensive care syndrome)
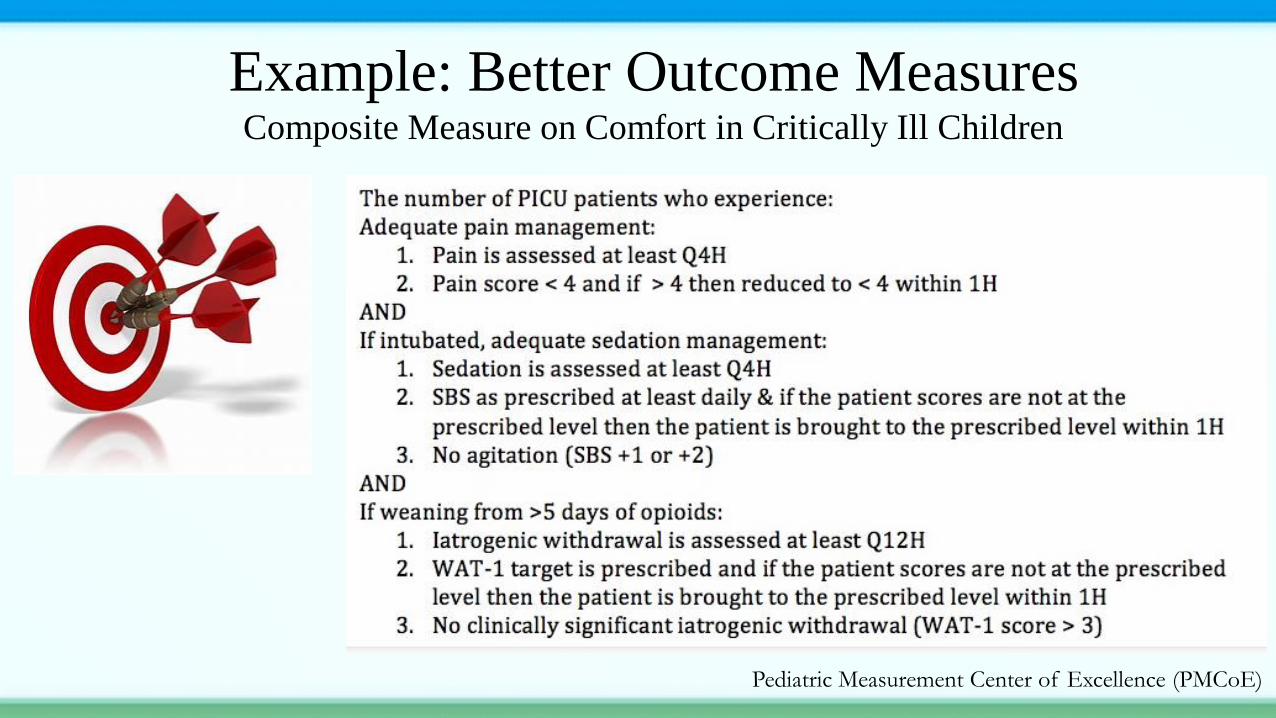
Example: Better Outcome Measures Composite Measure on Comfort in Critically Ill Children
Pediatric Measurement Center of Excellence (PMCoE)
Practice of Critical Care
• Shaped by multiple perspectives
• Core values
– Primacy of patient and family
– Spirit of inquiry
– Innovation
ICU Nursing Practice
• One that is patient and family centered
• One where nurses create healing environments for patients and
their families
• One where the practice of nursing is supported by systems that
enhance nursing’s capacity to optimize patient and family
outcomes.
Let’s continue
to “challenge
the givens”
Thank You