tia and stroke: diagnosis and treatment -...
TRANSCRIPT
TIA and Stroke:Diagnosis and Treatment
Robert Baldor, MD, FAAFP

Robert Baldor, MD, FAAFPProfessor and Vice Chair, Department of Family Medicine and Community Health/Director, Community-Based Education, Office of Undergraduate Medical Education/Director of Health Policy Education, Meyers Primary Care Institute/Medical Director, Center for Developmental Disabilities Evaluation and Research at the Eunice Kennedy Shriver Center, University of Massachusetts (UMass) Medical School, Worcester
Dr. Baldor has been teaching for 30 years and practices family medicine at the UMass Memorial Medical Center, Worcester. A member of the Massachusetts Governor’s Commission on Intellectual Disability, he has been recognized in The Best Doctors in America: Northeast Region and is a past-president of the Massachusetts Academy of Family Physicians. He publishes and presents regularly on a variety of family medicine topics and is an associate editor for The 5-Minute Clinical Consult. Dr. Baldor practices family medicine with a special interest in developmental and intellectual disabilities. Throughout the years, he has spoken on a variety of primary care topics at the AAFP's annual meeting.

Learning Objectives1. Assess patients presenting with possible signs of TIA or stroke; ordering appropriate imaging if necessary. 2. Develop collaborative care plans to assist patients in making behavioral modifications to decrease their stroke risk and recognize the warning signs of a stroke. 3. Propose appropriate treatment options to improve outcomes in patients who suffer a stroke. 4. Counsel patients and their family members on how to cope with the effects of stroke.

Apoplexy!• Hippocrates ‘struck down by violence’• Leading cause of disability, cognitive
impairment & death• 2nd leading cause of death worldwide

Risk FactorsModifiable
• Hypertension• Diabetes• CAD/PAD • Obesity• Tobacco use• Hyperlipidemia• Physical inactivity• ? Diet soda
Others …• Age• Sex (M>F)• Race• Prior stroke / TIA• Sickle Cell

Sickle Cell• 10% Stroke incidence• Screen annually with transcranial Doppler
ultrasound flow velocities from age 2 to 18• Treat prophylactically with transfusions• Hydroxyurea appears to be as effective
TWiTCH trialDec2015

Medications…• Combination BCPs
– Risk of stroke doubles (but still very low)– Progestin-only – no increased risk
• NSAIDs – Increased risk with prolonged, high dose– Use low dose for short periods of time
Long Hours ????!!!!????• Meta-analysis with significant association between
work hours and stroke• Working > 55 hours/week associated with 33% ↑
stroke risk vs < 40 hours
"Our findings suggest that more attention should be paid to the management of vascular risk factors in individuals who work long hours."
LancetAugust,2015;CreativeCommonsLicense

Depression ?• The Health & Retirement Study (1998-
2010) – 16,000 men & women – 1,200 strokes occurred
• High depressive symptoms 2X stroke risk
JAHA,May2015;CreativeCommonsLicense

Circle of Willis…
Modifiedfrom:https://commons.wikimedia.org/wiki/File:Circle_of_Willis_unlabeled.svg.Source:Gray519.png.Author:Rhcastilhos.SchematicrepresentationofthecircleofWillis,arteriesofthebrainandbrainstem.1.24.2007
Middle Cerebral
Anterior Cerebral
PosteriorCerebral
Internal Carotid Artery
Basilar Artery
Communicating Arteries

Which artery is most commonly involved with stroke?
1. Anterior cerebral artery (ACA)2. Middle cerebral artery (MCA)3. Posterior cerebral artery (PCA)4. Basilar artery

