tim sutton, cardiologist counties manukau dhb · 2019-06-04 · arnis diuretics digoxin...
TRANSCRIPT

Palliative care from a
cardiologist’s
perspective
Tim Sutton, Cardiologist
Counties Manukau DHB
1

Common cardiac conditions
Symptoms and their management
Focus on failing heart
Early and late treatments
Disease trajectory
End stages
Management of symptoms / medications
ICDs and what to do with them
Challenges
2

Common chronic cardiac diseases:
Ischaemic heart disease
Stable
Symptoms
Angina, breathlessness
Medications
Aspirin, statin, antianginals
Treatments
Medical therapy
Stenting
Bypass surgery
Unstable
– acute coronary syndromes
Symptoms
Chest discomfort, acute heart failure
Medications
Dual antiplatelet therapy, statin,
ACE inhibitors, beta blockers
Treatments
Medical therapy
Stenting
Bypass surgery3

Common chronic cardiac diseases:
Heart failure
Reduced EF (HFReF)
Symptoms
Breathlessness, swelling, fatigue, anorexia, angina
Medications
Preserved EF (HFPeF)
Drug Symptoms Survival Symptoms
Diuretic Yes Yes
ACE inhibitor Yes Yes
Beta blocker Yes Yes
ARA Yes Yes Maybe
Digoxin Maybe
Nitrates Yes 4

Advanced heart failure treatments
Cardiac resynchronisation (CRT) : P vs D
Implantable cardioverter defibrillator
Cardiac transplantation
Common chronic cardiac diseases:
Heart failure
5

Symptoms
None, palpitations, breathlessness, fatigue
Medications
To control symptoms
To prevent strokes
Interventions
Pulmonary vein isolation
Pacemaker and AV node ablation
Common chronic cardiac diseases:
Abnormal heart rhythms : Atrial fibrillation
Congestive heart failure 1
Hypertension 1
Age 1 or 2
Diabetes 1
Stroke 2
Vascular disease 1
Sex category F : 1
CHA2DS2VASc Score Annual Stroke risk (%)
0 <1
1 1.3
2 2.2
3 3.2
4 4
5 6.7
6 9.8
7 9.6
8 6.7
6.7 15.2
6

Too slow
Pacemaker
Too fast
Medication
Ablation
ICD
Common chronic cardiac diseases:
Abnormal heart rhythms : Too fast or slow
7

Mortality from Cardiac Disease in
New Zealand
0
20
40
60
80
100
120
140
160
180
1948 1953 1958 1963 1968 1973 1978 1983 1988 1993 1998 2003 2008 2013
Other forms of heart diseaseMortality rates, 1948–2013
TotalRate (per
Note: Rates are age standardised to the World Health Organization (WHO) standard world
0
50
100
150
200
250
300
350
400
1948 1953 1958 1963 1968 1973 1978 1983 1988 1993 1998 2003 2008 2013
Ischaemic heart diseaseMortality rates, 1948–2013
TotalRate (per
Note: Rates are age standardised to the World Health Organization (WHO) standard
0
1000
2000
3000
4000
5000
6000
7000
8000
1948 1953 1958 1963 1968 1973 1978 1983 1988 1993 1998 2003 2008 2013
Ischaemic heart diseaseNumber of deaths, 1948–2013
Total
0
500
1000
1500
2000
2500
1948 1953 1958 1963 1968 1973 1978 1983 1988 1993 1998 2003 2008 2013
Other forms of heart diseaseNumber of deaths, 1948–2013
Total
8

How do we die?
With a normal heart but other terminal disease
With cardiac disease, but not from a cardiac cause
With cardiac disease
Sudden cardiac death
Pump failure
9

Illness trajectories
and palliative care
BMJ. 330(7498):1007-1011
Valve disease or acute / subacute cardiomyopathy
Chronic heart failure or Atrial fibrillation
Multiple comorbidities
10

Appropriate care during then near the end of life
BMJ. 330 (7498):1007-1011
1997 Palliative care model
2017 Palliative
care model
11

