thyrotoxicosis and other thyroid diseases
TRANSCRIPT
THYROTOXICOSIS AND OTHER THYDROID DIEASES
KIZITO FELIXMANJU BUDIA

Thyroid hormone synthesis
THYROTOXOCOSIS
• Is a clinical syndrome which results from exposure of the body tissues to excess circulating levels of free thyroid hormones.
• Also know as hyperthyroidism.

Epidemiology
• It is common disorder with a prevalence of about 20/1000 females
• Males are affected five times less frequently
Aetiology
• Graves diseases (90% of cases)• Multinodular goitre• Autonomously functioning solitary thyroid
nodule• Thyroiditis ie subacute (de quervain’s),post partum
• Iodide induced ie drugs (amiodarone),radiographic constrast media,iodine prophylaxis programme
• Extra throidal source of thyroid hormone excess ie factitious hyperthyroidism, struma ovari

Aetiology cont…
• TSH induced ie inappropriate TSH secretion by pituitary,chriocarcinoma and hydatidiform mole
• Follicular carcinoma +_ metastatases
Clinical features
• Goitre ie diffuse +_ bruit, nodular
• Gastrointestinal ie weight loss, hyperdefecation,diarrhoea and steatorrhoea,anorexia,vomiting
• Cardiorespiratory ie palpitation,increased pulse pressure, ankle oedema in absence of hf,angina ,cardiomyopathy and cardiac failure,dyspnoea on exertion,exacerbation of asthma
• Neuro muscular ie nervousness, irritability,emotional lability,pshchosis,tremor,hyper reflexia ii sustained clonus,Muscle weakness ,proximal myopathy, bulbar myopathy,periodic paralysis
• Dermatological ie increased sweating, pruritus,palmar erythema, spidernaevi,onycholysis,alopecia,pigementation,viltigo,digital clubbing,pretibial myoedema

Clinical features….
• Reproductives ie amenorrhoea/ oligmenorrhoea,infertility, spontaneous abortion, loss of libido ,impotence
• Ocular ie lid retraction,lid lag,grittiness, excessive lacrimation,chemosis,exopthalmos,corneal ulceration, ophthalmoplegia, dilopia,papilloedema ,loss of visual acuity
• Other ie heat intolerance,fatigue ,apathy,gynaecomastia,lymphadenopathy,thirst,osteoporosis

GRAVES DIASEASE
• It is characterised by presence of diffuse thyroid enlargement, ophthlmopathy and rarely pretibial myxedema.
• Occurs at any age but unusual before puberty • Most commonly affects the 30-50 year old age
group.

Pathogensis of GD
• Is a major immunologically mediated form of hyperthyroidism
• Production of IgG antibodies directed against the TSH receptor on the thyroid follicular cell
• This stimulate thyroid hormone production and majority goiter formation
• The antibodies are called thyroid stimulating immunogloblins or TSH receptor antibodies(TRAb) can be detected in serum

Clinical features of GD
• Goitre
• Opthalmopathy
• Pretibial myxoedema

Management of GD
• Antithyroid drugs carbimazolemethimazole,Propythiouracil• Radioactive iodine• Beta adrenoceptor antagonist Propranolol(160mg daily in divided dose)Nadolol(40-80mg once daily)

Management…….
• NB : beta adrenoceptor antagonist will alleviate but not abolish symptoms of hyperthrodoism in 24-48 hours, used for a short term treatment.
• Subtotal throidectomy
TOXIC MULTINODULAR GOITRE
• This form of hyperthyroidism is more common in women.
• Mean age is 60 years• Thyroid hormones usually slightly elevated• Cvs features like AF or CF are common• Treatment with large doses of iodidne 131.

Toxic adenoma
• The nodule is a follicular adenoma which autonomously secretes excess thyroid hormones
• Nodule is >3cm• This inhibits endogenous TSH secretion and
atropy of the rest of the gland• Common in females 40 years above• Diagnosis by isotope scanning
Toxic adenoma…..
• Hyper thyroidism is mild with T3 –thyrotoxicosis
• Treatment is by hemi thyroidectomy or by iodine 131

Sub acute thyroiditis
• Is virus induced (coxsackie ,mumps or adenovirus) inflammation of the thyroid gland which results in release of colloid and its constituents into circulation.
• Characterized by pain in the thyroid region radiating to the jaw ,ears worsened by swallowing ,coughing and movements of the neck.