Etiology• Ischemic (85%)
– MCA occlusion → 90% of infarcts• Hemorrhage
– Intracerebral (10%)– Subarachnoid (5%)
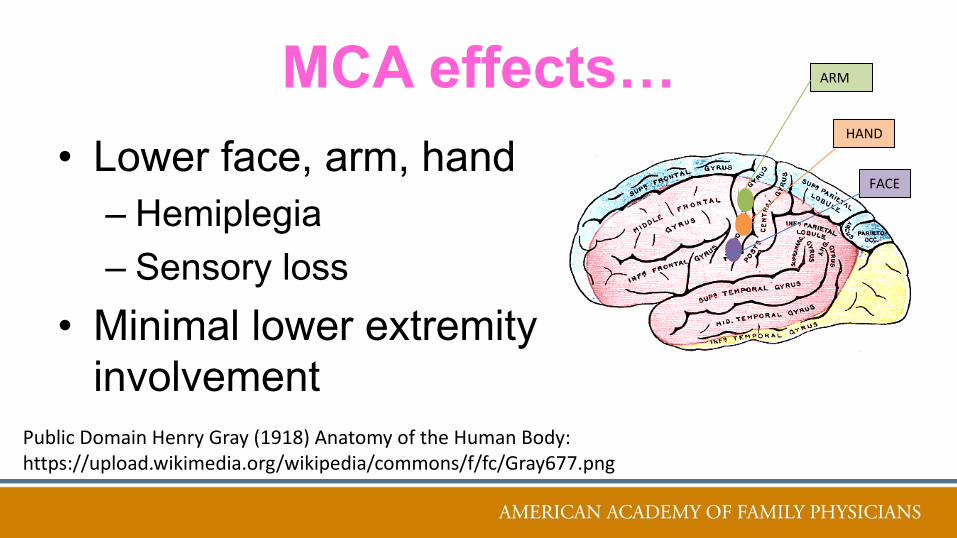
MCA effects…• Lower face, arm, hand
– Hemiplegia– Sensory loss
• Minimal lower extremity involvement
PublicDomainHenryGray(1918)AnatomyoftheHumanBody:https://upload.wikimedia.org/wikipedia/commons/f/fc/Gray677.png
ARM
FACE
HAND

Laterality determines speechL sided (dominant) stroke: Aphasia
R sided stroke: Apraxia and Neglect
Wernicke’sAreaReceptiveAphasia
(understandinglanguage)
Broca’sAreaExpressiveAphasia(makinglanguage)

ACA effects…• Less common stroke
– Leg weakness/sensory loss – Behavioral abnormalities– Incontinence
Modifiedfrom:PublicDomainHenryGray(1918)AnatomyoftheHumanBody:https://upload.wikimedia.org/wikipedia/commons/f/fc/Gray677.png
LEG

PCA effects…• Visual deficits
– Homonymous hemianopia– Alexia
• inability to understand written language
PublicDomainHenryGray(1918)AnatomyoftheHumanBody:https://upload.wikimedia.org/wikipedia/commons/f/fc/Gray677.png
Vision

Warning Signs …Face droopingArm weaknessSpeech difficultyTime to call 911
AmStrokeAssn

Ischemic Etiology• Large Artery
– Carotid atherosclerosis/dissection/vasculitis• Small Artery
– Lacunar infarct• Cardiac embolism
– Valve disease/Afib/Cardiomyopathy/Myxoma/ Patent foramen ovale

Intracranial Hemorrhage• Aneurysm or AVM rupture (47%)• Hypertensive (36%)• Tumor/Other (17%)
– A sense of unease, then……abrupt onset of symptoms, acute decompensation

CerebellarHemorrhageAtaxia,vomiting
PontineHemorrhageComa,decerebrateposturingorflaccidity
BasalGanglionBleedStupor,coma
Hypertensive ICHSmallarteryrupturedeepinbrain

Subarachnoid Hemorrhage“Worst headache of my life”
– 40% ‘Sentinel’ HA 2-8 weeks prior§ Photophobia§ Nuchal rigidity § Seizures§ Nausea and vomiting