Characteristics of the stages of
progressive heart failureD
isease
modif
yin
g o
r pote
nti
ally c
ura
tive
Supportive and palliative care
Stage I : Chronic disease management phase : NYHA I-III
Effective therapy to prolong survival and improve
Symptoms
Patient and carer education and supported
self management
Regular monitoring and
appropriate review
European Journal of Heart Failure (2009) 11, 433–443
12

Heart failure Treatment Timeline
Pre 1980s 1980s
Bed rest
Inactivity
Fluid
restriction
Diuretics
Digoxin
Heart
transplant
13

Heart failure Treatment Timeline
Pre 1980s 1980s
Bed rest
Inactivity
Fluid
restriction
Diuretics
Digoxin
Heart
transplant
Diuretics
Digoxin
Vasodilators
Inotropes
Heart
transplant
(in NZ)
14

Heart failure Treatment Timeline
Pre 1980s 1980s 1990
Bed rest
Inactivity
Fluid
restriction
Diuretics
Digoxin
Heart
transplant
Diuretics
Digoxin
Vasodilators
Inotropes
Heart
transplant
(in NZ)
Diuretics
ACE inhibitors /
ARBs
Betablockers
Aldosterone
receptor
antagonists
15

Mode of Death in Heart Failure with
Preserved and Reduced EF
J Am Coll Cardiol.2017; 69 (5) 556-69
16

Heart failure Treatment Timeline
Pre 1980s 1980s 1990 2000-20
Bed rest
Inactivity
Fluid
restriction
Diuretics
Digoxin
Heart
transplant
ICDs
Cardiac
resynchronisation
LVAD
ARNIs
Diuretics
Digoxin
Vasodilators
Inotropes
Heart
transplant
(in NZ)
Diuretics
ACE inhibitors /
ARBs
Betablockers
Aldosterone
receptor
antagonists
17

Heart failure Treatment Timeline
Pre 1980s 1980s 1990 2000-202020 and beyond
18

Heart failure Treatment Timeline
Pre 1980s 1980s 1990 2000-202020 and beyond
Bed rest
Inactivity
Fluid
restriction
Diuretics
Digoxin
Heart
transplant
ICDs
Cardiac
resynchronisation
LVAD
1st Palliative care
statement (2009)
ARNIs
Diuretics
Digoxin
Vasodilators
Inotropes
Heart
transplant
(in NZ)
Diuretics
ACE inhibitors /
ARBs
Betablockers
Aldosterone
receptor
antagonists
Gene therapy
Cell genesis
Artifical heart
19

Timeline of Palliative Care in Cardiology
20
Characteristics of the stages of
progressive heart failureD
isease
modif
yin
g o
r pote
nti
ally c
ura
tive
Supportive and palliative care
Stage I : Chronic disease management phase : NYHA I-III
Effective therapy to prolong survival and improve
Symptoms
Patient and carer education and supported
self management
Regular monitoring and
appropriate review
European Journal of Heart Failure (2009) 11, 433–44321

Characteristics of the stage of progressive heart
failureD
isease
modif
yin
g o
r pote
nti
ally c
ura
tive
Supportive and palliative care
Stage I : Chronic disease management phase : NYHA I-III
Effective therapy to prolong survival and improve symptoms
Patient and carer education and supported self management
Regular monitoring and appropriate review
European Journal of Heart Failure (2009) 11, 433–443
Stage II : Supportive and palliative care phase NYHA III-IV
Increased admissions to hospital
Goal of care shifts to maintaining optimal symptom control and
quality of life
Holistic, multidisciplinary involvement with patient and their carers
Start discussions re disease trajectory and advanced care plan22

Markers of
advancing disease Age
Recurrent hospitalision for
decompensated heart failure
and / or a related diagnosis
NYHA IV symptoms
Worsening renal function
Cardiac cachexia
Hyponatraemia
Refractory hypotension
necessitating withdrawal of
medical therapy
NYHA Class Symptoms
I Nil
II Mild
III Moderate
IV Severe or at rest
23

Jo 68 year Maori male
Rheumatic fever as a child – residual moderate AR
MI aged 55 - CABG and mechanical AVR performed
Post op EF 40% with inferior scar from MI
Community cardiac arrest – 57 : bystander CPR - good
recovery : secondary ICD implanted
Onset of permanent AF aged 60 – rate controlled
Gradually worsening LV function with evolution of
worsening MR and TR with pulmonary hypertension
24