Sub acute thyroiditis …..
• Palpable thyroid enlarged and tender• Affect females aged 20-40years• Thyroid hormones levels are raised for 4-6wks
until a preformed colloid is depleted• Hyperthyroidism is followed by hypothyroidism,
the normal thyroid functions within 4-6 months• Management NSAIDS for pain ,propranolol
160mgs,at times prednisolone 40mg daily for 3-4wks.no need for anti thyroid drugs

Hypothyroidism
• Defn • Hypothyroidism is diminished production of thyroid
hormone leading to clinical manifestations of thyroid insufficiency
• Iodine deficiency is the most common cause worldwide
• In areas of iodine sufficiency, autoimmune(Hashimoto’s thyroiditis) disease and iatrogenic causes(trmt of hyperthyroidism) are most common
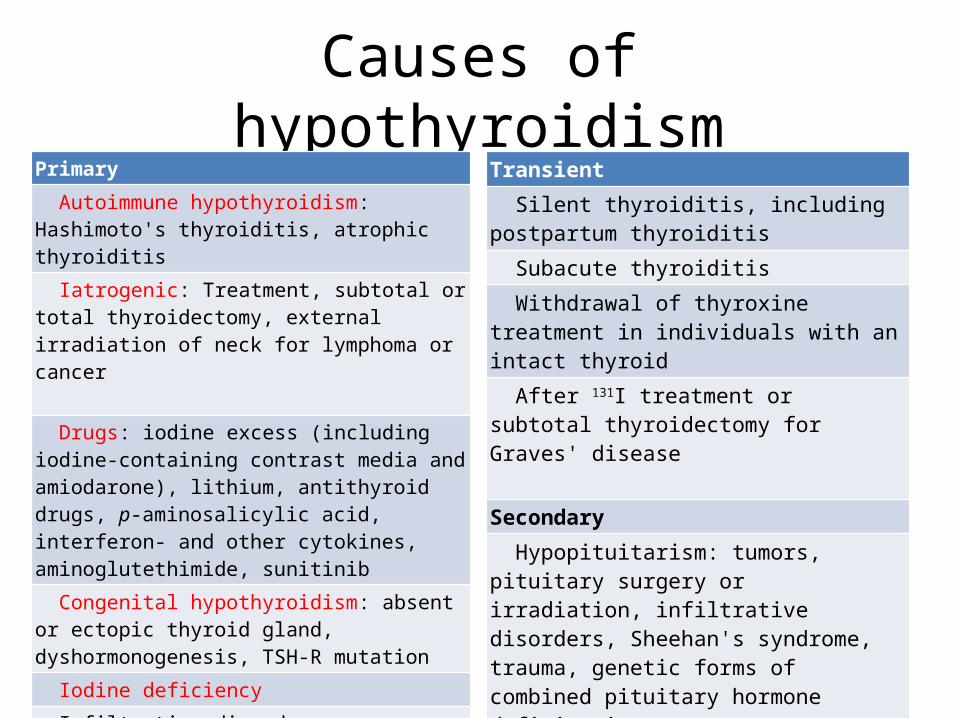
Causes of hypothyroidismPrimary Autoimmune hypothyroidism: Hashimoto's thyroiditis, atrophic thyroiditis
Iatrogenic: Treatment, subtotal or total thyroidectomy, external irradiation of neck for lymphoma or cancer Drugs: iodine excess (including iodine-containing contrast media and amiodarone), lithium, antithyroid drugs, p-aminosalicylic acid, interferon- and other cytokines, aminoglutethimide, sunitinib
Congenital hypothyroidism: absent or ectopic thyroid gland, dyshormonogenesis, TSH-R mutation
Iodine deficiency Infiltrative disorders: amyloidosis, sarcoidosis, hemochromatosis, scleroderma, cystinosis, Riedel's thyroiditis
Overexpression of type 3 deoiodinase in infantile hemangioma
Transient
Silent thyroiditis, including postpartum thyroiditis
Subacute thyroiditis
Withdrawal of thyroxine treatment in individuals with an intact thyroid
After 131I treatment or subtotal thyroidectomy for Graves' disease
Secondary
Hypopituitarism: tumors, pituitary surgery or irradiation, infiltrative disorders, Sheehan's syndrome, trauma, genetic forms of combined pituitary hormone deficiencies
Isolated TSH deficiency or inactivity
Bexarotene treatment
Hypothalamic disease: tumors, trauma, infiltrative disorders, idiopathic

