tinea - livelifepharmacy.com · tinea capitis—tinea of the head or ringworm of the scalp—best...
TRANSCRIPT
Tinea
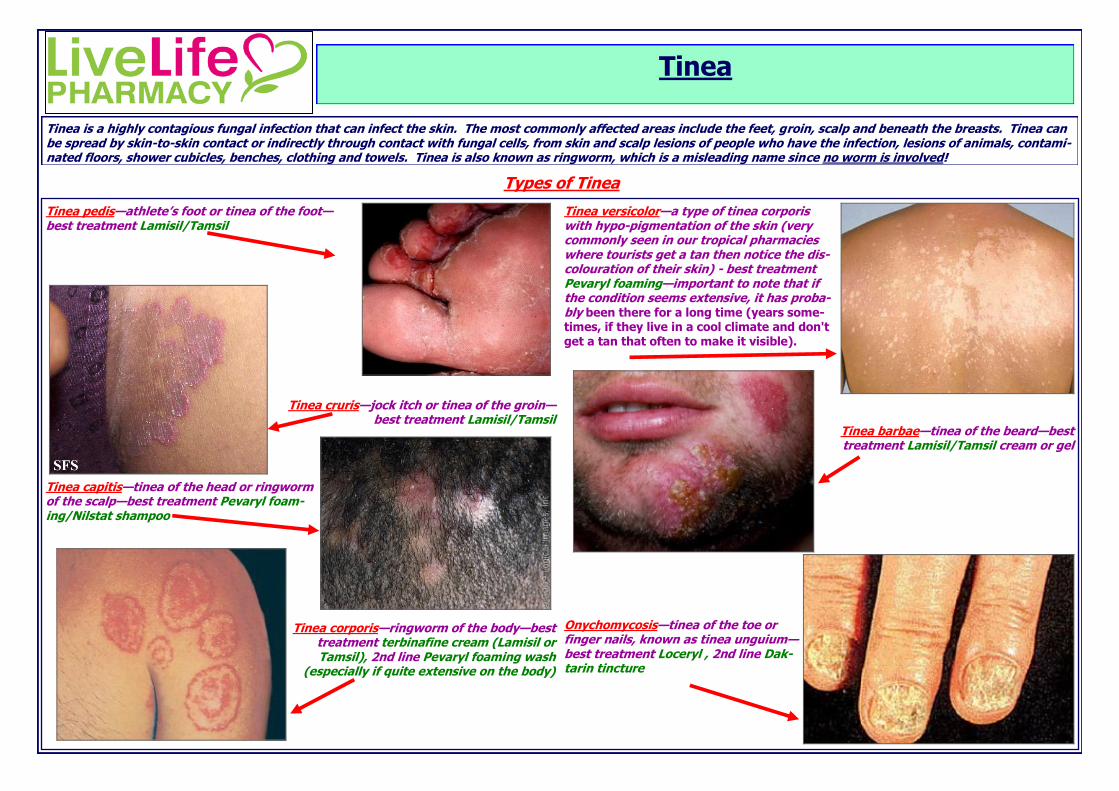
Tinea is a highly contagious fungal infection that can infect the skin. The most commonly affected areas include the feet, groin, scalp and beneath the breasts. Tinea can be spread by skin-to-skin contact or indirectly through contact with fungal cells, from skin and scalp lesions of people who have the infection, lesions of animals, contami-nated floors, shower cubicles, benches, clothing and towels. Tinea is also known as ringworm, which is a misleading name since no worm is involved!
Tinea pedis—athlete’s foot or tinea of the foot—best treatment Lamisil/Tamsil
Tinea cruris—jock itch or tinea of the groin—best treatment Lamisil/Tamsil
Tinea capitis—tinea of the head or ringworm of the scalp—best treatment Pevaryl foam-ing/Nilstat shampoo
Tinea corporis—ringworm of the body—best treatment terbinafine cream (Lamisil or Tamsil), 2nd line Pevaryl foaming wash
(especially if quite extensive on the body)
Tinea versicolor—a type of tinea corporis with hypo-pigmentation of the skin (very commonly seen in our tropical pharmacies where tourists get a tan then notice the dis-colouration of their skin) - best treatment Pevaryl foaming—important to note that if the condition seems extensive, it has proba-bly been there for a long time (years some-times, if they live in a cool climate and don't get a tan that often to make it visible).