Headache ‘Red Flags’…• Worse headache of my life…
– Sudden onset• 1st HA after age 50• Focal neurologic signs• S&S of systemic illness
– Fever, immunocompromise• Trauma
CreativeCommons:https://openclipart.org/detail/133015/al-with-red-flag
TIA…
10x more likely to have a stroke after a TIA
CreativeCommonsLicense
Transient Ischemic Attack• Temporary blockage of cerebral blood flow
– Thrombosis or embolism• A brief episode of neurologic dysfunction
– Symptoms typically lasting < 1 hour• Sudden onset, focal neurologic deficit or
speech disturbance..AHA/ASAStroke2009

ABCD2 TIA Scoring System(Age, BP, Clinical features, Duration, DM)
Sign/Symptom Points
Age≥60years 1
SBP≥140mmHgorDBP≥90mmHg 1
Unilateralweakness 2
Speechimpairmentwithoutweakness 1
TIADuration> 60minutes 2
TIADuration10-59minutes 1
Diabetesmellitus 1
ConsiderAdmission TotalPoints > 3
Lancet.2007

TIA Evaluation …• MRI performed within 24 hours
– R/O infarct
• Carotid Ultrasound– If > 60 years of age
• EKG, ECHO, Holter also reasonable
AHA/ASAStroke2009;Int JCPract April2015

TIA Treatment• Anti-coagulate if Afib• Antiplatelet if not• Carotid endarterectomy for critical stenosis• Treat HTN• Statin therapy
NEJMApril2016

Stroke Management
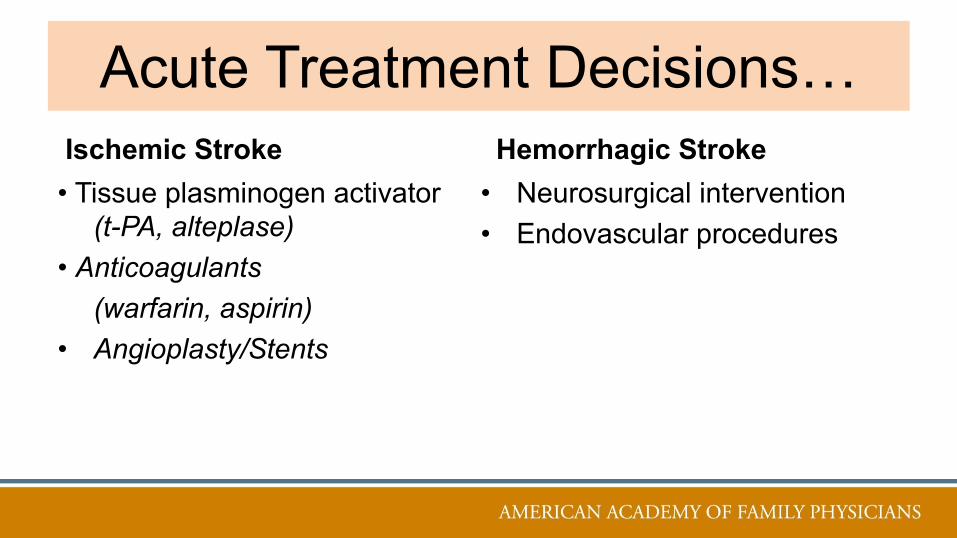
Acute Treatment Decisions…Ischemic Stroke• Tissue plasminogen activator
(t-PA, alteplase)• Anticoagulants
(warfarin, aspirin)• Angioplasty/Stents
Hemorrhagic Stroke• Neurosurgical intervention• Endovascular procedures