Examination• PR 70 BP 90/60 – no postural drop
• Looks cachectic
• JVP above earlobes: Chest clear : Metal heart sounds and murmurs : pulsatile liver with ascites: Oedema to sacrum
Investigations• Hb 85 with ferritin 45
• Creatinine 230 eGFR 22ml/min/1.73m2
• Albumin 27
25

Medications
• Warfarin
• Aspirin
• Metoprolol CR 95mg
• Digoxin 125mcg
• Losartan 50mg
• Bumetanide 3mg bd
• Atorvastatin 80mg
• Spironolactone 50mg od
• Allopurinol 300mg
• Metformin 1g bd
• Vitamin D 50 000
monthly
• Multivitamins
• Omeprazole 40mg o
26

Over last year:
• 4 admissions with heart failure :
• Sept 16 : 6 days
• Jan 17 : 4 days
• Apr 17 : 10 days
• Jun 17 : 17 days
• Struggling with ADLs : sleeps on 3 pillows or in a chair
• Weight 120kg in Sept 16 and now 105kg – but still oedematous
• Appetite not so good
27

Discussion with Joe
“How do you feel things are going with your health?”
Discussion about where things are heading
“If your were to pass away peacefully would you be comfortable
with this? And would you family?”
“Would you like to look at stopping some of your pills?”
28

Deprescription
• Statins
• Anticoagulants• Antiplatelets agents
• Anticoagulants
• Aldosterone receptor antagonists
• ACE inhibitors
• Beta blockers
• Diuretics
29

• What does function does an ICD have?
• Treating bradycardias through back up pacing
• Treating tachycardias through
o Overdrive pacing
o Defibrillating
NZMJ (2010): 123: 1309
ICD Deactivation
30

ICDs prolong life by preventing sudden death
ICDs do not modify the underlying disease
process
Patients with ICDs still die
Death may be
o Due to the underlying cardiac disease
o Due to an underlying non cardiac
pathology
o ICD failure
ICD Deactivation
31

When to discuss?
• Around the time of implantation
• When the patient’s quality of life is declining to the point
where they have reached a point where an ICD discharge
would delay the dying process without adding quality of life /
not be wanted by them
Who should discuss?
• Ideally done in the ambulatory setting
• Clinician who knows the patient and is familiar with their
disease, its management plan and the disease trajectory
• Can involve patient’s primary cardiologist if non cardiac
pathology
ICD Deactivation
32

ICD Deactivation
NZMJ (2010): 123: 1309
• Is not painful
• Will not cause sudden death when the ICD is deactivated
• Will help prevent what can be an unpleasant death
• Who deactivates the ICD?• ICD or Pacing technologist
• Pacing clinic / hospital / hospice
• Need documentation that this has been discussed with the patient and the family
Auckland /Northland DHB: 021 808 605 Counties Manukau DHB: 021 240 7535
Waitemata DHB: 021 806 98533

http://www.advancecareplanning.org.nz/healthcare/
Why am I making an advanced care plan?
When I am dying…
After my death….
34

Advance Directives
Among Hospitalised
Patients with Heart
Failure
JACC Heart Failure 2015 3 (2) 112-21
35

Characteristics of the stage of progressive heart
failureD
isease
modif
yin
g o
r pote
nti
ally c
ura
tive
Supportive and palliative care Bereavement care
Stage I : Chronic disease management phase : NYHA I-III
• Effective therapy to prolong survival and improve symptoms
• Patient and carer education and supported self
management
• Regular monitoring and appropriate review
Poor prognostic markers
Focus on patient / family
end of life cares and wishes
Emotional support
Stage III
Terminal care phase
36

Palliation of symptoms in
chronic heart failure
➢ Dyspnoea
➢ Diuretics for hypovolaemia
➢ Opiates
➢ Benzodiazepines
➢ Pain
➢ Antianginals
➢ Non NSAID based analgesia
➢ Annorexia / cachexia
➢ Treat the reversible
➢ Small regular meals / nutritional supplementation
➢ Fatigue
➢ Correct the reversible
➢ Exercise
➢ Psychological support
➢ Depression
➢ Psychological support
➢ SSRIs
37