Tinea barbae—tinea of the beard—best treatment Lamisil/Tamsil cream or gel
Onychomycosis—tinea of the toe or finger nails, known as tinea unguium—best treatment Loceryl , 2nd line Dak-tarin tincture
Types of Tinea
Signs and symptoms
Itching and stinging
Red, scaly rash that is shaped like a ring (annular)
Red patches that are often redder around the outside with normal skin
tone in the centre
Moist, red areas with cracking, splitting and peeling in the toe web
spaces
Small fluid filled blisters that may ooze
Yellow or white discoloration of the nails that may thicken and even
crumble
Bald spots on the scalp
On the feet, between the toes looks like soggy white skin, which peels
off, and it is really itchy. It can also be on the sole of the foot, or on top of it. It can start out looking like a blistery red dot, which quickly be-comes a peeling area of the skin.
The skin on the body can sometimes look healthy, with no scales, just
lighter colour than the skin around it (referred to as tinea versicolour, shown on the previous page of module). It is also important to note that in this particular type of tinea, the skin is not necessarily “itchy” or “irritated.”
Risk factors
Tinea infection on any body area is more likely to develop if you:
Live or work in hot, humid climates
Handle animals who have the infection
Perspire a lot
Do not dry skin well after bathing
Are a child or spend time with children
Have diabetes
Have a weakened immune system
Tinea on the feet is more likely to develop if you:
Wear synthetic socks that make feet sweat
Go barefoot in public showers and around pools
Wear tightly fitting shoes or plastic or rubber shoes (e.g. Gum boots)
Don’t wash and dry between the toes properly
Groin tinea is more likely to develop if you:
Perspire a lot
Are overweight
Are a male
Lifestyle advice
After washing, dry the skin thoroughly, particularly between the toes and within skin folds.
Expose the skin to the air as much as possible.
Wear cotton socks instead of synthetics.
Use antiperspirant deodorants to control excessive perspiration (sweating).
Wear thongs to swimming pools, locker rooms, gyms and other communal areas.
Wash socks, underwear, towel and bathmats in hot water and detergent, or use a laundry product designed to prevent re-infection.
While infected, avoid transferring the tinea to another body area. Use a separate, fresh towel to dry infected area and wash hands well after touching infected area.
Check family animals for tinea. On animals it looks like a patch of skin with fur missing—consult your vet.
Do not share towels, shoes, socks, underwear, hats or hair brushes and combs.
Clean the base of the shower or bath with disinfectant, so you don’t re-infect yourself or others.
Allow sweaty shoes to dry out before wearing again.
Use antiperspirants to avoid excessive sweating
Avoid using soap as it is alkaline (high pH) and will cause the skin to lose its natural acidity, allowing fungi to flourish.
Using a soap free alternative (such as Pinetarsol) is a good alternative, as it will keep the skin acidic and relieves itching.
Change out of wet swimmers/wetsuits as soon as possible, as the moisture can worsen fungal infections
Antifungal creams—these preparations are applied directly to the area and work by killing the fungus causing symptoms. Some common ingredients in these prepara-tions and examples of their brand names are as below:
Clotrimazole S2 (e.g. Canesten,
clonea, Pharmacy Action anti-fungal cream, Amcal anti-fungal
cream)
Bifonazole S2 (e.g. Canesten
once daily, mycospor)
Miconazole S2 (e.g. Resolve, Daktarin)
Terbinafine S2 (e.g. Lamisil and generic Tam-
sil) NB this is a very convenient product as it is applied only once daily for 7 days. This is because terbinafine is the only topical anti-fungal that kills the fungus (fungicidal); the rest are fungistatic - they stop it growing while the ingredient is used, then if use stops the fungus starts to grow again. This is why Terbinafine works so much better and faster, which is definitely what we want! Especially great if you don’t think you will apply other treatments twice or three times daily.
Antifungal/cortisone combination creams—hydrocortisone is often used in conjunction with
antifungal creams initially, if the itching is severe and/or there is significant redness/inflammation. However, please note you should not use hydro-cortisone alone on fungal infections because although it re-moves the redness, it allows the infection to spread rapidly and uncontrolled. Some common examples include:
Miconazole + hydrocortisone (Resolve plus—0.5% S2, 1%
S3)
Clotrimazole + hydrocortisone (Hydrozole S3)
Antifungal gels—similar to creams, these are applied directly to the skin for tinea infections; the difference being that these products are very cooling/soothing to the area and so sometimes are preferred.