• Non-contrastCTScanGoldStandard• Superiorforshowinghemorrhage
• ContrastCTidentifiesaneurysms,AVMs,tumors• NotrequiredtodetermineifatPA candidate
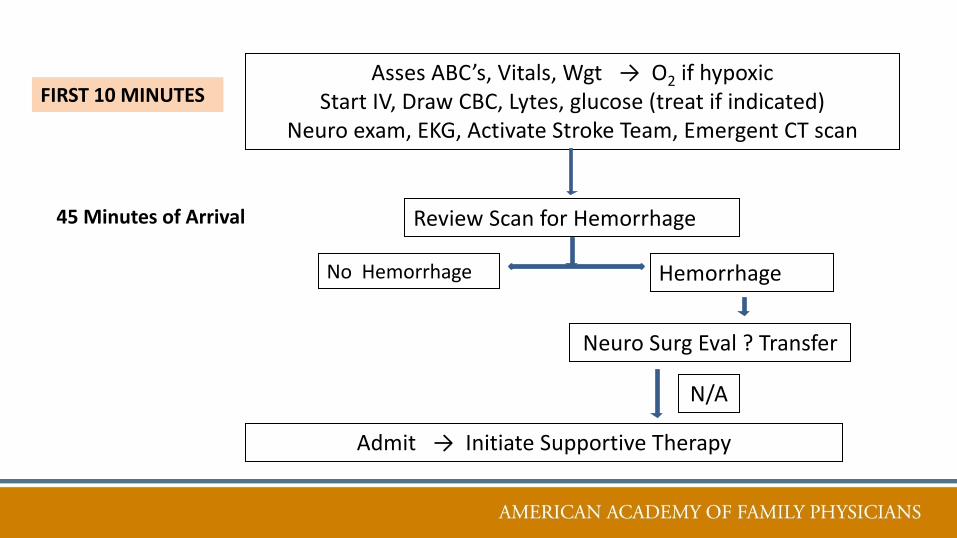
AssesABC’s,Vitals,Wgt →O2 ifhypoxicStartIV,DrawCBC,Lytes,glucose
Neuroexam,EKG,ActivateStrokeTeam,EmergentCTscanFIRST10MINUTES
JAMA9.2017
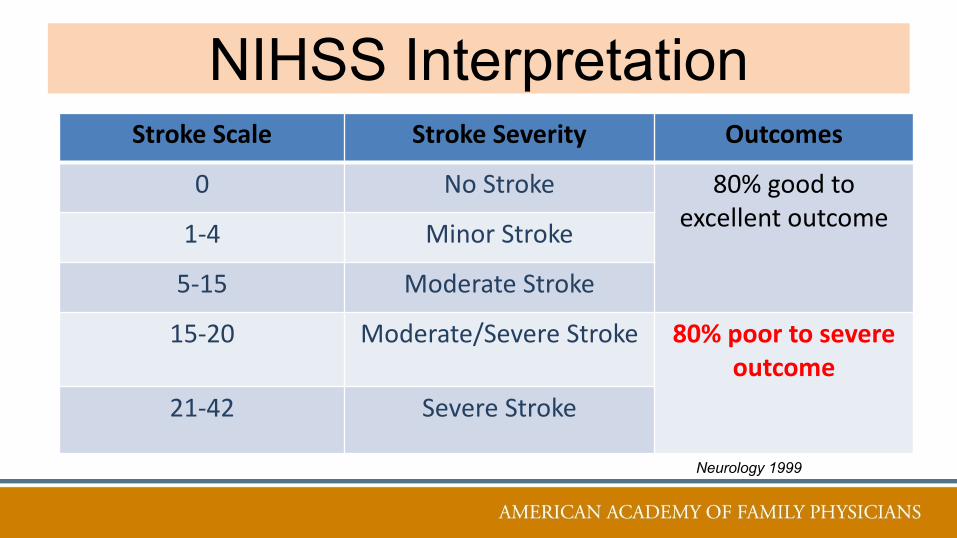
NIHSS Interpretation StrokeScale StrokeSeverity Outcomes
0 NoStroke 80%goodtoexcellentoutcome1-4 MinorStroke
5-15 ModerateStroke
15-20 Moderate/SevereStroke 80%poortosevereoutcome
21-42 SevereStroke
Neurology 1999