Symptoms and signs of hypothyroidism(in adults)
Symptoms •Tiredness, weakness•Dry skin•Feeling cold•Hair loss•Difficulty concentrating and poor memory•Constipation•Weight gain with poor appetite•Dyspnea•Hoarse voice•Menorrhagia (later oligomenorrhea or amenorrhea)•Paresthesia•Impaired hearing
Signs •Dry coarse skin; cool peripheral extremities•Puffy face, hands, and feet (myxedema)•Diffuse alopecia•Bradycardia•Peripheral edema•Delayed tendon reflex relaxation•Carpal tunnel syndrome•Serous cavity effusions

Evaluation of hypothyroidism
Measure TSH
Elevated Normal
MeasureUnbound T4
Normal
Mild hypothyroidism
TPOAb+ or symptomatic
T4 trmt
TPOAb- or no symptoms
Annualfollowup
Low
Primary hypothyroidism
TPOAb+
Autoimmune hypothyroidism
T4 trmt
TPOAb-
Rule out other causes of hypothyroidism
Pituitary disease suspected
No
No further tests
Yes
Measure unbound T4
Low Normal
Rule out drug effects, sick euthyroid syndrome, then evaluate ant. Pituitary fxn
No further tests

Congenital hypothyroidism
• Hypothyroidism occurs in about 1 in 4000 newborns• Neonatal hypothyroidism is due to – thyroid gland dysgenesis(80–85%),– inborn errors of thyroid hormone synthesis in 10–15%,
and– TSH-R antibody-mediated in 5% of affected newborns
• The developmental abnormalities are twice as common in girls
• Mutations are being increasingly identified, but the vast majority remain idiopathic

Congenital hypothyroidism contd..
• Clinical manifestations– The majority of infants appear normal at birth– <10% are diagnosed based on clinical features,o prolonged jaundice, o feeding problems, o Hypotonia,o enlarged tongue, o delayed bone maturation,o umbilical hernia
• Permanent neurologic damage if treatment is delayed• Other congenital malformations, especially cardiac, are four
times more common in congenital hypothyroidism

Diagnosis and treatment
• Neonatal screening programs have been established. These are generally based on measurement of TSH or T4 levels in heel-prick blood specimens.
• When the diagnosis is confirmed,– T4 is instituted at a dose of 10–15 g/kg per day, and the dose is
adjusted by close monitoring of TSH levels. – T4 requirements are relatively great during the first year of life, and a
high circulating T4 level is usually needed to normalize TSH.
• Early treatment with T4 results in normal IQ levels, but subtle neurodevelopmental abnormalities may occur in those with the most severe hypothyroidism at diagnosis or when treatment is delayed or suboptimal.

Autoimmune thyroiditis• Classification
– Hashimoto’s/Goitrous thyroiditis(goiter)– Atrophic thyroiditis(reducing residual gland)
• Subclinical vs overt/clinical hypothyroidism• Prevalence• Mean annual incidence 4 per 1000 women and 1 per 1000 men.
Subclinical hypothyroidism is found in 6–8% of women (10% over the age of 60) and 3% of men.
• More common in certain populations, such as Japanese, prob bse of genetic factors & chronic exposure to a high-iodine diet.
• The mean age at dx is 60 years, and prevalence of overt hypothyroidism increases with age.
• The annual risk of developing clinical hypothyroidism is about 4% when subclinical hypothyroidism is associated with positive TPO antibodies.
Pathophysiology of autoimmune thyroiditis
In Hashimoto's, • Marked lymphocytic
infiltration of the thyroid with germinal center formation,
• Atrophy of the thyroid follicles accompanied by oxyphil metaplasia, absence of colloid, and
• Mild to moderate fibrosis.
In atrophic thyroiditis• Lymphocyte infiltration is
less pronounced, • Thyroid follicles are almost
completely absent.• The fibrosis is much more
extensive