Lamisil dermgel (contains terbinafine and should be applied once
daily for 7 days) Antifungal once treatment solution—Lamisil Once is the only product that needs only one single application. When applied, Lamisil Once builds a film on the skin. After about three days, the film disappears but the active ingredient, terbinafine, remains in the skin where it works hard to fight off the infection.
Antifungal tinctures—These alcoholic liquids are designed for the treatment of fun-gal nail infections and penetrate the nail, drying to leave a protective coating. They provide effective treatment for fungal infections in the fingernails and toenails, but must be used until the infected nail is completely grown out (6-12 months!!!) and are only effective before the fungus reaches the nail bed, otherwise oral prescription medicines are required (consult your pharmacist). Some examples include:
Loceryl (contains amorolfine and is applied only once or twice weekly—very effec-
tive treatment and although seeming expensive, has enough volume to treat 1-2 nails for up to 12 months) **Most effective over-the-counter product**
Daktarin tincture (contains miconazole and is applied several times daily)
Canesten tincture (contains clotrimazole and is applied several times daily)
Canesten Fungal Nail Treatment Set (contains a urea cream for softening the nail
and a bifonazole cream for treating the fungus in the nail bed after removal of the infected nail—course is much shorter than other treatments
and is usually finished in 6-7 weeks).
Antifungal powders—these powders are infused with antifungal agents and treat the condition similarly to creams/gels, but with more of a “drying effect” for those peo-ple who feel that moisture is contributing to their tinea infection (e.g. people wear-ing boots and socks all day at work or sweating profusely). They are also particu-larly useful to use alongside creams/gels by dusting the shoes and socks for extra protection against the fungus.
Daktarin Powder/spray powder—contains myconazole and should be applied twice
daily every day until 2 weeks after symptoms subside **Most effective powder
and should be used when possible before mycil and tinaderm**
Mycil Powder—contains the antifungal agent tolnaflate and the antibacterial agent
chlorhexidine and should be applied 2-3 times daily every day until 2 weeks after symptoms subside
Tinaderm Powder/spray powder—also contains tolnaflate similar to Mycil Power
above
Treatment for “optimal care”
Shampoos and washes—these are very useful for the treatment of tinea capitis and tinea corporis.
Pevaryl foaming wash—this treatment contains 3 sa-
chets for treatment of tinea versicolor. One sachet is used every night for 3 nights, by wetting the skin then applying the contents of the sachet all over the body
and letting it dry. You then sleep with the treatment on the skin and wash it off the next morning. This is then repeated in one month and three months. **Most ef-fective treatment—poor compliance with others. You should purchase 3 boxes to ensure you don’t forget to do the 2 follow up treatment courses to clear the fungal infec-tion from the deepest layers of skin**
Nizoral shampoo—available as a 1% or 2% - the shampoo
is applied and left on for 10 minutes, then washed off. For tinea versicolour (a variety of tinea corporis mentioned earlier in the module), use daily for 10 days.
Selsun yellow—applied to the body for tinea versicolour and washed off once it
dries on the skin (usually around 30 minutes) and this is repeated several times over a 2 week period.
Head and Shoulders Shampoo/Conditions—contains zinc which can help with itch-
ing on the scalp and the dry, flaky skin that may accompany tinea.
Tea tree oil—Preliminary studies report tea tree oil to have activity against several fungal species. However, there is no conclusive evidence at this time and the use of this product should be “complementary” to other anti-fungal treatments listed above. At this stage, the recommended application for this product for tinea pedis (based on those used in studies) is: a 10% tea tree oil cream applied twice daily to the feet after they have been thoroughly washed and dried, or a 25-50% tea tree oil solution applied twice daily to the af-fected area for 4 weeks. For a fungal nail infection (onychomycosis): 100% tea tree oil, applied to the affect area twice daily for 6 months. Canesten Hygiene Rinse—Normal washing, especially at cold temperatures, may not completely remove the bacteria or fun-gal spores. This often leads to the bacteria and fungal spores being passed on to other garments, and ultimately re-infection or cross infection. Canesten Hygiene Rinse can break the cycle of re-infection and cross infection by helping to eliminate fun-gal spores that can remain in your clean washing increasing the risk of re-infection.
Thongs—if you are travelling and believe you may have picked up tinea pedis from public showers along the way, you could consider getting some rubber thongs!
Antiperspirants—you may be able to prevent the growth of some fungus by keeping the skin as dry as possible and avoiding excess perspiration.
Treatment for “optimal care” continued.....