AssesABC’s,Vitals,Wgt →O2 ifhypoxicStartIV,DrawCBC,Lytes,glucose(treatifindicated)
Neuroexam,EKG,ActivateStrokeTeam,EmergentCTscan
ReviewScanforHemorrhage
NoHemorrhage Hemorrhage
NeuroSurg Eval ?Transfer
FIRST10MINUTES
45MinutesofArrival
AssesABC’s,Vitals,Wgt →O2 ifhypoxicStartIV,DrawCBC,Lytes,glucose(treatifindicated)
Neuroexam,EKG,ActivateStrokeTeam,EmergentCTscan
ReviewScanforHemorrhage
NoHemorrhage Hemorrhage
NeuroSurg Eval ?Transfer
Admit→InitiateSupportiveTherapy
FIRST10MINUTES
45MinutesofArrival
N/A
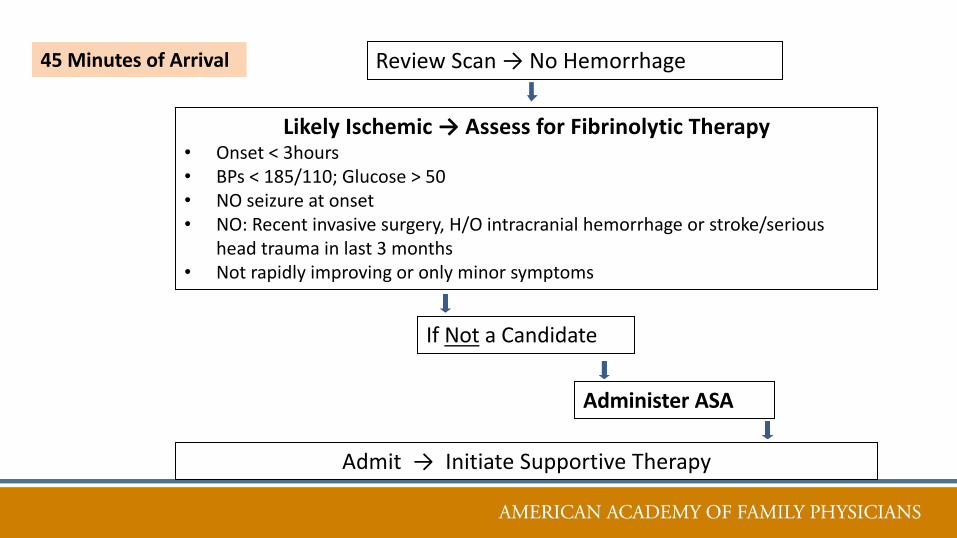
ReviewScan→NoHemorrhage45MinutesofArrival
LikelyIschemic→AssessforFibrinolyticTherapy• Onset<3hours• BPs<185/110;Glucose>50• NOseizureatonset• NO:Recentinvasivesurgery,H/Ointracranialhemorrhageorstroke/serious
headtraumainlast3months• Notrapidlyimprovingoronlyminorsymptoms
IfNot aCandidate
AdministerASA
Admit→InitiateSupportiveTherapy

ReviewScan→NoHemorrhageLikelyIschemic→CandidatefortPA
Admit→InitiateSupportiveTherapy
45MinutesofArrival
Give tPA
Review risks/benefitsDisability risk ¯ 30% despite 5% ICH risk
1hourofArrival
• Tissueplasminogenactivator• IVtPA window3hours

Endovascular Thrombectomy • Proximal ICA or MCA occlusion• Used in adjunct with tPA• Effective up to 6 hours
– MERCI system removes clot with corkscrew-like apparatus
– PENUMBRA system aspirates clotLancet2016;Stroke2016