Pathophysio contd.• Susceptibility determined by a combination of genetic and environmental
factors, & risk of either autoimmune hypothyroidism or Graves' disease is increased among siblings.
• HLA-DR polymorphisms are the best documented genetic risk factors, especially HLA-DR3, -DR4, and -DR5 in Caucasians.
• Both of these genetic associations are shared by other autoimmune diseases, which may explain the relationship between autoimmune hypothyroidism and other autoimmune diseases, especially type 1 diabetes mellitus, Addison's disease, pernicious anemia, and vitiligo.
• Envtal factors poorly defined at present. A high iodine intake may increase the risk of autoimmune hypothyroidism by immunologic effects or direct thyroid toxicity.
• There is no convincing evidence for a role of infection except for the congenital rubella syndrome, in which there is a high frequency of autoimmune hypothyroidism. Viral thyroiditis does not induce subsequent autoimmune thyroid disease.

Pathophysio contd..• The lymphocytic infiltrate is composed of activated CD4+ and CD8+ T cells as well
as B cells. Thyroid cell destruction is primarily mediated by the CD8+ cytotoxic T cells, which destroy their targets. In addition, local T cell production of cytokines, such as TNF, IL-1, and IFN-gamma, may render thyroid cells more susceptible to apoptosis mediated by death receptors.
• These cytokines also impair thyroid cell function directly and induce the expression of other proinflammatory molecules by the thyroid cells themselves, such as cytokines, HLA class I and class II molecules, adhesion molecules, CD40, and nitric oxide.
• Antibodies to TPO and Tg are clinically useful markers of thyroid autoimmunity, but any pathogenic effect is restricted to a secondary role in amplifying an ongoing autoimmune response.
• Up to 20% of patients have antibodies against the TSH-R, which, in contrast to TSI, do not stimulate the receptor but prevent the binding of TSH. These TSH-R-blocking antibodies, therefore, cause hypothyroidism and, especially in Asian patients, thyroid atrophy. Their transplacental passage may induce transient neonatal hypothyroidism.

Clinical manifestations• Features of thyroid hormone deficiency. • May be associated with S&S of other autoimmune diseases, particularly
vitiligo, pernicious anemia, Addison's disease, alopecia areata, and type 1 DM• Less-common assoc include celiac disease, dermatitis herpetiformis, chronic
active hepatitis, rheumatoid arthritis, SLE, myasthenia gravis, and Sjögren's syndrome.
• Thyroid-associated ophthalmopathy, which usually occurs in Graves' disease, occurs in about 5% of patients with autoimmune hypothyroidism.
• Autoimmune hypothyroidism is uncommon in children and usually presents with slow growth and delayed facial maturation. The appearance of permanent teeth is also delayed. Myopathy, with muscle swelling, is more common in children than in adults. In most cases, puberty is delayed, but precocious puberty sometimes occurs. There may be intellectual impairment if the onset is before 3 years and the hormone deficiency is severe.

Differential diagnosis
• An asymmetric goiter in Hashimoto's thyroiditis may be confused with– multinodular goiter or – thyroid carcinoma, in which thyroid antibodies may also
be present. – Ultrasound can be used to show the presence of a
solitary lesion or a multinodular goiter rather than the heterogeneous thyroid enlargement typical of Hashimoto's thyroiditis.
– FNA biopsy is useful in the investigation of focal nodules.