Pericardial disease in palliative care
(effusions)
Approximately 30% of effusions treated at MMH
are malignant
1 year survival < 10%
Treatment is for symptomatic relief
Pericardiocentesis
Pericardial window
Heart, lung and Circulation2014 Volume 23, Supplement 1, Page e38
38

Palliative care…through a team approach
Is applicable early in the course of illness in
conjunction with other therapies that are intended
to prolong life
Offers family a support system to help the family
cope during the patient’s illness and in their own
bereavement
Enhance quality of life and may positively
influence the course of illness
Offers a support system to help patients life as
actively as possible until death
Affirms life and regards dying as a normal process
Provides relief from distressing symptoms
Intends neither to hasten or postpone death
Taha Hinengaro
Taha TinanaTaha WhanauTaha Wairua39

General
Medical
team
Health
psychologist
Spiritual /
religious
leaders
Cardiology
team
Physiotherapist
Palliative
care team
Primary care
Cultural
supportLawyers
Occupational
therapist
Nursing
staff
Alternative
therapist
40

Heart failure (HF) patients experience high rates of hospitalisation and mortality:
20% at 6 months, 30% at 12 months : a prognosis worse than some cancers
Studies show that between 80 – 87% of HF patients with a predicted survival of less than 1
and 2 years were unaware HF was a terminal illness
National and international HF guidelines recommend the introduction of palliative care
at the start of the illness trajectory
30-day readmission rates used as a benchmarking measure between hospitals in
NZ and worldwide for cost analysis of HF admissions and quality of care
HF Audit, Hutt 2015 – 62% of HF patients readmitted within 30 days were dead
within 6 months
Only 12% of these patients received palliative care41

JACC : Jul 17: 70 (3): 331-41
Medication Usual and Palliative care Usual Care
ACE inhibitor 17 (22.7) 16 (21.3)
ARB 4 (5.3) 7 (9.3)
Aldosterone antagonist 30 (40.0) 22 (29.3)
Aspirin 54 (72.0) 46 (61.3)
Beta-blocker 51 (68.0) 48 (64.0)
Diuretics
Bumetanide 1 (1.3) 1 (1.3)
Furosemide 39 (52.0) 49 (65.3)
Torsemide 27 (36.0) 14 (18.7)
Statin 43 (57.3) 41 (54.7)
42

Challenges to palliative care in Cardiology
Disease trajectories are not well defined
Cardiology practice and training focused on life
prolonging intervention
Patient expectations
Lack of access to resource – in and outpatients
Pressure of time
Palliative care discussions can be time consuming and
emotionally intense
43

I can’t help
Isn’t this
someone else
job… The
palliative care
team are involved
I’m too busy….
I’ll see
him tomorrow
Maybe
he’ll
die before I
see him…
I can’t
change his
situation
I won’t know
what to say
What if
I upset him
more?
I should have
done the
‘death and dying’ paper
at university
Courtesy of Miriam Wood, Health Psychologist, CMDHB
44

Physicians and death : who cares for the carers?
Current Oncology2017 24(4) e277-284
45