Ischemic Stroke: BP Management• Maintain cerebral perfusion• ↑BP a response, not cause of arterial occlusion
– An effort to perfuse penumbra• Lower BP only if SBP > 220 or DBP >120• Or if tPA candidate…
– Labetalol 10 mg IV q 10 min, till BP ↓ 20%

What is the target Systolic BP for a hemorrhagic stroke?
1. Treat to < 2202. Treat to < 2003. Treat to < 1804. Treat to < 140

Hemorrhagic Stroke: BP Management
• Lower SYS BP < 180• No benefit for < 140
– IV nicardipine if needed• Avoid hemorrhagic expansion, especially
in AVMs and aneurysms
NEJM2016

What About Hypotension??• Maintain adequate cerebral blood flow• Keep BP > 100/70• Fluids and vasopressors if needed • Search for cause

Which is an independent risk factor for poor stroke outcomes?
1. Hypoglycemia2. Hyperglycemia
Supportive Therapy • Treat hyperglycemia
– Edema/infarct worsen
• Treat fevers > 37.5 C– Fever for > 24 hrs correlates with stroke extension– Don’t assume neurogenic – look for source

Basic Stroke Evaluation• Carotid ultrasonography ± transcranial Doppler• Transthoracic echocardiography (TEE)• ECG/markers of cardiac ischemia• EKG monitoring• Routine labs
– CBC; BMP (glucose)– RPR; ESR – INR; PT/INR, PTT
A Cryptogenic Stroke is:1. An infarct for which no probable cause is
identified after an adequate work-up2. An incidental infarct seen on an MRI not
obtained as part of a stroke work-up3. An infarct in an adult due to a previously
undiagnosed patent foramen ovale

Other considerations…• 30 day event monitor• Blood alcohol/tox screen • Pregnancy test • CXR (? lung disease) • EEG (? seizures) • Thrombotic W/U (unclear cause / +FH)
– Antiphospholipid syndrome

3 Main Rehab GoalsTailor to specific stroke-related sequela1. Prevent complications of inactivity 2. Treat medical complications3. Prevent recurrent stroke/cardiovascular events
1
StrokeMay2016

1. Complications of Inactivity• NPO/bedside swallow assessment for aspiration• Compression devices/ambulation for PE/DVT • Reposition q2h to avoid skin breakdown

2. Medical ComplicationsSpasticity• ROM exercises/thermal/electric stimulation/splinting• Dantrolene, tizanidine
Depression (↑ mortality)• Pharmaco/Psychotherapy
49

3. Prevention of RecurrenceNon-cardiogenic etiology• Antiplatelet therapy with aspirin • 60% ↓ risk of recurrent stroke next 6 weeks• 90% ↓ risk of stroke after TIA, in next 12 weeks
50
StrokeApril2015,,LancetMay2016

Antiplatelet Therapy Non-cardiogenic etiology
§ Aspirin alone (50-325 mg daily)§ Extended-release dipyridamole/aspirin
(Aggrenox) § Clopidogrel (Plavix) alone§ Ticagrelor (Brilinta) alone
StrokeApril2015,NEJMMay2016

USPSTF (April 2016)Grade B recommendation for low-dose (81mg) ASA for the primary prevention of CVD and colorectal CA in adults 50 to 59 years who:
– have a > 10% 10-year CVD risk,– are not at increased risk for bleeding,– have a life expectancy of at least 10 years,– and are willing to take daily ASA for > 10 years.