Others causes of hypothyroidism
• Iatrogenic hypothyroidism is a common cause of hypothyroidism and can often be detected by screening before symptoms develop.
• In the first 3–4 months after radioiodine treatment, transient hypothyroidism may occur due to reversible radiation damage.
• Low-dose thyroxine treatment can be withdrawn if recovery occurs.
• Mild hypothyroidism after subtotal thyroidectomy may also resolve after several months, as the gland remnant is stimulated by increased TSH levels
Other causes contd…• Iodine deficiency is responsible for endemic goiter and cretinism but is
an uncommon cause of adult hypothyroidism unless the iodine intake is very low or there are complicating factors, such as the consumption of thiocyanates in cassava or selenium deficiency.
• Though hypothyroidism due to iodine deficiency can be treated with thyroxine, public health measures to improve iodine intake should be advocated to eliminate this problem. Iodized salt or bread or a single bolus of oral or intramuscular iodized oil have all been used successfully.
• Paradoxically, chronic iodine excess can also induce goiter and hypothyroidism. The intracellular events that account for this effect are unclear, but individuals with autoimmune thyroiditis are especially susceptible. Iodine excess is responsible for the hypothyroidism that occurs in up to 13% of patients treated with amiodarone.
• Other drugs, particularly lithium, may also cause hypothyroidism.

Other causes contd..
• Secondary hypothyroidism is usually diagnosed in the context of other anterior pituitary hormone deficiencies; – Isolated TSH deficiency is very rare. TSH levels may be low,
normal, or even slightly increased in secondary hypothyroidism; the latter is due to secretion of immunoactive but bioinactive forms of TSH. The diagnosis is confirmed by detecting a low unbound T4 level.
– The goal of treatment is to maintain T4 levels in the upper half of the reference range, because TSH levels cannot be used to monitor therapy.

Treatment of hypothyroidism
• Clinical hypothyrodism• If no residual thyroid function, the daily
replacement dose of levothyroxine is usually 1.6 g/kg body weight (typically 100–150 g)
• After trmt of Graves’ disease, lower replacement dose(75-125microg/d)
• Adult pts < 60 without evidence of heart disease may be started on 50–100 g levothyroxine (T4) daily
• Adherence must be ensured and follow-up measurement of TSH is recommended at annual intervals

Trmt contd
• Subclinical hypothyroidism• no universally accepted recommendations• but most recently published guidelines dont recommend
routine treatment when TSH levels are below 10 mU/L• Important to confirm that any elevation of TSH is sustained
over a 3-month period before treatment is given. There is a risk that patients will progress to overt hypothyroidism, particularly when the TSH level is elevated and TPO antibodies are present.
• Treatment is by starting with a low dose of levothyroxine (25–50 g/d) with the goal of normalizing TSH. If thyroxine is not given, thyroid function should be evaluated annually.

Trmt contd
• Special considerations• Pregnant women; The dose of levothyroxine may need to
be increased by 50% during pregnancy and returned to previous levels after delivery.
• Elderly patients may require 20% less thyroxine than younger patients
• In the elderly, esp pts with known CAD, starting dose of levothyroxine is 12.5–25 g/d with similar increments every 2–3 months until TSH is normalized
• Emergency surgery is gen safe in pts with untreated hypothyroidism, although routine surgery in a hypothyroid patient should be deferred until euthyroid

Myxedema coma
• Clinical manifestations include reduced LOC, sometimes assoc with seizures, as well as the other features of hypothyroidism
• Hypothermia can reach 23°C (74°F).• h/o poor compliance or undiagnosed hypothy• Almost always occurs in the elderly• Ppted by factors that impair respiration• Hypoventilation, leading to hypoxia and hypercapnia,
hypoglycemia and dilutional hyponatremia contribute to its devt

Trmt of myxedema
• Trmt; levothyroxine single IV 500mcg/day or ngt if iv failed
• Alternatively liothyronine iv or ngt 10-25mcg 8-12 hourly• Another option is to combine levothyroxine (200 g) and
liothyronine (25 g) as a single, initial IV bolus followed by daily treatment with levothyroxine (50–100 g/d) and liothyronine (10 g every 8 h).
• Supportive therapy(correct assoc metabolic disturb, external warming if temp<30, parenteral hydrocortisone 50mg every 6 hourly, trmt of ppting factor, ventilation support, hypertonic saline, glucose

Other abnormalities
• Thyroid binding site abnormalities; X-linked TBG deficiency, TBG levels are elevated by estrogen, drugs, Mutations in TBG, TTR(transthyretin), and albumin may increase the binding affinity for T4 and/or T3 and cause disorders known as euthyroid hyperthyroxinemia or familial dysalbuminemic hyperthyroxinemia