BurnoutMeasures That May Help Prevent BurnoutMindful meditationReflective writingAdequate supervision and mentoringSustainable workloadPromotion of feelings of choice and controlAppropriate recognition and rewardSupportive work communityPromotion of fairness and justice in the workplaceTraining in communication skillsDevelopment of self-awareness skillsPractice of self-care activitiesContinuing educational activitiesParticipation in researchMindfulness-based stress reduction for teamMeaning-centered intervention for team
IndividualOverwhelming physical and emotional exhaustionFeelings of cynicism and detachment from the jobA sense of ineffectiveness and lack of accomplishmentOveridentification or overinvolvementIrritability and hypervigilanceSleep problems, including nightmaresSocial withdrawalProfessional and personal boundary violationsPoor judgmentPerfectionism and rigidityQuestioning the meaning of lifeQuestioning prior religious beliefsInterpersonal conflictsAvoidance of emotionally difficult clinical situationsAddictive behaviorsNumbness and detachmentDifficulty in concentratingFrequent illnessStaff conflicts
TeamLow moraleHigh job turnoverImpaired job performance (decreased empathy, Increased absenteeism)
JAMA, March 18, 2009—Vol 301, No. 11
46
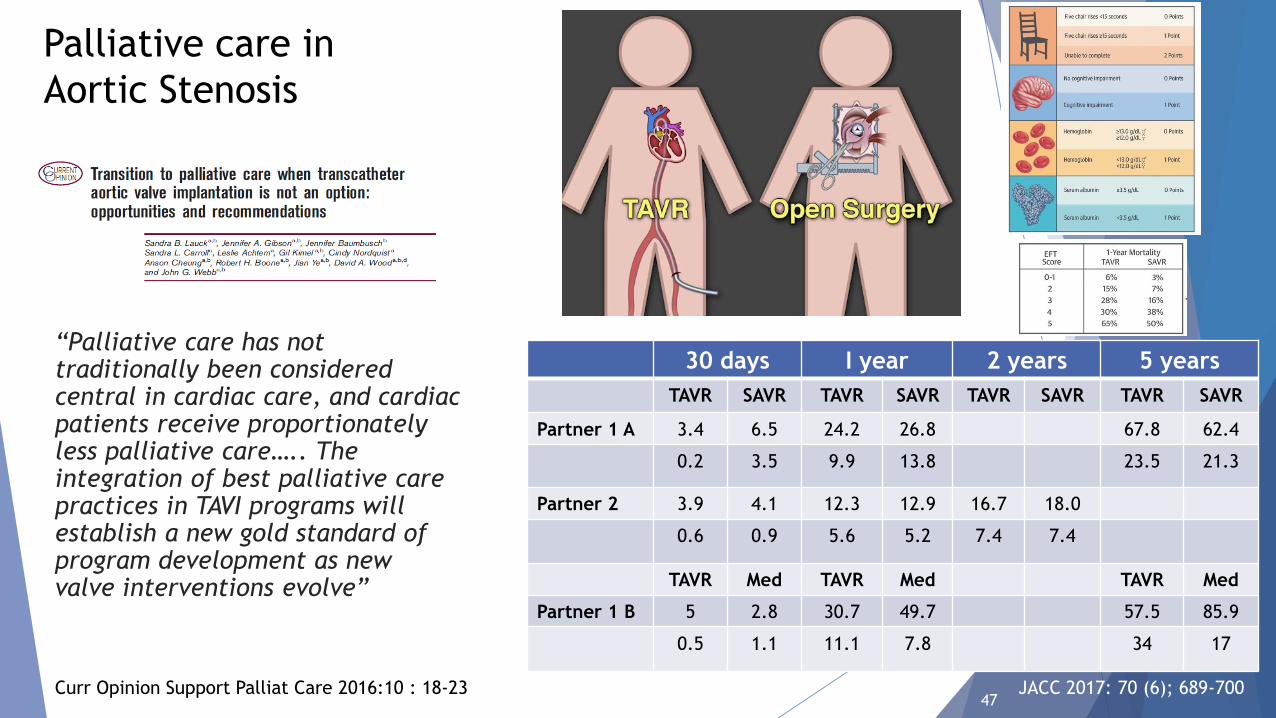
Palliative care in
Aortic Stenosis
“Palliative care has not traditionally been considered central in cardiac care, and cardiac patients receive proportionately less palliative care….. The integration of best palliative care practices in TAVI programs will establish a new gold standard of program development as new valve interventions evolve”
Curr Opinion Support Palliat Care 2016:10 : 18-23
30 days I year 2 years 5 years
TAVR SAVR TAVR SAVR TAVR SAVR TAVR SAVR
Partner 1 A 3.4 6.5 24.2 26.8 67.8 62.4
0.2 3.5 9.9 13.8 23.5 21.3
Partner 2 3.9 4.1 12.3 12.9 16.7 18.0
0.6 0.9 5.6 5.2 7.4 7.4
TAVR Med TAVR Med TAVR Med
Partner 1 B 5 2.8 30.7 49.7 57.5 85.9
0.5 1.1 11.1 7.8 34 17
JACC 2017: 70 (6); 689-70047

“Life is pleasant. Death is peaceful. It’s the transition that is troublesome”
Isaac Asimov
48