Cardiogenic Embolism Anti-coagulate or Not?
• Anticoagulation ↓ stroke risk 60-80% – But increases risk of bleeds…
• Calculators score relative risk vs benefit…
http://www.mdcalc.com/specialty/cardiology/link requires free login to access

To Predict Stroke Probability…• CHADS2• CHADS2 – VASc
– CHF, HTN, Age, DM, Sex, Stroke, Vascular Disease• ATRIA
– Proteinuria, GFR• ABC
– BNP, Troponin
Eur Heart2016

To Predict Bleeding Risk…HAS-BLED
– HTN, ABN renal/liver function, Stroke, Bleeding history, Labile INR, Elderly, Drugs/alcohol
ATRIA (AnTicoagulation and Risk factors In Afib)– Anemia, Renal Fxn, Age ( > 75), Prior Bleed, HTN
ORBIT– Older age (> 75), Reduced H/H anemia, Bleeding
history, renal Insufficiency, antiplatelet Treatment Eur HeartJ2015

Anticoagulants…Warfarin• Vit K antagonist• Reversal with prothrombin complex
concentrate (better than FFP)

Direct Oral Anticoagulants…Direct Thrombin Inhibitor• Dabigatran (Pradaxa)
– Idarucizumab (Praxbind) reversal

Direct Factor Xa Inhibitors • Apixaban (Eliquis)• Rivaroxaban (Xarelto)• Edoxaban (Savaysa) • Betrixaban (Bevyxxa)Reversal agents Andexa – not FDA approved

Warfarin or DOAC ??• DOAC non-inferior in ↓ stroke risk & all-
cause mortality for non-valvular Afib, while not increasing major bleeding complications– Apixaban & dabigatran w/lower bleeding rates
• Well-managed warfarin has low all-cause death rates and low complication rates…
JFPJune2016;JAMAMay2016,JAMAApril2016,BMJ2016
Bleeding concerns??• DOAC have short ½ lives vs warfarin
– Just stop the medication!• JFP review 2017
– Apixaban 5mg BID best efficacy & safety data
60

Carotid Endarterectomy (or Stenting) ?
• Stroke/TIA & carotid artery stenosis > 70%o Endarterectomy if perioperative M&M are < 6%
• ACT I & CREST studieso Stenting comparable to endarterectomy
NEJMFeb2016

• Control high blood pressure• Treat heart disease• Stop cigarette smoking• Reduce blood cholesterol levels
LancetJune2016;CreativeCommons:https://rkutchjm.files.wordpress.com/2013/06/prevention-works-to-lower-risk-of-disease.jpg

Mediterranean Diet Less likely to suffer an ischemic stroke • Fruits and vegetables, whole grains,
legumes, nuts, fish, poultry and olive oil• Limited consumption of red meat, sweets,
saturated fats
American Stroke Association, news release, Feb. 2015

Exercise…• Physically active lifestyle …
– At least 40 minutes of walking/biking per day– Plus 1 additional hour of exercise per week
AFPJune2016
• POC diagnostic test for ischemic stroke• PPAR-α gene therapy for insulin resistance• Stem cells to repair damage • VR video games…• Robotic exo-skeletons…
PLOSOne2016,Stroke2016CreativeCommonsLicense:http://thinkingfutures.net/resources/building-strategic-futures-guides/

Practice Recommendations…• Educate your patients about F.A.S.T. • Work with your community to insure timely
stroke protocols are in place• Emphasize stroke prevention• Develop post-stroke rehabilitation
protocols for your office
References1. Adams RJ, Albers G, Alberts MJ, et al. (1) Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack. (2) Update to the AHA/ASA recommendations for the prevention of stroke in patients with stroke and transient ischemic attack. 2008; http://www.guideline.gov/content.aspx?id=12950&search=stroke2. Yew KS, Cheng EM. Diagnosis of acute stroke. American family physician. Apr 15 2015;91(8):528-536.3. Randel A. AHA and ASA Release Guideline for Prevention of Future Stroke in Patients with Stroke or TIA. American family physician. Jan 15 2015;91(2):136-137.4. Simmons BB, Cirignano B, Gadegbeku AB. Transient ischemic attack: Part I. Diagnosis and evaluation. American family physician. Sep 15 2012;86(6):521-526.5. The Medical Letter on Drugs and Therapeutics. ISSUE 1465; March 30, 2015. Edoxaban(Savaysa) - The Fourth New Oral Anticoagulant